
Submitted:
09 August 2023
Posted:
10 August 2023
You are already at the latest version
Abstract
Background: Obtaining adipose-derived stem cells is limited by its capacity to differentiate. Stimulation by platelet-rich fibrin appears to have the beneficial effects to accelerate differentiation.
Objective: To obtain immunohistochemistry evidence of platelet-rich fibrin to accelerate differentiation of adipose-derived stem cells.
Methods: We used post-test only controlled-group design. Adipose-derived stem cells were isolated and cultured until 4 passages in α-MEM culture medium.
Results: GATA-4 expression increased in platelet-rich fibrin group compared with control group (68.20±6.82 vs 58.15±1.23 counts; p<0.05; 68.20±6.82 vs 52.96±2.02 counts; p<0.05). Troponin expression also increased in platelet-rich fibrin group (50.66±7.2 vs 10.73±2.39 counts; p<0.05; 50.66±7.2 vs 26.00±0.4 counts; p<0.05).
Conclusion: There is an immunohistochemistry benefit of platelet-rich fibrin to accelerate differentiation of adipose-derived stem cells into cardiomyocyte-like cells.
Keywords:
adipocyte-derived mesenchymal stem cells
; cardiomyocyte-like cells
; platelet rich fibrin
; growth factor
; stem cell therapy
INTRODUCTION
Coronary heart disease has a huge impact on age and quality of human life. Cardiomyocytes in adults have a limited capacity to regenerate after coronary heart disease. Where permanent damage to cardiomyocytes, loss of contraction function in the heart muscle and increased proliferation and turnover of fibroblast cells will lead to a progressive process of non-ischemic myocardial remodelling in the ventricles. And this remodelling process will cause progressive ventricular dilatation and lead to heart failure. Clinically there is no therapy that has the effect of regenerating myocardium in coronary heart disease. Therefore, cell therapy is the most ideal therapy for regeneration of damaged myocardium [1].
Bone marrow-derived MSCs (BMSCs) were the first cells to be recognized and most frequently studied in association with cardiovascular disease. Unfortunately, the use of BMSCs is invasive, painful, has a high morbidity rate and low success rate. On the other hand, adipocyte-derived mesenchymal stem cells (ADSCs) have an easier procedure and more promising results. It is said that ADSCs have better cell density than BMSCs (5% versus 0.1%) [2].
Growth factors play an important role in maintaining stem cell deficiency while blood derived growth factors and nutrients play an important role in stimulating stem cell proliferation. Platelets are the main source of growth factors that play a role in tissue regeneration. Platelet rich fibrin (PRF) is a new revolution in the concept of platelet therapy. Unlike platelet concentrates, this technique does not require a gelifying agent, but only centrifugation of natural blood without additives [3].
Several researchers believed that PRF contains a variety of growth factors which could stimulate stem cell proliferation and differentiation [4]. Transforming Growth Factor-β1 (TGF-β1) triggers fibrosis while Platelet-Derived Growth Factor (PDGF) contributes to mesenchymal cell migration and survival [5]. Insulin-Like Growth Factor-1 (IGF-1) prevents apoptosis, Vascular Endothelial Growth Factor (VEGF) stimulates vasculogenesis and angiogenesis and the function of Epidermal Growth Factor (EGF) in cell proliferation and differentiation [6]. PRF could assist MSC differentiation by forming a dynamic fibrin gel embedding platelets, leukocytes, type 1 collagen, osteocalcin, and providing slow release of several growth factors, accomplished by inhibition of both the extracellular receptor kinase and p38 mitogen-activated protein kinase pathway [7-8].
Although several studies have been conducted that prove the role of platelets and the growth factors contained therein in the differentiation process, there is no study that discusses the effect of adding PRF to ADSCs differentiation, so in this study researchers wanted to find out whether the addition of PRF could have an effect on ADSCs proliferation through further observations [9-12].
ADSCs express markers of MSCs, namely CD10, CD13, CD29, CD34, CD44, CD54, CD71, CD90, CD105, CD106, and CD117. ADSCs do not express hematopoietic cell lineage markers such as CD45, CD14, CD16, CD56, CD61, CD62E, CD104, and CD106; and also endothelial cell lineages namely CD31, CD144, and von Willebrand factor. Morphologically, these cells are like fibroblasts and retain their shape after expansion in vitro. The similarity between ADSCs and BMSCs suggests that ADSCs originate from circulating BMSCs that infiltrate into the adipose compartment through the vessel wall [13].
We used GATA-4 and Troponin T in this experiments. Immature, proliferative cardiomyocytes create a high demand for nucleotide biosynthesis, which is suppressed after cardiomyocytes mature. GATA-4 is a cardiac transcription factor and plays an important role in promoting myocardial transdifferentiation during early cardiomyogenesis. Conversely, high-glucose promotes nucleotide biosynthesis through the pentose phosphate pathway and inhibits cardiomyocyte maturation. Because cardiomyocyte maturation involves a remarkable increase of protein-built components, such as myofibrils, and extensive expansion of lipid bilayers in T-tubules, SR and mitochondria, protein and lipid biosynthesis are also expected to be highly active. Large poorly differentiated c-kit+ colony positive to Troponin T was identified in the mature myocardium.
OBJECTIVE
This research aimed to analyse the benefit of injectable platelet-rich fibrin to accelerate differentiation of adipose-derived mesenchymal stem cells into cardiomyocyte-like cells, as expressed by level of GATA-4 and Troponin.
METHODOLOGY
Ethical approval
This research had been obtaining an ethical approval from Institutional Review Board of Dr. Soetomo Academic General Hospital - Faculty of Medicine, Airlangga University (Institution Review Board number: IORG0007195; Reference Number: 1733/KEPK/XII/2019) issued on December 27th, 2019.
Preparation of platelet concentrates
The platelet concentrates including PRP and PRF were prepared according to a manufacture’s instruction. Briefly, 5 mL of whole blood was centrifuged for 10 min at 1000 rpm (45 G) at room temperature without brake (Centrifuge 5804 R; Eppendorf, Germany). The plasma rum was decanted up to the red blood cell sediment and then centrifuged again for 10 min at 5000 rpm (400 g) at 4 °C. Finally, the PRP was decanted and the final PRP sediment was suspended. For preparation of fresh PRF, 10 mL of whole blood was immediately centrifuged at 3000 rpm for 10 min at 4 °C and the fresh PRF clots identified as the middle layer.
Study design
This research is an experimental laboratory study (in vitro study) with the administration of plasma rich fibrin (PRF) in ADSCs culture. Where this study aims to determine the effect of the addition of PRF on the ability of ADSCs to differentiate into cardiomyocyte-like cells. This type of research is true experimental with randomized randomization with a "post-test only control group design" approach.
Study setting
This research is a laboratory research that will be conducted at the Stem cell Laboratory, Centre for Biomaterials and Tissue Bank, Dr. Soetomo Academic General Hospital. This research was conducted for between 1 January 2020 - 31 December 2021.
Sample size
Our sample comes from 1 donor but replicated into 3 groups of treatment and each group n=3. In this type of experimental research, there are 3 principles of processing research samples. Namely randomization, replication and control. In this study, these three principals were applied. Randomization was carried out before the research sample was divided into three groups. Furthermore, replication was carried out 3 times (triplications) after the research sample was divided into three groups. The principle of replication is to increase the accuracy of research results with minimal sample variation. Where, when applied to the principle of statistical data processing, replication must be carried out at least three times, this is done so that the calculation of the standard deviation can be carried out. This is in accordance with the principle of Triplicate calculation. Then the addition of control is done with negative control and positive control.
Materials
- Adipose-derived mesenchymal stem cells (ADSCs), namely mesenchymal stem cells (MSCs) obtained from minimal surgery procedures.
- Bio Safety Cabinet class II
- Centrifuge
- Inverted Microscope
- CO2 Incubator
- Pipette aid and micropipette
- Water bath
- Hot plate magnetic stirrer
- Dissecting set
- Vacuum pump
- 500 mL Beaker glass
- -MEM medium
- Phosphate buffer saline (PBS) with fetal bovine serum (FBS)
- Triple express
- Collagenase
- NaHCO3
- Trypan Blue
- 70% Alcohol
- 15 mL and 50 mL conical tube
- 5 cm dan 10 cm petri dish
- 24 wells and 12 wells of microplate
- Unit filter 0,22 μm (Millipore)
- CD34, CD45, CD105 staining
- GATA-4 antibody
- cTnT antibody
- Cardiomyocyte differentiated medium MSDS (SCM102; Sigma Aldrich; material safety data sheet)
- Platelet Rich Fibrin
Experimental procedures
This research was conducted through 5 stages, which can be explained as follows:
- Isolation and culture of ADSCs from adipose tissue obtained from minimal surgery procedures. Retrieval of ADSCs are accomplished from direct lipectomy using minimal invasive surgical procedures. Freshly obtained raw fat is washed with lactated Ringer’s solution to remove contaminating blood and remaining tumescent solution. The non-buoyant nucleated cells are proteolytically released from the adipose matrix by adding a solution 0.075 % Collagenase I dissolved in α -MEM medium is used to obtain 0.075 % Collagenase I (1 % penicillin/streptomycin) solution. Two other solutions are prepared, a red cell lysis and a growth media solution. To prepare the former, solid NH4Cl is dissolved in distilled water at 160 mM and vacuum sterilized with a 0.22 μm filter prior to aliquoting. The growth media is prepared by adding 10 % FBS and 1 % penicillin/streptomycin solution to α-MEM medium and sterile filtering. Both of these solutions are stored at 4 °C. The supernatant is discarded and, if the red blood cell lysis is desired, the cell pellet is resuspended in 2 mL of 160 mM NH4Cl to lyse any remaining red blood cells. The tubes are then incubated at room temperature for 10 min. Additional NH4Cl were added to lyse any remaining red blood cells. The admixture is centrifuged at 3,300 rpm for 10 min to re-pellet the ADSC-rich fraction; the supernatant is aspirated and the pellet resuspended in 5 mL of growth media. Next, the cell suspension is passed through a 70–100 μm cell strainer to eliminate major acellular debris and then rinsed with 5 mL additional growth media.
- Identification of ADSCs from adipose tissue by Flow Cytometry by observing the expression of CD 105 and the non-expression of CD 34 and CD 45.
- Culture of ADSCs on α −MEM medium and differentiation of cardiomyocytes. For culture, the suspension is plated into T-75 (75 cm2) tissue culture flasks at a density of 100,000 cells/cm2 (approximately 1 flask for every ~6 mL of fat used). The flasks are labeled to indicate that this is the primary isolation passage (P = 0) and incubated overnight at 37 °C in a humidified incubator with 5 % CO2. After 24 h, the media from the flasks is aspirated and rinsed twice with warm PBS before fresh growth media is added. After 7–10 days the cells will reach 70–80 % confluency and should be passaged or frozen. They should not be allowed to reach 100 % confluency, as this can stimulate differentiation of the cells.
- Preparation and administration of PRF in in vitro cultured ADSCs in treatment group
- Evaluation of tissue culture of ADSCs in the three groups with flowcytometry for GATA-4 and Immunocytochemistry for cTnT
Cells counting
Slices were incubated with several primary antibodies for GATA-4 and cTnT overnight at 4 °C, subsequently incubated with respective secondary antibodies for 1 h at room temperature, and finally counterstained with DAB Chromogen (for the cytoplasm) and Meyer Hematoxylin (for the nucleus). An LSM880 Meta confocal microscope (Carl Zeiss, Feldbach, Switzerland) was utilized for confocal images. For quantification, five random fields in each section were counted with Image J.
Statistical analysis
In this study, due to the number of samples < 30, the Shapiro Wilk test was used to test the normality of data. Data will be analysed inferentially using one way ANOVA if the data is normally distributed, or using the Kruskal-Wallis test if the data is not normally distributed. To analyse the differences between the two groups (post hoc) will use the Tukey if the data is normally distributed, or Mann-Whitney if the data is not normally distributed. The limit of significance is p=0.05.
RESULTS
Isolation and culture of ADSCs
ADSCs were isolated from adipose tissue, extracted by minimally invasive surgical method. This isolation procedure is adjusted to the standard stem cell laboratory at the Stem cell Laboratory, Centre for Biomaterials and Tissue Bank, Dr. Soetomo Academic General Hospital. After isolation, ADSCs were cultured and expanded up to the 4th passage with the aim of maintaining the stemness properties of ADSCs and avoiding further cell differentiation. The majority of cells were seen with a spindle-like shape as seen in the Supplementary material 1.
Phenotype Characterization of ADSCs
Based on the minimum criteria for the characterization of MSCs by The International Society for Cellular Therapy (ISCT), the majority of cells showed positive expression of CD73, CD90, and CD105, and negative expression of CD11b or CD14, CD19, CD34, CD45, and HLA-DR. In this study, ADSCs that had been taken from adipose tissue were examined for characterization of MSCs in the 4th passage culture. ADSCs culture showed positive expression of CD105+ and negative expression of CD34- and CD45- by Flow Cytometry examination. Phenotype identification is based on cell morphology viewed by an inverted microscope (x100 magnification) as the overall results can be seen in the Supplementary material 2.
Assessment of GATA-4 differentiation marker cardiomyocyte-like cells differentiation with flowcytometry
GATA-4 examination at the cardiomyocyte-like cells differentiation stage was carried out on day 5 because ADSCs already appeared confluent. To find out the difference test between the three groups, it begins with a distribution test to determine the normality of the distribution of the value data. Data normality test was performed using Shapiro Wilk. The distribution of the data is said to be normal if the p value > 0.05, in this study the data was normally distributed with the p value = 0.118.
From the results of the flowcytometry examination of the three groups, the ratio data of GATA-4 compared to the unexpressed GATA-4 in the ADSCs group was an average of 58.1467 + 1.23 % in the negative control group (α-MEM) (Figure 1); 52.9633 + 2.02 % in the positive control group (medium of differentiation) (Figure 2); and 68.20 + 6.82 % in the treatment group (medium of differentiation + PRF) (Figure 3). This result shows that the treatment group is superior to the negative control group and the positive control group is judged by the average ratio.
Because the distribution of the data is normal, ANOVA test was carried out to determine the difference between the three sample groups with p = 0.011. This shows that there is a significant difference in the ratio of GATA-4 (upper right quadrant) compared to unexpressed GATA-4 (lower right quadrant) between the three groups. While the T-test was conducted to determine the difference between the two groups. There were significant differences between the negative control group (α-MEM) compared to the treatment group (differentiation medium + PRF) and the positive control group (differentiation medium) compared to the treatment group (differentiation medium + PRF) with p<0.05. However, there was no significant difference between the negative control group (α-MEM) compared to the positive control group (medium of differentiation) with p=0.179 (Figure 4).
Assessment of expression of cardiomyocyte-like cells differentiation marker Troponin by Immunocytochemistry
Cardiac Troponin T (cTnT) is a late marker of cardiomyocyte-like cells that begins to be detected on day 10. On the day-10 of treatment, the three groups were assessed for immunocytochemical marker expression of cTnT. On immunocytochemistry examination, the determination of cardiomyocyte cells was morphologically visualized by staining the cytoplasm by DAB Chromogen and staining the nucleus by Meyer Hematoxylin. Description of cardiomyocyte-like cells appear more prominent than other cells, with prominent blue nuclei and prominent brown cytoplasm. In the three groups, the accumulation of cardiomyocyte-like cells per visual field was calculated. To find out the difference test between the three groups, it begins with a distribution test to determine the normality of the distribution of the value data. Due to the number of samples < 30, the data normality test used was Shapiro Wilk. The distribution of the data is said to be normal if the p>0.05, in this study the distribution of the data is normal with the p=0.315.
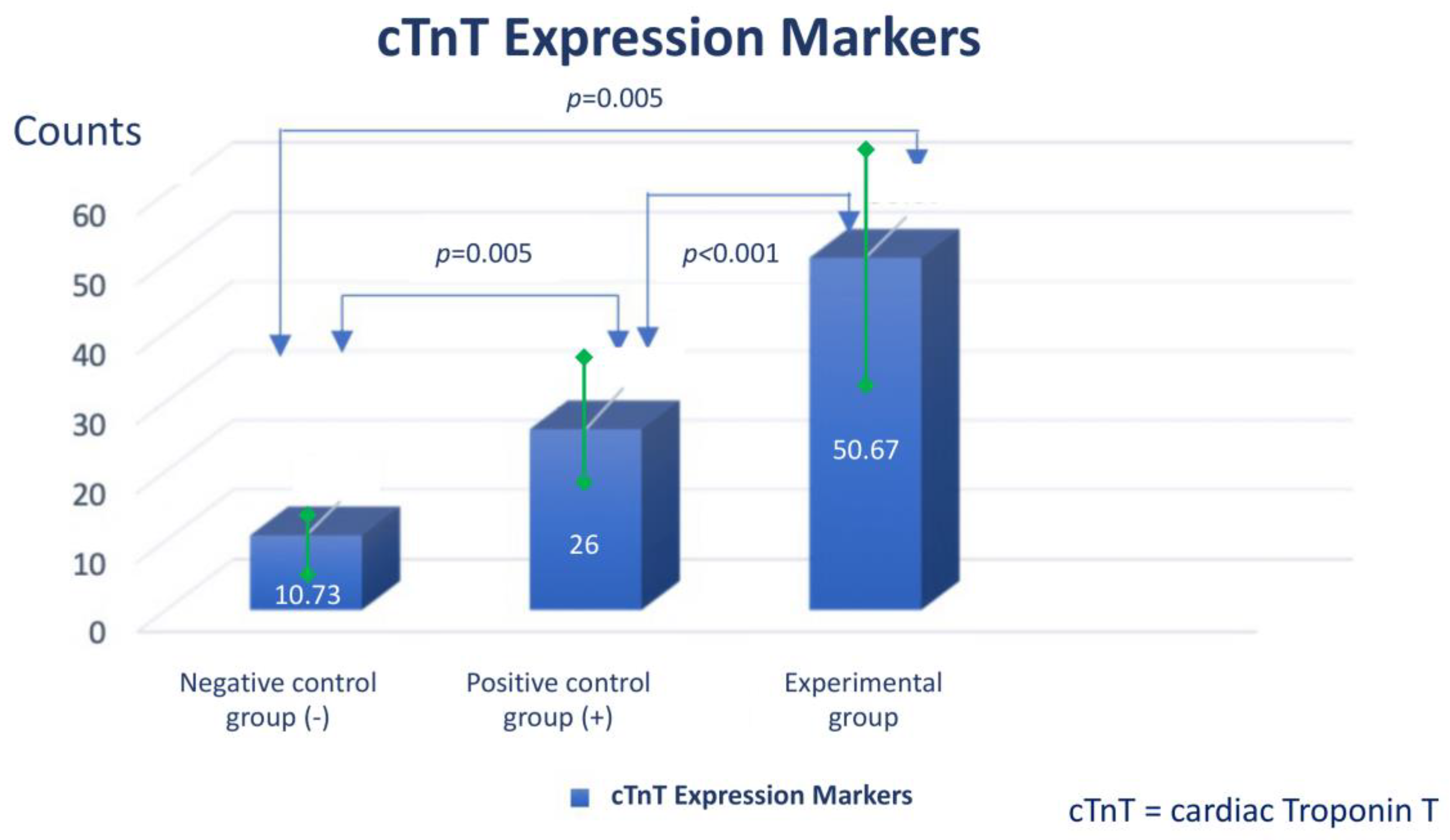
From the results of the immunocytochemistry examination of the three groups, the data obtained an average of 10.73 + 0.3 % in the negative control group (α-MEM) (Figure 5); 26.00 + 0.4 % in the positive control group (medium of differentiation) (Figure 6); and 50.6 + 7.2 % in the treatment group (differentiation medium + PRF) (Figure 7). This shows that the treatment group is superior when compared to the negative control group and the positive control group based from the mean cTnT expression.
Because the data were normally distributed, ANOVA test was carried out to determine the difference between the three sample groups with p=0.0001. This shows that there is a significant difference in the mean of cardiomyocyte-like cells expressed with troponin between the three groups. While the T-test was conducted to determine the difference between the two groups. There were significant differences between the negative control group (α-MEM) compared to the treatment group (differentiation medium + PRF), the negative control group (α-MEM) compared to the positive control group (differentiation medium), and the positive control group (differentiation medium). compared with the treatment group (medium of differentiation + PRF) with p<0.05 (Figure 8).
DISCUSSION
In the previous study by Mazini et al (2019), it was found that ADSC has a good self-renewal and differentiation abilities raise great interest in cell-based therapy. The most useful characteristic reported for ADSC is being the non-immunogenic profile compared to Bone Marrow. Interestingly, ADSC secrete different chemokines and cytokines and extracellular matrix (ECM) proteins that are involved in various biological process, including hematopoiesis, angiogenesis, leukocyte trafficking, immune, and inflammatory responses [14].
Platelet-rich fibrin (PRF) was firstly introduced with the overall aim to increase the number of platelets and leucocytes. The important things is that PRF could be an interesting additional substances in the stem cell formula in the field of regenerative cardiovascular medicine. PRF can be obtained from natural coagulation after being separated from the red thrombus by centrifugation. During centrifugation process, the beginning of PRF started from the introduction of L-PRF, A-PRF and injectable PRF (~ 60 g for 3 min) with lower g-forces centrifugation times [15].
PRF can affect central signalling pathways, possesses an anti-inflammatory effect, and is capable of cardiomyogenesis. Addition of PRF could stimulate various growth factors in mesenchymal and endothelial cells such as TGFβ, PDGF, and VEGF. PRF enhanced the phosphorylation of Akt, heat shock protein 47 and lysis oxidase. [15].
In this study, two examinations were carried out at the stage of differentiation of cardiomyocyte-like cells. In the first examination, namely at the cardiac progenitors stage in the treatment group that assessed GATA-4 expression by flow cytometry, it showed a significant increase in the PRF group compared to the negative control group and the positive control group (68.20 ± 6.82 vs 58.15 ± 1.23 p<0.05; 68.20 ± 6.82 vs. 52.96 ± 2.02 p<0.05). And in the second examination, namely at the stage of mature cardiomyocyte-like cells assessing troponin expression with immunocytochemistry showed a significant increase in the PRF group compared to the negative control group and positive control group (50.66 ± 7.2 vs 10.73 ± 2.39 p<0.05; 50.66 ± 7.2 vs 26.00 ± 0.4 p< 0.05). This is in accordance with the research hypothesis which states that there is an effect of adding PRF to the differentiation of ADSCs into cardiomyocyte-like cells.
Adipose tissue is a potential source of adult stem cells that can perform multipotent differentiation. Where adipose-derived mesenchymal stem cells (ADSCs) have very similar properties to bone marrow-derived MSCs including the ability to differentiate into osteoblasts, adipocytes and chondrocytes under certain in vitro conditions. Similar to other mesenchymal stem cells, various studies have shown that ADSCs have the potential to undergo adipogenesis, chondrogenesis, osteogenesis, myogenesis, and vasculogenesis. Because MSCs have many surface antigens, the International Society of Cellular Therapy (ISCT) in 2006 determined the minimum criteria for defining the culture of MSCs, namely (a) having plastic adherent properties on standard culture media, (b) positive expression of CD73, CD90, and CD105 , and negative expression of CD11b or CD14, CD19 or CD79a, CD45, and HLA-DR, and (c) have the potential for differentiation into adipocytes, chondrocytes, and osteoblasts using staining in in vitro cell cultures. This study used the expression phenotype characteristics of CD105+, CD34- and CD45- on ADSCs cultured in Passage-4 by flow cytometry technique. This is in accordance with the minimum criteria for the characterization of MSCs presented by ISCT [16].
Coronary heart disease among other cardiovascular diseases has a very large influence on age and quality of human life. Cardiomyocytes in an adult have a limited capacity to perform regeneration after coronary heart disease. Where permanent damage to cardiomyocytes, loss of contraction function in the heart muscle and increased proliferation and turnover of fibroblast cells will lead to a progressive process of non-ischemic myocardial remodelling in the ventricles [9]. And this remodelling process will cause progressive ventricular dilatation and result in heart failure. Clinically there is no therapy that has the effect of regenerating myocardium in coronary heart disease. Therefore, cell therapy is the most ideal therapy for regeneration of damaged myocardium [17].
Platelet rich blood derivatives have been widely used in various fields of medicine and stem cells for tissue engineering because of their consistent ability to increase the potential for proliferation, migration and differentiation of stem cells. Platelet rich fibrin (PRF) is a new revolution in the concept of platelet therapy. Unlike platelet concentrates, this technique does not require a jellifying agent, but only centrifugation of natural blood without additives [18-21]. Platelets are composed of granules including alpha granules, dense granules, and glycogen granules. Alpha granules are the main granules that contribute to wound healing through the various growth factors contained in it. Growth factors present in PRF include platelet derived growth factor (PDGF), transforming growth factor-β1 (TGF-β1), vascular endothelial growth factor (VEGF), insulin like growth factor-1 (IGF-1), epidermal growth factor (EGF), fibroblasts growth factor and others [22].
The factor reaches the target cell and binds to transmembrane receptors and activates various intracytoplasmic proteins causing actions related to gene expression that have effects such as cell mitosis or collagen production. With the high content of growth factors possessed by PRF and the simplicity of manufacture, PRF can be an alternative for use in the field of cell therapy. Unfortunately, there are no studies linking the benefits of PRF with cardiomyocyte-like cells differentiation. This is what underlies this research. In previous studies, the optimum concentration of PRF varied from 50%, 10%, to less than 1%. Soffer et al, suggested a PRF of 0.5-1% as the optimum concentration for the rate of cell proliferation and mineralization [23]. However, Ferreira et al, found that 2% PRF was the optimum concentration for osteoblast proliferation [24]. In addition, Castegnaro et al. (2011) reported that 10% PRF was sufficient to induce cell proliferation in MSCs derived from adipose tissue [25]. In the study of Govindasamy et al. (2011), 2% platelet lysate was referred to as the optimal concentration for mesenchymal stem cell and dental pulp stem cell proliferation and osteogenesis [26]. Research conducted by Kang et al. (2011) stated that 2% PRF extract can increase the proliferation of human alveolar bone marrow stem cells (hABMSCs) [27]. In this study, the treatment group was given PRF with a concentration of 2%.
Similar to other mesenchymal stem cells, various studies have shown that ADSCs have the potential to undergo adipogenesis, chondrogenesis, osteogenesis, myogenesis, and vasculogenesis. Where are the various reagents from the previous study could induce ADSCs differentiation into cardiomyocyte-like cells including 5-azacytidine (5-Aza), angiotensin II (Ang II), and transforming growth factor- (TGF- 1). In a study conducted by Safwani et al, in 2011 it was stated that 5-Aza was not effective for inducing cardio genesis in ADSCs. Therefore, in this study, it is suggested that the addition of growth factors is believed to help the induction of ADSCs. A study conducted by Planat Barnard et al, in 2004 confirmed that the use of growth factors for cardiomyocyte-like cells differentiation is necessary [27].
The role of platelets in cardiomyocyte-like cells differentiation is said to lie in the growth factors contained therein. Where platelet activation that occurs in the cardiac recovery phase after ischemic damage causes the release of the alpha-granule component which is the main content of platelets which will mediate the formation of cardiac progenitor cells to become mature cardiomyocyte-like cells [28].
CONCLUSION
The addition of injectable platelet-rich fibrin could accelerate differentiation of adipose-derived mesenchymal stem cells into cardiomyocyte-like cells. It can be seen by increasing the expression of GATA-4 and Troponin. However, further research is needed by examining markers at each stage of cardiomyocyte formation starting from cardiac mesoderm to mature cardiomyocyte-like cells.
SUMMARY POINTS
- ▪
- Before the beginning of the cell therapy and transplantation era, clinically there is no therapy for permanent damage of cardiomyocytes that has the effect of stimulate regenerating myocardium
- ▪
- Platelet-rich fibrin contains a variety of growth factors, thus can affect central signalling pathways, possesses an anti-inflammatory effect, and is capable of cardiomyogenesis
- ▪
- The addition of injectable platelet-rich fibrin appears to have benefit to accelerate the differentiation from adipose-derived mesenchymal stem cells into cardiomyocyte-like cells, as can be seen by increasing the expression of GATA-4 and Troponin.
- ▪
-
Author Contributions: please list the contributions of each author to the piece; please refer to the Author Disclosure Form for our authorship criteria.
- o
- I Gde Rurus Suryawan1* : Conceptualization, Funding, Methodology, Supervision
- o
- Andrianto2 : Project administration, Visualization, Supervision
- o
- Arisya Agita3 : Data curation, Methodology
- o
- Anudya Kartika Ratri4 : Writing – Original Draft
- o
- Ricardo Adrian Nugraha5 : Writing – Original Draft, Statistical analysis
- ▪
- Acknowledgements: We would like to show our gratitude to Prof. Dr. Fedik Abdul Rantam as Consultant of Stem Cell at Tissue Bank, Dr. Soetomo Academic General Hospital and Prof. Dr. Maria Inge Lusida as Head of Institute of Tropical Disease, Universitas Airlangga for sharing their pearls of wisdom with us during the writing process, for their comments on the later version of the manuscript, although any errors are our own and should not tarnish the reputations of these esteemed persons. We would also like to thank for anonymous residents and staffs from Department of Cardiology and Vascular Medicine, Faculty of Medicine Universitas Airlangga - Dr. Soetomo Academic General Hospital for their technical contribution and so-called insights.
- ▪
- Financial disclosure: None declared.
- ▪
- Information pertaining to writing assistance: None declared.
- ▪
- Ethic statement: This research had been obtaining an ethical approval from Institutional Review Board of Dr. Soetomo Academic General Hospital - Faculty of Medicine, Airlangga University (Institution Review Board number: IORG0007195; Reference Number: 1733/KEPK/XII/2019) issued on December 27th, 2019.
- ▪
- Informed consent: Written informed consent had been obtained from study participants.
- ▪
- Data sharing statement: The data that support the findings of this study are available from the corresponding author upon reasonable request.
- ▪
- Plain language summary (PLS; within article):
- ▪
- It is difficult to grow and differentiate adult stem cells such as adipose derived stem cells, to achieve perfect cardiac regeneration therapy.
- ▪
- There is a major difference between platelet-rich plasma (PRP) and platelet-rich fibrin (PRF). PRP injections are created by isolating the platelets from a patient's blood and concentrating them into a serum. PRF injections, on the other hand, are created by adding a fibrin matrix to the platelets, which creates a more cohesive and stable injectable product.
- ▪
- Our experiment try to evaluate the benefit of platelet-rich fibrin in various clinical scenarios, especially to grow cardiomyotes-like cells, with positive GATA-4 and Troponin expression.
- ▪
- Tweetable abstract: How to Improve Differentiation of Cardiomyocytes-like Cells Faster with the Addition of Injectable Platelet-Rich Fibrin in the Cell Cultures
- ▪
- Ethic statement: This research had been obtaining an ethical approval from Institutional Review Board of Dr. Soetomo Academic General Hospital - Faculty of Medicine, Airlangga University (Institution Review Board number: IORG0007195; Reference Number: 1733/KEPK/XII/2019) issued on December 27th, 2019.
- ▪
- Informed consent: Written informed consent had been obtained from study participants.
References
- Soltani L, Rahmani H, Joupari MD et al. Effects of 5-Azacytidine on Differentiation of Ovine Mesenchymal Stem Cells. Int. J. Stem. Cell. Res & Transplant. 3(02), 96–100 (2015). * (this study is interesting because 5-azacytidine in culture of hMSCs for 28 days could induce differentiation towards cardiomyogenic lineage, whereas same cultural condition for a period of 24h lead to cardiac-like muscle cells).
- Ma T, Sun J, Zhao Z et al. A brief review: adipose-derived stem cells and their therapeutic potential in cardiovascular diseases. Stem. Cell. Res & Ther. 8(1), 1–8 (2017). [CrossRef]
- Castro F, Munozledo. The Mammalian limbal Stem Cell Niche : A Complex Interaction Between Cells, Growth Factors and Extracellular Matrix. Switzerland : Springer International Publishing. 23-56 (2015).
- Miron R, et al. Platelet rich fibrin and soft tissue wound healing: a systematic review. Issue Eng Part B Rev. 23, 83–99 (2016). [CrossRef]
- Al-Khawlani E, et al. Evaluation of platelet-rich fibrin versus platelet-rich plasma on the outcome of mandibular fracture: a comparative study. Egypt J Oral Maxillofac Surg. 5, 96–102 (2014).
- Miron RJ, et al. Platelet-rich fibrin and soft tissue wound healing: a systematic review. Tissue Eng Part B Rev. 23, 83–99 (2017). [CrossRef]
- Neiva RF, et al. The synergistic effect of leukocyte platelet-rich fibrin and micrometer/nanometer surface texturing on bone healing around immediately placed implants: an experimental study in dogs. Biomed Res Int. 2016. [CrossRef]
- Duan X, Lin Z, Lin X et al. Study of platelet-rich fibrin combined with rat periodontal ligament stem cells in periodontal tissue regeneration. J. Cel. & Mol. Med. 22(2), 1047-1055 (2017).* (this study is interesting because this is one of the most earliest study to use platelet-rich fibrin combination to enhance stem cell regeneration).
- Apte RS, Chen DS, Ferrara N. VEGF in signaling and disease: beyond discovery and development. Cell. 176, 1248–64 (2019). [CrossRef]
- Priyadarshini et al published P, Samuel S, Kurkalli BG, Kumar C, Kumar BM, Shetty N, Shetty V, Vishwanath K. In vitro Comparison of Adipogenic Differentiation in Human Adipose-Derived Stem Cells Cultured with Collagen Gel and Platelet-Rich Fibrin. Indian J Plast Surg. 2021 Aug 26;54(3):278-283. [CrossRef]
- Bagheri-Hosseinabadi, Z., Salehinejad, P. & Mesbah-Namin, S.A. Differentiation of human adipose-derived stem cells into cardiomyocyte-like cells in fibrin scaffold by a histone deacetylase inhibitor. BioMed Eng OnLine 16, 134 (2017). [CrossRef]
- Badimon L, Oñate B, Vilahur G. Adipose-derived Mesenchymal Stem Cells and Their Reparative Potential in Ischemic Heart Disease. Rev Esp Cardiol (Engl Ed). 2015 Jul;68(7):599-611. (embedded AD-MSCs in PRF)) in the main manuscript to discuss the background of your work further; then proceed to clarify the novelty of your work.”. [CrossRef]
- Zuk PA and Zhu M. Human Adipose Tissue Is a Source of Multipotent Stem Cells. The. Am. Society. For. Cell. Bio. (2002).
- Mazini L, Rochette L, Amine M et al. Regenerative Capacity of Adipose Derived Stem Cells (ADSCs), Comparison with Mesenchymal Stem Cells (MSCs). Int. J. Mol. Sci. 20(10), 2523 (2019). [CrossRef]
- Strauss FJ, Nasirzade J, Kargarpoor Z et al. Effect of platelet-rich fibrin on cell proliferation, migration, differentiation, inflammation, and osteoclastogenesis: a systematic review of in vitro studies. Clin. Oral. Investig. 24(2):569-584 (2020). [CrossRef]
- Dominici M, Le Blanc K, Mueller I et al. Minimal Criteria for Defining Multipotent Mesenchymal Stromal Cells. The International Society for Cellular Therapy Position Statement. Cytotherapy 8(4), 315–317 (2006). [CrossRef]
- Talman V and Ruskoaho H. Cardiac fibrosis in myocardial infarction—from repair and remodeling to regeneration. Cell. Tissue. Res. 365(3), 563–581 (2016). [CrossRef]
- Hashimoto H, Olson EN, Bassel-Duby R. Therapeutic approaches for cardiac regeneration and repair. Nat. Rev. Cardiol. 15(10), 585–600 (2018). [CrossRef]
- Masoudi E, Ribas J, Kaushik G et al. Platelet-Rich Blood Derivatives for Stem Cell-Based tissue Engineering and Regeneration. Current. Stem. Cell. Reports. 2(1), 33-42 (2016). [CrossRef]
- Meshram VS, Lambade PN, Tiwari ST. The Autologous Platelet Rich Fibrin: A novel approach in osseus regeneration after cystic enucleation: A pilot study. Ind. J. Dental. Res. 26, 560- 564 (2015). [CrossRef]
- Naik B, Karunakar P, Jayadev M et al. Role of Platelet richfibrin in wound healing : A critical review. J. Conservatives. Dentist. 16(4) (2013). [CrossRef]
- Shah R, Triveni MG, Thomas R, et al. An Update on the Protocols and Biologic Actions of Platelet Rich Fibrin in Dentistry. Eur. J. Prosthodontics. & Restorative. Dentist. 25, 64-72 (2017).
- Soffer E, Ouhayoun JP, Anagnostou F. Fibrin sealants and platelet preparations in bone and periodontal healing. Oral. Surg. Oral. Med. Oral. Pathol. Oral. Radiol. Endod. 95(5), 521-8 (2003). [CrossRef]
- Ferreira JR, Teixeira GQ, Santos SG et al. Mesenchymal Stromal Cell Secretome: Influencing Therapeutic Potential by Cellular Pre-conditioning. Front. Immunol. 9, 2837 (2018). [CrossRef]
- Castegnaro S, Chieregato K, Maddalena M et al. Effect of platelet lysate on the functional and molecular characteristics of mesenchymal stem cells isolated from adipose tissue. Curr. Stem. Cell. Res. Ther. 6(2), 105-14 (2011) * (this study is interesting because human platelet lysate tends to share similar properties with platelet-rich fibrin in term of non-hematopoietic, adult, fibroblast-like, multipotent cells that are plastic adherent in standard culture conditions). [CrossRef]
- Govindasamy V, Ronald VS, Abdullah AN et al. Differentiation of dental pulp stem cells into islet-like aggregates. J. Dent. Res. 90(5), 646-52 (2011). * (this study is interesting when studying a step and protocol to isolated, propagated, and characterized stem cells). [CrossRef]
- Planat-Benard V, Silvestre JS, Cousin B et al. Plasticity of human adipose lineage cells toward endothelial cells: physiological and therapeutic perspectives. Circulation. 109(5), 656-63 (2004). [CrossRef]
- Walsh TG, Poole AW. Platelets Protect Cardiomyocytes from Ischaemic Damage. TH Open. 1(1), e24-32 (2017) * (this study is interesting because we could learn that components of stromal cell-derived factor (SDF)-1α and transforming growth factor (TGF) β1 in the platelet exhibit cardioprotective effects. [CrossRef]
Figure 1.
Flowcytometry of GATA-4 in the negative control group (α-MEM). From the results of the flowcytometry examination, the ratio data of GATA-4 compared to the unexpressed GATA-4 in the ADSCs group was an average of 58.1467 + 1.23 counts in the negative control group (α-MEM).
Figure 1.
Flowcytometry of GATA-4 in the negative control group (α-MEM). From the results of the flowcytometry examination, the ratio data of GATA-4 compared to the unexpressed GATA-4 in the ADSCs group was an average of 58.1467 + 1.23 counts in the negative control group (α-MEM).
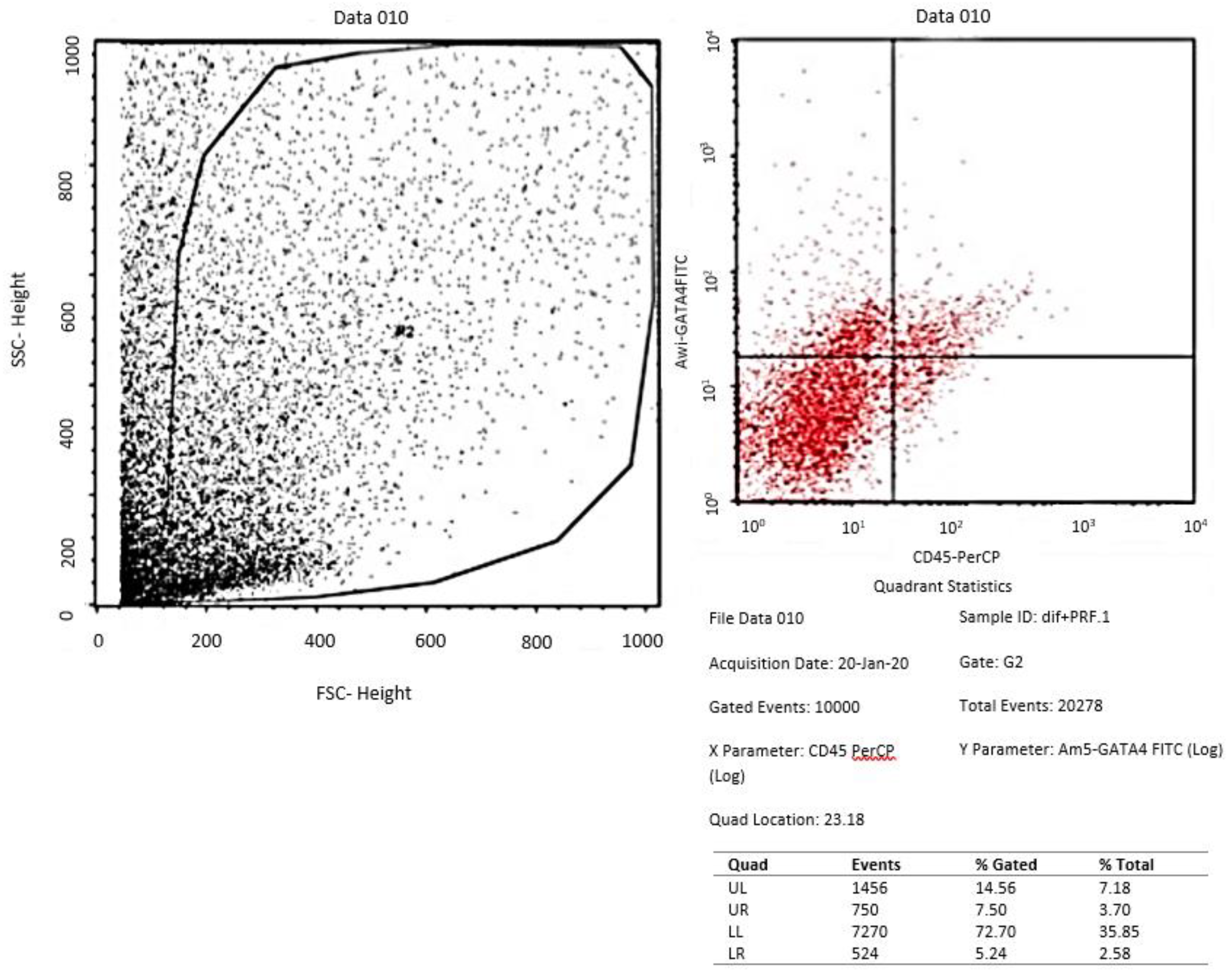
Figure 2.
Flowcytometry of GATA-4 in the positive control group (medium of differentiation). From the results of the flowcytometry examination, the ratio data of GATA-4 compared to the unexpressed GATA-4 in the ADSCs group was an average of 52.9633 + 2.02 counts in the positive control group (medium of differentiation).
Figure 2.
Flowcytometry of GATA-4 in the positive control group (medium of differentiation). From the results of the flowcytometry examination, the ratio data of GATA-4 compared to the unexpressed GATA-4 in the ADSCs group was an average of 52.9633 + 2.02 counts in the positive control group (medium of differentiation).

Figure 3.
Flowcytometry of GATA-4 in the treatment group (medium of differentiation + PRF). From the results of the flowcytometry examination, the ratio data of GATA-4 compared to the unexpressed GATA-4 in the ADSCs group was an average of 68.20 + 6.82 counts in the treatment group (medium of differentiation + PRF).
Figure 3.
Flowcytometry of GATA-4 in the treatment group (medium of differentiation + PRF). From the results of the flowcytometry examination, the ratio data of GATA-4 compared to the unexpressed GATA-4 in the ADSCs group was an average of 68.20 + 6.82 counts in the treatment group (medium of differentiation + PRF).
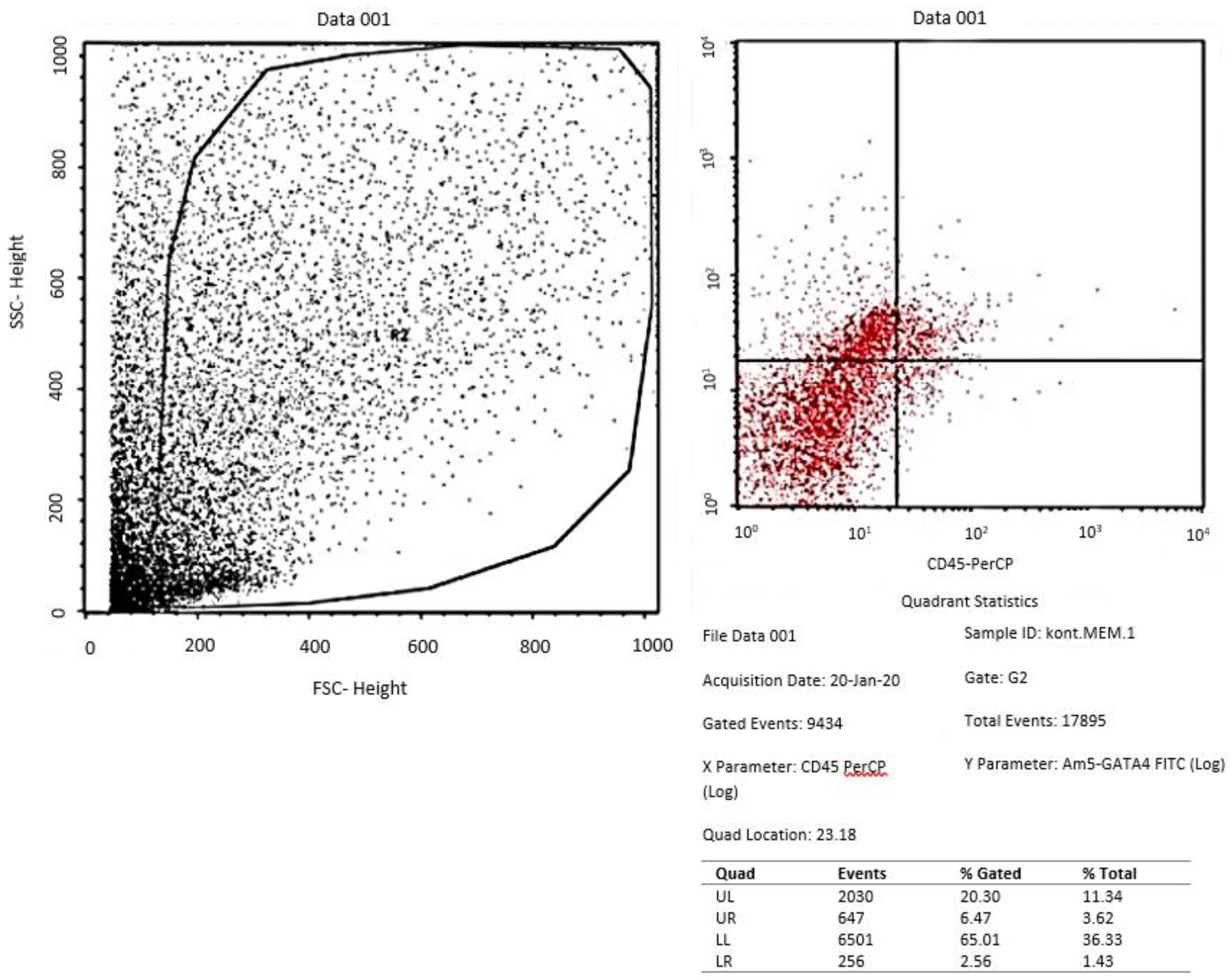
Figure 4.
Bar diagram showed the ratio of GATA-4 expression divided to unexpressed GATA-4 in the three group of ADSCs. There was no significant difference between the negative control group (α-MEM) compared to the positive control group (medium of differentiation) with p=0.179.
Figure 4.
Bar diagram showed the ratio of GATA-4 expression divided to unexpressed GATA-4 in the three group of ADSCs. There was no significant difference between the negative control group (α-MEM) compared to the positive control group (medium of differentiation) with p=0.179.
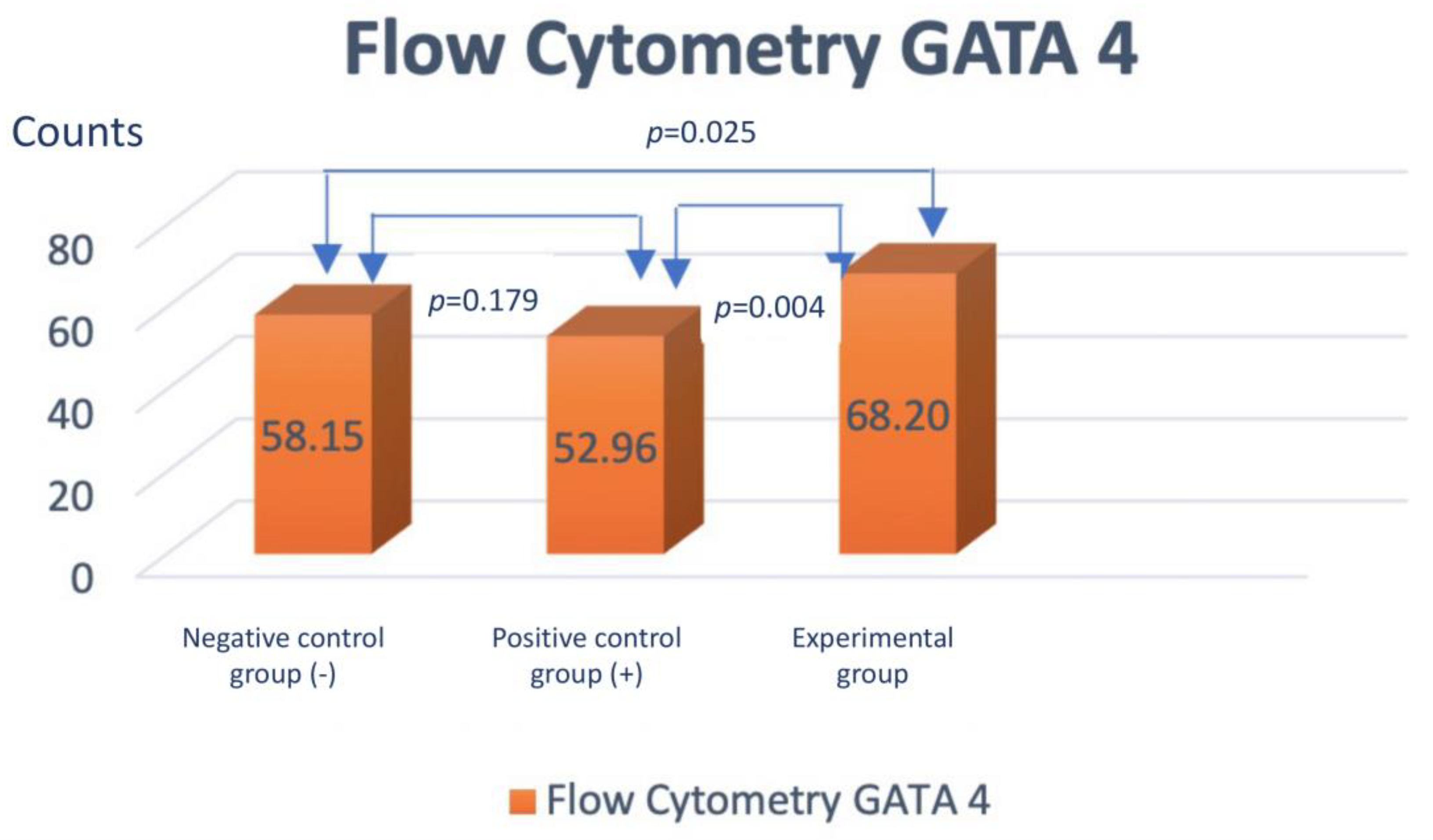
Figure 5.
Immunocytochemistry of cardiac troponin T in the negative control group (α-MEM) with 400x magnification. From the results of the immunocytochemistry examination of the three groups, the data obtained an average of 10.73 + 0.3 counts in the negative control group (α-MEM).
Figure 5.
Immunocytochemistry of cardiac troponin T in the negative control group (α-MEM) with 400x magnification. From the results of the immunocytochemistry examination of the three groups, the data obtained an average of 10.73 + 0.3 counts in the negative control group (α-MEM).
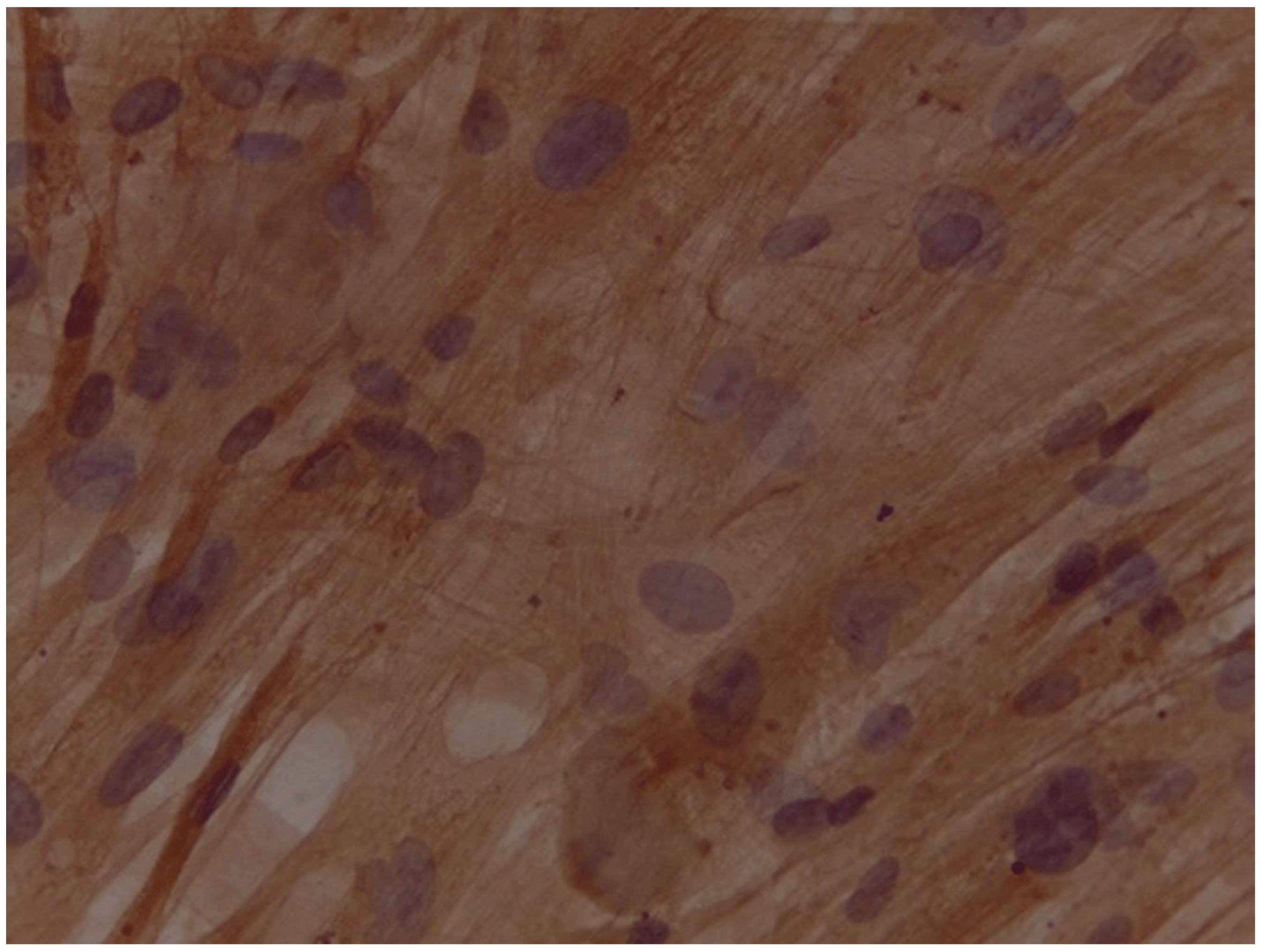
Figure 6.
Immunocytochemistry of cardiac troponin T the positive control group (medium of differentiation) with 400x magnification. From the results of the immunocytochemistry examination of the three groups, the data obtained an average of 26.00 + 0.4 counts in the positive control group (medium of differentiation).
Figure 6.
Immunocytochemistry of cardiac troponin T the positive control group (medium of differentiation) with 400x magnification. From the results of the immunocytochemistry examination of the three groups, the data obtained an average of 26.00 + 0.4 counts in the positive control group (medium of differentiation).
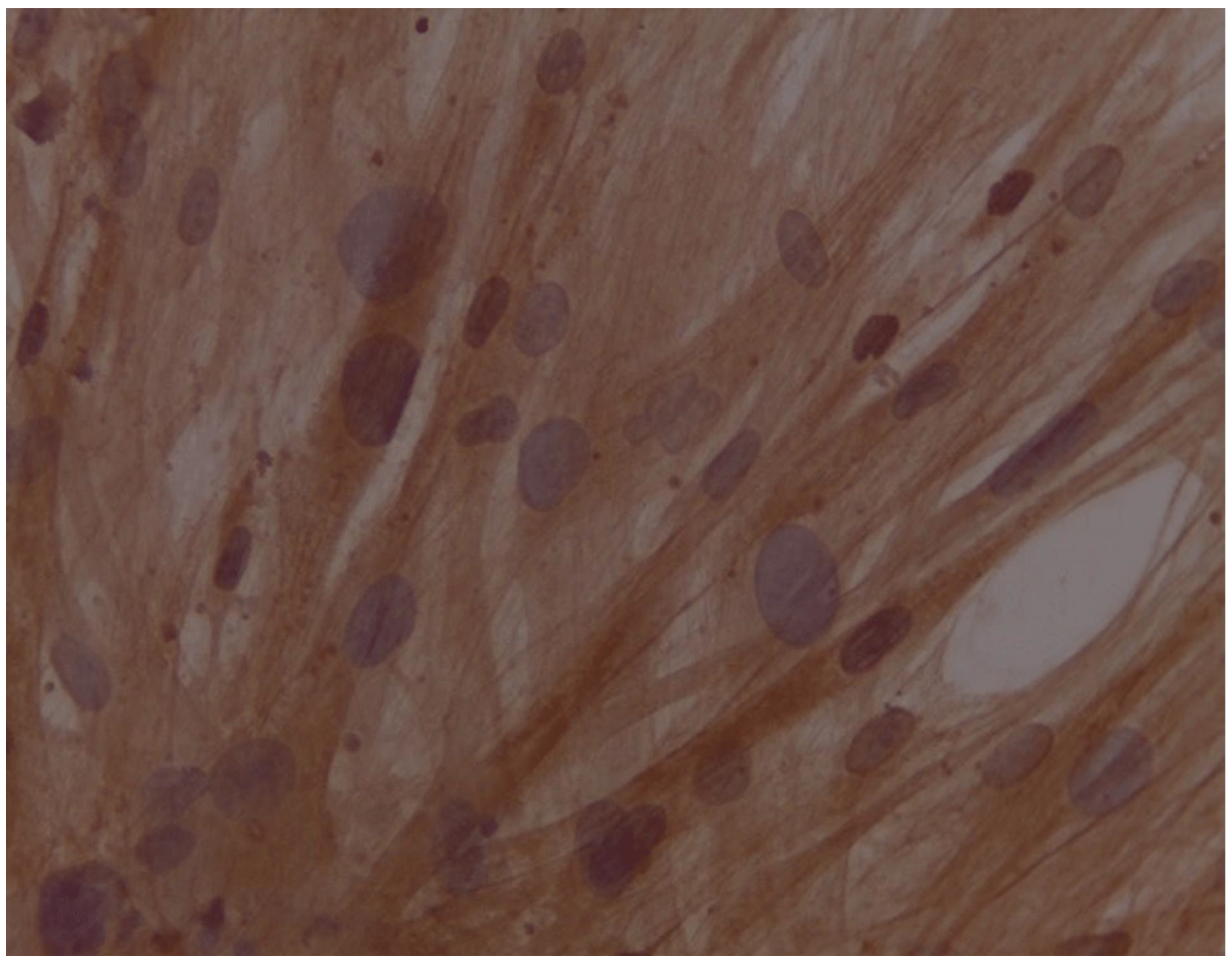
Figure 7.
Immunocytochemistry of cardiac troponin T in the treatment group (medium of differentiation + PRF) with 400x magnification. From the results of the immunocytochemistry examination of the three groups, the data obtained an average of 50.6 + 7.2 counts in the treatment group (differentiation medium + PRF).
Figure 7.
Immunocytochemistry of cardiac troponin T in the treatment group (medium of differentiation + PRF) with 400x magnification. From the results of the immunocytochemistry examination of the three groups, the data obtained an average of 50.6 + 7.2 counts in the treatment group (differentiation medium + PRF).
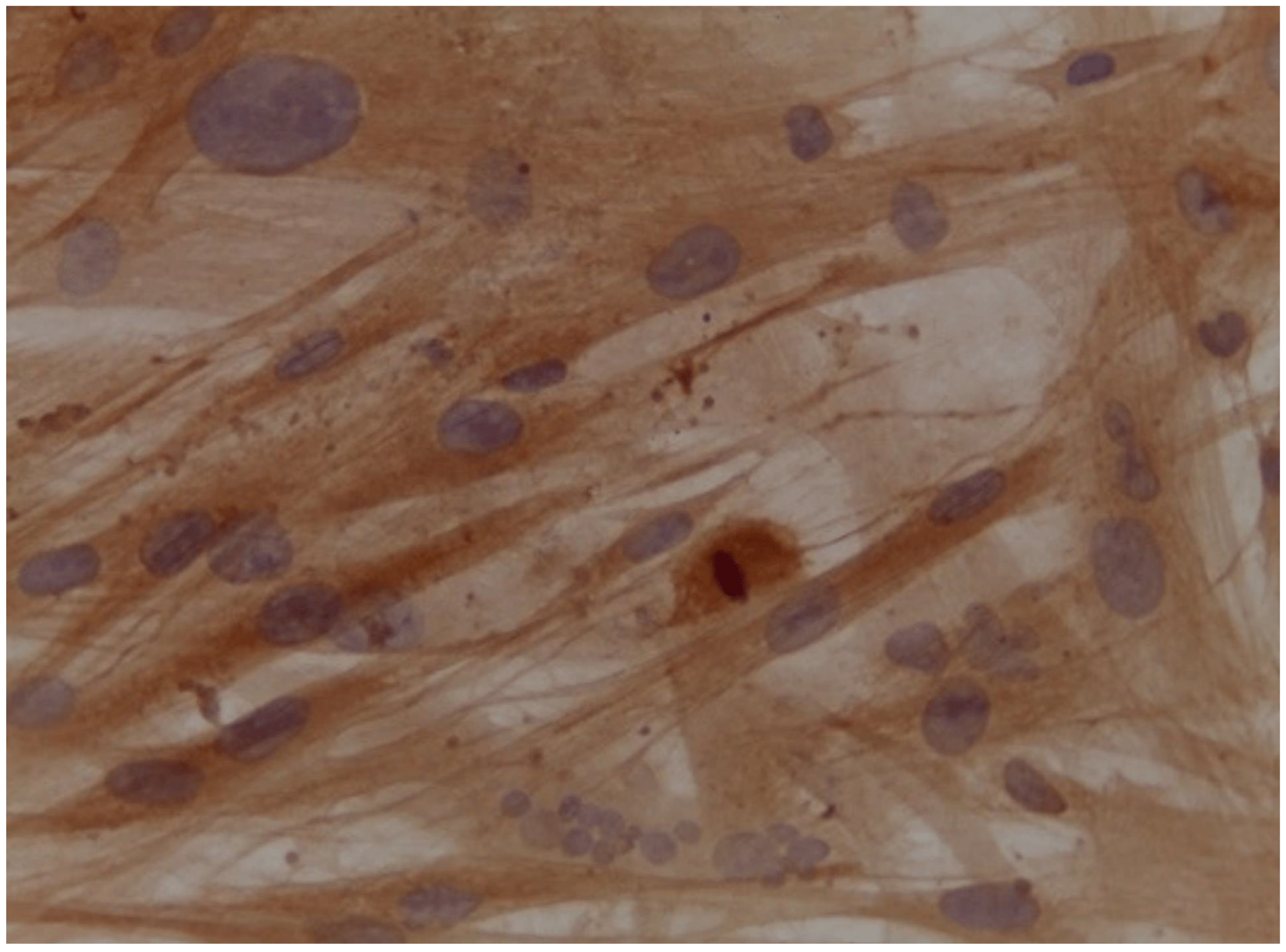
Figure 8.
Bar diagram showed mean cardiac troponin T expression by immunocytochemistry in the three group of ADSCs. ANOVA test was carried out to determine the difference between the three sample groups with p=0.0001.
Figure 8.
Bar diagram showed mean cardiac troponin T expression by immunocytochemistry in the three group of ADSCs. ANOVA test was carried out to determine the difference between the three sample groups with p=0.0001.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



