Submitted:
24 July 2023
Posted:
09 August 2023
Read the latest preprint version here
Abstract
Overhydration (OH) is a common medical problem found in patients with kidney or heart failure, but still a specific marker has not been found. Clinicians today use bioimpedance spectroscopy (BIS), ultrasound (US) markers of fluid overload or markers of heart and kidney function like NT-pro-BNP, GFR or creatinine levels. New serum markers such as Ca-125, Galectin-3 (Gal-3), Adrenomedullin (AMD) and Urocortin-2 (UCN-2), are being researched with promising results. The need to discover a more precise marker of overhydration is dire mainly because physical examination is extremely imprecise. Signs and symptoms of fluid overload like edema or gradual increase of body mass are not always present, especially in patients with chronic kidney disease. This review paper summarizes actual knowledge of a patient's hydration status estimation focusing especially on kidney diseases.
Keywords:
Fluid status 1
; overhydration 2
; hydration status 3
; renal failure 4
; kidney failure 5
; heart failure 6
; Ca-125 7
; NT-pro-BNP 8
; VEXUS 9
; BIS 10
1. Introduction
Fluid state assessment is one of the most important measurements which doctors perform in patients with kidney disease. Total body water (TBW) consists approximately 50% to 60% of an adult's total body weight and it is over 73% of a lean body mass [1]. The hydration status varies depending on muscle mass, fat body mass, electrolyte balance or physiological states like pregnancy. Naturally the percentage of TBW decreases with age due to decrease in muscle mass and metabolism. Fluid overload is a known risk factor of hypertension, heart failure (HF) and increased mortality in patients with kidney failure [1,2,3]. A study performed by Zoccali et. all showed that overhydrated patients with end stage kidney disease (ESKD) have a 62% higher risk of mortality than non-overhydrated ones [2]. In a paper by Hung et al. we can find information that among a research group of 338 patients with chronic kidney disease (CKD) only 48% were euvolemic [4]. Zoccali, Hung et. all were not the only researchers who noticed and described the dependency between normohydration and long term survival in patients with kidney diseases [2,3,4,5,6,7,8,9,10,11,12,13,14,15,16,17,18,19,20]. Taking this into consideration, it is an enormous challenge for modern physicians to precisely assess and treat the patients overhydration (OH), because it can lead to irreparable damages in the organism and consequently to death [14,18]. Clinical symptoms of OH may include distal and proximal swelling, dyspnoea, hypertension, jugular venous pressure assessment. In physical examination which includes auscultation, palpation, percussion doctors can also hear crackles in the lungs, particularly in the lower parts. Additionally, the hepato-jugular reflux can be noticed when the pressure applied to the liver causes a sustained rise in jugular blood pressure which can be observed as an under-skin pulsation. The symptoms can be present not only in OH caused by kidney failure, but also in heart or liver diseases, infections and cancerogenesis. A presence or absence of clinical symptoms does not exclude OH due to kidney diseases. One of the first signs of OH is presence of pitting pedal oedema, but this symptom can be also caused by stasis or excess vascular permeability [9]. A cross-sectional study of hemodialysis patients showed that it correlates with body mass index but does not reflect volume status [9]}. Individuals who suffer from CKD may also develop HF, hepatic failure or else pneumonia which additionally influences volume status. This makes a physical examination very hard to interpret as visible symptoms can be caused by other factors than fluid status. Patients’ diagnosis should be confirmed by using other available clinical tests like estimation of the dry body weight (dry-weight is defined as the lowest tolerated postdialysis weight achieved via gradual change in postdialysis weight at which there are minimal signs or symptoms of hypovolemia or hypervolemia [81], blood or urine tests which can suggest the kidney malfunction or radiological examination. Doctors should have a holistic approach to OH problem and combine all available methods to establish the patient's hydration status and manage between methods depending on the individual's needs [18]. In present-day medicine we can estimate the dry body weight assessing blood pressure, signs and symptoms of OH, blood volume monitoring and bedside ultrasound [21]. The gold standard of testing body composition and body water distribution is called bioimpedance spectroscopy (BIS). It allows measuring intracellular and extracellular water so it can help to establish the exact cell mass [23]. This method is non-invasive as it requires only placement of electrodes on patients’ body which allows to measure tissue conductivity, hence the water balance [23]. BIS seems to be a gold standard in theory, but practically not all clinics or dialysis stations have got the necessary equipment. This adequate and modern tool is quite expensive and is sometimes unaffordable for a public health facility. It has also limited clinical application in certain conditions. This method cannot estimate the accurate water cell ratio in pregnant women where there are multiple volume changes in time. Its usefulness in patients after limb amputations or with implanted electronical devices like a pacemaker is also diminished. Additionally, in patients who undergo dialysis results were different among researchers and between devices which were used [23]. This method works well on healthy individuals, but in clinical populations the results vary [18,23]. Nephrologists also use laboratory markers which help to establish the hydration state like NT-pro-BNP or BNP. The main difference between two markers is that BNP is a biologically active marker whereas NT-pro-BNP is not. The inactive pro peptide is more stable in the bloodstream and it strongly correlates with heart failure, cardiovascular congestion and death [21]. Adrenomedullin and its derivative pro-adrenomedullin (MR-pro-AMD) , which are markers of endothelial injury, are under active research mainly in populations with HF, sepsis, or kidney failure. Both tend to correlate with a clinical state and available indirect markers of OH like NT-pro-BNP. Gal-3 seems to correspond more to the kidney failure and mortality rate than OH itself, but it shows a precise correlation during the clinical and pre-clinical studies as an organ failure indicator. Ucn-2 is a protein sensitive to vasodilatation due to an increase in fluid volume, but it gives mixed results when considered as a strict OH marker. The new and promising marker is also Ca-125, which is nowadays widely investigated by cardiologists in patients with heart failure. This marker tends to increase together with OH status but needs to be further investigated.
Volume status can also be assessed with imaging methods. POCUS (point-of care ultrasonography) allows to observe the signs of OH like presence of fluid in pleura or peritoneum, higher diameter of jugular vein, IVC (inferior vena cava), abnormal flow through hepatic vein, portal vein or renal vein and estimation of the pressure inside these structures [24]. A special protocol called Venous Access Ultrasound Score (VEXUS) was also developed and validated.
A holistic approach in hydration estimation of the hydration status in CKD patients is illustrated in the Figure 1.
The main aim of this review is to determine whether modern medicine is in need of the new overhydration marker. During the brief research in both literature and clinical work we assume that there is a lack of a precise hydration status marker, but it is very desirable to improve the available methods of treatment.
2. Results
This section may be divided by subheadings. It should provide a concise and precise description of the experimental results, their interpretation, as well as the experimental conclusions that can be drawn.
Out of 1480 identified in PubMed records, 991 were screened, 39 retrieved and assessed for eligibility and 36 finally included in the review (27 original studies and 8 reviews/commentaries). The entire selection process is illustrated in Figure 2. The basic characteristics of the original articles on the researched subject are summarised in Table 1; Table 2. We have identified 1 experimental study.
As we can notice from Table 1 none of the investigated OH markers include water balance and kidney function. Nowadays, the best method of assessment is to combine those methods together with the patient's examination. It is important to develop, investigate and combine all available methods and their correlations. In Table 2 there is a list of research papers which combine some methods together mentioned in this paper and their correlation with OH.
3. Discussion
3.1. Available markers
As mentioned in Table 1 modern medicine can estimate volume status using various following methods.
3.2. Gold standard: Bioimpedance spectroscopy (BIS)
Bioimpedance spectroscopy is a useful non-invasive tool which allows distinguishing between ECW (external cell water) and ICW (internal cell water). It requires only placement of electrodes on a distal part of the body (ankle-wrist) to measure water conduction inside the body [23]. The difference between both values measured by Body Composition Monitor (BCM) can be defined either as normo- or overhydration [4]. ECW is measured on very low frequencies as there is almost no conduction, while on contrary TBW is estimated on high frequencies, when total conduction on cell membranes occurs [23]. The conducted electricity is not harmful to the patient and has no influence on further diagnosis or daily life. This is a contemporary gold standard to estimate the water balance in patients' bodies, however it is not without limitations as not all clinical states are well calculated by the device and therefore hard to interpret [18,23]. For instance BIS gives mixed results for pregnant women, patients post-CABG procedure, with gastrointestinal diseases, kidney disorders, after limb amputations or in obese individuals [23]. Clinical cases cited above are characterized by alterations in body water distribution, particularly in CKD patients fluid status can be also affected by changes in haematocrit, and other clinical parameters [22,23]. Additionally, the assumption that the fat-free mass (FFM) is estimated to 73.2% does not apply for overweight patients as they exhibit expanded ECW:TBW ratio even after the weight loss [23]. Another BIS limitation is the establishment that the body shape is cylindrical with uniform cross- sectional areas and this homogenous composition is again different in overweight people [23]. This tool is also quite expensive and not all health facilities can afford to buy this.
Even so, plenty of clinical studies have been performed with a usage of BIS and gave an encouraging result for patients not only with CKD. A study among COVID-19 patients showed that higher OH estimation by BIS correlates with intensive care unit (ICU) hospitalizations mortality [32]. In terms of kidney failure, the equipment can be used for people receiving haemodialysis, peritoneal dialysis or who are not under renal replacement therapy. Vega’s et al. original paper showed that there is an association between OH status calculated by BIS and higher mortality in patients with CKD stages 4-5 not yet undergoing kidney replacement therapy. Kaplan-Mayer analysis confirmed higher mortality in patients with an excess fluid overload [12]. Study performed by Hung et al. in 2013 focused on the dependency between calculated OH and known risk factor of cardiac incidents in patients with CKD. This research showed that results obtained by BCM contributed to other risk factors of cardiac incidents like male sex, diabetes mellitus, high systolic blood pressure, previous cardiac incident and proteinuria [4]. There is however a serious limitation of this paper as there is no data presented on patients diet as well as fluid intake [4]. Another research paper which included patients on hemodialysis (HD) showed that OH calculated by BIS is an independent predictor of death in dialysis population [20]. Unfortunately, patients with metallic joint prostheses, cardiac pacemakers, decompensated cirrhosis, and limb amputations were excluded from the test due to BIS technique limitation. In a study performed on peritoneal dialysis (PD) patients, BIS water balance calculations correlated with the urine protein loss and higher creatinine, independently from the duration of dialysis therapy [28]. A different study which included 711 patients on peritoneal dialysis found that volume of OH calculated by BCM and peritoneal protein clearance were independent predictors of all-cause mortality. The correlation between both variables can be explained by the contribution of protein loss due to hypoalbuminemia and fluid accumulation [13]. BIS hydration status calculations can correlate with other OH tests available in hospital conditions. Study among 138 patients from Spain revealed a positive correlation between OH status achieved by BIS and albuminuria, creatinine increase or dyslipidemia [10]. It turned out that OH patients had approximately a 4-times higher probability of death and that increase in urine volume lowered it significantly [10]. In a metanalysis by Wang et al. among almost 105 000 patients who underwent dialysis, one third of them had fluid overload detected by BIS [3]. The estimated risk factor for mortality and cardiovascular event was ECW/TBW >0.4 [3]. In a research study of not dialysis-dependent 179 patients with CKD of all stages OH measured by BCM correlated with urinary protease activity and progression of renal dysfunction as well as with an increase of NT-pro-BNP and systolic blood pressure [25]. The correlation was also true for other markers of renal malfunction like increase in creatinine, albuminuria and drop of eGFR [25]. Optimisation of fluid status based on the BIS calculations allows to reduce the fluid overload and leads to better control of hypertension according to Macheck et. al clinical study [33]. BCM (body composition monitor) results obtained before and after a HD were correlated with a clinical indicator of OH like blood pressure and presence of abscesses. Unfortunately, again patients with pacemakers and large metallic implants were again excluded from the study due to metal interactions with BCM.
Progression towards ESKD correlates with a higher OH status. This interaction was observed by Hung et al. in an almost three yearlong study of patients with CKD stages 3-5. OH appeared to be a more important mortality risk factor than hypertension [17]. Rat model created to stimulate water retention in CKD proved that fluid retention stimulated hypertension, albuminuria, expression of inflammation markers and atherosclerosis [17]. Some symptoms were attenuated after treatment with indapamide which suggest that OH has a significant role in pathophysiological processes mentioned above. The similar connection between OH calculated by BIS was noticed by Kim et al. on a group of 147 HD patients [34]. OH correlated negatively with creatinine, serum albumin, white blood cells count, platelets, uric acid, potassium, phosphorus or triglycerides [34]. Rate of OH change per 1 kg before and after the HD was higher for ECW than ICW. After dialysis there was a noticeable drop in parameters like estimated protein mass, mineral mass, and soft lean mass whereas body fat increased. Segmental BIA analysis calculated that water loss was greater in legs than in arms, it can be caused by verticalization and consequently movement of the fluids according to the force of gravity. The important limitation of this study was the usage of different device for HD group and control, as well as BIS for research group was measured in supine position and control group in upright one. BIS also neither improved life expectancy nor helped in maintaining dry body weight in Siriopol et al. study on HD patients [16]. In Covic et al. systematic review and metaanalysis on 1312 patients with CKD, BIS-based dialysis therapy did not reduce the all-time mortality rate. Along with this observation BIS had no influence on body change, but improved the systolic blood pressure [35]. In Park et. al study of dialysis patients, BIS did not detect the difference between hydration status between CKD population and a control group of healthy individuals even though the other indicators of OH increased [36].
3.3. Serum markers
3.3.1. NT-pro-BNP
N-terminal pro-brain natriuretic peptide (NT-pro-BNP) is a peptide hormone mainly synthesized by ventricular cardiomyocytes in response to stretch e.g. during the increased cardiac filling pressure and cleared by kidneys [37,38]. Elevated serum level of NT-pro-BNP is observed in HF and during cardiac ischemia, pulmonary embolism, cor pulmonale, hypertension, hyperthyroidism, Cushing syndrome, hyperaldosteronism, cirrhosis, subarachnoid haemorrhage, and kidney failure. This marker also varies among sex groups, age and has lower values in obese individuals. Its blood concentration can be affected by medications like corticosteroids, diuretics, ACE inhibitors or thyroid hormones. It has been shown that monitoring NT-pro-BNP changes over time is a powerful diagnostic indicator as life expectancy seems to be prolonged when its concentration decreases [38]. In terms of kidney function in patients with HF, NT-pro-BNP also increases and remains significantly higher in patients with accompanying CKD [38]. HF in patients with CKD is a dangerous clinical issue with poor treatment results. It is not only due to the volume overload but also development of anaemia. All listed pathologies cause an increase in both left ventricular end-diastolic volume and mass which eventually leads to HF [39]. The African American Study of Kidney Disease and Hypertension enrolled patients with CKD to find an association between the risk of cardiovascular incidence and NT-pro-BNP levels in the population. It turned out that individuals with an increased plasma level of NT-pro-BNP were more likely to have cardiovascular complications and this risk was particularly seen in patients who suffered from albuminuria [40]. Elevated NT-pro-BNP levels indicate an increased risk of cardiovascular event in HD population with no other signs of HF according to a study by Goto et al. This marker was an independent risk factor, as it showed no correlation with age, body mass index, blood pressure and heart rate [41]. Therefore NT-pro-BNP, mainly used in cardiology drew the attention of nephrologists. A large clinical study performed on older Chinese patients (above 60 years of age) with concomitant coronary artery disease and with or without CKD revealed that decrease in GFR independently affected NT-pro-BNP. It predicted death with a cut-off value of 369.5 pg/mL in patients with preserved kidney function and a cut-off value of 2584.1 pg/mL in CKD ones [42]. Its clinical application was also found by nephrologists in patients with CKD as it tends to correlate with other OH indicators. Schaub et al. in a metanalysis which included 4287 patients posed a question whether NT-pro-BNP has different diagnostic and prognostic utility in patients with kidney dysfunction. The correlation between GFR and natriuretic peptide were found to be statistically significant and ranged from −0.21 to −0.58 which means that during the decline in renal function, NT-pro-BNP level increases [43]. Elevated serum level of the peptide in patients with kidney dysfunction compared to patients with normal NT-pro-BNP confers an increased risk of mortality when compared to healthy controls [43]. Increase in serum level in patients with kidney disease can be due to decrease in the blood clearance ability, but it still correlates with higher mortality among patients. NT-pro-BNP seemed to predict mortality better in patients with CKD than in non-CKD patients. eGFR and NT-pro-BNP independent relation was noticed also in a study on 599 dyspnoeic patients with renal malfunction. Elevated NT-pro-BNP was the strongest risk factor of 60-days mortality and was acclaimed as a marker of chronic heart failure (CHF) independently from kidney function in dyspnoeic patients [44]. Similar results were obtained by DeFilippi et al. investigation and one-year mortality rates were 36.3% in patients with CKD and 19.0% without CKD, respectively [45]. NT-pro-BNP showed a similar result in dialysis and patients in a study by Park et al. Its level was significantly higher in patients with any type of dialysis treatment, when compared to control group. NT-pro-BNP also correlated with AMD, even though BMC did not detect any differences in OH status between control and treatment group [36]. NT-pro -BNP tends to grow in individuals with fluid excess during clinical studies on various methods of estimating hydration status [17,18,25,27,28,30]. It was elevated during the increase in protein clearance during peritoneal dialysis [28], associated with pleural effusion and IVC diameter [18,30], ECW/TBW ratio [17,25,27] but not with peripheral oedema [9,18]. It has been compared during estimating hydration status with Ca-125 and in some studies both markers were elevated together with fluid excess [27] and in some cases only Ca-125 increased [29]. Núñez-Marín et. al. noticed that Ca-125 but no NT-pro-BNP correlated with VEXUS indicators of OH in patients with HF [29]. NT-pro-BNP correlated in establishing OH by BIS in Vega et. al study, together with a decrease in serum albumin, increase in CRP and proteinuria [12]. Fluid retention in patients with CKD calculated by BIS corresponded with an increase in NT-pro-BNP as the difference in euvolemia vs hypervolemia serum levels was 4.7 times higher [17]. In Schork et al. study NT-pro-BNP level also corresponded to OH calculated by BIS in CKD patients [25]. Basing on POCUS and BIS calculations NT-pro-BNP level corresponds to the obtained results as it is correlated with AKI in Beaubien-Souligny et al. two studies [24,30]. Even though this marker is a very promising and helpful tool its level is not always significant. Patients who were guided by lung POCUS and BIS signs of OH tended to have a lover level of NT-pro-BNP, however this difference was not statistically significant [16].
3.3.2. Ca-125
Carbohydrate antigen 125 (Ca-125) is a complex glycoprotein which is widely used in cancer diagnosis, especially ovarian cancer [75]. It is synthesized mainly by mesothelial cells in pericardium, peritoneum or pleura [75]. It is not well known why cells produce Ca-125, but it seems to be stimulated by inflammation process and mechanical injury [18]. Recently it became a promising marker for congestive heart failure as its blood concentration correlates with the severity of the illness [75]. It increases with a decline of heart function according to New York Heart Association (NYHA) I/II to stage III or IV [18]. In a study conducted by Arik et al. among different cancer markers and their correlation with kidney failure, only Ca-125 and Ca 19.9 were found to be significant. There was no correlation found with PSA, AFP, or CEA [76]. Ca-125 also strongly correlates with the diameter of IVC as well as with a presence of fluid in pleural cavity and peripheral oedema [75]. This phenomenon was investigated by Yilmaz et al. in patients with end stage kidney disease [26]. The level of this marker correlated with the advancement of CKD as well as with the level of NT-pro-BNP, C-reactive protein and with greater left ventricular end-diastolic diameter. A group of patients with a normal level of Ca-125 had higher albumin levels and haemoglobin when compared to a group with an elevated Ca-125. Núñez-Marín et al. did not find a correlation between IVC and Ca-125, but in their study carbohydrate antigen was independently associated with congestive pattern of intrarenal venous flow [29]. This study also showed that not NT-pro-BNP but Ca-125 correlates with an Doppler signs of volume overload. Carbohydrate antigen 125 appeared to increase with NT-pro-BNP, 24h peritoneal dialysate creatinine to serum creatinine ratio, decrease in albumin level and ECW/TBW ratio in an analysis which included 489 adult patients who underwent peritoneal dialysis [27]. There was no correlation between the Ca-125 level and 24h urinary creatinine clearance or CRP [27]. Scientists postulate that the noticeable decrease in albumin level was due to dilution effect, not a massive loss or cachexia. Ca-125 despite being a cancer marker has a great chance to become a fluid balance indicator. Results are very promising; however, correlations are not always cohesive, and more studies are needed.
3.3.3. Adrenomedullin and proadrenomedullin
ADM is a peptide hormone synthesized by endothelial and vascular smooth muscle cells of organs like lungs, brain, kidneys, heart and adrenal medulla as a response to increase in fluid volume [46,47]. Its function is vasodilatation, preservation of endothelial integrity and inhibition a renin-angiotensin-aldosterone system (protects heart and kidneys from damage induced by angiotensin II) [47]. It tends to decrease while using a diuretics, RAA-blockers which lead to the assumption that fluid overload activates sympathetic nervous system which stimulates its production [47]. In experimental and epidemiological studies it also shows anti-inflammatory as well as anti-oxidant properties, and ability to limit the arterial intima hyperplasia when organs are exposed to damage [48]. ADM is significantly elevated in HF, sepsis and other clinical states which lead to heart malfunction. It has been widely explored from more than 20 years as a potential marker of HF. The negative correlation between elevation of ADM and a decrease in left ventricular ejection fraction was noticed by Nishikimi et. al, together with a positive correlation with hike in NYHA classes and NT-pro-BNP plasma level [49]. This marker could be used also by nephrologists to investigate its correlation with the hydration status, not only in patients with concomitant HF as it gives a very promising result in cardiological research. However, ADM is difficult to measure from a blood sample as it is rapidly cleared from the circulation and even when present in bloodstream, it is covered by binding protein which makes it inaccessible for immunometric analysis [48,50]. Pro-ADM is a precursor of ADM, which its mid-regional fragment called Mid-Regional ADM (MR-pro-AMD) is more stable and can directly reflects the blood level of adrenomedullin [48,50]. It seem to be a better predictor of 90-days mortality due to cardiac incident than NT-pro-BNP and also its elevated level reflects poor 12-months survival in patients with HF [49]. MR-pro-ADM also correlates with indicators of vascular failure and other cardiological important factors included not only in the SCORE scale. In a cross-sectional study performed by Koyama et al. on almost 4000 patients showed that MR-pro-ADM was significantly higher in individuals with vascular failure, defined by brachial-ankle pulse wave velocity together with risk factors like obesity, hypertension, T2DM or dyslipidaemia [48]. The peptide is also investigated in Intensive Care Units among critically ill patients with a septic shock and systematic inflammatory response syndrome. Control healthy population had a mean value of MR-pro-ADM blood level 0.4 nmol/l while ill one 2.5 nmol/l and it tend to gradually increase with a severity of sepsis and intensity of fluid resuscitation [50]. MR-pro-AMD also correlated with the APACHE II score, SAPS II score, IL-6, creatinine, and age [50]. In the ENVOL study, proadrenomedullin indicator strongly positively correlated with a sodium imbalance, OH and current SOFA score [51]. In this investigation, only MR-pro-AMD and angiotensin II levels were significantly corresponding to sodium status, while Pro-atrial Natriuretic Peptide (MR-pro-ANP), renin, aldosterone, cortisol, norepinephrine, epinephrine, copeptin, pro-endothelin and EPO were not [51]. When considered as an OH marker in CKD population, it also seems to be very promising. MR-pro-AMD was investigated in HD population for up to 7 years in Austria. Majority of patients (82%) included in the study had an elevated MR-pro-AMD level ≥1.895 nmol/L and it was significantly higher in people who passed away during the study [52]. The peptide also correlated with other investigated marker, MR-pro-ANP which was elevated in 99% of patients and both parameters correlated with each other (r2= 0.62). The two indicators were strongly related to the probability of the death due to HF, but not within the entire group of fatal and non-fatal cardiovascular disease events. ADM seems to reflect the decompensated organ’s reaction to the multifractional injuries in preserving the integrity of the cardiovascular system in ESRD. MR-pro-AMD increased not only in patients with diagnosed HF, but also together with the advancement of renal disease. MR-pro-AMD tends to correlate with a relative OH status in patients with both haemo- and peritoneal dialysis (n=40) in Park et al. study. Its increase intensify together with the advancement of CKD, significantly correlated with NT-pro-BNP and cardiac markers (LV mass, LV mass index, ejection fraction, and left atrial diameter) [36]. These results make both ADM and MR-pro-ADM great perspective to become independent indicators of OH.
3.3.4. Galectin-3
Gal-3 protein was discovered in early 80s and since then its role has been studied in several organs, including kidneys [53]. Its increased expression can be connected to kidney injury and failure. In pre-clinical models it is overexpressed in diabetic nephropathy, toxic injury, cardiorenal syndrome or ischemia/reperfusion injury. In renal carcinoma cells Gal-3 shows that crucial for its expression is hypoxia and it level elevates gradually with a disease stage [54]. Gal-3 is also connected to immune-associated kidney damage like sepsis, cancer or autoimmune diseases [53,55]. It increases also in a model of congenital polycystic kidney (CPK) and tends to elevate deliberately together with the stage of renal disease. Gal-3 increases gradually with the advancement of CPK according to the Ozkurt et al study [56]. At the cellular level Gal-3 is associated with renal fibrogenesis and chronic inflammation [57]. A pathomorphological analysis indicated that higher Gal-3 concentration is associated with interstitial fibrosis, tubular atrophy, and vascular intimal fibrosis. In a 4 year clinical trial on 280 patients with renal disease urinary Gal-3 also correlated negatively with eGFR and positively with proteinuria [58]. The protein also shows a dependency with AKI development. In a transitional study on patients with a severe sepsis, Gal-3 increased gradually in patients with AKI, with a good prediction performance of illness [53]. In a study on 57-patients hospitalized in the ICU, Gal-3 was an independent factor of AKI prediction and it was significantly higher in patients who died during the research [55]. The protein was also detected in AKI which had developed after an intensive cancer treatment. In an experimental animal study the decrease of Gal-3 contributes to alleviating AKI induced by cisplatin[61]. When considered as OH marker, there is no direct connection, but the protein increases together with a renal and heart malfunction due to fluid overload. In a HF population Gal-3 was associated with an increased risk of death after adjustment on a renal injury biomarker [53]. In an observational study on 1200 patients with HF Gal-3 showed a negative correlation with eGFR, and connection with a mortality risk when diminished renal function is present [62]. Patients with higher Gal-3 concentration than established mean value (23.2 ng/ml) had a higher mortality rate than those with a lower marker level. However, it has no prognostic value of mortality risk when renal function was preserved. Not only as a renal injury marker, but also as a heart injury indicator in ERSD population. In HD children population Gal-3 increases together with a left ventricular diastolic dysfunction [63]. The clinical guidelines announced by the American Heart Association/American College of Cardiology marked the capability of Gal-3 as a predictor of mortality and hospitalization in cases with HF [63]. This property makes Gal-3 a good marker used both ways; in the ESRD when HF is suspected and the other way round. Even though it is not a direct OH indicator it should be considered as a marker of renal disease due to its correlation with the organ damage.
3.3.5. Urocortin-2
Ucn-2 is a peptide which has a similar structure to the corticotropin-release factor and binds via its receptor CRHRH-2[64]. This receptor is mainly found in central nervous system, heart and in endothelial and smooth muscle cells of the systemic vasculature. Its actions on animals tissues include vasodilation, positive inotropic and chronotropic effects together with cardioprotective abilities [65]. Ucn-2 increase is seen in HF, left ventricular systolic dysfunction, non-ischemic dilated cardiomyopathy and pulmonary arterial hypertension (PAH) [65]. The significant adverse effect is that it can cause a significant decrease in blood pressure which lead to worsening renal function in patients with ESKD [65]. When its action was compared with metoprolol, it increased heart haemodynamic parameters due to its ino- and chronotropic effects together with an increase in mean arterial pressure (MAP) [66]. The peptide activity on neurohormonal and renal function is still not well understood. Ucn-2 acts on diuresis stimulation, increase creatinine clearance and inhibits sodium retention, but this phenomenon which is seen in animals is not always present in humans [67]. Experimental study on rat model investigated Ucn-2 action on renal arteries. Urocortin dilatated renal arteries, and the magnitude of this effect did not vary between animals gender, but it seem that the mechanism is different in females (more dependent on Ca2+ released from sarcoplasmic reticulum) than males (probably not cAMP or sarcoplasmic Ca2+ release- mediated) [68]. Due to its potential to become a marker of HF, Ucn-2 is still undergoing tests on both models. Study on a group of 8 healthy men confirmed the haemodynamic effect as well as the ability to decrease MAP, vascular resistance, and increase the left ventricular ejection fraction [69]. The strong limitation of this study is the extremely small research group. In a combined clinical and experimental study, Ucn-2 was able to decrease PAH, improved right ventricle function as well as improved pulmonary circulation [70]. The peptide did not alter the sodium, potassium, NT-pro-BNP concentrations, but it increased the release of angiotensin II and renin. However, Ucn-2 plasma level did not differ between the patients who suffered from PAH and healthy group, but it increased m-RNA expression was observed in people with right ventricle failure. Rats treated with the protein had a decrease in an extra fluid build-up in the lungs, which is probably the effect of improvement of LV function. In a study on the HF population its elevated level correlated positively with higher sodium retention score, uric acid concentration, peripheral oedema, and hepatomegaly presence. It correlated negatively with IVC collapse ability [65]. There was no association between Ucn-2 and renal function or haemoglobin level in this study. When considered as an OH status marker or factor which can improve the renal function, the results differ between studies. In an investigation performed on 12 sheep which received a murine Ucn-2 injection (via pulmonary artery catheter), the diminishing effect of HF factors as well as improving renal function were obtained. It was able to decrease the MAP, left atrial pressure together with a suppression of cardio remodelling factors production (aldosterone, arginine vasopressin, and endothelin 1) [64]. Decrease in creatinine and sodium blood level combined with the increase in urine output indicate the improvement of renal function. The same scientific group compared Ucn-2 effect on heart and kidney function on another sheep model but compared with dobutamine [71]. Effect on heart haemodynamic was comparable between the substances, but Ucn-2 expressed better improvement on central venous and left atrial pressures. Dobutamine and Ucn-2 improved renal function, but the significant sodium excretion was altered by Ucn-2. What is more interesting, Ucn-2 decreased the overall OH status while dobutamine increased it. When compared to another drug it also had given better results on both HF and OH. Similarly, to the article mentioned above, in an animal study Ucn-2 noticed better effect on diuresis, creatinine level, sodium balance than furosemide. It was able to decrease better renin level, aldosterone and vasopressin concentration [72]. The heart function also improved as pressure drops together with a peripheral resistance. Ucn-2 attenuated furosemide function, which is a promising property, as some patients with ESKD develop a diuretics resistance. Experimental study on rats to investigate the possible Ucn-2 influence on renal dysfunction and injury caused by ischaemia or reperfusion showed that it was not able to decrease the organ failure [73]. Ucn-2 did not increase the creatinine clearance nor stopped anuria; higher dose of protein caused even decrease in renal function. The opposite effect was observed in human study by Chan et al. where Ucn-2 revised renal function and slashed RAA activity when compared to placebo [74]. Treated group required lower dose of furosemide and indirect OH marker NT-pro-BNP decreased after the infusion. Ucn-2 needs to be more investigated in a future as it gives good results on animal model and these properties should be investigated among humans.
3.3.6. Imaging studies
Ultrasonography is one of the common tests performed in clinical trials either in a specific room or beside the patient’s bed – POCUS. In terms of hydration status, doctors can depict and measure the width of IVC, jugular veins, hepatic portal vein and renal veins. The assessment of fluid inside the pleural cavity or in the peritoneum can also be helpful. POCUS is nowadays one of the components of physical examination inextricably connected with auscultation, palpation and inspection [77]. It is used to verify standard diagnostic exam as auscultation can be normal (81%) in patients with a lung fluid overload noticed in US test [18]. Other simple radiological tests are inconclusive as the presence of fluid in the pleural cavity can be seen using an X-ray only when at least 200 ml of fluid is present [7]. POCUS accelerates the diagnosis or exclusion of some pathologies in real time without a need for a consultation[31]. Koratala et al. gave an example of a patient with CKD who had missed one dialysis session and suffered from shortness of breath, POCUS revealed fluid around his heart in pericardium [77]. Lung POCUS can reveal an extravascular fluid as diffuse B-line pattern. Both symptomatic and asymptomatic lungs congestion worsens outcomes in patients with CKD [11]. Lung USG is also used by nephrologists to guide dry body weight estimation during HD [77]. When patients are closer to their ideal body mass, fewer symptoms of OH are present in USG. The most promising results in prediction of OH were obtained by lung US [78]. B line score were more accurate than BIS and they can help to recognize asymptomatic lung congestion in HD patients [8]. Dynamical changes of B-lines during hemofiltration, the residual congestion at the end of HD can be used to titrate dry body mass [11]. In another study guided by Lutradis et al., scientists studied the effect of estimation of dry body weight based on lungs USG for 8 weeks in ambulatory conditions [79]. It appeared that patients guided by this protocol maintained dry body weight better and noticed a decrease in blood pressure when compared to a group guided by normal criteria [79]. A positive correlation between line B score changes and dry body weight was observed [79]. On the other hand, a study on 250 HD patients to adjust dry body mass using lung POCUS together with BIS did not improve life expectancy or cardiovascular events [16]. Sick people with fluid overload or right ventricle failure develop clinically important organ congestion due to fluid retention and it can be seen as IVC dilatation or fluid presence in a third space [24]. In a study on HD individuals authors demonstrated that a decrease in dry body weight of 0.7 kg resulted in reduction of IVC diameter and improved left heart contraction function [8]. Extracellular fluid estimated by US correlates also with BIS method in HD patients [19]. POCUS examination is useful also in estimating the life expectancy of HF patients, as in a study on 80 individuals admission IVC diameter ≥1.9 cm was associated with a higher mortality at 90 and 180 days in people hospitalized for acute heart failure [18]. IVC size and flow is a sign of elevation of right atrial pressure due to heart malfunction or fluid overload within a vessel. IVC enlargement is associated with an increase of the Ca-125 in patients with HF [75]. IVC is used for evaluation of right ventricle preload, but it should be taken with a caution in mechanically ventilated patients (modification by positive pressure) [7,18]. To expand a diagnostic application of US, the assessment of vessels width together with venous pressure has found its application. Venous Excess Ultrasound Score (VEXUS) is used by clinicians in combination with IVC measurement, hepatic vein Doppler, portal vein pulsation and blood flow in renal vessels [80]. Many clinical studies indicate a positive correlation between alterations in hepatic portal vein flow and AKI incidence after a cardiac surgery [24,30,31,80]. POCUS allows to visualise venous anatomy together with assessment of blood velocity using Doppler. Beaubien-Souligny proposed 5 prototypes of VEXUS grading system based on the changes in venous ultrasound markers: waveform of portal, hepatic and intrarenal veins together with IVC diameter [24]. Only one proposed model corresponded with AKI development, but other OH markers like IVC, NT-pro-BNP, cumulative fluid balance or central venous pressure were associated with all systems. Research points that IVC has got a poor diagnostic sensitivity (specificity 41%), which suggests that a simple US test for OH is not sufficient [24]. The study led by the same team on 145 patients after cardiac surgery, 49 who developed AKI had an increase in portal vein flow, NT-pro-BNP and IVC measurement [30]. Doppler flow in renal veins is nowadays widely investigated by cardiologists as fluid overload is one of the markers of HF. Hepatic veins can indicate the diastolic function of right ventricle [7]. Increase in portal vein pulsatile flow is a marker of hepatic hypertension present in congestive heart failure. During the decline in function of the right ventricle, the flow in renal veins becomes monophasic and strongly correlates with the number of unplanned hospitalizations and death from cardiovascular disease [7]. Doppler signs of fluid overload were diminished after administration of diuretics in Argaiz et al. study which allowed POCUS to become a marker of OH in patients with CHF in this analysis [31]. Together with changes in venous congestion there was a decrease in the NT-pro-BNP level, there was no change in proteinuria or haematuria [31]. Another cardiological study by Núñez-Marín et al. investigated a correlation between intrarenal Doppler, Ca-125 and NT-pro-BNP. Patients with higher congestion scores in renal veins had a greater evidence of clinical and ECHO features of fluid overload [29]. NT-pro-BNP was not concordant with renal Doppler flow, but Ca-125 was independently correlated. There is a hypothesis that fluid overload causes an increase in inflammatory cytokines production as well as hydrostatic pressure which consequently leads to Ca-125 overproduction and release [29]. Once again, simple IVC diameter was not an independent determinant of congestive intrarenal venous flow and consequently a determinant of OH [29]. The lack of correlation between OH signs and IVC diameter or collapse index was described by Agarwal et al. It is also important to notice that clinical appearance of OH in the form of oedema was not related to NT-pro-BNP, right atrial pressure or relative blood volume [9]. This paper gives an information that even though IVC and other additional markers of OH are promising, they do not always correlate with a clinical state. As noticed and described above, the width of IVC is not always an indicator of fluid overload as its dilatation was present in healthy 98 athletes, illnesses like valvulopathies and pulmonary hypertension [80]. The key role to assess the patient’s hydration status using USG also is the physicians experience and may vary between patients with obesity or hyperventilation which may mask the real problem. Misinterpretation can be also caused by inappropriate patient positioning or presence of catheter [18].
4. Materials and methods
We undertook a systematic search through the PubMed database from inception to November 10, 2022. We searched both with individual keywords with all subheadings included. Individual keywords used were “overhydration renal disease”, “overhydration NT-pro BNP”, “overhydration creatinine”, “overhydration dialysis”, “overhydration bioimpedance”, “bioimpedance renal disease”, “renal failure Ca-125”, “VEXUS”, “POCUS nephrology”, “Adrenomedullin”, “pro-ADM dialysis” “Galectin-3 renal”, “Ucn-2 renal”. The results were merged with duplicates discarded. Remaining articles were screened for relevance (based on their title, abstract, or full text). All articles about hydration status were included due to paucity of data: original studies and reviews/perspectives were both experimental and human. Articles were included only if they were clearly related to other subject matters or were only published in English.
5. Conclusion and results
Modern medicine stands in a huge need for OH markers and as described in this review, there is no specific and accurate one. The presence or absence of symptoms during a simple physical examination does not exclude fluid overload. The combination of BIS, POCUS with VEXUS protocole together seem to have a promising and good results. The addition of serum markers like NT-pro-BNP or Ca-125 broadens the viewpoint on volume status when compared to studies based on only one OH test. The great potential of Ca-125 noticed by cardiologists should be deeply investigated by nephrologists not only in patients with HF. The markers mentioned in the study: ADM, pro-ADM, Ucn-2, Gal-3 need to be further investigated as OH markers.
Conflicts of Interest
The authors declare no conflict of interest. The funders had no role in the design of the study; in the collection, analyses, or interpretation of data; in the writing of the manuscript; or in the decision to publish the results.
Abbreviations
| ADM | adrenomedullin |
| AKI | acute kidney injury |
| BCM | Body Composition Monitor |
| BIS | Bioimpendance spectroscopy |
| Ca-125 | Carbohydrate antigen 125 |
| CKD | chronic kidney disease |
| CPK | congenital polycystic kidney |
| CT | computer tomography |
| ECW | internal cell water |
| eGFR | estimated GFR |
| ESRD | end stage renal disease |
| FDA | Food and Drug Administration |
| FFM | fat free mass |
| GFR | glomerular filtration rate |
| HD | haemodialysis |
| HF | heart failure |
| ICU | intensive care unit |
| ICW | internal cell water |
| IVC | inferior vena cava |
| MAP | mean arterial pressure |
| MRI | magnetic resonance imagining |
| MR-pro-AMD | Mid-regional AMD |
| MR-pro-AMP | Pro-atrial Natriuretic Peptide |
| NYHA | New York Heart Association |
| OH | overhydration |
| PAH | pulmonary arterial hypertension |
| POCUS | point of care ultrasonography |
| Pro-ADM | proadrenomedullin |
| TBW | total body water |
| USG | ultrasonography |
| VEXUS | Venous Excess Ultrasound Score |
References
- Ohashi, Y.; Sakai, K.; Hase, H.; Joki, N. Dry weight targeting: The art and science of conventional hemodialysis. Semin. Dial. 2018, 31, 551–556. [Google Scholar] [CrossRef] [PubMed]
- Zoccali, C.; Moissl, U.; Chazot, C.; Mallamaci, F.; Tripepi, G.; Arkossy, O.; Wabel, P.; Stuard, S. Chronic Fluid Overload and Mortality in ESRD. 2017.
- Wang, Y.; Gu, Z. Effect of bioimpedance-defined overhydration parameters on mortality and cardiovascular events in patients undergoing dialysis: a systematic review and meta-analysis. J. Int. Med. Res. 2021, 49. [Google Scholar] [CrossRef] [PubMed]
- Hung, S.C.; Kuo, K.L.; Peng, C.H.; Wu, C.H.; Lien, Y.C.; Wang, Y.C.; Tarng, D.C. Volume overload correlates with cardiovascular risk factors in patients with chronic kidney disease. Kidney Int. 2014, 85, 703–709. [Google Scholar] [CrossRef] [PubMed]
- Donati, P.A.; Guevara, J.M.; Ardiles, V.; Guillemi, E.C.; Londoño, L.; Dubin, A. Caudal vena cava collapsibility index as a tool to predict fluid responsiveness in dogs. J. Vet. Emerg. Crit. Care 2020, 30, 677–686. [Google Scholar] [CrossRef]
- Hansen, B. Fluid Overload. Front. Vet. Sci. 2021, 8, 1–7. [Google Scholar] [CrossRef] [PubMed]
- Beaubien-Souligny, W.; Bouchard, J.; Desjardins, G.; Lamarche, Y.; Liszkowski, M.; Robillard, P.; Denault, A. Extracardiac Signs of Fluid Overload in the Critically Ill Cardiac Patient: A Focused Evaluation Using Bedside Ultrasound. Can. J. Cardiol. 2017, 33, 88–100. [Google Scholar] [CrossRef]
- Loutradis, C.; Papadopoulos, C.E.; Sachpekidis, V.; Ekart, R.; Krunic, B.; Karpetas, A.; Bikos, A.; Tsouchnikas, I.; Mitsopoulos, E.; Papagianni, A.; et al. Lung Ultrasound–Guided Dry Weight Assessment and Echocardiographic Measures in Hypertensive Hemodialysis Patients: A Randomized Controlled Study. Am. J. Kidney Dis. 2020, 75, 11–20. [Google Scholar] [CrossRef]
- Agarwal, R.; Andersen, M.J.; Pratt, J.H. On the importance of pedal edema in hemodialysis patients. Clin. J. Am. Soc. Nephrol. 2008, 3, 153–158. [Google Scholar] [CrossRef]
- Zubiaga; Aguilar; Ruíz-Tovar; Calpena; García; Durán Hydration status according to impedance vectors and its association with clinical and biochemical outcomes and mortality in patients with chronic kidney disease. Nutr Hosp 2016, 33, 832–837.
- Koratala, A.; Ronco, C.; Kazory, A. The Promising Role of Lung Ultrasound in Assessment of Volume Status for Patients Receiving Maintenance Renal Replacement Therapy. Blood Purif. 2020, 49, 643–646. [Google Scholar] [CrossRef]
- Vega, A.; Abad, S.; Macías, N.; Aragoncillo, I.; García-Prieto, A.; Linares, T.; Torres, E.; Hernández, A.; Luño, J. Any grade of relative overhydration is associated with long-term mortality in patients with Stages 4 and 5 non-dialysis chronic kidney disease. Clin. Kidney J. 2018, 11, 372–376. [Google Scholar] [CrossRef] [PubMed]
- Lu, W.; Pang, W.F.; Jin, L.; Li, H.; Chow, K.M.; Kwan, B.C.H.; Leung, C.B.; Li, P.K.T.; Szeto, C.C. Peritoneal protein clearance predicts mortality in peritoneal dialysis patients. Clin. Exp. Nephrol. 2019, 23, 551–560. [Google Scholar] [CrossRef] [PubMed]
- Chazot, C.; Wabel, P.; Chamney, P.; Moissl, U.; Wieskotten, S.; Wizemann, V.; Le, S.F. Original Articles Importance of normohydration for the long-term survival of haemodialysis patients. 2012, 2404–2410. [CrossRef]
- Gracia-Iguacel, C.; González-Parra, E.; Mahillo, I.; Ortiz, A. Low intracellular water, overhydration, and mortality in hemodialysis patients. J. Clin. Med. 2020, 9, 1–11. [Google Scholar] [CrossRef] [PubMed]
- Siriopol, D.; Onofriescu, M.; Voroneanu, L.; Apetrii, M.; Nistor, I.; Hogas, S.; Kanbay, M.; Sascau, R.; Scripcariu, D.; Covic, A. Dry weight assessment by combined ultrasound and bioimpedance monitoring in low cardiovascular risk hemodialysis patients: a randomized controlled trial. Int. Urol. Nephrol. 2017, 49, 143–153. [Google Scholar] [CrossRef] [PubMed]
- Hung, S.C.; Lai, Y.S.; Kuo, K.L.; Tarng, D.C. Volume overload and adverse outcomes in chronic kidney disease: clinical observational and animal studies. J. Am. Heart Assoc. 2015, 4, 1–12. [Google Scholar] [CrossRef]
- Koratala, A.; Ronco, C.; Kazory, A. Diagnosis of Fluid Overload: from Conventional to Contemporary Concepts. Cardiorenal Med. 2022. [Google Scholar] [CrossRef]
- Dekker, M.J.E.; Kooman, J.P. Fluid status assessment in hemodialysis patients and the association with outcome: Review of recent literature. Curr. Opin. Nephrol. Hypertens. 2018, 27, 188–193. [Google Scholar] [CrossRef]
- Onofriescu, M.; Siriopol, D.; Voroneanu, L.; Hogas, S.; Nistor, I.; Apetrii, M.; Florea, L.; Veisa, G.; Mititiuc, I.; Kanbay, M.; et al. Overhydration, cardiac function and survival in hemodialysis patients. PLoS One 2015, 10, 1–13. [Google Scholar] [CrossRef]
- Krediet, R.T.; Smit, W.; Coester, A.M.; Struijk, D.G. Dry body weight and ultrafiltration targets in peritoneal dialysis. Contrib. Nephrol. 2009, 163, 90–95. [Google Scholar] [CrossRef]
- Dolgos, S.; Hartmann, A.; Bollerslev, J.; Vörös, P.; Rosivall, L. The importance of body composition and dry weight assessments in patients with chronic kidney disease (Review). Acta Physiol. Hung. 2011, 98, 105–116. [Google Scholar] [CrossRef]
- Earthman, C.; Traughber, D.; Dobratz, J.; Howell, W. Bioimpedance spectroscopy for clinical assessment of fluid distribution and Body cell mass. Nutr. Clin. Pract. 2007, 22, 389–405. [Google Scholar] [CrossRef] [PubMed]
- Beaubien-Souligny, W.; Rola, P.; Haycock, K.; Bouchard, J.; Lamarche, Y.; Spiegel, R.; Denault, A.Y. Quantifying systemic congestion with Point-Of-Care ultrasound: development of the venous excess ultrasound grading system. Ultrasound J. 2020, 12. [Google Scholar] [CrossRef] [PubMed]
- Schork, A.; Bohnert, B.N.; Heyne, N.; Birkenfeld, A.L.; Artunc, F. Overhydration Measured by Bioimpedance Spectroscopy and Urinary Serine Protease Activity Are Risk Factors for Progression of Chronic Kidney Disease. Kidney Blood Press. Res. 2020, 45, 955–968. [Google Scholar] [CrossRef] [PubMed]
- Yilmaz, H.; Gürel, O.M.; Çelik, H.T.; Şahiner, E.; Yildirim, M.E.; Bilgiç, M.A.; Bavbek, N.; Akcay, A. CA 125 levels and left ventricular function in patients with end-stage renal disease on maintenance hemodialysis. Ren. Fail. 2014, 36, 210–216. [Google Scholar] [CrossRef] [PubMed]
- Wijayaratne, D.; Muthuppalaniappan, V.M.; Davenport, A. Serum CA125 a potential marker of volume status for peritoneal dialysis patients? Int. J. Artif. Organs 2021, 44, 1029–1033. [Google Scholar] [CrossRef] [PubMed]
- Guedes, A.M.; Marques, R.; Domingos, A.T.; Silva, A.P.; Bernardo, I.; Neves, P.L.; Rodrigues, A.; Krediet, R.T. Overhydration May Be the Missing Link between Peritoneal Protein Clearance and Mortality. Nephron 2021, 145, 474–480. [Google Scholar] [CrossRef] [PubMed]
- Núñez-Marín, G.; de la Espriella, R.; Santas, E.; Lorenzo, M.; Miñana, G.; Núñez, E.; Bodí, V.; González, M.; Górriz, J.L.; Bonanad, C.; et al. CA125 but not NT-proBNP predicts the presence of a congestive intrarenal venous flow in patients with acute heart failure. Eur. Hear. Journal. Acute Cardiovasc. Care 2021, 10, 475–483. [Google Scholar] [CrossRef] [PubMed]
- Beaubien-Souligny, W.; Benkreira, A.; Robillard, P.; Bouabdallaoui, N.; Chassé, M.; Desjardins, G.; Lamarche, Y.; White, M.; Bouchard, J.; Denault, A. Alterations in portal vein flow and intrarenal venous flow are associated with acute kidney injury after cardiac surgery: A prospective observational cohort study. J. Am. Heart Assoc. 2018, 7. [Google Scholar] [CrossRef] [PubMed]
- Argaiz, E.R.; Rola, P.; Gamba, G. Dynamic Changes in Portal Vein Flow during Decongestion in Patients with Heart Failure and Cardio-Renal Syndrome: A POCUS Case Series. CardioRenal Med. 2021, 11, 59–66. [Google Scholar] [CrossRef] [PubMed]
- Cornejo-Pareja, I.; Vegas-Aguilar, I.M.; Lukaski, H.; Talluri, A.; Bellido-Guerrero, D.; Tinahones, F.J.; García-Almeida, J.M. Overhydration Assessed Using Bioelectrical Impedance Vector Analysis Adversely Affects 90-Day Clinical Outcome among SARS-CoV2 Patients: A New Approach. Nutrients 2022, 14. [Google Scholar] [CrossRef]
- MacHek, P.; Jirka, T.; Moissl, U.; Chamney, P.; Wabel, P. Guided optimization of fluid status in haemodialysis patients. Nephrol. Dial. Transplant. 2010, 25, 538–544. [Google Scholar] [CrossRef] [PubMed]
- Kim, H.; Choi, G.H.; Shim, K.E.; Lee, J.H.; Heo, N.J.; Joo, K.W.; Yoon, J.W.; Oh, Y.K. Changes in bioimpedance analysis components before and after hemodialysis. Kidney Res. Clin. Pract. 2018, 37, 393–403. [Google Scholar] [CrossRef] [PubMed]
- Covic, A.; Ciumanghel, A.I.; Siriopol, D.; Kanbay, M.; Dumea, R.; Gavrilovici, C.; Nistor, I. Value of bioimpedance analysis estimated “dry weight” in maintenance dialysis patients: a systematic review and meta-analysis. Int. Urol. Nephrol. 2017, 49, 2231–2245. [Google Scholar] [CrossRef] [PubMed]
- Park, W.Y.; Park, S.; Kim, Y.W.; Jin, K. Clinical efficacy of biomarkers for evaluation of volume status in dialysis patients. Med. (United States) 2020, 99, 1–7. [Google Scholar] [CrossRef] [PubMed]
- Wang, A.Y.M.; Lam, C.W.K.; Yu, C.M.; Wang, M.; Chan, I.H.S.; Zhang, Y.; Lui, S.F.; Sanderson, J.E. N-terminal pro-brain natriuretic peptide: An independent risk predictor of cardiovascular congestion, mortality, and adverse cardiovascular outcomes in chronic peritoneal dialysis patients. J. Am. Soc. Nephrol. 2007, 18, 321–330. [Google Scholar] [CrossRef] [PubMed]
- Koratala, A.; Kazory, A. Natriuretic Peptides as Biomarkers for Congestive States: The Cardiorenal Divergence. Dis. Markers 2017, 2017. [Google Scholar] [CrossRef] [PubMed]
- London, G. Pathophysiology of cardiovascular damage in the early renal population. Nephrol. Dial. Transplant. 2001, 16, 3–6. [Google Scholar] [CrossRef]
- Astor, B.C.; Yi, S.; Hiremath, L.; Corbin, T.; Pogue, V.; Wilkening, B.; Peterson, G.; Lewis, J.; Lash, J.P.; Van Lente, F.; et al. N-terminal prohormone brain natriuretic peptide as a predictor of cardiovascular disease and mortality in blacks with hypertensive kidney disease: The African American Study of Kidney Disease and Hypertension (AASK). Circulation 2008, 117, 1685–1692. [Google Scholar] [CrossRef]
- Goto, T.; Takase, H.; Toriyama, T.; Sugiura, T.; Kurita, Y.; Tsuru, N.; Masuda, H.; Hayashi, K.; Ueda, R.; Dohi, Y. Increased circulating levels of natriuretic peptides predict future cardiac event in patients with chronic hemodialysis. Nephron 2002, 92, 610–615. [Google Scholar] [CrossRef]
- Fu, S.; Luo, L.; Ye, P.; Yi, S.; Liu, Y.; Zhu, B.; Wang, L.; Xiao, T.; Bai, Y. The ability of NT-proBNP to detect chronic heart failure and predict all-cause mortality is higher in elderly Chinese coronary artery disease patients with chronic kidney disease. Clin. Interv. Aging 2013, 8, 409–417. [Google Scholar] [CrossRef]
- LA, O.; A, S.; JS, B. Amino-terminal Pro B-Type Natriuretic Peptide for Diagnosis and Prognosis in Patients with Renal Dysfunction: A Systematic Review and Meta-Analysis. Physiol. Behav. 2017, 176, 139–148. [Google Scholar] [CrossRef]
- Anwaruddin, S.; Lloyd-Jones, D.M.; Baggish, A.; Chen, A.; Krauser, D.; Tung, R.; Chae, C.; Januzzi, J.L. Renal function, congestive heart failure, and amino-terminal pro-brain natriuretic peptide measurement: Results from the ProBNP investigation of dyspnea in the emergency department (PRIDE) study. J. Am. Coll. Cardiol. 2006, 47, 91–97. [Google Scholar] [CrossRef] [PubMed]
- DeFilippi, C.R.; Seliger, S.L.; Maynard, S.; Christenson, R.H. Impact of renal disease on natriuretic peptide testing for diagnosing decompensated heart failure and predicting mortality. Clin. Chem. 2007, 53, 1511–1519. [Google Scholar] [CrossRef] [PubMed]
- Pousset, F.; Masson, F.; Chavirovskaia, O.; Isnard, R.; Carayon, A.; Golmard, J.L.; Lechat, P.; Thomas, D.; Komajda, M. Plasma adrenomedullin, a new independent predictor of prognosis in patients with chronic heart failure. Eur. Heart J. 2000, 21, 1009–1014. [Google Scholar] [CrossRef] [PubMed]
- Voors, A.A.; Kremer, D.; Geven, C.; ter Maaten, J.M.; Struck, J.; Bergmann, A.; Pickkers, P.; Metra, M.; Mebazaa, A.; Düngen, H.D.; et al. Adrenomedullin in heart failure: pathophysiology and therapeutic application. Eur. J. Heart Fail. 2019, 21, 163–171. [Google Scholar] [CrossRef] [PubMed]
- Koyama, T.; Kuriyama, N.; Suzuki, Y.; Saito, S.; Tanaka, R.; Iwao, M.; Tanaka, M.; Maki, T.; Itoh, H.; Ihara, M.; et al. Mid-regional pro-adrenomedullin is a novel biomarker for arterial stiffness as the criterion for vascular failure in a cross-sectional study. Sci. Rep. 2021, 11, 1–7. [Google Scholar] [CrossRef]
- Nishikimi, T.; Nakagawa, Y. Adrenomedullin as a Biomarker of Heart Failure. Heart Fail. Clin. 2018, 14, 49–55. [Google Scholar] [CrossRef]
- Christ-Crain, M.; Morgenthaler, N.G.; Struck, J.; Harbarth, S.; Bergmann, A.; Müller, B. Mid-regional pro-adrenomedullin as a prognostic marker in sepsis: an observational study. Crit. Care 2005, 9, 816–824. [Google Scholar] [CrossRef]
- Vigué, B.; Leblanc, P.E.; Moati, F.; Pussard, E.; Foufa, H.; Rodrigues, A.; Figueiredo, S.; Harrois, A.; Mazoit, J.X.; Rafi, H.; et al. Mid-regional pro-adrenomedullin (MR-proADM), a marker of positive fluid balance in critically ill patients: Results of the ENVOL study. Crit. Care 2016, 20, 1–9. [Google Scholar] [CrossRef]
- Gouya, G.; Sturm, G.; Lamina, C.; Zitt, E.; Freistätter, O.; Struck, J.; Wolzt, M.; Knoll, F.; Lins, F.; Lhotta, K.; et al. The association of mid-regional pro-adrenomedullin and mid-regional pro-atrial natriuretic peptide with mortality in an incident dialysis cohort. PLoS One 2011, 6. [Google Scholar] [CrossRef]
- Boutin, L.; Dépret, F.; Gayat, E.; Legrand, M.; Chadjichristos, C.E. Galectin-3 in Kidney Diseases: From an Old Protein to a New Therapeutic Target. Int. J. Mol. Sci. 2022, 23. [Google Scholar] [CrossRef] [PubMed]
- Gu, X.; Meng, H.; Wang, J.; Wang, R.; Cao, M.; Liu, S.; Chen, H.; Xu, Y. Hypoxia contributes to galectin-3 expression in renal carcinoma cells. Eur. J. Pharmacol. 2021, 890, 173637. [Google Scholar] [CrossRef] [PubMed]
- Sun, H.; Jiang, H.; Eliaz, A.; Kellum, J.A.; Peng, Z.; Eliaz, I. Galectin-3 in septic acute kidney injury: a translational study. Crit. Care 2021, 25, 1–11. [Google Scholar] [CrossRef] [PubMed]
- Ozkurt, S.; Dogan, I.; Ozcan, O.; Fidan, N.; Bozaci, I.; Yilmaz, B.; Bilgin, M. Correlation of serum galectin-3 level with renal volume and function in adult polycystic kidney disease. Int. Urol. Nephrol. 2019, 51, 1191–1197. [Google Scholar] [CrossRef]
- Ou, S.M.; Tsai, M.T.; Chen, H.Y.; Li, F.A.; Tseng, W.C.; Lee, K.H.; Chang, F.P.; Lin, Y.P.; Yang, R.B.; Tarng, D.C. Identification of Galectin-3 as Potential Biomarkers for Renal Fibrosis by RNA-Sequencing and Clinicopathologic Findings of Kidney Biopsy. Front. Med. 2021, 8, 1–11. [Google Scholar] [CrossRef]
- Ou, S.M.; Tsai, M.T.; Chen, H.Y.; Li, F.A.; Lee, K.H.; Tseng, W.C.; Chang, F.P.; Lin, Y.P.; Yang, R.B.; Tarng, D.C. Urinary Galectin-3 as a Novel Biomarker for the Prediction of Renal Fibrosis and Kidney Disease Progression. Biomedicines 2022, 10, 1–13. [Google Scholar] [CrossRef]
- Ding, H.; Shen, Y.; Lin, C.; Qin, L.; He, S.; Dai, M.; Okitsu, S.L.; DeMartino, J.A.; Guo, Q.; Shen, N. Urinary galectin-3 binding protein (G3BP) as a biomarker for disease activity and renal pathology characteristics in lupus nephritis. Arthritis Res. Ther. 2022, 24, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Tang, H.; Zhang, P.; Zeng, L.; Zhao, Y.; Xie, L.; Chen, B. Mesenchymal stem cells ameliorate renal fibrosis by galectin-3/Akt/GSK3β/Snail signaling pathway in adenine-induced nephropathy rat. Stem Cell Res. Ther. 2021, 12, 1–22. [Google Scholar] [CrossRef]
- Li, H.Y.; Yang, S.; Li, J.C.; Feng, J.X. Galectin 3 inhibition attenuates renal injury progression in cisplatin-induced nephrotoxicity. Biosci. Rep. 2018, 38, 1–10. [Google Scholar] [CrossRef]
- Caravaca Perez, P.; González-Juanatey, J.R.; Nuche, J.; Matute-Blanco, L.; Serrano, I.; Martínez Selles, M.; Vázquez García, R.; Martínez Dolz, L.; Gómez-Bueno, M.; Pascual Figal, D.; et al. Renal Function Impact in the Prognostic Value of Galectin-3 in Acute Heart Failure. Front. Cardiovasc. Med. 2022, 9, 1–11. [Google Scholar] [CrossRef]
- Elsadek, A.; Ibrahim, M.; El Fallah, A.A.; Elian, M.; Deraz, S.E. Galectin-3 as an early marker of diastolic dysfunction in children with end-stage renal disease on regular hemodialysis. Ann. Pediatr. Cardiol. 2022, 15, 266–272. [Google Scholar] [CrossRef] [PubMed]
- Rademaker, M.T.; Charles, C.J.; Ellmers, L.J.; Lewis, L.K.; Nicholls, M.G.; Richards, A.M. Prolonged urocortin 2 administration in experimental heart failure: Sustained hemodynamic, endocrine, and renal effects. Hypertension 2011, 57, 1136–1144. [Google Scholar] [CrossRef] [PubMed]
- Pintalhao, M.; Maia-Rocha, C.; Castro-Chaves, P.; Adão, R.; Barros, A.S.; Clara Martins, R.; Leite-Moreira, A.; Bettencourt, P.; Bras-Silva, C. Urocortin-2 in Acute Heart Failure: Role as a Marker of Volume Overload and Pulmonary Hypertension. Curr. Probl. Cardiol. 2022, 47, 1–17. [Google Scholar] [CrossRef] [PubMed]
- Rademaker, M.T.; Charles, C.J.; Nicholls, G.; Richards, M. Urocortin 2 sustains haemodynamic and renal function during introduction of beta-blockade in experimental heart failure. J. Hypertens. 2011, 29, 1787–1795. [Google Scholar] [CrossRef]
- Garg, V.; Frishman, W.H. A New Potential Approach to Inotropic Therapy in the Treatment of Heart Failure: Urocortin. Cardiol. Rev. 2013, 21, 160–165. [Google Scholar] [CrossRef] [PubMed]
- Sanz, E.; Monge, L.; Fernández, N.; Climent, B.; Diéguez, G.; Garcia-Villalón, A.L. Mechanisms of relaxation by urocortin in renal arteries from male and female rats. Br. J. Pharmacol. 2003, 140, 1003–1007. [Google Scholar] [CrossRef]
- Davis, M.E.; Pemberton, C.J.; Yandle, T.G.; Fisher, S.F.; Lainchbury, J.G.; Frampton, C.M.; Rademaker, M.T.; Richards, A.M. Urocortin 2 Infusion in Healthy Humans. Hemodynamic, Neurohormonal, and Renal Responses. J. Am. Coll. Cardiol. 2007, 49, 461–471. [Google Scholar] [CrossRef]
- Adão, R.; Mendes-Ferreira, P.; Santos-Ribeiro, D.; Maia-Rocha, C.; Pimentel, L.D.; Monteiro-Pinto, C.; Mulvaney, E.P.; Reid, H.M.; Kinsella, B.T.; Potus, F.; et al. Urocortin-2 improves right ventricular function and attenuates pulmonary arterial hypertension. Cardiovasc. Res. 2018, 114, 1165–1177. [Google Scholar] [CrossRef]
- Rademaker, M.T.; Ellmers, L.J.; Charles, C.J.; Mark Richards, A. Urocortin 2 protects heart and kidney structure and function in an ovine model of acute decompensated heart failure: Comparison with dobutamine. Int. J. Cardiol. 2015, 197, 56–65. [Google Scholar] [CrossRef]
- Rademaker, M.T.; Charles, C.J.; Nicholls, M.G.; Richards, A.M. Urocortin 2 inhibits furosemide-induced activation of renin and enhances renal function and diuretic responsiveness in experimental heart failure. Circ. Hear. Fail. 2009, 2, 532–540. [Google Scholar] [CrossRef]
- Patel, N.S.A.; Collin, M.; Thiemermann, C. Urocortin does not reduce the renal injury and dysfunction caused by experimental ischaemia/reperfusion. Eur. J. Pharmacol. 2004, 496, 175–180. [Google Scholar] [CrossRef] [PubMed]
- Chan, W.Y.W.; Frampton, C.M.; Crozier, I.G.; Troughton, R.W.; Richards, A.M. Urocortin-2 infusion in acute decompensated heart failure: Findings from the UNICORN study (urocortin-2 in the treatment of acute heart failure as an adjunct over conventional therapy). JACC Hear. Fail. 2013, 1, 433–441. [Google Scholar] [CrossRef]
- Núñez, J.; de la Espriella, R.; Miñana, G.; Santas, E.; Llácer, P.; Núñez, E.; Palau, P.; Bodí, V.; Chorro, F.J.; Sanchis, J.; et al. Antigen carbohydrate 125 as a biomarker in heart failure: a narrative review. Eur. J. Heart Fail. 2021, 23, 1445–1457. [Google Scholar] [CrossRef] [PubMed]
- Arik, N.; Adam, B.; Akpolat, T.; Haşil, K.; Tabak, S. Serum tumour markers in renal failure. Int. Urol. Nephrol. 1996, 28, 601–604. [Google Scholar] [CrossRef]
- Koratala, A.; Reisinger, N. POCUS for Nephrologists: Basic Principles and a General Approach. Kidney360 2021, 2, 1660–1668. [Google Scholar] [CrossRef] [PubMed]
- Alexiadis, G.; Panagoutsos, S.; Roumeliotis, S.; Stibiris, I.; Markos, A.; Kantartzi, K.; Passadakis, P. Comparison of multiple fluid status assessment methods in patients on chronic hemodialysis. Int. Urol. Nephrol. 2017, 49, 525–532. [Google Scholar] [CrossRef] [PubMed]
- Loutradis, C.; Sarafidis, P.A.; Ekart, R.; Papadopoulos, C.; Sachpekidis, V.; Alexandrou, M.E.; Papadopoulou, D.; Efstratiadis, G.; Papagianni, A.; London, G.; et al. The effect of dry-weight reduction guided by lung ultrasound on ambulatory blood pressure in hemodialysis patients: a randomized controlled trial. Kidney Int. 2019, 95, 1505–1513. [Google Scholar] [CrossRef]
- Gupta, S.; Tomar, D.S. Vexus—the third eye for the intensivist? Indian J. Crit. Care Med. 2020, 24, 746–747. [Google Scholar] [CrossRef]
- Sinha, Arjun D. Agarwal, Rajiv- Can Chronic Volume Overload Be Recognized and Prevented in Hemodialysis Patients? The Pitfalls of the Clinical Examination in Assessing Volume Status. Seminars in Dialysis. 2009, 22, 480–482. [Google Scholar] [CrossRef] [PubMed]
Figure 1.
the combination of available and future methods of OH status diagnosis in CKD patients.
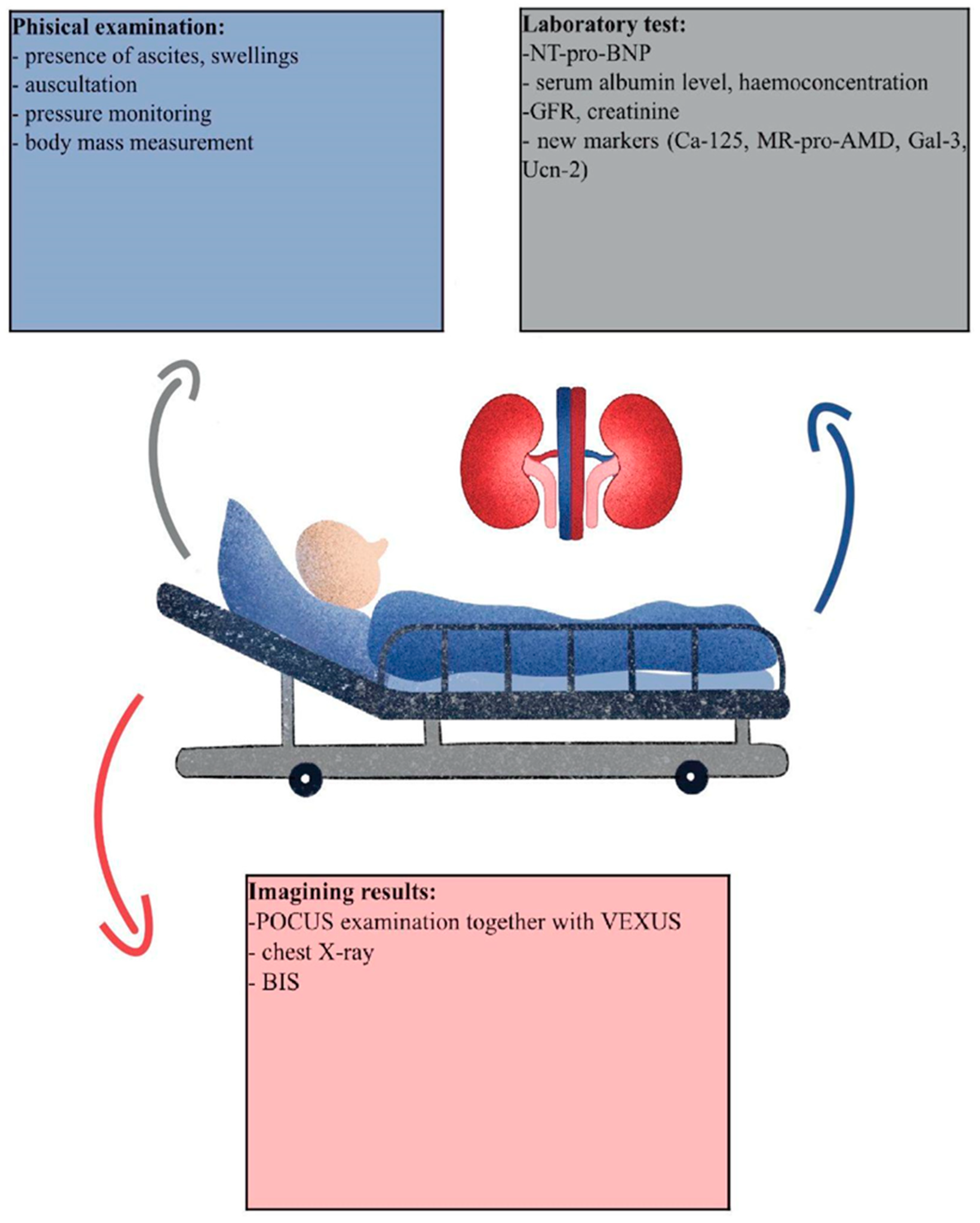
Figure 2.
Research strategy.
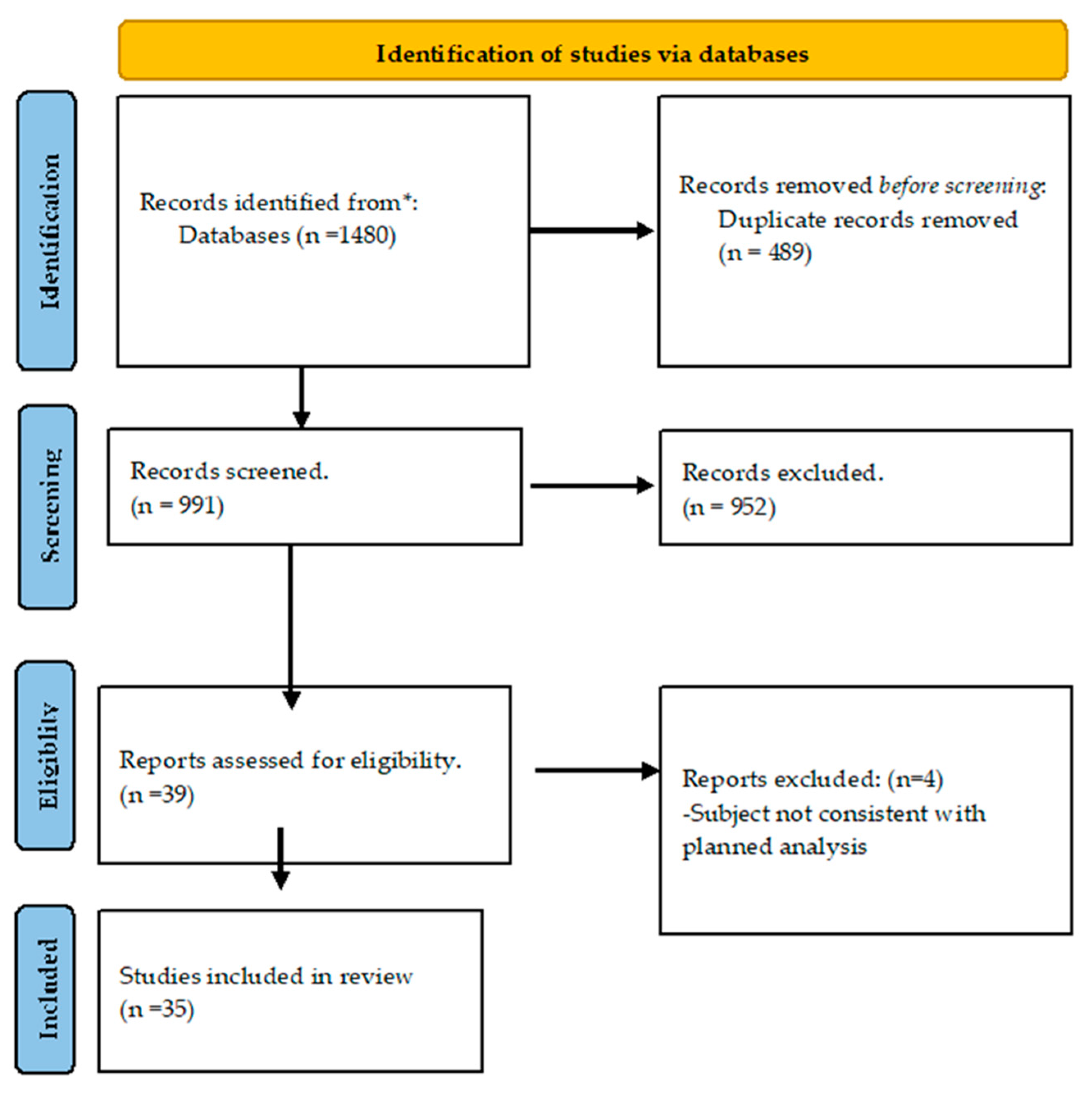

Table 1.
Available methods of estimation of the volume status.
| Name of the test | Includes kidney function? | Includes water balance? | Clinical application | Limitation |
|---|---|---|---|---|
| BIS | No | Yes | Content of ICW and ECW | Not all clinical conditions |
| USG | No | Yes | IVC diameter, VEXUS protocol, IJV?. | Not all structures are always available during the test. Depends on doctors’ experience |
| NT-pro-BNP | No | No | Correlation with OH consequences like heart failure and inflammation process. | Neither kidney nor OH direct marker |
| Ca-125 | No | Yes | Cancer marker, research among the usage in HF and CKD | Novel approach, needs further research |
| ADM/ MR-pro-ADM | No | Yes | Marker of vasodilatation and vessel injury due to fluid overload | Does not correlate in all studies with other available markers, needs further investigation |
| Gal-3 | Yes | No | Marker of renal injury, inflammation and fibrogenesis | Does not correlate directly with OH, but with kidney function, needs further investigation |
| Ucn-2 | No | No | Increases heart dynamic properties, stimulates diuresis and sodium excretion | Needs further investigation as mixed results are obtained |
Table 2.
Markers researched with correlation to hydration status.
| Author | BIS | Creatinine | eGFR | NT-pro-BNP | Ca-125 | USG |
|---|---|---|---|---|---|---|
| Schork et al.[25] | + | +* | + | + | N/M | N/M |
| Hung et al. [17] | + | +* | + | + | N/M | N/M |
| Yilmaz et al. [26] | N/M | N/M | N/M | + | + | + |
| Wijayaratne et al. [27] | + | - | N/M | + | + | N/M |
| Guedes et al. [28] | + | + | N/M | N/M | N/M | + |
| Núñez-Marín et al. [29] | N/M | N/M | N/M | - | + | + (vexus) |
| Beaubien-Souligny [24] | N/M | + | N/M | + | N/M | + |
| Beaubien-Souligny et al. [30] | N/M | + | + | + | N/M | + |
| Argaiz et al. [31] | N/M | + | N/M | + | N/M | + |
| Vega et al. [12] | + | + | N/M | + | N/M | N/M |
+ correlation found. - correlation not found. N/M- marker not mentioned in the paper. * -creatinine/albumin ratio.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



