
Submitted:
07 August 2023
Posted:
08 August 2023
You are already at the latest version
Abstract
This scoping review aims to identify the available evidence concerning the clinical and psychosocial impacts of the communication of oral potentially malignant disorders (OPMDs), and to map and analyze knowledge gaps regarding truth-telling about risk factors, malignant transformation, treatment, and follow-up approaches. Search strategy was performed using electronic databases (Medline/PubMed, Scopus, Embase, and Web of Science) and one grey literature database (Google Scholar). Studies focused on communicating the diagnosis of OPMDs and the patients' perceptions were included. Study selection and data extraction were performed by two authors in a two-phase process. Five publications were included in the qualitative analysis. Each publication involved a different study design, study population, types of OPMDs, and results on the important aspects of the professional-patient communication about the diagnosis of OPMDs. Although specific protocols on OPMDs communication have not yet been reported, there is an elevated interest on this topic since the strategies and skills on professional communication could provide better clinical outcomes to the patients. A list of recommendation strategies on how to communicate an OPMD diagnosis is proposed; however, future studies are still needed to design specific communication protocols for OPMD.
Keywords:
oral potentially malignant disorders
; communication
; truth-telling
; scoping review
1. Introduction
Oral potentially malignant disorders (OPMDs) are a group of conditions that predispose oral mucosa to malignant transformation, specifically to oral squamous cell carcinoma (OSCC), the most common head and neck cancer in adults. Although the minority of these disorders progress to cancer, early diagnosis is particularly important given the high mortality rate of late-stage OSCC [1].
It has been estimated that the overall worldwide prevalence of OPMDs is around 4.5%, with wide differences according to the geographic regions [2]. Although the overall malignant transformation rate across all OPMDs group is relatively low (7.9%), and each type of disorder has a highly variable rate of transformation (ranging from 1.4% to 49.5%), the risk of progression to OSCC is always a possibility and should be considered in the clinical follow-up of all patients affected by OPMDs [3].
The OPMDs present heterogeneous etiologies, and their biology is characterized by mutations in the genetic codes of oral epithelial cells with or without clinical and histomorphological alterations that may lead to OSCC development [4]. According to the World Health Organization Collaborating Centre for Oral Cancer (2020), the OPMD group is composed of: Leukoplakia, Proliferative Verrucous Leukoplakia (PVL), Erythroplakia, Oral Submucous Fibrosis (OSF), Oral Lichen Planus (OLP), Actinic Keratosis (Actinic Cheilitis) (AK/AC), Palatal Lesions in Reverse Smokers, Oral Lupus Erythematosus (OLE), Dyskeratosis Congenita (DC), Oral Lichenoid Lesion (OLL), and Oral Graft versus Host Disease (OGVHD) [1].
Communication with the patient has been recognized as one of the most important skills by practitioners to help approach difficult issues and focus on patients’ values and preferences. Professional-patient communication has several potential positive outcomes, including reduced patient anxiety, increased patient satisfaction, motivation and adherence to healthy behaviors, and better oral health outcomes [5,6,7]. Delivering bad news has been widely studied in the oncological settings, however, communication protocols for the diagnosis of OPMDs are unknown, even knowing the clinical and psychosocial impact. Thus, this review seeks relevant and sensitive aspects of communication following the diagnosis of an OPMD, emphasizing topics such as risk of malignant transformation, signs and symptoms observed, changes in lifestyles, cessation of exposure to risk factors, uncertainties related to treatment and the necessity for lifelong follow-up [8,9,10,11,12,13].
Since professional-patient communication about the diagnosis of OPMDs has been sparsely addressed in the scientific literature, a scoping review was the preferred study design by the authors, rather than a systematic review, to examine a comprehensive range of available sources and synthesize the evidence on communication techniques, truth-telling in OPMDs communication, and the clinical and psychosocial impacts of patients. Moreover, we intend to report gaps in the knowledge for future primary studies that investigate communication strategies for patients diagnosed with OPMDs.
2. Materials and Methods
2.1. Protocol and registration
This scoping review was performed according to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses extension for Scoping Reviews (PRISMA-ScR) [14] (Supplementary File 1). A protocol describing the research design was registered on Open Science Framework (OSF) (https://osf.io/az3fy).
2.2. Information sources and search
Medline/PubMed, Embase, Web of Science, and Scopus databases were searched for studies published until October 12, 2021. Additionally, a search on the grey literature (Google Scholar) was carried out and the reference lists of included studies was manually screened looking for additional relevant studies. The search was conducted by combining three groups of keywords (communication, oral potentially malignant disorders, and oral cavity), each of them containing their synonyms or related keywords, and combined with the Boolean operator “and”. Supplementary Table 1 shows the search strategy used in each database.
2.3. Selection of sources of evidence
Once the search was completed, all citations were uploaded into EndNote X7 (Clarivate Analytics, PA, USA) and duplicate records were removed. The titles and abstracts of all studies identified in the electronic searches were individually read by two reviewers (L.P.A.A. and A.R.S.S.), excluding articles that clearly did not meet the eligibility criteria using the online software Rayyan (Qatar Computing Research Institute, Doha, Qatar) [15]. The two reviewers proceeded with reading the full text of the articles screened to identify the eligible articles, and all the primary reasons for exclusions were registered. The study selection was always based on full-text assessment.
The inclusion criteria of this scoping review were applied following the question based on the PCC (Population, Concept and Context): Are there protocols about correctly informing diagnosis to patients with OPMDs? When correctly informed what is its clinical and psychosocial impact? In which, Population: Patients diagnosed with OPMD with no restrictions regarding sex, ethnicity, age, or geographic location. Concept: studies related to the main topics that a patient with OPMD should be aware of (clinical manifestations, the probability of progressing to OSCC, risk factors of OPMDs, treatment uncertainties, lifelong follow-up, and psychosocial impacts). Context: studies describing communication strategies, recommendations, or protocols, with an emphasis on the perception of patients and clinicians about the diagnosis and management of OPMD. No restrictions regarding language nor publication date were applied.
The following exclusion criteria were applied: (1) studies of oral conditions other than OPMD; (2) potentially malignant conditions in anatomical sites other than the oral cavity; (3) clinical trials focused only on screening, risk factors, diagnosis or diagnostic test accuracy, and treatment of OPMD; (4) laboratory research with animal experimentation and in vitro studies, conference abstracts, posters, book chapters, and full-text not available; (5) overlapping information, we included the most recently reported or those providing more data.
2.4. Data synthesis and descriptive analysis
From the included studies, a data sheet was created for the extraction of data regarding the publication characteristics (authors, study design, country, publication year), OPMD type, and communication characteristics according to relevant topics for clinician and patients when an OPMD is diagnosed. Due to the strong evidence gaps that were noted about communication of bad news on OPMDs, the authors designed descriptive recommendations related to the main topics that the health professional should be aware of when communicating to the patient with an OPMD, considering the patients' preferences and values. These recommendation strategies were built by carefully analyzing all the aspects and topics addressed in the different published outcomes related to patients-professional perception about OPMD diagnosis.
3. Results
3.1. Selection and characteristics of sources of evidence
The search resulted in 9,124 identified records and 6,455 records remained after duplicates were removed. 6,437 references were excluded during initial screening of titles and abstracts, remaining 18 studies for phase 2 of study selection. After full-text assessment, 13 studies were excluded (Supplementary Table 2) and 5 studies were included in the scoping review, of which one was a comment [16], one was a review [17], two were qualitative studies [18,19] and one reported a case series [20] (Figure 1).
Two studies assessed oral leukoplakia exclusively, other two evaluated OPMDs without describing which clinical subtypes were included, and one study reported 13 cases of OPMDs including: oral leukoplakia, palatal lesions in reverse smokers, erythroplakia, PVL, OLP, OLL, OLE, and OSF. The United Kingdom (n=1), The Netherlands (n=2), India (n=1), and Taiwan (n=1) were the countries where the included studies were carried out. Table 1 summarizes the characteristics of the five selected studies.
3.2. Synthesis of results
The results related to the communication themes that were part of the purpose of this scoping review are presented in Table 2. We could identify some critical issues regarding OPMDs communication, such as insecurity to talk about the diagnosis, need for training on communication techniques, and inadequate patient health literacy [16,18,19]. According to the main topics covered in the literature, communication on OPMDs related to risk factors, malignant transformation, treatment approaches, follow-up approaches, and clinical/psychosocial impacts were collected. In addition, patients' preferences and some general recommendations reported in the included studies were obtained. Therefore, the absence of specific protocols on how to communicate the diagnosis of OPMDs creates a problem, as it is necessary to identify relevant information to the patient and tell the truth when communicating OPMDs. In Table 3, we have created a list of recommended strategies for OPMD communication.
4. Discussion
We reviewed studies from different parts of the world, noting the clinical and psychological impacts that giving bad news relaying an OPMD diagnosis has on patients and their families. Unfortunately, there are no studies focused on communication protocols for patients who are diagnosed with OPMDs. For this reason, the present scoping review extracted and synthesized the main results that would be relevant in OPMD communication. We mainly focused on the following aspects that we consider imperative when diagnosing an OPMD: risk factors related to the disorder, malignant transformation rates, physical impairment and functional limitations, psychological and social impacts, and treatment-related (treatment uncertainties, effects of treatment on daily life, lifelong follow-up factors).
4.1. Challenges for professionals in delivering bad news regarding OPMDs
There are protocols based on communicating bad news in the medical context and, in relation to the dentistry field, a recent review of communication protocols in oral cancer patients showed available models such as SPIKES and ABCDE, which recommend communication techniques considering patients’ preferences [7,21]. In a personal view study about telling the truth to patients with cancer, the author highlights the following sentence which could also be applicable in the context of OPMDs: “when the relationship between patients and their oncologists is recognized as an open-ended dynamic process of ascertainment and constant reassessment of a truth shared between them, it acquires a different strength and character. Truth-telling then becomes a bidirectional process aimed at constructing—rather than merely discovering—the truth and at helping people with cancer to make sense of having and living with their disease” [6].
OPMDs communication carries several challenging points for professionals, as there is still controversy about the different diagnostic techniques, the correlation with the histopathological characteristics, the uncertainties with the choice of treatment, and the probability of the disease recurrence or turning into cancer, among others. All this means that the scientific evidence has not yet reached consensus or uniformity with the different techniques of diagnosis, treatment, and follow-up [16,17].
Health literacy has been reported as one of the most important factors to take into consideration when communicating bad news, and represents a challenge for health professionals, as several studies demonstrate the difficulty of communication with patients possessing inadequate health literacy [9,22]. In oncology, for example, one study has shown that adequate health literacy is necessary in terms of understanding and using cancer prevention and early detection strategies. In addition, patients are unaware of the main symptoms and signs of cancer, which may lead to the late diagnosis. On the other hand, there are verbal and written communication barriers that generate difficulties in relation to cancer treatment, as there are risks and benefits that must be understood and communicated correctly prior to decision-making [23]. The aforementioned challenge shows an interesting point that we must take into account when communicating an OPMD, as knowing the patient's health literacy level can help with the necessary tools, as well as the appropriate words, to deliver the OPMD diagnosis.
4.2. Communication about risk factors related to OPMDs
There is a group of known risk factors associated with OPMD such as tobacco use, alcohol consumption, betel quid chewing, sun exposure, to a lesser extent transmitted infection of human papillomavirus (HPV, mainly type 16), oral microbiome alteration, among others, that are well recognized [24]. Communication on risk factors was shown in one study that reported proactivity by dentists in talking about smoking cessation, however, some of the professionals were not comfortable talking about alcohol as a risk factor or quitting / moderation of alcohol use [18]. Communication about risk factors directly depends on the geographic region and the prevalence of OPMD, as certain cultural risk factors influence the type and pattern of disorders. For example, betel quid/areca nut chewing habits are widely prevalent in South Asian populations resulting in a greater prevalence of OPMDs [25]. Another challenging component in risk factor communication is when an OPMD is found in patients with different epidemiological profiles and with no exposure to an environmental factor, in other words, factors other than tobacco and alcohol which may be implicated in the development of oral cancer as encountered in some younger patients. The dentist must be able to provide a balanced biological context for patients' questions about their OPMDs diagnosis and the absence of external risk factors, as well as when they compare with people exposed to risk factors without a diagnosis of OPMD.
4.3. Communication about rates of malignant transformation
Reporting rates of malignant transformation must be within the epidemiological and clinicopathological context of each patient, as each type of OPMD has a highly variable rate of malignant transformation [3]. Currently, the grade of dysplasia present within an OPMD is seen as the most reliable marker for malignant transformation [26]. However, investigations about molecular techniques assessing the prognostic value of biomarkers for OPMD are still insufficient to support the malignant transformation, especially regarding their clinical application [4]. In this scoping review, it was not possible to observe direct results in patient communication about rates of malignant transformation, however, we found some studies that reported higher degrees of anxiety when the patient was informed about the chance of the lesion progressing into cancer [19,27].
4.4. Treatment-related communication
Treatment-related communication in the OPMDs context is even complicated by a lack of robust evidence concerning both treatment effectiveness for OPMDs and future OSCC risk [28]. The decisions related to the type of treatment are the most controversial in the literature, and this decision should be based on the published evidence, circumstances and context of each patient. It is necessary to inform the patient about the uncertainties in outcomes of treatment, always lay out the facts so they do not feel disappointed about having to repeat the same intervention or change direction of management [9]. Follow-up protocols change depending on the type of OPMD. Furthermore, there is no consensus on the specific time interval for follow up/surveillance as there are no studies showing efficacy regarding better clinical outcomes [16,17]. However, periodic follow-up visits are advised in all OPMD cases [29]. Patients must understand that although the time interval depends on clinical criteria, they will need to undergo lifelong follow-up.
4.5. Communicating clinical/psychosocial implications to patients
No specific protocol studies were found to learn on communicating the clinical and psychological impacts of patients who are diagnosed with OPMD. However, during literature search carried out in this study, we observed that there are many studies concerning quality of life in patients diagnosed with OPMDs, particularly, those related to lichen planus, leukoplakia, and oral submucous fibrosis [8,9,10,11,12,13]. The findings of these studies suggested that in general, the signs and symptoms generated by OPMDs are the most important factors due to physical impairment and functional limitations. OPMD has a debilitating effect on psychological well-being and social interactions, thus, patients should be informed about future physical and psychosocial problems and try to delineate treatment plans focused on reducing these impacts.
4.6. Patients' preferences on OPMD communication
The patient's perception of the OPMD diagnostic process has been reported in screening studies and diagnostic test accuracy that reported patients’ values and preferences in the assessment of clinically evident lesions in the oral cavity [29,30]. The three main topics reported by the authors were: (i) fear and anxiety as some of the most relevant barriers for seeking care; (ii) the acceptability of conducting a clinical examination to identify OPMD; and the last and most important: (iii) participants highlighted the interest of being educated about ways to reduce their risk of having oral cancer and suggested that mass media coverage could be an effective way to increase awareness about the early manifestation of OPMD and OSCC. Nevertheless, the authors conclude that more information on patients' values and preferences is required [29]. Studies on web-based information have revealed the presence of misinformation in the electronic media on the subject of OPMDs and the necessity to develop and portray accurate information on this topic to the general public [31,32]. Professional organizations concerned with Oral Medicine have the duty to publish such electronic patient information leaflets.
4.7. General recommendations on OPMD communication
Diagnosis of OPMDs can occur in private practice by a clinician or at academic institutions. Thus, communication skills are recommended as part of the curriculum in dental schools. [33]. Breaking bad news not only might be challenging for the patient and caregivers, but also for a student without any experience [34]. Worked examples and simulated patients are resourceful strategies that could benefit teaching these difficult communications skills to students [34,35,36]. Communication skills training could also include role-play sessions, videos on patient communications, presentation and experience sharing from tutors and senior students [37].
Our findings clearly indicate that more qualitative investigations are needed to determine communication protocols for each type of OPMD, as well as to identify the perception of professionals and patients. As noted, only leukoplakia was directly related to communication, and its author outlined relevant information on how this information should be reported to a patient [16,17]. Therefore, it is necessary to implement adequate communication strategies and to provide effective communication protocols for full range of OPMDs.
The potential limitation of the present scoping review was the limited data reported to answer communication protocols in OPMD diagnosis. Future studies should focus on determining what information is provided for patients diagnosed with common OPMDs and, on the other hand, determining what questions patients have asked their dentists and what information they prioritize about OPMD. The main strength of our study is fundamentally due to its originality, as it is the first scoping review that offers to address the main highlights in the OPMD communication based on scientific evidence.
5. Conclusions
Finally, the most obvious finding to emerge from this study is that there are no communication protocols for patients who are diagnosed with OPMDs. Healthcare professionals must develop and practice communication skills throughout their training and practice; starting by incorporating specific training in Dental School curriculum. Due to limitation of time available in clinical settings, developing and making available an easily accessible and accurate web-based patient information sheet that could be recommended to an OPMD patient should be considered by professional bodies. Recommendations such as applying the SPIKES protocol in clinical practice and telling the truth to the patient based on scientific evidence are strategies exposed in this scoping review.
Supplementary Materials
The following supporting information can be downloaded at the website of this paper posted on Preprints.org. Table S1: Database search strategy; Table S2: Excluded articles and the reasons for exclusion (n=13); File S1: PRISMA-ScR checklist.
Author Contributions
Conceptualization, L.P.A.A. and A.R.S.S.; methodology, L.P.A.A. and T.C.E.P.; formal analysis, L.P.A.A., T.C.E.P., M.D.F.; investigation, L.P.A.A., M.A.L. and A.R.S.S.; resources, M.A.L.; data curation, L.P.A.A. and T.C.E.P.; writing—original draft preparation, L.P.A.A.; writing—review and editing, T.C.E.P. and M.D.F.; visualization, J.B.E., C.A.M., S.W.; supervision, J.B.E., C.A.M., S.W.; project administration, A.R.S.S.; funding acquisition, none. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
Not applicable.
Acknowledgments
The authors would like to gratefully acknowledge the financial support of the Coordination for the Improvement of Higher Education Personnel – Brazil (CAPES) – Finance code: 001 and of the National Council for Scientific and Technological Development (CNPq), Brazil.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Warnakulasuriya, S.; Kujan, O.; Aguirre-Urizar, J.M.; Bagan, J.V.; González-Moles, M.; Kerr, A.R.; Lodi, G.; Mello, F.W.; Monteiro, L.; Ogden, G.R.; et al. Oral potentially malignant disorders: A consensus report from an international seminar on nomenclature and classification, convened by the WHO Collaborating Centre for Oral Cancer. Oral Dis. 2020, 27, 1862–1880. [Google Scholar] [CrossRef] [PubMed]
- Mello, F.W.; Miguel, A.F.P.; Dutra, K.L.; Porporatti, A.L.; Warnakulasuriya, S.; Guerra, E.N.S.; Rivero, E.R.C. Prevalence of oral potentially malignant disorders: A systematic review and meta-analysis. J. Oral Pathol. Med. 2018, 47, 633–640. [Google Scholar] [CrossRef] [PubMed]
- Iocca, O.; Sollecito, T.P.; Alawi, F.; Weinstein, G.S.; Newman, J.G.; De Virgilio, A.; Di Maio, P.; Spriano, G.; López, S.P.; Shanti, R.M. Potentially malignant disorders of the oral cavity and oral dysplasia: A systematic review and meta-analysis of malignant transformation rate by subtype. Head Neck 2019, 42, 539–555. [Google Scholar] [CrossRef] [PubMed]
- Nikitakis, N.G.; Pentenero, M.; Georgaki, M.; Poh, C.F.; Peterson, D.E.; Edwards, P.; Lingen, M.; Sauk, J.J. Molecular markers associated with development and progression of potentially premalignant oral epithelial lesions: Current knowledge and future implications. Oral Surgery, Oral Med. Oral Pathol. Oral Radiol. 2018, 125, 650–669. [Google Scholar] [CrossRef]
- Ranjan, P. How can Doctors Improve their Communication Skills? J. Clin. Diagn. Res. 2015, 9, JE01–4. [Google Scholar] [CrossRef]
- Surbone, A. Telling the truth to patients with cancer: what is the truth? Lancet Oncol. 2006, 7, 944–950. [Google Scholar] [CrossRef]
- Alves, C.G.B.; Treister, N.S.; Ribeiro, A.C.P.; Brandão, T.B.; Tonaki, J.O.; Lopes, M.A.; Rivera, C.; Santos-Silva, A.R. Strategies for communicating oral and oropharyngeal cancer diagnosis: why talk about it? Oral Surgery, Oral Med. Oral Pathol. Oral Radiol. 2020, 129, 347–356. [Google Scholar] [CrossRef]
- Tadakamadla, J.; Kumar, S.; Johnson, N.W. Quality of life in patients with oral potentially malignant disorders: a systematic review. Oral Surgery, Oral Med. Oral Pathol. Oral Radiol. 2015, 119, 644–655. [Google Scholar] [CrossRef]
- Tadakamadla, J.; Kumar, S.; Lalloo, R.; Johnson, N.W. Qualitative analysis of the impact of Oral Potentially Malignant Disorders on daily life activities. PLOS ONE 2017, 12, e0175531. [Google Scholar] [CrossRef]
- Tadakamadla, J.; Kumar, S.; Lalloo, R.; Babu, D.B.G.; Johnson, N.W. Impact of oral potentially malignant disorders on quality of life. J. Oral Pathol. Med. 2017, 47, 60–65. [Google Scholar] [CrossRef]
- Gondivkar, S.M.; Gadbail, A.R.; Gondivkar, R.S.; Sarode, S.C.; Sarode, G.S.; Patil, S. Impact of oral potentially malignant disorders on quality of life: a systematic review. Futur. Oncol. 2018, 14, 995–1010. [Google Scholar] [CrossRef] [PubMed]
- Gondivkar, S.M.; Bhowate, R.R.; Gadbail, A.R.; Sarode, S.C.; Patil, S. Quality of life and oral potentially malignant disorders: Critical appraisal and prospects. World J. Clin. Oncol. 2018, 9, 56–59. [Google Scholar] [CrossRef] [PubMed]
- Kumar, K.; Khandpur, M.; Khandpur, S.; Mehrotra, D.; Tiwari, S.C.; Kumar, S. Quality of life among Oral Potentially Malignant Disorder (OPMD) patients: A prospective study. J. Oral Biol. Craniofacial Res. 2020, 11, 88–91. [Google Scholar] [CrossRef] [PubMed]
- Tricco, A. C.; Lillie, E.; Zarin, W.; O’Brien, K. K.; Colquhoun, H.; Levac, D.; Moher, D.; Peters, M. D. J.; Horsley, T.; Weeks, L.; et al. PRISMA Extension for Scoping Reviews (PRISMA-ScR): Checklist and Explanation. Ann Intern Med 2018, 169, 467–473. [Google Scholar] [CrossRef]
- Ouzzani, M.; Hammady, H.; Fedorowicz, Z.; Elmagarmid, A. Rayyan—A web and mobile app for systematic reviews. Syst. Rev. 2016, 5, 210. [Google Scholar] [CrossRef]
- van der Waal, I. Knowledge about oral leukoplakia for use at different levels of expertise, including patients. Oral Dis. 2018, 24, 174–178. [Google Scholar] [CrossRef]
- van der Waal, I. Oral Leukoplakia: Present Views on Diagnosis, Management, Communication with Patients, and Research. Curr. Oral Heal. Rep. 2019, 6, 9–13. [Google Scholar] [CrossRef]
- Brocklehurst, P.R.; Baker, S.R.; Speight, P.M. A qualitative study examining the experience of primary care dentists in the detection and management of potentially malignant lesions. 2. Mechanics of the referral and patient communication. Br. Dent. J. 2010, 208, E4–E4. [Google Scholar] [CrossRef]
- Lin, H.-Y.; Chen, S.-C.; Peng, H.-L.; Chen, M.-K. Unmet information needs and clinical characteristics in patients with precancerous oral lesions. Eur. J. Cancer Care 2015, 24, 911–919. [Google Scholar] [CrossRef]
- Raman, P. Communication, Counseling and Compassionate Care: The least explored and challenging Palliative Care approaches among Primary Care Physicians - Clinical Case series of Oral Potentially malignant disorders in Tamil Nadu. J. Fam. Med. Prim. Care 2021, 10, 572–577. [Google Scholar] [CrossRef]
- Baile, W.F.; Buckman, R.; Lenzi, R.; Glober, G.; Beale, E.A.; Kudelka, A.P. SPIKES—A Six-Step Protocol for Delivering Bad News: Application to the Patient with Cancer. Oncol. 2000, 5, 302–311. [Google Scholar] [CrossRef] [PubMed]
- Rozier, R.G.; Horowitz, A.M.; Podschun, G. Dentist-patient communication techniques used in the United States. J. Am. Dent. Assoc. 2011, 142, 518–530. [Google Scholar] [CrossRef]
- Marin, E.; Davis, T.C.; Williams, M.V.; Ma, E.M.; Parker, R.M.; Glass, J. Health Literacy and Cancer Communication. CA: A Cancer J. Clin. 2002, 52, 134–149. [Google Scholar] [CrossRef]
- Lorini, L.; Atín, C.B.; Thavaraj, S.; Müller-Richter, U.; Ferranti, M.A.; Romero, J.P.; Barba, M.S.; García-Cuenca, A.d.P.; García, I.B.; Bossi, P.; et al. Overview of Oral Potentially Malignant Disorders: From Risk Factors to Specific Therapies. Cancers 2021, 13, 3696. [Google Scholar] [CrossRef] [PubMed]
- Gunjal, S.; Pateel, D.G.S.; Yang, Y.-H.; Doss, J.G.; Bilal, S.; Maling, T.H.; Mehrotra, R.; Cheong, S.C.; Zain, R.B.M. An Overview on Betel Quid and Areca Nut Practice and Control in Selected Asian and South East Asian Countries. Subst. Use Misuse 2020, 55, 1533–1544. [Google Scholar] [CrossRef]
- Odell, E.; Kujan, O.; Warnakulasuriya, S.; Sloan, P. Oral epithelial dysplasia: Recognition, grading and clinical significance. Oral Dis. 2021, 27, 1947–1976. [Google Scholar] [CrossRef]
- Rana, M.; Gellrich, N.-C.; Rana, M. Comparison of health-related quality of life of patients with different precancer and oral cancer stages. Clin. Oral Investig. 2014, 19, 481–488. [Google Scholar] [CrossRef]
- Kerr, A.R.; Lodi, G. Management of oral potentially malignant disorders. Oral Dis. 2021, 27, 2008–2025. [Google Scholar] [CrossRef]
- Lingen, M.W.; Abt, E.; Agrawal, N.; Chaturvedi, A.K.; Cohen, E.; D’souza, G.; Gurenlian, J.; Kalmar, J.R.; Kerr, A.R.; Lambert, P.M.; et al. Evidence-based clinical practice guideline for the evaluation of potentially malignant disorders in the oral cavity. J. Am. Dent. Assoc. 2017, 148, 712–727. [Google Scholar] [CrossRef]
- Lingen, M.W.; Tampi, M.P.; Urquhart, O.; Abt, E.; Agrawal, N.; Chaturvedi, A.K.; Cohen, E.; D’souza, G.; Gurenlian, J.; Kalmar, J.R.; et al. Adjuncts for the evaluation of potentially malignant disorders in the oral cavity. J. Am. Dent. Assoc. 2017, 148, 797–813. [Google Scholar] [CrossRef]
- Alsoghier, A.; Ni Riordain, R.; Fedele, S.; Porter, S. Web-based information on oral dysplasia and precancer of the mouth – Quality and readability. Oral Oncol. 2018, 82, 69–74. [Google Scholar] [CrossRef]
- Panta, P.; Sarode, S.C.; Sarode, G.S.; Patil, S. Potential of web-resource on ‘oral dysplasia and precancer’! Oral Oncol. 2018, 84, 126–127. [Google Scholar] [CrossRef] [PubMed]
- Güneri, P.; Epstein, J.; Botto, R.W. Breaking bad medical news in a dental care setting. J. Am. Dent. Assoc. 2013, 144, 381–386. [Google Scholar] [CrossRef]
- Karnieli-Miller, O.; Pelles, S.; Meitar, D. Position paper: Teaching breaking bad news (BBN) to undergraduate medical students. Patient Educ. Couns. 2022, 105, 2899–2904. [Google Scholar] [CrossRef] [PubMed]
- Curtin, S.; McConnell, M. Teaching dental students how to deliver bad news: S-P-I-K-E-S model. J Dent Educ 2012, 76, 360–365. [Google Scholar] [CrossRef] [PubMed]
- Bosshard, M.; Schmitz, F.M.; Guttormsen, S.; Nater, U.M.; Gomez, P.; Berendonk, C. From threat to challenge—Improving medical students’ stress response and communication skills performance through the combination of stress arousal reappraisal and preparatory worked example-based learning when breaking bad news to simulated patients: study protocol for a randomized controlled trial. BMC Psychol. 2023, 11, 1–14. [Google Scholar] [CrossRef]
- Botelho, M.G.; Lee, U.Y.A.; Luk, K.Y.C. An exploration of clinical communication needs among undergraduate dental students. Eur. J. Dent. Educ. 2022, 27, 707–718. [Google Scholar] [CrossRef]
Figure 1.
Flow diagram of literature search and selection criteria adapted from PRISMA.
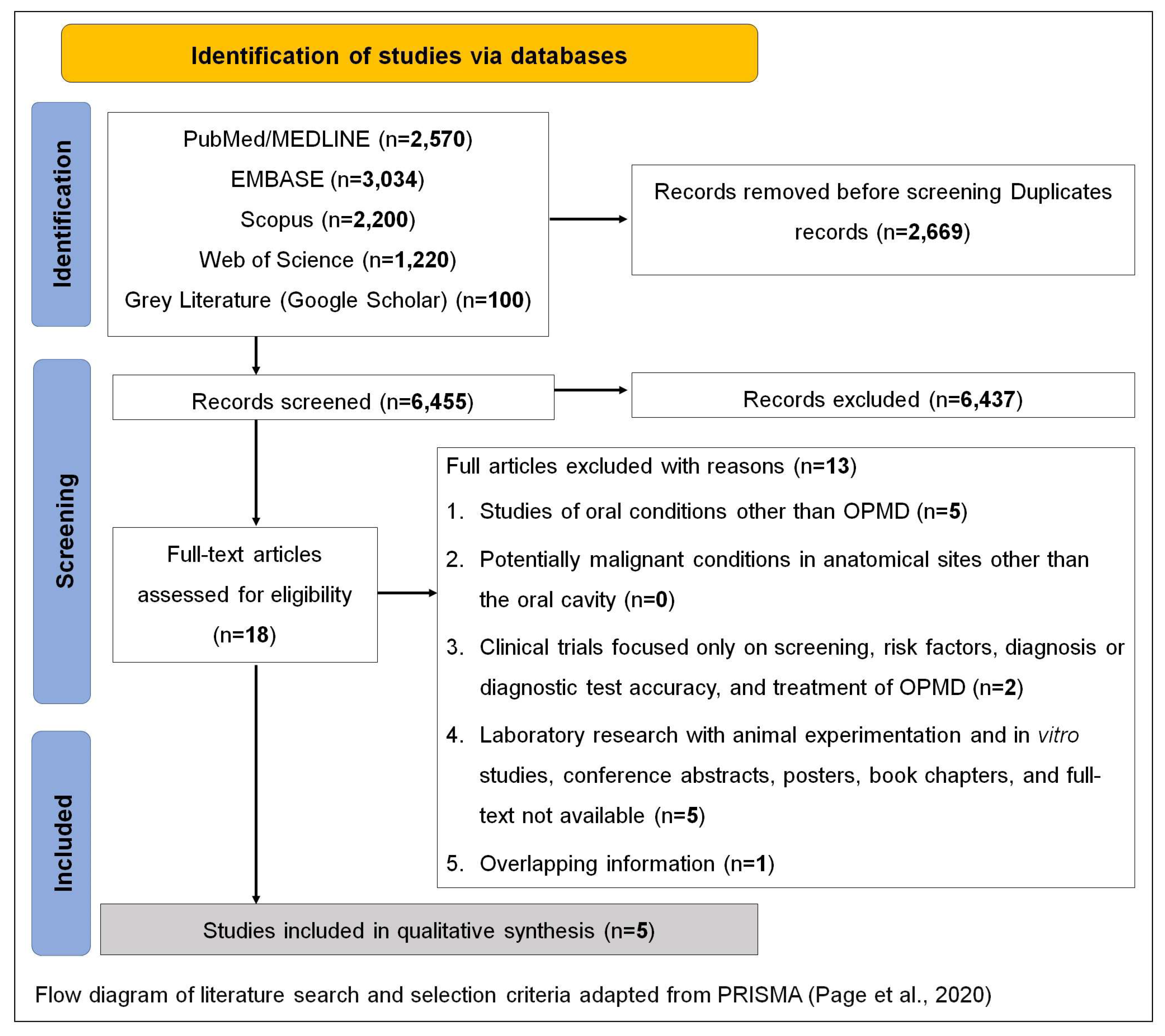

Table 1.
Characteristics of the five included studies.
| # | Author (Year) | Country | Study design | Population | Sample | OPMD studied | Thematic aspects on OPMD communication |
|---|---|---|---|---|---|---|---|
| 1 | Brocklehurst et al. (2010) [18] | The United Kingdom | Semi-structured interviews | Dental practices | 18 | OPMD | Information that is given to the patient The patient's response to being told that a potentially malignant lesion has been detected The advice given to the patient about the known risk factors of malignant disease Comments on the management of potentially malignant disorders in practice before a referral is made Practical aspects of the referral process detailing how dentists refer and who they send their referrals to |
| 2 | Raman P. (2021) [20] | India | Case report | Patients with OPMD | 13 | Oral Leukoplakia Palatal Lesions in Reverse Smokers Erythroplakia PVL OLP OLL OLE OSF |
Communication and habit counseling of patients with OPMD |
| 3 | Van der Waal I. (2018) [16] | The Netherlands | Comment | NA | NA | Leukoplakia | This study discussed how the subject of oral leukoplakia might be communicated among the various healthcare workers and among patients The article comments aspects such as definition, clinical classification, biopsy, the presence of epithelial dysplasia is an important risk marker of malignant transformation, |
| 4 | Van der Waal, I. (2019) [17] | The Netherlands | Review | NA | NA | Leukoplakia | How to inform a patient who has a leukoplakia? |
| 5 | Lin H, et al (2015) [19] | Taiwan | Cross-sectional descriptive study | Patients with OPMD | 106 | OPMD | This study investigated: anxiety, attitudes towards cancer prevention and unmet information needs; differences in anxiety and attitudes towards cancer prevention between met and unmet information needs; and the associated factors of unmet information needs for patients with precancerous oral lesions. |
* Legend: OSF: Oral Submucous Fibrosis; OLP: Oral Lichen Planus; OLE: Oral Lupus Erythematosus; OLL: Oral Lichenoid Lesion; PVL: Proliferative Verrucous Leukoplakia (PVL).
Table 2.
Findings according with OPMD communication.
| OPMD themes | Findings |
|---|---|
| Insecurity to talk about the diagnosis | • “The most common explanation given to patients, once a lesion was found, was that the dentist would like a second opinion” [18] • “There was a concern expressed by some primary care dentists about the problem of not providing the patient with enough information to prompt them to attend for their appointment with secondary care” [18] |
| Need for training on communication techniques | • “The appropriate use of language was a concern for many dentists in order to avoid patient anxiety. In fact, some would deliberately describe the lesion in different terms, avoiding any terms associated with malignancy” [18] • “The present study suggests that more can be done to train primary care dentists in health promotion and patient communication” [18] |
| Patient health literacy | • “It is a challenge to properly inform patients affected by leukoplakia. Some patients are very well educated and are looking for rather detailed information at a high, sometimes even academic level. They may want to be involved in the decisions that have to be taken, for example, in the taking of a biopsy or, even more so, in the decision to be treated or not to be treated” [16] • “The majority of patients, want to be guided in their decision-making by their doctor and will ask for clear and concise information. One should realize that most of the available information on oral leukoplakia, in writing or through the Internet, is much too complicated for lay people” [16] • “Health education and individual counselling should be provided to satisfy the information needs of this population” [19] • “Patients with unmet information needs had higher levels of anxiety than those whose information needs were met poor health literacy for patients who had betel nut use, low health literacy and insufficient skills for obtaining, reading and understanding information to make appropriate health decisions” [19] |
| Risk factors | • “While some of the dentists did provide leaflets at their practice, there were also some who did not believe in providing patients with any more information” [18] • “Many practices were proactive in talking about smoking cessation” [18] • “A common complaint among those dentists who had tried to provide smoking cessation was that they felt frustrated because it had no unit of dental activity value and they could not prescribe the nicotine replacement therapy” [18] • “Further work is required to understand why dentists do not feel comfortable talking about alcohol as a risk factor” [18] • “Patients with precancerous oral lesions who had high levels of state anxiety, long duration of time since quitting betel nut chewing and were without a history of oral cancer were more likely to have unmet information needs” [19] • “The participants in our study reported betel nut use and showed passive motivation for regular oral mucosal screening, indicating that they were at risk for developing pre-malignant oral lesions” [19] • “Enhancing provider–patient interaction and presenting essential information first can help patients follow the instructions for cancer prevention” [19] • “Unmet information needs were associated with the time since quitting betel nut chewing and a history of oral cavity cancer. Patients who had quit using a harmful substance and who also had previous illness experiences were different from those who were willing to adopt health promotion behavior such as cancer prevention. Because of their prior experience of illness and their decision to quit betel nut chewing, these patients might have a higher intention to participate in oral mucosal screening, including regular follow-up testing and future cancer prevention program” [19] |
| Malignant transformation | • Leukoplakia: “A probably frequently occurring confusion is that, in the absence of epithelial dysplasia, the pathologist may conclude his report by saying “This is not a premalignant lesion.” As mentioned before, oral leukoplakia is primarily a clinical term without specific histopathological features. At histopathological examination, one may or may not observe epithelial dysplasia” [16] • “The patient should be informed that the leukoplakia may recur within a period varying from some weeks, months, or several years. They also should know that the risk of oral cancer development may not be eliminated by the excision. Although the efficacy of follow-up visits has never been shown, it seems preferable to offer such visits, mainly for reassurance of the patient" [17] |
| Treatment approaches | • “Oral leukoplakia can be treated by a variety of modalities such as cold-knife surgery or laser surgery, CO2 evaporation, photodynamic treatment, and non-medical treatments. As has been shown in numerous studies, including a Cochrane review, not any of these treatment modalities are truly effective in preventing or decreasing the risk of malignant transformation. Therefore, the question remains whether or not to treat oral leukoplakia” [16] • “Spontaneous regression of non-dysplastic leukoplakia is in my experience extremely rare as well” [16] • “The increased morbidity in such instances should be properly weighted against the expected benefit of the treatment” [16] • “In large, diffuse or multiple oral leukoplakias, one may choose to perform an “excisional” biopsy of the clinically most suspected area only, if present, or to perform multiple biopsies (mapping). In any case, the patient should play an important role in this shared decision taking. Some will prefer not to have active treatment while others persist to be treated, even in case of extensive or multiple oral leukoplakias. A similar divergence in opinion may arise in case of recurrence. Some patients do not want to undergo treatment again, while others insist on retreatment” [17] • “The inadequate expression of emotions and lack of stress release may interfere with information-seeking and treatment decisions. Support and listening are needed to help these patients deal with the treatment-decision process” [19] |
| Follow-up approaches | • “There is no evidence that lifelong follow-up programs for treated or untreated patients with leukoplakia are effective in preventing the development of oral cancer. Most likely, follow-up programs will not result in improved survival in case of cancer development either. Nevertheless, it is common practice, i.e. For reassurance of the patient, to follow up the patients. Depending on various aspects, such as the extent of the leukoplakia and the presence and degree of epithelial dysplasia, intervals may vary from 3 to 6 months, lifelong. Changes in the clinical presentation and, particularly, symptoms are ominous signs of malignant transformation” [16] • “It is well understood that such follow-up programs may not be feasible all over the world. Besides, there is the issue of patients’ compliance. After several years of uneventful follow-up, some patients will discontinue the follow-up program” [16] |
| Clinical/psychosocial impacts | • “Patients reported their mouth condition having a debilitating effect on their psychological well-being and social interactions” [9] • “Physical impairment and functional limitations’ were the most important theme for many of the patients” [9] • “The impacts of OPMD also extended beyond physical impairment and functional limitations to aspects of daily living, notably psychological and social wellbeing” [9] • “A high level of anxiety about precancerous oral lesions was more prevalent among patients with unmet information needs than among those whose information needs were met” [19] |
| Patient preferences on OPMD communication | • “The majority of the dentists questioned suggested that patients were not overly distressed about a positive screen, they just go along with the suggestion” [18] • “Most patients will not be interested to listen to an academic lecture by their doctor on the various aspects of oral leukoplakia but, instead, they want to be informed in an understandable way particularly when it comes to the further management” [17] • “Patients reported higher information needs related to ‘To be fully informed about your test results as soon as possible.’ and ‘To be fully informed about all of the benefits and side effects of treatment or surgery before you agree to have it.” [19] |
| Recommendations | • “A primary care physician should be responsible, humble, knowledgeable, and skillful to deliver an effective holistic care by inculcating the practice of effective communication of bad news, timely habit cessation counseling and compassionate care as a part of routine dental screening” [20] • “There is a delayed presentation of oral pre cancer and oral cancer in India, as approximately 50% of patients are diagnosed at last stage since the asymptomatic pre cancer lesions are missed by oral physicians/dentists either due to lack of timely communication and habit counseling, lack of knowledge, or inappropriate attitude, putting all in a nut shell - sheer lack of empathy and commitment towards patient care and society” [20] • “The author believes that the three most important, least explored and challenging palliative care approaches namely, “Communication,” “Counseling,” and “Compassionate care,” should be effectively practiced by a primary care physician, to improve their level of commitment to society and attitude towards patient care which can help in early diagnosis of OPMD and decreased incidence of oral cancer, thus improving quality of life of patients” [20] • “Communication on this subject with patients should be in easy to understand wording, avoiding professional terminology as much as possible” [16] • “One may consider to send a brief summary of the discussion held with the patient in easy to understand language” [16] |
Table 3.
Recommendation strategies on patient information in OPMD communication according to the problems and needs observed in the literature.
Table 3.
Recommendation strategies on patient information in OPMD communication according to the problems and needs observed in the literature.
| OPMD themes | Findings |
|---|---|
|
Communication technique SPIKES protocol* [12,21] |
• S: Setting
• P: Perception
• I: Invitation
• K: Knowledge
• E: Empathy
• S: Summarize and strategize
|
|
Telling the truth about: Risk factors Malignant transformation, treatment approaches Follow-up approaches Clinical/psychosocial impacts |
• Know your patient's health literacy level to define the methodology and communication tools that will be used to inform the OPMD diagnosis • Have leaflets with images that help explain the diagnosis to the patient • Avoid professional terminology as much as possible • Speak proper terms of malignancy “the white or red patch can turn into cancer” • Inform about the risk factors associated with diagnosed OPMD, and explain the scientific reasons for this association • Raise awareness of the importance of avoiding life style risk factors when they are present • Inform about the potential malignancy rate of diagnosed OPMD according to the clinical, demographic and geographic characteristics of the population in which the patient is inserted • Talk about the uncertainties that exist in determining whether the diagnosed OPMD will change to oral cancer • Inform about the main clinical manifestations of diagnosed OPMD, as well as the impact that these manifestations could have on daily life • Explain the available treatment modalities and make a decision prioritizing the patients' well-being, the potential morbidities of treatment (eg. excision of large areas) as well as their values and preferences • Talk about the uncertainties that exist regarding recurrence and malignant transformation, even after treatment • Raise awareness of the need for continuous follow-up throughout life, especially with the aim of avoiding late diagnosis • Explain that the interval between follow-up appointments will depend on several factors, such as clinical characteristics, the professional's judgment and updates of scientific evidence on follow-up protocols for each OPMD • Although a patient's health literacy is relevant to understanding their condition, ask the patient repeatedly about the doubts and emphasize the most important points until he/she fully understands • Explain to observe any changes of symptoms (eg. pain) and report back even before the next review appointment |
| Recommendations for dental students | • In the academic setting, dental students must repeatedly accompany the senior professional in communicating bad news, in order to have the opportunity to learn and practice, before carrying out the communication alone. • Training in communications skills, the SPIKES protocol, possible emotional reactions from patients and caregivers, as well as having the knowledge to answer questions they might have should be included in dental school curriculum • Different teaching modalities by means of education and practice are recommended, such as worked examples and simulated patients, role-play sessions, videos on patient communications, presentation and experience sharing from tutors and senior students |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



