
Submitted:
18 July 2023
Posted:
19 July 2023
You are already at the latest version
Abstract
Asthma is a heterogeneous and very complex group of diseases, which includes different clinical phenotypes depending on symptoms, progression, exacerbation pattern or response to treatment among other characteristics. The allergic phenotype is the most frequent, especially in pediatric asthma. It is characterized by sensitization (production of specific IgE) to allergens, and frequent comorbidity with rhinitis and atopic dermatitis. An allergen is a substance that triggers the production of specific IgE antibodies in susceptible individuals, who present symptoms that will depend on the type and intensity of the allergenic load and the tissue where the interaction occurs. Airborne allergens cause their effects in the respiratory tract and eyes, and can be indoor or outdoor, perennial or seasonal. Although allergens such as mites, pollens or animal dander are generally considered as a single particle, it is important to note that they contain different molecules which could trigger distinct specific IgE molecules on different patients.The key points that a physician who treats asthma should be aware of are:
Keywords:
airborne allergens
; allergic inflammation
; asthma
; allergic rhinoconjunctivitis
; sensitization
; allergy
Introduction
Approximately 8.000 to 10.000 liters of air circulate daily through the respiratory tract, which may contain potentially pathogenic particles and microorganisms. The immune system is responsible for distinguishing the self from the foreign, continuously detecting antigens and particles that may be harmful so they can be effectively eliminated. This defensive process takes place by means of complex mechanisms that are perfectly coordinated in an orderly manner, in which numerous cells and biological mediators participate, triggering a controlled inflammatory response, which will end with the elimination of the threaten agent and the resolution of the inflammation.
Adaptive or antigen-specific immunity is based on the coordinated action of T and B lymphocytes in a system capable of maintain immunological memory that allows the development of a rapid response in case of re-exposure to a certain antigen. The basis of allergic diseases lies in an inappropriate adaptative response driven by T helper type 2 (Th2) lymphocytes against allergens, which leads to excessive production by B lymphocytes of isotype E immunoglobulins (IgE) specific to one or more of such allergens, triggering tissue damage.
From a clinical point of view, airborne allergens are major responsible for allergic rhinitis, conjunctivitis and asthma, chronic diseases that could be seasonal or perennial, affect quality of life and generate high health care costs. Allergic asthma is a multifactorial disease, in which genetic predisposition (atopy) is modulated by exposure to allergens, infections and environmental factors among others.
Atopy
The term atopy, from the Greek α (a) = out, without; τοποζ (topos) = place; and therefore, out of place, strange, illogical, was introduced by Coca and Cooke in 1923 (1) to describe the immediate cutaneous reactions of papule and erythema produced in response to allergens in patients with asthma and allergic rhinitis. Atopy was later defined as the genetic predisposition of some individuals to produce excessive amounts of specific IgE antibodies directed against environmental substances called allergens. In other words, it is the tendency of some individuals to develop IgE-mediated allergic diseases. This definition does not imply the presence of clinical symptoms, but only describes immunological reactivity and a risk of allergic disease.
Subpopulations of T helper lymphocytes Th1 and Th2.
Three types of helper cells are known to coordinate responses to intracellular parasites: Th1 (T helper lymphocyte), helminth (Th2) and extracellularly growing bacteria and fungi (Th17), with different cytokine production profiles. Th1 lymphocytes produce Interleukin 2 (IL-2), interferon gamma (IFN γ) and tumor necrosis factor β (TNF-β), promoting responses against intracellular germs due to their capacity to activate macrophages and other mechanisms of cellular immunity, in addition to inducing B lymphocytes to produce complement-binding antibodies. Th2 produce among others IL-4, IL-5, IL-13, whose main functions are to induce IgE antibody synthesis by plasma cells and eosinophil chemotaxis.
During fetal life there is an immunological shift towards Th2 in order to stop Th1 responses that could be toxic to the placenta, thus avoiding a possible miscarriage due to immunological rejection (it should not be forgotten that half of the genetic endowment of the fetus is allogenic, of paternal origin). After birth, there is a shift from the Th2 to the Th1 response in order to protect the organism against potentially pathogenic antigens, like virus and bacteria. Successive exposures to germs (pathogens or saprophytes) will consolidate the protective Th1 memory response. In contrast, in atopic children this change of cytokine pattern does not occur completely, enhancing the Th2 response and inhibiting the Th1 response, which favors the production of IgE and the allergic inflammatory response to common allergens.
Allergy vs allergic sensitization
The term Allergy, αλλοζ (allos) = other; εργον (ergon) = action, was proposed in 1906 by Von Pirquet (2). That "action of the other" alluded to the altered reaction (alter = other) of the immune system allergy sufferers to substances harmless to the rest of the population. The term allergy is usually synonymous with IgE-mediated immediate hypersensitivity, being the clinical expression of atopic predisposition, and includes asthma, rhinitis, conjunctivitis, atopic dermatitis and allergic reactions to food, drugs and hymenoptera venom. Both terms, atopy and allergy, are used interchangeably in research and clinical practice to refer to immunological processes related to allergic diseases, whose familial clustering suggests hereditary transmission. In order to facilitate clear communication between healthcare professionals, the European Academy of Allergology and Clinical Immunology (EAACI) recommended a nomenclature for allergy-related terms (3) , updated in 2003 by the World Allergy Organization (WAO) (4), which defines allergy as "a hypersensitivity reaction initiated by immunological mechanisms" and atopy as "the personal or familial tendency to produce IgE antibodies in response to low doses of allergens, usually proteins, and to develop typical conditions such as asthma, rhinitis or eczema".
It is important to distinguish between the term sensitization i.e., production of specific Ig E against allergens, demonstrable by skin prick test and/or determination of specific serum Ig E, and the term allergy, that implies that sensitization already produces clinical symptoms. An individual may present positive tests against a particular allergen for which he or she has never presented related symptoms, similarly, other patients resolve their symptoms spontaneously or after receiving immunotherapy, but they all continue to present positive tests, which would indicate that those individuals have acquired tolerance by immunomodulation, constituting what is called subclinical or asymptomatic sensitization.
Immunoglobulin E
In 1966, Kimishige and Teruko Ishizaka isolated in patients sensitized to ragweed pollen an immunoglobulin different from those already known, which specifically bound to the antigens of this pollen (5). In 1967, Johansson et al. studied a patient affected by myeloma, in whom they also found an immunoglobulin with characteristics different from those previously known (6). The equivalence of the globulin discovered simultaneously by the two groups of researchers was later proven, and after an international consensus meeting in 1968 it was named Immunoglobulin E (IgE), whose two main functions are defense against parasites and participation in the allergic reaction.
IgE is cytophilic, as its half-life is of 2-3 days when free in serum but is longer when bound to the surface of mast cells and basophils, suggesting that it is intended for local rather than systemic activity. Like immunoglobulins A, G, M and D, Ig E consists of 4 polypeptide chains linked by disulfide bonds. The two light L chains are identical to those of the other immunoglobulins, while the two heavy H chains are specific, giving to IgE the characteristic of binding to allergen epitopes via the Fab fragment (antigen binding) and to cells via the Fc fragment (crystallizable). L chains have a variable region (VL) and a constant region (CL). H chains have a variable region (VH) and four constants (CH). Allergens require at least two IgE binding epitopes to facilitate the cross-linking needed to activate mast cells and basophils (7).
Pathophysiology of allergic reaction
For an allergen to be capable of inducing sensitization via the respiratory route, it must overcome anatomophysiological barriers (mucociliary unit, epithelia and mucous membranes among others), and be phagocytized by antigen presenting cells (APC), such as the dendritic cell. Then, the APCs process the allergen and migrate to the secondary lymphoid organs, where they present them, bound to the Major Histocompatibility Complex type II, to the allergen-specific memory T-helper lymphocytes, which induce the differentiation and clonal expansion of allergen-specific Th2 lymphocytes. These Th2 cells secrete, among others, Interleukins IL-4 and IL-13, which induce B cells to produce allergen-specific IgE, IL-5 (that promotes eosinophilic inflammation), IL-9 and IL-13 ( important in bronchial hyperresponsiveness and remodeling). Repeated exposure to the allergen in a susceptible individual induces sensitization, a process in which specific IgE antibodies are produced, initially without causing symptoms. Such exposure can occur through percutaneous, respiratory, or digestive routes, and it is not known why some individuals become sensitized to allergens, or why diverse allergic patients can show different sensitization profiles to one or more protein components of a particular allergen source.
In successive re-exposures to the allergen, the inflammatory response is much more rapid as it is mediated by clones of allergen specific Th2 cells. The allergen (specifically its epitopes) interacts with IgE bound to the high affinity receptor (Fcε RI) on the surface of tissue mast cells or peripheral basophils, or to the low affinity receptors (Fcε RII) present on lymphocytes, platelets, and macrophages. Then cell activation and release of mediators occurs, which produce the typical symptoms of acute allergic reaction (bronchospasm, rhinitis, anaphylaxis). After repeated cycles of acute inflammation followed by repair, an infiltrate of resident cells (mainly neutrophils and eosinophils) is established, releasing cytokines which, by amplifying and prolonging the inflammation, chronify it, resulting in chronic manifestations of allergic respiratory diseases, such as bronchial hyperresponsiveness or nasal congestion, caused by allergic and non-allergenic substances such as viruses, tobacco smoke or cold air.
The Airborne Allergen
Ambient air is an example of an aerosol, which is defined as a system of solid and liquid particles dissolved in a gas. One liter of air contains a dynamic distribution of millions of particles that can remain floating in both solid and liquid form. All other environmental conditions being equal (humidity, temperature, air speed), the duration of the particles in suspension is inversely proportional to their size.
Allergens are proteins or glycoproteins of molecular weight between 5 and 100 kDa, which in most cases are water-soluble. Only a small percentage of all known animal and vegetable proteins are known as allergens (8). It has been suggested that the allergenicity of many proteins may be determined by their homology to helminth proteins that induce Th2 responses. (9). They show the characteristic of promoting the production of specific IgE antibodies (sensitization) and activating an IgE-mediated immune response in susceptible individuals, being innocuous in the majority of the population. Thus, only subjects with a personal predisposition to produce specific IgE to allergens will react abnormally, presenting symptoms that will depend on the type and intensity of the allergen load and the specific tissue where the interaction occurs (nose, eyes, bronchial or digestive tract). Such allergenic proteins could be structural proteins or enzymatic proteins, the latter being critical in the development of allergic sensitization and appear to be strongly associated with heightened allergenicity(10). Mites, cockroaches and molds possess strong proteolytic activity (11), that increase permeability and directly activate the airway epithelium, being transported through it to interact with immune cells, leading to increased inflammation (7). Finally, carbohydrate and lipid residues associated with allergenic proteins may act as adjuvants stimulating Th2 responses.
There are several types of allergens: pneumoallergens (inhaled), trophoallergens (ingested), occupational, drug allergens and hymenoptera venom. Airborne allergens cause their effects on the respiratory and ocular tracts and can be classified according to their area of exposure into indoor allergens (mites, epithelia, fungi, pests) or outdoor allergens (pollens, fungal spores), and according to the time of exposure into perennial or seasonal. Although allergens such as mites, pollens or animal epithelium are generally considered as a whole, it is important to note that only small portions (epitopes) of these substances can bind IgE, as a key and lock. There are also specific epitopes for other antibodies and cells. The size of pneumoallergen-carrying particles is important: those larger than 10-20 μm will be dropped in the nasal and conjunctival mucosa, producing rhinoconjunctivitis; between 2 and 5 μm will be deposited in the tracheobronchial tree, producing asthma; and those smaller than 1 μm reach the alveoli.
The physician who diagnoses and treats allergic respiratory diseases must have knowledge of the characteristics (geographical distribution, concentration, seasonality, avoidance reommendations) of both indoor and outdoor allergens. Most respiratory allergens meet certain characteristics (Table 1) and the requirements postulated by August Thommen in 1931 (Table 2).
Major and minor allergen. Panallergen, cross-reaction.
The main (genuine) allergen of a substance is the one that induces a cutaneous reaction or the production of specific IgE in more than 50% of patients sensitized to it. They are usually the most abundant or those with the highest sensitizing capacity, in addition to being genuine or specific to the allergenic substance. On the other hand, minor allergens have a recognition frequency of less than 50% of sensitized patients, as is the case with panallergens, which are responsible for cross-sensitization between different substances. This definition is not exclusive, and an allergen can behave as a minor allergen in a given population and as a major allergen in another. In general, major allergens are usually species-specific, while minor allergens include various panallergens. Circulating IgE in the serum of allergic individuals can recognize different allergens in a substance, which can be demonstrated by immunoblotting.
International nomenclature of allergens
More than 16000 protein families have been described, of which only some are allergenic. Allergens are identified according to WHO/IUIS (International Union of Immunological Societies) regulations, so that for each substance the first three letters of the genus are used followed by the first letter of the species and a number according to the order of characterization. Thus, Lol p1 is the first allergen that was identified from the grass Lolium perenne. The Allergome platform (www.allergome.org) is a continuously updated database that collects information on all known allergen sources, currently more than 2500, with more than 3200 identified allergenic molecules.
Indoor Airborne Allergens
Mites
Mites are microscopic arthropods about 300 µm long, blind, and photophobic, that exchange O2 and CO2 through their body surface. Like other decomposer insects, they select food that has been pre-decomposed by fungi. Their life cycle from egg to adult mite is about 30 days. Mites belong to the class Arachnida, subclass Acari, Order Astigmata. There are two groups of dust mites, house dust mites (HDMs) and storage mites (SMs), that have been identified in the household environment(12) The most relevant families for allergenic purposes are Pyroglyphidae (Dermatophagoides pteronyssinus, Dermatophagoides farinae and Euroglyphus mainei), Glycyphagidae (Glycyphagus domesticus and Lepidoglyphus destructor), Echimyopodidae (Blomia tropicalis) and Acaridae (Tyrophagus putrescentiae, Acarus siro). Allergens from mites have a high sensitizing capacity, constituting by their frequency and ubiquity the main inner pneumoallergen in asthma.
The ideal habitat for Dermatophagoides is domestic environment in areas with temperatures above 25°C and relative humidity higher than 75-80%, conditions that occur in homes in coastal areas. They grow in dust, accumulate in carpets, rugs, mattresses, pillows and curtains, and feed on human flaking. In this type of environment, they reach average concentrations of 100 to 500 mites per gram of dust, where concentrations above 100 mites/gram of dust are considered to initiate allergic responses in sensitized individuals. At more than 1,000 m above sea level and/or in arid environments, Dermatophagoides population is drastically reduced until it disappears in situations of ambient humidity below 55%, which demonstrates their low resistance to desiccation(13).
Different allergenic components of dust mite extracts could activate innate immunity through triggering pattern recognition receptors (PRR), and then lead to allergic inflammation(12). The most important allergens of the mites are found both in feces (each mite produces about 10-20 feces particles per day) and bodies. The diameter of fecal particles ranges from 15-30 microns, so large to remain airborne for more than a few minutes. The most important allergens (groups 1 and 2), act as proteases(14), which in addition to induce the production of specific IgE, are able to detach elements of the respiratory epithelium, making it more permeable to allergens and other irritating particles, acting as adjuvants in Th2 allergic inflammation, and increasing bronchial hyperresponsiveness.
Even if the level of exposure to mites is reduced, there is still a threshold capable of producing allergic sensitization and/or symptoms. Only a drastic decrease in mite exposure can help to improve the control of asthma and rhinitis, as showed Boner et al (13), with Italian children with asthma who improve when staying in an allergen-free environment at high altitude, at the Alps. In addition to less exposure to dust mites, this mountain environment also favors lower levels of pollens and fungi, less environmental pollution, and more sun exposure, with immunomodulatory and anti-inflammatory effects (15). Other avoidance measures are not as effective, because although they can reduce mite concentration, they do not do so to a sufficient level to have an impact on symptoms reduction (Table 3). There is another handicap, which is that since mites are invisible to the human eye, it is difficult for patients and families to perform avoidance measures that are not noticeable in real life.
Pet dander
The origin of the dog dates back to 20,000-30,000 years ago. Coming from the wolf (Canis lupus lupus), a symbiosis was established in which both species gained: the dog got food and shelter, and the human protection, and both got emotional companionship, becoming progressively a domestic animal (Canis familiaris). Domestic cats (Felis domesticus) are descended from the African wild cat (Felis silvestris lybica), which was domesticated about 9,000 years ago, especially by the peoples of the Near East and Egypt, in a mutually beneficial relationship where the felines avoided rodent pests that ruined granaries and in return obtained food and care. In recent years we are witnessing an exponential increase in the number of pets, which previously lived outside the home, but now stay indoors (often in bedrooms), even when the owners are not at home. In the USA there are 70% of households (90,5 million families) with pets (total of approximately 85 million cats and 78 million dogs) (17), and 90% of Americans consider them to be part of the family(18).
About 10% of the population in developed countries presents allergy to dog and/or cat, although only 50% of those own a pet. The explanation for this sensitization is that these are ubiquitous allergens, acting as hidden "mines", due to their presence in private and public places such as transport, leisure areas and even hospitals. Thus, the presence of dog and cat allergens has been demonstrated in homes (19) and automobiles (20) whose owners do not have furry pets, in concentrations sufficient to generate sensitization and even allergy (established at 1 and 8 mcg/g for Fel d1 and 2 and 10 mcg/g for Can f1 respectively). These allergens, especially Fel d1, can float in the air for several days (21), and even after the pet is removed from the home, these allergens persist for months in the environment, making it a public health problem, because the higher the number of people with pets, the greater levels of allergens are transferred, growing their load in public and private common spaces.
In cat allergy the clear protagonist is Fel d1 or secretoglobin, since about 95% of patients are sensitized to this allergen present perianal and sebaceous glands and in saliva. It is carried by particles larger than 9 microns, but it is also transported by particles < 5 microns, so they are able to reach the distal bronchi and can induce asthma besides rhinitis symptoms. In contrast to the cat, the sensitization profiles against the dog are more diverse. There is no single predominant allergen, the most frequent being Can f1, f5 and f2. Can f1 and Can f2 are lipocalins coming from saliva, and act as ligands transporting pheromones, steroids or retinol. Mammals express exogenous lipocalins (saliva, skin, urine), whereas humans have endogenous lipocalins. Given the homology between human lipocalins and those of other mammals, the human immune system inhibits T cell responses so as not to create a conflict of autoimmunity against its own. Such inhibition would favor allergic B/Th2 responses, to avoid autoimmune responses potentially dangerous (22). Another major dog allergen is Can f5, androgen-regulated prostatic kallikrein, which is greatly diminished in neutered males and nonexistent in females, so that subjects monosensitized to Can f5 will only show symptoms with unneutered male dogs. It may show cross-reactivity with human prostate-specific antigen, being responsible for allergic reactions to semen in women sensitized to Can f5 (23).
Allergens are carried by particles present in saliva, dander, urine and hair. These particles, depending on their weight, are deposited on the floor and furniture or remain suspended in the air. Differences have been observed in the geometric means of Can f1 levels in the hair and skin of different breeds, but there is also a large variability (up to x100 and x1000) between individuals of the same breed(24). These differences may be influenced among others by the number of dogs, size, cleanliness of the home, age, hydration, and frequency and type of washing. No differences have been observed in the levels of Can f1 in the dust in suspension in the homes, which are those that really impact on the respiratory system, regardless of the breed of dog. Therefore, there is no evidence to confirm that there are hypoallergenic breeds(25).
Sensitization to pet allergens is bell-shaped, i.e., at both low and high levels of exposure there is a lower frequency of sensitization, while at medium levels of exposure, this frequency is higher (26). On the other hand, immunological tolerance (understood as levels of specific protective IgG) is acquired at high levels of exposure (26). This fact translates clinically into subjects with a high level of allergen exposure at home who acquire tolerance and barely show symptoms as long as they maintain permanent contact with their pet, but who may lose it in case of absence of it. This is what happens in the so-called "thanksgiving" phenomenon, whereby students who have been away from home for a long time, without contact with pets, return home and show symptoms again. Conversely, asthmatic children due to cat allergy who are on vacation at home, when returning to classrooms with a high percentage of cat owners show more symptoms and use of medication (27). In this context, an elegant Swedish study showed that when pupils changed clothes when entering the school, the concentration of allergens on the walls and air in the classroom, and on pupils' clothes was similar to that in other classrooms where all pupils had been banned from having pets in their homes, so that may be a measure to consider (28).
A consensus of Spanish allergists (29) establishes recommendations on the diagnostic and therapeutic management of dog and cat allergy, among which there are avoidance measures (Table 4). Separately such measures do not have sufficient evidence of efficacy, so they should be applied in combination, in order to reduce allergen exposure.
Cockroaches
Cockroach allergy is an important risk factor for hospital admissions, ER visits and asthma morbidity, exerting a greater impact on the latter than dust mites or pets (30). The prevalence of cockroach allergy ranges in the United States from 17 to 41%, while in Europe 25% of asthmatic children are sensitized to cockroaches (31). Allergens from cockroaches are detected in 85% of homes in inner cities in the United States, where 60-80% of asthmatic children show a positive prick to cockroach extract (32).
Of the approximately 4000 species of cockroaches, the most frequently encountered in the domestic environment and therefore of allergenic interest are Blatella germanica, Periplaneta americana and Blatta orientalis. They are insects that live in humid, dark and temperate areas and feed on plant, paper, tissues, insect remains and food. Their allergens come from dried remains of the cytoskeleton, secretions, eggs and fecal matter, which can become airborne and cause perennial allergic symptoms. After extermination, allergens can remain in the environment for several months, carried in particles < 10 µm, with the capacity to penetrate the respiratory tract. The main allergens (33) are Bla g1 (30-50% of all sensitized patients) with cross-reactivity to tropomyosin from other arthropods, Bla g2 (60-80%), Bla g4 (60%) and Bla g5 (70%). These allergens can directly activate bronchial epithelial cells, inducing the production of cytokines (TSLP, IL-25, IL-33) and chemokines with the ability to recruit inflammatory cells. In addition, most of these allergens contain glycans, which enable them to activate mast cell-bound IgE responses.
They produce perennial asthma, with worsening in winter, usually without clear exposure to cockroaches. It is an allergenic source that usually goes unnoticed because it is not usually part of the battery of extracts used in the diagnosis by prick test. Thus, patients can remain undiagnosed for some time, so its detection will depend on the level of suspicion of the physician who request a prick test and/or specific IgE, even in the absence of visible pests in the patient's home.
Outdoor Airborne Allergens
Pollens
Pollens are the viable male gametes, essential for the reproduction of most plants. Their function is to reach, through a process called pollination, the female part of a flower of the same species and fertilize it. Pollination can be entomophilous, carried out by insects, or anemophilous, with the wind being responsible for disseminating the pollen grains through the atmosphere. Anemophilous pollens are considered the most relevant allergens in the group of respiratory allergies, and in the specific case of asthma they occupy the second place after mites.
Their most important characteristic is seasonality, so that the atmospheric concentration of a pollen occurs in certain months of the year, usually during spring and summer, depending on the geographical and climatic environment. Precipitation during autumn and winter and the heat during the preceding months influence the germination and growth of plants, and therefore the amount of pollen released. The main anemophilous plant species are grasses, trees and weeds, whose pollen covering (exine) provides them with resistance to adverse environmental conditions. Poacea (grasses) are the most important family causing pollen allergy worldwide. The most relevant trees are those of the phagales order (birch, hazel, and oak), predominant in Northern Europe, while in Mediterranean Europe olive pollen (Olea) is of special interest. The best-known weeds are Parietaria and Artemisia, both in Europe, and Ambrosia (ragweed) in North America. For practical purposes, physicians should be aware of the pollination periods of the different allergenic plants in the geographic area where they practice, as exposure to pollen peaks increases risks of allergic and asthmatic symptoms(34). As different allergenic sources pollinate simultaneously, it can be difficult to identify the cause of a patient's symptoms.
Airborne pollen concentrations at ground level are higher on windy and sunny days, and follow a circadian rhythm, being highest in the morning, coinciding with pollen emission, and in the evening, as less warm air descends from the upper layers of the atmosphere. The pollen calendar consists of a graphic representation that summarizes the annual distribution of the main types of pollen prevalent in a specific geographical location, data that are of special relevance for patients and physicians when establishing diagnostic, therapeutic and preventive strategies. Pollen grains, with a diameter ranging from 10 to 100 µm, are retained in the conjunctiva and upper respiratory tract, mainly causing rhinoconjunctivitis. They are too large to access the bronchi, except when exposed to osmotic rupture or environmental degradation, which releases pollen allergens that are integrated into particles smaller than 5-8 µm, becoming bioaerosols with a significant allergenic load. (35). Such sub-pollen particles remain airborne for a longer time (although they may go undetected by traditional detection methods) and can reach the bronchi, inducing bronchial constriction (35), especially if physical exercise and/or oral respiration are performed. Moreover, their enzymes can produce reactive oxygen species (36).
It is important that patients and their families know the symptoms of both asthma and allergic rhinoconjunctivitis so that they can be detected and treated as early as possible. Each patient with pollinosis should have an action plan established by the physician, which includes a daily (preventive) treatment, and "rescue" treatments to be used in case of the appearance of symptoms. Apart from pharmacological treatments, the only measures that can slow down the evolution of seasonal allergy are allergen avoidance and specific immunotherapy. Although it is practically impossible for patients to avoid total contact with allergens coming from pollen, some general measures should be considered (Table 5), the main one being to know which pollen produces their symptoms, as well as the pollination period of the species in their area of residence, information available on the Internet or specific Apps. FFP2 self-filtering masks should be used, which retain 95% of airborne particles larger than 0.1 µm. On the other hand, there are intranasal filters, with pores of 1 µm. Surgical masks are not suitable for filtering environmental pollen.
Pollen is a complex mixture of allergenic proteins and other non-allergenic ingredients. Traditionally, the etiological diagnosis of respiratory allergy has been based on clinical history and skin prick testing, using extracts containing different allergens of pollen, and on the determination of serum IgE levels specific for this mixture of allergens. These tests are very sensitive but less specific, and to determine the individual sensitization profile of a particular patient it is necessary to use molecular diagnostics, also known as Component Resolved Diagnosis (CRD) (37). The component is ultimately responsible for the allergic reaction, so the diagnosis should be aimed at identifying the specific IgE responses to these individual allergenic components. In addition, allergen microarrays with more than 100 purified allergen molecules enable simultaneous IgE measurement using only minute amounts of blood.
Most pollen allergic to pollen begin to have symptoms at 6-7 years of age. However, some children start earlier, from 3-4 years of age, and in other cases it manifests at later ages. In at-risk preschoolers (with specific IgE sensitization to pollens and with pollinic parents), immunological intervention by means of specific immunotherapy (SIT) in a preventive manner, before the onset of rhinoconjunctivitis and/or asthma, could induce immunotolerance(38), taking advantage of an immunological window of opportunity at these ages, this measure being more effective than mere allergen avoidance.
Molds
It is estimated that more than 1 million fungal species exist, although only 80,000 have been described, of which 112 genera are thought to contain allergens (39). There are 4 genera associated with the development of respiratory allergy in humans: Alternaria, Cladosporium, Penicillium and Aspergillus. Fungi can behave as saprophytes, symbiotics or parasites. They live on decaying organic matter, soils, textiles, food, and plants, and require an optimum temperature of 25º C (4º - 40º C) for their development. The genera Alternaria and Cladosporium are the most frequently associated with allergic respiratory diseases, with Alternaria being the one with the highest prevalence of sensitization. Despite Alt a1 being the A. alternata major allergen, other allergens, such as Alt a 6 or Alt a 14, have been suggested to be included in the diagnosis panel of fungal allergy (40). The prevalence of sensitization to molds in the general population ranges between 3-10%, rising to 10-20% in patients with asthma and/or rhinitis (39), being more frequent in childhood. In addition, by stimulating the innate immune system, they can enhance the inflammation caused by other unrelated allergens, such as pollen or mites, which polysensitization is frequent.
Molds can act as indoor allergens, and since light promotes sporulation (asexual reproduction), also as outdoor allergens, predominantly in agricultural regions. Mycelia and fungal spores contain allergenic material. Fungal spores show a broad spectrum of different shapes and sizes, ranging from less than 2 to 250 μm, and constitute the largest component of all environmental aerobiological particles in our enviroment(41), exceeding the concentration of pollen grains. Spore concentration is strongly influenced by climatic factors (temperature, rainfall, winds, relative humidity) and circadian patterns (light and dark). The highest levels in the northern hemisphere are found between June and October, when nutritional sources are available, and decrease in winter. As with pollens, spore concentration does not fully correlate with human exposure, because there are fragmented spores and submicron particles unaccounted for in the samplers that contain appreciable amounts of allergens capable of depositing in the respiratory tract. Spore concentrations of Alternaria equal or greater than 100 spores/ m3 are believed to evoke allergic symptoms whereas the equivalent value for Cladosporium is estimated to be 3,000 spores/m3(39). Molds play an important role in the development of respiratory allergy, as they are associated with rhinitis, asthma and in particular severe asthma (42), ER visits, hospitalizations, and ICU admissions. A meta-analysis (43) found an increased risk of respiratory allergy in children exposed early to fungi/dampness, which should be taken into account when establishing primary prevention measures for respiratory problems associated with indoor allergens.
Relationship between Environmental Exposure and Respiratory Allergy
The interaction between genetic predisposition and external factors programs immune function by early in life, after moving from a protective intrauterine environment to external exposures through the skin, respiratory system, and digestive tract (44). During the last months of pregnancy and the first months of extrauterine life, immunological maturation takes place, producing the first responses to allergens presented to the fetus through the placenta. Depending on a series of events, the child may be marked for life with an adequate Th2/Th1 balance, or with a Th2 predominance typical of atopic patients, which will favor the appearance of allergic problems later.
The increase in the prevalence of allergic diseases in Western lifestyle countries has been described as a real “epidemic”. The causes of this increase are not fully known, and many hypotheses have been put forward to explain this phenomenon, most related to changes in lifestyle habits and environmental and family factors. Among other aspects, the Western lifestyle is characterized by polluted (indoor and outdoor) environments, changes in the population's dietary habits and lifestyle: reduction of typical childhood infections, sedentarism, consumption of ultra-processed food, obesity, exposure to tobacco smoke, and increased time spent indoors, among other factors. Numerous investigations have attempted to associate the increased prevalence of allergic diseases with exposure to microbial exposure, traffic-related air pollution (TRAP), or tobacco smoke (44). The use of antibiotics during childhood has been associated with a higher prevalence of asthma and other allergic diseases (45), which could be due to an alteration the microbiome.
Human activity, with the use of intensive crops, fertilizers, and transgenic species, is responsible for the increased production of pollen allergen components and released into the atmosphere. For years, temperatures have been rising worldwide, and this warming is causing pollination periods to start earlier and persist longer and more intensely, as well as increasing spore production and modifying the allergenicity of fungi (46) . It is also observed that different plant species are progressively spreading their habitats to areas where they were not present before. An example of this is the ragweed, native to Eastern Europe, for which it is predicted that in the coming decades we will see a significant increase in the frequency of sensitization in the Western European population (47). There are complex interactions between air pollution and climate change on the one hand, allergens and adjuvants on the other, and the immune system they influence, involving physical, chemical and biological factors(48).
The anthropocenic era is also characterized by a sharp increase in the concentration of carbon dioxide, ozone, nitrogen oxides and particulate matter from fossil fuels. Pollution is an important cause of respiratory tract symptoms in both atopic and non-atopic population. The increase in the prevalence of allergic diseases in recent decades has been paralleled by the replacement of coal by diesel as an energy source, which has led to a significant decrease in smog, but also to a change in the composition of particulate pollutants. These particles, small in mass but with a large surface area, bind polyaromatic hydrocarbons that have very important biological effects, including increased T-lymphocyte response to allergens. This contributes to the fact that the prevalence of pollinosis is twice as high in urban areas as in rural areas, even though pollen concentrations are much higher in the latter (49). The first description of the influence of diesel engine fumes on the increased prevalence of pollinosis was made by Dr. Muranaka's et al in 1986, after observing in a murine model how the IgE antibody response to Japanese cedar pollen increased significantly when exposed to pollen mixed with diesel particles (50). Diaz Sanchez et al performed nasal challenge with ragweed pollen mixed with diesel pollutants in patients allergic to such pollen. They found that the increase in specific IgE present in nasal secretion was twenty times greater than the increase produced after nasal challenge with non-diesel ragweed pollen. (51). There are several mechanisms by which diesel can enhance the allergic response and thus the symptoms of rhinitis and asthma:
- By binding aeroallergens, which allows to their higher concentration and permanence in the air.
- Decreasing mucociliary clearance and increasing permeability of the respiratory epithelium to allergens, which thus remain longer in the respiratory mucosa and therefore have greater exposure to the immune system.
- Increasing the allergenicity of pollen and the production of chemical mediators responsible for allergic reactions and airway inflammation.
Allergen Avoidance in Allergic Respiratory Diseases
The route of exposure and the amount of allergen determine the risk of allergic sensitization. Thus, exposure by the digestive route tends to generate tolerance mechanisms more easily, whereas the transdermal or respiratory route involve a greater risk of sensitization (52).
Allergen avoidance is a preventive measure at three levels:
- Primary, in at-risk patients (with a family or personal history of atopy).
- Secondary, in sensitized patients who have not yet presented associated symptoms (or these are mild).
- Tertiary, in allergic patients, to reduce the risk of symptom exacerbations.
Avoidance measures may fail due to a perceived lack of efficacy on symptom reduction or lack of time needed to achieve sufficient allergen reduction. The efficacy of different methods is difficult to establish, and most have low levels of evidence. The effect of interventions is limited, and meta-analyses may show partial beneficial results in some parameters (i.e. nasal symptoms, quality of life), but not in others (i.e. lung function, bronchial symptoms). Such interventions are included within a series of general measures grouped in health education, such as knowledge of their own disease, exacerbation triggers, symptom recognition, self-management, and inhaled medication administration technique, among others.
Treatment of Allergic Respiratory Diseases
There are several levels of respiratory allergy treatment (Figure 1), ranging from less to more allergen-specific:
- Symptomatic treatment: antihistamines (oral or topical on nasal or conjunctival mucosa), inhaled bronchodilators. They relieve symptoms temporarily, so they are used as rescue medication.
- Anti-inflammatory treatment: leukotriene receptors antagonists (oral), and glucocorticoids (nasal, inhaled) used preventively on a perennial or seasonal basis, depending on the type of respiratory allergy. Systemic corticosteroids are reserved for the treatment of asthma attacks or in the maintenance of severe asthma not controlled with other treatments.
- Biological treatments: directed against cytokines or IgE, which act as therapeutic targets in the different subtypes (endotypes or phenotypes) of asthma. As they are directed against specific therapeutic targets, they are not able to control all the clinical and functional aspects that characterize asthma, nor completely eliminate the risk of future exacerbations. Currently, none of the biologicals approved for the treatment of severe asthma demonstrated any disease-modifying effect(53), as this type of treatment is effective as long as it is administered, but no permanent effect has been demonstrated after the treatment is stopped.
- Immunotherapy: with the drugs of the previous sections used in monotherapy or in combination, some intermediate targets (biological drugs) or the consequences (anti-inflammatory and symptomatic treatments) of respiratory allergy would be partially treated, but not the etiology (inflammation of allergic cause). In the case of respiratory allergy, pharmacological and biological treatments should be combined with allergen-specific immunotherapy (AIT), consisting of the administration of repeated doses of allergenic extracts during 3 to 5 years, to induce prolonged immunological tolerance to the responsible allergens. AIT is currently the only treatment capable of altering the natural history of allergic diseases(54), preventing the development of asthma in patients with rhinoconjunctivitis (55) and the acquisition of new sensitizations in monosensitized patients(38). Since it has been shown that most subjects with allergic sensitization before the age of 8 will develop rhinitis and/or asthma before adulthood(56), those immunological changes occurring at this window of opportunity could lead to tolerance to the allergen, which would be accompanied by a reduction in symptoms and in the need for medication and other health resources, as well as an increase in the quality of life perceived by the patient. In a revision of five metanalysis, AIT proved to be at least as potent as pharmacotherapy in controlling the symptoms of seasonal allergic rhinitis as early as the first season of treatment(57).
Conflicts of Interest
The authors declare no conflict of interest.
References
- Coca, A.F.; Cooke, R.A. On the Classification of the Phenomena of Hypersensitiveness. The Journal of Immunology. 1923, 8, 163–182. [Google Scholar] [CrossRef]
- Kay, A.B. 100 years of “Allergy”: Can von Pirquet’s word be rescued? Clinical Experimental Allergy. 2006, 36, 555–559. [Google Scholar] [CrossRef]
- Johansson, S.G.O.; Hourihane, J.O.; Bousquet, J.; Bruijnzeel-Koomen, C.; Dreborg, S.; Haahtela, T.; et al. A revised nomenclature for allergy: An EAACI position statement from the EAACI nomenclature task force. Allergy. 2001, 56, 813–824. [Google Scholar] [CrossRef]
- Johansson, S.G.O.; Bieber, T.; Dahl, R.; Friedmann, P.S.; Lanier, B.Q.; Lockey, R.F.; et al. Revised nomenclature for allergy for global use: Report of the Nomenclature Review Committee of the World Allergy Organization, October 2003. Journal of Allergy and Clinical Immunology. 2004, 113, 832–836. [Google Scholar] [CrossRef]
- Ishizaka, K.; Ishizaka, T.; Hornbrook, M.M. Physico-chemical properties of human reaginic antibody. IV. Presence of a unique immunoglobulin as a carrier of reaginic activity. J Immunol. 1966, 97, 75–85. [Google Scholar] [CrossRef]
- Johansson, S.G.; Bennich, H. Immunological studies of an atypical (myeloma) immunoglobulin. Immunology. 1967, 13, 381–394. [Google Scholar]
- Scheurer, S.; Toda, M.; Vieths, S. What makes an allergen? Clinical & Experimental Allergy. 2015, 45, 1150–1161. [Google Scholar]
- Radauer, C.; Bublin, M.; Wagner, S.; Mari, A.; Breiteneder, H. Allergens are distributed into few protein families and possess a restricted number of biochemical functions. Journal of Allergy and Clinical Immunology. 2008, 121, 847–852.e7. [Google Scholar] [CrossRef] [PubMed]
- Fitzsimmons, C.M.; Falcone, F.H.; Dunne, D.W. Helminth Allergens, Parasite-Specific IgE, and Its Protective Role in Human Immunity. Front Immunol. 2014, 5. [Google Scholar] [CrossRef] [PubMed]
- Matsumura, Y. Role of Allergen Source-Derived Proteases in Sensitization via Airway Epithelial Cells. J Allergy (Cairo). 2012, 2012, 1–11. [Google Scholar] [CrossRef] [PubMed]
- Gershwin, L.J. Effects of allergenic extracts on airway epithelium. Curr Allergy Asthma Rep. 2007, 7, 357–362. [Google Scholar] [CrossRef] [PubMed]
- Yu, S.J.; Liao, E.C.; Tsai, J.J. House dust mite allergy: Environment evaluation and disease prevention. Asia Pac Allergy. 2014, 4, 241–252. [Google Scholar] [CrossRef] [PubMed]
- Boner, A.L.; Peroni, D.G.; Piacentini, G.L.; Venge, P. Influence of allergen avoidance at high altitude on serum markers of eosinophil activation in children with allergic asthma. Clinical Experimental Allergy. 1993, 23, 1021–1026. [Google Scholar] [CrossRef] [PubMed]
- Reithofer, M.; Jahn-Schmid, B. Allergens with Protease Activity from House Dust Mites. Int J Mol Sci. 2017, 18, 1368. [Google Scholar] [CrossRef] [PubMed]
- Rijssenbeek-Nouwens, L.H.; Bel, E.H. High-altitude treatment: A therapeutic option for patients with severe, refractory asthma? Clinical & Experimental Allergy. 2011, 41, 775–782. [Google Scholar]
- Global Initiative for Asthma. Global Strategy for Asthma and Prevention. 2022. Available online: www.ginasthma.org (accessed on 28 June 2023).
- Insurance Information Institute. Facts + Statistics: Pet Ownership and Insurance | III [Internet]. Available online: https://www.iii.org/fact-statistic/facts-statistics-pet-ownership-and-insurance#top (accessed on 28 June 2023).
- YouGov® US. Most pet owners say their pets are part of the family [Internet]. 2019. Available online: https://today.yougov.com/topics/society/articles-reports/2019/12/13/how-americas-pet-owners-feel-about-their-furry-fri (accessed on 28 June 2023).
- Arbes, S.J.; Cohn, R.D.; Yin, M.; Muilenberg, M.L.; Friedman, W.; Zeldin, D.C. Dog allergen (Can f 1) and cat allergen (Fel d 1) in US homes: Results from the National Survey of Lead and Allergens in Housing. Journal of Allergy and Clinical Immunology. 2004, 114, 111–117. [Google Scholar] [CrossRef]
- Neal, J.S.; Arlian, L.G.; Morgan, M.S. Relationship among house-dust mites, Der 1, Fel d 1, and Can f 1 on clothing and automobile seats with respect to densities in houses. Annals of Allergy, Asthma & Immunology. 2002, 88, 410–415. [Google Scholar]
- Custovic, A.; Simpson, A.; Pahdi, H.; Green, R.M.; Chapman, M.D.; Woodcock, A. Distribution, aerodynamic characteristics, and removal of the major cat allergen Fel d 1 in British homes. Thorax. 1998, 53, 33–38. [Google Scholar] [CrossRef]
- Virtanen, T.; Kinnunen, T.; Rytkönen-Nissinen, M. Mammalian lipocalin allergens - insights into their enigmatic allergenicity. Clinical & Experimental Allergy. 2012, 42, 494–504. [Google Scholar]
- Basagaña, M.; Bartolomé, B.; Pastor, C.; Torres, F.; Alonso, R.; Vivanco, F.; et al. Allergy to human seminal fluid: Cross-reactivity with dog dander. Journal of Allergy and Clinical Immunology. 2008, 121, 233–239. [Google Scholar] [CrossRef]
- Vredegoor, D.W.; Willemse, T.; Chapman, M.D.; Heederik, D.J.J.; Krop, E.J.M. Can f 1 levels in hair and homes of different dog breeds: Lack of evidence to describe any dog breed as hypoallergenic. Journal of Allergy and Clinical Immunology. 2012, 130, 904–909.e7. [Google Scholar] [CrossRef] [PubMed]
- Butt, A.; Rashid, D.; Lockey, R.F. Do hypoallergenic cats and dogs exist? Annals of Allergy, Asthma & Immunology. 2012, 108, 74–76. [Google Scholar]
- Platts-Mills, T.; Vaughan, J.; Squillace, S.; Woodfolk, J.; Sporik, R. Sensitisation, asthma, and a modified Th2 response in children exposed to cat allergen: A population-based cross-sectional study. The Lancet. 2001, 357, 752–756. [Google Scholar] [CrossRef] [PubMed]
- Almqvist, C.; Wickman, M.; Perfetti, L.; Berglind, N.; Renström, A.; Hedrén, M.; et al. Worsening of Asthma in Children Allergic to Cats, after Indirect Exposure to Cat at School. Am J Respir Crit Care Med. 2001, 163, 694–698. [Google Scholar] [CrossRef] [PubMed]
- Karlsson, A.S.; Andersson, B.; Renström, A.; Svedmyr, J.; Larsson, K.; Borres, M.P. Airborne cat allergen reduction in classrooms that use special school clothing or ban pet ownership. Journal of Allergy and Clinical Immunology. 2004, 113, 1172–1177. [Google Scholar] [CrossRef]
- Dávila, I.; Domínguez-Ortega, J.; Navarro-Pulido, A.; Alonso, A.; Antolín-Amerigo, D.; González-Mancebo, E.; et al. Consensus document on dog and cat allergy. Allergy. 2018, 73, 1206–1222. [Google Scholar] [CrossRef]
- Togias, A.; Fenton, M.J.; Gergen, P.J.; Rotrosen, D.; Fauci, A.S. Asthma in the inner city: The perspective of the National Institute of Allergy and Infectious Diseases. Journal of Allergy and Clinical Immunology. 2010, 125, 540–544. [Google Scholar] [CrossRef]
- Do, D.C.; Zhao, Y.; Gao, P. Cockroach allergen exposure and risk of asthma. Allergy. 2016, 71, 463–474. [Google Scholar] [CrossRef]
- Sohn, M.H.; Kim, K.E. The Cockroach and Allergic Diseases. Allergy Asthma Immunol Res. 2012, 4, 264. [Google Scholar] [CrossRef]
- Arruda, L.K.; Vailes, L.D.; Ferriani, V.P.; Santos, A.B.; Pomés, A.; Chapman, M.D. Cockroach allergens and asthma. J Allergy Clin Immunol. 2001, 107, 419–428. [Google Scholar] [CrossRef]
- Kitinoja, M.A.; Hugg, T.T.; Siddika, N.; Rodriguez Yanez, D.; Jaakkola, M.S.; Jaakkola, J.J.K. Short-term exposure to pollen and the risk of allergic and asthmatic manifestations: A systematic review and meta-analysis. BMJ Open. 2020, 10, e029069. [Google Scholar] [CrossRef] [PubMed]
- Suphioglu, C. Thunderstorm Asthma Due to Grass Pollen. Int Arch Allergy Immunol. 1998, 116, 253–260. [Google Scholar] [CrossRef] [PubMed]
- Bacsi, A.; Choudhury, B.; Dharajiya, N.; Sur, S.; Boldogh, I. Subpollen particles: Carriers of allergenic proteins and oxidases. Journal of Allergy and Clinical Immunology. 2006, 118, 844–850. [Google Scholar] [CrossRef] [PubMed]
- Pablos, I.; Wildner, S.; Asam, C.; Wallner, M.; Gadermaier, G. Pollen Allergens for Molecular Diagnosis. Curr Allergy Asthma Rep. 2016, 16, 31. [Google Scholar] [CrossRef] [PubMed]
- Matricardi, P.M. Allergen-specific immunoprophylaxis: Toward secondary prevention of allergic rhinitis? Pediatr Allergy Immunol. 2014, 25, 15–18. [Google Scholar] [CrossRef] [PubMed]
- Twaroch, T.E.; Curin, M.; Valenta, R.; Swoboda, I. Mold Allergens in Respiratory Allergy: From Structure to Therapy. Allergy Asthma Immunol Res. 2015, 7, 205. [Google Scholar] [CrossRef]
- Abel-Fernández, E.; Martínez, M.J.; Galán, T.; Pineda, F. Going over Fungal Allergy: Alternaria alternata and Its Allergens. Journal of Fungi. 2023, 9, 582. [Google Scholar] [CrossRef]
- D’Amato, G.; Spieksma, F.T.h.M. Aerobiologic and clinical aspects of mould allergy in Europe. Allergy. 1995, 50, 870–877. [Google Scholar] [CrossRef]
- Zureik, M.; Neukirch, C.; Leynaert, B.; Liard, R.; Bousquet, J.; Neukirch, F. Sensitisation to airborne moulds and severity of asthma: Cross sectional study from European Community respiratory health survey. BMJ. 2002, 325, 411–417. [Google Scholar] [CrossRef]
- Tischer, C.; Chen, C.M.; Heinrich, J. Association between domestic mould and mould components, and asthma and allergy in children: A systematic review. European Respiratory Journal. 2011, 38, 812–824. [Google Scholar] [CrossRef]
- Murrison, L.B.; Brandt, E.B.; Myers, J.B.; Hershey, G.K.K. Environmental exposures and mechanisms in allergy and asthma development. Journal of Clinical Investigation. 2019, 129, 1504–1515. [Google Scholar] [CrossRef] [PubMed]
- Droste, J.H.; Wieringa, M.H.; Weyler, J.J.; Nelen, V.J.; Vermeire, P.A.; Van Bever, H.P. Does the use of antibiotics in early childhood increase the risk of asthma and allergic disease? Clin Exp Allergy. 2000, 30, 1547–1553. [Google Scholar] [CrossRef] [PubMed]
- Reinmuth-Selzle, K.; Kampf, C.J.; Lucas, K.; Lang-Yona, N.; Fröhlich-Nowoisky, J.; Shiraiwa, M.; et al. Air Pollution and Climate Change Effects on Allergies in the Anthropocene: Abundance, Interaction, and Modification of Allergens and Adjuvants. Environ Sci Technol. 2017, 51, 4119–4141. [Google Scholar] [CrossRef] [PubMed]
- Lake, I.R.; Jones, N.R.; Agnew, M.; Goodess, C.M.; Giorgi, F.; Hamaoui-Laguel, L.; et al. Climate Change and Future Pollen Allergy in Europe. Environ Health Perspect. 2017, 125, 385–391. [Google Scholar] [CrossRef]
- Reinmuth-Selzle, K.; Kampf, C.J.; Lucas, K.; Lang-Yona, N.; Fröhlich-Nowoisky, J.; Shiraiwa, M.; et al. Air Pollution and Climate Change Effects on Allergies in the Anthropocene: Abundance, Interaction, and Modification of Allergens and Adjuvants. Environ Sci Technol. 2017, 51, 4119–4141. [Google Scholar] [CrossRef]
- D’Amato, G. Urban air pollution and plant-derived respiratory allergy. Clin Exp Allergy. 2000, 30, 628–636. [Google Scholar] [CrossRef]
- Muranaka, M.; Suzuki, S.; Koizumi, K.; Takafuji, S.; Miyamoto, T.; Ikemori, R.; et al. Adjuvant activity of diesel-exhaust particulates for the production of IgE antibody in mice. J Allergy Clin Immunol. 1986, 77, 616–623. [Google Scholar] [CrossRef]
- Diaz-Sanchez, D.; Tsien, A.; Fleming, J.; Saxon, A. Combined diesel exhaust particulate and ragweed allergen challenge markedly enhances human in vivo nasal ragweed-specific IgE and skews cytokine production to a T helper cell 2-type pattern. J Immunol. 1997, 158, 2406–2413. [Google Scholar] [CrossRef]
- Lack, G. Epidemiologic risks for food allergy. Journal of Allergy and Clinical Immunology. 2008, 121, 1331–1336. [Google Scholar] [CrossRef]
- Agache, I.; Akdis, C.A.; Akdis, M.; Canonica, G.W.; Casale, T.; Chivato, T.; et al. EAACI Biologicals Guidelines—Recommendations for severe asthma. Allergy. 2021, 76, 14–44. [Google Scholar] [CrossRef]
- Alvaro-Lozano, M.; Akdis, C.A.; Akdis, M.; Alviani, C.; Angier, E.; Arasi, S.; et al. Allergen Immunotherapy in Children User’s Guide. Pediatric Allergy and Immunology. 2020, 31, 1–101. [Google Scholar] [CrossRef] [PubMed]
- Jacobsen, L.; Niggemann, B.; Dreborg, S.; Ferdousi, H.A.; Halken, S.; Høst, A.; et al. Specific immunotherapy has long-term preventive effect of seasonal and perennial asthma: 10-year follow-up on the PAT study. Allergy. 2007, 62, 943–948. [Google Scholar] [CrossRef] [PubMed]
- Bunne, J.; Hedman, L.; Perzanowski, M.; Bjerg, A.; Winberg, A.; Andersson, M.; et al. The Majority of Children Sensitized Before School-Age Develop Allergic Disease Before Adulthood: A Longitudinal Population-Based Study. J Allergy Clin Immunol Pract. 2022, 10, 577–585.e3. [Google Scholar] [CrossRef] [PubMed]
- Matricardi, P.M.; Kuna, P.; Panetta, V.; Wahn, U.; Narkus, A. Subcutaneous immunotherapy and pharmacotherapy in seasonal allergic rhinitis: A comparison based on meta-analyses. Journal of Allergy and Clinical Immunology. 2011, 128, 791–799.e6. [Google Scholar] [CrossRef]
Figure 1.
Scheme of pathophysiology and treatment of respiratory allergic diseases (authors' own work).
Figure 1.
Scheme of pathophysiology and treatment of respiratory allergic diseases (authors' own work).
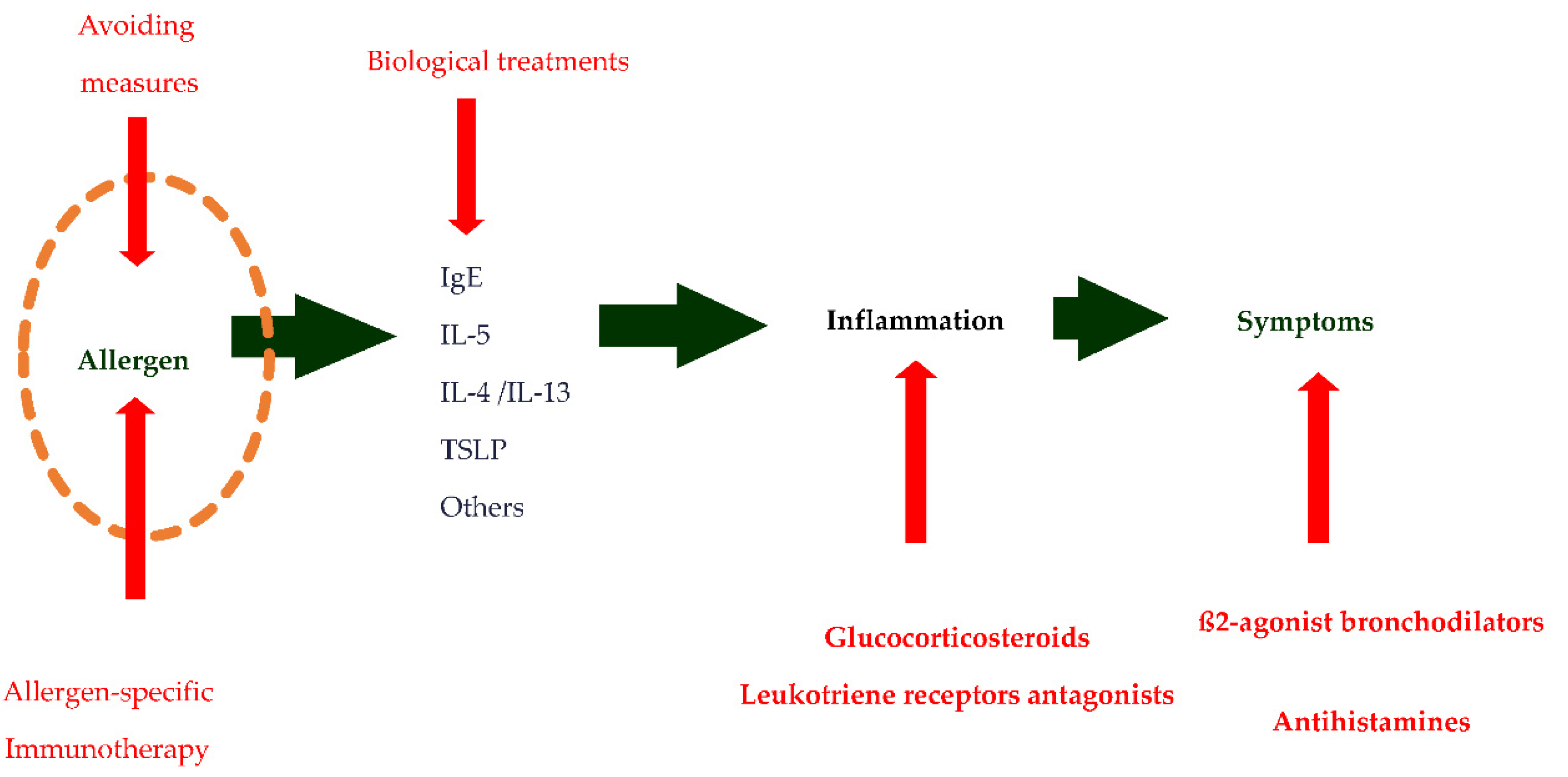

Table 1.
Main characteristics of respiratory allergens.
|
Table 2.
Thommen's postulates. Requirements for a substance to be considered a respiratory allergen.
Table 2.
Thommen's postulates. Requirements for a substance to be considered a respiratory allergen.
|
Table 3.
Effectiveness of avoidance measures for house dust mites. Modified from Box 3.10, GINA 2022 (16).
Table 3.
Effectiveness of avoidance measures for house dust mites. Modified from Box 3.10, GINA 2022 (16).
| Measure | Evidence on reducing allergen (grade of evidence) | Evidence of clinical benefit (grade of evidence) |
| Encase bedding in impermeable covers (pore diameter < 10 µm) | Some (A) | Adults: none (A)乐Children: some (B) |
| Replace carpets with hard flooring | Some (B) | None (D) |
| Wash bedding weekly on hot cycle (55-60º C), use of heater drier | Some (C) | None (D) |
| Acaricides and or tannic acid | Weak (C) | None (D) |
| Vacuum cleaners with HEPA filter and reinforced bags | Weak (C) | None (D) |
| Wash the soft toys in hot water, freeze them or remove them. | None (D) | None |
| Remove objects that accumulate dust | None (D) | None (D) |
Table 4.
Effectiveness of avoidance measures for pets. Modified from (29).
| Measure | Level of Evidence | Degree of recommendation |
| Thermostatically controlled laminar flow | 2 | B |
| Washing pets ≥ 2 times per week | 4 | C |
| Removing pet out of the bedroom | 5 | D |
| Bed covers and pillowcases / wash linen with chemicals | 5 | D |
| air purifiers and vacuum cleaners with HEPA filters | 5 | D |
| Binder lotions that encapsulate allergens on the fur of the animal | 5 | D |
Table 5.
Instructions to avoid pollens. Adapted from: Working Group on Respiratory Allergy and Asthma. Spanish Society of Clinical Immunology, Asthma and Pediatric Allergy (SEICAP). Available at: https://seicap.es/wp-content/uploads/2022/05/Instrucciones-para-evitar-polenes.pdf (last update 19.3.2023).
Table 5.
Instructions to avoid pollens. Adapted from: Working Group on Respiratory Allergy and Asthma. Spanish Society of Clinical Immunology, Asthma and Pediatric Allergy (SEICAP). Available at: https://seicap.es/wp-content/uploads/2022/05/Instrucciones-para-evitar-polenes.pdf (last update 19.3.2023).
|
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



