
Submitted:
15 July 2023
Posted:
19 July 2023
You are already at the latest version
Abstract
The advent of immunotherapy has revolutionized the treatment of advanced non-small cell lung cancer (NSCLC), improving the prognosis of this disease and becoming a key part of the treatment, especially in the population without an oncogenic driver mutation. Two different groups of immune checkpoint inhibitors (ICIs) are used in lung cancer: Anti- Cytotoxic T-lymphocyte antigen-4 (Anti-CTLA 4) and Anti- T-cell receptor programmed cell death-1 or its ligand (Anti-PD-1 and Anti PD-L1). Here in, we review an uptodate on the use of immunotherapy for advanced NSCLC.
Keywords:
Immune checkpoint inhibitors (ICIs)
; Non–small cell lung cancer (NSCLC)
; PD-1
; PD-L1
; CTLA-4
Introduction
The introduction of immunotherapy has brought about a remarkable transformation in the advanced non-small cell lung cancer (NSCLC) approach, improving the prognosis of this disease and becoming a key part of the treatment, especially in the population without target mutations(1). Two pathways have been linked to the use of immunotherapy in lung cancer: Cytotoxic T-lymphocyte antigen-4 (CTLA-4) and T-cell receptor programmed cell death-1 (PD-1)(1,2). Therefore, therapeutic antibodies targeting CTLA-4, PD-1, and its ligand (PDL1) are now approved as monotherapy and in combination with chemotherapy (Table 1)(1). Here in, we review the use of immunotherapy for advanced NSCLC.
Mechanism of action
Tumour cells express tumour-specific antigens, which are presented on antigen-presenting cells (APCs), allowing the T cell to recognize the tumour. Subsequently, the CD28 receptor on T cells engages the B7 receptor (CD80/86) on APC and activates the T cell (3).
Immune checkpoint are proteins on the surface of T cells and other immune cells that act as negative regulators of immune activity. The first checkpoint to be discovered was CTLA-4 (1,4). CTLA-4 competes with CD28 for B7, inducing T cell cycle arrest and suppress T-cell activation (5,6). PD-1 is expressed on different immunological cells, including B cells, natural killer cells, and monocytes (6). PD-1 regulates the activation of T cells and B lymphocytes directly, by binding to its PD-L1 and PD-L2 ligands (7). This complex inhibits the kinase signalling pathway that normally activates T cells (3,7). Some tumours express PD-L1 and PD-L2, it helps to protect against immune response and allows tumour proliferation.
Biomarkers
The results of the use of immunotherapy in different neoplasia create the need to find a biomarker that can predict the response to treatment. Thus, new tumour biomarkers were developed depending on the drug used and the type of neoplasia.
- PD-L1:
The role of PD-L1 expression in predicting response to PD-1 checkpoint blockade is controversial (1,2). This is due to the different methods used to determine the percentage, the different cut-offs, the heterogeneity of the expression and where it is measured (tumour cells or immune cells) (8). In this case, the definition of a positive or negative PD-L1 test result depends on the individual antibody, clone, and platform and is different for each immune checkpoint inhibitor (ICI) (8,9).
For nivolumab trials, Dako developed a 5H1 or 28-8 assay, while pembrolizumab employs the Dako 22C3 assay for its detection. For Atezolizumab, most IMPOWER trials used the Ventana SP263 assay and evaluated PD-L1 expression in tumour and immune cells (9,10).
It has not yet been possible to obtain the equivalence between different clones, which would standardise the measurement and make the ICI comparable. The Blueprint PD-L1 IHC Assay Comparison Project evaluated the comparability of four of the different immunohistochemical assays (22C3, 28-8, SP142 and SP263). The comparison showed that the percentage of PD-L1 stained tumour cells was comparable between the 22C3, 28-8, and SP263 assays, while the SP142 assay showed fewer stained tumour cells. However, equivalence has not yet been demonstrated and some data suggest that PD-L1 expression is heterogeneous (11–13).
Although not the ideal biomarker, PD-L1 expression is currently the best biomarker available to assess whether patients are candidates for ICI. The use of IHC testing for PD-L1 expression is recommended ideally before first-line treatment in all patients with mNSCLC (14). However, it is not required to prescribe first-line therapy with certain ICI regimens (14,15).
- Tumour mutational burden (TMB):
It is an approximate measure of the total number of somatic mutations (14,16).. When the number of mutations increases, a high level of neoantigens is generated that activates the response of the immune system against the tumour (17). Some studies have shown the likely use of TMB as a biomarker to decide whether to use immunotherapy in patients with mNSCLC. However, update data did not find any difference between high and low TMB (≥10 versus <10 mutations per megabase, respectively) (18).
As in PD-L1, there are technical problems with measuring TMB, which include the lack of a standard cut-off for high TMB levels, standard measurements across laboratories, and the waiting time for the result (15,16). For these reasons, the measurement of TMB is not recommended for evaluation prior to the use of immunotherapy (16).
Chemotherapy free regimens
Single agent
Single-agents are recommended as first-line therapy for patients with metastatic NSCLC (mNSCLC) with negative test results for actionable driver mutations, PD-L1 expression levels of 50% or more and regardless of histology. In this setting, we have approvals for pembrolizumab, atezolizumab, and cemiplimab-rwlc (Table 2) (14,15,19).
Pembrolizumab
Pembrolizumab is another humanized IgG4; it works by blocking the protein PD-1. KEYNOTE-024 compared single-agent pembrolizumab versus platinum-based chemotherapy (CT) as first-line therapy for patients with mNSCLC with PD-L1 expression levels of 50% or more, without driver mutation and regardless of histology. This phase 3 randomized clinical trial (RCT) had as primary endpoint progression free survival (PFS). During every 3 weeks, patients received a fixed dose of 200 mg for up to 35 cycles or the investigator’s choice of platinum-based CT. Crossover between groups was allowed as the disease progressed. The median PFS was significantly longer in the pembrolizumab group versus the CT group (10.3 versus 6.0 months; HR 0.50; 95% CI0.37-0.68, p < 0.001). The ORR was higher in the pembrolizumab group than in the chemotherapy group (44.8% vs 27.8%) and OS at 6 months was 80.2% versus 72.4%, respectively (HR 0.60; 95% CI 0.41-0.89; p = 0.005). Treatment-related adverse events (TRAE) of any type occurred in 73.4% of patients in the pembrolizumab group, the most common were diarrhoea (14.3%), fatigue (10.4%), and pyrexia (10.4%). Only 26.6% of the patients presented grade 3 to 5 TRAE (20).
The 5-year update was published in 2020. With a median follow-up of 59.9 months (55.1-68.4), patients in the pembrolizumab arm had a statistically significant benefit in PFS (7.7 vs 5.5 months; HR 0.5; 95% CI 0.39 - 0.65) and overall survival rate at 5 years (OS) (31.9% vs 16.3%). In addition, PFS2, that included disease progression following the introduction of anticancer treatment or in the event of mortality, was higher in the pembrolizumab group versus chemotherapy (24.1 versus 8.5 months; HR, 0.51; 95% CI 0.39 - 0.67). With these findings, we can conclude that pembrolizumab has a durable and clinically meaningful long-term OS benefit versus chemotherapy as first-line therapy in this population (21).
For patients PD-L1 with expression levels of 1% or more, but without EGFR mutations or ALK rearrangements, KEYNOTE-042 was performed. This phase 3 RCT, with a follow-up of 12.8 months, compared single-agent pembrolizumab versus platinum-based CT as first-line therapy for patients with untreated advanced NSCLC, regardless of histology. The main objectives focused on OS among patients with a tumour proportion score equal to or greater than 50%, 20% and 1%, which was longer for pembrolizumab treatment (≥50 % HR 0.69, 95% CI 0.56-0.85, p = 0.0003; <20 % HR 0.77, CI 0.64-0.92, p = 0.0020, and <1% HR 0.81, CI 0.71-0.93, p = 0.0018). The median OS was 20.0 months for pembrolizumab versus 12.2 months for chemotherapy (TPS of 50% or greater), 17.7 months versus 13.0 months (TPS of 20% or greater), and 16.7 months versus 12.1 months (TPS of 1% or greater). Treatment-related adverse events of grade 3 or higher were observed in 18% (113/636) of patients treated with pembrolizumab (21,22).
5-year update results from this trial reports; with a median follow-up time of 61.1 months (50.0-76.3), OS was consistently higher in patients who received pembrolizumab, in all three groups (TPS ≥ 50%, HR 0.68 [0.57 to 0.81]; TPS ≥ 20%, HR 0.75 [0.64 to 0.87]; TPS ≥ 1%, HR 0.79 [0.70 to 0.89]). 5-year OS rates were 21.9%, 19.4%, and 16.6%, in each group, respectively. No new toxicities were reported (21,22). Although this is approved by the FDA, we do not use it because the benefit in the PDL1+ population in general is driven by high expressors. The OS curve in patients with PDL1 from 1 to 49% was not significant.
Atezolizumab
Atezolizumab is a humanized IgG1 monoclonal antibody that targets PDL1. Based on results of IMpower 110, the FDA approved in 2021 the use of atezolizumab for patients with mNSCLC, PD-L1 high expresses, squamous and non-squamous histology and negative test results for actionable driver mutations; as a first-line therapy option (3,7) . The IMpower 110, a phase 3 randomized clinical trial (RCT), compared first-line therapy with single-agent atezolizumab versus platinum-based chemotherapy (CT) in patients with untreated PD-L1 ≥ 1% (on tumour or tumour-infiltrating immune cells as assessed by the SP142 IHC assay) mNSCLC. In the experimental group, patients received first-line atezolizumab monotherapy followed by maintenance therapy with atezolizumab. The patients in the control group received platinum (cisplatin or carboplatin)/pemetrexed followed by maintenance with pemetrex for nonsquamous histology and cisplatin/gemcitabine for squamous histology. Atezolizumab significantly prolonged OS (20.2 versus 13.1 months; HR 0.59; 95% CI 0.40-0.89, p = 0.0106) only in patients with high PD-L1 expression (PD-L1 ≥ 50% of tumour cells or PD-L1 stained tumour-infiltrating immune cells covering ≥ 10% of the tumour area) (23). An update, with 3-year of follow-up, confirmed the OS benefit in this population (20.2 versus 14.7 months; HR 0.76, 95% CI 0.54-1.09) (24). Despite these excellent results, we should emphasise that in this study the crossover from the chemotherapy to atezolizumab arm was not permitted. Treatment-related adverse events (TRAE) were found for 90.2% of patients receiving atezolizumab. Grade 3 to 4 TRAE occurred in 12.9% of patients receiving atezolizumab monotherapy versus 44.1% with chemotherapy. The most commonly observed severe adverse events with atezolizumab were pneumonia (2.8%), COPD (2.1%), and pneumonitis (2.1%); 28% of patients had serious adverse reactions (23).
Cemiplimab
Cemiplimab is a fully human immunoglobulin IgG4 monoclonal antibody that targets PD-1 (25).It was approved in 2021 by the FDA regarding the results of EMPOWER-Lung 1. In EMPOWER-Lung 1, single-agent cemiplimab showed more effectiveness than platinum-based CT for patients with mNSCLC with PD-L1 levels of 50% or more, without driver mutation and regardless of histology. It was a multicentre phase 3 RCT. Crossover from CT to cemiplimab was allowed. In the population of PD-L1 50% population (n= 563), median OS was not reached in the cemiplimab group versus 14.2 months In the CT group, there was a notable improvement in median progression-free survival (PFS) compared to the cemiplimab group (8.2 months versus 5.7 months, HR 0.54; p < 0.0001). Additionally, grades 3 to 4 treatment-related adverse events were documented in 28% (98 out of 355) of cemiplimab group and treated-related deaths occurred in 2.5% (9/355) of patients; due to autoimmune myocarditis, cardiac failure, cardiopulmonary failure, cardiorespiratory arrest, nephritis, respiratory failure, septic shock, tumour hyper progression, and unknown (26). An update, after 3 years of follow-up, showed sustained improvement in OS, PFS, and objective response rate (ORR), despite a 75% crossover rate. In the cemiplimab group, the median OS was 26.1 versus 13.3 months in the CT group (HR 0.57; 95% CI 0.46-0.71, p < 0.0001); median PFS was 8.1 versus 5.3 months (HR 0.51; 95% CI 0.42-0.62, p < 0.0001) and ORR was 46.5% versus 21.0% (OR 3.26; p < 0.0001). In addition, crossover patients obtained durable responses and an ORR of 31.3% (27).
Immunotherapy combinations
- Nivolumab plus ipilimumab
Nivolumab is a fully human immunoglobulin G4 (IgG4) monoclonal antibody against the PD-1 and ipilimumab is an anti-CTLA4. The combination of both demonstrated efficacy in metastatic melanoma, improves ORR and survival compared with monotherapy (25). These encouraging results prompted the study in lung cancer.
CheckMate 227 compared nivolumab plus ipilimumab, nivolumab monotherapy, and chemotherapy in patients with untreated metastatic non-squamous or squamous NSCLC. This was a Phase 3 RCT, including patients with PD-L1 expression levels ≥ 1% or more and less than 1%, PS 0 to 1, and without driver mutations. The primary endpoint was OS and CT was compared to nivolumab plus ipilimumab in patients’ level of expression of with a PD-L1 of 1% or higher. Furthermore, a co-primary analysis was performed in patients with high TMB levels (<10 mutations / megabase). The median OS was 17.1 months with nivolumab plus ipilimumab and 14.9 months with chemotherapy (p = 0.007), with 2-year OS rates of 40.0% and 32.8%, respectively. The benefit of OS was also observed in patients with PD-L1 expression less than 1%, with a median duration of 17.2 months vs 12.2 months, in the group of nivolumab plus ipilimumab and chemotherapy, respectively. Grade 3 to 4 TRAE were 32.8% in patients who received nivolumab plus ipilimumab. The most common of any grade were skin reactions (34.0%) and endocrine events (23.8%) (28).
A 5-year updated data showed that OS was improved regardless of TMB or PD-L1 expression levels for experimental group when compared to patients under CT treatment. In patients with PD-L1 ≥ 1%, the OS rate was 24% for nivolumab plus ipilimumab versus 14% for CT. Furthermore, in patients with PD-L1 < 1% was 19% versus 7%, in each group, respectively. Quality of life in 5-year survivors was similar to the general US population through the 5-year follow-up (28,29).
- Durvalumab plus tremelimumab
The MYSTIC trial was a phase 3 RCT, designed to compare durvalumab plus tremelimumab, durvalumab alone, and chemotherapy in patients with mNSCLC without EGFR / ALK genetic changes. The primary endpoints were OS for durvalumab versus chemotherapy, OS and PFS for durvalumab plus tremelimumab versus chemotherapy assessed in patients with <25% expression of PD-L1. The median OS was higher for patients who received durvalumab compared with CT but was not significant (HR 0.76; 97.5% CI 0.56-1.02; p = 0.04). For the group who received durvalumab plus tremelimumab the median OS was higher than CT , but also was not significant (HR 0.85; 98.77% CI0.61-1.17; p = 0.20). In addition, no significant differences were found in PFS for durvalumab plus tremelimumab arm versus CT arm (HR 1.05; 99.5% CI 0.72-1.53; p = 0.71). This trial did not reach its primary endpoints. However, exploratory evaluations revealed that an optimal benefit in OS was observed with durvalumab plus tremelimumab at a threshold of 20 mut / Mb for tumour mutational burden (30).
Combinations with chemotherapy
In the previous section, we resume the different options of single agent immunotherapy for patients with more than ≥1% of PDL1 expression. On the other hand, different combinations of immunotherapy plus chemotherapy were approved for patients with mNSCLC (Table 3).
- Atezolizumab
IMpower150, a phase 3 RCT, evaluated the efficacy of atezolizumab in three groups in metastatic non-squamous NSCLC wild-type EGFR and ALK patients. One group received atezolizumab + carboplatin + paclitaxel (ACP), another group received bevacizumab + carboplatin + paclitaxel (BCP), and a third group received atezolizumab + BCP (ABCP) each 3 weeks (4-6 cycles). Subsequently, maintenance treatment with either atezolizumab, bevacizumab, or a combination of both was administered. The primary end points were PFS in patients with high expression of an effector T-cell (Teff) gene signature in the tumour and overall survival in the WT population. The median PFS was longer in the ABCP group than in the BCP group (8.3 versus 6.8 months; HR 0.62; 95% CI 0.52-0.74; p<0.001) and the median OS was 19.2 months in the ABCP group and 14.7 months in the BCP group (HR 0.78; 95% CI 0.64-0.96, p = 0.02) (31).
This trial also enrolled individuals with EGFR or ALK rearrangements (n = 108) and disease progression on prior TKI. In this population, the initial results showed a higher correlation with ABCP than with BCP (9.7 versus 6.1 months; HR 0.59; 95% CI 0.37-0.94) (31). However, the update with 3-year follow-up demonstrated that the benefit in OS was not statistically significant for the ABCP group versus BCP in sensitising EGFR mutations (HR 0.60; 0.31-1.14 in 95% CI) and for previous patients with TKI (HR 0.74; 0.38-1.46 in 95% CI) (32).
In 2021, an update with a median follow-up of 39.8 months was published. In the final analysis, there were no statistically significant improvements in OS between ACP vs BCP (19.0 versus 14.7 months; HR 0.84; 0.71-1.00 in 95% CI). The OS benefit was sustained with ABCP versus BCP (19.5 versus 14.7 months; HR 0.80; 95% CI 0.67-0.95). Within the subsets defined as high PD-L1 and positive PD-L1 according to SP142, the median OS was longer with ABCP and ACP versus BCP; while in the negative PDL1 subgroup there were no differences in OS between ACP and ABCP versus BCP (33).
IMpower130, a multicentre phase 3 RCT, evaluated atezolizumab + carboplatin + nab-paclitaxel compared to CT in patients with metastatic non-squamous NSCLC without EGFR mutations or ALK rearrangements, according of PD-L1 tumour expression. The primary endpoints were PFS and OS in the intention-to-treat population. The median OS was 18.6 versus 13.9 months (HR 0.79; 95% CI 0.64-0.98; p = 0.033) and the median PFS was 7.0 versus 5.5 months (HR 0.64; 95% CI 0.54-0.77, p<0.0001) in the atezolizumab plus CT group and in the CT group, respectively. Regarding TRAE, neutropenia emerged as the predominant grade 3 or higher adverse event (32% versus 28%) followed by anemia (29% versus 20%). A 2% (8/473) incidence of deaths related to treatment was documented in the atezolizumab + CT arm, being inferior for CT-only arm, with less than 1% (1/232) of the individuals (34).
IMpower 131, a multicenter phase 3 trial, included patients with metastatic squamous NSCLC without EGFR mutations or ALK rearrangements regardless of PD-L1 status, divided in 1: 1 arm to receive atezolizumab plus carboplatin plus paclitaxel (A/CP), atezolizumab plus carboplatin plus nab-paclitaxel (A/CnP) or carboplatin plus nab-paclitaxel (CnP). The primary endpoints were PFS and OS. PFS was improved in A+CnP versus CnP (6.3 versus 5.6; HR 0.71, 95% CI 0.60-0.85; p= 0.0001). However, OS had not reached a significant benefit (14.2 versus 13.5; HR 0.88, 0.73-1.05 in a 95% CI; p = 0.16). Improvement in OS improvement with A+CnP versus CnP was observed in the high PD-L1 subgroup (HR = 0.48, 95% CI 0.29-0.81), although it was not officially tested. TRAEs grade 3 and 4 occurred in 68.0% and 47.9% (A+CnP) and 57.5% and 28.7% (CnP) of patients, respectively (35).
IMpower132 evaluated the use of atezolizumab + platinum-based chemotherapy + pemetrexed in the first line in patients with mNSCLC. Patients were enrolled regardless of PD-L1 expression and randomized in two arms: carboplatin/cisplatin + pemetrexed +/- atezolizumab; following maintenance with pemetrexed +/- atezolizumab. Primary endpoints were PFS and OS. In the primary analysis, the median follow-up was 14.8 months, PFS showed a significant improvement in patients who received atezolizumab versus only chemotherapy (7.6 versus 5.2 months; HR 0.60, 95% CI 0.49-0.72, p < 0.0001). OS was not statistically significant at the interim analysis (18.1 versus 13.6 months; HR 0.81, 95% CI 0.64-1.03, p = 0.0797). Atezolizumab resulted in grades 3 or 4 treatment-related adverse events for almost 55% of the treated patients (34–36).
- Cemiplimab
EMPOWER-Lung 3, evaluated the efficacy of cemiplimab plus platinum-doublet CT as an initial therapy option for a NSCLC, regardless PD-L1 expression or histology. This study includes stage III/IV NSCLC without a driver mutation (EGFR, ALK, or ROS1). The primary end point was OS. After 16.4 months of follow-up, median OS was 21.9 months with cemiplimab plus chemotherapy versus 13.0 months with placebo + CT (HR 0.71; 95% CI, 0.53- 0.93; P = 0.014). Adverse events of grade 3 were found in 43.6% of the patients who received cemiplimab plus chemotherapy. Immune-related adverse events occurred in 19% and one patient died from immune-mediated pneumonitis (37).
In March 2023, a 2-year update data was published. After 28.4 months of median follow-up, cemiplimab plus chemotherapy significantly improved median OS compared to chemotherapy alone (21.1 versus 12.9 months; HR 0.65, 95% CI 0.51–0.82, p = 0.0003); median PFS was 8.2 months versus 5.5 months (HR 0.55, 95% CI 0.44–0.68, p < 0.0001), and ORR were 43.6% versus 22.1%, respectively. Safety was similar to the previous report (48.7%) and no immune-related deaths were reported (37,38).
- Nivolumab/Ipilimumab
In the phase 3 RCT known as CheckMate 9LA, the efficacy of first-line treatment with nivolumab/ipilimumab and two cycles of platinum-doublet induction chemotherapy was compared to four cycles of chemotherapy alone in patients diagnosed with mNSCLC without driver mutations, regardless of their PD-L1 expression levels and histology. The patients were randomly assigned and stratified by tumour histology, sex, and PD-L1 expression. The primary endpoint was OS. At the interim analysis, with a median follow-up of 9.7 months, OS improved significantly in patients in the experimental arm (14.1 versus 10.7 months; HR 0.69; 96.71% CI 0.55-0.87, p = 0.00065). The most common grade 3 to 4 TRAEs were neutropenia (7%), anaemia (6%), diarrhoea (4%), increased lipase (6%), and febrile neutropenia (4%). Seven deaths in the experimental group (acute kidney failure, diarrhoea, hepatotoxicity, hepatitis, pneumonitis, sepsis with acute renal insufficiency, and thrombocytopenia) and six deaths in the control group (anaemia, febrile neutropenia, pancytopenia, pulmonary sepsis, respiratory failure, and sepsis; one patient each) were treatment related, accounting for 2% in both groups. In the experimental group, there were seven treatment-related deaths attributed to various causes, including urinary, respiratory, and haematopoietic causes. Likewise, within the control group, six deaths attributed to treatment were reported, representing 2% of the patients in both groups (39,40).
3-year update data showed a median OS of 15.8 in the experimental group when compared to 11 months in the control. PFS was 6.4 versus 5.3 months, in the experimental and the control arm, respectively. PD-L1 status did not influence the response rate; patients with PD-L1 ≥ 1% had the important finding of 28% of patients alive at 36 months, while in PD-L1–negative population 25% of patients were alive at 36 months. For patients with high expression of PD-L1, the median OS was 19 months (39).
- Pembrolizumab
KEYNOTE-189, compared platinum (carboplatin or cisplatin) plus pemetrexed +/- pembrolizumab in patients with metastatic non-squamous NSCLC not previously treated with no EGFR mutations or ALK rearrangements. Patients received doublet chemotherapy plus 200 mg of pembrolizumab or placebo every 3 weeks for 4 cycles, followed by pembrolizumab or placebo plus pemetrexed for up to a total of 35 cycles as maintenance therapy. The primary endpoints were OS and PFS. The transition to pembrolizumab monotherapy was allowed. After a median follow-up of 10.5 months, OS at 12 months in the experimental group was better than that of the control group (69.2% versus 49.4%; HR 0.49; 95% CI 0.38- 0.64; p<0.001), regardless of PD-L1 categories. Median PFS was 8.8 versus 4.9 months (HR 0.52; 95% CI 0.43- 0.64; P<0.001). Adverse events of grade 3 or higher occurred in 67.2% of patients who received pembrolizumab and were similar in both arms (41).
At ASCO 2022, 5-year updates were presented. With a median follow up of 64.6 months (60.1-72.4), patients who received pembrolizumab had a consistent benefit in OS (22 versus 10.6 months; HR 0.6; 95% CI 0.50-0.72) and PFS ( 9 versus 4.9 months; HR 0.5; 95% CI 0.42‒0.60). The 5-year OS rates were 19.4% versus 11.3%, respectively. Among the 57 patients who completed 35 cycles of pembrolizumab, the ORR was 86.0% and the 3-year OS rate after the completion of 35 cycles of pembrolizumab was 71.9%. The effective crossover rate was 40.8%. Grade 3‒5 TRAEs occurred in 72.8% (295/405 patients). This data confirmed and supported the benefit of pembrolizumab plus chemotherapy in these patients; regardless of PD-L1 status (42) .
For metastatic squamous cell NSCLC patients, KEYNOTE-407, a phase 3 RCT, compared carboplatin plus paclitaxel or albumin-bound paclitaxel +/- pembrolizumab, regardless of the level of PD-L1 expression. Participants were given carboplatin along with paclitaxel or nab-paclitaxel in the initial four cycles, following pembrolizumab or a placebo for a maximum of 35 cycles. The primary endpoints were OS and PFS. After a median follow-up of 7.8 months, the median OS was 15.9 months and 11.3 months in the pembrolizumab and the placebo group, respectively (HR 0.64; 95% CI 0.49 - 0.85, p <0.001). PFS was higher in patients who received CT + pembrolizumab versus CT + placebo (6.4 versus 4.8 months; HR 56; 95% CI 0.45-0.7, p<0.001). TRAE of grade 3 or higher happened in approximately 70% of the patients treated by the pembrolizumab combination. The placebo-CT group showed better adherence to treatment with only 6.4% of discontinuation, while 13.3% was verified in the combination (43).
The 5-year efficacy and safety follow-up reported that 127 of 281 patients crossed from the placebo group to the pembrolizumab group and an additional 26 patients received subsequent anti–PD-L1 therapy, with an effective crossover rate of 51.1%. The median OS was 17.2 versus 11.6 months, for the pembrolizumab+ CT and placebo + CT group (HR 0.71; 95% CI 0.59-0.85) and the 5-year OS rates were 18.4% and 9.7%, respectively. Median PFS was higher in the pembrolizumab versus placebo group (8 versus 5.1 months; HR 0.62; CI 0.52-0.74). In the group of 55 patients who completed 35 cycles of pembrolizumab, ORR was 90.9%, and 3-y OS rate after completion of 35 cycles was 69.5%. TRAE of grade 3 to 5 occurred in 74.8% and 70.0% of the patients in each group, respectively. This data consolidates the previous findings and maintain pembrolizumab + CT as an established initial therapeutic choice for advanced NSCLC that has spread, irrespective of the level of PD-L1 expression (44).
In addition, a pooled analysis of three randomized trials (KEYNOTE-407, KEYNOTE-189, and KEYNOTE-021 cohort G) in patients with advanced/mNSCLC and PD-L1 levels less than 1%. Among 33.4% (444/ 1328) of the patients with PD-L1 negative tumours, OS (HR, 0.63; 95% CI, 0.50- 0.79) and PFS (HR 0.68; 95% CI 0.56-0.83) was improved in participants who received pembrolizumab + CT versus CT alone. Patients who completed 35 courses of pembrolizumab (n 16) presented 87.5% (95% CI, 61.7%-98.4%) of ORR, and 100% of OS after three years. Adverse events associated with treatment were documented in 99.2% and 98.9% of the individuals, with severe or more serious cases observed in 71.4% and 72.0% of the study participants who received pembrolizumab plus CT and CT alone, respectively. Immune-mediated adverse effects were experienced by 29% (45).
- Tremelimumab plus durvalumab
POSEIDON, a phase 3 RCT, evaluated the effectiveness of tremelimumab plus durvalumab in 1013 individuals diagnosed with mNSCLC without mutations in EGFR and ALK, regardless histology. There were three treatment groups: 1) tremelimumab plus durvalumab plus platinum-based chemotherapy; 2) durvalumab plus platinum-based chemotherapy; and 3) platinum-based chemotherapy alone. Primary end points were PFS and OS for group 2 versus group 3. The results showed that PFS improved significantly in patients who received durvalumab (5.5 versus 4.8 months; HR 0.74; 95% CI 0.62 - 0.89, p = 0.0009); OS was not significantly different (5.5 versus 4.8 months; HR 0.86; 95% CI 0.72 - 1.02, p = 0.0758). In addition, patients in group 1, had a significantly higher PFS (6.2 v 4.8 months; HR 0.72; 95% CI 0.60 - 0.86, p = 0.0003) and OS (14.0 versus 11.7 months; HR 0.77; 95% CI 0.65 - 0.92; p = 0.0030). Regarding TRAES, grade 3- 4 were presented in 51.8%, 44.6%, and 44.4% of patients in group 1, 2 and 3, respectively. In group 1 the most common TRAE included, pneumonia (11%), anaemia (5%), diarrhoea (2.4%), thrombocytopenia (2.4%), pyrexia (2.4%), and febrile neutropenia (2.1%). Treatment-related deaths occurred in 3.3% (11/330) of patients in group 1 and 2.4% (8/333) in group 3; and 15.5%, 14.1%, and 9.9% discontinued treatment, in group 1, 2 and 3, respectively (45,46).
Second line therapy
In case a patient had not been exposed to immunotherapy in the first line, a single agent is recommended as a subsequent therapy option for select patients with mNSCLC. In this setting, pembrolizumab is approved in patients with levels of PD-L1 greater than 1% and nivolumab or atezolizumab for patients regardless of levels of PD-L1 (Table 4).
Atezolizumab
Two phase 2 trials, BIRCH and POPLAR, showed a benefit in OS for patients who received single agent atezolizumab with NSCLC with high expression of PD-L1 (assessed by the SP142 PD-L1 immunohistochemical assay) in multiple lines of therapy (23).
The OAK, a phase 3 RCT, assessed the efficacy and safety of atezolizumab versus docetaxel in previously treated patients with NSCLC regardless of histology. Patients had received one to two previous chemotherapy regimens for stage IIIB or IV, except docetaxel, CD137 agonists, anti-CTLA4, anti PD-L1 or PD-1. Co-primary endpoints were overall survival in the ITT and PD-L1-expression population (≥1 % PD-L1 on tumour cells or tumour-infiltrating immune cells). In the ITT population, OS improved significantly in patients who received atezolizumab versus docetaxel (13.8 versus 9.6 months; HR 0.73; 95% CI 0.62-0.87, p = 0.0003) and in patients with positive PDL1 OS was 15.7 versus 10.3 months (HR 0.74; 95% CI 0.58-0.93, p = 0.0102) for patients in the atezolizumab and docetaxel group, respectively. OS was similar in non-squamous (HR 0.73; 95% CI 0.60-0.89) and squamous (HR 0.73 ; 95% CI 0.54-0.98). TRAE grades 3 to 4 were reported as inferior for atezolizumab versus docetaxel (15% vs 43%) (23,47).
Results of OAK reported a continued benefit of atezolizumab in OS, with a median OS of 13.3 versus 9.8 months, in favour of the atezolizumab group (HR 0.78, 95% CI 0.68-0.89). The 4-year OS rates were 15.5% (12.4-18.7) and 8.7% (6.2-11.3) for atezolizumab and docetaxel, respectively. Grade 3-4 TRAE occurred in 16% of atezolizumab 4-year survivors. Atezolizumab had improved OS benefit compared with docetaxel regardless of PD-L1 expression and histology groups (48) .
Nivolumab
CheckMate-057, a RCT of phase 3, compared the efficacy of nivolumab versus docetaxel as a subsequent therapy for patients diagnosed with metastatic non-squamous NSCLC. The primary endpoint was OS, the median OS was 12.2 months for the nivolumab group compared to 9.4 months for the docetaxel group (HR 0.73; 95% CI 0.59-0.89, p = 0.002). The median duration of the response was 17.2 months with nivolumab compared to 5.6 months for docetaxel. Grade 3 to 5 TRAEs were found in 10% of the patients receiving nivolumab versus 54% of the patients treated with docetaxel. No significant differences in OS were observed between nivolumab and docetaxel as subsequent therapies. However, nivolumab demonstrated a longer response duration and fewer adverse effects compared to docetaxel (49).
For patients with mNSCLC characterized by squamous cell histology who experienced disease progression after the initial course of CT, CheckMate-017, a phase 3 RCT, compared the efficacy and safety of nivolumab versus docetaxel. The primary endpoint was OS, median OS was 9.2 months for nivolumab compared with 6.0 months for docetaxel (HR 0.59; 95% CI 0.44–0.79; p < 0.001). ORR was 20% with nivolumab compared to 9% with docetaxel (p = 0.008) and median PFS was 3.5 versus 2.8 months (HR 0.62; 95% CI 0.47 to 0.81, P<0.001) for nivolumab and docetaxel, respectively. PD-L1 expression was not found to be correlated with the nivolumab response. Grade 3-4 TRAEs were reported in 7% of patients with nivolumab and 55% of patients with docetaxel. No deaths related to nivolumab were reported, but 3 deaths occurred in docetaxel arm (50).
In a pooled 5-year update data for CheckMate-057 and CheckMate-017, after the minimum follow-up of 64.2 and 64.5 months for CheckMate 017 and 057, respectively, pooled 5-year OS rates were 13.4% versus 2.6%, respectively; and 5-year PFS rates were 8.0% versus 0%, respectively. TRAE were reported in 25.8% (8/31) patients treated with nivolumab and between 3-5 years of follow-up, seven of whom experienced new events; one (3.2%) TRAE was grade 3, and there was no grade 4 TRAEs (51).
Pembrolizumab
KEYNOTE-010, a phase 2/3 RCT, evaluated the efficacy of pembrolizumab with a single agent in patients with current or former smokers treated with advanced PD-L1 positive ( 1%), regardless of histology. There were three arms: pembrolizumab at 2 mg/kg, pembrolizumab at 10 mg/kg, and docetaxel at 75 mg/m² every 3 weeks. The primary endpoints were OS and PFS in the total population and in patients with PD-L1 ≥ 50% of tumour cells. The median OS was 10.4 months, 12.7 months and 5.5 months for the lowest dose of pembrolizumab, the highest dose and docetaxel, respectively. In both the low-dose group (HR 0.71; 95% CI 0.58-0.88, p = 0.0008) and the high-dose group (HR 0.61; CI 0.49-0.75, p < 0.0001) OS was significantly longer than the CT group. No significant difference was founded for PFS between three groups. For patients with at least 50% PD-L1 expression, OS in low dose pembrolizumab (14.9 vs 8.2 months; HR 0.54, CI 0.38-0.77, p = 0.0002) and PFS (5 versus 4.1 months; HR 0.59, 95% CI 0.44-0.78, p = 0.0001) was significantly longer. Furthermore, in the high dose group (OS 17.3 versus 8.2 months; HR 0.50; 95% CI 0.36-0.70; p < 0.0001) and PFS (5.2 vs 4.1 months; HR 0.59, CI 0.45–0.78, p<0.0001) was higher than in the docetaxel group. Grade 3 - 5 TRAE were presented in 13% (43/339), 16% (55/343) and in 35% (109/309) in low dose, high dose, and docetaxel group, respectively. Regarding mortal cases, six treatment-related deaths occurred in patients receiving pembrolizumab (three at each dose) and five occurred in the docetaxel arm (52).
The follow-up of 5 years, for efficacy and safety, in the KEYNOTE-010 research reported a maintain benefit for these patients in OS. With a median follow-up of 67.4 months (60.0‒77.9). The median OS was 16.9 months versus 8.2 months (HR 0.55; CI 0.44-0.69) in the PD-L1 TPS ≥50% group and 11.8 months versus 8.4 months (HR 0.70; CI 0.61-0.80) in the PD-L1 TPS ≥1% group. The 5-year OS rates for pembrolizumab versus docetaxel were 25.0% versus 8.2% in patients with PD-L1 TPS ≥50% and 15.6% versus 6.5% with PD-L1 TPS ≥1. Exploratory biomarker analysis revealed that a higher tumour mutational burden (≥175 mutations per exome) was associated with improved results with pembrolizumab (52,53).
Adverse effects
Unique immune-mediated adverse events are associated with ICI, and these are completely different from traditional chemotherapy toxicities (54). The range of possible immune-mediated adverse events includes cardiovascular, dermatologic, endocrine, gastrointestinal, neurologic, and pulmonary events (55).
A metanalysis was performed to evaluate the safety and effectiveness of ICIs in NSCLC. Grade 3 to 5 TRAEs and health-related quality of life (HRQoL) were secondary outcomes. A total of 5893 participants were included. For single agent ICIs, 5 RCTs were included with a total of 3346 participants. Patients had PD-L1 expression ≥ 50%, grades 3 to 4 TRAEs are less susceptible to the occurrence of adverse events when utilizing single-agent immune checkpoint inhibitors in comparison to platinum-based chemotherapy (RR: 0.41, 95% CI 0.33 to 0.50). Quality of life data were accessible for a sole study involving individuals with PD-L1 expression of 50% or higher, which indicated that ICI potentially enhance quality of life at the 15-week mark compared to platinum-based chemotherapy (RR: 1.51, 95% CI 1.08 to 2.10). For double agent ICI, TRAEs were not reported according to PD-L1 expression levels. The incidence of severe adverse events (grade 3-4) adverse events may not vary significantly between double-ICI treatment and platinum-based chemotherapy (RR: 0.78, 95% CI 0.55 to 1.09). The trials did not report data on HRQoL, PFS and ORR according to the PD L1 groups (56).
In 2022, another metanalysis evaluated serious (grade 3-5) and other (grade 1-2) TRAEs. 23,322 patients from 52 RCTs were included. The overall incidences of serious TRAEs were 37.0% in CT arm, 33.0% in PD-1 arm, and 37.0% in PD-L1 arm. In combined groups, it was 47.0% in the PD-L1 plus CT arm, 43.0% in PD-1 plus CTLA-4 arm, and 48.0% in ICI plus target arm. The incidence of each serious TRAEs was higher in combined groups. The ICIs groups presented a significant higher incidence in colitis, hepatobiliary disorders, pneumonitis, and rash compared with CT. A positive correlation between serious hepatitis (p < 0.0001) and clinical efficacy (PFS) were reported in PDL1 arm, likewise serious pneumonitis (p = 0.0049) and rash (p < 0.0001) in PD-1 arm (57).
In Table 5. we listed the possible adverse events. In the case of patients experiencing immune-mediated adverse events, the administration of intravenous high-dose corticosteroids is recommended. The severity of the reaction must be taken into account (55,58,59).
Discussion/ practical considerations
-Biomarkers
Immunotherapy has become the standard therapy for metastatic lung cancer without a driver mutation. However, there is still controversy regarding how to determine the population that benefits the most. Various efforts have been made in the quest for developing the ideal marker.
KRAS mutations are associated with good response to ICIs; co-mutation status has been described as a resistance mechanism to target treatment and has an influence on ICIs response (60) . The most common co-mutations were STK11 (encoding LKB1) and KEAP1, these had a negative influence in the response to immunotherapy, specifically in KRAS-mutated tumours. The role of STK11/ LKB1 and KEAP1 mutation/Nrf2 activation as a negative prognostic/predictive biomarker is promising but requires more investigation (61).
In conclusion, the development of biomarkers (TMB, CD8, MHC-I, mIF, etc.) for the response to immunotherapy need further study; however, nowadays the PD-L1 could be considered as the standard for clinical practice. The challenge also lies in identifying the biomarkers that indicate which patients require CTLA-4 blockade in addition to PD-L1 (61).
-Regimen selection
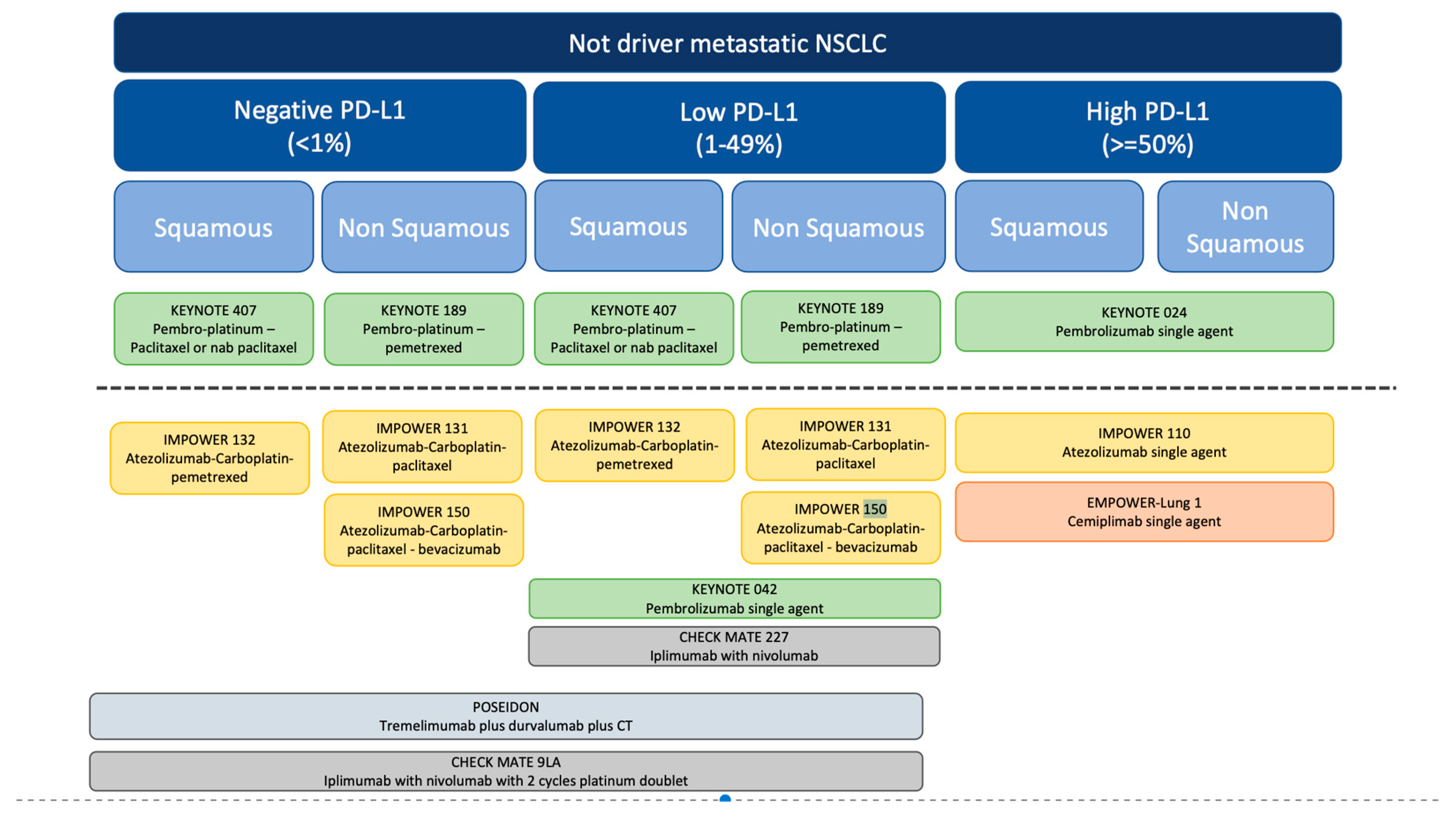
Currently, we have various treatment options available for immunotherapy, including monotherapy as well as combinations with chemotherapy, antiangiogenic agents, or other immunotherapeutic agents. The decision is complex, given the absence of comparative studies among all the approved options (Figure 1). However, some characteristics that can guide the decision are the expression rate of PD-L1, the histology of the tumour, some clinical characteristics, the type of toxicity and the preferences of the patient (19).
In patients with high PD-L1-expression (PD-L1≥50%), 2y-OS was 50% with pembrolizumab (KEYNOTE-024), 52% with pembrolizumab plus CT (KEYNOTE-189), and 48% with nivolumab plus ipilimumab (CheckMate-227). Considering these findings, it is advisable to consider single-agent ICIs for patients with high PD-L1 expression levels. In addition, results from KEYNOTE-598 did not find advantages for combination of ipilimumab with pembrolizumab in these patients. Certain patient groups with a high burden of extensive disease, severe related symptoms, and extensive disease itself may derive benefits from an initial combination regimen involving CT plus an anti-PD-1/PD-L1 antibody (62).
In patients with any PD-L1 expression (PD-L1 negative <1% and PD-L1 low 1–49%), the combination of CT plus Pembrolizumab has demonstrated a significant efficacy (KEYNOTE-407) (62). The combinations of CT and immunotherapy tested in the IMpower150 and CheckMate9LA trials demonstrated comparable benefits, but they also carried a higher risk of toxicity (33,40) .
-Duration of therapy
The ideal duration of anti-PD-1 and PD-L1 antibody therapy has not been definitively established at this time. Checkmate 153 trial, a phase IIIb/IV RCT, showed that OS is longer in patients with stable or responding disease who continue nivolumab compared with patients who stopped at 12 months (not reached vs 32·5 months, HR 0·61, 95% CI 0·37–0·99) (63)
However, excellent survival outcomes were reported in patients who completed 24 months of nivolumab and pembrolizumab (64,65). Additionally, a significant group of patients with disease progression after therapy completion can be successfully re-treated with an anti-PD-1/PD-L1 antibody (62).
The existing data provides support for the continuation of ICI treatment for a minimum of two years in patients who maintain disease stability or show a positive response to the therapy (19). However, prospective data is required to define the optimal duration of maintenance therapy.
-Effectiveness in target population
Currently, there is no evidence to suggest that second-line or subsequent-line treatment with immunotherapy provides benefits to patients with a driver mutation (64,65). Moreover, certain studies have demonstrated reduced effectiveness of immunotherapy in this specific group of patients (52,54). However, in these trials, the subgroup analysis included an insufficient number of patients to establish statistical significance (47,49,50).
The combination of immunotherapy agents and targeted TKIs resulted in notable increases in severe toxicities, including pneumonitis and hepatitis, without demonstrating any clinical benefit (66,67). Fortunately, advancements in the field of genomics and molecular biology have facilitated a better understanding of the behaviour of these tumour types, and currently there are other therapeutic alternatives available for this specific population (19).
Figure 1.
Algorithm for the Use of ICIs in not driver mNSCLC.
Conclusion
Immunotherapy has revolutionized the treatment of mNSCLC, improving overall survival and progression-free survival considerably. Currently, there exist multiple treatment options, necessitating the selection of the most suitable profile based on the patient being treated. This selection process involves evaluating histological characteristics, PD-L1 status, and relevant clinical features. While an ideal biomarker that enables such differentiation is yet to be identified, there is no doubt that PD-L1 has demonstrated significant clinical utility thus far.
References
- Punekar, S.R.; Shum, E.; Grello, C.M.; Lau, S.C.; Velcheti, V. Immunotherapy in non-small cell lung cancer: Past, present, and future directions. Front. Oncol. 2022, 12, 877594. [Google Scholar] [CrossRef] [PubMed]
- Steven A, Fisher SA, Robinson BW. Immunotherapy for lung cancer. Respirology [Internet]. 2016 Jul;21(5). Available online: https://pubmed.ncbi.nlm.nih.gov/27101251/ (accessed on 27 May 2023).
- Hsu, M.L.; Naidoo, J. Principles of Immunotherapy in Non-Small Cell Lung Cancer. Thorac. Surg. Clin. 2020, 30, 187–198. [Google Scholar] [CrossRef] [PubMed]
- Rowshanravan, B.; Halliday, N.; Sansom, D.M. CTLA-4: a moving target in immunotherapy. Blood 2018, 131, 58–67. [Google Scholar] [CrossRef] [PubMed]
- Hosseini, A.; Gharibi, T.; Marofi, F.; Babaloo, Z.; Baradaran, B. CTLA-4: From mechanism to autoimmune therapy. Int. Immunopharmacol. 2020, 80, 106221. [Google Scholar] [CrossRef]
- Buchbinder EI, Desai A. CTLA-4 and PD-1 Pathways: Similarities, Differences, and Implications of Their Inhibition. Am J Clin Oncol [Internet]. 2016 Feb;39(1). Available online: https://pubmed.ncbi.nlm.nih.gov/26558876/ (accessed on 27 May 2023).
- Freeman, G.J.; Long, A.J.; Iwai, Y.; Bourque, K.; Chernova, T.; Nishimura, H.; Fitz, L.J.; Malenkovich, N.; Okazaki, T.; Byrne, M.C.; et al. Engagement of the Pd-1 Immunoinhibitory Receptor by a Novel B7 Family Member Leads to Negative Regulation of Lymphocyte Activation. J. Exp. Med. 2000, 192, 1027–1034. [Google Scholar] [CrossRef]
- Yu H, Boyle TA, Zhou C, Rimm DL, Hirsch FR. PD-L1 Expression in Lung Cancer. J Thorac Oncol [Internet]. 2016 Jul;11(7). Available online: https://pubmed.ncbi.nlm.nih.gov/27117833/ (accessed on 27 May 2023).
- Kerr KM, Tsao MS, Nicholson AG, Yatabe Y, Wistuba II, Hirsch FR. Programmed Death-Ligand 1 Immunohistochemistry in Lung Cancer: In what state is this art? J Thorac Oncol [Internet]. 2015 Jul;10(7). Available online: https://pubmed.ncbi.nlm.nih.gov/26134220/ (accessed on 27 May 2023).
- Büttner R, Gosney JR, Skov BG, Adam J, Motoi N, Bloom KJ, et al. Programmed Death-Ligand 1 Immunohistochemistry Testing: A Review of Analytical Assays and Clinical Implementation in Non-Small-Cell Lung Cancer. J Clin Oncol [Internet]. 2017 Dec 1;35(34). Available online: https://pubmed.ncbi.nlm.nih.gov/29053400/ (accessed on 27 May 2023).
- Hirsch, F.R.; McElhinny, A.; Stanforth, D.; Ranger-Moore, J.; Jansson, M.; Kulangara, K.; Richardson, W.; Towne, P.; Hanks, D.; Vennapusa, B.; et al. PD-L1 Immunohistochemistry Assays for Lung Cancer: Results from Phase 1 of the Blueprint PD-L1 IHC Assay Comparison Project. J. Thorac. Oncol. 2017, 12, 208–222. [Google Scholar] [CrossRef]
- Bassanelli, M.; Sioletic, S.; Martini, M.; Giacinti, S.; Viterbo, A.; Staddon, A.; Liberati, F.; Ceribelli, A. Heterogeneity of PD-L1 Expression and Relationship with Biology of NSCLC. Anticancer. Res. 2018, 38, 3789–3796. [Google Scholar] [CrossRef]
- Munari, E.; Zamboni, G.; Lunardi, G.; Marchionni, L.; Marconi, M.; Sommaggio, M.; Brunelli, M.; Martignoni, G.; Netto, G.J.; Hoque, M.O.; et al. PD-L1 Expression Heterogeneity in Non–Small Cell Lung Cancer: Defining Criteria for Harmonization between Biopsy Specimens and Whole Sections. J. Thorac. Oncol. 2018, 13, 1113–1120. [Google Scholar] [CrossRef]
- Hendriks, L.; Kerr, K.; Menis, J.; Mok, T.; Nestle, U.; Passaro, A.; Peters, S.; Planchard, D.; Smit, E.; Solomon, B.; et al. Non-oncogene-addicted metastatic non-small-cell lung cancer: ESMO Clinical Practice Guideline for diagnosis, treatment and follow-up. Ann. Oncol. 2023, 34, 358–376. [Google Scholar] [CrossRef]
- Ettinger DS, Wood DE, Aisner DL, Akerley W, Bauman JR, Bharat A, et al. NCCN Guidelines Insights: Non-Small Cell Lung Cancer, Version 2.2021. J Natl Compr Canc Netw [Internet]. 2021 Mar 2;19(3). Available online: https://pubmed.ncbi.nlm.nih.gov/33668021/ (accessed on 27 May 2023).
- Bodor, J.N.; Boumber, Y.; Borghaei, H. Biomarkers for immune checkpoint inhibition in non-small cell lung cancer (NSCLC). Cancer 2020, 126, 260–270. [Google Scholar] [CrossRef]
- Sesma, A.; Pardo, J.; Cruellas, M.; Gálvez, E.M.; Gascón, M.; Isla, D.; Martínez-Lostao, L.; Ocáriz, M.; Paño, J.R.; Quílez, E.; et al. From Tumor Mutational Burden to Blood T Cell Receptor: Looking for the Best Predictive Biomarker in Lung Cancer Treated with Immunotherapy. Cancers 2020, 12, 2974. [Google Scholar] [CrossRef] [PubMed]
- Hellmann, M.D.; Paz-Ares, L.; Bernabe Caro, R.; Zurawski, B.; Kim, S.-W.; Carcereny Costa, E.; Park, K.; Alexandru, A.; Lupinacci, L.; de la Mora Jimenez, E.; et al. Nivolumab plus Ipilimumab in Advanced Non–Small-Cell Lung Cancer. N. Engl. J. Med. 2019, 381, 2020–2031. [Google Scholar] [CrossRef] [PubMed]
- Thai, A.A.; Solomon, B.J.; Sequist, L.V.; Gainor, J.F.; Heist, R.S. Lung cancer. Lancet 2021, 398, 535–554. [Google Scholar] [CrossRef] [PubMed]
- Reck, M.; Rodríguez-Abreu, D.; Robinson, A.G.; Hui, R.; Csőszi, T.; Fülöp, A.; Gottfried, M.; Peled, N.; Tafreshi, A.; Cuffe, S.; et al. Pembrolizumab versus Chemotherapy for PD-L1–Positive Non–Small-Cell Lung Cancer. N. Engl. J. Med. 2016, 375, 1823–1833. [Google Scholar] [CrossRef] [PubMed]
- Reck, M.; Rodríguez-Abreu, D.; Robinson, A.G.; Hui, R.; Csőszi, T.; Fülöp, A.; Gottfried, M.; Peled, N.; Tafreshi, A.; Cuffe, S.; et al. Five-Year Outcomes With Pembrolizumab Versus Chemotherapy for Metastatic Non–Small-Cell Lung Cancer With PD-L1 Tumor Proportion Score ≥ 50%. J. Clin. Oncol. 2021, 39, 2339–2349. [Google Scholar] [CrossRef] [PubMed]
- Mok, T.S.K.; Wu, Y.-L.; Kudaba, I.; Kowalski, D.M.; Cho, B.C.; Turna, H.Z.; Castro, G., Jr.; Srimuninnimit, V.; Laktionov, K.K.; Bondarenko, I.; et al. Pembrolizumab versus chemotherapy for previously untreated, PD-L1-expressing, locally advanced or metastatic non-small-cell lung cancer (KEYNOTE-042): a randomised, open-label, controlled, phase 3 trial. Lancet 2019, 393, 1819–1830. [Google Scholar] [CrossRef]
- Herbst, R.S.; Giaccone, G.; de Marinis, F.; Reinmuth, N.; Vergnenegre, A.; Barrios, C.H.; Morise, M.; Felip, E.; Andric, Z.; Geater, S.; et al. Atezolizumab for First-Line Treatment of PD-L1–Selected Patients with NSCLC. New Engl. J. Med. 2020, 383, 1328–1339. [Google Scholar] [CrossRef]
- Jassem, J.; de Marinis, F.; Giaccone, G.; Vergnenegre, A.; Barrios, C.H.; Morise, M.; Felip, E.; Oprean, C.; Kim, Y.-C.; Andric, Z.; et al. Updated Overall Survival Analysis From IMpower110: Atezolizumab Versus Platinum-Based Chemotherapy in Treatment-Naive Programmed Death-Ligand 1–Selected NSCLC. J. Thorac. Oncol. 2021, 16, 1872–1882. [Google Scholar] [CrossRef]
- Shiravand, Y.; Khodadadi, F.; Kashani, S.M.A.; Hosseini-Fard, S.R.; Hosseini, S.; Sadeghirad, H.; Ladwa, R.; O’byrne, K.; Kulasinghe, A. Immune Checkpoint Inhibitors in Cancer Therapy. Curr. Oncol. 2022, 29, 3044–3060. [Google Scholar] [CrossRef]
- Sezer, A.; Kilickap, S.; Gümüş, M.; Bondarenko, I.; Özgüroğlu, M.; Gogishvili, M.; Turk, H.M.; Cicin, I.; Bentsion, D.; Gladkov, O.; et al. Cemiplimab monotherapy for first-line treatment of advanced non-small-cell lung cancer with PD-L1 of at least 50%: a multicentre, open-label, global, phase 3, randomised, controlled trial. Lancet 2021, 397, 592–604. [Google Scholar] [CrossRef]
- Garassino, M.; Kilickap, S.; Özgüroğlu, M.; Sezer, A.; Gumus, M.; Bondarenko, I.; Gogishvili, M.; Nechaeva, M.; Schenker, M.; Cicin, I.; et al. OA01.05 Three-year Outcomes per PD-L1 Status and Continued Cemiplimab Beyond Progression + Chemotherapy: EMPOWER-Lung 1. J. Thorac. Oncol. 2023, 18, e2–e3. [Google Scholar] [CrossRef] [PubMed]
- Hellmann, M.D.; Ciuleanu, T.-E.; Pluzanski, A.; Lee, J.S.; Otterson, G.A.; Audigier-Valette, C.; Minenza, E.; Linardou, H.; Burgers, S.; Salman, P.; et al. Nivolumab plus Ipilimumab in Lung Cancer with a High Tumor Mutational Burden. N. Engl. J. Med. 2018, 378, 2093–2104. [Google Scholar] [CrossRef] [PubMed]
- Brahmer JR, Lee JS, Ciuleanu TE, Bernabe CR, Nishio M, Urban L, et al. Five-Year Survival Outcomes With Nivolumab Plus Ipilimumab Versus Chemotherapy as First-Line Treatment for Metastatic Non-Small-Cell Lung Cancer in CheckMate 227. J Clin Oncol [Internet]. 2023 Feb 20;41(6). Available online: https://pubmed.ncbi.nlm.nih.gov/36223558/ (accessed on 27 May 2023).
- Rizvi NA, Cho BC, Reinmuth N, Lee KH, Luft A, Ahn MJ, et al. Durvalumab With or Without Tremelimumab vs Standard Chemotherapy in First-line Treatment of Metastatic Non-Small Cell Lung Cancer: The MYSTIC Phase 3 Randomized Clinical Trial. JAMA oncology [Internet]. 2020 May 1;6(5). Available online: https://pubmed.ncbi.nlm.nih.gov/32271377/ (accessed on 26 June 2023).
- Socinski, M.A.; Jotte, R.M.; Cappuzzo, F.; Orlandi, F.; Stroyakovskiy, D.; Nogami, N.; Rodríguez-Abreu, D.; Moro-Sibilot, D.; Thomas, C.A.; Barlesi, F.; et al. Atezolizumab for First-Line Treatment of Metastatic Nonsquamous NSCLC. N. Engl. J. Med. 2018, 378, 2288–2301. [Google Scholar] [CrossRef] [PubMed]
- Nogami, N.; Barlesi, F.; Socinski, M.A.; Reck, M.; Thomas, C.A.; Cappuzzo, F.; Mok, T.S.; Finley, G.; Aerts, J.G.; Orlandi, F.; et al. IMpower150 Final Exploratory Analyses for Atezolizumab Plus Bevacizumab and Chemotherapy in Key NSCLC Patient Subgroups With EGFR Mutations or Metastases in the Liver or Brain. J. Thorac. Oncol. 2021, 17, 309–323. [Google Scholar] [CrossRef] [PubMed]
- IMpower150 Final Overall Survival Analyses for Atezolizumab Plus Bevacizumab and Chemotherapy in First-Line Metastatic Nonsquamous NSCLC. J Thorac Oncol. 2021, 16, 1909–1924. [CrossRef]
- West, H.; McCleod, M.; Hussein, M.; Morabito, A.; Rittmeyer, A.; Conter, H.J.; Kopp, H.-G.; Daniel, D.; McCune, S.; Mekhail, T.; et al. Atezolizumab in combination with carboplatin plus nab-paclitaxel chemotherapy compared with chemotherapy alone as first-line treatment for metastatic non-squamous non-small-cell lung cancer (IMpower130): a multicentre, randomised, open-label, phase 3 trial. Lancet Oncol. 2019, 20, 924–937. [Google Scholar] [CrossRef]
- Jotte, R.; Cappuzzo, F.; Vynnychenko, I.; Stroyakovskiy, D.; Rodríguez-Abreu, D.; Hussein, M.; Soo, R.; Conter, H.J.; Kozuki, T.; Huang, K.-C.; et al. Atezolizumab in Combination With Carboplatin and Nab-Paclitaxel in Advanced Squamous NSCLC (IMpower131): Results From a Randomized Phase III Trial. J. Thorac. Oncol. 2020, 15, 1351–1360. [Google Scholar] [CrossRef]
- Nishio, M.; Saito, H.; Goto, K.; Watanabe, S.; Sueoka-Aragane, N.; Okuma, Y.; Kasahara, K.; Chikamori, K.; Nakagawa, Y.; Kawakami, T. IMpower132: Atezolizumab plus platinum-based chemotherapy vs chemotherapy for advanced NSCLC in Japanese patients. Cancer Sci. 2021, 112, 1534–1544. [Google Scholar] [CrossRef]
- Gogishvili, M.; Melkadze, T.; Makharadze, T.; Giorgadze, D.; Dvorkin, M.; Penkov, K.; Laktionov, K.; Nemsadze, G.; Nechaeva, M.; Rozhkova, I.; et al. Cemiplimab plus chemotherapy versus chemotherapy alone in non-small cell lung cancer: a randomized, controlled, double-blind phase 3 trial. Nat. Med. 2022, 28, 2374–2380. [Google Scholar] [CrossRef]
- Makharadze, T.; Gogishvili, M.; Melkadze, T.; Baramidze, A.; Giorgadze, D.; Penkov, K.; Laktionov, K.; Nemsadze, G.; Nechaeva, M.; Rozhkova, I.; et al. Cemiplimab Plus Chemotherapy Versus Chemotherapy Alone in Advanced NSCLC: 2-Year Follow-Up From the Phase 3 EMPOWER-Lung 3 Part 2 Trial. J. Thorac. Oncol. 2023, 18, 755–768. [Google Scholar] [CrossRef]
- Paz-Ares, L.G.; Ciuleanu, T.-E.; Cobo, M.; Bennouna, J.; Schenker, M.; Cheng, Y.; Juan-Vidal, O.; Mizutani, H.; Lingua, A.; Reyes-Cosmelli, F.; et al. First-Line Nivolumab Plus Ipilimumab With Chemotherapy Versus Chemotherapy Alone for Metastatic NSCLC in CheckMate 9LA: 3-Year Clinical Update and Outcomes in Patients With Brain Metastases or Select Somatic Mutations. J. Thorac. Oncol. 2022, 18, 204–222. [Google Scholar] [CrossRef]
- Paz-Ares, L.; Ciuleanu, T.-E.; Cobo, M.; Schenker, M.; Zurawski, B.; Menezes, J.; Richardet, E.; Bennouna, J.; Felip, E.; Juan-Vidal, O.; et al. First-line nivolumab plus ipilimumab combined with two cycles of chemotherapy in patients with non-small-cell lung cancer (CheckMate 9LA): an international, randomised, open-label, phase 3 trial. Lancet Oncol. 2021, 22, 198–211. [Google Scholar] [CrossRef] [PubMed]
- Gandhi, L.; Rodríguez-Abreu, D.; Gadgeel, S.; Esteban, E.; Felip, E.; De Angelis, F.; Domine, M.; Clingan, P.; Hochmair, M.J.; Powell, S.F.; et al. Pembrolizumab plus Chemotherapy in Metastatic Non–Small-Cell Lung Cancer. N. Engl. J. Med. 2018, 378, 2078–2092. [Google Scholar] [CrossRef] [PubMed]
- Garassino, M.C.; Gadgeel, S.; Speranza, G.; Felip, E.; Esteban, E.; Dómine, M.; Hochmair, M.J.; Powell, S.F.; Bischoff, H.G.; Peled, N.; et al. Pembrolizumab Plus Pemetrexed and Platinum in Nonsquamous Non–Small-Cell Lung Cancer: 5-Year Outcomes From the Phase 3 KEYNOTE-189 Study. J. Clin. Oncol. 2023, 41, 1992–1998. [Google Scholar] [CrossRef] [PubMed]
- Paz-Ares, L.; Luft, A.; Vicente, D.; Tafreshi, A.; Gümüş, M.; Mazières, J.; Hermes, B.; Çay Şenler, F.; Csőszi, T.; Fülöp, A.; et al. Pembrolizumab plus Chemotherapy for Squamous Non–Small-Cell Lung Cancer. N. Engl. J. Med. 2018, 379, 2040–2051. [Google Scholar] [CrossRef]
- Novello, S.; Kowalski, D.M.; Luft, A.; Gümüş, M.; Vicente, D.; Mazières, J.; Rodríguez-Cid, J.; Tafreshi, A.; Cheng, Y.; Lee, K.H.; et al. Pembrolizumab Plus Chemotherapy in Squamous Non–Small-Cell Lung Cancer: 5-Year Update of the Phase III KEYNOTE-407 Study. J. Clin. Oncol. 2023, 41, 1999–2006. [Google Scholar] [CrossRef]
- Borghaei, H.; Langer, C.J.; Paz-Ares, L.; Rodríguez-Abreu, D.; Halmos, B.; Garassino, M.C.; Houghton, B.; Kurata, T.; Cheng, Y.; Lin, J.; et al. Pembrolizumab plus chemotherapy versus chemotherapy alone in patients with advanced non–small cell lung cancer without tumor PD-L1 expression: A pooled analysis of 3 randomized controlled trials. Cancer 2020, 126, 4867–4877. [Google Scholar] [CrossRef]
- Johnson, M.L.; Cho, B.C.; Luft, A.; Alatorre-Alexander, J.; Geater, S.L.; Laktionov, K.; Kim, S.-W.; Ursol, G.; Hussein, M.; Lim, F.L.; et al. Durvalumab With or Without Tremelimumab in Combination With Chemotherapy as First-Line Therapy for Metastatic Non–Small-Cell Lung Cancer: The Phase III POSEIDON Study. J. Clin. Oncol. 2023, 41, 1213–1227. [Google Scholar] [CrossRef]
- Rittmeyer, A.; Barlesi, F.; Waterkamp, D.; Park, K.; Ciardiello, F.; von Pawel, J.; Gadgeel, S.M.; Hida, T.; Kowalski, D.M.; Dols, M.C.; et al. Atezolizumab versus docetaxel in patients with previously treated non-small-cell lung cancer (OAK): a phase 3, open-label, multicentre randomised controlled trial. Lancet 2017, 389, 255–265. [Google Scholar] [CrossRef]
- Mazieres, J.; Rittmeyer, A.; Gadgeel, S.; Hida, T.; Gandara, D.R.; Cortinovis, D.L.; Barlesi, F.; Yu, W.; Matheny, C.; Ballinger, M.; et al. Atezolizumab Versus Docetaxel in Pretreated Patients With NSCLC: Final Results From the Randomized Phase 2 POPLAR and Phase 3 OAK Clinical Trials. J. Thorac. Oncol. 2020, 16, 140–150. [Google Scholar] [CrossRef]
- Borghaei, H.; Paz-Ares, L.; Horn, L.; Spigel, D.R.; Steins, M.; Ready, N.E.; Chow, L.Q.; Vokes, E.E.; Felip, E.; Holgado, E.; et al. Nivolumab versus Docetaxel in Advanced Nonsquamous Non-Small-Cell Lung Cancer. N. Engl. J. Med. 2015, 373, 1627–1639. [Google Scholar] [CrossRef]
- CheckMate 171: A phase 2 trial of nivolumab in patients with previously treated advanced squamous non-small cell lung cancer, including ECOG PS 2 and elderly populations_OLD [Internet]. Available online: https://es.ereprints.elsevier.cc/checkmate-171-phase-2-trial-nivolumab-patients-previously-treated-advanced-squamous-non-small-cell/fulltext (accessed on 28 May 2023).
- Borghaei H, Gettinger S, Vokes EE, Chow LQM, Burgio MA, de Castro Carpeno J, et al. Five-Year Outcomes From the Randomized, Phase III Trials CheckMate 017 and 057: Nivolumab Versus Docetaxel in Previously Treated Non-Small-Cell Lung Cancer. J Clin Oncol [Internet]. 2021 Mar 1;39(7). Available online: https://pubmed.ncbi.nlm.nih.gov/33449799/ (accessed on 28 May 2023).
- Herbst, R.S.; Baas, P.; Kim, D.-W.; Felip, E.; Pérez-Gracia, J.L.; Han, J.-Y.; Molina, J.; Kim, J.-H.; Arvis, C.D.; Ahn, M.-J.; et al. Pembrolizumab versus docetaxel for previously treated, PD-L1-positive, advanced non-small-cell lung cancer (KEYNOTE-010): a randomised controlled trial. Lancet 2015, 387, 1540–1550. [Google Scholar] [CrossRef] [PubMed]
- Herbst, R.S.; Garon, E.B.; Kim, D.-W.; Cho, B.C.; Gervais, R.; Perez-Gracia, J.L.; Han, J.-Y.; Majem, M.; Forster, M.D.; Monnet, I.; et al. Five Year Survival Update From KEYNOTE-010: Pembrolizumab Versus Docetaxel for Previously Treated, Programmed Death-Ligand 1–Positive Advanced NSCLC. J. Thorac. Oncol. 2021, 16, 1718–1732. [Google Scholar] [CrossRef] [PubMed]
- Brown TJ, Mamtani R, Bange EM. Immunotherapy Adverse Effects. JAMA oncology [Internet]. 2021 Dec 1;7(12). Available online: https://pubmed.ncbi.nlm.nih.gov/34709372/ (accessed on 28 May 2023).
- Martins, F.; Sofiya, L.; Sykiotis, G.P.; Lamine, F.; Maillard, M.; Fraga, M.; Shabafrouz, K.; Ribi, C.; Cairoli, A.; Guex-Crosier, Y.; et al. Adverse effects of immune-checkpoint inhibitors: Epidemiology, management and surveillance. Nat. Rev. Clin. Oncol. 2019, 16, 563–580. [Google Scholar] [CrossRef] [PubMed]
- Ferrara R, Imbimbo M, Malouf R, Paget-Bailly S, Calais F, Marchal C, et al. Single or combined immune checkpoint inhibitors compared to first-line platinum-based chemotherapy with or without bevacizumab for people with advanced non-small cell lung cancer. Cochrane Database Syst Rev [Internet]. 2021;2021(4). Available online: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC8092423/ (accessed on 26 June 2023).
- Zhou, C.; Li, M.; Wang, Z.; An, D.; Li, B. Adverse events of immunotherapy in non-small cell lung cancer: A systematic review and network meta-analysis. Int. Immunopharmacol. 2021, 102, 108353. [Google Scholar] [CrossRef]
- Kichloo, A.; Albosta, M.; Dahiya, D.; Guidi, J.C.; Aljadah, M.; Singh, J.; Shaka, H.; Wani, F.; Kumar, A.; Lekkala, M. Systemic adverse effects and toxicities associated with immunotherapy: A review. World J. Clin. Oncol. 2021, 12, 150–163. [Google Scholar] [CrossRef]
- Thompson JA, Schneider BJ, Brahmer J, Achufusi A, Armand P, Berkenstock MK, et al. Management of Immunotherapy-Related Toxicities, Version 1.2022, NCCN Clinical Practice Guidelines in Oncology. J Natl Compr Canc Netw [Internet]. 2022 Apr;20(4). Available online: https://pubmed.ncbi.nlm.nih.gov/35390769/ (accessed on 28 May 2023).
- Di Federico A, De Giglio A, Parisi C, Gelsomino F. STK11/LKB1 and KEAP1 mutations in non-small cell lung cancer: Prognostic rather than predictive? Eur J Cancer [Internet]. 2021 Nov;157. Available online: https://pubmed.ncbi.nlm.nih.gov/34500370/ (accessed on 26 June 2023).
- Sholl, L.M. Biomarkers of response to checkpoint inhibitors beyond PD-L1 in lung cancer. Mod. Pathol. 2022, 35, 66–74. [Google Scholar] [CrossRef]
- Grant, M.J.; Herbst, R.S.; Goldberg, S.B. Selecting the optimal immunotherapy regimen in driver-negative metastatic NSCLC. Nat. Rev. Clin. Oncol. 2021, 18, 625–644. [Google Scholar] [CrossRef]
- Waterhouse, D.M.; Garon, E.B.; Chandler, J.; McCleod, M.; Hussein, M.; Jotte, R.; Horn, L.; Daniel, D.B.; Keogh, G.; Creelan, B.; et al. Continuous Versus 1-Year Fixed-Duration Nivolumab in Previously Treated Advanced Non–Small-Cell Lung Cancer: CheckMate 153. J. Clin. Oncol. 2020, 38, 3863–3873. [Google Scholar] [CrossRef]
- Mazieres, J.; Drilon, A.; Lusque, A.B.; Mhanna, L.; Cortot, A.; Mezquita, L.; Thai, A.A.; Mascaux, C.; Couraud, S.; Veillon, R.; et al. Immune checkpoint inhibitors for patients with advanced lung cancer and oncogenic driver alterations: results from the IMMUNOTARGET registry. Ann. Oncol. 2019, 30, 1321–1328. [Google Scholar] [CrossRef]
- Gainor, J.F.; Shaw, A.T.; Sequist, L.V.; Fu, X.; Azzoli, C.G.; Piotrowska, Z.; Huynh, T.G.; Zhao, L.; Fulton, L.; Schultz, K.R.; et al. EGFR Mutations and ALK Rearrangements Are Associated with Low Response Rates to PD-1 Pathway Blockade in Non–Small Cell Lung Cancer: A Retrospective Analysis. Clin. Cancer Res. 2016, 22, 4585–4593. [Google Scholar] [CrossRef] [PubMed]
- Shaw, A.T.; Lee, S.-H.; Ramalingam, S.S.; Bauer, T.M.; Boyer, M.J.; Costa, E.C.; Felip, E.; Han, J.-Y.; Hida, T.; Hughes, B.G.M.; et al. Avelumab (anti–PD-L1) in combination with crizotinib or lorlatinib in patients with previously treated advanced NSCLC: Phase 1b results from JAVELIN Lung 101. J. Clin. Oncol. 2018, 36, 9008–9008. [Google Scholar] [CrossRef]
- Oxnard, G.R.; Yang, J.C.-H.; Yu, H.; Kim, S.-W.; Saka, H.; Horn, L.; Goto, K.; Ohe, Y.; Mann, H.; Thress, K.S.; et al. TATTON: a multi-arm, phase Ib trial of osimertinib combined with selumetinib, savolitinib, or durvalumab in EGFR-mutant lung cancer. Ann. Oncol. 2020, 31, 507–516. [Google Scholar] [CrossRef] [PubMed]

Table 1.
ICI approved for treatment in metastatic NSCLC.
| Drug | Type | Indications |
|---|---|---|
| Atezolizumab | Anti-PD-L1 | First-line treatment (*, **): - Monotherapy for patients with mNSCLC without EGFR or ALK genomic tumour aberrations and PD-L1 stained ≥ 50% of tumour cells or PD-L1 stained tumour-infiltrating immune cells ≥ 10%. - In combination with bevacizumab and chemotherapy (platinum- based + paclitaxel/nab-paclitaxel) for patients with metastatic non-squamous NSCLC without EGFR or ALK aberrations and regardless PDL1 status. - In combination with chemotherapy (platinum- based + paclitaxel/nab-paclitaxel/ pemetrexed) for patients with metastatic non-squamous NSCLC without EGFR or ALK aberrations and regardless PDL1 status. Subsequent line monotherapy for the treatment of patients with mNSCLC who have disease progression during or following platinum-containing chemotherapy regardles histology and PDL1 status (*, **). |
| Cemiplimab | Anti-PD1 | First-line treatment (*, **): - Monotherapy for patients with mNSCLC with no EGFR, ALK or ROS1 aberrations and with high PD-L1 expression [Tumour Proportion Score (TPS) ≥ 50%]. - In combination with chemotherapy for patients with mNSCLC without EGFR, ALK or ROS1 aberrations, regardless histology and PD-L1 status. |
| Nivolumab | Anti-PD1 | Subsequent line monotherapy for the treatment mNSCLC who has been progressed after platinum-based chemotherapy. Patients with EGFR or ALK aberrations must have disease progression at least one target therapy (*, **). |
| Nivolumab/ Ipililumab | Anti-PD1/ Anti-CTLA4 | First-line treatment (*, **): - In combination for patients with mNSCLC expressing PD-L1 ≥1%, with no EGFR or ALK genomic tumour aberrations. - In combination with platinum-based chemotherapy for 2 cycles in adults, whose tumours have no EGFR mutation or ALK translocation, regardless PDL-1 expression. |
| Pembrolizumab | Anti-PD1 | First-line treatment (*, **): - Single agent for patients with NSCLC expressing PD-L1 (TPS) ≥1% with no EGFR or ALK genomic tumour aberrations. - In combination with pemetrexed and platinum chemotherapy for patients with metastatic non-squamous NSCLC, without EGFR or ALK genomic tumour aberrations. - In combination with carboplatin and either paclitaxel or nab-paclitaxel for patients with metastatic squamous NSCLC. Subsequent-line treatment (*, **): - Single agent patients with mNSCLC with PD-L1 (TPS ≥1%), whose had progression on or after platinum-containing chemotherapy. Patients with EGFR or ALK aberrations must have disease progression at least one target therapy. |
| Tremelimumab/ Durvalumab | Anti-CTLA4/Anti-PD-L1 | First-line treatment in combination with platinum-based chemotherapy for the treatment of patients with mNSCLC without EGFR or ALK genomic tumour aberrations, regardless histology. |
(*) Approved by U.S. Food and Drug Administration (FDA). (**) Approved by European Medicines Agency (EMA).
Table 2.
Single agents ICI for treatment of NSCLC at first line.
| ICIs | Trial | Population | Primary endpoint | ORR | PFS | OS | 5y/ 3y *-ORR | 5y/3y*- PFS | 5y/3y*-OS |
|---|---|---|---|---|---|---|---|---|---|
| Atezolizumab | IMpower 110 | PD-L1 ≥ 50% or IC ≥10%; squamous and non-squamous histology | OS | 38.3 vs 28.6 % | 8.1 vs 5.0 months | 20.2 vs 13.1 months | 40.2% | 8.2 months | 20.2 vs 14.7 months |
| Cemiplimab | EMPOWER-Lung 1 | PD-L1 ≥ 50%; squamous and non-squamous histology | OS and PFS | 39.0 vs 20% | 8.2 vs 5.7 months | NR vs 14.2 months | 46.5 vs 21.0%* | 8.1 vs 5.3 months* | 26.1 months* |
| Nivolumab plus ipilimumab | CheckMate 227 | PD-L1 ≥ 1%; squamous and non-squamous histology | OS | 35.9 vs 30.0% | 5.1 vs 5.6 months | 17.1 vs 14.9 months | 24% | ||
| Pembrolizumab | KEYNOTE-024 | PD-L1 ≥ 50%; squamous and non-squamous histology | PFS | 45% | 10.3 months | 26.3 months (80.2%). | 46.1 vs 31.1% | 7.7 vs 5.5 months | 26.3 vs 13.4 months (31.9%) |
| KEYNOTE-042 | PD-L1 ≥ 1%; squamous and non-squamous histology | OS | 27vs 27% | 5.4 vs 6.5 months | 16.7 vs 12.1 months | 27.3% | 5.6 months | 16.4 months |
Table 3.
ICI Combined agents for the treatment of NSCLC in the first line.
| ICIs | Trial | Population | Primary endpoint | ORR | PFS | OS | 5y/ 3y *-ORR | 5y/3y*- PFS | 5y/3y*-OS |
|---|---|---|---|---|---|---|---|---|---|
| Atezolizumab plus Bevacizumab plus CT | IMpower150 | Any PD-L1 and Non-squamous histology | PFS and OS | 63.5% (ABCP) vs 48.0% (BCP) |
8.3 vs 6.8 months ABCP vs BCP HR 0.62 (95% CI 0.52-0.74) |
19.5 vs 14.7 months ABCP vs BCP: HR 0.78 (95% CI 0.64-0.96) |
8.4 vs 6.8 months ABCP vs BCP HR 0.57 (95% CI 0.48-0.67) |
19.5 vs 14.7 months HR 0.80 (95% CI 0.67-0.95) | |
| Atezolizumab plus platinum plus paclitaxel/nab paclitaxel | IMpower130 | Any PD-L1 and Non-squamous histology | PFS and OS | 49.2% vs 31.9% | 7.0 versus 5.5 months (HR 0.64; 95% CI 0.54-0.77) | 18.6 versus 13.9 months (HR 0.79; 95% CI 0·64-0·98) | - | - | - |
| Atezolizumab plus platinum plus paclitaxel/nab paclitaxel | IMpower131 | Any PD-L1 and squamous histology | PFS and OS | 49.4% vs 41.3% | 6.3 vs 5.6 months HR 0.71 (95% CI 0.60–0.85) | 14.2 versus 13.5 months (HR 0.88; 95% CI 0.73-1.05) | - | - | - |
| Atezolizumab plus platinum plus pemetrexed | IMpower132 | Any PD-L1 and Non-squamous histology | PFS and OS | 47% vs 32% | 7.6 versus 5.2 months; HR 0.60, 95% CI 0.49-0.72 | 18.1 versus 13.6 months; HR 0.81, 95% CI 0.64-1.03 | - | - | 17.5 vs 13.6 months*; HR 0.86 (0.71-1.06) |
| Cemiplimab plus platinum-doublet chemotherapy | EMPOWER-Lung 3 | Any PD-L1; squamous and Non-squamous histology | OS | 43.3% vs 22.7% | 8.2 vs 5.0 months HR = 0.56; 95% CI, 0.44–0.70 | 21.9 vs 13.9 months; HR 0.71; 95% CI, 0.53- 0.93 | 43.6% versus 22.1% | 8.2 months versus 5.5 months (HR 0.55, 95% CI 0.44–0.68 | 21.1 versus 12.9 months; HR 0.65, 95% CI 0.51–0.82 |
| Nivolumab plus ipilimumab and 2 cycles of platinum-doublet chemotherapy | CheckMate 9LA | Any PD-L1; squamous and Non-squamous histology | OS | 37.7% vs 25.1% | 6.8 vs 5.0 months HR 0.70 [97·48% CI 0.57–0.86 |
14.1 versus 10.7 months; HR 0.69; 96.71% CI 0.55-0.87 | 38% vs 25%* | 6.4 versus 5.3 months * | 15.8 versus 11 months *; HR 0.74, 95% CI 0.62–0.87 |
| Pembrolizumab plus platinum (carboplatin or cisplatin) plus pemetrexed | KEYNOTE-189 | Any PD-L1 and Non-squamous histology | PFS and OS | 47.6% vs 18.9% | 8.8 vs 4.9 months HR 0.52 (95% CI 0.43–0.64) |
NR vs 11.3 months; HR 0.49; 95% CI 0.38 - 0.64 |
48.3% vs 19.9% | 9.0 versus 4.9 months; HR 0.5; 95% CI 0.42‒0.60 | 22.0 versus 10.6 months; HR 0.6; 95% CI 0.50-0.72 |
| Pembrolizumab plus platinum (carboplatin or cisplatin) plus Paclitaxel or nab-paclitaxel | KEYNOTE-407 | Any PD-L1 and squamous histology | PFS and OS | 57.9% vs 38.4% | 6.4 versus 4.8 months; HR 56; 95% CI 0.45-0.70 | 15.9 months and 11.3 months HR 0.64; 95% CI 0.49 - 0.85 | 66.2% vs 38.8% | 8 versus 5.1 months; HR 0.62; CI 0.52-0.74 | 17.2 versus 11.6 months HR 0.71; 95% CI 0.59-0.85 |
| Tremelimumab plus durvalumab plus CT | POSEIDON | Any PD-L1; squamous and Non-squamous histology | PFS and OS | 46.3% vs 33.4% | 6.2 v 4.8 months; HR 0.72; 95% CI 0.60 - 0.86 | 14.0 versus 11.7 months; HR 0.77; 95% CI 0.65 - 0.92 | - | - | - |
Table 4.
Second line ICI treatments.
| ICIs | Trial | Population | Primary endpoint | ORR | PFS | OS |
|---|---|---|---|---|---|---|
| Atezolizumab | OAK | Patients with NSCLC, any histology, whose had received one or two previous chemotherapy regimens for stage IIIB or IV, except docetaxel, CD137 agonists, anti-CTLA4, anti PD-L1 or PD-1. | OS | 14% vs 13% | 2.8 VS 4.0 months; HR 0.95 95% CI 0.82-1.10 | 13.8 vs 9.6 months; HR 0.73; 95% CI 0.62-0.87. 4y rate: 15.5% vs 8.7%. |
| Nivolumab | CheckMate-057 | Patients with metastatic non-squamous NSCLC who progressed after the first line with platinum-based doublet CT. | OS | 19% vs 12% | 2.3 vs 4.7 months (HR 0.92; 95% CI 0.77-1.11 | 12.2 vs 9.4 months (HR 0.73; 95% CI 0.59-0.89 |
| CheckMate-017 | Patients with metastatic squamous NSCLC who progressed after the first line with platinum-based doublet CT. | OS | 20% vs 9% | 3.5 versus 2.8 months (HR 0.62; 95% CI 0.47- 0.81 | 9.2 vs 6.0 months HR 0.59; 95% CI 0.44–0.79 | |
| Pembrolizumab | KEYNOTE-010 | Previously treated patients with PD-L1 positive (≥1%) advanced NSCLC, regardless histology | PFS and OS | 18% vs 9% | 4.0 versus 4.0 months (HR 0·79, 0·66–0·94 | 12.7 vs 5.5 months HR 0.71; 95% CI 0.58-0.88 5y: 11.8 months versus 8.4 months (HR 0.70; CI 0.61–0.80) |
Table 5.
Immune-mediated adverse events.
| Drug | Dose | Diarrhea | Colitis | Pulmonary | Rash | Neurological | Endocrinopathy | Hepatic | Renal |
|---|---|---|---|---|---|---|---|---|---|
| Atezolizumab | |||||||||
| IMPOWER 110 | 1,200 mg 3-weekly | - | - | 4.9% | - | - | - | - | - |
| IMPOWER 150 | 1,200 mg 3-weekly | 20.6% | - | - | 13.3% | 49.4% (neuropathy included) | - | - | |
| OAK | 1,200 mg 3-weekly | 15.4% | 0.3% | 1% | - | - | - | 0.3% | - |
| Cemiplimab | |||||||||
| EMPOWER-Lung 1 | 350 mg 3-weekly | 5% | 1% | 6% | 5% | 3% | - | 6% | 1% |
| EMPOWER-Lung 1 | 350 mg 3-weekly | 10.6% | - | 12.5% | - | - | - | 30% | - |
| Nivolumab | |||||||||
| CheckMate 057 |
3 mg/kg, 2-weekly | 8% | 1% | 4.9% | 9% | 0.3% | 10.5% |
10.8% | 2% |
| Nivolumab/ Ipililumab | |||||||||
| CHECK MATE 227 |
1 mg/kg 6-weekly ipilimumab plus 3 mg/kg 2-weekly nivolumab (576) |
16.3% | 1% | 3% | 16.7% | - |
12.3% |
3.5% | - |
| Pembrolizumab | |||||||||
| KEYNOTE-054 | 200 mg, 3-weekly | 19.1% | 3.7% | 4.7% | 16.1% | – | 23.4% | 1.8% | 0.4% |
| KEYNOTE-010 | 10 mg/kg, 3-weekly | 6% | 1% | 4% | 13% | – | 16.5% | 1% | – |
| KEYNOTE-189 | 200 mg, 3-weekly | - | 2.2% | 4.4% | 2% | - | 12.8% | - | 1.7% |
| KEYNOTE-042 | 200 mg, 3-weekly | 5% | 1% | 8% | 7% | 1% | 18% | 7% | <1% |
| Tremelimumab/ Durvalumab | |||||||||
| POSEIDON | 13.9% | 3.9% | 3.6% | 3.9% | - | - | - | - |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



