
Submitted:
02 August 2023
Posted:
04 August 2023
You are already at the latest version
Abstract
Pleural mesothelioma (PM) comprises three main subtypes: epithelioid, biphasic and sarcomatoid, which have a different impact on prognosis and treatment definition. However, PM subtyping can be complex given the inter- and intra-tumour morphological heterogeneity. We aim to use immunohistochemistry (IHC) to evaluate five markers (Mesothelin, Claudin-15, Complement Factor B, Plasminogen Activator Inhibitor 1, and p21-activated Kinase 4), whose encoding genes have been previously reported as deregulated among PM subtypes. Immunohistochemical expressions were determined in a case series of 73 PMs, and cut-offs for the epithelioid and non-epithelioid subtypes were selected. Further validation was performed on an independent cohort (30 PMs). For biphasic PM, the percentage of the epithelioid component was assessed, and IHC evaluation was also performed on the individual components separately. Mesothelin and Claudin-15 showed a good sensitivity (79% and 84%) and specificity (84% and 73%) for the epithelioid subtype. CFB and PAK4 had an inferior performance, with higher sensitivity (89% and 84%), but lower specificity (64% and 36%). In the biphasic group, all markers showed a different expression when comparing epithelioid with sarcomatoid areas. Mesothelin, Claudin-15 and CFB can be useful in subtype discrimination. PAI1 and PAK4 can improve component distinction in biphasic PM.
Keywords:
pleural mesothelioma
; subtypes
; immunohistochemistry
; Mesothelin
; Claudin-15
; Complement Factor B (CFB)
; Plasminogen Activator Inhibitor 1 (PAI1)
; p21-activated kinase 4 (PAK4).
1. Introduction
Pleural mesothelioma (PM), a rare malignant tumour of the serosae linings, involves the pleuro-pericardial surface [1]. It is a neoplasm closely associated with occupational exposure to asbestos, and median survival in untreated patients is less than a year [2].
To date, the diagnosis of pleural mesothelioma remains difficult. Morphological evaluation may provide some essentials for a correct classification, but it must be assisted by auxiliary diagnostic techniques such as immunohistochemistry (IHC) and, more recently, molecular tests.
The PM classification into three subtypes (epithelioid, sarcomatoid, and biphasic) is based on the presence of epithelioid, sarcomatoid, or both histologies in the tumour. Importantly, the subtype classification is a powerful predictor of survival for patients with PM and it influences subsequent treatment [3-5].
Given the inter- and intra-tumour morphological heterogeneity, histological subtyping can be complex. Chirieac and colleagues showed that, while the diagnosis of the sarcomatoid subtype (SS) was consistent in the comparison between diagnostic biopsies and subsequent resections, the concordance in the epithelioid subtype (ES) was lower. In fact, 20% of the epitheloid subtypeS was reclassified as biphasic mesotheliomas in the final diagnosis, because a sarcomatoid component had been evidenced [6].
The usefulness of immunohistochemical markers in the sarcomatoid setting is limited [7] and further markers are needed to identify this component (pure or mixed in the biphasic subtype - BS), owing to its prognostic and therapeutic implications.
Recent studies have focused on gene expression analysis in PM, in order to highlight subtype biomarkers that can be useful to refine histological classification and patient risk stratification [8,9].
In line with these studies, our group has previously analysed the expression of 117 genes, which play a key role in carcinogenesis processes. The results showed that several genes were deregulated in the three PM subtypes.
In particular, five genes were differently expressed across all subtypes: SERPINE 1 (gene encoding for the major inhibitor of tissue plasminogen activation and urokinase) was upregulated in sarcomatoid versus biphasic and in biphasic versus epithelioid PM; CFB (Complement factor B), MSLN (Mesothelin) and CLDN15 (Claudin-15) were all upregulated in epithelioid versus biphasic and in biphasic versus sarcomatoid PM; PAK4 (p21-activated kinase 4) was upregulated in biphasic PM versus the epithelioid subtype and in the latter versus the sarcomatoid PM [10].
The present study aims to validate these five IHC markers, previously selected by gene-expression analysis (Plasminogen Activator Inhibitor 1 – PAI1 – encoded by the SERPINE1 gene, CFB, Mesothelin, Claudin-15, and PAK4), to improve the diagnosis and subtyping of pleural mesothelioma.
2. Materials and Methods
2.1. Study Cohorts
A total of 103 PM patients diagnosed at the University Hospital of Pisa between 2011 and 2022 were included in the study and the samples were retrospectively collected. Two different cohorts were tested. The training cohort included 73 PM specimens previously investigated by gene-expression analysis [10]. In detail, 31 samples were epithelioid PMs (16 biopsies and 15 surgical resections), 25 were biphasic PMs (11 biopsies and 14 surgical resections), and 17 were sarcomatoid PMs (12 biopsies and 5 surgical resections).
The validation cohort consisted of 30 samples, with the following histologic subtypes: 11 epithelioid PMs (5 biopsies and 6 surgical resections), 11 biphasic PMs (9 biopsies and 2 surgical resections), and 8 sarcomatoid PMs (7 biopsies and 1 surgical resection).
All samples were formalin-fixed and paraffin-embedded (FFPE), and were selected from the archive of the Operative Unit of Pathological Anatomy III of the University Hospital of Pisa. The diagnosis and pathological features were independently examined by two pathologists (GA and ID) and, for ES, the tumour grade was assessed according to the 5th edition of the WHO classification of thoracic tumours [1]. For biphasic PM, the percentage of epithelioid components was determined independently by two pathologists, and the median value was considered for statistical evaluation. For surgical resections, the most representative paraffin sample of each neoplasm was selected for immunohistochemical analysis.
2.2. IHC Analysis and Scoring
Immunohistochemical analysis was performed on 3-μm-thick tissue sections that were prepared on slides treated with a positive charge. After deparaffinization in xylene, the sections underwent an antigenic unmasking phase performed by incubation at 100°C for 80 minutes in the ready-to-use solution ULTRA Cell Conditioning 1 Solution (Ventana Medical Systems). Sections were then incubated with antibodies at 36°C for 36 minutes. The following antibodies were used: anti-Plasminogen Activator Inhibitor 1 (murine monoclonal antibody, clone 1D5, Abcam, 1:100 dilution); anti-Complement Factor B (rabbit polyclonal antibody, ThermoFisher, dilution 1:200); anti-Claudin15 (rabbit polyclonal antibody, Abcam, dilution 1:100); anti-p21-activated kinase 4 (rabbit polyclonal antibody, Abcam, dilution 1:600), and anti-Mesothelin (rabbit monoclonal antibody, SP74, Abcam, dilution 1:50). Analysis was conducted with the BenchMark ULTRA semiautomated staining instrument (Ventana Medical Systems), using the UltraView DAB IHC Detection Kit (Ventana Medical Systems). Following a series of washes, the sections were counterstained with Haematoxylin II and with Bluing Reagent (VentanaMedical Systems), dehydrated by passages in ethanol with increasing concentration, and then mounted.
In all cases, immunohistochemical evaluation was performed independently by two pathologists (GA and ID), who were blinded to all clinical and pathological data. Selected cases were discussed with a third pathologist (GF) for confirmation. In our study, mesothelin immunohistochemical expression was scored for membranous staining at any intensity in total tumour cells, as in most of the studies in the literature [11,12]. CFB, Claudin-15, PAI1 and PAK4 immunohistochemical expression were scored for cytoplasmic and/or membranous staining at any intensity in all tumour cells. In the biphasic subtype, IHC evaluation was also performed on the individual components separately.
There are no studies in the literature focused on the CFB and PAK4 immunohistochemical expression in PM, and the evaluation of MSLN, CLDN15 and PAI1 immunohistochemical expression has widely varied by using different scores and thresholds for defining positivity [11-14]. Therefore, in our study, marker positivity was determined on the basis of the proportion of cells stained out of the total number of cells (Tumour Proportion Score – TPS, calculated in increments of 5 %). Staining intensity (weak: 1; intermediate: 2; and strong: 3) was also determined. In order to consider the different intensities and the percentage of staining in our samples, we further evaluated the immunohistochemical results by means of a semiquantitative approach used to assign an H-score to tumour samples, as previously described [11]. H-score was calculated by multiplying the percentage of positive cells by the predominant staining intensity.
2.3. Statistical Analysis
Correlations were assessed by Pearson’s method. Two-group and three-group comparisons were performed by Mann-Whitney’s and Kruskal-Wallis’ followed by Dunn’s tests, respectively. Receiver operating characteristic (ROC) analyses were conducted in two steps following the procedures of the pROC R package v.1.18.0. Firstly, the Area Under the Curve (AUC) was computed by using the training set. The best cut-off was chosen following Youden’s method. Sensitivity, specificity, accuracy, negative predictive value (NPV) and positive predictive value (PPV) were calculated at the best cut-off value. Secondly, the cut-offs were validated on an independent cohort. Confidence intervals (CI) were assessed by 2000 bootstrap resampling. All analyses were performed in R environment (https://www.r-project.org/, v.4.2.2, last accessed April 18, 2023).
3. Results
3.1. Patient characteristics
The median age of the 103 PM patients was 72 years (range, 40–87). There were 83 males and 20 females with a male to female ratio of 4.15:1. For all the epithelioid PMs (42 samples), 26 (61.9%) tumors were low grade and 16 (38.1%) were high grade. The histologic features and the clinical data available are summarized in Table 1. In the biphasic subtype, the percentage of epithelioid component was widely variable with a range of 10% to 90%, median of 40%.
3.2. Different Immunohistochemical Expression among Subtypes
Firstly, the five immunohistochemical markers were evaluated on the training cohort to assess the correlation with the gene expression data on the same samples. Mesothelin, Claudin-15 and CFB were more expressed in epithelioid PMs (Figure 1) than in sarcomatoid and biphasic PMs, and in the latter than in the sarcomatoid PMs.
PAI1 staining was more evident in mesothelioma with SS (p<0.0001) and BS (p<0.0001) than in epithelioid MPs. No significant differences were observed in the PA1 expression between BS and SS, although assessment with TPS showed a trend for higher protein levels in SS (p=0.09, Figure 2).
3.3. Score and Cut-off Selection for Subtype Discrimination: Training Cohort
IHC expression of 4 out of 5 markers (PAI1, Mesothelin, Claudin-15 and CFB) significantly correlated with gene-expression levels. PAK4 mRNA-protein levels were not correlated. For all five markers, TPS and H-score produced similar results, although the former showed a slightly better correlation with mRNA levels. For this reason and to simplify the interpretation of IHC markers, TPS was used for all downstream analyses (Figure S1). ROC analyses were carried out for each marker, in order to assess the performance in discriminating epithelioid compared to non-epithelioid PMs. Mesothelin and Claudin-15 showed the largest AUC values: 0.97 and 0.85, respectively. Lower AUC values were obtained for PAI1, CFB and PAK4, with decreasing values of 0.79, 0.76 and 0.60, respectively.
The best cut-off value was then selected for all immunohistochemical markers. Sensitivity, specificity, accuracy, PPV and NPV were computed. The cut-offs selected for Mesothelin (67.5%) and Claudin-15 (77.5%) were very satisfactory in terms of sensitivity, specificity, and accuracy, showing a good ability to discriminate the subtypes.
The proposed cut-off for CFB (65%) maintained a good accuracy and sensitivity for ES but a lower specificity (0.61) was assessed. Similar results were obtained for PAI1 cut-off (72.5%); indeed, specificity for the non-epithelioid subtype was 0.65.
3.4. Validation Cohort
We then applied the cut-offs selected in the training phase to the validation cohort. The proposed cut-offs for Mesothelin and Claudin-15 maintained a good ability to discriminate the subtypes even in the independent cohort, with an accuracy of 0.83 and 0.80, respectively. For CFB, the proposed cut-off tested in the validation cohort showed an improved accuracy (0.80), with high sensitivity (0.89) and moderate specificity (0.64) in the identification of ES. Unlike the above-mentioned markers, the proposed cut-off for PAK4 (TPS≥62.5%), had a lower performance in discriminating between epithelioid and non-epithelioid PMs, showing an accuracy of 0.67, with a sensitivity of 0.84 and specificity of 0.36. Finally, the expression of PAI1 in the validation cohort was controversial since it was found to be more expressed in epithelioid PMs than in epithelioid BS.
To evaluate the consistency of the cut-offs proposed in the training phase, the optimal cut-offs were also estimated in the validation cohort (Tables 3 and S1).
3.5. Epithelioid PMs: IHC and Histological Features
Association analyses between immunohistochemical expression and tumour grade in the ES showed that PMs with higher mesothelin levels generally had a low grade (p=0.02), absence of necrosis (p=0.01), fewer mitoses (p=0.008), and lower nuclear pleomorphism (p=0,03). Epithelioid PMs with higher expression of PAK4 were frequently high-grade (p =0.03). No significant results were observed between the tumour grade and immunohistochemical expression of Claudin-15 and CFB. Finally, PAI1 expression levels were higher in low-grade neoplasms (p =0.04) and in cases without necrosis (p = 0.02).
3.6. Biphasic PMs: IHC and Discrimination between Components
To further corroborate the findings, we evaluated the IHC expression levels of the five markers in the BS to investigate differences between the two components (i.e., epithelioid and sarcomatoid) when mixed in the same tumour (Figure 3 and S2). For this purpose, we also assessed the IHC expression of the markers in the individual components independently.
First, we correlated the percentage of the epithelioid component with the IHC expression of the markers in the entire tumour (i.e., epithelioid and sarcomatoid component). Staining levels of Mesothelin, CFB and Claudin-15 showed a positive correlation with the proportion of the epithelioid component. The marker assessment for each single component (i.e., either epithelioid or sarcomatoid) showed similar results. In fact, higher expression levels were observed in epithelioid compared to sarcomatoid areas.
PAI1 and PAK4 showed no significant correlation with the percentage of epithelioid component (p=0.49 and p=0.89, respectively). On the other hand, they showed a higher expression level in the sarcomatoid than in the epithelioid (p<0,0001) component.
4. Discussion
Identification of IHC markers in PM has always been a topic of strong interest, especially for the differential diagnosis with benign mimickers and metastatic tumours. Nevertheless, the histological subtype represents a critical prognostic factor for PM diagnosis, and influences the therapeutic approach as much as the tumour stage. According to the National Comprehensive Cancer Network guidelines, only patients with clinical stage I to IIIA, epithelioid histology and good performance status can access surgery [15].
GATA-3, MDM2, HIF1-α and CD10 with potential in subtype distinction have been proposed among the IHC markers; these markers are highly expressed in non-epithelioid subtypes. Conversely, CAIX expression is virtually strong and diffuse in the ES and negative in the sarcomatoid component [16-19].
The use of these markers is limited since few studies have evaluated their expression in PMs, and only a few sarcomatoid and biphasic PMs have been evaluated.
In our study, all the IHC markers tested have displayed a differential expression across the three subtypes, consistent with gene-expression data from the same cohort. Only the expression of PAK4 was controversial and not completely in keeping with our previous gene-expression analysis [10].
Among the IHC markers reported here, Mesothelin is one of the most studied. Consistently with other reports [12,20], it is highly expressed in ES compared to non-epithelioid subtypes. These findings hold true within BS: indeed, Mesothelin is more expressed in the epithelioid than in the sarcomatoid portion, and its expression levels positively correlate with the percentage of the epithelioid component in BS.
Higher Mesothelin levels in ES were also associated with reduced nuclear atypia, as already observed by Sandeck and colleagues [21]. In our ES series, the Mesothelin expression is associated with low mitosis count, absence of necrosis and, therefore, with low-grade. These histologic features, as increased expression of Mesothelin, are associated with better prognosis in patients with epithelioid mesothelioma [1,11,20].
Interest in this marker has grown in recent years owing to anti-Mesothelin targeted therapies. Patients treated with anetumab ravtansine, an anti-Mesothelin antibody conjugated to a maytansine derivative tubulin inhibitor, experienced a better progression-free and overall survival in a preliminary evaluation. Of note, only patients with Mesothelin membrane staining observed in >50% of tumour cells were included in the study [22]. In this work, the rate of positivity for Mesothelin staining is higher than in previous studies, probably due to the use of different scores and antibodies (e.g., 5B2, MN1, MSVA-235)[12,20,23-26]. Only Vizcaya et al. used the same clone (i.e., SP74) and found similar results to ours [11].
Concerning Claudin-15, the epithelioid subtype has a higher expression than non-epithelioid PMs, in agreement with previous research [13]. Among the non-epithelioid PMs, Claudin-15 is more expressed in BS. in contrast to Watanabe et al.. However, the reason is probably due to the small sample size of the study (only 8 biphasic PMs and 6 sarcomatoid PMs). In the biphasic group, the Claudin-15 expression correlates with the percentage of the epithelioid component and it is higher in the epithelioid compared to the sarcomatoid fraction.
Further studies will be needed to confirm the role of Claudin15 in PM subtyping, including its potential prognostic significance. In breast cancer, a low Claudin-15 expression is associated with triple-negative tumours, which are the most aggressive neoplastic group [27]. indeed, some authors suggest that the decreased Claudin expression leads to cellular adhesion loss. This could represent an additional step towards epithelial-to-mesenchymal transition [28] and could explain the low Claudin-15 expression in sarcomatoid mesothelioma.
In this study, the CFB expression was higher in the ES than in the non-epithelioid subtypes. The CFB expression could be useful in subtype distinction, showing a different expression in the two components and a correlation with the percentage of epithelioid portion in the biphasic group.
CFB staining has not been previously evaluated in PM. In lung cancer [29] and in pancreatic adenocarcinoma [30], low CFB expression was associated with poor overall survival and more aggressive disease; consistently, in our cohort, SS showed the lowest CFB expression.
Previous studies have hypothesized that CFB suppression can induce cellular reprogramming (activation of a senescence-associated secretory phenotype), with the acquisition of a more aggressive morphology [31,32].
As regards PAI1, conflicting results between the two cohorts were obtained; however, in the biphasic group the sarcomatoid component has higher in the PAI1 than in the epithelioid expression. In ES, high levels of PAI1 are associated with features of better prognosis, i.e. low grade and absence of necrosis. On the contrary, Sidi et al. [14] showed that high PAI1 expression was associated with poorer survival and progression-free time.
Finally, the PAK4 expression does not accurately discriminate between histological subtypes; despite this, different expression levels were observed between the two components in the BS. Interestingly, epithelioid PMs with increased PAK4 expression were frequently high-grade.
To the best of our knowledge, no other studies have evaluated the PAK4 expression in PM, and contrasting results have been reported in other malignancies. PAK4 overexpression is associated with poor prognosis in gastric tumour, non-small cell lung cancer, oral squamous cell carcinoma, colon cancer and clear cell renal carcinoma [33-37]. On the contrary, lower PAK4 expression was associated with worse prognosis in pancreatic carcinoma and endometrial cancer [20,38].
Some limitations associated with the present study should be mentioned. Firstly, with the exclusion of CLDN15, a cut-off optimization might be necessary. Large differences in optimal cut-off were observed between training and test phases for the other markers, although the subtyping performance of mesothelin was remarkable in both phases.
Secondly, clinical information and follow-up data were not available, thus limiting the prognostic evaluation of these markers.
Despite these limitations, our study has demonstrated that MSLN, CLDN15 and CFB are useful in subtype discrimination, confirming predilection for the epithelioid subtype. Given the high expression in the sarcomatoid component, PAK4 and PAI1 could support the diagnosis of non-epithelioid subtypes, since these components require new immunohistochemical markers for identification.
Further studies should evaluate the usefulness of these markers in subtyping and in the prognostic stratification of PM patients.
Supplementary Materials
The following supporting information can be downloaded at the website of this paper posted on Preprints.org, Figure S1: Correlation between immunohistochemical results and gene expression levels; Figure S2: Immunohistochemical expression in the two components of biphasic subtype and correlation with the percentage of epithelioid component; Table S1: High immunohistochemical expression (> cut-off) among subtypes: Training and Validation cohort.
Author Contributions
Conception of the work and result interpretation: GA, IDS, and GF. Immunohistochemistry and data analysis: AMP and CN. Sample collections and result interpretation: MGM, ML, CCZ, and FM. Pathological diagnosis: GA, IDS, and GF. Writing and review, RB and AP. All authors contributed to the article and approved the submitted version.
Funding
This research received no external funding.
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki and approved by the Ethics Committee “Comitato Etico di Area Vasta Nord Ovest” (CEAVNO) for Clinical Experimentation (protocol code 9989; February 20, 2019).
Informed Consent Statement
Patient consent was waived due to the retrospective nature of the study and since the data were anonymized.
Data Availability Statement
The original contributions presented in the study are included in the article and supplementary files. Further inquiries can be directed to the corresponding author.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Sauter, J.B., R.; Dacic, S.; Gill, RR. . In Thoracic Tumours, 5th ed.; Board, T.W.C.o.T.E., Ed.; International Agency for Research on Cancer (IARC): Lyon, France, 2021; Volume 5, pp. 204–219. [Google Scholar]
- Brims, F. Epidemiology and Clinical Aspects of Malignant Pleural Mesothelioma. Cancers (Basel) 2021, 13. [Google Scholar] [CrossRef] [PubMed]
- Verma, V.; Ahern, C.A.; Berlind, C.G.; Lindsay, W.D.; Shabason, J.; Sharma, S.; Culligan, M.J.; Grover, S.; Friedberg, J.S.; Simone, C.B., 2nd. Survival by Histologic Subtype of Malignant Pleural Mesothelioma and the Impact of Surgical Resection on Overall Survival. Clin Lung Cancer 2018, 19, e901–e912. [Google Scholar] [CrossRef] [PubMed]
- Nelson, D.B.; Rice, D.C.; Niu, J.; Atay, S.; Vaporciyan, A.A.; Antonoff, M.; Hofstetter, W.L.; Walsh, G.L.; Swisher, S.G.; Roth, J.A.; et al. Long-Term Survival Outcomes of Cancer-Directed Surgery for Malignant Pleural Mesothelioma: Propensity Score Matching Analysis. J Clin Oncol 2017, 35, 3354–3362. [Google Scholar] [CrossRef] [PubMed]
- Hung, Y.P.; Chirieac, L.R. Pathology of Malignant Pleural Mesothelioma. Thorac Surg Clin 2020, 30, 367–382. [Google Scholar] [CrossRef] [PubMed]
- Chirieac, L.R.; Hung, Y.P.; Foo, W.C.; Hofer, M.D.; VanderLaan, P.A.; Richards, W.G.; Sugarbaker, D.J.; Bueno, R. Diagnostic value of biopsy sampling in predicting histology in patients with diffuse malignant pleural mesothelioma. Cancer 2019, 125, 4164–4171. [Google Scholar] [CrossRef]
- Klebe, S.; Brownlee, N.A.; Mahar, A.; Burchette, J.L.; Sporn, T.A.; Vollmer, R.T.; Roggli, V.L. Sarcomatoid mesothelioma: a clinical-pathologic correlation of 326 cases. Mod Pathol 2010, 23, 470–479. [Google Scholar] [CrossRef]
- Bueno, R.; Stawiski, E.W.; Goldstein, L.D.; Durinck, S.; De Rienzo, A.; Modrusan, Z.; Gnad, F.; Nguyen, T.T.; Jaiswal, B.S.; Chirieac, L.R.; et al. Comprehensive genomic analysis of malignant pleural mesothelioma identifies recurrent mutations, gene fusions and splicing alterations. Nat Genet 2016, 48, 407–416. [Google Scholar] [CrossRef]
- Alcala, N.; Mangiante, L.; Le-Stang, N.; Gustafson, C.E.; Boyault, S.; Damiola, F.; Alcala, K.; Brevet, M.; Thivolet-Bejui, F.; Blanc-Fournier, C.; et al. Redefining malignant pleural mesothelioma types as a continuum uncovers immune-vascular interactions. EBioMedicine 2019, 48, 191–202. [Google Scholar] [CrossRef]
- Bruno, R.; Poma, A.M.; Ali, G.; Distefano, C.; Proietti, A.; Chella, A.; Lucchi, M.; Melfi, F.; Franco, R.; Fontanini, G. Gene Expression Analysis of Biphasic Pleural Mesothelioma: New Potential Diagnostic and Prognostic Markers. Diagnostics (Basel) 2022, 12. [Google Scholar] [CrossRef]
- Vizcaya, D.; Farahmand, B.; Walter, A.O.; Kneip, C.; Johrens, K.; Tukiainen, M.; Schmitz, A.A. Prognosis of patients with malignant mesothelioma by expression of programmed cell death 1 ligand 1 and mesothelin in a contemporary cohort in Finland. Cancer Treat Res Commun 2020, 25, 100260. [Google Scholar] [CrossRef]
- Inaguma, S.; Wang, Z.; Lasota, J.; Onda, M.; Czapiewski, P.; Langfort, R.; Rys, J.; Szpor, J.; Waloszczyk, P.; Okon, K.; et al. Comprehensive immunohistochemical study of mesothelin (MSLN) using different monoclonal antibodies 5B2 and MN-1 in 1562 tumors with evaluation of its prognostic value in malignant pleural mesothelioma. Oncotarget 2017, 8, 26744–26754. [Google Scholar] [CrossRef] [PubMed]
- Watanabe, M.; Higashi, T.; Ozeki, K.; Higashi, A.Y.; Sugimoto, K.; Mine, H.; Takagi, H.; Ozaki, Y.; Muto, S.; Okabe, N.; et al. CLDN15 is a novel diagnostic marker for malignant pleural mesothelioma. Sci Rep 2021, 11, 12554. [Google Scholar] [CrossRef] [PubMed]
- Sidi, R.; Pasello, G.; Opitz, I.; Soltermann, A.; Tutic, M.; Rehrauer, H.; Weder, W.; Stahel, R.A.; Felley-Bosco, E. Induction of senescence markers after neo-adjuvant chemotherapy of malignant pleural mesothelioma and association with clinical outcome: an exploratory analysis. Eur J Cancer 2011, 47, 326–332. [Google Scholar] [CrossRef]
- Ettinger, D.S.; Wood, D.E.; Akerley, W.; Bazhenova, L.A.; Borghaei, H.; Camidge, D.R.; Cheney, R.T.; Chirieac, L.R.; D'Amico, T.A.; Dilling, T.; et al. NCCN Guidelines Insights: Malignant Pleural Mesothelioma, Version 3.2016. J Natl Compr Canc Netw 2016, 14, 825–836. [Google Scholar] [CrossRef] [PubMed]
- Capkova, L.; Koubkova, L.; Kodet, R. Expression of carbonic anhydrase IX (CAIX) in malignant mesothelioma. An immunohistochemical and immunocytochemical study. Neoplasma 2014, 61, 161–169. [Google Scholar] [CrossRef]
- Prabhakaran, S.; Hocking, A.; Kim, C.; Hussey, M.; Klebe, S. The potential utility of GATA binding protein 3 for diagnosis of malignant pleural mesotheliomas. Hum Pathol 2020, 105, 1–8. [Google Scholar] [CrossRef]
- Kadota, K.; Villena-Vargas, J.; Nitadori, J.; Sima, C.S.; Jones, D.R.; Travis, W.D.; Adusumilli, P.S. Tumoral CD10 expression correlates with aggressive histology and prognosis in patients with malignant pleural mesothelioma. Ann Surg Oncol 2015, 22, 3136–3143. [Google Scholar] [CrossRef]
- Pasello, G.; Urso, L.; Mencoboni, M.; Grosso, F.; Ceresoli, G.L.; Lunardi, F.; Vuljan, S.E.; Bertorelle, R.; Sacchetto, V.; Ciminale, V.; et al. MDM2 and HIF1alpha expression levels in different histologic subtypes of malignant pleural mesothelioma: correlation with pathological and clinical data. Oncotarget 2015, 6, 42053–42066. [Google Scholar] [CrossRef]
- Chu, G.J.; Linton, A.; Kao, S.; Klebe, S.; Adelstein, S.; Yeo, D.; Rasko, J.E.J.; Cooper, W.A. High mesothelin expression by immunohistochemistry predicts improved survival in pleural mesothelioma. Histopathology 2023, 83, 202–210. [Google Scholar] [CrossRef]
- Sandeck, H.P.; Roe, O.D.; Kjaerheim, K.; Willen, H.; Larsson, E. Re-evaluation of histological diagnoses of malignant mesothelioma by immunohistochemistry. Diagn Pathol 2010, 5, 47. [Google Scholar] [CrossRef]
- Kindler, H.L.; Novello, S.; Bearz, A.; Ceresoli, G.L.; Aerts, J.; Spicer, J.; Taylor, P.; Nackaerts, K.; Greystoke, A.; Jennens, R.; et al. Anetumab ravtansine versus vinorelbine in patients with relapsed, mesothelin-positive malignant pleural mesothelioma (ARCS-M): a randomised, open-label phase 2 trial. Lancet Oncol 2022, 23, 540–552. [Google Scholar] [CrossRef] [PubMed]
- Ordonez, N.G. Mesothelioma with signet-ring cell features: report of 23 cases. Mod Pathol 2013, 26, 370–384. [Google Scholar] [CrossRef] [PubMed]
- Hager, T.; Borchert, S.; Wessolly, M.; Mathilakathu, A.; Mairinger, E.; Kollmeier, J.; Mairinger, T.; Hegedus, B.; Greimelmaier, K.; Wohlschlaeger, J.; et al. One Third of Malignant Pleural Mesothelioma Shows High Immunohistochemical Expression of MSLN or CXCR4 Which Indicates Potent Candidates for Endo-Radiotherapy. Int J Mol Sci 2023, 24. [Google Scholar] [CrossRef]
- Weidemann, S.; Gagelmann, P.; Gorbokon, N.; Lennartz, M.; Menz, A.; Luebke, A.M.; Kluth, M.; Hube-Magg, C.; Blessin, N.C.; Fraune, C.; et al. Mesothelin Expression in Human Tumors: A Tissue Microarray Study on 12,679 Tumors. Biomedicines 2021, 9. [Google Scholar] [CrossRef] [PubMed]
- Tan, K.; Kajino, K.; Momose, S.; Masaoka, A.; Sasahara, K.; Shiomi, K.; Izumi, H.; Abe, M.; Ohtsuji, N.; Wang, T.; et al. Mesothelin (MSLN) promoter is hypomethylated in malignant mesothelioma, but its expression is not associated with methylation status of the promoter. Hum Pathol 2010, 41, 1330–1338. [Google Scholar] [CrossRef]
- Zhang, D.; Sun, B.; Zhao, X.; Sun, H.; An, J.; Lin, X.; Zhu, D.; Zhao, X.; Wang, X.; Liu, F.; et al. Twist1 accelerates tumour vasculogenic mimicry by inhibiting Claudin15 expression in triple-negative breast cancer. J Cell Mol Med 2020, 24, 7163–7174. [Google Scholar] [CrossRef]
- Tabaries, S.; Annis, M.G.; Hsu, B.E.; Tam, C.E.; Savage, P.; Park, M.; Siegel, P.M. Lyn modulates Claudin-2 expression and is a therapeutic target for breast cancer liver metastasis. Oncotarget 2015, 6, 9476–9487. [Google Scholar] [CrossRef]
- He, C.; Li, Y.; Zhang, R.; Chen, J.; Feng, X.; Duan, Y. Low CFB expression is independently associated with poor overall and disease-free survival in patients with lung adenocarcinoma. Oncol Lett 2021, 21, 478. [Google Scholar] [CrossRef]
- Shimazaki, R.; Takano, S.; Satoh, M.; Takada, M.; Miyahara, Y.; Sasaki, K.; Yoshitomi, H.; Kagawa, S.; Furukawa, K.; Takayashiki, T.; et al. Complement factor B regulates cellular senescence and is associated with poor prognosis in pancreatic cancer. Cell Oncol (Dordr) 2021, 44, 937–950. [Google Scholar] [CrossRef]
- Milanovic, M.; Fan, D.N.Y.; Belenki, D.; Dabritz, J.H.M.; Zhao, Z.; Yu, Y.; Dorr, J.R.; Dimitrova, L.; Lenze, D.; Monteiro Barbosa, I.A.; et al. Senescence-associated reprogramming promotes cancer stemness. Nature 2018, 553, 96–100. [Google Scholar] [CrossRef]
- Dou, Z.; Berger, S.L. Senescence Elicits Stemness: A Surprising Mechanism for Cancer Relapse. Cell Metab 2018, 27, 710–711. [Google Scholar] [CrossRef] [PubMed]
- Li, D.; Zhang, Y.; Li, Z.; Wang, X.; Qu, X.; Liu, Y. Activated Pak4 expression correlates with poor prognosis in human gastric cancer patients. Tumour Biol 2015, 36, 9431–9436. [Google Scholar] [CrossRef] [PubMed]
- Cai, S.; Ye, Z.; Wang, X.; Pan, Y.; Weng, Y.; Lao, S.; Wei, H.; Li, L. Overexpression of P21-activated kinase 4 is associated with poor prognosis in non-small cell lung cancer and promotes migration and invasion. J Exp Clin Cancer Res 2015, 34, 48. [Google Scholar] [CrossRef] [PubMed]
- Begum, A.; Imoto, I.; Kozaki, K.; Tsuda, H.; Suzuki, E.; Amagasa, T.; Inazawa, J. Identification of PAK4 as a putative target gene for amplification within 19q13.12-q13.2 in oral squamous-cell carcinoma. Cancer Sci 2009, 100, 1908–1916. [Google Scholar] [CrossRef] [PubMed]
- Liu, W.; Yang, Y.; Liu, Y.; Liu, H.; Zhang, W.; Xu, L.; Zhu, Y.; Xu, J. p21-Activated kinase 4 predicts early recurrence and poor survival in patients with nonmetastatic clear cell renal cell carcinoma. Urol Oncol 2015, 33, 205 e213-221. [Google Scholar] [CrossRef]
- Song, B.; Wang, W.; Zheng, Y.; Yang, J.; Xu, Z. P21-activated kinase 1 and 4 were associated with colorectal cancer metastasis and infiltration. J Surg Res 2015, 196, 130–135. [Google Scholar] [CrossRef]
- Park, S.; Kim, J.W.; Kim, H.; Kim, J.W.; Kim, Y.J.; Lee, K.W.; Kim, J.H.; Kim, J.H.; Hwang, J.H.; Choi, Y.R.; et al. Prognostic value of p21-activated kinase 4 in resected pancreatic cancer. APMIS 2017, 125, 699–707. [Google Scholar] [CrossRef]
Figure 1.
(A) A case of epithelioid mesothelioma (hematoxylin and eosin stain); (B) diffuse and strong membranous expression for Mesothelin; (C) Claudin-15 showing diffuse cytoplasmatic expression; (D) diffuse cytoplasmatic expression for CFB (magnification × 100).
Figure 1.
(A) A case of epithelioid mesothelioma (hematoxylin and eosin stain); (B) diffuse and strong membranous expression for Mesothelin; (C) Claudin-15 showing diffuse cytoplasmatic expression; (D) diffuse cytoplasmatic expression for CFB (magnification × 100).
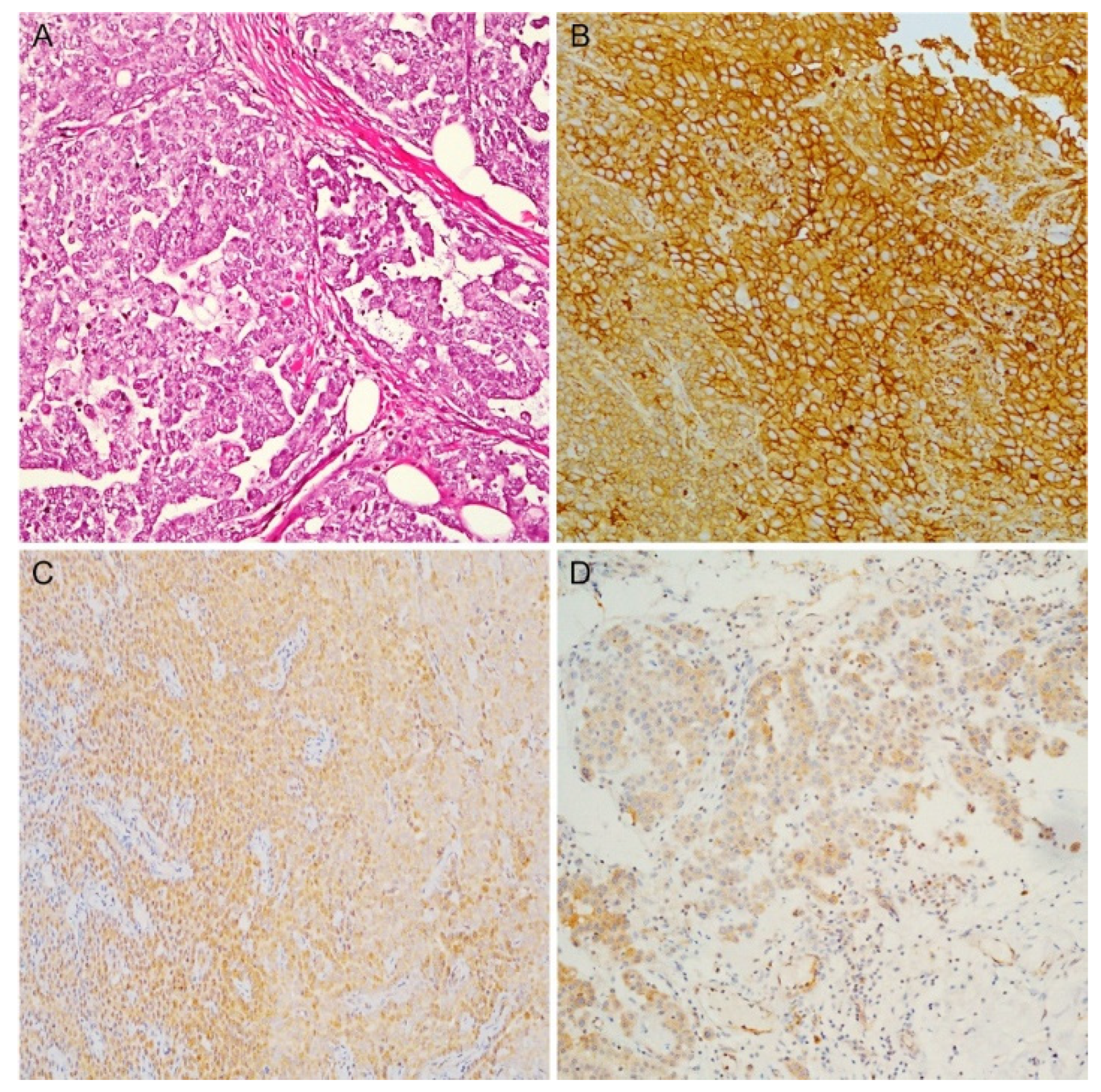
Figure 2.
A case of sarcomatoid mesothelioma (A) with malignant spindle cell growth (hematoxylin and eosin stain); (B) PAI1 and (C) PAK4 diffuse expression (magnification ×100).
Figure 2.
A case of sarcomatoid mesothelioma (A) with malignant spindle cell growth (hematoxylin and eosin stain); (B) PAI1 and (C) PAK4 diffuse expression (magnification ×100).
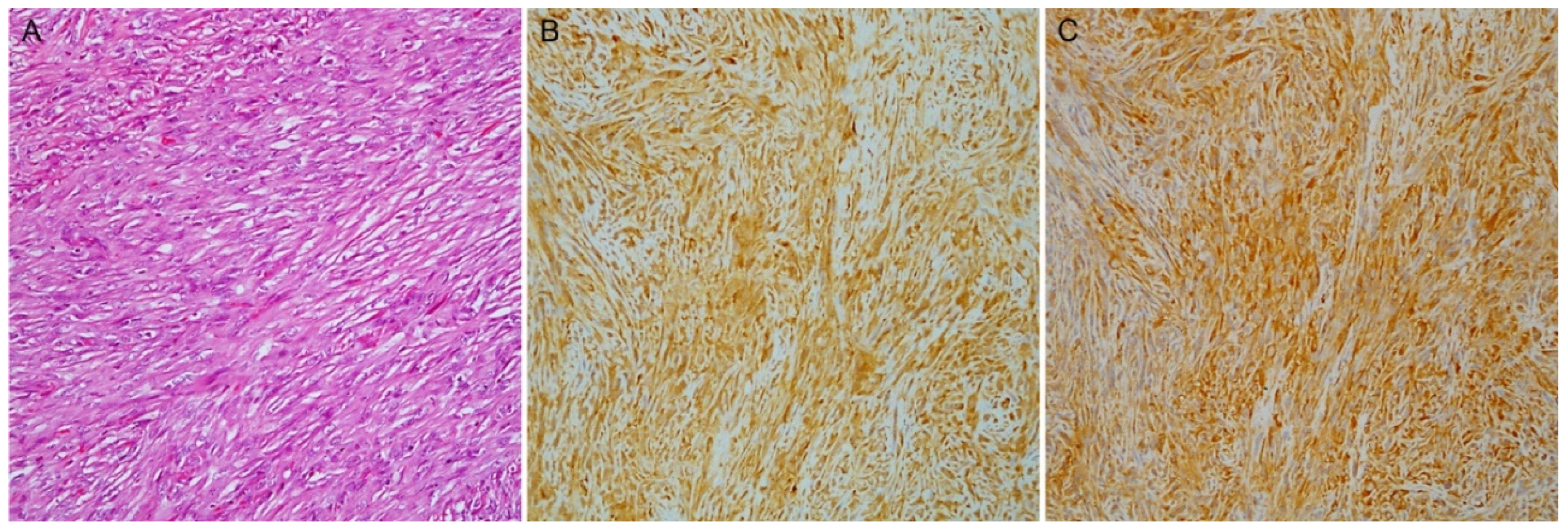
Figure 3.
A case of biphasic mesothelioma. (A) Haematoxylin and eosin stain with the epithelioid (left) and the sarcomatoid component (right); (B) Mesothelin, (C) Claudin-15 and (D) CFB higher expression in epithelioid component; (E) PAI1 and (F) PAK4 higher expression in sarcomatoid component (magnification × 100).
Figure 3.
A case of biphasic mesothelioma. (A) Haematoxylin and eosin stain with the epithelioid (left) and the sarcomatoid component (right); (B) Mesothelin, (C) Claudin-15 and (D) CFB higher expression in epithelioid component; (E) PAI1 and (F) PAK4 higher expression in sarcomatoid component (magnification × 100).
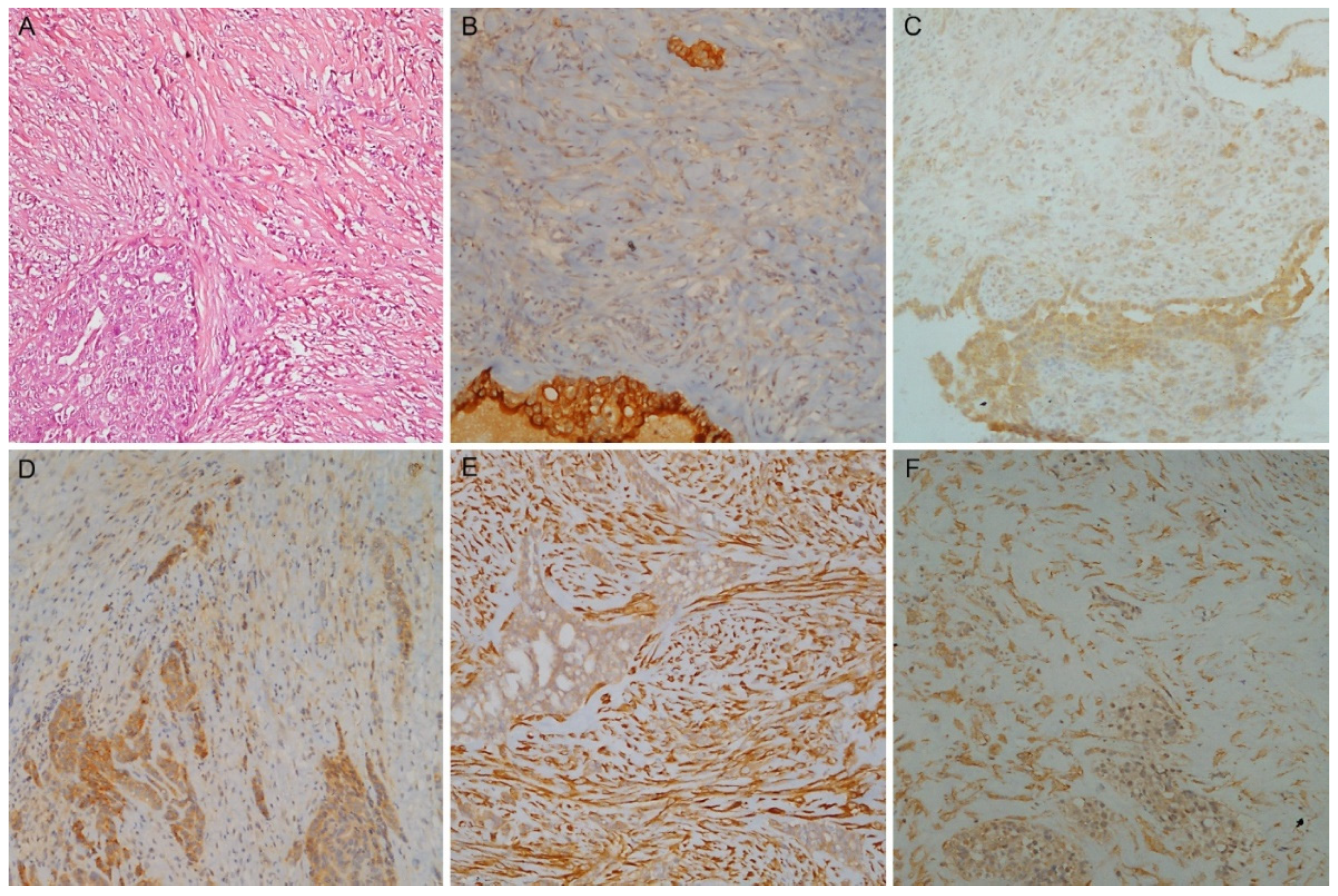

Table 1.
Clinicopathological characteristics of patients with pleural mesothelioma.
| Characteristics | Training Cohort (n=73) | Validation Cohort (n=30) |
| Age, years, median (range) | 71 (40-85) | 75 (54-87) |
| Sex, male, n (%) | 58 (79.5) | 25 (83.3) |
| Mesothelioma Subtype | ||
| Epithelioid, n (%) | 31 (42.5) | 11 (36.7) |
| Biphasic, n (%) | 25 (34.2) | 11 (36.7) |
| Sarcomatoid, n (%) | 17 (23.3) | 8 (26.6) |
| Epithelioid subtype (n=42) | Training Cohort (n=31) | Validation Cohort (n=11) |
| High grade, n (%) | 12 (38.7) | 3 (27.3) |
| Mitosis number score | ||
| 1 (≤ 1 mitosis/2 mm2) | 11 (35.5) | 5 (45.4) |
| 2 (2–4 mitoses/2 mm2) | 15 (48.4) | 3 (27.3) |
| 3 (≥ 5 mitoses/2 mm2) | 5 (16.1) | 3 (27.3) |
| Nuclear atypia score | ||
| 1 | 8 (25.8) | 3 (27.3) |
| 2 | 17 (54.8) | 5 (45.4) |
| 3 | 6 (19.4) | 3 (27.3) |
| Necrosis presence | 13 (41.9) | 4 (36.4) |
Table 2.
Immunohistochemical expression among subtypes (training cohort=73).
| Scores |
CFB Median (IQR) |
Mesothelin Median (IQR) |
Claudin-15 Median (IQR) |
PAI1 Median (IQR) |
PAK4 Median (IQR) |
|
| ES | TPS H-score |
70 (55-90) 120 (55-180) |
92.5 (81.25-95) 270 (190-285) |
85 (70-95) 190 (130-210) |
60 (50-80) 120 (82.5-170) |
70 (52.5-82.5) 120 (85-160) |
| BS | TPS H-score |
60 (30-70) 80 (40-120) |
50 (30-70) 117.5 (60-187.5) |
70 (60-75) 150 (130-195) |
85 (80-90) 210 (160-270) |
80 (70-90) 210 (180-240) |
| SS | TPS H-score |
10 (5-20) 10 (5-20) |
0 (0-10) 0 (0-15) |
35 (30-60) 60 (35-80) |
90 (80-95) 210 (190-255) |
70 (65-90) 160 (110-195) |
|
ES vs BS p-value |
TPS H-score |
0.04 0.05 |
<0.0001 <0.0001 |
0.0006 0.17 |
0.001 <0.0001 |
0.05 <0.0001 |
|
ES vs SS p-value |
TPS H-score |
<0.0001 <0.0001 |
<0.0001 <0.0001 |
<0.0001 <0.0001 |
<0.0001 <0.0001 |
0.23 0.04 |
|
BS vs SS p-value |
TPS H-score |
0.0003 0.0001 |
0.0001 <0.0001 |
0.004 <0.0001 |
0.09 0.23 |
0.25 0.03 |
CFB: Complement factor B; PAI1: Plasminogen activator inhibitor 1, PAK4: p21-activated kinase 4; ES: epithelioid subtype; BS: biphasic subtype; SS: sarcomatoid subtype; IQR: interquartile range; TPS: Tumour Proportion Score.
Table 3.
Cut-off selection and performance among subtypes: Training and Validation cohort.
| Training cohort | |||||
| Mesothelin | Claudin-15 | CFB | PAI1 | PAK4 | |
| Cut-off | 67.5 % | 77.5 % | 65 % | 72.5 % | 62.5 % |
| AUC | 0.97 (0.93-0.99) | 0.85 (0.75-0.93) | 0.76 (0.64-0.87) | 0.79 (0.67-0.89) | 0.60 (0.47-0.73) |
| Sensitivity | 0.88 (0.76-0.98) | 0.88 (0.57-1) | 0.86 (0.55-1) | 0.88 (0.62-0.98) | 0.86 (0.43-0.98) |
| Specificity | 1 (0.94-1) | 0.71 (0.51-0.94) | 0.61 (0.32-0.90) | 0.65 (0.42-0.84) | 0.42 (0.23-0.81) |
| Accuracy | 0.93 (0.86-0.97) | 0.81 (0.70-0.89) | 0.75 (0.66-0.82) | 0.77 (0.67-0.85) | 0.67 (0.58-0.77) |
| NPV | 0.86 (0.76-0.97) | 0.83 (0.61-1) | 0.76 (0.57-1) | 0.79 (0.60-0.95) | 0.70 (0.50-0.89) |
| PPV | 1 (0.95-1) | 0.80 (0.72-0.94) | 0.76 (0.67-0.90) | 0.76 (0.68-0.87) | 0.67 (0.61-0.77) |
| Validation cohort | |||||
| Mesothelin | Claudin-15 | CFB | PAI1 | PAK4 | |
| AUC* | 0.98 (0.92-1) | 0.84 (0.66-0.97) | 0.80 (0.59-0.97) | NA | 0.75 (0.57-0.90) |
| Sensitivity* | 0.79 (0.58-0.95) | 0.84 (0.68-1) | 0.89 (0.74-1) | NA | 0.84 (0.68-1) |
| Specificity* | 0.91 (0.73-1) | 0.73 (0.45-1) | 0.64 (0.36-0.91) | NA | 0.36 (0.09-0.64) |
| Accuracy* | 0.83 (0.70-0.93) | 0.80 (0.63-0.93) | 0.80 (0.67-0.93) | NA | 0.67 (0.53-0.80) |
| NPV* | 0.71 (0.56-0.92) | 0.73 (0.50-1) | 0.78 (0.55-1) | NA | 0.57 (0.25-1) |
| PPV* | 0.94 (0.81-1) | 0.84 (0.71-1) | 0.81 (0.70-0.95) | NA | 0.70 (0.60-0.81) |
| Best cut-off on Validation cohort | |||||
| 87.5% | 75% | 47.5% | 65% | 77.5% | |
AUC: Area Under the Curve; NPV: Negative Predictive Value; PPV: Positive Predictive Value; CFB: Complement factor B; PAI1: Plasminogen activator inhibitor 1, PAK4: p21-activated kinase 4. NA: Not Available because of inconsistent expression levels with the training cohort. *Calculation based on the Training cohort.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



