
Submitted:
19 July 2023
Posted:
21 July 2023
You are already at the latest version
Abstract
Abdominal injuries in children caused by guns are a rare clinical entity globally. But, in countries with undefined legal regulations and in the war zones urban violence is a great social problem among older children and adolescents. This manuscript provides details regarding two cases of severe gunshot injuries in young children. The injuries were very complicated and included damage to the parenchymatous and hollow organs as well as major blood vessels. The clinical presentation on admission was very serious and dramatic, but the patients survived. However, one patient developed numerous complications that required repeated surgical interventions and long treatment. The article provides a detailed description of injuries and how to treat them. Patient care requires a multidisciplinary approach, and the initial decision on further treatment depends on the patient's hemodynamic stability.
Keywords:
gunshot wounds
; children
Introduction
Abdominal injuries in children caused by guns are a rare clinical entity globally. But, in countries with undefined legal regulations and in war zones urban violence is a great social problem among older children and adolescents [1]. Abdominal injuries can occur as a result of blunt or penetrating trauma. In children, blunt force injuries are much more likely, in approximately 85% of children [2].
Most penetrating injuries are caused by firearms or various types of daggers. According to literature data, more than 90% of gunshot injuries in older children (above 12 years) and adolescents are caused by a gun [3]. According to localization, the most common affected sites are the gastrointestinal tract, liver, major blood vessels, kidneys, and spleen [4].
Case Reports
Case Report 1
A 16-year-old patient was transported by ambulance because of an abdominal injury caused by a firearm, shot from a gun. The patient was conscious, oriented, afebrile, tachycardic, and hypotensive with a tension of 80/40 mmHg. The skin was extremely pale and discolored. Physical examination recorded gunshot wounds, the entry wound was located in the right para umbilical and the exit wound was in the left sacral region.
The patient was clinical, laboratory, and ultrasound examined and immediately transferred to the intensive care unit. Laboratory values on admission were: red blood cells 2.1, leucocytes 15.6, Hemoglobin 54, hematocrit 19, and platelets 89. Ultrasound findings (FAST) revealed the presence of free fluid in the abdomen without lesions of solid organs. After emergency resuscitation and blood transfusion, urgent surgical intervention was done. The patient's condition was very poor and additional diagnostic procedures will contribute to faster deterioration of the patient.
During the operation, multiple injuries of the mesocolon transversum (Figure 1a,b) and mesentery of the small intestine, laceration of the D3 duodenum as well as retroperitoneal hematoma at the level of the femoral fossa on the right were recorded. After the opening of the retroperitoneum, injuries of the v.cava inferior in the form of a 2cm long laceration and a 3,5 cm long laceration of the right v.iliaca communis were recorded (Figure 1c). The primary suture of injured blood vessels was done. The duodenum was then mobilized by Koher's maneuver to find the laceration of the duodenum in the D3 area below the ampulla of Water (Figure 1d), and the primary suture of the duodenum was done (Figure 1e). Injuries of the mesocolon transversum and mesentery of the small intestine are treated with single sutures. Two drains were placed, the first one in the right paracolic, and the second one in the recto-vesical space (Figure 1f). The patient spent 5 days in the intensive care unit, treated with triple antibiotic therapy, analgesics, and proton pump inhibitors. On the sixth and seventh postoperative days, the drains were removed. The passage of the gastrointestinal system was established on the third postoperative day, and the 10th day after the intervention he was discharged from the hospital. During two controls, color Doppler examinations, blood vessels were normal. A month after the surgical intervention, a gastroscopy was performed, and the examination was normal.
Case Report 2
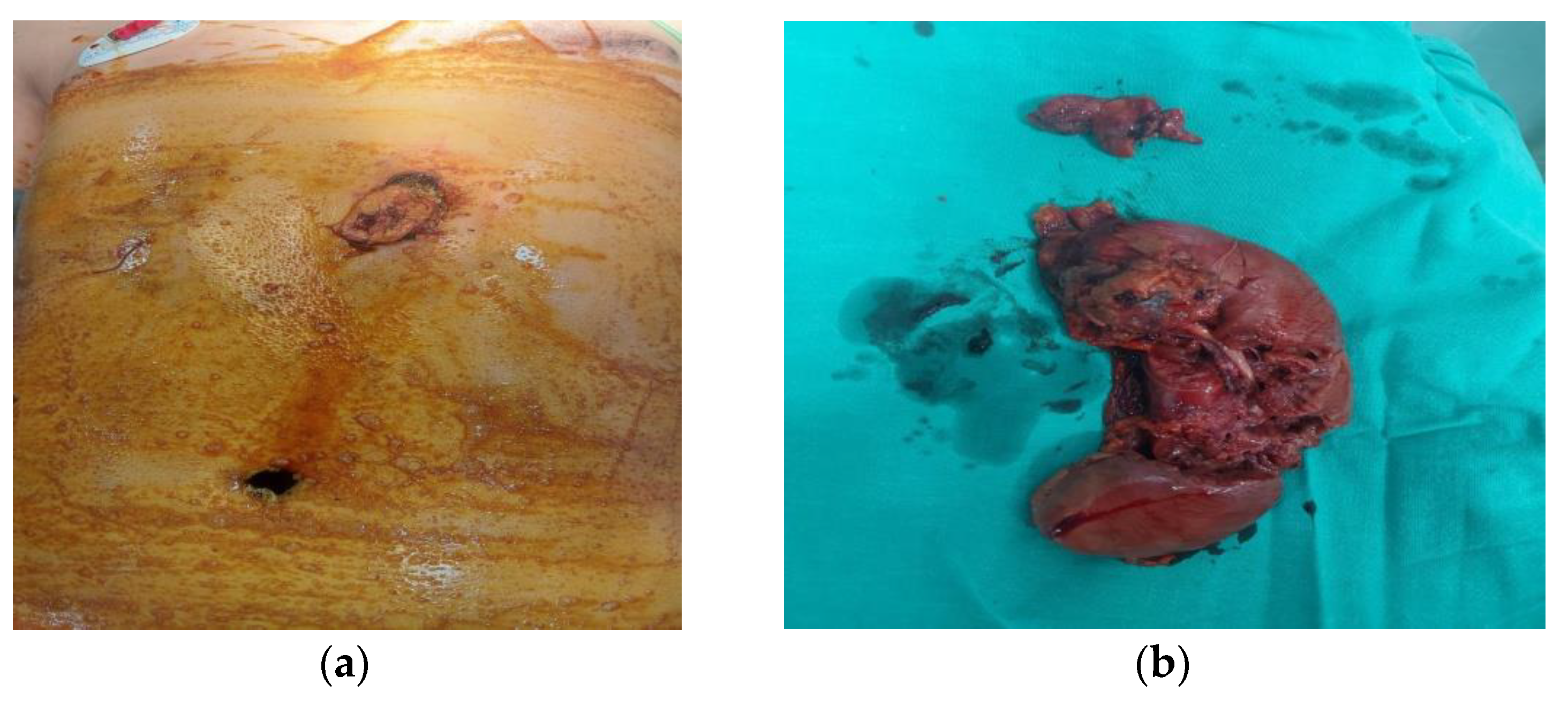
A 12-year-old patient was brought to the hospital with a penetrating abdominal injury inflicted by an automatic rifle. The patient was confused, with no verbal communication, extremely pale, and drenched in a cold sweat. Physical examination recorded an entry wound in the epigastric area left of the xiphoid, and an exit wound in the left paravertebral area (Figure 2a).
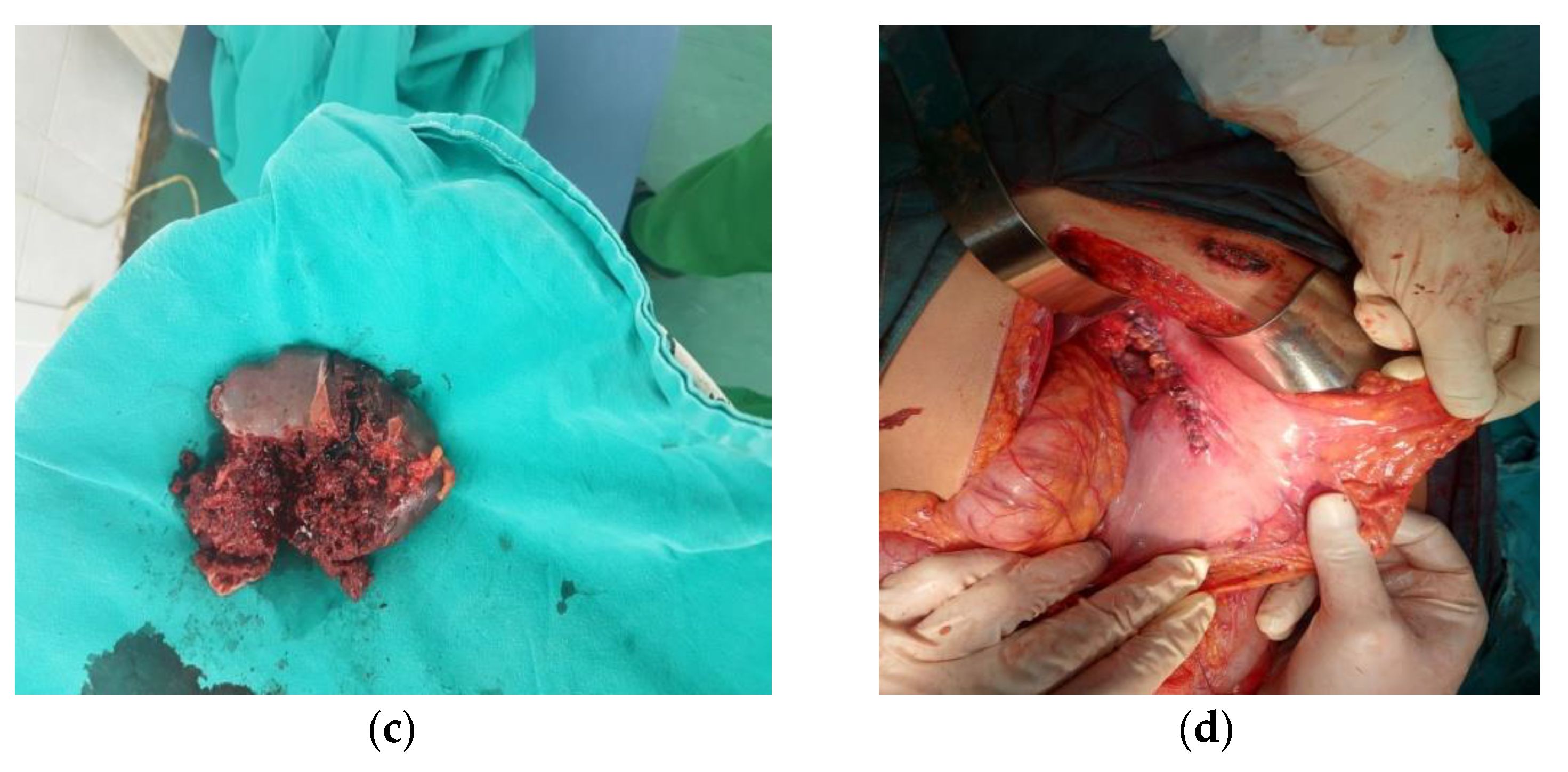
The patient was transferred to the intensive care unit, blood was taken for laboratory analysis and blood tests. The patient was extremely hypotensive with a blood pressure of 70/30 mm Hg and a surgeon decided to do an urgent surgical intervention only after transfusion of 2 units of blood. After opening the abdomen, the following injuries were recorded: injury of the anterior and posterior walls of the stomach in the length of 6cm on the front wall and about 15cm on the back wall, a complete transection of the pancreas and conquassation of two-thirds of the pancreas in the body and tail area, conquassation of the spleen with transsection of the splenic vein and artery (Figure 2b), lesion of the left kidney with transection of the renal vein and artery (Figure 2c), transsection of the left ureter, lesion of the left lobe of the liver and complete transection of the left m.quadratus lumborum. About 1,800 ml of blood was evacuated from the abdominal cavity. Due to complete devascularisation, a splenectomy was performed, followed by a nephrectomy with ureterectomy, partial pancrectomy of the distal part of the pancreas, suture of the head of the pancreas, and stomach suture (Fig,2d). Drains were placed in retroperitoneal, left paracolic, and rectovesical space. During the surgical intervention, the patient received six units of blood. After the surgery, he was transferred to the intensive care unit. His condition was stable until the nineteenth postoperative day when he deteriorated rapidly due to a massive abdominal hemorrhage due hemorrhagic pancreatitis, located at the site of the confluence of the left renal artery in the aorta. During the second operation, three drains were placed in the abdominal cavity, as well as intestinal adhesiolysis. Twenty-four days after the surgery, intestinal contents appeared on the drain and another operation followed. The anastomotic leak was on the anterior wall of the stomach. Lavage of the abdominal cavity was done, with the gastrostomy and gastroplasty by Mikulić and with placing an open abdomen system ABTHERA. Twenty-five days after the last intervention, intestinal contents were again in the drain and reoperation was done. The colonic gangrene in the area of the hepatic flexure was found, with subsequent right hemicolectomy, Brooke ileostomy, and the open ABTHERA system was again installed. Twenty-eighth postoperative day after this intervention, the bile content was verified on the drains, which indicated the presence of an intestinal fistula. A new surgical procedure was performed, the ABTHERA system was removed, a protective Stamm-Kaden gastrostomy was performed, drains were replaced, the abdomen was closed with tension, and in the upper part of the wound Vacuum-assisted wound closure system (VAC) was placed. Finally, after 2 weeks VAC was extracted, and a contrast passage of the gastroduodenal was performed, as well as fiberoptic pan endoscopy. The patient was discharged from the hospital for home treatment after 128 days. Six months after discharge, the patient was hospitalized again for ileus, due to small intestinal adhesions. Surgery was performed, with the partial resection of the ileum and T-T anastomosis due to ileum injury during adhesiolysis. The postoperative days went smoothly. He has been operated 6 times. Today, he comes regularly for check-ups, his general condition is good and his local findings are normal.
Discussion
Firearm injuries among children are a huge clinical and public health problem that has become a growing concern in recent decades, especially in counties where gun ownership is widespread [5]. The severity of firearm injuries is directly proportional to the distance of the projectile fired. Injuries less than 3 meters away cause massive tissue damage and are usually fatal. Thus, tissues with higher specific gravity suffer more, mostly bone and muscle tissue and parenchymal organs as it is in our cases [4,6]. In recent decades, the incidence of these injuries has been constantly increasing, and these injuries have become one of the leading causes of child mortality in the United States of America in 2020 [7]. Intentional injuries are most common among boys over 12 years old (over 80%), as we reported in our study. DiScala reports similar data in his study analyzing data from the National Pediatric Trauma Registry and the United States National Electronic Injury Surveillance System [8]. The abdomen and pelvis were the most commonly affected areas of the body where the injuries occurred, which was different from other studies where the head and chest were the major body parts affected [9].
Management of patients with penetrating abdominal injuries requires a multidisciplinary approach. The initial step is the application of the advanced life support algorithm using the ABCDE approach. There is no unique standard of treatment for patients with penetrating abdominal injuries. Previously, the initial approach to treatment was urgent surgical exploration. However, analyzing this approach, some authors claim that it is associated with a higher incidence of complications, a higher percentage of unnecessary explorations, and a longer hospital stay. Conservative treatment measures are increasingly gaining importance in hemodynamically stable patients. Renz et al. show the frequency of complications after unnecessary laparotomies as high as 41.3% [10]. Also, laparoscopy can be used for the diagnosis and, in some cases, the treatment of injuries, reducing the percentage of complications that arise as a result of an open surgical approach [11]. But the subject of the greatest debate in the literature, without clearly defined recommendations is what to do in patients with severe instability. Should we risk fatal deterioration of the patient due to additional time for diagnosis or to perform a surgical intervention as early as possible.
Further procedures depend on the patient's hemodynamic stability. Hemodynamically stable patients allow more time for physical examination, laboratory, and radiological diagnosis. But critically unstable patients with very severe injuries require urgent surgical treatment without further diagnosis as we had to do in one injured patient. Some authors point out that the preparation of the operating room should begin immediately after the admission of unstable patients [12]. Lynch et al. believe that urgent laparotomy is indicated in patients with pneumoperitoneum, in patients with evisceration of intraperitoneal contents, and in patients in whom hemodynamic instability is maintained despite intensive resuscitation (transfusion of more than 50% of the total blood volume ) [13]. There is a big discrepancy in the literature data about the method of intravenous resuscitation of fluids or blood derivatives. While some authors recommend intensive resuscitation, others suggest careful intravenous resuscitation until control of active bleeding is achieved on the operating table. They believe that with limited fluid replacement, maintaining blood pressure at lower values , and limiting dilutional coagulopathy, a better survival rate is achieved [14].
After opening the abdomen, our primary goal was bleeding control. The temperature of the patient's body, the operating room, and the blood products is very important and must be above 35C0, to prevent a lethal triad consisting of hypothermia (< 34C0), acidosis (pH < 7.2) and coagulopathy (pTT> 55s) [15]. The treatment of hollow organ injuries depends on the severity of the injury. Injuries of solid organs such as the spleen and liver, with bleeding, can be solved with local hemostatic maneuvers, while in more severe cases resection with the suture is required. Treatment of injuries to the main blood vessels of the abdomen is of priority importance because lesions of these organs are associated with high mortality [12].
Observing the risk factors for the fatal outcome of such injuries, Tyburski et al. believe that an initial systolic pressure of less than 90 mm Hg as well as a body temperature of less than 34C0 is the most important risk factors for a fatal outcome [16]. Other authors emphasize the importance of base deficit as one of the predictive factors, not only of injury severity but also of fatal outcome [17].
Conclusions
Abdominal injuries caused by firearms in recent decades represent a very important cause of morbidity and mortality in children. The incidence varies and is directly proportional to the degree of violence in society. As expected, the dominant number of such injuries is among boys, the average age of which is over 12 years. Patient care requires a multidisciplinary approach , and the initial decision on further treatment depends on the patient's hemodynamic stability. While hemodynamically stable patients provide the opportunity for additional diagnostic procedures and conservative treatment, hemodynamically unstable patients require immediate surgical intervention.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Beraldo, R.F.; Forlin, E. Firearm-Related Musculoskeletal Injuries in Brazilian Children and Teenagers. Rev Bras Ortop (Sao Paulo). 2019, 54, 685–691. [Google Scholar] [PubMed]
- Drexel, S.; Azarow, K.; Jafri, M. Abdominal Trauma Evaluation for the Pediatric Surgeon. Surg Clin N Am 2017, 59–74. [Google Scholar] [CrossRef] [PubMed]
- Amick, L.F. Penetrating trauma in the pediatric patient. Clin PediatrEmerg Med 2001, 2, 63–70. [Google Scholar] [CrossRef]
- Stefanopoulos, P.; Tsiatis, N.; Herbstein, J. Gunshot wounds. Encyclopedia of Forensic Sciences, Third Edition 2023, 3, 75–98. [Google Scholar]
- Murray, C.J.; Lopez, A.D. Mortality by cause for eight regions of the world: Global Burden of Disease Study. Lancet. 1997, 349, 1269–1276. [Google Scholar] [CrossRef]
- Shrestha R, Kanchan T, Krishan K. Gunshot Wounds Forensic Pathology. [Updated 2022 May 15]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2023 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK556119/.
- Roberts, B.; James, D.; Haft, J.; Balakrishnan, N.; Prince, J.; Sathya, C. Wounding patterns in pediatric firearm fatalities. Injury. 2023, 54, 154–159. [Google Scholar] [CrossRef]
- DiScala, C.; Sege, R. Outcomes in Children and Young Adults Who Are Hospitalized for Firearms-Related Injuries. Pediatrics 2004, 113, 1306–12. [Google Scholar] [CrossRef]
- Chugtai, B.R.; Uraizy, S.M.A.; Rashid, M.A.; Chaudary, T.H.; Ahmed, B.; Qureshi, G.A.A. Incidence of Homicidal Deaths. The Professional. 2002, 9, 316–319. [Google Scholar]
- Renz, B.M.; Feliciano, D.V. Unnecessary laparotomies for trauma: a prospective study of morbidity. J Trauma. 1995, 38, 350–6. [Google Scholar] [CrossRef]
- Gaines, B.A.; Rutkoski, J.D. The role of laparoscopy in pediatric trauma. Semin Pediatr Surg. 2010, 19, 300–3. [Google Scholar] [CrossRef]
- Cotton, B.A.; Nance, M.L. Penetrating trauma in children. Semin Pediatr Surg. 2004, 13, 87–97. [Google Scholar] [CrossRef] [PubMed]
- Lynch, T.; Kilgar, J.; Al Shibli, A. Pediatric Abdominal Trauma. CurrPediatr Rev. 2018, 14, 59–63. [Google Scholar] [CrossRef] [PubMed]
- Deakin, C.D. Early fluid resuscitation in hemorrhagic shock. EurJEmerg Med 1994, 1, 83–8. [Google Scholar]
- Polites, S.F.; Habermann, E.B.; Glasgow, A.E.; et al. Damage control laparotomy for abdominal trauma in children. Pediatr Surg Int 2017, 33, 587–92. [Google Scholar] [CrossRef] [PubMed]
- Tyburski, J.G.; Wilson, R.F.; Dente, C.; Steffes, C.; Carlin, A.M. Factors affecting mortality rates in patients with abdominal vascular injuries. J Trauma. 2001, 50, 1020–6. [Google Scholar] [CrossRef] [PubMed]
- Kincaid, E.H.; Chang, M.C.; Letton, R.W.; Chen, J.G.; Meredith, J.W. Admission base deficit in pediatric trauma: a study using the National Trauma Data Bank. J Trauma. 2001, 51, 332–5. [Google Scholar] [CrossRef] [PubMed]
Figure 1.
1a and 1b. Multiple injuries of the mesocolon transversum and mesentery of the small intestine, 1c. rupture of D3 duodenal portion, 1d. laceration of v cava inferior and right v. iliaca communis. 1e. the primary suture of the duodenum, 1f. Two drains were placed, the first one in the right paracolic, and the second one in the recto-vesical space.
Figure 1.
1a and 1b. Multiple injuries of the mesocolon transversum and mesentery of the small intestine, 1c. rupture of D3 duodenal portion, 1d. laceration of v cava inferior and right v. iliaca communis. 1e. the primary suture of the duodenum, 1f. Two drains were placed, the first one in the right paracolic, and the second one in the recto-vesical space.
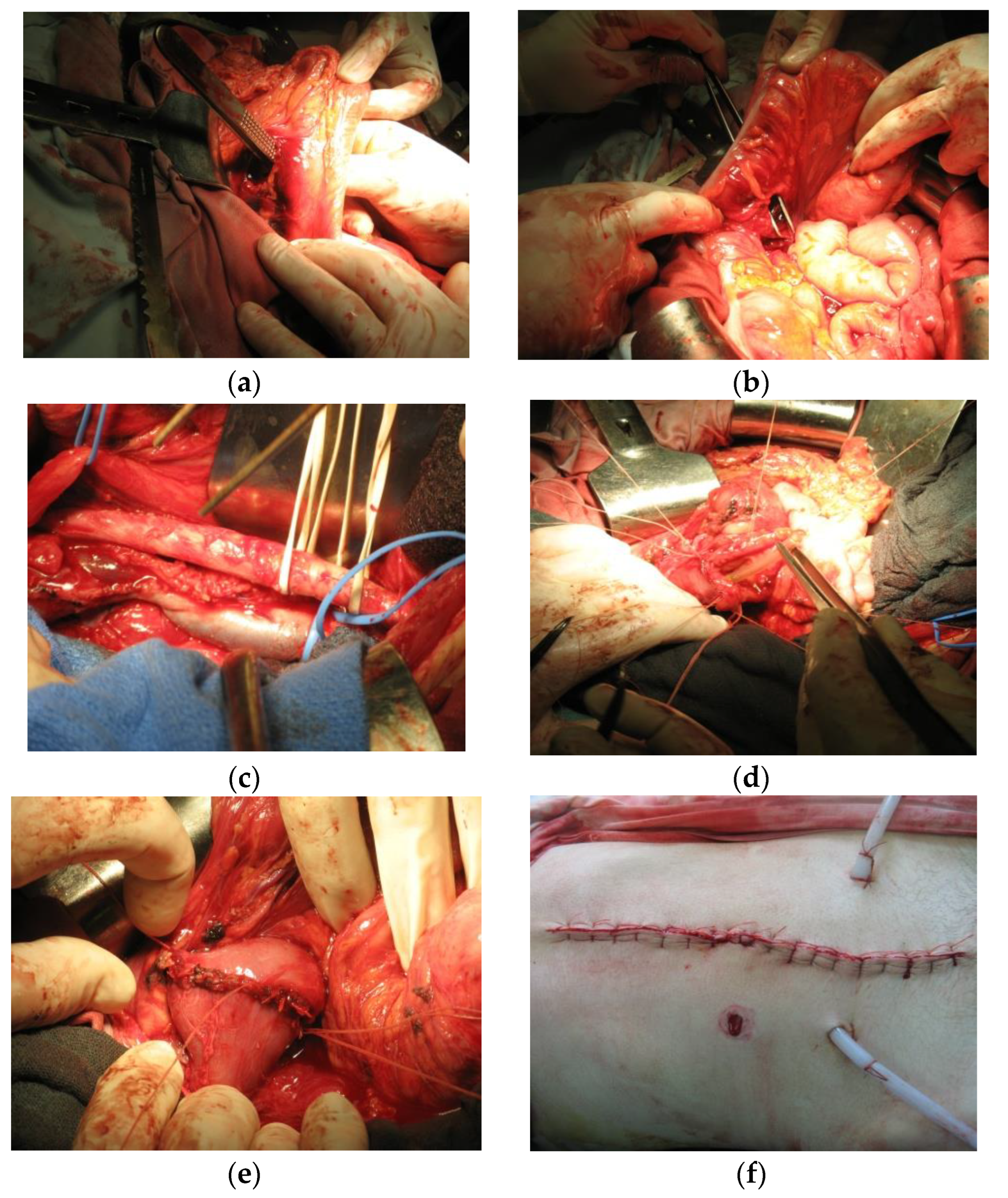
Figure 2.
2a.Patient with an entry wound in the epigastric area left of the xiphoid, and an exit wound in the left paravertebral area, 2b. conquassation of the spleen with transsection of the splenic vein and artery, 2c. lesion of the left kidney with transection of the renal vein and artery, 2d. primary stomach suture.
Figure 2.
2a.Patient with an entry wound in the epigastric area left of the xiphoid, and an exit wound in the left paravertebral area, 2b. conquassation of the spleen with transsection of the splenic vein and artery, 2c. lesion of the left kidney with transection of the renal vein and artery, 2d. primary stomach suture.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



