
Submitted:
09 August 2023
Posted:
10 August 2023
You are already at the latest version
Abstract
Pediatric chronic pain is an important public health issue given its notable impact on numerous domains of living. Pediatric chronic pain is also often comorbid with emotional, developmental, or behavioral conditions which can lead to more severe negative outcomes and an even greater reduction in positive outcomes compared to those without comorbidities. Flourishing is a positive outcome that chronic pain status has been shown to impact. We explored flourishing in children aged 6-17 years living with chronic pain as well as those with chronic pain and comorbidities using data from the 2018/2019 National Survey of Child Health. There were significant associa-tions between chronic pain condition status and all demographic variables (sex, age, race/ethnicity, poverty level, parental education, health insurance status). Results of hierarchical logistic regression found that chronic pain condition status significantly predicted flourishing. Children with chronic pain were 2.33 times less likely to flourish, and children with chronic pain plus an emotional, developmental, or behavioral comorbidity were 13 times less likely to flourish than typical peers. Given their significantly lower likelihood of flourishing, there is an urgent need for interventions targeted at children experiencing chronic pain and mental health comor-bidities.
Keywords:
chronic pain
; mental health
; comorbidities
; flourishing
1. Introduction
In their 2020 Guidelines on the Management of Chronic Pain in Children, the World Health Organization (WHO) identified chronic pain – pain that persists or recurs for more than three months – as the leading cause of morbidity in children [1]. The impact on a child living with chronic pain can be severe, deleterious, and far-reaching, with literature finding school functioning, peer and social interactions, sleep, and family relationships among the factors compromised [2,3,4]. One study estimated that almost three-quarters of children with chronic pain suffered physical impairment, half were absent from school, and more than a third had problems sleeping [5]. Moreover, pain frequency and intensity have also been shown to impact self-reported quality of life, with children and adolescents who experience extreme pain more often demonstrating impairments in psychological functioning, physical status, and functional status [6]. Additionally, as is the case with most pediatric chronic health conditions, the negative impact of chronic pain extends beyond the individual child affected, with parents and caregivers reporting that their own life is greatly impacted and restricted [6,7].
1.1. The Unique Nature of Pediatric Chronic Pain
WHO has emphasized the importance of understanding the physiological, developmental, and social uniqueness of pediatric chronic pain as distinct from adult chronic pain and the need for research examining pediatric populations specifically [1]. While it is known that chronic pain is common in children and adolescents, prevalence rates vary widely in the literature [8]. It is known that certain demographic characteristics play an important role in pediatric chronic pain. For example, lower socioeconomic status is associated with a higher prevalence of pain in general, as well as a higher prevalence of headaches, the most common pain in children and adolescents [8,9].
Moreover, age and sex also appear to be associated with pediatric pain prevalence. A 2000 Dutch prevalence study on children aged between 0 and 18 years highlighted the fact that pain prevalence differed between sexes and changed with age [10]. It was found that chronic pain was significantly higher in girls and that pain increased significantly with age. The study emphasizes that girls in their early teenage years, between 12 and 14 years, are at the highest risk of chronic pain. Another study from 2003 also found the highest incidence rate of chronic pain to be in girls aged 14 years [9]. A 2011 systematic review further reiterated this finding, reporting that pain prevalence rates were higher in girls and increased with age for most pain types [8].
1.2. Chronic Pain and Emotional, Developmental, or Behavioral Comorbidities
Pediatric chronic pain is often comorbid with psychological, developmental, and behavioral conditions [11]. Pediatric chronic pain has been linked to a greater risk of psychopathology both during childhood and adolescence, as well as into adulthood [12]. Moreover, even if chronic pain is resolved by adulthood, studies have shown that individuals who experienced pain in their youth are more likely to develop an anxiety or depressive disorder in their adult years [13]. Pediatric chronic pain has also been linked to behavioral problems, with the Biobehavioral Model of Pediatric Pain finding that greater pain intensity and duration are associated with a greater risk of behavioral problems [14]. A 2016 narrative review on comorbidities in pediatric chronic pain highlighted the inextricable link between chronic pain and emotional, developmental, and behavioral comorbidities due to their shared neurobiology and mutually maintaining cognitive and behavioral factors [15].
1.3. Flourishing and Chronic Pain
While much of the literature on pediatric chronic pain has focused on negative outcomes, there is less literature that examines positive health indicators in children with chronic pain. One such indicator is flourishing. A 2022 scoping review identified only four papers relating to flourishing and pediatric chronic pain, with much of the discussion of pain focusing on disability rather than thriving [16]. There is no single definition of flourishing, rather it is an umbrella term for the reduction in negative functioning and the increase in positive functioning including, but not limited to, optimism, resilience, psychological flexibility, acceptance, benefit-finding, and hope. Essentially an individual is flourishing when they are experiencing high levels of emotional, psychological, and social well-being that go beyond the absence of negative outcomes [17].
A 2015 qualitative study published in the UK looked at adjustment in children and adolescents living with juvenile idiopathic arthritis (JIA) [18]. It was found that adolescents with JIA reported benefits of living with chronic pain including self-growth, enhanced maturity, a can-do attitude, and resilience. A greater sense of social support further enhanced these positive outcomes. These benefits gave those living with chronic pain a greater sense of control over their lives and bodies. Another study from 2008 investigated the psychosocial impact of pain on social development in adolescents [19]. Three self-perceived factors of social development were identified by adolescents living with chronic pain: emotional adjustment, identity formation, and independence. A Canadian study that used similar self-report measures to explore benefit finding in youth with chronic pain highlighted the complexity of the relationship between chronic pain and flourishing [20]. It was reported that benefit finding is a significant predictor of pain intensity and quality of life.
Overall, literature on chronic pain and flourishing is in its infancy and notably, there is no known literature on flourishing and children or adolescents with chronic pain plus an emotional, developmental, or behavioral comorbidity. Furthermore, the few studies that have been published have notable limitations. They feature relatively small sample sizes and the only known studies are not geographically diverse, only representing the experiences of children and adolescents from Western Educated Industrialized Rich Democratic (WEIRD) societies like the UK and Canada. Moreover, a majority of the participants used in these studies were from a European middle-class background. These samples are not representative of a global population and the experience of chronic pain by children and adolescents across multiple contexts thus exacerbates the risk of health disparities.
1.4. Objective and Aims
Given the limitations of the small number of known studies on pediatric chronic pain and positive health indicators, particularly regarding chronic pain and comorbidities, this study aimed to use a large, nationally representative sample to examine whether children and adolescents with chronic pain and children with chronic pain plus an emotional, developmental, or behavioral comorbidity demonstrate less flourishing than their typically developing peers. Developmental systems theory was used as the overall framework for this study, with development being conceptualized as a result of dynamic, bidirectional interactions between genes and environments across multiple systems [21]. We hypothesized that children and adolescents with chronic pain would be less likely to flourish than their typically developing peers. We further hypothesized that those children and adolescents with chronic pain and an emotional, developmental, or behavioral comorbidity would be even less likely to flourish than those with chronic pain only or typically developing peers.
2. Methods
2.1. Data
Data was taken from the 2018-2019 National Survey of Children’s Health (NSCH), a nationally representative, cross-sectional sample of children and adolescents conducted by the United States Census Bureau and funded by the United States Health Resources and Services Administration (HRSA). The NSCH randomly sampled households across the United States – via online and mailed surveys – who had at least one child between the age of 0 and 17 years (Data Resource Center for Child and Adolescent Health, 2019). Data is publicly available online at no cost.
2.2. Participants
This study was limited to 6 -17-year-olds (N =31,435) with the sample being made up of 15,950 males (50.7%) and 15,485 females (49.3%). Sociodemographic factors of the selected sample were examined including the child’s sex, age, race/ethnicity, poverty level, whether the child comes from a working poor household, highest level of parental education, and health insurance status.
2.3. Variables and Measures
2.3.1. Chronic Pain Condition Status Groups
Children experiencing chronic pain were selected based on a parent reporting yes to “During the past 12 months, has this child had frequent or chronic difficulty with repeated or chronic physical pain, including headaches or other back or body pain?” and a parent reporting one special health care need (i.e., use or need of prescription medication; above average use or need of medical, mental health or educational services; functional limitations compared with others of the same age that is not mental health related). Children with chronic pain plus an emotional, developmental, or behavioral comorbidity (referred to hereafter as chronic pain plus) were selected based on meeting the above criteria for the chronic pain group and parent report of yes to “Does this child have any kind of emotional, developmental, or behavioral problem for which he or she needs treatment or counseling?” The typical peer group was made up of participants aged between 6 and 17 years who did not meet the criteria for the chronic pain or chronic pain plus groups.
2.3.2. Flourishing Categories
The outcome variable was parent report of overall flourishing for children aged between 6 and 17 years, as well as responses to each of the three item-level flourishing criteria (i.e., shows interest and curiosity in learning new things, works to finish tasks they start, and can stay calm and in control when faced with a challenge). Individual items were coded as 1 – “Always”, 2 – “Usually”, 3 – “Sometimes”, and 4 – “Never.” Overall flourishing was coded with both three levels (1 – “Always/usually response to 0-1 items”, 2 – “Always/usually response to 2 items”, and 3 – “Always/usually response to all 3 items.”) and two levels (1 – “Always/usually response to 0-2 items”, 2 – “Always/usually response to all 3 items.”). The two-level version of the variable was used for logistic regression.
2.3.3. Predictors
Demographic variables used in the study included age (6 -11 years/12 -17 years), sex (male/female), and race/ethnicity (White/Non-Hispanic, Hispanic, Black/Non-Hispanic, Other/Multi-racial, non-Hispanic). Family-based demographic variables included poverty level (0-99% Federal Poverty Level [FPL], 100-199% FPL, 200-399% FPL, >400% FPL), highest level of parental education (less than high school, high school or GED, some college or technical school, college degree or higher), and current health insurance status (public insurance only, private health insurance only, public and private insurance, uninsured). All variables were treated as categorical except age, poverty level, and parental education which were treated as ordinal.
2.4. Statistical Analysis
The analysis was conducted using the program IBM SPSS 27. The prevalence in the sample of chronic pain plus, chronic pain, and typical peers was calculated. We conducted tests of the association of demographic covariates and chronic pain status group using chi-square for categorical variables and Kendall's tau-b for ordinal variables. In the primary analysis, a hierarchical binary logistic regression was used to determine whether chronic pain status (chronic pain plus, chronic pain, typical peers) significantly predicted flourishing over and above demographic covariates.
3. Results
The first research question asked about the frequency in the chronic pain status groups among children aged 6 -17 years in the United States. The estimated prevalence of chronic pain was 4.0% and chronic pain plus was 3.9% with typical peers making up 92.1%.
The second research question asked what the sociodemographic characteristics were among children aged 6 -17 years across chronic pain status groups. Demographics for the sample and results of tests of association are in Table 1. A larger percentage of both the chronic pain and chronic pain plus groups were female than male. Across all three chronic pain status groups, a larger percentage were aged between 12 and 17 years. A majority of the sample across all three pain status groups were White, non-Hispanic. Tests of association between chronic pain status and demographic variables were conducted. Hypotheses were that there would be significant associations such that decreasing severity of chronic pain condition status (i.e., chronic pain plus, chronic pain, typical peers) would be associated with younger age, being male, being White, higher socioeconomic status, higher parental education, and greater health insurance status. There were significant associations between chronic pain status and all demographic variables, in expected directions.
Additional tests of association between chronic pain condition status, using only the chronic pain plus and chronic pain categories of the variable, and demographic variables also were conducted. This was potentially important because it could differentiate these two rarely studied groups. Again, hypotheses were that there would be significant associations such that decreasing severity of chronic pain condition status (i.e., chronic pain plus, chronic pain) would be associated with being male, higher socioeconomic status, higher parental education, and greater health insurance status. Results were significant, in the hypothesized direction, and a weak association for sex, χ2 (2484) = 17.54, p < .001, Cramer’s V = .08; poverty level, τb (2484) = .06, p = .001; parental education; τb (2484) = .04, p = .04; and health insurance status, χ2 (2459) = 64.1605, p < .001, Cramer’s V = .16; but not significant for age, race/ethnicity, and working poor. Of note, the chronic pain plus group was significantly less female (51.8%) than the pain group (60.1%).
The third research question was whether there was an association between chronic pain condition status and flourishing in children aged 6-17 years. The hypothesis was that there would be a significant association such that as chronic pain condition status is less severe, flourishing increases. Figure 1 shows flourishing across the three chronic pain status groups. There was a significant moderate association between chronic pain condition status and flourishing, τb (31405) = .249, p < .001, which indicates that this association is likely in the population. There was also a significant moderate association between chronic pain condition status and the two-level version of flourishing, τb (31405) = .237, p < .001.
Overall flourishing was made up of three items, and the association of chronic pain condition status and each item of flourishing were significant in the expected direction: shows interest and curiosity in learning new things, τb (31354) = -.145, p < .001, a weak association; works to finish the tasks they start, τb (30936) = -.177, p < .001, a weak association; and stays calm and in control when faced with a challenge, τb (31196) = -.207, p < .001, a moderate association. When examining only the chronic pain plus and chronic pain categories of the chronic pain status group variable, the association of chronic pain condition status and each item of flourishing also were significant in the expected direction: shows interest and curiosity in learning new things, τb (2477) = -.25, p < .001, a moderate association; works to finish the tasks they start, τb (2454) = -.35, p < .001, a strong association; and stays calm and in control when faced with a challenge, τb (2468) = -.41, p < .001, a strong association.
The fourth research question was whether chronic pain condition status would add significant incremental predictive utility in the prediction of flourishing over and above a block of demographic predictors. The hypothesis was that chronic pain condition status would provide significant incremental predictive utility over and above a block of demographic predictors. Hierarchical binary logistic regression was used to evaluate a model for predicting flourishing. The model was composed of two blocks of predictors. The first block of predictors consisted of age, sex, race/ethnicity, poverty level, parental education, and health insurance status. Chronic pain condition status constituted the second block of predictors.
Initial assumptions of logistic regression (independence of observations, categories of outcome variable and categorical predictor variables mutually exclusive and exhaustive, sufficient ratio of cases per predictor variable [here > 3000:1]) were met. To assess multicollinearity among the predictors, all of which are categorical, the predictor variables were dummy coded, and multiple linear regression was run with these dummy variables to generate VIF and tolerance values. Dummy variables associated with some categories of the poverty level (tolerance = .23, VIF = 4.39) and working poor families (tolerance = .28, VIF =3.53) variables indicated that these two variables had a potentially problematic degree of multicollinearity. For all other predictor variables, tolerance was > .2 and VIF was < 1.6, indicating an absence of significant multicollinearity. After removing the working poor variable, tolerance was > .6 and VIF was < 1.7 for all predictor variables. Thus, the logistic regression analysis was repeated after excluding the working poor variable. As to the absence of outliers, leverage points, or highly influential points, 285 of 30893 cases (0.92%) had a standardized residual value > 2.5, with 4 of those cases having a standardized residual value > 3.0. This was deemed to be a negligible portion of the sample; thus, the assumption was met.
Results of the hierarchical logistic regression are provided in Table 2. As expected, both the initial model, which consisted of the first block of predictors (age, sex, race/ethnicity, poverty level, parental education, and health insurance status), χ2 = 1153.13, p < .001, and the full model, which consisted of the first and second block of predictors (chronic pain condition status), χ2 = 2846.85, p = .000, significantly outperformed the null model. The Hosmer and Lemeshow test indicated that both the initial, χ2 = 7.40, p = .49, and full model, χ2 = 12.94, p =.11, fit the data appropriately. In addition, a pseudo R2 measure, used in logistic regression as a means to determine the goodness of fit of a model, yielded Nagelkerke pseudo R2 =.054 for the initial model and Nagelkerke pseudo R2 = .131 for the full model. This indicates that the full model better predicted flourishing than the initial model.
As expected, sex, age, race/ethnicity, poverty level, parental education, and health insurance status were all significant predictors of flourishing in the full model. Looking at the odds ratios for pairwise comparisons for demographic predictors in the full model, most were significant with a few exceptions. For the race/ethnicity variable, comparisons between White and Black (p = .757) and White and other/multi-racial, non-Hispanic (p = .145) were not significant. For health insurance status, the comparison between being uninsured and having both private and public health insurance (p = .280) was not significant.
As expected, the second block of predictors (chronic pain condition status) provided significant incremental utility in predicting flourishing, χ2 = 1693.72, p < .001). In other words, adding chronic pain condition status to the initial model increased the ability of the full model to predict flourishing over and above the other predictors. Classification statistics for both the initial and full models are provided in Table 3 and Table 4. The addition of the chronic pain condition status marginally increased classification accuracy over the initial model from 75.4% to 77.8%.
Overall, chronic pain condition status significantly predicted flourishing, Wald χ2 = 1379.61, p < .001. Using the reciprocal of the odds ratios (and their confidence intervals) from Table 2, the odds of not flourishing for children with chronic pain is 2.33 times greater than for typical peers (OR = 2.33, 95% CI, 2.05 to 2.63). Of particular note, the odds of not flourishing for children with chronic pain and comorbidities is 13 times greater than for typical peers (OR = 12.99, 95% CI: 11.24 to 14.93).
4. Discussion
Using secondary data analysis of a nationally representative sample of American children between 6 and 17 years with chronic pain (determined by parent report of chronic pain with functional impairments during the last 12 months), we found that chronic pain was strongly associated with reduced flourishing. Moreover, we found that for those children and adolescents living with chronic pain plus an emotional, developmental, or behavioral comorbidity there was an even stronger association with reduced flourishing over and above what was found for children who experienced chronic pain without comorbidities. Specifically, children with chronic pain were 2.33 times less likely to flourish than typical peers, and children with chronic pain plus an emotional, developmental, or behavioral comorbidity were 13 times less likely to flourish than their typical peers. Ultimately, these results suggest that while chronic pain alone is problematic for flourishing, children and adolescents who also live with an emotional, developmental, or behavioral comorbidity have a much greater risk of not flourishing. These results are not only consistent with our hypotheses, but they are also consistent with the findings of prior studies on both chronic pain and flourishing and chronic pain plus comorbidities and flourishing [15,18,19].
From a nationally representative dataset, chronic pain occurred in 4.0% of our sample and the prevalence of chronic pain plus comorbidities was 3.9%. The overall chronic pain prevalence (7.9%) fell toward the lower end of the large prevalence range (6% - 57%) identified in the existing literature base [8,22]. However, in this study, we identified children and adolescents with chronic pain through parent endorsement of the criteria “this child had frequent or chronic difficulty with repeated or chronic physical pain, including headaches or other back or body pain” over the past 12 months plus parent report of at least one special health need (e.g., use or need of prescription medication; above average use or need of medical, mental health or educational services; functional limitations compared with others of the same age that is not mental health related). This allowed us to identify children who were functionally limited by their chronic pain and/or required the help of professional services. To identify those with comorbidities, parent response to the question “Does this child have any kind of emotional, developmental, or behavioral problem for which he or she needs treatment or counseling?” was used in addition to the chronic pain criteria outlined above. This was a different approach to identifying children and adolescents with chronic pain who were functionally limited by their chronic pain, with comparable studies identifying participants with chronic pain exclusively by parental report of chronic pain in the last 12 months. Therefore, our more nuanced and stringent inclusion criteria may be the reason our overall prevalence rate was lower than that reported in other studies [22].
Identifying and managing chronic pain and associated comorbidities is extremely important in both the short and long term. In addition to pain-related functional impairment, poorer social, emotional, physical, and socioeconomic outcomes are more likely to be experienced by those who experience chronic pain during childhood than typical peers [2,3,13]. These negative outcomes not only burden the individuals but their families, immediate communities, and the greater population. Therefore, healthcare systems must work to reduce chronic pain and the commonly associated emotional, developmental, or behavioral comorbidities. Moreover, given the potentially more deleterious outcomes for those with chronic pain and comorbidities as identified by this study and other recent similar studies, resources are needed to evaluate and treat chronic pain effectively in pediatric populations [23]. The even greater risk of not flourishing for those in the chronic pain and comorbidities group identified by the results of this study underscores the need for more consistent screening that considers mental health, as well as resiliency factors, in pediatric patients. All too often, screenings are focused exclusively on medical factors or current pain status and fail to consider other needs.
The developmental systems theory underpinned this study, as both chronic pain and flourishing are complex and multidimensional with several factors playing an important role in their relationship [21]. Looking at the sociodemographic variables included in the model (age, sex, race/ethnicity, poverty level, parental education, and health insurance status), there was a significant association between chronic pain condition status and demographic variables. Looking only at the chronic pain plus and chronic pain groups, results were significant for sex, poverty level, parental education, and health insurance status but not for age, race/ethnicity, and working poor. While many of these demographic characteristics are consistent with previous research related to risk and resiliency, it is important for practitioners to uniquely consider parental education and gender [24]. Notably, as seen in previous literature, those in the chronic pain group were more likely to be female (60.1%) than male (39.9%), however, the chronic pain plus group did not have such a substantial sex disparity, with males and females each representing close to 50%. This is an important finding for practitioners as male children tend to be overlooked relative to emotional screening [25,26].
4.1. Implications
The results of the study highlight a clear need for practitioners to improve universal screening of pediatric chronic pain and common mental health comorbidities. By accurately identifying the children and adolescents who are impacted by chronic pain, interventions can be focused not only on reducing negative outcomes but also on promoting positive outcomes like flourishing. Moreover, when assessing pediatric pain, those with mental health comorbidities must be identified, as traditional chronic pain treatments may not be sufficient to help facilitate positive outcomes for this population. Healthcare professionals need to be educated regarding the fact that chronic pain treatments may not be as successful if they do not consider mental health comorbidities. The uniqueness of those with chronic pain plus an emotional, developmental, or behavioral comorbidity highlighted in the results also underscores the need for the development of specific interventions that target chronic pain as well as mental health comorbidities in pediatric populations.
The results also emphasize the need for more evidence-based interventions specifically targeted at low-income, low-education families. Given the negative outcomes that can occur later in life if chronic pain is not addressed during childhood, it is particularly important that healthcare professionals who work with the populations who are most impacted, as well as parents, caregivers, and teachers in these communities, are educated about how to identify and treat chronic pain [4]. Education programs must be mindful of those children whose parents have a lower level of education though, and they must consider how to make psychoeducation accessible and subsequently impactful to all children living with chronic pain.
4.2. Limitations
The findings of this study should be assessed with the following limitations in mind. Firstly, chronic pain was identified exclusively by parent responses to two questions based exclusively on the child’s health and behavior over the last 12 months. While this allowed us to identify children and adolescents who were experiencing chronic pain that was impacting their functioning or requiring medical attention, this was a more specific criteria than what has been used by comparable studies which resulted in a smaller reported prevalence. Moreover, given the cross-sectional study design, it is not possible to infer a causal pathway between chronic pain condition status and flourishing. This relationship may be bidirectional, with a lack of flourishing leading to chronic pain and emotional, developmental, and behavioral comorbidities.
5. Conclusions
Ultimately, our findings suggest that while children and adolescents living with chronic pain are less likely to flourish than typical peers, those who live with chronic pain plus an emotional, developmental, or behavioral comorbidity are even more vulnerable to reduced flourishing. Therefore, there is an urgent need to provide specialized care to these children and to expand the scope of chronic pain screening and treatment to include common mental health comorbidities.
Author Contributions
Conceptualization by Madeline Foster and Jessica Emick; methodology by Madeline Foster, Jessica Emick, and Nathan Griffith; formal analysis by Nathan Griffith; writing –original draft preparation by Madeline Foster; writing –review and editing by Madeline Foster, Jessica Emick, and Nathan Griffith; supervision by Jessica Emick; funding acquisition by Jessica Emick. All authors have read and agreed to the published version of the manuscript.
Funding
This research was funded by Jessica Emick’s Fielding Graduate University Faculty Research Grant.
Institutional Review Board Statement
Ethical review and approval were not required for this study as no data was collected and the data used was not identifiable.
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Data Availability Statement
The National Survey of Children’s Health is a publicly available dataset funded by the Health Resources and Services Administration and the Maternal and Child Health Bureau. Data is publicly available at https://www.childhealthdata.org/
Conflicts of Interest
The authors declare no conflict of interest.
References
- World Health Organization. (2020). Guidelines on the management of chronic pain in children. https://www.who.int/publications/i/item/9789240017870.
- Groenewald, C.B.; Tham, S.W.; Palermo, T.M. Impaired school functioning in children with chronic pain: A national perspective. The Clinical Journal of Pain 2020, 36, 693–699. [Google Scholar] [CrossRef] [PubMed]
- Landry, B.W.; et al. Managing chronic pain in children and adolescents: a clinical review. PM&R 2015, 7, S295–S315. [Google Scholar]
- Palermo, T.M. Impact of recurrent and chronic pain on child and family daily functioning: a critical review of the literature. Journal of Developmental & Behavioral Pediatrics 2000, 21, 58–69. [Google Scholar]
- Konijnenberg, A.Y.; Uiterwaal, C.S.P.M.; Kimpen, J.L.L.; van der Hoeven, J.; Buitelaar, J.K.; de Graeff-Meeder, E.R. Children with unexplained chronic pain: substantial impairment in everyday life. Archives of Disease in Childhood 2005, 90, 680–686. [Google Scholar] [CrossRef] [PubMed]
- Hunfeld, J.A.M.; Passchier, J.; Perquin, C.W.; Hazebroek-Kampschreur, A.A.J.M.; van Suijlekom-Smit, L.W.A.; Van Der Wouden, J.C. Quality of life in adolescents with chronic pain in the head or at other locations. Cephalalgia 2001, 21, 201–206. [Google Scholar] [CrossRef] [PubMed]
- Palermo, T.M.; Eccleston, C. Parents of children and adolescents with chronic pain. Pain 2009, 146, 15–17. [Google Scholar] [CrossRef]
- King, S.; Chambers, C.T.; Huguet, A.; MacNevin, R.C.; McGrath, P.J.; Parker, L.; MacDonald, A.J. The epidemiology of chronic pain in children and adolescents revisited: a systematic review. Pain 2011, 152, 2729–2738. [Google Scholar] [CrossRef]
- Eccleston, C.; Malleson, P. Managing chronic pain in children and adolescents. BMJ 2003, 326, 1408–1409. [Google Scholar] [CrossRef]
- Perquin, C.W.; Hazebroek-Kampschreur, A.A.; Hunfeld, J.A.; Bohnen, A.M.; van Suijlekom-Smit, L.W.; Passchier, J.; Van Der Wouden, J.C. Pain in children and adolescents: a common experience. Pain 2000, 87, 51–58. [Google Scholar] [CrossRef]
- Miller, M.M.; Meints, S.M.; Hirsh, A.T. Catastrophizing, pain, and functional outcomes for children with chronic pain: a meta-analytic review. Pain 2018, 159, 2442. [Google Scholar] [CrossRef]
- Shelby, G.D.; et al. Functional abdominal pain in childhood and long-term vulnerability to anxiety disorders. Pediatrics 2013, 132, 475–482. [Google Scholar] [CrossRef] [PubMed]
- Hotopf, M.; Carr, S.; Mayou, R.; Wadsworth, M.; Wessely, S. Why do children have chronic abdominal pain, and what happens to them when they grow up? Population-based cohort study. BMJ 1998, 316, 1196–1200. [Google Scholar] [CrossRef] [PubMed]
- Varni, J.W.; Rapoff, M.A.; Waldron, S.A.; Gragg, R.A.; Bernstein, B.H.; Lindsley, C.B. Chronic pain and emotional distress in children and adolescents. Journal of Developmental & Behavioral Pediatrics 1996, 17, 154–161. [Google Scholar]
- Vinall, J.; Pavlova, M.; Asmundson, G.J.; Rasic, N.; Noel, M. Mental health comorbidities in pediatric chronic pain: a narrative review of epidemiology, models, neurobiological mechanisms and treatment. Children 2016, 3, 40. [Google Scholar] [CrossRef]
- Parsons, R.D.; McParland, J.L.; Halligan, S.L.; Goubert, L.; Jordan, A. Flourishing among adolescents living with chronic pain and their parents: A scoping review. Paediatric and Neonatal Pain 2022. [Google Scholar] [CrossRef]
- Keyes, C.L. The mental health continuum: From languishing to flourishing in life. Journal of Health and Social Behavior 2002, 207–222. [Google Scholar] [CrossRef]
- Cartwright, T.; Fraser, E.; Edmunds, S.; Wilkinson, N.; Jacobs, K. Journeys of adjustment: the experiences of adolescents living with juvenile idiopathic arthritis. Child: Care, Health and Development 2015, 41, 734–743. [Google Scholar] [CrossRef]
- Eccleston, C.; Wastell, S.; Crombez, G.; Jordan, A. Adolescent social development and chronic pain. European Journal of Pain 2008, 12, 765–774. [Google Scholar] [CrossRef]
- Soltani, S.; Neville, A.; Hurtubise, K.; Hildenbrand, A.; Noel, M. Finding silver linings: A preliminary examination of benefit finding in youth with chronic pain. Journal of Pediatric Psychology 2018, 43, 285–293. [Google Scholar] [CrossRef]
- Tinajero, C.; Páramo, M.F. The systems approach in developmental psychology: Fundamental concepts and principles. Psicologia: Teoria e Pesquisa 2012, 28, 457–465. [Google Scholar] [CrossRef]
- Tham, S.W.; Law, E.F.; Palermo, T.M.; Kapos, F.P.; Mendoza, J.A.; Groenewald, C.B. Household Food Insufficiency and Chronic Pain among Children in the US: A National Study. Children 2023, 10, 185. [Google Scholar] [CrossRef]
- Corser, J.; Caes, L.; Bateman, S.; Noel, M.; Jordan, A. ‘A whirlwind of everything’: The lived experience of adolescents with co-occurring chronic pain and mental health symptoms. European Journal of Pain 2023. [Google Scholar] [CrossRef]
- Goubert, L.; Trompetter, H. Towards a science and practice of resilience in the face of pain. European Journal of Pain 2017, 21, 1301–1315. [Google Scholar] [CrossRef] [PubMed]
- Chaplin, T.M.; Aldao, A. Gender differences in emotion expression in children: a meta-analytic review. Psychological Bulletin 2013, 139, 735. [Google Scholar] [CrossRef] [PubMed]
- Van Droogenbroeck, F.; Spruyt, B.; Keppens, G. Gender differences in mental health problems among adolescents and the role of social support: results from the Belgian health interview surveys 2008 and 2013. BMC Psychiatry 2018, 18, 1–9. [Google Scholar] [CrossRef] [PubMed]
Figure 1.
Flourishing in Chronic Pain Plus, Chronic Pain, and Typical Groups.
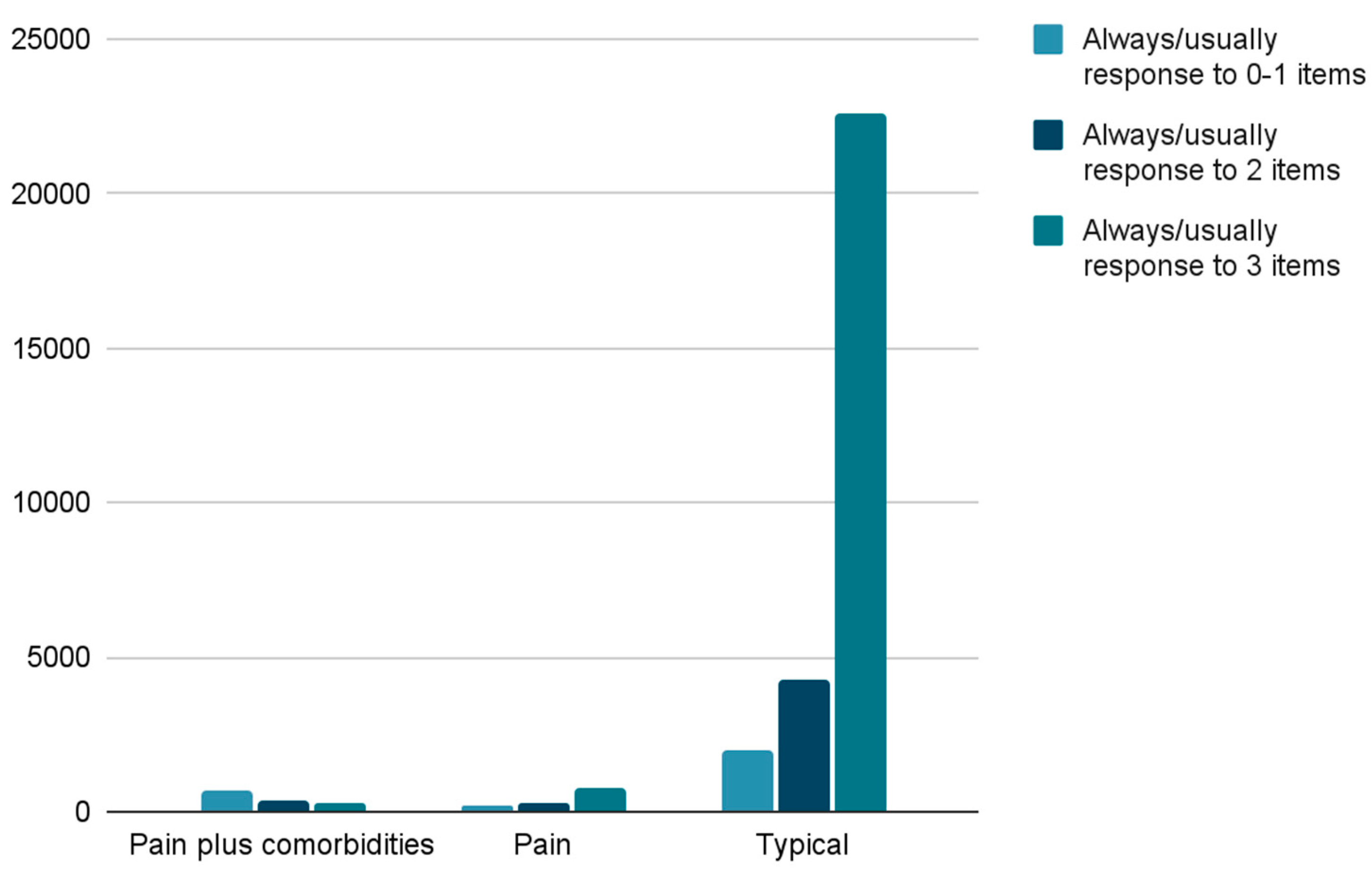

Table 1.
Demographic Table.
| Characteristic | Chronic Pain Plus | Chronic Pain | Typical Peers | χ2 | Cramer’s V |
| Age, years | -.10abc | .10 | |||
| 6 – 11 years | 355 (27.9%)c | 315 (26.0%) | 12991 (44.9%) | ||
| 12 – 17 years | 918 (72.1%) | 896 (74.0%) | 15960 (55.1%) | ||
| Sex | 63.98b | .05 | |||
| Male | 355 (27.9%)c | 315 (26.0%) | 12991 (44.9%) | ||
| Female | 918 (72.1%) | 896 (74.0%) | 15960 (55.1%) | ||
| Race/Ethnicity | 43.98b | .03 | |||
| White, non-Hispanic |
907 (71.2%) | 872 (72.0%) | 19912 (68.8%) | ||
| Hispanic | 143 (11.2%) | 121 (10.0%) | 3485 (12.0%) | ||
| Black Non-Hispanic |
110 (8.6%) | 97 (8.0%) | 1832 (6.3%) | ||
| Other/ multi-racial, non-Hispanic |
113 (8.9%) | 121 (10.0%) | 3722 (12.9%) | ||
| Working Poor | 9.02d | .02 | |||
| Working Poor | 111 (4.6%) | 118 (4.9%) | 2192 (90.5%) | ||
| Not Working Poor |
1140 (4.0%) | 1075 (3.8%) | 26097 (92.2%) | ||
| Poverty Level | .08ab | .07 | |||
| 0-99% FPL | 248 (19.5%) | 198 (16.4%) | 3013 (10.4%) | ||
| 100-199% FPL | 304 (23.9%) | 246 (20.3%) | 4456 (15.4%) | ||
| 200-399% FPL | 357 (28.0%) | 369 (30.5%) | 9043 (31.2%) | ||
| >400% FPL | 364 (28.6%) | 398 (32.9%) | 12439 (43.0%) | ||
| Parental education | .06ab | .05 | |||
| Less than high school | 41 (3.2%) | 36 (3.0%) | 823 (2.8%) | ||
| High school or GED | 206 (16.2%) | 204 (16.8%) | 3846 (13.3%) | ||
| Some college or technical school | 434 (34.1%) | 340 (28.1%) | 6704 (23.2%) | ||
| College degree or higher |
592 (46.5%) | 631 (52.1%) | 17578 (60.7%) | ||
| Health Insurance | 887.64b | .12 | |||
| Public insurance only |
466 (36.9%) | 328 (27.4%) | 4727 (16.6%) | ||
| Private health insurance only |
606 (48.0%) | 750 (62.7%) | 21454 (75.4%) | ||
| Public and private insurance |
152 (12.0%) | 75 (6.3%) | 742 (2.6%) | ||
| Uninsured | 38 (3.0%) | 44 (3.7%) | 1,536 (5.4%) |
* a Kendall’s tau-b used, b p < .001, c percentage of sample, d p < .01.
Table 2.
Results of Logistic Regression (Full Model)
| Variable | b | SE | Wald | p | OR | 95% CI | |
| Lower | Upper | ||||||
| Constant | -.784 | .096 | 66.67 | <.001 | .457 | ||
| Sex (Male)a | -.308 | .028 | 119.81 | <.001 | .736 | .696 | .777 |
| Age (6-11 years) | -.250 | .028 | 77.73 | <.001 | .779 | .737 | .823 |
| Race/Ethnicity (White) | 20.85 | <.001 | |||||
| Hispanic | -.173 | .043 | 16.01 | <.001 | .841 | .773 | .916 |
| Black | -.018 | .057 | -.10 | .757 | .983 | .879 | 1.098 |
| Other/Multi-racial, non-Hispanic | .064 | .044 | 2.12 | .145 | 1.066 | .978 | 1.162 |
| Poverty (400% FPL or greater) | 50.38 | <.001 | |||||
| 0-99% FPL | -.267 | .055 | 23.87 | <.001 | .766 | .688 | .852 |
| 100-199% FPL | -.228 | .047 | 24.07 | <.001 | .796 | .727 | .872 |
| 200-399% FPL | -.230 | .035 | 42.99 | <.001 | .794 | .742 | .851 |
| Parent Education (College degree or higher) | 172.18 | <.001 | |||||
| Less than high school | -.843 | .080 | 111.69 | <.001 | .430 | .368 | .503 |
| High school or GED | -.404 | .044 | 84.53 | <.001 | .668 | .612 | .728 |
| Some college or technical school | -.293 | .035 | 69.08 | <.001 | .746 | .696 | .799 |
| Health insurance (Uninsured) | 63.76 | <.001 | |||||
| Public health insurance only | -.132 | .065 | 4.16 | .041 | .876 | .771 | .995 |
| Private health insurance only | .192 | .062 | 9.69 | .002 | 1.212 | 1.074 | 1.368 |
| Public and private insurance | -.100 | .093 | 1.17 | .280 | .904 | .754 | 1.085 |
| Pain condition status (Typical) | 1379.61 | <.001 | |||||
| Chronic pain plus | -2.560 | .072 | 1259.52 | <.001 | .077 | .067 | .089 |
| Chronic pain | -8.44 | .063 | 178.68 | <.001 | .430 | .380 | .487 |
* a Reference category.
Table 3.
Summary of Classification Statistics from Hierarchical Logistic Regression Analysis.
| Variable | Initial Model | Full Model |
| Accuracy | 75.4% | 77.8% |
Table 4.
Classification Statistics from Hierarchical Logistic Regression Analysis (full model)
| Not Flourishing | Flourishing | Percentage correct |
|
| Observed | |||
| Not flourishing | 1156 | 6451 | 15.2% |
| Flourishing | 401 | 22885 | 98.3% |
| Overall percentage | 77.8% |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



