
Submitted:
23 July 2023
Posted:
24 July 2023
You are already at the latest version
Abstract
Background: Arthroscopic revision rotator cuff repair (ARRCR) is challenging. Biologic strategies seem to be promising. The aim was to evaluate the effectiveness of combination of microfractures of the greater tuberosity, augmentation with collagen patch graft, and platelet concentrate injections in ARRCR.
Methods: A retrospective comparative study was conducted on patients that underwent ARRCR with minimum two-years follow-up. Patients in the augmentation group underwent ARRCR combined with microfractures, collagen patch graft, and postoperative subacromial injections of platelet concentrate. A standard rotator cuff repair was performed in the control group. Primary outcome: Constant Murley score (CMS). Secondary outcomes: disease-specific health-related quality of life by using the Disabilities of the Arm, Shoulder and Hand (DASH) score; assessment of tendon integrity with magnetic resonance at least six months after surgery. Significance was set at p < 0.05.
Results: Forty patients were included. Mean follow-up was 36.2 + 8.7 months. The mean CMS was greater in the augmentation group (p = 0.022). No differences could be found for DASH score. Healing failure rate was higher in the control group (p = 0.002).
Conclusion: Biologic augmentation of ARRCR by combination of microfractures, collagen patch graft and subacromial injections of platelet concentrate is an effective strategy in improving tendon healing rate.
Keywords:
rotator cuff
; retears
; revision
; augmentation
; platelet concentrate
; patch graft
1. Introduction
Revision rotator cuff repair (RCR) represents a real challenge for patients and surgeons as well. A wide range of options has been described, from arthroscopic repair revision up to reverse shoulder replacement. The perfect choice could not rely only on surgeons’ skill and experience, but it must be tailored on potential predictors of outcome. Patient’s age, symptoms and functional demand are greatly relevant to the treatment choice and only symptomatic retears should be considered for revision surgery.
Failure of RCR can be related to mechanical and biologic factors. Mechanical failure is mainly related to surgical technique, while biological failure relies on poor tissue quality. Furthermore, failure can be defined as retear when mechanical stresses exceed structural properties of degenerated tendons or those of poorly differentiated tendon-to-bone junction. In this case, late failure is observed, after biologic fixation occurred. Alternatively, failure can be a consequence of non-healing, which is related to insufficient primary (mechanical) or secondary (biologic) tendon-to-bone fixation. Nevertheless, assessing the cause of failure is rather difficult, because in most cases failure is due to a combination of factors. Therefore, an effective approach in revision RCR should be focused on improving both mechanics and biology of the repair.
Biomechanical studies ensured the effectiveness of technological advances in the use of sutures, tapes and different repair configurations to improve primary tendon-to-bone fixation,[1] in both primary and revision RCR. Similarly, new biotechnologies offer several possible options and combinations for mechanical and biologic enhancement of RCR. As an instance, patch grafts are supposed to implement mechanical features,[2,3] while cell therapies and growth factors (GFs) could improve healing potential of the repaired tendons.[4] Although promising and appealing, these augmentation strategies have high costs, and the lack of evidence on their effectiveness limited their common use, especially as combined treatments.
The purpose of the present paper was to evaluate the effectiveness of combination of a collagen patch graft, microfractures of the greater tuberosity and platelet concentrate (PC) injections in arthroscopic revision RCR (ARRCR).
The hypothesis of the study was that the combined use of tendon augmentation techniques would improve outcome of ARRCR.
2. Materials and Methods
2.1. Study Design
The study was designed as a retrospective comparative study on prospectively collected data from a consecutive cohort of patients. The local IRB and Ethic Committee approved the study protocol. The study was conducted according to the principles of good clinical practice and of the Declaration of Helsinki and its updated version (Tokyo 2004).
2.2. Patients
All patients who underwent ARRCR for symptomatic failure of previous posterosuperior RCR were considered eligible for the study. Patients were enrolled only after accepting the invitation to enter the study and signing a consent form. Symptomatic failure had been diagnosed according to clinical examination and confirmed by magnetic resonance imaging (MRI). Structural integrity had been assessed on MRI and classified according to Sugaya et al.[5]
Revision RCR was indicated when recurrent or persistent symptoms of pain and weakness in elevation and/or external rotation were associated with major structural failure (Sugaya’s type-IV and type-V[5]). Other inclusion criteria were: age older than 18, and minimum 2-year follow-up. Exclusion criteria were: prior surgery to the affected shoulder other than primary and revision RCR, irreparable rotator cuff tear (as diagnosed at the time of revision surgery), rotator-cuff-tear arthropathy (grade >3 according to Hamada et al.[6]), infections, rheumatic or neurologic diseases involving the shoulder girdles and worker’s compensation.
2.3. Treatment
Two groups of patients were investigated, who differed for surgical technique of ARRCR.
All the surgical procedures were performed in beach-chair position under general anesthesia or interscalene block or a combination of both. After initial diagnostic arthroscopy, release of scar adhesions and debridement of tendon edges, tear shape and tendon mobility were assessed. Reparability of rotator cuff was defined as the possibility to reattach the tendon to the medial side of the tendon footprint without excessive tension or extensive tendon releases, such as interval slides. Hardware from previous surgery were removed whenever possible (Figure 1).
Cuff repair was then performed according to tear pattern. A tendon-to-bone repair was accomplished, when possible, by using PEEK knotted suture anchors double-loaded with #2 high-strength sutures (5.5 FT Corkscrew; Arthrex, Naples, FL, USA). Anchors were always placed at the medial edge of the tendon footprint in a single-row configuration (Figure 2).
In L-shaped, reverse-L-shaped, U-shaped and V-shaped tears, tendon-to-bone repair was combined with margin-convergence technique consisting of side-to-side repair with #2 high-strength sutures (FiberWire; Arthex).
In the control group, cortical abrasion of the greater tuberosity was accomplished before anchor placement. In the augmentation group, cortical bone of the greater tuberosity was not abraded; after anchor placement and suture passage and before knot tying, multiple microfractures were performed using an angled arthroscopic awl for small joints onto the footprint area, between and just lateral to the suture anchors (Figure 3).
After knot tying, all the remaining exposed area of the greater tuberosity was vented with multiple microfractures (Figure 4).
Repair was augmented in group 2 by using an extracellular matrix (ECM) made from porcine dermis (DX Reinforcement Matrix; Arthrex). The patch was carefully sized to be placed on the bursal side of the tendon and over the greater tuberosity. Two #2 high-strength sutures (FiberWire) were used to fix the graft to the rotator cuff medially; after tying the knots for medial fixation, the same sutures were passed over the patch and fixed to the greater tuberosity with two knotless PEEK anchors (4.5-mm Pushlock; Arthrex) in a Suture-Bridge configuration (Figure 5).
Three weekly subacromial injections of platelet concentrate (autologous conditioned plasma, ACP® Double-Syringe System, Arthrex) were performed in patients of group 2, starting 7-10 days after surgery.[7]
All patients of both groups underwent the same postoperative treatment. The operated limb was immobilized in a shoulder abduction sling for 6 weeks. Rehabilitation program started four weeks after surgery. The first phase (4 to 8 weeks post-op) focused on recovery of range of motion (ROM); the second phase (8 to 12 weeks post-op) focused on muscle strengthening in closed kinetic chain; the third phase (12 to 16 weeks post-op) consisted of muscle strengthening exercises in open kinetic chain, proprioceptive exercises, and postural rehabilitation of the kinetic chain.
2.4. Outcome Measurements
Patients were clinically evaluated once a month until the third month and then 6 months after surgery. A postoperative MRI was performed at 6-months. Baseline socio-demographic information and medical history were collected from medical records at the time of enrollment.
The primary outcome of the study was the functional assessment of the shoulder by the Constant-Murley score (CMS).[8] The CMS is based on subjective (sleep, work, recreational activities) and objective (range of motion and strength) components, adjusted for age and gender.[9] The summary score ranges from 0 (worst result) to 100 (best result).
Secondary clinical outcome was the assessment of disease-specific health-related quality of life by using the national validated versions of the DASH (Disability of Arm, Shoulder and Hand) questionnaire in its short version (Quick-DASH).[10] This is a self-administered questionnaire that measures physical ability and symptoms of the upper extremity and explores the impact of functional impairment and pain on daily living tasks, as well as social and recreational activities, work, and sleep. Scoring of the questionnaire is based on a metric scale, ranging from 0 points (minimum disability, best result) to 100 points (maximum disability, poorest result).
A further secondary outcome was the evaluation of the structural integrity of the repaired rotator cuff on postoperative MRI. Repair integrity was measured on coronal, sagittal and axial scans on T2-weighted sequences and classified according to the dichotomized classification of Sugaya: repaired cuff was considered healed in Sugaya type I -III or re-torn in case of Sugaya type IV or V.[11]
Primary and secondary clinical outcome measures were collected at follow-up visits by an examiner blinded to participants’ allocation.
2.5. Data Analysis
Sample size calculation was performed using the power analysis software G*Power v. 3.1.9.6. The sample size was calculated according to the primary outcome (CMS) and on the mean postoperative score (60.4 ± 6.7) obtained in a previous study from a population of patients with the same clinical characteristics undergoing ARRCR[12] Based on the literature, the minimal clinically important difference (MCID) in CMS in a population of subjects undergoing rotator cuff surgery is considered to be a change of 10.4 points from baseline[13] Based on these data, the effect size (ES) was calculated equal to 1.55. Using an a priori power analysis model and a two-tailed alternative hypothesis, given an alpha level = 0.05, and a power (1-beta) = 0.95, a minimum sample of 12 cases for each group was calculated.
Propensity score (PS) matching was done for the surgical treatment between standard and augmented ARRCR. A logistic regression model was used to obtain 2 similar groups in terms of age, sex, and follow-up. A 1:1 nearest-neighbor algorithm with a caliper of 1.1 was applied to match patients using their corresponding propensity scores. PS matching was conducted using R (Version 13.0; R Development Core Team).
Data analysis was performed using SPSS Statistics 26 software (IBM, Harmonk, NY, USA).
Descriptive statistics for discrete variables were reported as mean and standard deviation as verified for normal distribution by Shapiro-Wilk test. Otherwise, median and interquartile range (IQR) were considered. Categorical variables were expressed as absolute frequencies and percentages.
Comparison between groups for all continuous variables at baseline and at follow-up was carried out with the Student’s t-test for normally distributed data, otherwise Mann-Whitney U-test was used. Within-group differences (baseline vs follow-up) for continuous variables were analyzed by paired t-test, or by Wilcoxon signed-rank test for data with non-normal distribution. Differences for categorical variables were assessed by chi-squared test. Significance was considered for p values < 0.05.
3. Results
A total of 40 patients (18 males and 22 females), 20 patients per group, were included into the study. Mean age was 63.6 ± 7.3 years. Demographic data of study population are reported in Table 1.
No significant differences between groups were found for baseline characteristics (Table 2).
The mean follow-up was 36.2 + 8.7 months (range, 24-51 months). Significant improvement was observed at follow-up compared to baseline conditions for all the outcome measures in both groups (p<0.001). At comparison between groups, CMS was significantly better in the augmentation group than in the control group. DASH score was lower (better) in the augmentation group, albeit the difference was not significant. Assessment of structural integrity showed a significantly lower failure rate in the augmentation group (20%) than in the control group (55%) (Table 3).
4. Discussion
The main finding of this study is that the combined use of biologic augmentation techniques such as collagen patch graft, microfractures, and platelet concentrate provided better functional and structural outcomes compared to the standard ARRCR. No complications were reported with use of porcine patch grafts.
Patches had been proposed to enhance biomechanics and biology. They are composed of an acellular extracellular matrix (ECM), which is supposed to reduce the load on the repaired tendon so it can be protected during the healing phase, and to induce native tissue to integrate by favoring vascularization and local cellular growth. Biomechanical studies [2,3] showed improvement in initial strength of the construct as well as a recent studies [15,16] supported clinical benefits of patch augmentation in rotator cuff repair, explained by the reduction of retear rate and pain.
Several types of patches are available, like xenograft, allograft and synthetic [17]. Porcine small intestine submucosa patches were the first to be proposed, but they showed very poor results and frequent complications[18], and therefore had been largely abandoned. Conversely, dermal xenograft, like the patch used in the current study, showed encouraging functional and structural results in the primary setting [19,20]. Nevertheless, human dermal allografts and synthetic grafts revealed more promising biomechanical and early clinical results than xenografts[21]. Regardless the type of patches, longer operative time and costs are undeniable disadvantages of this procedure. However, a recent study[22] showed that a graft augmentation may represent a cost-effective procedure even in primary rotator cuff repair.
Microfractures of the greater tuberosity were also performed in the present study to increase the healing potential.[23] Arajwat et al. [24], in their meta-analysis, confirmed that bone marrow stimulation reduces the retear rate. A recent randomized clinical study[25] conducted on 69 patients who underwent a rotator cuff repair showed that small and deep bone vents (nanofractures) of the greater tuberosity halves the retear rate at twelve months follow-up.
Last biologic strategy we used to maximize tendon healing was the use of platelet concentrate.
ACP was injected 7 -10 days after surgery for two main reasons: 1) to avoid a possible dilution or washout of its effect, which may occur with arthroscopic fluid lavage[26]; 2) to allow a potentially prolonged upregulation of growth factors involved in the tendon healing cascade. Animal studies on rats have shown that application of platelet-derived growth factors at day 7 have a more pronounced effect on tendon cellular maturation and biomechanical strength than earlier application[27,28]. This is probably due to the fact that the inflammatory phase (capillary proliferation and collagen protein production) reaches its peak 10 days after repair.[29]
The role of platelet-derived GFs in rotator cuff surgery is still matter of debate. However, a recent systematic review of meta-analysis[4] showed that they are effective in reducing retears, improving functional outcome scores and reducing short-term pain. Thirteen meta-analyses were included. The authors explained that there is a conflict of conclusions between early and later studies: the former reported poorer results than the latter. Later meta-analysis seemed to have appropriate numbers, therefore the authors concluded that platelet concentrate is recommended for augmenting rotator cuff repair, and differences in preparation, application, and consistency do not affect the outcomes.
The added value of the present study relies in the integrated approach of three different biologic augmentation strategies for revision rotator cuff repair. The rationale of our treatment consisted of a combination GFs that may stimulate proliferation and differentiation of multipotent bone marrow cells attracted at the tendon repair site through bone vents, and a scaffold that potentially provide support for in-situ seeding of bone marrow cells while protecting tendon from retear during early postoperative period.
Only few case series without control group attempted an integrated approach in revision setting by use of collagen patch enriched with platelet-rich plasma (PRP) and bone marrow aspirate concentrate (BMAC) from the proximal humerus.[30,31,32] Overall functional improvement and pain reduction was reported, although one study reported up to 40% revision rate.[32] Other two studies[30,31] reported similar results. Particularly, 45% of patients achieved the minimal clinically important difference (MCID), 41% the substantial clinical benefit (SCB), and 32% reached or exceeded the patient-acceptable symptomatic state (PASS) criteria for the ASES score. Although these studies do not seem to be encouraging, it must be noticed that structural failure rate in revision of large recurrent rotator cuff retears by standard arthroscopic repair has been reported varying from 36% to 90%[33,34,35]. Conversely, the present study showed that patients who underwent a similar integrated approach experienced successful healing rate approximating 80% with significantly better functional outcome compared to a standard RCR. Better functional outcome could be explained by the fact that an intact RCR maintains at least the preoperative state of fatty infiltration and muscle atrophy [36]. Skoff et al.[35] proposed revision rotator cuff reconstruction using a bridging graft composed of autogenous long head of biceps tendon (LHBT) saturated with concentrated autologous bone marrow from iliac crest in 25 patients. The authors showed functional improvement and 91% structural integrity at a mean follow-up of 68 months. The idea to use an autograft, such as LHBT, is surely easy and cost-effective and augmentation with LHBT in primary RCR has been reported with the aim to reduce retear risk.[37] However, in revision RCR, the LHBT is usually no longer available to be used as scaffold augmentation and an alternative option must be considered.
The study has some limitations. First, the retrospective design impairs its external validity; further, the sample size is inadequate for a stratified analysis according to potential predictors of outcome, such as patient’s age, tear size, and alterations of rotator cuff muscles (fatty infiltration and muscle atrophy). Finally, single short-term follow-up at minimum 2 years could not provide sufficient information regarding possible deterioration of anatomic and functional outcomes over time.
5. Conclusions
Biologic augmentation of revision RCR by combination of microfractures, collagen patch graft and subacromial injections of platelet concentrate is an effective strategy in improving tendon healing rate.
Author Contributions
Conceptualization, Maristella Francesca Saccomanno and Giuseppe Milano; Formal analysis, Giuseppe Milano; Investigation, Andrea Bergomi and Andrea Pratobevera; Methodology, Marco Paderno and Giuseppe Milano; Supervision, Giuseppe Milano; Writing – original draft, Alessandro Colosio; Writing – review & editing, Maristella Francesca Saccomanno and Giuseppe Milano.
Funding
This research received no external funding
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study
Conflicts of Interest
Giuseppe Milano reports a relationship with Arthrex Inc that includes: consulting or advisory. The other authors declare no conflict of interest.
References
- Shi, B.Y.; Diaz, M.; Binkley, M.; McFarland, E.G.; Srikumaran, U. Biomechanical Strength of Rotator Cuff Repairs: A Systematic Review and Meta-Regression Analysis of Cadaveric Studies. Am. J. Sports Med. 2019, 47, 1984–1993. [Google Scholar] [CrossRef]
- Ely, E.E.; Figueroa, N.M.; Gilot, G.J. Biomechanical Analysis of Rotator Cuff Repairs with Extracellular Matrix Graft Augmentation. Orthopedics 2014, 37, 608–614. [Google Scholar] [CrossRef]
- Omae, H.; Steinmann, S.P.; Zhao, C.; Zobitz, M.E.; Wongtriratanachai, P.; Sperling, J.W.; An, K.-N. Biomechanical Effect of Rotator Cuff Augmentation with an Acellular Dermal Matrix Graft: A Cadaver Study. Clin. Biomech. Bristol Avon 2012, 27, 789–792. [Google Scholar] [CrossRef] [PubMed]
- Ahmad, Z.; Ang, S.; Rushton, N.; Harvey, A.; Akhtar, K.; Dawson-Bowling, S.; Noorani, A. Platelet-Rich Plasma Augmentation of Arthroscopic Rotator Cuff Repair Lowers Retear Rates and Improves Short-Term Postoperative Functional Outcome Scores: A Systematic Review of Meta-Analyses. Arthrosc. Sports Med. Rehabil. 2022, 4, e823–e833. [Google Scholar] [CrossRef] [PubMed]
- Sugaya, H.; Maeda, K.; Matsuki, K.; Moriishi, J. Functional and Structural Outcome after Arthroscopic Full-Thickness Rotator Cuff Repair: Single-Row versus Dual-Row Fixation. Arthroscopy 2005, 21, 1307–1316. [Google Scholar] [CrossRef]
- Hamada, K.; Fukuda, H.; Mikasa, M.; Kobayashi, Y. Roentgenographic Findings in Massive Rotator Cuff Tears. A Long-Term Observation. Clin. Orthop. 1990, 92–96. [Google Scholar] [CrossRef]
- Snow, M.; Hussain, F.; Pagkalos, J.; Kowalski, T.; Green, M.; Massoud, S.; James, S. The Effect of Delayed Injection of Leukocyte-Rich Platelet-Rich Plasma Following Rotator Cuff Repair on Patient Function: A Randomized Double-Blind Controlled Trial. Arthroscopy 2020, 36, 648–657. [Google Scholar] [CrossRef]
- Constant, C.R.; Murley, A.H. A Clinical Method of Functional Assessment of the Shoulder. Clin. Orthop. 1987, 160–164. [Google Scholar] [CrossRef]
- Yian, E.H.; Ramappa, A.J.; Arneberg, O.; Gerber, C. The Constant Score in Normal Shoulders. J. Shoulder Elbow Surg. 2005, 14, 128–133. [Google Scholar] [CrossRef] [PubMed]
- Padua, R.; Padua, L.; Ceccarelli, E.; Romanini, E.; Zanoli, G.; Amadio, P.C.; Campi, A. Italian Version of the Disability of the Arm, Shoulder and Hand (DASH) Questionnaire. Cross-Cultural Adaptation and Validation. J. Hand Surg. Edinb. Scotl. 2003, 28, 179–186. [Google Scholar] [CrossRef] [PubMed]
- Neyton, L.; Godenèche, A.; Nové-Josserand, L.; Carrillon, Y.; Cléchet, J.; Hardy, M.B. Arthroscopic Suture-Bridge Repair for Small to Medium Size Supraspinatus Tear: Healing Rate and Retear Pattern. Arthroscopy 2013, 29, 10–17. [Google Scholar] [CrossRef]
- Piasecki, D.P.; Verma, N.N.; Nho, S.J.; Bhatia, S.; Boniquit, N.; Cole, B.J.; Nicholson, G.P.; Romeo, A.A. Outcomes after Arthroscopic Revision Rotator Cuff Repair. Am. J. Sports Med. 2010, 38, 40–46. [Google Scholar] [CrossRef]
- Kukkonen, J.; Kauko, T.; Vahlberg, T.; Joukainen, A.; Aärimaa, V. Investigating Minimal Clinically Important Difference for Constant Score in Patients Undergoing Rotator Cuff Surgery. J. Shoulder Elbow Surg. 2013, 22, 1650–1655. [Google Scholar] [CrossRef] [PubMed]
- Cvetanovich, G.L.; Gowd, A.K.; Liu, J.N.; Nwachukwu, B.U.; Cabarcas, B.C.; Cole, B.J.; Forsythe, B.; Romeo, A.A.; Verma, N.N. Establishing Clinically Significant Outcome after Arthroscopic Rotator Cuff Repair. J. Shoulder Elbow Surg. 2019, 28, 939–948. [Google Scholar] [CrossRef] [PubMed]
- de Andrade, A.L.L.; Garcia, T.A.; Brandão, H. de S.; Sardeli, A.V.; Mouraria, G.G.; Belangero, W.D. Benefits of Patch Augmentation on Rotator Cuff Repair: A Systematic Review and Meta-Analysis. Orthop. J. Sports Med. 2022, 10, 23259671211071144. [Google Scholar] [CrossRef]
- Kim, K.-T.; Kim, G.-H.; Cha, D.-H.; Lee, J.-H.; Lee, Y.-B. A Comparison of Clinical Outcomes in Rotator Cuff Re-Tear Patients Who Had Either an Arthroscopic Primary Repair or Arthroscopic Patch Augmentation for Large-to-Massive Rotator Cuff Tears. Diagn. Basel Switz. 2023, 13, 1961. [Google Scholar] [CrossRef]
- Chalmers, P.N.; Tashjian, R.Z. Patch Augmentation in Rotator Cuff Repair. Curr. Rev. Musculoskelet. Med. 2020, 13, 561–571. [Google Scholar] [CrossRef] [PubMed]
- Sclamberg, S.G.; Tibone, J.E.; Itamura, J.M.; Kasraeian, S. Six-Month Magnetic Resonance Imaging Follow-up of Large and Massive Rotator Cuff Repairs Reinforced with Porcine Small Intestinal Submucosa. J. Shoulder Elbow Surg. 2004, 13, 538–541. [Google Scholar] [CrossRef]
- Gupta, A.K.; Hug, K.; Berkoff, D.J.; Boggess, B.R.; Gavigan, M.; Malley, P.C.; Toth, A.P. Dermal Tissue Allograft for the Repair of Massive Irreparable Rotator Cuff Tears. Am. J. Sports Med. 2012, 40, 141–147. [Google Scholar] [CrossRef] [PubMed]
- Consigliere, P.; Bernasconi, A.; Dimock, R.; Narvani, A.A. Clinical Outcomes and Structural Integrity Rate of Arthroscopic Augmented Rotator Cuff Repairs Using Extracellular Porcine Matrix Patch. Shoulder Elb. 2022, 14, 38–51. [Google Scholar] [CrossRef]
- Karuppaiah, K.; Sinha, J. Scaffolds in the Management of Massive Rotator Cuff Tears: Current Concepts and Literature Review. EFORT Open Rev. 2019, 4, 557–566. [Google Scholar] [CrossRef] [PubMed]
- Quigley, R.; Verma, N.; Evuarherhe, A.; Cole, B.J. Rotator Cuff Repair with Graft Augmentation Improves Function, Decreases Revisions, and Is Cost-Effective. Arthroscopy 2022, 38, 2166–2174. [Google Scholar] [CrossRef] [PubMed]
- Milano, G.; Saccomanno, M.F.; Careri, S.; Taccardo, G.; De Vitis, R.; Fabbriciani, C. Efficacy of Marrow-Stimulating Technique in Arthroscopic Rotator Cuff Repair: A Prospective Randomized Study. Arthroscopy 2013, 29, 802–810. [Google Scholar] [CrossRef]
- Ajrawat, P.; Dwyer, T.; Almasri, M.; Veillette, C.; Romeo, A.; Leroux, T.; Theodoropoulos, J.; Nauth, A.; Henry, P.; Chahal, J. Bone Marrow Stimulation Decreases Retear Rates after Primary Arthroscopic Rotator Cuff Repair: A Systematic Review and Meta-Analysis. J. Shoulder Elbow Surg. 2019, 28, 782–791. [Google Scholar] [CrossRef] [PubMed]
- Ruiz Ibán, M.A.; Sanchez Alepuz, E.; Diaz Heredia, J.; Hachem, A.-I.; Ezagüi Bentolila, L.; Calvo, A.; Verdú, C.; de Rus Aznar, I.; Soler Romagosa, F. Footprint Preparation with Nanofractures in a Supraspinatus Repair Cuts in Half the Retear Rate at 1-Year Follow-up. A Randomized Controlled Trial. Knee Surg. Sports Traumatol. Arthrosc. 2021, 29, 2249–2256. [Google Scholar] [CrossRef]
- Wang, A.; McCann, P.; Colliver, J.; Koh, E.; Ackland, T.; Joss, B.; Zheng, M.; Breidahl, B. Do Postoperative Platelet-Rich Plasma Injections Accelerate Early Tendon Healing and Functional Recovery after Arthroscopic Supraspinatus Repair? A Randomized Controlled Trial. Am. J. Sports Med. 2015, 43, 1430–1437. [Google Scholar] [CrossRef] [PubMed]
- Chan, B.P.; Fu, S.C.; Qin, L.; Rolf, C.; Chan, K.M. Supplementation-Time Dependence of Growth Factors in Promoting Tendon Healing. Clin. Orthop. 2006, 448, 240–247. [Google Scholar] [CrossRef]
- Kajikawa, Y.; Morihara, T.; Sakamoto, H.; Matsuda, K.; Oshima, Y.; Yoshida, A.; Nagae, M.; Arai, Y.; Kawata, M.; Kubo, T. Platelet-Rich Plasma Enhances the Initial Mobilization of Circulation-Derived Cells for Tendon Healing. J. Cell. Physiol. 2008, 215, 837–845. [Google Scholar] [CrossRef]
- Galatz, L.M.; Sandell, L.J.; Rothermich, S.Y.; Das, R.; Mastny, A.; Havlioglu, N.; Silva, M.J.; Thomopoulos, S. Characteristics of the Rat Supraspinatus Tendon during Tendon-to-Bone Healing after Acute Injury. J. Orthop. Res. Off. Publ. Orthop. Res. Soc. 2006, 24, 541–550. [Google Scholar] [CrossRef]
- Berthold, D.P.; Garvin, P.; Mancini, M.R.; Uyeki, C.L.; LeVasseur, M.R.; Mazzocca, A.D.; Voss, A. Arthroscopic Rotator Cuff Repair with Biologically Enhanced Patch Augmentation. Oper. Orthopadie Traumatol. 2022, 34, 4–12. [Google Scholar] [CrossRef] [PubMed]
- Muench, L.N.; Kia, C.; Berthold, D.P.; Uyeki, C.; Otto, A.; Cote, M.P.; McCarthy, M.B.; Beitzel, K.; Arciero, R.A.; Mazzocca, A.D. Preliminary Clinical Outcomes Following Biologic Augmentation of Arthroscopic Rotator Cuff Repair Using Subacromial Bursa, Concentrated Bone Marrow Aspirate, and Platelet-Rich Plasma. Arthrosc. Sports Med. Rehabil. 2020, 2, e803–e813. [Google Scholar] [CrossRef]
- Voss, A.; McCarthy, M.B.; Bellas, N.; Kellner, R.; Beitzel, K.; Dyrna, F.; Imhoff, A.B.; Mazzocca, A.D.; Muench, L.N.; Berthold, D.P. Significant Improvement in Shoulder Function and Pain in Patients Following Biologic Augmentation of Revision Arthroscopic Rotator Cuff Repair Using an Autologous Fibrin Scaffold and Bone Marrow Aspirate Derived From the Proximal Humerus. Arthrosc. Sports Med. Rehabil. 2021, 3, e1819–e1825. [Google Scholar] [CrossRef] [PubMed]
- Azar, M.; Van der Meijden, O.; Pireau, N.; Chelli, M.; Gonzalez, J.-F.; Boileau, P. Arthroscopic Revision Cuff Repair: Do Tendons Have a Second Chance to Heal? J. Shoulder Elbow Surg. 2022, 31, 2521–2531. [Google Scholar] [CrossRef] [PubMed]
- Kim, S.C.; Shim, S.B.; Kim, W.J.; Yoo, J.C. Preoperative Rotator Cuff Tendon Integrity, Tear Size, and Muscle Atrophy and Fatty Infiltration Are Associated with Structural Outcomes of Arthroscopic Revision Rotator Cuff Repair. Knee Surg. Sports Traumatol. Arthrosc. 2022, 30, 2029–2038. [Google Scholar] [CrossRef] [PubMed]
- Skoff, H. Follow-up on a Biological Revision Technique for Large, Recurrent, Retracted, Rotator Cuff Tears. J. Am. Acad. Orthop. Surg. 2022, 30, e487–e494. [Google Scholar] [CrossRef]
- Lacheta, L.; Siebenlist, S.; Scheiderer, B.; Beitzel, K.; Woertler, K.; Imhoff, A.B.; Buchmann, S.; Willinger, L. Intact Revision Rotator Cuff Repair Stabilizes Muscle Atrophy and Fatty Infiltration after Minimum Follow up of Two Years. BMC Musculoskelet. Disord. 2023, 24, 515. [Google Scholar] [CrossRef]
- Milano, G.; Marchi, G.; Bertoni, G.; Vaisitti, N.; Galli, S.; Scaini, A.; Saccomanno, M.F. Augmented Repair of Large to Massive Delaminated Rotator Cuff Tears With Autologous Long Head of the Biceps Tendon Graft: The Arthroscopic “Cuff-Plus” Technique. Arthrosc. Tech. 2020, 9, e1683–e1688. [Google Scholar] [CrossRef] [PubMed]
Figure 1.
Right shoulder: scope in the posterior portal. Hardware removal attempt: a metallic anchor was used during the primary repair. A nitinol wire is used to secure the anchor (a), before removing it (b).
Figure 1.
Right shoulder: scope in the posterior portal. Hardware removal attempt: a metallic anchor was used during the primary repair. A nitinol wire is used to secure the anchor (a), before removing it (b).
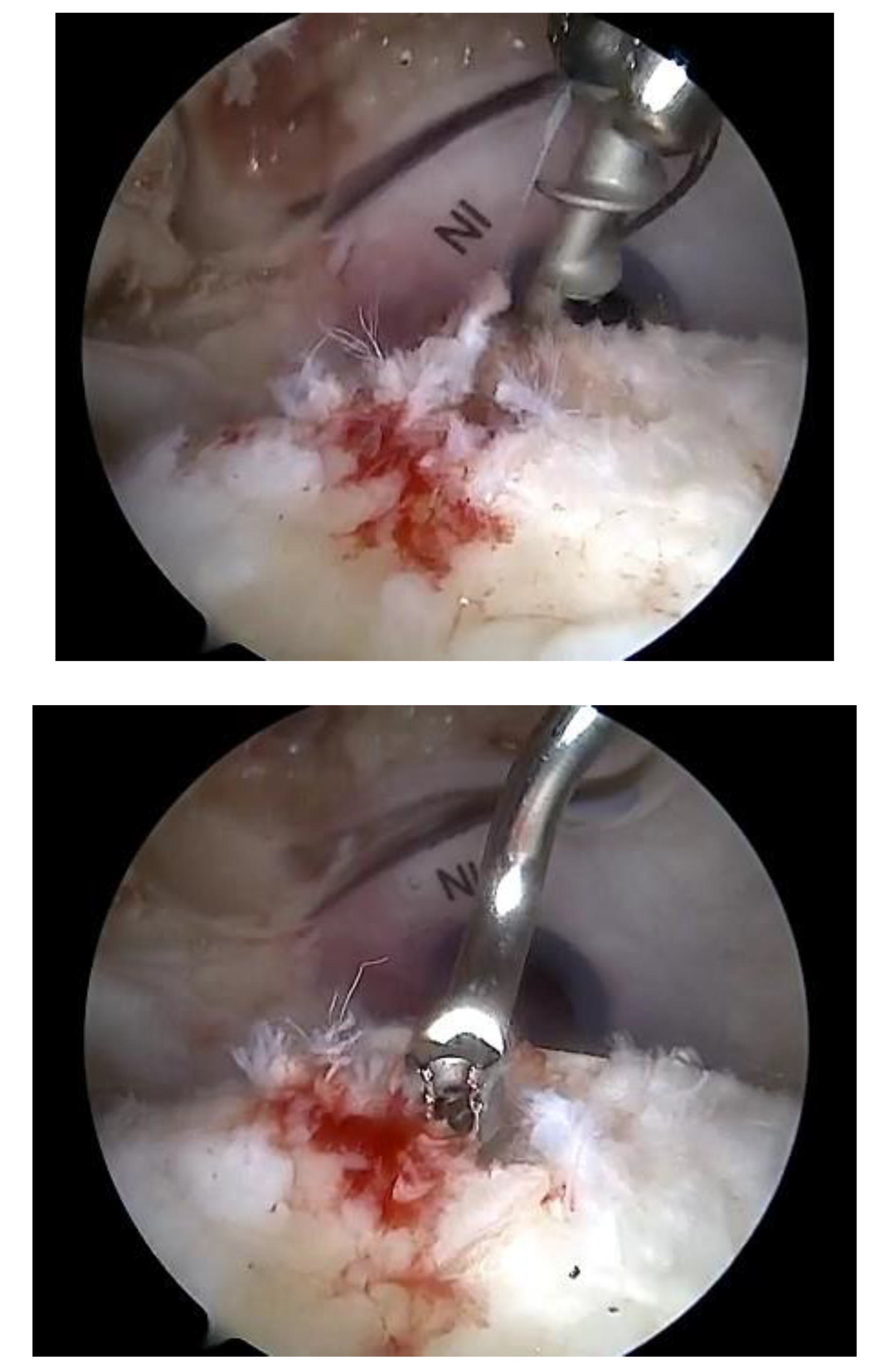
Figure 2.
Right shoulder: scope in the lateral portal. Anchor placement. A PEEK knotted suture anchors double-loaded with #2 high-strength sutures was placed at the medial edge of the tendon footprint.
Figure 2.
Right shoulder: scope in the lateral portal. Anchor placement. A PEEK knotted suture anchors double-loaded with #2 high-strength sutures was placed at the medial edge of the tendon footprint.

Figure 3.
Right shoulder: scope in the lateral portal. after anchor placement and suture passage and before knot tying, multiple microfractures were performed using an angled arthroscopic awl for small joints onto the footprint area, between and just lateral to the suture anchors.
Figure 3.
Right shoulder: scope in the lateral portal. after anchor placement and suture passage and before knot tying, multiple microfractures were performed using an angled arthroscopic awl for small joints onto the footprint area, between and just lateral to the suture anchors.
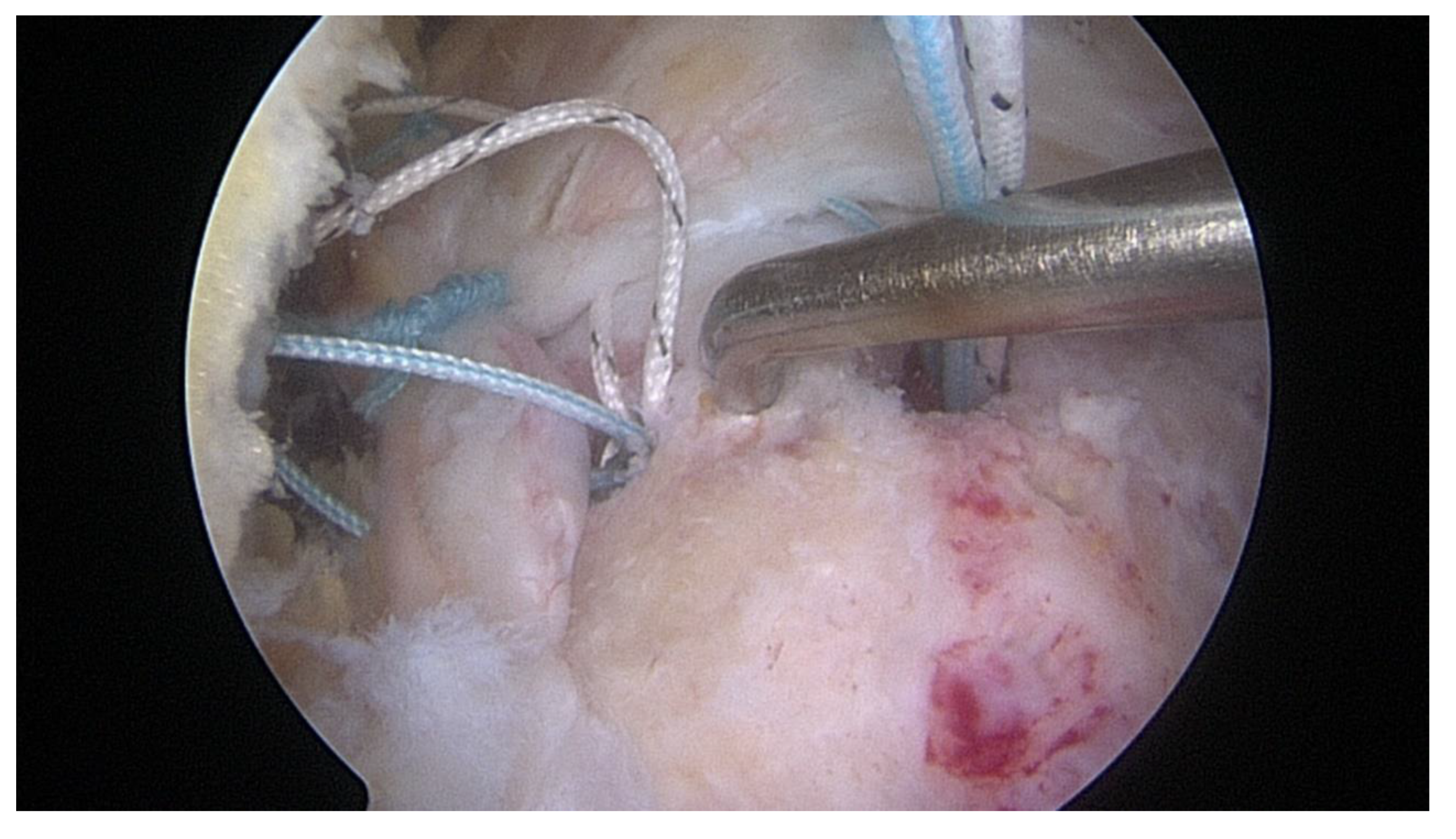
Figure 4.
Right shoulder: scope in the posterior portal. After knot tying, all the remaining exposed area of the greater tuberosity was vented with multiple microfractures. The ECM patch graft was then applied on top to cover the entire area.
Figure 4.
Right shoulder: scope in the posterior portal. After knot tying, all the remaining exposed area of the greater tuberosity was vented with multiple microfractures. The ECM patch graft was then applied on top to cover the entire area.
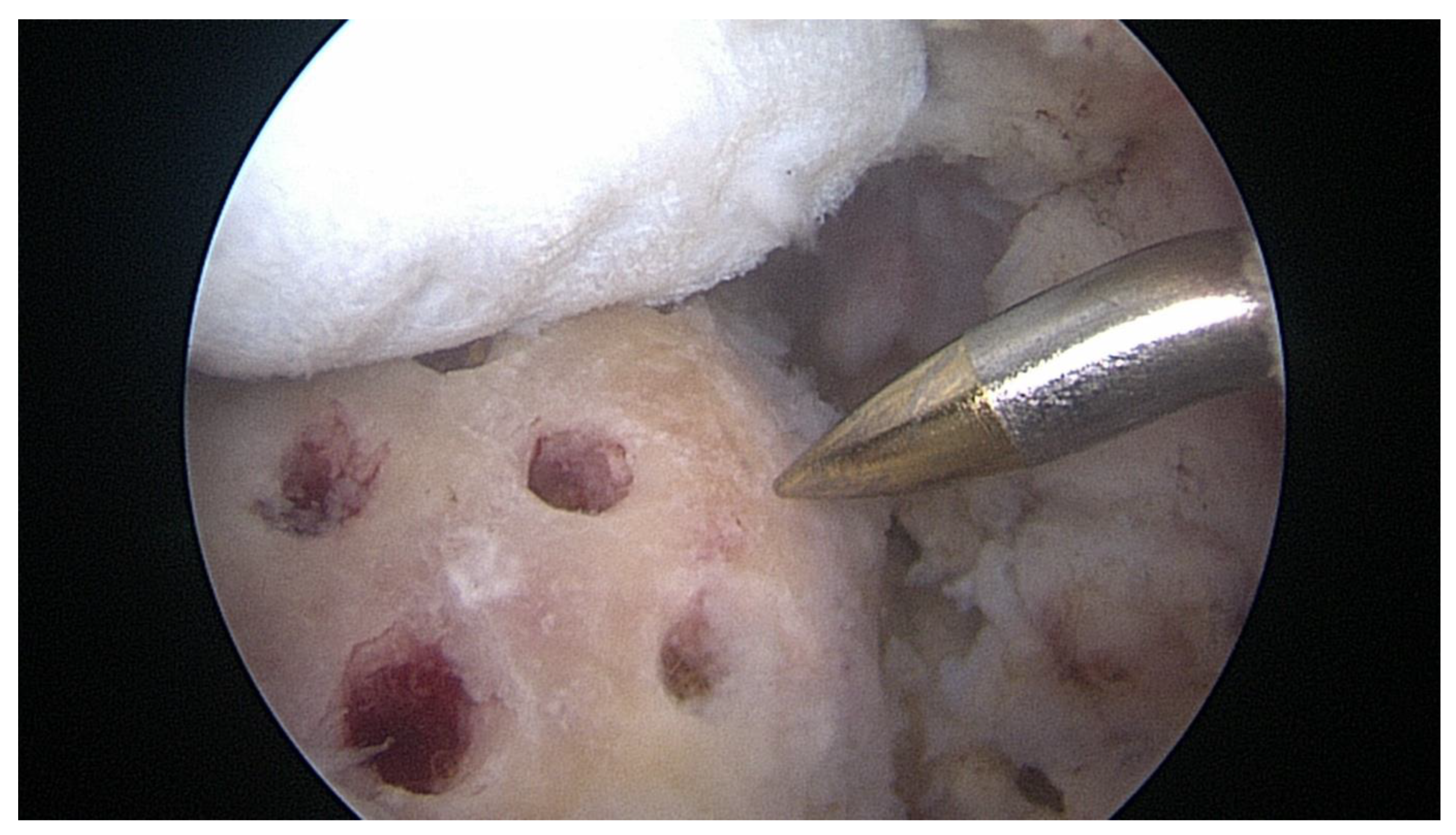
Figure 5.
Right shoulder: scope in the lateral portal. Final view. The ECM patch graft was fixed over the RCR in a suture bridge configuration.
Figure 5.
Right shoulder: scope in the lateral portal. Final view. The ECM patch graft was fixed over the RCR in a suture bridge configuration.


Table 1.
Demographic data of the study population.
| Variables | Overall | |
|---|---|---|
| N=40 | ||
| Gender | Male, N (%) | 18 (45%) |
| Female, N (%) | 22 (55%) | |
| Dominance | No, N (%) | 10 (25%) |
| Yes, N (%) | 30 (75%) | |
| Type of work | Manual, N (%) | 18 (45%) |
| Sedentary, N (%) | 22 (55%) | |
| Tear size | Large, N (%) | 29 (72.5%) |
| Massive, N (%) | 11 (27.5%) | |
Table 2.
Differences between groups for baseline characteristics.
| Variables | Controls | Augment | p | |
|---|---|---|---|---|
| N=20 | N=20 | |||
| Age (years) | Mean + SD | 63.8 + 7.3 | 63.3 + 7.5 | 0.832 |
| Gender | Male, N (%) | 10 (50%) | 8 (40%) | 0.376 |
| Female, N (%) | 10 (50%) | 12 (60%) | ||
| Dominance | No, N (%) | 4 (20%) | 6 (30%) | 0.358 |
| Yes, N (%) | 16 (80%) | 14 (70%) | ||
| Type of work | Manual, N (%) | 7 (35%) | 11 (55%) | 0.170 |
| Sedentary, N (%) | 13 (65%) | 9 (45%) | ||
| Tear size | Large, N (%) | 16 (80%) | 13 (65%) | 0.240 |
| Massive, N (%) | 4 (20%) | 7 (35%) | ||
| Follow-up (months) | Mean + SD | 36.2 + 9.1 | 36.1 + 8.6 | 0.986 |
| Constant score | Mean + SD | 47.9 + 12.7 | 48.7 + 18.6 | 0.873 |
| Quick-DASH | Mean + SD | 59.8 + 18.3 | 57.4 + 9.9 | 0.610 |
Table 3.
Differences between groups for clinical and structural outcomes.
| Variables | Controls | Augment | p | |
|---|---|---|---|---|
| N=20 | N=20 | |||
| Constant score | Mean + SD | 80.7 + 16.6 | 91.5 + 11.5 | 0.022* |
| Quick-DASH | Mean + SD | 28.6 + 21.6 | 20.1 + 17.4 | 0.178 |
| Tendon healing | Yes, N (%) | 6 (30%) | 16 (80%) | 0.002* |
| No, N (%) | 14 (70%) | 4 (20%) | ||
*Statistically significant difference.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



