
Submitted:
14 July 2023
Posted:
18 July 2023
You are already at the latest version
Abstract
Background: Misconceptions and knowledge gaps about antibiotic use contribute to inappropriate antibiotic use and antimicrobial resistance. Aim: Identifying and prioritizing misconceptions and knowledge gaps about antibiotic use from a healthcare professionals’ perspective. Methods: A modified Delphi study of two rounds with an expert meeting. A literature search was conducted to create statements about misconceptions and knowledge gaps about antibiotic use. These were rated by healthcare professionals from five EU countries representing general practice, out-of-hour services, nursing homes, and pharmacies. Consensus was achieved if ≥80% of the participants rated 4+ on a five-point Likert scale during the second Delphi round. Results. In total, 44 misconceptions were identified through the literature search within four themes: 1) antimicrobial resistance in general, 2) use of antibiotics in general, 3) use of antibiotics for respiratory tract infections, and 4) use of antibiotics for urinary tract infections. Consensus was reached for more than half of the statements within each setting. Conclusions. Experts from different settings and nationalities acknowledge that multiple misconceptions and knowledge gaps can contribute to inappropriate use of antibiotics in the community. These results provide valuable information to use in educational campaigns for patients and healthcare professionals to improve the use of antibiotics.
Keywords:
antimicrobial resistance
; antibiotics
; antibiotic use
; misconceptions and knowledge gaps
; general practice
; out-of-hours services
; nursing homes
; community pharmacies
1. Introduction
The rise in antimicrobial resistance (AMR) impacts the effectiveness of antibiotics dramatically [1]; a 2022 systematic analysis [2] estimated 4.95 million deaths globally in 2019 due to AMR of which about 1.27 million were directly attributable to infections caused by resistant bacteria. Inappropriate use of antibiotics, i.e., overprescribing and misuse, is the main driver of AMR [3]. To ensure effectiveness of antibiotics in the future, it is essential to improve rational antibiotic use.
Misconceptions and lack of knowledge about antibiotics are important factors contributing to inappropriate antibiotic use [4]. According to the literature, from the patient perspective, these include false perceptions of use and effectiveness of antibiotics and lack of understanding of AMR. From the perspective of the healthcare professionals (HCPs), a perceived demand of antibiotics by the patients and fear of under-treatment are among the misconceptions that can lead to overprescribing of antibiotics [4].
To address misconceptions and knowledge gaps, it is crucial to identify these systematically and use this information to develop suitable information materials that can be implemented in antimicrobial stewardship programs. Antimicrobial stewardship programs lead to a sustainable change in the behavior of antibiotic prescribing and consumption [5] when they involve all relevant settings and local stakeholders [6,7]. Therefore, it is important to include the end-users in the design process to increase the applicability and suitability of the intervention materials [8].
Whilst knowledge and perceptions about antibiotic use and AMR have been thoroughly studied, such studies often focus on patients [9,10] or students [11,12] in specific settings or countries, and many assess only basic knowledge about indications and efficacy of antibiotics. There has been limited focus on specific groups of HCPs, such as prescribers [13,14] or pharmacists [15]. Furthermore, we lack insight in knowledge gaps and misconceptions that different HCPs in the community setting in Europe come across during their daily practice.
This study is part of the Health Alliance for Prudent Prescribing and Yield of Antibiotics in a Patient-Centered Perspective (HAPPY PATIENT) project [16] that aims to reduce the misuse of antibiotics in human health by involving HCPs from four healthcare settings (general practice, out-of-hours services (OoHS), nursing homes, and community pharmacies) across five target countries (France, Greece, Lithuania, Poland, Spain). The present study aimed to identify and prioritize misconceptions and knowledge gaps that lead to inappropriate use of antibiotics from the perspective of HCPs working in the aforementioned settings. The information about misconceptions and knowledge gaps was used for the development of setting-specific interventions in the HAPPY PATIENT project.
2. Results
2.1. Literature search
The literature search resulted in 46 statements representing knowledge gaps and misconceptions on antibiotic use. The statements were extracted from a total of 27 publications (Supplementary file S3]. These statements were divided into four domains: 1) AMR in general, 2) use of antibiotics in general, 3) antibiotics for acute respiratory tract infections, and 4) antibiotics for urinary tract infections. After review of the statements by the HAPPY PATIENT project consortium members, a total of 44 final statements were included in the study.
2.2. Delphi process
Altogether, 66 experts completed the first round of the Delphi study, of whom 45 (68%) completed the second round (Table 1).
Healthcare professionals in general practice rated 39 statements to be important or very important with at least 80% consensus, which was higher than in OoHS (26 statements), nursing homes (18 statements) and pharmacies (31 statements). After the expert meeting and the second Delphi round, the number of statements that reached consensus changed in all settings. It decreased in general practice (34 statements) and increased in OoHS (30 statements), nursing homes (24 statements) and pharmacies (36 statements) (Table 2).
2.3. Antimicrobial resistance
Four out of eight statements within the theme of AMR reached consensus for importance in all four settings (Table 3), for the other statements there was no consensus in at least two settings. The experts experience that patients do not consider AMR a problem in their country and that not all antibiotics are at risk of becoming ineffective. Regarding HCPs, there is misconception about resistance not being a problem at their own workplaces and that newly discovered antibiotics will solve the problem of resistance.
2.4. General use of antibiotics
In the four settings, consensus of importance was reached for two of nine statements (Table 3). Across all settings there was consensus that patients believe that antibiotics are effective against all type of infections. Furthermore, there was consensus that HCPs erroneously believe that the benefits of prescribing antibiotics when unsure of the bacterial or viral origin of the symptoms outweigh the harms of exposure to antibiotics. For an additional four statements a consensus of importance was reached in three of the four settings.
2.5. The use of antibiotics for respiratory tract infections
Of the fifteen statements on the use of antibiotics for respiratory tract infections four were deemed important by the experts (Table 3). This included the only statement from the patients’ perspective that certain symptoms imply the need for antibiotics. This extends to the statements from the perspective of HCPs, where the misconceptions of sore throat with regional symptoms and fever, cough with purulent sputum or purulent nasal discharge suggest a bacterial infection that require antibiotics, are considered important.
2.6. The use of antibiotics for urinary tract infections
The final statements for which consensus of importance was reached in four settings were three of the twelve statements regarding antibiotic use for urinary tract infections (Table 3). Two of these were similar to statements for respiratory tract infections where there is misconception about the presence of specific symptoms, which would imply the need for antibiotics. The third statement concerns the use of antibiotics to prevent complications of an uncomplicated urinary tract infection.
3. Discussion.
3.1. Main findings
In total, 44 misconceptions were identified through the literature search, eleven targeting patients and 33 targeting HCPs. Healthcare professionals in all settings recognize there are numerous misconceptions or knowledge gaps about AMR, however, the setting in which they act influences which specific misconceptions they rate as important. To a certain extent, this can be explained by the nature of the different settings; in nursing homes, sharing of leftover antibiotics with family or friends is not considered a relevant misconception. Similarly, as pharmacists generally do not use diagnostic tests, diagnostic tests are not rated important in this setting. Generally, the experts reached consensus on a list of misconceptions regarding antibiotics, therewith establishing a fundament for the development of interventions to improve antibiotic use and increase knowledge.
3.2. Strengths and limitations of the study
The main strength of this study is that we used input from a panel of experts who have profound experience within their fields and in antimicrobial stewardship initiatives. Additionally, the sample of experts was interdisciplinary and cross-national. Previous studies have shown that a heterogeneous sample allows for a wider range of perspectives to be taken into consideration, and thus, leading to a better performance and increased quality and acceptance of decision [18,20,21,22].The rating of the statements was conducted anonymously, thus the discussion and consensus process were not dominated by only a small group of experts [18,19,20].
This study has several limitations that are inherent to the Delphi methodology or introduced through modifications for the specific aims of this study. Common limitations of the Delphi methodology include the lack of a definition on how to define consensus [23], who qualifies as an expert [18,24] and lack of agreement about the optimal number of rating rounds [18,19,20,23,25]. Additionally, the size of the Likert scale has been debated in the literature and may come with some methodological limitations [19,23,24,26]. We used a five-point Likert scale, as it ranks high in terms of reliability, validity, and ease of use.
Lack of English fluency is a limitation of the study, however, our partners in the target countries facilitated the communication with the participants in national languages we reduced the limitation of the language barriers by translating all the statements, instructions, and all study material.
The typical first round of “idea generation” was replaced with a literature search and the study participants received a pre-selected list of statements upon which they were invited to make a judgement. The main advantage of this modification is that the study participants start from a common base, and it allows for an easier data analysis and interpretation [25]. However, this meant that the participants could not introduce new statements, which may have resulted in biased responses [25]. Nevertheless, this type of bias was limited by conducting a broad and structured literature search and discussing the statements with the HAPPY PATIENT consortium.
Finally, the multi-national and multi-disciplinary nature of the study, meant excluding potentially relevant details for specific countries, however, this approach facilitates the creation of educational content based on the results that can be easily transferred to other settings and countries within the EU.
3.3. Comparison with existing literature
A 2015 systematic review [27] on physicians’ knowledge, perceptions and behavior towards antibiotic prescribing in ambulatory and hospital settings found that physicians still have inadequate knowledge about AMR and misconceptions about antibiotic prescribing. The review reports that physicians in many studies did not consider AMR to be a problem in their own clinical practice and would prescribe antibiotics despite knowing that they would have limited benefit for the patients. Similarly, other researchers found that HCPs are aware of AMR being a problem in general, but they do not believe it is a problem in their clinical practice [28]; that HCPs prefer to overprescribe antibiotics to avoid clinical failure or when they are in doubt [28,29,30]; that national antibiotic prescription guidelines have low impact on HCPs prescribing attitudes [28,31]; and that HCPs tend to overprescribe antibiotics to meet patients’ expectations [29,32,33] .
In line with other studies that were conducted in various healthcare settings, we found that some common misconceptions that need to be addressed in intervention materials are 1) that HCPs do not believe that AMR is a problem in their own practice and 2) that they often prescribe antibiotics when they are in doubt about the cause of the infection. Additionally, our study pointed out that antibiotics for UTIs are overprescribed especially in the nursing homes, as the HCPs often misinterpret non-specific symptoms for UTI, or may treat asymptomatic bacteriuria more often than not, despite the fact that bacteria in the urinary tract are very common among the elderly [34].
Previous studies exploring knowledge gaps and misconceptions from the patient perspective found that it is a common misconception that antibiotics are effective against viral infections [35,36,37,38]; that they are effective against or reduce the duration of symptoms of the flu or the common cold [35,36,37,38]; that a cough of duration longer than two weeks requires antibiotic treatment [38]; that it is fine to take antibiotics if they were used in the past to treat similar symptoms [37,38]; and that the public has limited knowledge about AMR and how it occurs [36,37,38,39,40]. Our study affirmed that all the above-mentioned patient misconceptions about antibiotics and AMR are a very common issue that HCPs face in their daily practice and may lead to misuse of antibiotics.
Based on this study, we developed six educational tools (e.g. leaflets, posters, checklists) aimed at HCPs and the public that can be used in the different healthcare settings involved in the study (Supplementary file S4). These tools aim to support the communication between the HCPs and the patients when they discuss their infection and the need and use of antibiotics. The tools contain information about several community-acquired infections, antimicrobial stewardship messages, use of antibiotics, infection prevention messages, and more. Previous antimicrobial stewardship campaigns have created similar educational tools that aim to increase patient knowledge about antibiotics and AMR [41,42,43,44]. The authors encourage practicing HCPs and researchers to use the materials and to develop new material based on this study.
4. Materials and Methods
4.1. Design
4.2. Recruitment and sample size
A panel consisting of experts from the four different settings (general practice, OoHS, nursing homes, and community pharmacies) and the five target countries (France, Greece, Lithuania, Poland, and Spain) was recruited. A member of the HAPPY PATIENT consortium from each country recruited the experts (List of project partners in Supplementary file S1) through national and European professional associations of HCPs, who were then asked to identify other potential experts. We aimed to recruit three experts per county per setting, resulting in 60 experts to complete both rounds of the Delphi process.
Experts were eligible and invited for inclusion if they: a) were HCPs with knowledge and experience within diagnosis of common community-acquired infections, antibiotic use, management of medicines, and antimicrobial stewardship programs; and ii) had no conflicts of interest in participating in the study. There were no restrictions on English fluency, as all materials were translated into national languages.
4.3. Identification of misconceptions and knowledge gaps
We conducted a literature review during May-June 2021 in PubMed, REX library system, and Google Scholar. Search terms included “(antibiotics) AND (misconceptions)”, “(antibiotics) AND (knowledge)”, “(antimicrobial resistance) AND (misconceptions)”, “(antimicrobial resistance) AND (public knowledge)”, “(urinary tract infection) AND (misconceptions)”, “(respiratory tract infection) AND (misconceptions)”, “(respiratory tract infection) AND (diagnosis)”, “(urinary tract infection) AND (diagnosis)”. Studies were included if published in a peer-reviewed scientific journal in English, regardless of publication date, sample size, study design or geographical location. A.C. and G.C. reviewed titles and abstracts to identify knowledge gaps and misconceptions that lead to inappropriate prescribing, dispensing and consumption of antibiotics when managing community-acquired infections, from the perspective of the patient and the HCP. Succeeding the literature review, A.C. and G.C. extracted statements of potential knowledge gaps and misconceptions that may lead to inappropriate use of antibiotics. Subsequently, an iterative review process took place, where the HAPPY PATIENT project consortium reviewed the statements and suggested revisions in the phrasing and in- and exclusion of statements. Emphasis was placed on including statements that were relevant across all target countries.
4.4. Data collection
Two rounds of data collection were implemented between September 2021 and January 2022. SurveyXact® was used to distribute the online survey. A link to each survey was distributed via email to all participants by our host partners, followed by reminders in each survey round.
4.4.1. Round 1
The first round of data collection took place during September-October 2021. The experts received the pre-defined list of 44 statements (Supplementary file S2) and they were instructed to rate the importance of each statement on a 5-point Likert scale: 1=not important, 2=little important, 3=neutral/I don’t know, 4=important, 5=very important. The experts evaluated each statement based on how important they believed the statement contributed to the misuse of antibiotics and the need to be addressed in future intervention materials. The experts were invited to prioritize common misconceptions about AMR, diagnosis and management of community-acquired infections that HCPs face during their daily communication with patients, as well as misconceptions or knowledge gaps of their peers working in their respective healthcare settings that lead to misuse of antibiotics. Response rates were monitored regularly and email reminders were sent to the participants who had not responded to the survey two and four weeks after the initial email invitation.
4.4.2. Feedback and expert meetings
After the first round was completed, all participants received personalized feedback, which included the median, minimal and maximal ratings of each statement. This allowed participants to reflect on their answers based on the group median and provided the basis for the subsequent discussions during the consensus meetings.
During four meetings (one per setting) in November 2021, experts discussed disagreements, provided clarifications, and elaborated on similarities and differences across countries that would benefit the consensus process. During the meetings, no items were discarded from the survey; however, minor changes for some of the statements were suggested and implemented before the second round of the modified Delphi process.
4.4.3. Round 2
The data collection for the second Delphi round took place during December 2021-January 2022. The second survey contained all statements of the first round. In this round, the participants had the opportunity to reassess their initial responses, based on the feedback material and the expert meeting discussions [18,21], and resubmit their rating on the same 5-point Likert scale as in round 1. Response rates were monitored, and email reminders were sent to participants who had not yet completed the survey.
4.5. Definition of consensus and end of Delphi process
Consensus was achieved if ≥80% of the participants rated a statement with 4+ on the five-point Likert scale during the second Delphi round.
4.6. Data analysis
To identify the most important knowledge gaps/misconceptions for each of the four settings included in the study, the data analysis was conducted per setting. All data was imported and analyzed in IBM SPSS version 27. We ran descriptive statistics and calculated frequencies, median, mean and standard deviation, minimum and maximum ratings for all the statements.
5. Conclusions
Experts from four different settings from five EU countries rated the most important knowledge gaps and misconceptions impacting on inappropriate use of antibiotics for the management of community-acquired infections. The results of this study give an overview of different topics that need to be addressed in educational campaigns to optimize antibiotic use. This study has resulted in the development of different intervention materials and can be used as a guide in the development of future antimicrobial stewardship programs targeting the management of community-acquired infections.
Supplementary Materials
The following supporting information can be downloaded at the website of this paper posted on Preprints.org. Supplementary file S1, Supplementary file S2, Supplementary file S3, Supplementary file S4.
Author Contributions
Conceptualization, L.B. and G.C.; study design, A.C., L.B., and G.C.; literature search, A.C. and G.C; development of final list of statements, A.C., G.C., and L.B.; data collection and data analysis, A.C. and L.B.; advisory on study design, data collection and data analysis, M.P.H., G.C.; development of individualized feedback material, A.C.; facilitation of expert meetings, A.C.; interpretation of data, A.C., M.L., K.T., L.B.; writing – original draft preparation, A.C. and M.L.; writing – review and editing, L.B., G.C., K.T., M.P.H.; supervision, L.B., G.C., K.T., M.P.H.; project administration, A.C. All authors have read and approved the final manuscript.
Funding
This publication was funded by the European Union’s Third Health Programme (2014–2020), project ID 900024. The funding body had no role in the design of the study and collection, analysis, and interpretation of data or in writing the manuscript.
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Data Availability Statement
The datasets used and/or analyzed during the current study are available from the corresponding author on request.
Acknowledgments
The authors would like to thank all partners and members of the HAPPY PATIENT consortium for their contribution to this study with specific thanks to all partners in the target countries who have recruited and facilitated communication with the study participants, and translated all study materials into the local languages. Additionally, the authors would like to thank Jette Nygaard Jensen for critically reviewing the manuscript.
Conflicts of Interest
The authors declare no conflict of interest.
List of abbreviations:
| AMR | Antimicrobial resistance |
| HCP(s) | Healthcare professional(s) |
| EU | European Union |
| HAPPY PATIENT | Health Alliance for Prudent Prescribing and Yield of Antibiotics in a Patient-Centred Perspective |
| OoHS | Out-of-hours services |
| RTIs | Respiratory tract infections |
| UTIs | Urinary tract infections |
References
- World Health Organisation. Antimicrobial resistance [Internet]. 2021 [cited 2022 Oct 25]. Available from: https://www.who.int/news-room/fact-sheets/detail/antimicrobial-resistance.
- Murray CJ, Shunji Ikuta K, Sharara F, Swetschinski L, Robles Aguilar G, Gray A, et al. Global burden of bacterial antimicrobial resistance in 2019: a systematic analysis. The Lancet [Internet]. 2022 [cited 2022 Oct 25];399:629–55. [CrossRef]
- Ventola CL. The Antibiotic Resistance Crisis: Part 1: Causes and Threats. Pharmacy and Therapeutics [Internet]. 2015 [cited 2022 Oct 25];40(4):277. Available from: /pmc/articles/PMC4378521/.
- Llor C, Bjerrum L. Antimicrobial resistance: risk associated with antibiotic overuse and initiatives to reduce the problem. Ther Adv Drug Saf [Internet]. 2014 [cited 2022 Dec 7];5(6):229. Available from: /pmc/articles/PMC4232501/.
- Charani E, Cooke J, Holmes A. Antibiotic stewardship programmes-what’s missing? Antibiotic prescribing-a global concern. J Antimicrob Chemother [Internet]. 2010 [cited 2022 Oct 25];65:2275–7. Available from: https://academic.oup.com/jac/article/65/11/2275/768215.
- Macdougall C, Polk RE. Antimicrobial Stewardship Programs in Health Care Systems. Clin Microbiol Rev. 2005;18(4):638–56.
- Slettli Wathne J, Kåre L, Kleppe S, Harthug S, Blix HS, Nilsen RM, et al. The effect of antibiotic stewardship interventions with stakeholder involvement in hospital settings: a multicentre, cluster randomized controlled intervention study. [cited 2022 Oct 25] . [CrossRef]
- van Buul LW, Sikkens JJ, van Agtmael MA, H Kramer MH, van der Steen JT, P M Hertogh CM. Participatory action research in antimicrobial stewardship: a novel approach to improving antimicrobial prescribing in hospitals and long-term care facilities. [cited 2022 Oct 25]; Available from: https://academic.oup.com/jac/article/69/7/1734/2911110.
- Napolitano F, Izzo MT, di Giuseppe G, Angelillo IF. Public Knowledge, Attitudes, and Experience Regarding the Use of Antibiotics in Italy. PLoS One [Internet]. 2013 Dec 23 [cited 2022 Dec 7];8(12):e84177. Available from: https://journals.plos.org/plosone/article?id=10.1371/journal.pone.0084177.
- Tangcharoensathien V, Chanvatik S, Kosiyaporn H, Kirivan S, Kaewkhankhaeng W, Thunyahan A, et al. Population knowledge and awareness of antibiotic use and antimicrobial resistance: results from national household survey 2019 and changes from 2017. BMC Public Health [Internet]. 2021 Dec 1 [cited 2022 Dec 7];21(1):1–14. Available from: https://bmcpublichealth.biomedcentral.com/articles/10.1186/s12889-021-12237-y.
- Jairoun A, Hassan N, Ali A, Jairoun O, Shahwan M, Hassali M. University students’ knowledge, attitudes, and practice regarding antibiotic use and associated factors: a cross-sectional study in the United Arab Emirates. Int J Gen Med [Internet]. 2019 [cited 2022 Dec 7];12:235. Available from: /pmc/articles/PMC6607982/.
- Sakr S, Ghaddar A, Hamam B, Sheet I. Antibiotic use and resistance: An unprecedented assessment of university students’ knowledge, attitude and practices (KAP) in Lebanon. BMC Public Health [Internet]. 2020 Apr 19 [cited 2022 Dec 7];20(1):1–9. Available from: https://bmcpublichealth.biomedcentral.com/articles/10.1186/s12889-020-08676-8.
- Karasneh RA, Al-Azzam SI, Ababneh M, Al-Azzeh O, Al-Batayneh OB, Muflih SM, et al. Prescribers’ knowledge, attitudes and behaviors on antibiotics, antibiotic use and antibiotic resistance in jordan. Antibiotics [Internet]. 2021 Jul 1 [cited 2022 Dec 7];10(7):858. Available from: https://www.mdpi.com/2079-6382/10/7/858/htm.
- El-Sokkary R, Kishk R, El-Din SM, Nemr N, Mahrous N, Alfishawy M, et al. Antibiotic Use and Resistance Among Prescribers: Current Status of Knowledge, Attitude, and Practice in Egypt. Infect Drug Resist [Internet]. 2021 [cited 2022 Dec 7];14:1209–18. Available from: https://pubmed.ncbi.nlm.nih.gov/33790591/.
- Al-Taani GM, Al-Azzam S, Karasneh RA, Sadeq AS, Mazrouei N al, Bond SE, et al. Pharmacists’ Knowledge, Attitudes, Behaviors and Information Sources on Antibiotic Use and Resistance in Jordan. Antibiotics (Basel) [Internet]. 2022 Feb 1 [cited 2022 Dec 7];11(2). Available from: https://pubmed.ncbi.nlm.nih.gov/35203777/.
- Bjerrum A, García-Sangenís A, Modena D, Córdoba G, Bjerrum L, Chalkidou A, et al. Health alliance for prudent prescribing and yield of antibiotics in a patient-centred perspective (HAPPY PATIENT): a before-and-after intervention and implementation study protocol. BMC Primary Care [Internet]. 2022 Dec 1 [cited 2022 Dec 7];23(1):1–11. Available from: https://bmcprimcare.biomedcentral.com/articles/10.1186/s12875-022-01710-1.
- Boulkedid R, Abdoul H, Loustau M, Sibony O, Alberti C. Using and Reporting the Delphi Method for Selecting Healthcare Quality Indicators: A Systematic Review. PLoS One [Internet]. 2011 [cited 2022 Oct 25];6(6):20476. Available from: /pmc/articles/PMC3111406/.
- Trevelyan EG, Robinson N. Delphi methodology in health research: how to do it? Eur J Integr Med. 2015 Aug 1;7(4):423–8.
- Mcmillan SS, King M, Tully MP. How to use the nominal group and Delphi techniques. Int J Clin Pharm. 2016;38:655–62.
- Belton I, MacDonald A, Wright G, Hamlin I. Improving the practical application of the Delphi method in group-based judgment: A six-step prescription for a well-founded and defensible process. Technol Forecast Soc Change. 2019 Oct 1;147:72–82.
- Skulmoski GJ, Hartman FT, Krahn J. The Delphi Method for Graduate Research The Delphi Method for Graduate Research 2. Journal of Information Technology Education. 2007;6.
- Powell C. The Delphi technique: myths and realities. J Adv Nurs [Internet]. 2003 Feb 1 [cited 2022 Oct 25];41(4):376–82. Available from: https://onlinelibrary.wiley.com/doi/full/10.1046/j.1365-2648.2003.02537.x.
- Boulkedid R, Abdoul H, Loustau M, Sibony O, Alberti C. Using and Reporting the Delphi Method for Selecting Healthcare Quality Indicators: A Systematic Review. PLoS One [Internet]. 2011 [cited 2022 Nov 17];6(6):20476. Available from: /pmc/articles/PMC3111406/.
- Lange T, Kopkow C, Lützner J, Günther KP, Gravius S, Scharf HP, et al. Comparison of different rating scales for the use in Delphi studies: Different scales lead to different consensus and show different test-retest reliability. BMC Med Res Methodol [Internet]. 2020 Feb 10 [cited 2022 Nov 17];20(1):1–11. Available from: https://bmcmedresmethodol.biomedcentral.com/articles/10.1186/s12874-020-0912-8.
- Keeney S, Hasson F, Mckenna H. The Delphi Technique in Nursing and Health Research. The Delphi Technique in Nursing and Health Research [Internet]. 2010 Dec 3 [cited 2022 Nov 22]; Available from: https://onlinelibrary.wiley.com/doi/book/10.1002/9781444392029.
- Toma C, Picioreanu I. The Delphi Technique: Methodological Considerations and the Need for Reporting Guidelines in Medical Journals. Int J Public Health Res [Internet]. 2016 [cited 2022 Nov 17];4(6):47–59. Available from: http://www.openscienceonline.com/journal/ijphr.
- Md Rezal RS, Hassali MA, Alrasheedy AA, Saleem F, Md Yusof FA, Godman B. Physicians’ knowledge, perceptions and behaviour towards antibiotic prescribing: a systematic review of the literature. Expert Rev Anti Infect Ther [Internet]. 2015 May 1 [cited 2022 Dec 7];13(5):665–80. Available from: https://pubmed.ncbi.nlm.nih.gov/25813839/.
- Harris A, Chandramohan S, Awali RA, Grewal M, Tillotson G, Chopra T. Physicians’ attitude and knowledge regarding antibiotic use and resistance in ambulatory settings. Am J Infect Control. 2019 Aug 1;47(8):864–8.
- Teixeira Rodrigues A, Roque F, Falcão A, Figueiras A, Herdeiro MT. Understanding physician antibiotic prescribing behaviour: a systematic review of qualitative studies. Int J Antimicrob Agents. 2013 Mar 1;41(3):203–12.
- Dempsey PP, Businger AC, Whaley LE, Gagne JJ, Linder JA. Primary care clinicians perceptions about antibiotic prescribing for acute bronchitis: A qualitative study. BMC Fam Pract [Internet]. 2014 Dec 12 [cited 2022 Nov 28];15(1):1–10. Available from: https://bmcprimcare.biomedcentral.com/articles/10.1186/s12875-014-0194-5.
- Gourgoulis GM, Katerelos P, Maragos A, Gargalianos P, Lazanas M, Maltezou HC. Antibiotic prescription and knowledge about antibiotic costs of physicians in primary health care centers in Greece. Am J Infect Control. 2013 Dec 1;41(12):1296–7.
- Cordoba G, Siersma V, Lopez-Valcarcel B, Bjerrum L, Llor C, Aabenhus R, et al. Prescribing style and variation in antibiotic prescriptions for sore throat: cross-sectional study across six countries. BMC Fam Pract [Internet]. 2015 [cited 2022 Dec 7];16(1). Available from: https://pubmed.ncbi.nlm.nih.gov/25630870/.
- van der Velden A, Duerden MG, Bell J, Oxford JS, Altiner A, Kozlov R, et al. Prescriber and Patient Responsibilities in Treatment of Acute Respiratory Tract Infections — Essential for Conservation of Antibiotics. Antibiotics [Internet]. 2013 Jun 4 [cited 2022 Dec 7];2(2):316. Available from: /pmc/articles/PMC4790342/.
- Zalmanovici Trestioreanu A, Lador A, Sauerbrun-Cutler MT, Leibovici L. Antibiotics for asymptomatic bacteriuria. Cochrane Database Syst Rev [Internet]. 2015 Apr 8 [cited 2022 Dec 7];2015(4). Available from: /pmc/articles/PMC8407041/.
- Mcnulty CAM, Collin SM, Cooper E, Lecky DM, Butler CC. Public understanding and use of antibiotics in England: findings from a household survey in 2017. BMJ Open [Internet]. 2019 Oct 1 [cited 2022 Dec 7];9(10):e030845. Available from: https://bmjopen.bmj.com/content/9/10/e030845.
- Pavydė E, Veikutis V, Mačiulienė A, Mačiulis V, Petrikonis K, Stankevičius E. Public Knowledge, Beliefs and Behavior on Antibiotic Use and Self-Medication in Lithuania. Int J Environ Res Public Health [Internet]. 2015 Jun 17 [cited 2022 Dec 7];12(6):7002. Available from: /pmc/articles/PMC4483745/.
- Godycki-Cwirko M, Cals JWL, Francis N, Verheij T, Butler CC, Goossens H, et al. Public Beliefs on Antibiotics and Symptoms of Respiratory Tract Infections among Rural and Urban Population in Poland: A Questionnaire Study. PLoS One [Internet]. 2014 Oct 2 [cited 2022 Dec 7];9(10):e109248. Available from: https://journals.plos.org/plosone/article?id=10.1371/journal.pone.0109248.
- Cals JWL, Boumans D, Lardinois RJM, Gonzales R, Hopstaken RM, Butler CC, et al. Public beliefs on antibiotics and respiratory tract infections: an internet-based questionnaire study. The British Journal of General Practice [Internet]. 2007 Dec 12 [cited 2022 Dec 7];57(545):942. Available from: /pmc/articles/PMC2084132/.
- van Hecke O, Butler CC, Wang K, Tonkin-Crine S. Parents’ perceptions of antibiotic use and antibiotic resistance (PAUSE): a qualitative interview study. Journal of Antimicrobial Chemotherapy [Internet]. 2019 Jun 1 [cited 2022 Dec 7];74(6):1741–7. Available from: https://academic.oup.com/jac/article/74/6/1741/5382160.
- McCullough AR, Parekh S, Rathbone J, del Mar CB, Hoffmann TC. A systematic review of the public’s knowledge and beliefs about antibiotic resistance. Journal of Antimicrobial Chemotherapy [Internet]. 2016 Jan 1 [cited 2022 Dec 7];71(1):27–33. Available from: https://academic.oup.com/jac/article/71/1/27/2363966.
- Course: TARGET antibiotics toolkit hub [Internet]. [cited 2022 Dec 7]. Available from: https://elearning.rcgp.org.uk/course/view.php?id=553.
- Antibiotic awareness: posters and leaflets - GOV.UK [Internet]. [cited 2022 Dec 7]. Available from: https://www.gov.uk/government/publications/european-antibiotic-awareness-day-and-antibiotic-guardian-posters-and-leaflets.
- Print Materials | Antibiotic Use | CDC [Internet]. [cited 2022 Dec 7]. Available from: https://www.cdc.gov/antibiotic-use/print-materials.html.
- Communication toolkit to promote prudent antibiotic use aimed at primary care prescribers [Internet]. [cited 2022 Dec 7]. Available from: https://antibiotic.ecdc.europa.eu/en/toolkit-primary-care-prescribers.
Figure 1.
Flow chart of the study process.
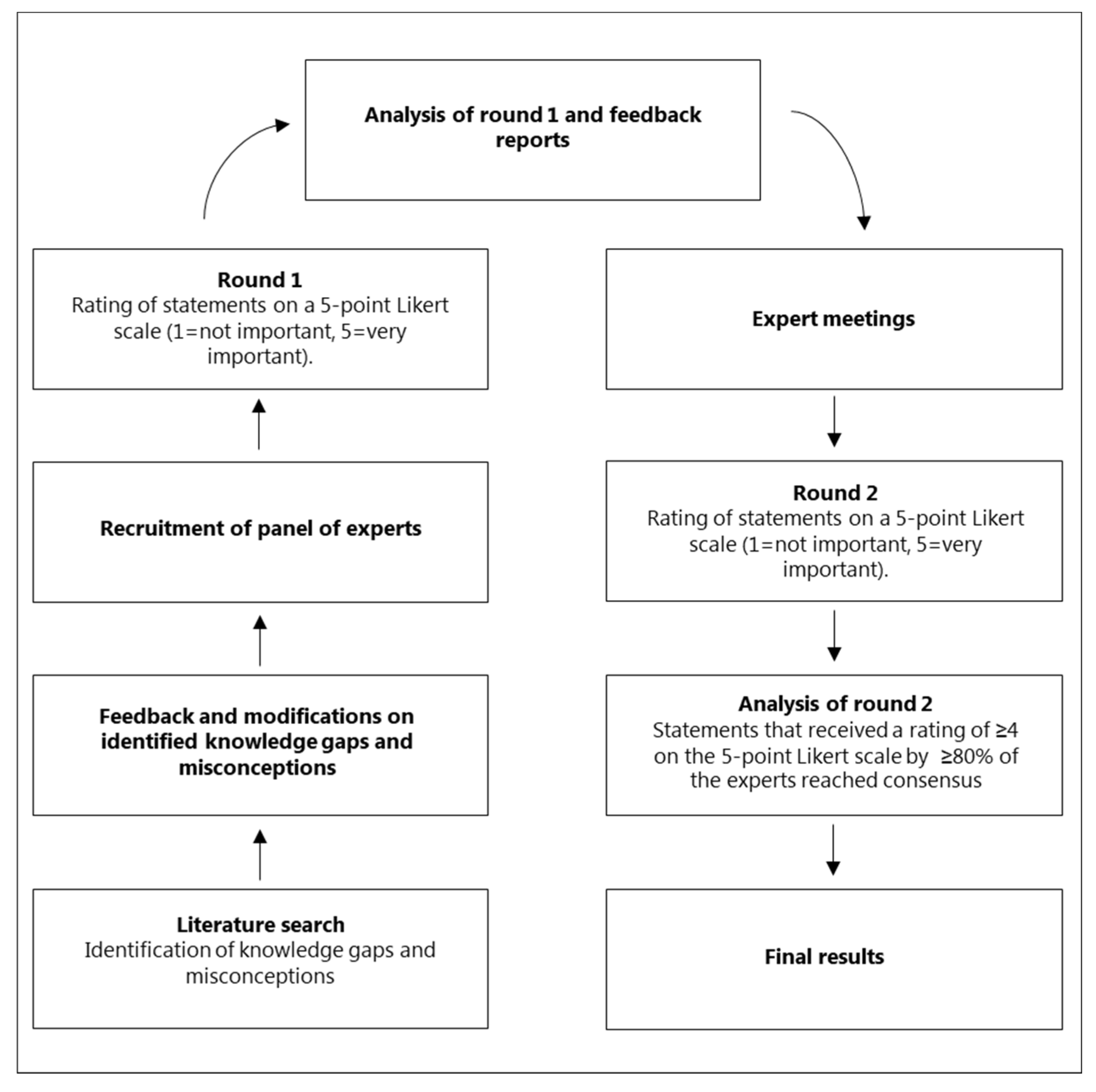

Table 1.
Overview of participants who completed both Delphi rounds.
| General practice | Out-of-hours Services | Nursing homes | Pharmacies | Total | |
|---|---|---|---|---|---|
| France | 2 | 2 | 1 | 2 | 7 |
| Greece | 2 | 1 | 0 | 1 | 4 |
| Lithuania | 3 | 3 | 2 | 3 | 11 |
| Poland | 3 | 3 | 3 | 3 | 12 |
| Spain | 3 | 3 | 2 | 3 | 11 |
| Total | 13 | 12 | 8 | 12 | 45 |
Table 2.
Statements that reached 80% consensus for the first and second round. Data are presented separately for the four settings.
Table 2.
Statements that reached 80% consensus for the first and second round. Data are presented separately for the four settings.
| General Practice | Out-of-Hours Services | Nursing Homes | Community Pharmacies | |||||
|---|---|---|---|---|---|---|---|---|
| Round 1 (N=17) | Round 2 (N=13) | Round 1 (N=16) | Round 2 (N=12) | Round 1 (N=15) | Round 2 (N=8) | Round 1 (N=18) | Round 2 (N=12) | |
| Theme 1: AMR1 (8) | 8 | 6 | 8 | 4 | 6 | 6 | 7 | 7 |
| Theme 2: Antibiotic use (9) | 7 | 4 | 8 | 6 | 5 | 5 | 8 | 9 |
| Theme 3: RTIs2 (15) |
13 | 12 | 8 | 12 | 6 | 5 | 11 | 12 |
| Theme 4: UTIs3 (12) |
11 | 12 | 2 | 8 | 1 | 8 | 5 | 8 |
| Total (44): | 39 | 34 | 26 | 30 | 18 | 24 | 31 | 36 |
1AMR: Antimicrobial resistance 2RTIs: Respiratory tract infections 3UTIs: Urinary tract infection.
Table 3.
Mean and percentage of consensus for all statements per setting divided by theme.
| No | Statements Divided by Theme | Mean | Consensus Level (%) | Mean | Consensus Level (%) | Mean | Consensus Level (%) | Mean | Consensus Level (%) | 4-Setting Consensus |
|---|---|---|---|---|---|---|---|---|---|---|
| Theme 1: Statements related to antimicrobial resistance in general | General practice | Out-of-hours services | Nursing homes | Community pharmacies | All settings | |||||
| 1 | Bacteria resistant to antibiotics are only present in hospitals* | 4.46 | 100.0 | 3.92 | 66.6 | 4.38 | 75.0 | 4.46 | 91.7 | |
| 2 | Antimicrobial resistance is not a problem in my country* | 4.46 | 84.6 | 4.46 | 91.7 | 4.46 | 87.5 | 4.46 | 91.7 | x |
| 3 | I cannot contribute to the increase of antimicrobial resistance* | 4.38 | 92.4 | 4.25 | 75.0 | 4.38 | 87.5 | 4.38 | 91.7 | |
| 4 | Others, not me, are responsible for controlling the problem of antimicrobial resistance† | 4.23 | 92.3 | 4.00 | 75.0 | 4.23 | 87.5 | 4.23 | 91.7 | |
| 5 | Antimicrobial Resistance is not a problem where I work† | 4.15 | 92.3 | 4.15 | 83.3 | 4.15 | 100.0 | 4.15 | 83.3 | x |
| 6 | Antimicrobial resistance is not an important problem because better antibiotics are continuously being discovered† | 4.08 | 84.7 | 4.08 | 91.7 | 4.08 | 100.0 | 4.08 | 91.7 | x |
| 7 | Not all antibiotics are at risk of becoming ineffective against infections by resistant bacteria* | 4.00 | 77.0 | 4.00 | 83.3 | 4.00 | 62.5 | 4.00 | 91.6 | x |
| 8 | If I am not exposed to antibiotics (e.g. directly by consuming antibiotics, or indirectly via the environment), then I cannot carry or transmit antibiotic-resistant bacteria* | 4.00 | 77.0 | 4.00 | 75.0 | 3.85 | 87.5 | 3.67 | 66.7 | |
| Theme 2: Statements about the use of antibiotics in general | General practice | Out-of-hours services | Nursing homes | Community pharmacies | All settings | |||||
| 9 | It is fine to use leftover antibiotics (or sharing antibiotics with family and friends) without consulting a healthcare professional, when experiencing similar symptoms to previous acute infections* | 4.92 | 100.0 | 4.92 | 91.6 | 4.13 | 75.0 | 4.92 | 100.0 | |
| 10 | The single presence of fever suggests high probability of bacterial infection and need of antibiotics* | 4.46 | 92.3 | 4.17 | 75.0 | 4.46 | 87.5 | 4.46 | 100.0 | |
| 11 | The benefits of prescribing antibiotics when unsure of the bacterial or viral origin of the symptoms outweigh the harms of exposure to antibiotics† | 4.46 | 84.6 | 4.46 | 100.0 | 4.46 | 100.0 | 4.46 | 100.0 | x |
| 12 | Antibiotics are effective against all type of infections* | 4.38 | 84.6 | 4.38 | 100.0 | 4.38 | 100.0 | 4.38 | 100.0 | x |
| 13 | Broad spectrum antibiotics, such as quinolones and 3rd - 5th generation cephalosporines, are the best treatment options because they cover a wide range of bacteria† | 3.85 | 69.3 | 3.85 | 91.6 | 3.85 | 87.5 | 3.85 | 83.3 | |
| 14 | Ending the consultation without an antibiotic prescription, when the patient is asking for it, indicates lack of empathy from the doctor* | 3.85 | 77.0 | 3.85 | 91.7 | 4.13 | 75.0 | 3.85 | 91.7 | |
| 15 | Ending the consultation without an antibiotic prescription indicates that the doctor is not taking my symptoms seriously enough* | 3.77 | 69.3 | 4.25 | 91.7 | 3.77 | 100.0 | 3.77 | 91.7 | |
| 16 | Ciprofloxacin, doxycycline, levofloxacin, ofloxacin, tetracycline, trimethoprim do not cause sensitivity to sunlight† | 3.23 | 53.9 | 3.67 | 66.7 | 4.00 | 75.0 | 3.23 | 83.4 | |
| 17 | A good doctor is the one that prescribes the newest type of antibiotics† | 3.15 | 53.9 | 3.83 | 75.0 | 4.13 | 75.0 | 3.15 | 91.6 | |
| Theme 3: Statements about the use of antibiotics for respiratory tract infections | General practice | Out-of-hours services | Nursing homes | Community pharmacies | All settings | |||||
| 18 | More than 2 weeks coughing suggests a high probability of bacterial infection and need of antibiotics† | 4.69 | 92.3 | 4.69 | 100.0 | 4.00 | 75.0 | 4.69 | 100.0 | |
| 19 | As soon as I feel symptoms like sore throat, running nose, fever I should seek medical care to get antibiotics* | 4.62 | 92.3 | 4.62 | 83.3 | 4.62 | 100.0 | 4.62 | 91.6 | x |
| 20 | All children with middle ear inflammation and ear pain require antibiotic therapy† | 4.54 | 92.3 | 4.54 | 91.7 | 3.50 | 50.0 | 4.54 | 100.0 | |
| 21 | The single presence of tonsillar exudate in patients with sore throat suggests a high probability of bacterial infection and need of antibiotics† | 4.46 | 92.3 | 4.46 | 91.6 | 4.00 | 75.0 | 4.46 | 83.3 | |
| 22 | In patients with sore throat and other symptoms such as tonsillar exudates, fever, tender anterior cervical adenopathy, antibiotics have a great impact in the course of symptoms by shortening the length of symptoms by more than two days† | 4.46 | 100.0 | 4.46 | 91.7 | 4.46 | 100.0 | 4.46 | 83.4 | x |
| 23 | Based on the characteristics of the cough the health care professional can differentiate the viral or bacterial origin of the cough. For example, a chesty cough (wet, productive or phlegmy) means that it is caused by a bacterium† | 4.38 | 92.3 | 4.38 | 91.7 | 3.38 | 62.5 | 4.38 | 83.4 | |
| 24 | A patient with the combination of two or more of the following symptoms : a) nasal congestion, b) nasal discharge, c) pain in the face/teeth, d) reduced sense of smell, e) fever; requires antibiotic therapy independently of the number of days with symptoms† | 4.31 | 92.3 | 4.31 | 83.3 | 3.63 | 62.5 | 4.31 | 100.0 | |
| 25 | Cough with purulent sputum (or change of color of the sputum) suggests a high probability of bacterial infection and need of antibiotics† | 4.31 | 84.6 | 4.31 | 91.6 | 4.31 | 100.0 | 4.31 | 100.0 | x |
| 26 | The single presence of tender anterior cervical adenopathy in patients with sore throat suggests a high probability of bacterial infection and need of antibiotics† | 4.23 | 84.7 | 4.00 | 75.0 | 4.23 | 87.5 | 4.17 | 75.0 | |
| 27 | Purulent nasal discharge suggests a high probability of bacterial infection and need of antibiotics† | 4.23 | 84.6 | 4.23 | 91.7 | 4.23 | 87.5 | 4.23 | 100.0 | x |
| 28 | The majority of patients with a sore throat require antibiotic treatment† | 4.15 | 84.7 | 4.15 | 83.4 | 3.63 | 62.5 | 4.15 | 91.7 | |
| 29 | A bacterial infection is the most common cause of the single or combined presentation of the following symptoms: a) nasal congestion, b) nasal discharge, c) pain in the face/teeth, d) reduced sense of smell, e) fever† | 3.92 | 84.6 | 4.17 | 75.0 | 3.88 | 75.0 | 4.50 | 83.4 | |
| 30 | The presence of cough without other symptom suggests a high probability of bacterial infection and need of antibiotics† | 4.08 | 77.0 | 4.08 | 83.3 | 3.75 | 62.5 | 4.08 | 91.7 | |
| 31 | Macrolides are the best first option for treating a bacterial lower respiratory tract infection in order to cover typical and atypical pathogens† | 3.85 | 69.3 | 3.85 | 91.6 | 4.13 | 75.0 | 3.83 | 66.7 | |
| 32 | A sinus X-Ray can help doctors to discriminate the bacterial or viral origin of the rhinosinusitis symptoms† | 3.31 | 53.9 | 3.33 | 58.3 | 3.50 | 50.0 | 3.33 | 41.6 | |
| Theme 4: Statements about the use of antibiotics for urinary tract infections | General practice | Out-of-hours services | Nursing homes | Community pharmacies | All settings | |||||
| 33 | The single presence of painful discharge of urine suggests a high probability of bacterial infection and need of antibiotics† | 4.69 | 100.0 | 4.69 | 83.3 | 4.69 | 87.5 | 4.69 | 91.6 | x |
| 34 | The single presence of frequent urination suggests a high probability of bacterial infection and need of antibiotics† | 4.54 | 100.0 | 4.54 | 91.7 | 4.00 | 75.0 | 4.54 | 100.0 | |
| 35 | The single presence of burning sensation during urination suggests a high probability of bacterial infection and need of antibiotics† | 4.54 | 100.0 | 4.54 | 91.7 | 3.88 | 75.0 | 4.54 | 100.0 | |
| 36 | The single presence of blood in urine suggests a high probability of bacterial infection and need of antibiotics† | 4.46 | 92.3 | 4.46 | 83.3 | 4.46 | 87.5 | 4.46 | 100.0 | x |
| 37 | When a patient comes with acute UTI symptoms it is okay to prescribe antibiotics, despite of the negative result of a dipstick test [nitrites (-), leucocytes (-)]. A negative dipstick test is not a good predictor of absence of UTI† | 4.46 | 100.0 | 4.46 | 100.0 | 4.46 | 87.5 | 3.17 | 25.0 | |
| 38 | Leucocytes positive and nitrite negative result in a dipstick test indicates with high certainty bacterial infection and need of antibiotics† | 4.31 | 92.3 | 4.00 | 75.0 | 4.31 | 87.5 | 3.58 | 41.7 | |
| 39 | The single presence of smelly urine suggests a high probability of bacterial infection and need of antibiotics† | 4.31 | 84.7 | 3.92 | 75.0 | 4.00 | 75.0 | 4.31 | 83.4 | |
| 40 | The single presence of cloudy urine suggests a high probability of bacterial infection and need of antibiotics† | 4.31 | 84.7 | 3.75 | 66.7 | 4.31 | 87.5 | 4.31 | 83.4 | |
| 41 | A positive dipstick in the elderly without urinary tract symptoms is a strong indicator for urinary tract infection and requires antibiotics† | 4.31 | 92.3 | 4.31 | 83.4 | 4.31 | 100.0 | 3.67 | 50.0 | |
| 42 | The single presence of persistent urge to urinate suggests a high probability of bacterial infection and need of antibiotics† | 4.23 | 84.7 | 4.23 | 83.3 | 3.75 | 75.0 | 4.23 | 100.0 | |
| 43 | In an uncomplicated UTI, antibiotic treatment should be started as soon as possible to prevent the dissemination of the infection to the kidneys and bloodstream, independently of the risk of complication† | 4.23 | 84.7 | 4.23 | 83.3 | 4.23 | 87.5 | 4.23 | 91.7 | x |
| 44 | Cognitive changes (e.g. agitation, confusion) in the elderly suggest a high probability of bacterial infection and the need of antibiotics, even without the presence of urinary tract symptoms† | 4.00 | 84.7 | 4.08 | 75.0 | 4.00 | 87.5 | 3.75 | 58.3 | |
Notes: The statements from the point of view of the healthcare professional and the patient are marked differently in the table (* From the point of view of the patient, † from the point of view of the healthcare professional). Statements have reached consensus where the consensus level is ≥ 80%.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



