
Submitted:
18 July 2023
Posted:
19 July 2023
You are already at the latest version
Abstract
Abstract: Background and Objectives: A growing number of epidemiologic studies have found that diabetes mellitus may increase cancer risk and is implicated in numerous other metabolic and inflammatory disorders. The increase in pro-inflammatory cytokines plays a major role in insulin resistance and leads to hypoalbuminemia, and micro- and macrovascular diabetes complications, including kidney disease and anemia. This study aimed to investigate the utility of CEA, CRP, serum albumin level, hemoglobin, and LDH as biomarkers for cancer risk and the biological implications of diabetes on the evolution and prognosis of oncological patients. Material and methods: We conducted a retrospective, longitudinal, observational study, on a total group of 434 patients, 217 diagnosed with a form of cancer and with type 2 diabetes as a comorbidity, and the other 217 – control group, without diabetes. These patients were admitted to the oncology clinic. In subgroups, the same number of patients was considered, depending on the location of the oncological pathology. Anemia, hypoalbuminemia, elevated lactate dehydrogenase, glycated hemoglobin, and C-reactive protein levels are more pronounced in subjects with type 2 diabetes and cancer. Conclusions: The presence of diabetes negatively affects the clinical and biological prognosis of cancer patients.
Keywords:
diabetes
; cancer
; anemia
; albumin
1. Introduction
A growing number of epidemiological studies have found that diabetes mellitus increases the risk of developing many types of cancer [1]. The association between these two diseases was first time discussed over 75 years ago. Recent and multiple evidence had shown that diabetes is associated with an increased risk of cancer and a higher mortality rate in cancer patients [2]. An epidemiologic study that enrolled 420 patients with type 2 diabetes mellitus concluded that the most frequent association between diabetes and neoplasia was for lung, breast, pancreatic, and colorectal cancers [3]. Lactate dehydrogenase (LDH) levels, complete blood count, carcinoembryonic antigen (CEA), glycated hemoglobin (HbA1c), and C-reactive protein (CRP) are accessible biomarkers, forming part of the standard patient assessment; it could be predictive factors for cancer in diabetic patients and can guide the oncologist in terms of the patient prognosis at the onset of treatment [4]. We believe that these biomarkers can also be used by a diabetes doctor to be able to suspect the presence of cancer, especially when an unexplained glycemic imbalance occurs. Developing colorectal cancer is 27% more possible in patients with type 2 diabetes mellitus than in non-diabetic patients [5]. Various studies have also demonstrated that the risk of colon cancer recurrence is higher in diabetic patients [5].
One study of 47 patients with diabetes and colorectal cancer showed an average HbA1c value of 6.0%, and 45% of them had an HbA1c of at least 7% [5]. There is insufficient information on CEA in colorectal cancer patients with diabetes. Several studies showed a statistically significant correlation between elevated CEA levels and diabetes as well as a correlation between serum CEA levels and HbA1c levels [5]. Insulin resistance and relative insulin deficiency are characteristic of type 2 diabetic patients, they are often overweight and elderly with diabetes oncoming than type 1 diabetic subjects. Obesity promotes insulin resistance and is considered one of the main reasons for the current diabetes epidemic [5]. Albumin is a major protein synthesized in the liver. Energy intake is a very important factor in the normal physiology of albumin production. In fact, reduced serum albumin levels are observed in diseases associated with malnutrition, while high serum albumin levels are associated with metabolic syndrome, an indicator of obesity and overeating. In addition, a link between serum albumin and insulin resistance has recently been suggested [6].
Long-term type 2 diabetes mellitus is associated with about 1.5 increased risk of pancreatic cancer. [7] A causal relationship between diabetes and pancreatic cancer is also supported by prediagnosis measurements of glucose and insulin levels in prospective studies [7]. Insulin resistance and associated hyperglycemia, hyperinsulinemia, and inflammation are the underlying mechanisms contributing to the development of diabetes-associated pancreatic cancer. The mechanism of the relationship between diabetes and pancreatic cancer is elusive and could include metabolic, hormonal, and immunologic changes that influence tumor growth. Insulin resistance and compensatory hyperinsulinemia are maybe the most suspected mechanisms underlying the relationship between type 2 diabetes mellitus and pancreatic cancer [7].
Diabetes was associated with a significantly more pronounced risk of lung cancer compared with patients without diabetes when the analysis was restricted to studies that accounted for smoking status. In contrast, this association disappeared when the analysis was restricted to studies that did not consider smoking status [8]. Subjects with type 1 and type 2 diabetes had a higher level of fasting plasma lactate, versus the group without diabetes [9].
Chronic hyperlactatemia maintained by increased lactate formation from adipocytes in obese individuals has been found to precede the onset of diabetes [10] and might contribute to the appearance of the disease. Taken together, these data suggest that chronic hyperlactatemia may indicate the early stages of insulin resistance. Several epidemiological analyses have shown that high lactate levels may predict the onset of diabetes.
LDH’s prognostic value in patients with lung cancer was investigated by some researchers, but the findings were inconclusive. According to some studies, patients with lung cancer have worse prognoses when their LDH levels are higher. Some researchers discovered that this correlation was insignificant [11]. Higher pretreatment LDH levels have been associated with poorer overall survival in subjects with lung cancer [11].
Anemia is the most common hematologic change in patients with malignancies [12]. It may be the first diagnostic clue for underlying malignant disease and contribute to symptomatology and treatment decisions. Cytokine production associated with the tumor is an important factor in the appearance of anemia in cancer patients. A malignant tumor can also affect bone marrow – fibrosis -, which can also result in anemia. Bone marrow is known for its rich blood supply and is, therefore, a common site for metastasis to develop [13]. Bone marrow fibrosis, originally characterized by Wartofsky and Burman, was originally called "low T3 syndrome" [13]. Breast malignancy, prostate, and lung are the most involved types of cancer, although almost all types of cancers can lead to this complication. Normocytic, normochromic anemia occurs frequently in patients with a variety of inflammatory disorders, with many contributing factors.
The objectives of the study were to assess the utility of CEA, CRP, serum albumin level, hemoglobin, and LDH as biomarkers of cancer risk and the biological implications of diabetes on the evolution and prognosis of oncological patients.
2. Materials and Methods
We performed a retrospective, longitudinal, observational study, over a period of 2 years, between 2016 and 2017, on two equal groups of patients, 217 already having type 2 diabetes and recently diagnosed with breast, lung, colorectal, or pancreatic cancer (the most frequent types of tumors associated with type 2 diabetes), and the other 217, without diabetes. All of them were hospitalized in the Oncology Medical Clinic of the Clinical County Emergency Hospital Craiova, Romania.
Criteria for inclusion: patients with a maximum performance status of 2, hospitalized in the Oncology Medical Clinic of Emergency Clinical County Hospital Craiova (Romania) at the initiation of oncologic treatment, with the diagnosis of lung, breast, colon, or pancreatic cancer, who signed an informed consent. These patients were divided into two subgroups: subgroup 1 with type 2 diabetes, and subgroup 2 without diabetes.
Criteria for exclusion – both patients with other types of tumors and patients with other types of inflammatory, acute, or chronic conditions were excluded; also, patients for whom insufficient data was recorded or who did not sign an informed consent.
The study group was represented by 217 patients, already with type two diabetes, who were hospitalized in the Oncology Medical Clinic of the Emergency Clinical County Hospital Craiova (ECCHC), in the period 2016 – 2017, with a performance status of a maximum of 2, with the intention of beginning oncologic specific treatment: 81 patients with lung cancer, 45 patients with colon cancer, 38 patients with pancreatic cancer, and 53 patients with breast cancer). After that, another equal group was formed, composed of 217 patients – a group without type 2 diabetes. All data, for all 434 patients, were collected from the medical records of patients hospitalized in the Oncology Medical Clinic of ECCHC.
In this study, at the moment of the first admission, we evaluated the values of hemoglobin, CRP, HbA1c, LDH, alkaline phosphatase (FAL), serum albumin, and CEA in subgroup 1, with diabetes, and we compared them with the values found in subgroup 2, without diabetes. The HbA1c values in subgroup 2 were less than 5.7%, so type 2 diabetes and prediabetes were excluded [5,7], not only through HbA1c but also through personal history.
There were used the following ECCHC laboratory analyzers: COULTER DXH for hemoglobin, MINDRAY BS 800 for CRP and LDH levels, ARCHITECT C8000 for serum albumin, COBAS E411-2 for CEA and HbA1c.
Statistical analysis was realized using Microsoft Office Pack - Microsoft Excel 2000 to collect data and obtain graphics and average values, and the MATLAB v.9.0 (2016) Student T-Test program, to test the normality of data and to expose the statistically significant differences between the two analyzed groups, the average values in the study group is compared with those of patients in the group without diabetes, a p-value < 0.05 being considered statistically significant. A confidence coefficient was also used, ‘r’ value close to 1 considering a positive correlation.
Ethical concerns. The protocol of the study was approved by the Ethics Committee of the University of Medicine and Pharmacy of Craiova, approval number 39/20.01.2023.
3. Results
3.1. General results
The average values in the study group, compared with those of patients in the group without diabetes, were strongly correlated, p-value resulted was 0.002.
In subgroup 1 - of 217 patients with type 2 diabetes and cancer, compared with subgroup 2, the average value of hemoglobin was 11.3 g/dL at the moment of diagnosis of cancer, vs. 12.4 g/dL for the group without diabetes (p = 0.0001) (Figure 1).
LDH studied in the entire group, was more pronounced in the diabetes subgroup at the moment of cancer diagnosis (average 337 U/L) versus the group without diabetes, 292 U/L (p = 0.0033) (Figure 2).
HbA1c in subgroup 1 had rates between 5.7% and 13.1%, with an average value of 8.57%, which suggests poor diabetes control in relation to neoplasia.
A large number of patients in the studied group had an average albumin level of 28.9 g/L, showing the nutritional status of patients with diabetes and cancer. In the group without diabetes, the average value of albumin was 35.3 g/L, showing that metabolic disorders were already present. (p< 0.001) (Figure 3).
A positive correlation in the whole analyzed group was identified between LDH values, and serum albumin values (r = 0.76), but also between LDH and hemoglobin value (r = 0.82), especially in those patients diagnosed in stage IV (Figure 4 and Figure 5)
CRP levels in subgroup 1 were significantly higher when compared with the group without diabetes, with an average value of 73.47 mg/L, and 38.3 mg/L in subgroup 2, results which suggest a higher inflammation level in patients who had as comorbidity type 2 diabetes (p < 0.001) (Figure 7).
Also, a positive correlation between hemoglobin and C-reactive protein was found (Figure 8)
Also, correlations between LDH and CRP levels (r= 0.83) and LDH and FAL (r = 0.72) were found. All these correlations suggest a sustained inflammatory response of the body in the presence of type two diabetes, more pronounced as the body is more hematological and nutritionally balanced.
3.2. Study of biological tests by tumor localization
3.2.1. Lung Cancer
In 81 patients with diabetes, the average value of hemoglobin at the moment of lung cancer diagnosis was 11.5 g/dL, versus 12.5 g/dL for the group without diabetes, and patients without diabetes (p = 0.003). LDH levels were not significantly increased in comparison with the group without diabetes (308 U/L in diabetic patients vs. 330 U/L in non-diabetic subjects). The average albumin levels for diabetic patients with lung cancer were 28.5 g/L and in the non-diabetic group 34.9 g/L (p < 0.001). CRP levels were also significantly elevated in patients from subgroup 1 (average value 91 mg/L) vs. 40.2 mg/L in the group without diabetes (p = 0.0022). HbA1c level was between 5.7% and 13.1%, with an average value of 12%.
3.2.2. Colon Cancer
In subgroup 1, the average value of hemoglobin was 11.2 g/dL, compared with the non-diabetic group, 12.1 g/dL (p = 0.01). LDH levels were elevated in the study group when cancer was diagnosed (average value 411 mg/dL) compared with the group without diabetes, 273 mg/dL (p = 0.0017).
A major difference was observed for albumin levels, showing that nutritional balance for colon cancer in association with type 2 diabetes is fragile (average albumin 28.3 g/L in diabetic patients vs. 36.6 g/L in the non-diabetic group) (p = 0.00023). CRP levels were also increased in the study group vs. the group without diabetes (59.9 mg/L vs. 39.2 mg/L, p = 0.008). CEA levels, studied in pancreatic and colon cancer patients, were significantly elevated in non-diabetic colon cancer cases, with an average value of 288 ng/mL vs. 44.3 ng/mL in diabetic patients.
3.2.3. Pancreatic cancer
Anemia at the moment of diagnosis was more common in pancreatic cancer with type 2 diabetes as comorbidity, with an average value of hemoglobin of 11.3 g/dL, against 12.4 g/dL for non-diabetic pancreatic cancer cases (p = 0.006). The average LDH level was 344 mg/dL in the diabetes subgroup, and 305 mg/dL in the non-diabetes subgroup, indicating a worse prognosis of the disease in diabetic patients.
CEA value was 3-fold higher in diabetics (average value 39.2 mg/dL), against 12.9 mg/dL in nondiabetic patients. Inflammatory markers were higher in diabetes patients (CRP average value 63.3 mg/dL vs. 38.7 mg/dL in the non-diabetes group).
There was no significant difference in albumin values (29.6 g/L in the study group vs. 34.1 g/L in the group without diabetes, p = 0.00091).
The average HbA1c value in diabetes patients at the moment of diagnosis of pancreatic cancer was 8.69%.
3.2.4. In the breast cancer
In the breast cancer subgroup, the average value of hemoglobin was lower in the group of diabetes patients (11.05 g/dL) and 12.6 g/dL in non-diabetic patients (p = 0.00011). LDH levels were elevated in the diabetes group, 312 mg/dL, versus 223 mg/dL (p = 0.00029), which suggests an increased inflammation in diabetes patients, confirmed by CRP values (64.9 mg/dL vs. 31.4 mg/dL in non-diabetes group, p = 0.0022).
Denutrition was more pronounced in diabetes group patients (29.6 g/L vs. 35.1 g/L for non-diabetes, p < 0.0001). The average value of HbA1c was 8.49%.
In the analyzed group of oncological patients with diabetes, only 41 of them performed at least 3 months of specific oncological treatment, which included surgery, chemotherapy, or external irradiation. Instead, in the control group, 88 patients could be treated for at least 3 months.
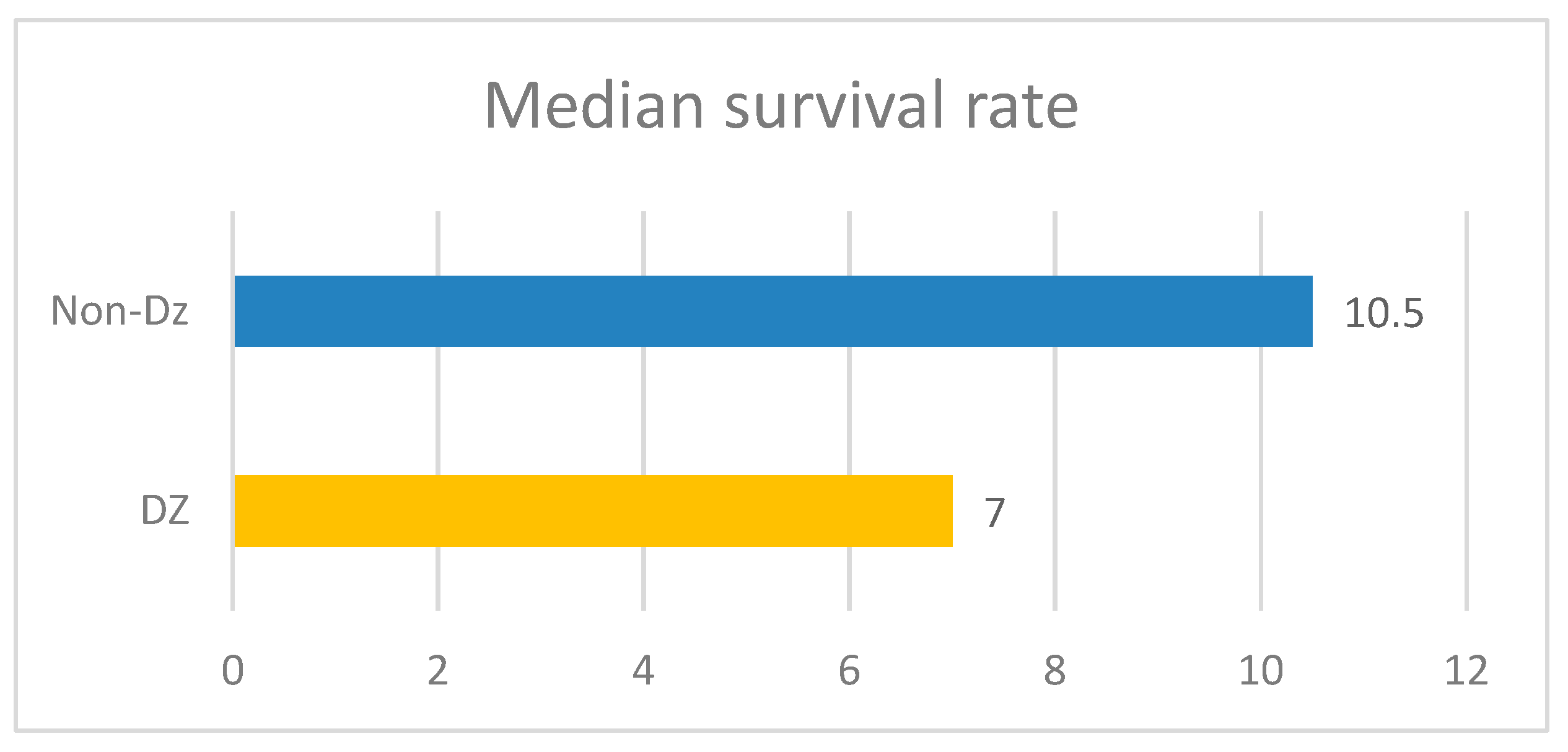
The median duration of oncological treatment in cancer patients with associated diabetes was 4 months, while in the control group, it was 6 months. The median duration of survival in the diabetic patient group was 7 months, while the median survival in the control group was 10 months (Figure 9).
4. Discussion
This study was designed to assess the utility of CEA, CRP, serum albumin level, hemoglobin, and LDH as biomarkers of cancer risk (colon, lung, breast, pancreatic cancer) in obese and/or diabetic patients, and for studying correlations between them and the prognosis of cancer patients with associated type 2 diabetes, being at the onset of treatment.
In our study, it was found that anemia, hypoalbuminemia, elevated lactate dehydrogenase, glycated hemoglobin, and C-reactive protein levels are more pronounced in subjects with type 2 diabetes and cancer (p = 0.002). These biomarkers may be an indicator of a patient's inflammatory state for diabetic patients, and a neoplasm can be sought.
Hematologic markers that reflect systemic inflammation can also be used to predict the prognosis of cancer. Systemic inflammatory responses play a significant role in carcinogenesis, cancer progression influencing tumoral responses under oncologic treatment, and survival [4].
Recent studies show that type 2 diabetes is an independent risk factor for the progression of several cancers. Although these two diseases have an important number of common risk factors, the connection between them is still not well understood, posing a challenge for clinical management [9].
The incidence of diabetes has been increasing in the past two decades (464.237 million in 2019) and is expected to increase further, estimated at more than 700 million in 2045 [14,15].
Given the increasing interest of the European Community and the Romanian government in implementing comprehensive prevention programs against the spread of cancer and type 2 diabetes [31] and the fact that many diabetic patients develop a malignancy during their lifetime [4], we wanted also to investigate the impact of type 2 diabetes on the oncological patient and how predictive factors can be used. Diabetes is a concomitant disease that can also influence the therapeutic response to cancer therapy [4]. The duration of treatment in a patient who also has diabetes was shorter compared to those patients without diabetes, which also has an impact on survival, its median is 7 months in the diabetic group, compared to 10 months in cancer patients without diabetes.
LDH level in the diabetic group for each type of cancer that was studied, but the most significant difference was in colorectal cancer (411 mg/dL vs. 273 mg/dL in the group without diabetes), and breast cancer sub-group (312 mg/dL vs. 223 mg/dL in non-diabetic cases). Increased lactate alters the microenvironment, provides nutrients to cancer cells, and leads to acidosis, inflammation, angiogenesis, immunosuppression, and radiation resistance. Bonuccelli et al (2010) showed that ketones and lactate promote tumor growth and metastatic disorders, which may state why diabetic subjects have increased cancer incidence and poor prognosis due to increased lactate production [16]. The body of a human contains LDH in a variety of tissues. In order for lactic acid and pyruvic acid to react, an enzyme called LDH is required. Usually, anaerobic environments like the intratumoral environment are where the reaction between lactic acid and pyruvic acid takes place. The environment around tumors contains high levels of LDH reflex anaerobic glycolytic metabolism. The patients in the high metastatic score group had significantly higher serum LDH concentrations than those in the low metastatic score group, according to other studies [16].
A major reason for the development of cancer is that the immune system loses its ability to effectively eliminate aberrant cells. High levels of lactate have a deleterious effect on immune cells infiltrating the tumor. Finally, lactate is an inflammatory mediator [18] and could be a biomarker of inflammatory processes promoting tumor development [19]. This specific inflammatory microenvironment also promotes tumor metastasis [4], leading to a negative prognosis [20].
Malignancies can also attack the bone marrow (bone marrow fibrosis), which can also lead to anemia. The bone marrow has a rich blood supply and is, therefore, a frequent site for the development of metastases [13]. Breast cancer, prostate, and lung malignancies are most frequently associated with anemia, although anemia may be encountered in almost all cancers. Normocytic normochromic anemia is also common in patients with several inflammatory diseases. Iron may be plentiful in the bone marrow but is not absorbed and does not enter the bloodstream, making it unavailable for erythropoiesis [12]. Due to diabetes mellitus, nephropathy may occur, which further undermines renal production of erythropoietin, contributing to anemia [21]. Anemia in diabetic patients affects the quality of life and is associated with disease progression and the development of comorbidities [22].
The increase in pro-inflammatory cytokines plays a major role in insulin resistance and leads to the occurrence of microvascular and macrovascular diabetic complications. Increasing IL -6 results in an anti-erythropoietic effect, as this cytokine alters the sensitivity of precursor cells to erythropoietin and promotes cellular death of immature erythrocytes, leading to a further decrease in the number of circulating erythrocytes and a decrease in circulating hemoglobin. Our study highlighted that higher CRP values were found in diabetics and cancer patients, (Average value 73.47 g/L) compared with nondiabetic patients (average CRP value 38.3 g/L). Positive correlations between inflammatory biomarkers, serum albumin and hemoglobin values were found, suggesting a more sustained inflammatory response, as the nutritional and biologic status is more balanced.
Genetic syndromes, inflammatory bowel diseases, history of abdominal radiation therapy, dietary factors (red meat, alcohol, high-fat/low-fiber diet), and tobacco use are the most incriminated factors for developing digestive tube malignancies [23,24]. There are risk factors (obesity and physical inactivity) common to those with diabetes mellitus. Inflammation associated with diabetes may also contribute to the development and progression of colorectal cancer [25]. CRP levels were more significant in the diabetic group than in the non-diabetic group with colorectal cancer (49.9 mg/L vs. 39.1 mg/dL), supporting this fact. In a study, the researchers reported that Increased lactate dehydrogenase release in HT-29 colon cells has been linked to the biological mechanisms of Diclofenac-induced cell death while chrysin alleviated this effect [26,27].
There was no difference between patients with colorectal cancer who had diabetes and those who did not, according to a recent case-control study on the relationship between type 2 diabetes and colorectal cancer. The same study discovered that diabetic patients with colorectal cancer had a higher CEA than the group without diabetes and that their value decreased much more quickly under specific treatment than the group of patients without type 2 diabetes. This finding may have an impact on treatment choices [22].
For pancreatic cancer, there is increasing evidence that inflammation plays an important role in its development [28]. Our study found that inflammatory markers are higher in diabetic patients (CRP average value 59.96 mg/dL vs. 39.2 mg/dL in the non-diabetic group). Inflammatory pathways are frequently activated by obesity and macronutrient intake. Glucose and fat intake can trigger inflammation by increasing oxidative stress and activating transcription factors such as nuclear factor-κB, activating protein-1, and early growth response-1 [25]. Some adipocytokines are key compounds involved in innate immunity, inflammation, apoptosis, and metabolism. Significant levels of proinflammatory cytokines promote angiogenesis, tumor progression, and metastasis [7]. A high level of glycemia is directly related to the development of an inflammatory state, as evidenced by the increased expression of proinflammatory cytokines such as IL -6, TNF-α, and NFκB. Studies show that the longer the disease persists and/or the poorer the glycemic control, the more severe the inflammatory process. The increase in pro-inflammatory cytokines plays a major role in insulin resistance and leads to the occurrence of diabetic macrovascular cardiovascular and microvascular complications and anemia.
Denutrition is a known major problem both for diabetics and cancer patients. This study revealed that low plasmatic albumin levels were found in diabetic patients (average value of albumin 28.9 g/L), compared with non-diabetic patients (35.3 g/L).
Uncontrolled type 2 diabetes in cancer patients was also specific in our study, confirmed by an average value of HbA1c of 8.57%.
Several studies suggest an important association between the depth of anemia and HbA1c levels in patients with diabetes, underlying the hypothesis that anemia is more common in poorly controlled diabetics [12,29]. In our study, hemoglobin and HbA1c levels were not correlated.
Cell proliferation and tissue damage are induced by chronic inflammation [30]. Diabetes and cancer are in a vicious cycle with each other, and lactate plays a central role in this interaction. Insulin resistance/diabetes and cancer lead to high lactate levels; conversely, high lactate levels promote the development and progression of diabetes and cancer [9].
The study limitations are represented by the limited biological tests available, with few options of state-settled biomarkers for the basic biological assessment of the hospitalized patient, which can be used for this purpose.
5. Conclusions
This study was not conducted in clinical trials, and its results from current practice, which show a statistically significant correlation between inflammatory biomarkers in the presence of cancer and type 2 diabetes, can be applied in clinical practice and can lead to improved oncological patient prognosis. Hemoglobin, LDH, CRP, and albumin levels could be used as predictive factors for cancer patients with associated type 2 diabetes, highlighting the importance and impact of metabolic and inflammatory disorders encountered in these chronic diseases. Anemia was strongly correlated with type 2 diabetes and cancer, in lung, colon, breast, and pancreatic cancers; there was a higher incidence of anemia among poorly controlled diabetics. Lactate dehydrogenase levels in the diabetic patients group were significantly elevated in type 2 diabetes associated with cancer, versus the non-diabetic patients group. Inflammation biomarkers, hemoglobin values, and serum albumin levels are also strongly correlated, suggesting a more sustained inflammatory response, as the nutritional and biologic status is more balanced. Better diabetes control can contribute to a favorable prognosis of malignancies. The presence of diabetes negatively influences the evolution and prognosis of cancer patients, median treatment period, and survival rate were lower in diabetic patients.
Institutional Review Board Statement
The protocol of the study received the approval of the Ethics Committee of the University of Medicine and Pharmacy of Craiova, approval number 39/20.01.2023.
References
- Coughlin, S.S.; Calle, E.E.; Teras, L.R.; Petrelli, J.; Thun, M.J. Diabetes mellitus as a predictor of cancer mortality in a large cohortof US adults. American Journal of Epidemiology, 2004, 159, 1160–1167. [Google Scholar]
- Barone, B.B.; Yeh, H.C.; Snyder, C.F.; Peairs, K.S.; Stein, K.B.; Derr, R.L.; Wolff, A.C.; Brancati, F.L. Long-term all-cause mortality in cancer patients with preexisting diabetes mellitus: a systematic review and meta-analysis. Diabetes care 2010, 33, 931–939. [Google Scholar]
- Badulescu, F.; Stan, M.C.; Crişan, A.; Cîmpeanu, R.; Andrei, I. Epidemiological aspects of oncological pathology in patients with diabetes (2007-2017). Oncolog-Hematolog.ro, 2017, 38, 10–15. [Google Scholar]
- Guo, G; Chen, X.; Cai, X.; Chen, Y.; Wang, H.; Fan, L.; Bai, L.; Qiu, H.; Zhang, B. Inflammation-based markers can predict the prognosis of geriatric patients with metastatic colorectal cancer receiving first-line chemotherapy. Translational Cancer Research 2019, 8, 1137–1147.
- González, N.; Prieto, I.; Del Puerto-Nevado, L. Update on the relationship between diabetes and colorectal cancer: epidemiology, potential molecular mechanisms, and therapeutic implications. Oncotarget. 2017, 8(11), 18456–18485. [Google Scholar]
- Bae, J.C.; Seo, S.H.; Hur, K.Y.; Kim, J.H.; Lee, M. S.; Lee, M.K.; Lee, W.Y.; Rhee, E. J.; Oh, K.W. Association between Serum Albumin, Insulin Resistance, and Incident Diabetes in Nondiabetic Subjects. Endocrinology and metabolism (Seoul, Korea) 2013, 28, 26–32. [Google Scholar]
- Li, D. Diabetes and pancreatic cancer. Molecular carcinogenesis 2012, 51, 64–74. [Google Scholar]
- Lee, J.Y.; Jeon, I.; Lee, J.M.; Yoon, J.M.; Park, S.M. Diabetes mellitus as an independent risk factor for lung cancer: a meta-analysisof observational studies. European Journal of Cancer 2013, 49, 2411–2423. [Google Scholar]
- Yong, W.; Yunzhou, D.; Mohammad, A.; Yanjun, L.; Yahya, E.; Jaydutt, V.V. Lactate, a Neglected Factor for Diabetes and Cancer Interaction. Mediators of Inflammation, 2016, 2016, 6456018. [Google Scholar]
- Qvisth, V.; Hagström-Toft, E.; Moberg, E.; Sjöberg, S.; Bolinder, J. Lactate release from adipose tissue and skelet-al muscle in vivo:Defective insulin regulation in insulin-resistant obese women. American Journal of Physiology-Endocrinology and Metabolism 2007, 292, 709–714. [Google Scholar]
- Deng, T.; Zhang, J.; Meng, Y.; Zhou, Y.; Li, W. Higher pretreatment lactate dehydrogenase concentration predicts worse overall survival in patients with lung cancer. Medicine (Baltimore) 2018, 97, 12524. [Google Scholar]
- Antwi-Bafour, S.; Hammond, S.; Adjei, J.K.; Kyeremeh, R.; Martin-Odoom, A.; Ekem, I. A case-control study of prevalence ofanemia among patients with type 2 diabetes. Journal of Medical Case Reports 2016, 10, 10. [Google Scholar]
- Porta, M.G.D.; Malcovati, L. Myelodysplastic syndromes with bone marrow fibrosis. Haematologica 2011, 96, 180–183. [Google Scholar]
- Johari, T.Y.; Ghoneim, M.A.; Moselhy, S.S. Thyroid profile and LDH Isoenzymes as prognostic biomarkers for diabetic and/or obese subjects. African Health Sciences 2018, 18, 697–706. [Google Scholar]
- International Diabetes Federation. IDF Diabetes Atlas, 9th edn. Brussels, Belgium: 2019, http://www.diabetesatlas.
- Bonuccelli, G.; Tsirigos, A.; Whitaker-Menezes, D. Ketones and lactate "fuel" tumor growth and metastasis: Evidence thatepithelial cancer cells use oxidative mitochondrial metabolism. Cell Cycle 2010, 9, 3506–3514. [Google Scholar]
- Lerch, M.M.; Conwell, D.L.; Mayerle, J. The anti-inflammasome effect of lactate and the lactate GPR81-receptor in pancreaticand liver inflammation. Gastroenterology 2014, 146, 1602–1605. [Google Scholar]
- Shime, H.; Yabu, M.; Akazawa, T. Tumor-secreted lactic acid promotes IL-23/IL-17 proinflammatory pathway. Journal ofImmunology 2018, 180, 7175–7183. [Google Scholar]
- Arcidiacono, B.; Iiritano, S.; Nocera, A. Insulin resistance and cancer risk: an overview of the pathogeneticmechanisms. Experimental Diabetes Research, 2012, 2012, 789174. [Google Scholar]
- Jha, V.; Garcia-Garcia, G.; Iseki, K. Chronic kidney disease: global dimension and perspectives. Lancet 2013, 382, 260–272. [Google Scholar]
- Angelousi, A.; Larger, E. Anaemia, a common but often unrecognized risk in diabetic patients: a review. Diabetes & Metabolism 2015, 41, 18–27. [Google Scholar]
- Karlin, N.J.; Amin, S.B.; Kosiorek, H.E.; Buras, M.R.; Verona, P.M.; Cook, C.B. Survival and glycemic control in patients with colorectal cancer and diabetes mellitus. Future Science OA 2018, 4, 335. [Google Scholar]
- Diaconu, C.C.; Arsene, D.; Bălăceanu, A.; Bartoş, D. A rare tumor revealed by abdominal trauma: case presentation. Romanian Journal of Morphology and Embryology 2014, 55, 973–976. [Google Scholar] [PubMed]
- Paraschiv, B.; Toma, C.L.; Diaconu, C. Bronchiolo-alveolar carcinoma in a young patient: a case report. Archivos de Bronconeumología 2013, 49, 315–316. [Google Scholar]
- Greer, J.B.; Whitcomb, D.C. Inflammation and pancreatic cancer: an evidence-based review. Current Opinion in Pharmacology 2009, 9, 411–418. [Google Scholar] [PubMed]
- Özbolat, S. N., & Ayna, A. Chrysin suppresses HT-29 cell death induced by diclofenac through apoptosis and oxidative damage. 2021, 73, 1419–1428.
- Varışlı, B., Caglayan, C., Kandemir, F. M., Gür, C., Ayna, A., Genç, A., & Taysı, S. Chrysin mitigates diclofenac-induced hepatotoxicity by modulating oxidative stress, apoptosis, autophagy and endoplasmic reticulum stress in rats. Molecular Biology Reports 2023, 50, 433–442.
- Mohanty, P.; Ghanim, H.; Hamouda, W.; Aljada, A.; Garg, R.; Dandona, P. Both lipid and protein intakes stimulate increased generation of reactive oxygen species by polymorphonuclear leukocytes and mononuclear cells. The American Journal of Clinical Nutrition, 2002, 75, 767–772. [Google Scholar] [CrossRef]
- Bălăceanu, A.; Diaconu, C.; Mateescu, D.; Stănică, A. Hepatocellular carcinoma with hepatic and pulmonary metastasis, inferior vena cava and left pulmonary artery thrombosis in a patient with asymptomatic hepatitis C. Case report. Medical Ultrasonography 2010, 12, 345–348. [Google Scholar]
- An S, Shim H, Kim K, Kim B, Bang HJ, Do H, Lee HR, Kim Y. Pretreatment inflammatory markers predicting treatment outcomes in colorectal cancer. Ann Coloproctol. 2022, 38, 97–108. [CrossRef]
- “Healthier Together” Eu Non-Communicable Diseases initiative, 22, doi : 102875/195572, https://health.ec.europa.eu/system/files/2022-06/eu-ncd-initiative_publication_en_0. 20 June.
Figure 1.
Hemoglobin values in the study groups.
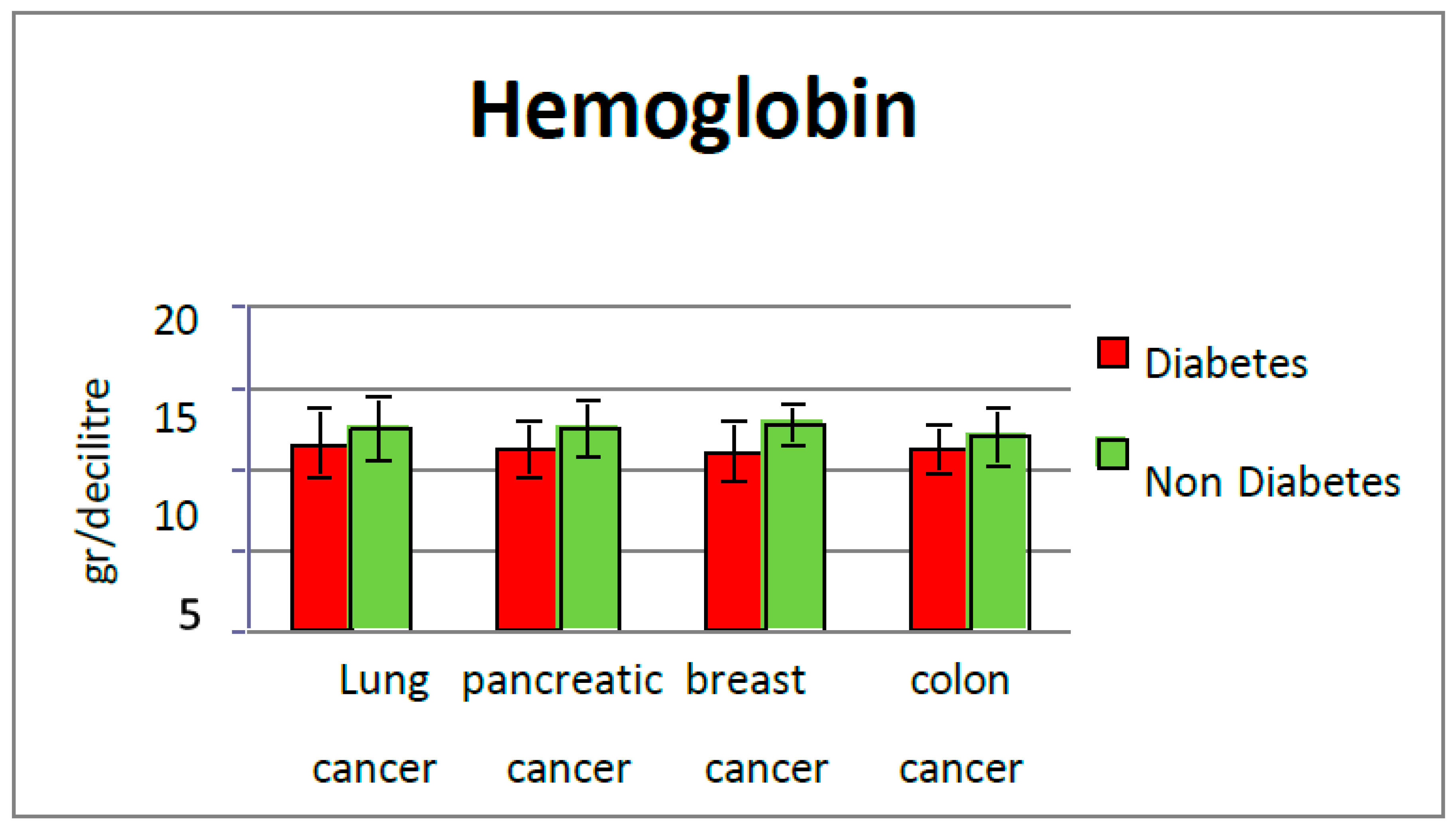
Figure 2.
LDH values in the study groups.
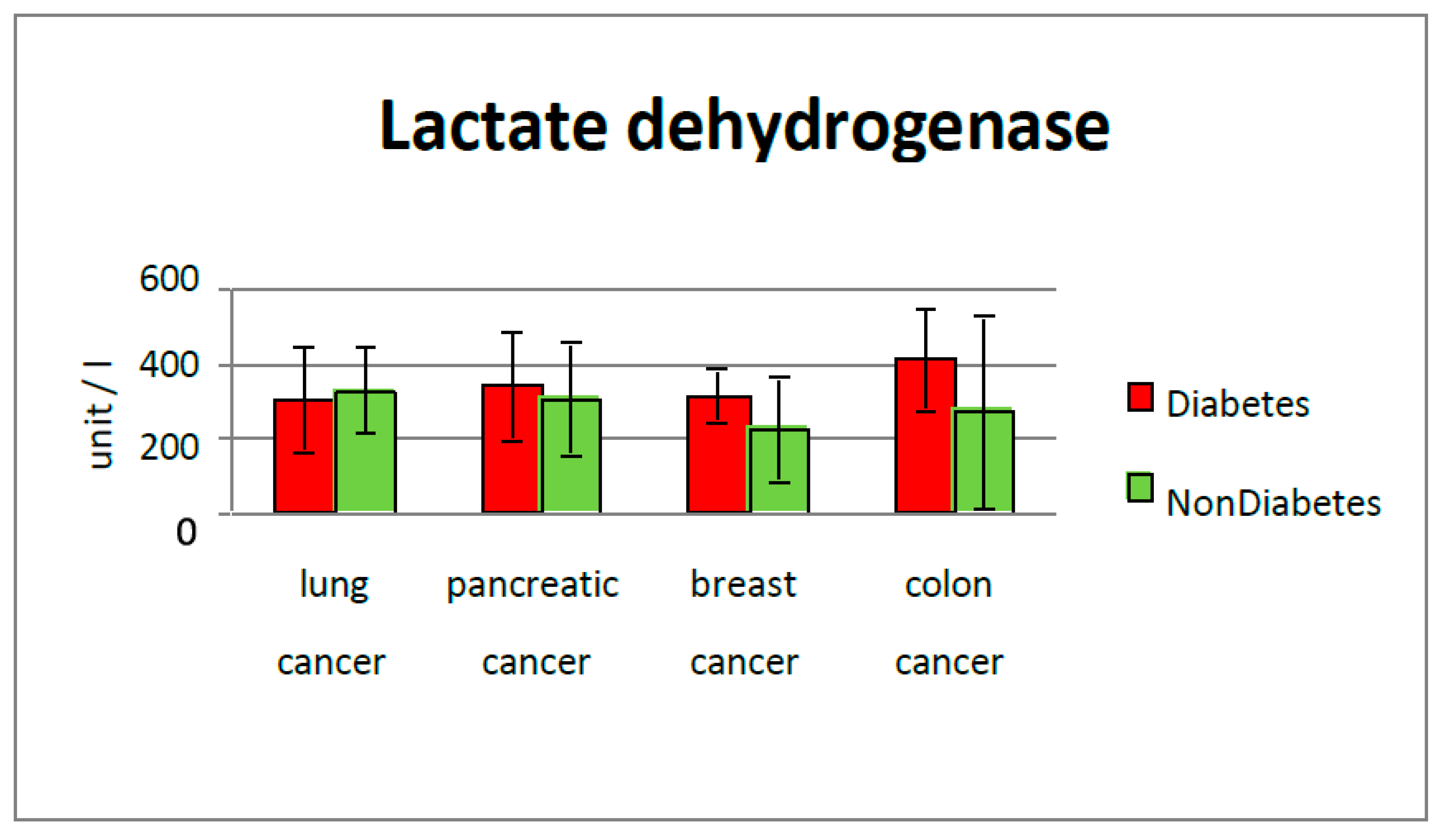
Figure 3.
Albumin values in the study groups.
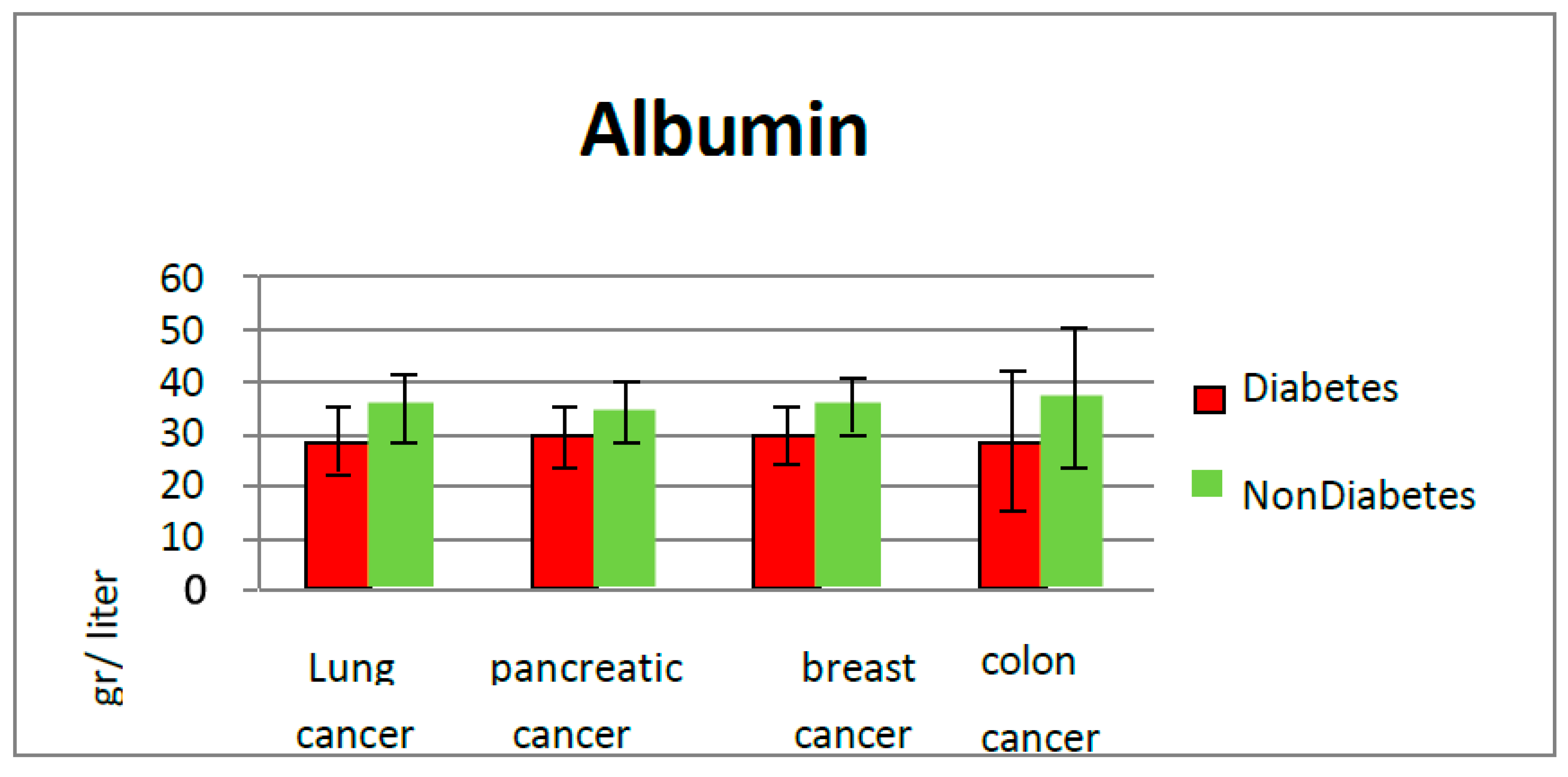
Figure 4.
Positive correlation between albumin and LDH levels (r=0.91).
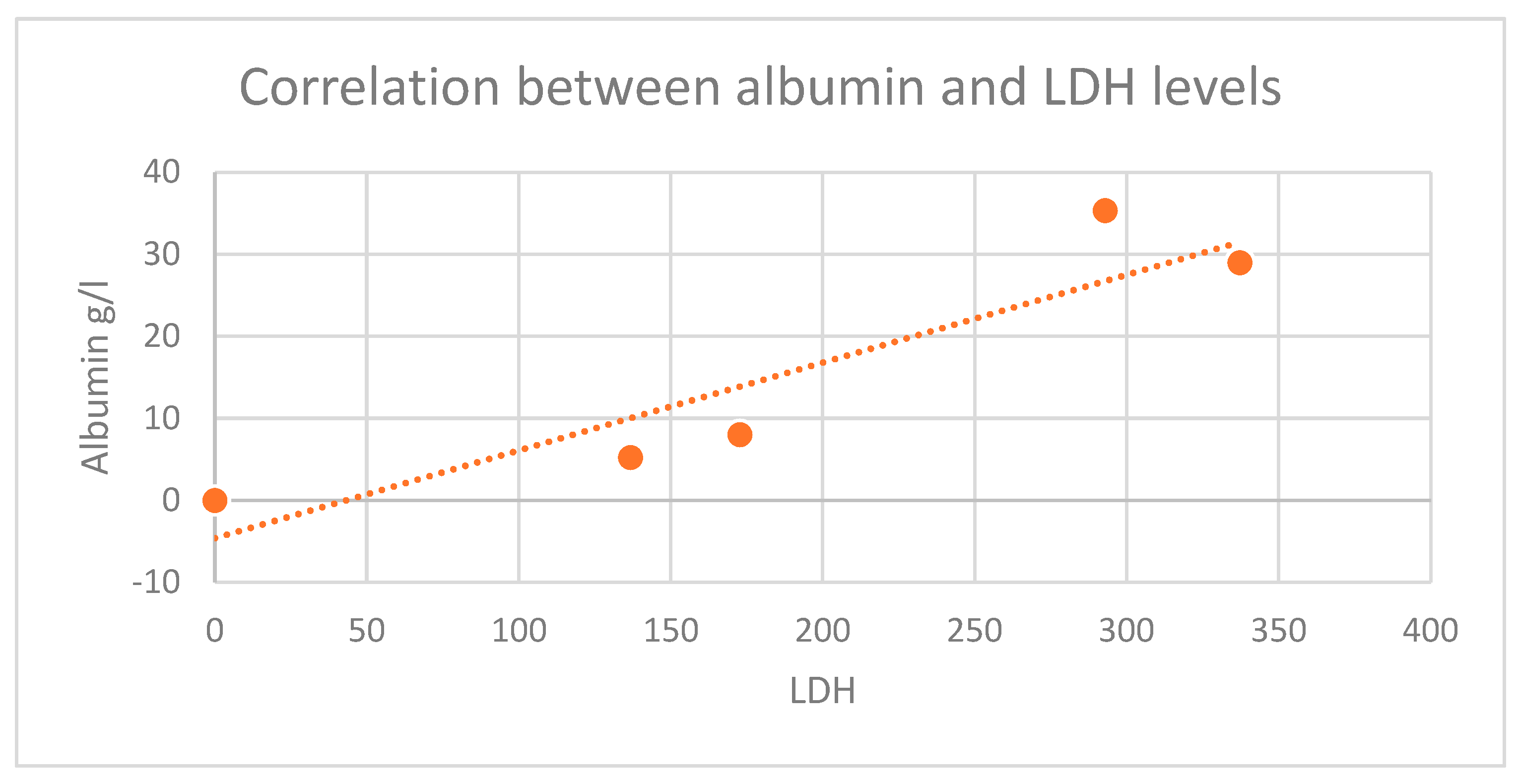
Figure 5.
Positive correlation between LDH and hemoglobin values (r=0.91).
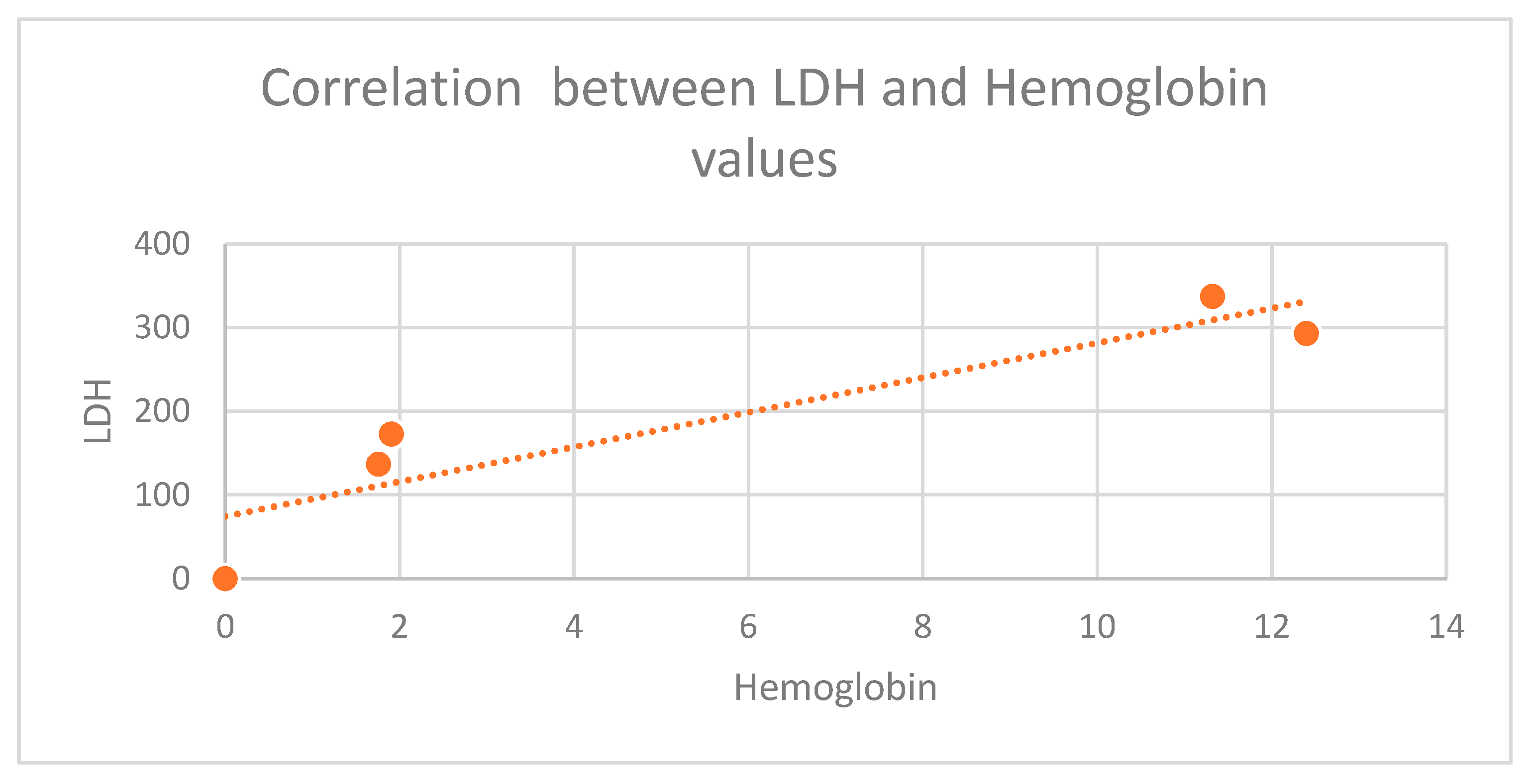
Figure 6.
Positive correlation between hemoglobin and albumin levels (r=0.99).
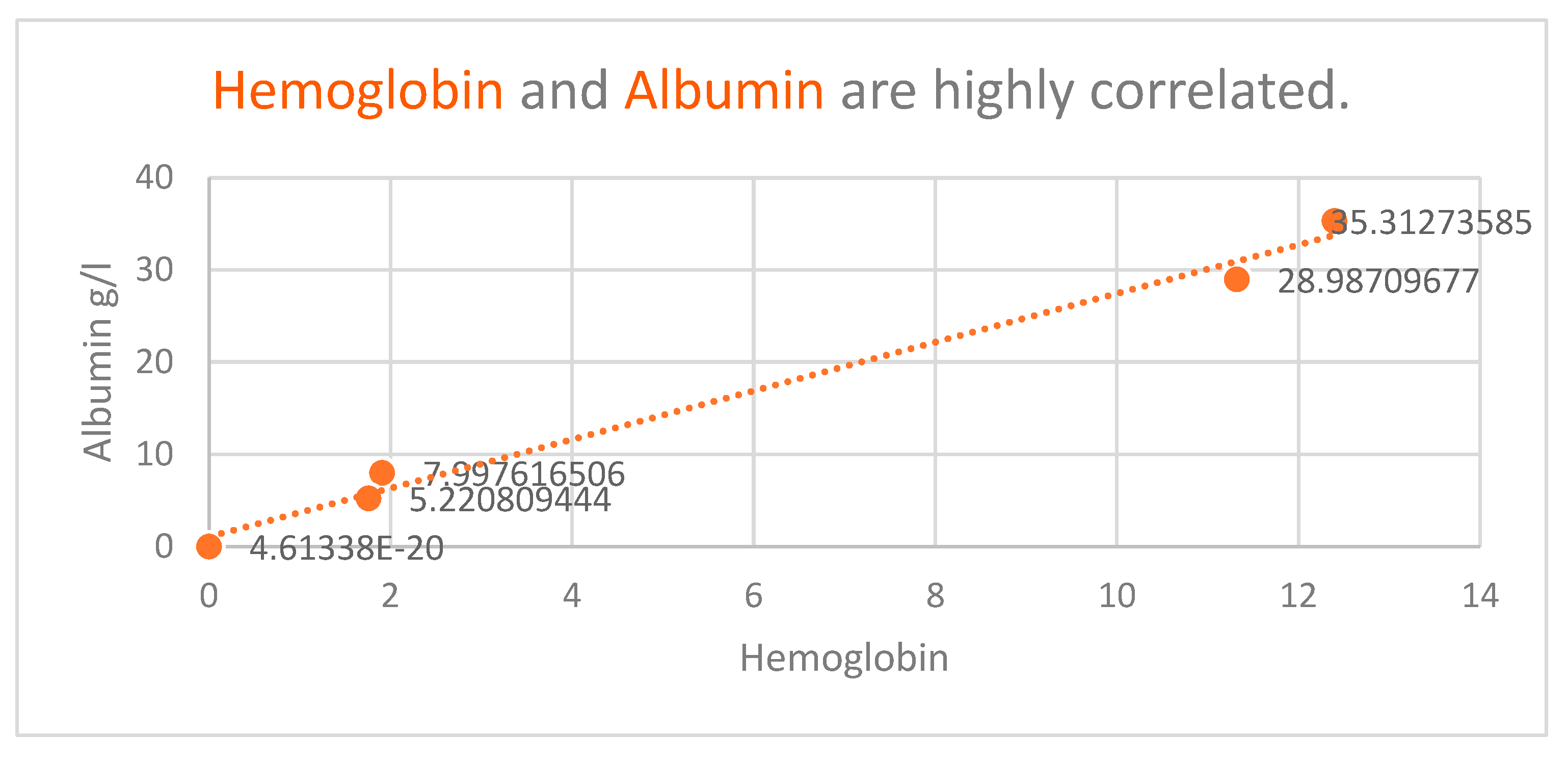
Figure 7.
CRP values in the study groups.
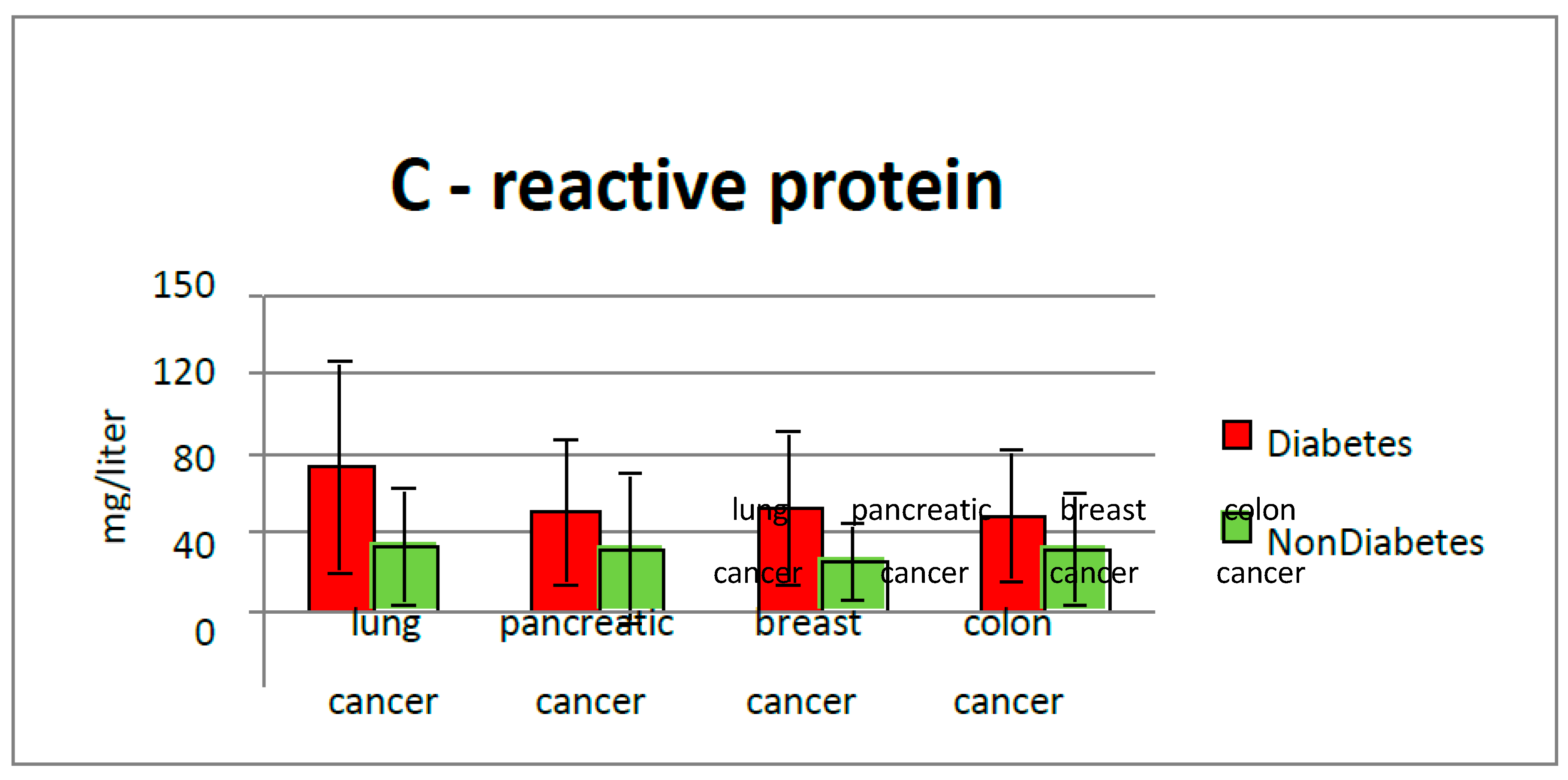
Figure 8.
CRP values in the study groups correlated with hemoglobin values.
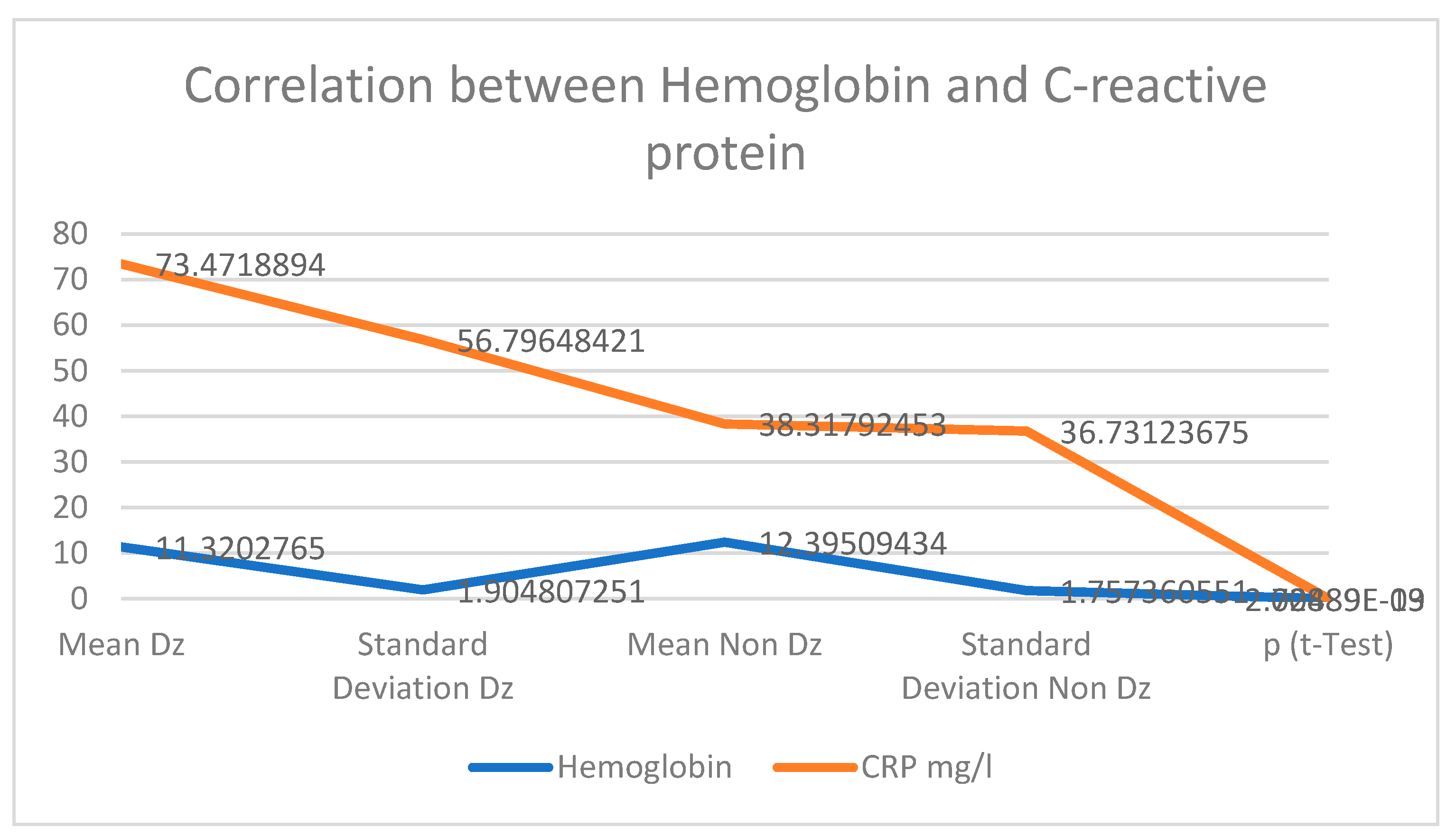
Figure 9.
Median survival rate in diabetic patients versus control group.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



