
Submitted:
17 July 2023
Posted:
19 July 2023
You are already at the latest version
Preprints on COVID-19 and SARS-CoV-2
Abstract
Background: We studied the outcomes of SARS-CoV-2 (COVID) hospitalizations and their association with myocardial injury and thrombosis. Methods: Retrospective analysis of the National Inpatient Sample 2020 database. Results: We identified 335,799 hospitalizations with COVID. Of these, 1.6% (5,355) were diagnosed with non-ST-segment myocardial infarction (COVNSTEMI). The mean age of COVID hospitalizations was 71.7, with 60.50% being males. The population prevalence included 53.10% Whites, 17.80% Blacks, 19.20% Hispanics, and 4.10% Asians. The average length of stay (LOS) was 10 days, and 37.60% of patients died during their hospitalization. The average cost of hospitalization (TOTCHG) was $156,633. The COVSTEMI group comprised 1,364 cases, with a mean age of 67.4, in-hospital mortality of 47.4%, and the mean TOTCHG was $177,600. The DVTCOV group comprised 2,869 cases, while the PECOV group had 4,828 cases. Male predominance was observed in both groups, with mean ages of 66 years in the DVTCOV group and 64 years in the PECOV group. The DVTCOV group had a LOS of 16 days, with 24.71% mortality, while the PECOV group had a LOS of 11 days, with 19.20% mortality. The average TOTCHG in the DVTCOV group was $248,900, whereas it was $145,378 in the PECOV group. Conclusion: Our study revealed significant mortality rates across different groups, including 38% in COVNSTEMI, 47% in COVSTEMI, 25% in DVTCOV, and 19% in PECOV. These findings highlight the severity of COVID-related complications and the substantial financial burden of hospitalization.
Keywords:
SARS‐CoV‐2
; COVID‐19
; Pulmonary embolism
; PE
; deep venous thrombosis
; DVT
; hospitalization
Introduction
Coronavirus originates from the Latin word ‘corona,’ meaning ‘crown’. It causes various respiratory illnesses varying from mild cold to severe respiratory distress syndrome. The novel coronavirus disease, also called severe acute respiratory syndrome (SARS)-CoV-2 and coronavirus disease 2019 (COVID-19), has become a global disease burden [1]. First discovered in Wuhan city of China, towards the end of December 2019 and was declared a global pandemic by the WHO in March 2020. There have been about 6,831,681 deaths worldwide and 110,364 deaths in the United States [2,3].
COVID-19 primarily affects the respiratory system, followed by the cardiovascular, hepatic, renal, gastrointestinal, and central nervous systems [4]. Symptoms, including breathlessness and respiratory failure, are the common clinical features seen [4]. According to previous reports, among all hospitalized patients with COVID-19, approximately 14–30% developed acute respiratory distress syndrome, with an associated mortality rate of 45–75% [5].
The COVID-19 has several important cardiovascular sequelae [6,7,8]. Patients with prior cardiovascular disease are at higher risk for adverse events from COVID-19, while individuals without a history of cardiovascular disease are at risk for new-onset cardiovascular complications [8].
Thrombotic complications in patients diagnosed with COVID-19 have become major cardiovascular complications, leading to worsened outcomes [9,10]. Pulmonary embolism (PE), deep vein thrombosis, ischemic stroke, and myocardial infarction are examples of complications that have been described in patients associated with COVID-19 infections [9,11].
The mechanisms by which COVID-19 causes these thrombotic complications are not fully understood. Data on the prevalence and predictors of various cardiovascular complications (e.g., MI, stroke, or acute limb ischemia) remain limited [9,10]. Research postulates include possible excessive inflammation, hypoxia, immobilization, and diffuse intravascular coagulation in the setting of COVID-19 infection as contributors to a hypercoagulable and prothrombotic state [12,13].
There need to be more studies detailing the outcome pattern of patients hospitalized with Covid 19. This study aims to describe the outcomes of covid 19 infections among hospitalized patients with a history of pulmonary embolism and deep venous thrombosis.
Methods and Results
Database
We retrospectively analyzed the Nationwide Inpatient Sample (NIS) database of 2020. We objectively selected our sample using the International Classification of Disease Tenth Edition (ICD-10) code. The NIS is a publicly available deidentified database that contains over 90% of hospitalizations within the United States. It includes 48 states' hospitalization records, including Maryland. It records 20% of all hospital admissions weighted to reflect the real-world population. Since the NIS is deidentified and publicly available, it does not require Institutional Review Board (IRB) approval.
Population of Interest
We identified hospitalization with a diagnosis of COVID-19. Using the ICD-10 code U071. Within this population, we looked for hospitalizations diagnosed with lower extremity deep venous thrombosis (DVTCOV) and pulmonary embolism (PECOV). Our outcomes of interest were the length of hospitalization (LOS), the average cost of hospitalization, and in-hospital mortality. We excluded the non-covid population from this study.
Analysis
Data from 2020 was implored for the analyses. We preferred the 2020 dataset because it captured the diagnosis of the novel COVID-19 more succinctly than the 2019 dataset. The 2020 NIS database was pooled from 48 states, including Maryland, representing 97% of the United States population, making the NIS the largest inpatient database. We applied a descriptive statistical method for demographics and baseline characteristics of patients, which are presented as percentages. We reported prevalence in percentages, LOS, and TOTCH in means.
Variables and Significance
We included demographic and socioeconomic factors, such as age, sex, and ethnicity. Results with p values of <0.05 were adopted as statistically significant. All analyses were performed using Statistical Analysis System (SAS) software version 9.4 (SAS Institute Inc., Cary, NC).
Results
We identified 335,799 hospitalizations with COVID-19, of which 5850 (1.74%) and 9381 (2.79%) had a concurrent diagnosis of lower limb deep venous thrombosis (LDVT) and pulmonary embolism (PE) respectively, (p<0.0001).
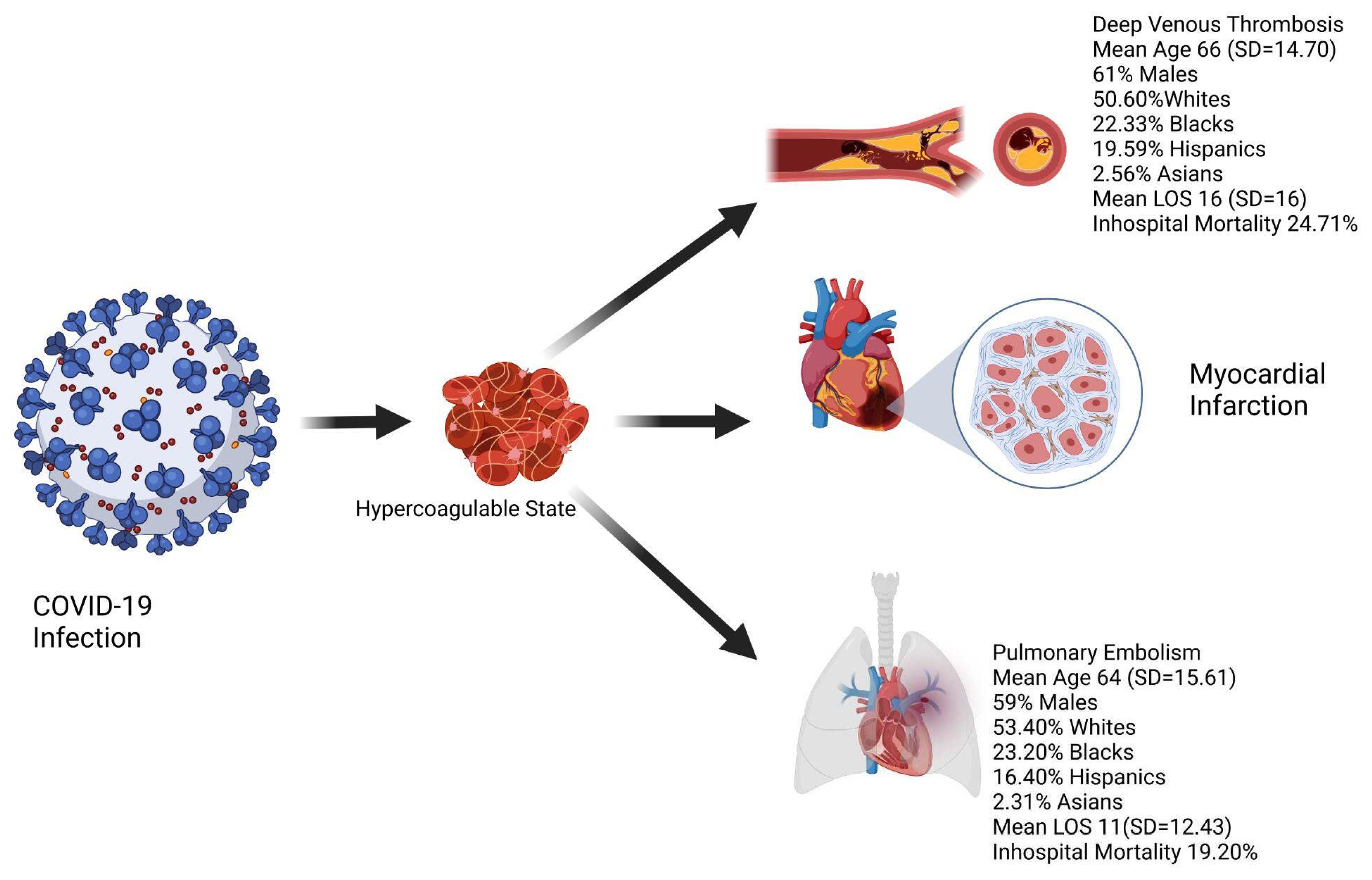
In the DVTCOV group, there were 2,869 (50.60%) Whites, 1,266 (22.33%) Blacks, 1,111 (19.59%) Hispanics, and 145 (2.56%) Asians (p<0.0001). While in the PECOV group, the Whites were 4828 (53.40%), 2,098 (23.20%) Blacks, 1,482 (16.40%) Hispanics, and 209 (2.31%) Asians (p<0.0001).
There was a male predominance in both groups. The DVTCOV group had 61% males (See Figure 1 below), and the PECOV group had 59% males (p<0.0001). The mean age was 66 years (SD=14.7) in the DVTCOV group and 64 years (SD=15.6) in the PECOV group. Figure 1 depicts our findings.
Regarding LOS and in-hospital mortality, the DVTCOV group had a mean LOS of 16 days (SD=16) and 1445 (24.71%) deaths (p<0.0001). The PECOV group had a mean LOS of 11 days (SD= 12.4) and 1799 (19.20%) deaths (p<0.0001). The average hospital charge in the DVTCOV group was $248,900 (SD= 399,860), while in the PECOV group, it was $145,378 (SD=289608) (p<0.0001). There were 5355 COVID-19 hospitalizations diagnosed with NSTEMI (COVNSTEMI), with a mean age of 71.7 (SD=13.3) and 60.50% were males, and population prevalence was 53.10% Whites, 17.80% Blacks, 19.20% Hispanics, and 4.10% Asians (p<0.0001). LOS 10 (SD=12.4), 2,012 (37.60%) died during their hospitalization (p<0.0001). TOTCHG $156,633 (SD=245,450) (p<0.0001). The COVSTEMI group had 1364 cases, 52.91% Whites, 15.37% Blacks, mean age 67.4 (SD=13.7), 66.7% males, and an in-hospital mortality of 47.4% (646) (p<0.0001). The mean TOTCHG $177600 (SD=266142)
Discussion
This study revealed that PE and DVT are part of the spectrum of clinical manifestations of hospitalized COVID-19 patients. A high rate of thrombotic events has been reported in hospitalized COVID-19 patients [14]. Microvascular abnormalities in COVID-19 include endothelial inflammation, disruption of intercellular junctions, and microthrombi formation [15]. Studies have revealed a distinct COVID-19-associated coagulopathy, increased cytokines, and activation of platelets, endothelium, and complement in COVID-19. This proinflammatory condition results in immunothrombosis, as the host defense mechanism becomes dysregulated, leading to the excessive formation of immunologically mediated thrombi [15].
We discovered that 3% of patients hospitalized for COVID-19 had PE, while 2% had lower limb deep venous thrombosis (LDVT). These findings of concurrent PE and DVT in hospitalized COVID-19 patients were lower compared to other studies. Erben et al. reported an incidence of 9% of hospitalized patients having DVT/PE [16], Ameri et al. found a PE rate of 7.5% in hospitalized COVID-19 patients [17], Fauvel et al. reported a PE rate of 8.3% [18]. However, Poissy et al. reported 20.6% of PE in hospitalized COVID-19 patients [19], Badr et al. noted an incidence of 32% of hospitalized COVID-19 with PE [20], Miró et al. identified 4.92% of hospitalized COVID-19 patients having PE [21], while Benito et al., reported a PE incidence rate of 2.6% [22].
Baccellieri et al. reported 14.5% of hospitalized COVID-19 patients with lower limb DVT (DVTCOV) [14], and Franco-Moreno et al. noted an incidence of 7.7% of DVTCOV [23]. These varied incidences of DVTCOV and PECOV from multiple studies may result from the severity of the disease condition, coexisting morbidity, the age of patients, and the institution of thromboprophylaxis. Although several studies have reported a high incidence of PE in hospitalized COVID-19 patients [17,18,19,20], surprisingly, our findings revealed a low incidence of PE in hospitalized COVID-19. This may be due to the prompt initiation of thromboprophylaxis and the extent of severity of COVID-19 in patients. Studies have reported that DVTCOV mainly occurs in the infrapopliteal vein [24,25]. Cai et al. suggested that DVTCOV is associated with an increased risk of bilateral-sided DVT, especially in younger patients [24]. The study timing also has an impact on the incidence. The studies conducted before the widespread use of the COVID-19 vaccine may differ tremendously from studies after its implementation. This is supported by various data that suggest that the severity of COVID-19 infection is remarkably less in the vaccinated population [CDC].
Findings from our study revealed the mean age of patients in the DVTCOV group was 66 years, while that of the PECOV group was 64 years. This is consistent with other studies, which showed the mean age of hospitalized COVID-19 patients with DVT and/or PE was around 60 years [14,15,22]. Our findings were also consistent with those of Xu et al., which showed the mean age was 62 years for PECOV patients [26]. This may be due to other risk factors associated with this age group, including hypertension, diabetes mellitus, heart failure, smoking, obesity, dyslipidemia, malignancy, and chronic kidney disease (CKD), which are involved in ongoing inflammatory states. We discovered 50.60% of patients with lower limb DVT were whites, and 61% of patients in the DVTCOV group were males, while in the PECOV group, 53.40% were whites and 59% were male. This observation is lower when compared to other studies. Baccellieri et al. showed that 90% of hospitalized COVID-19 patients with DVT were Caucasians, while 76% of DVTCOV patients were males [14]. Ameri et al. showed that 78.8% of PECOV patients were males [17], collaborating with the Badr et al. study, which showed 78.4% of PECOV patients were males [20]. Similarly, Xu et al. also noted 73% of males in the PECOV group, but in contrast to our findings, whites made up 28% while blacks were 33% [26]. It has been shown that male gender is a non-modifiable risk factor for PE, especially in COVID-19 [18].
This study showed that the average length of stay was 16 days for hospitalized COVID-19 patients with DVT, while that for PE was 11 days. Studies have revealed that hospitalized COVID-19 with PE may require ICU care and invasive mechanical ventilation [22], which could account for the increased length of stay in the hospital. Baccellieri et al. showed that the median hospital stay for hospitalized COVID-19 patients with DVT was 24 days [14]. In comparison, Xu et al. showed a mean length of stay of 13 days for hospitalized COVID-19 patients with PE [26], consistent with our findings for the PECOV group. Our study revealed that patients in the DVTCOV group had an increased length of hospitalization than those in the PECOV group. This may result from the sequelae that could arise in the DVTCOV group, with an increased risk of PE and the need to continuously evaluate patients using anticoagulants and regular deep vein imaging to determine its progression or resolution.
Regarding in-hospital mortality, our findings revealed that the DVTCOV group had 25% mortality while the PECOV group had 19%. Baccellieri et al. noted a mortality rate of 17% in hospitalized COVID-19 patients with DVT [14], while Pereira de Godoy et al. identified a mortality of 67% in hospitalized COVID-19 patients with DVT [27]. Fu et al. revealed in a meta-analysis that the mortality rate of COVID-19 patients with PE had significant mortality 21.9% compared to non-PE patients [28], Badr et al. revealed a mortality of 25.5% in PECOV patients [20], while Xu et al. noted a mortality rate of 20% in PECOV patients [26]. These high mortality rates in both the DVTCOV and PECOV groups may be synergistically related to other complications of COVID-19, which include myocarditis, shock, ARDS, arrhythmias, multiorgan dysfunction, etc., in conjunction with debilitating risk factors for comorbidities, immobility, older age, and ongoing systemic inflammation.
Our study showed the average hospital charge for the DVTCOV group to be $248,900, while that of the PECOV group was $145378. In comparison with patients with COVID-19 without DVT and PE, Ohsfeldt et al. showed the median cost for hospitalized COVID-19 patients to be $11,267 the cost per day was $1772. It gave an insight into the ICU cost of COVID-19 patients, with a median cost of $13,443, and the cost per day was $2902. However, patients requiring mechanical ventilation had hospital and ICU costs of $47,454 and $41,510 [29]. These findings reveal the enormous financial burden on patients in the DVTCOV and PECOV groups regarding hospital charges. The reasons for such costs could be due to various interventions undertaken during hospitalization, including invasive mechanical ventilators or extracorporeal membrane oxygenation (ECMO), length of hospital stay, ICU care, and presence of comorbidities.
Studies have shown that COVID-19 infection is involved in developing acute myocardial complications, including different forms of myocardial injury, such as myocardial infarction, myocarditis, and stress cardiomyopathy [30,31]. The suggested mechanisms include microvascular dysfunction, myocardial injury from hemodynamic instability or hypoxemia, thrombosis with coronary artery plaque destabilization due to inflammatory hypercoagulability, inflammatory myocarditis, and stress cardiomyopathy [32,33,34].
This study revealed 1.6% of COVNSTEMI patients' were hospitalized, while that of COVSTEMI was 0.4%. Our findings showed a smaller incidence of COVNSTEMI hospitalization compared to Majeed et al., which reported a 4.6% COVNSTEMI hospitalization [35]. In comparison, Case et al. showed an incidence of 5% COVNSTEMI hospitalization [36]. In the same vein, Rodriguez-Leor et al. observed an incidence of 9.0% of hospitalized COVSTEMI patients from all consecutive hospitalized STEMI patients [37]. In comparison, Choudry et al. reported an incidence of 33.9% of COVSTEMI patients from all consecutive hospitalized STEMI patients [38]. However, Saad et al. revealed an incidence of 0.7% COVSTEMI hospitalization in a multicenter study of out-of-hospital STEMI cases [39]; similarly, Case et al. noted an incidence of 0.7% COVSTEMI hospitalization [36]. We observed the mean age of COVNSTEMI hospitalization was 71.7 years, consistent with other studies showing that COVNSTEMI mainly occurred in older patients [35,40]; however, the mean age of COVSTEMI was 67.4 years. These findings may be due to the prevalence of other cardiovascular risk factors (hypertension, hyperlipidemia, and smoking) that are predominant in this age group, with concurrent inflammatory comorbidities, including diabetes mellitus and chronic kidney disease. Moreover, the older age group has been known to be more susceptible to cardiovascular complications of COVID-19 [41], with this viral disease associated with endothelial dysfunction, extensive systemic inflammation, and cytokine storm, serving as an important risk factor for plaque rupture and thrombus formation [42,43].
Our study showed racial disparities in the incidence of COVNSTEMI and COVSTEMI hospitalizations, with whites accounting for 53% in both hospitalizations while blacks were 18% and 15%, respectively. This is consistent with Majeed et al., as they reported 51% of Caucasians with COVNSTEMI, with that of blacks being 18% [35]. Interestingly, Case et al. observed that black patients with acute myocardial infarction were more likely to be COVID-19 positive than whites [36]. Studies have reported that the African American population was the most hit during the COVID-19 pandemic [44,45].
The in-hospital mortality for the COVNSTEMI group was 37.60% compared with that of 47.4% in the COVSTEMI group. Majeed et al. discovered the mortality rate for the COVNSTEMI group was 37.30% [35], consistent with our findings. In comparison, Saad et al. revealed the rate of in-hospital mortality in the COVSTEMI group to be 78.5% [39], Bangalore et al. reported a mortality rate of 72% [46]; however, Hamadeh et al. reported a mortality of 12% [47,48,49]. It is known that patients having acute myocardial infarction with concomitant COVID-19 have a significantly increased risk of mortality compared to those without COVID-19 [36]. Multiple factors have been shown to be associated with this finding; they include the presence of high levels of inflammatory markers, older age, underlying comorbidities, need for ICU admission and mechanical ventilation, and some of these patients have coronary angiography and subsequent revascularization deferred due to their sicker clinical state [36].
The mean treatment cost for the COVNSTEMI group and that of the COVSTEMI group were $156,633 and $177600, respectively. Majeed et al. reported that COVNSTEMI patients' mean hospitalization cost was $149,121 [35]. These findings could be due to invasive cardiac interventions undertaken, including ICU admission and mechanical ventilation, length of hospitalization, treatment of comorbidities, and other complications.
Limitations of the Study
The NIS database is helpful for research purposes. However, its design is an administrative tool for billing purposes and relies on the coders' accuracy, hence the possibility of overbilling, underbilling, and wrong coding. Some missing frequencies may impact analysis (although less likely) during the analyses. The NIS cannot differentiate between multiple hospitalizations for a single patient, hence can result in duplication. The NIS dataset cannot differentiate between hospitalizations vaccinated or not vaccinated against the COVID-19 virus. This made it impossible to estimate the prevalence of DVT and PE in these subgroups.
Conclusion
Based on our analysis of the Nationwide Inpatient Sample (NIS) 2020 database, our findings indicate that there is a significant association between COVID-19 hospitalizations and deep venous thrombosis (DVT) and pulmonary embolism (PE). Moreover, we observed a male predominance in both DVT and PE groups. Our analysis revealed that the mean LOS was more days in the DVT group. than the PE group. Furthermore, the in-hospital mortality rate was higher in the DVT group than in the PE group. We also found that the average hospital charge was higher in the DVT group than in the PE group.
These findings underscore the need for close monitoring of COVID-19 patients for thrombotic complications, especially those with a higher risk of DVT and PE, including males and older adults. Our results also highlight the substantial financial burden associated with hospitalization for DVT and PE in COVID-19 patients. Therefore, preventive measures and early management of thrombotic complications may improve patient outcomes and reduce the overall healthcare cost associated with COVID-19 hospitalizations.
Author contribution
All authors played several overlapping contributory roles such as: Conceptualization, design, cross referencing, and fact checking, Formal Analysis and interpretation of data, project administration, curation, visualization, writing – original draft, writing – review & editing, Supervision, oversight, and leadership, correspondence, data curation, quality control, internal review, communications, data collection and archiving, software, literature search, validation and approval.
Source(s) of fund support
The research did not receive any specific funding from any source.
Disclaimers
This article has not been submitted to other publications and/or presented at a conference or meeting.
Regulatory Approval or Research Subject Protection Requirements
This manuscript does not require regulatory approval.
Ethical approval
This Paper does not require ethical approval.
Data Availability
The data used in this study was from a publicly available data (NIS)
Conflict of interest
All authors declare that they have no conflicts of interest.
References
- Umakanthan S, Sahu P, Ranade A, v., et al., Origin, transmission, diagnosis, and management of coronavirus disease 2019 (COVID-19). Postgrad Med J. 2020;96(1142):753-758. [CrossRef]
- Weekly Review. https://covid.cdc.gov/covid-data-tracker.
- Global Situation Situation in REGION Russian Federation. https://covid19.who.int.
- Miller IF, Becker AD, Grenfell BT, Metcalf CJE. Disease and healthcare burden of COVID-19 in the United States. Nat Med. 2020;26(8):1212-1217. [CrossRef]
- Potere N, Valeriani E, Candeloro M, et al., Acute complications and mortality in hospitalized patients with coronavirus disease 2019: A systematic review and meta-analysis. Crit Care. 2020;24(1). [CrossRef]
- Driggin E, Madhavan M v., Bikdeli B, et al. Cardiovascular Considerations for Patients, Health Care Workers, and Health Systems During the COVID-19 Pandemic. J Am Coll Cardiol. 2020;75(18):2352-2371. [CrossRef]
- Clerkin KJ, Fried JA, Raikhelkar J, et al. COVID-19 and Cardiovascular Disease. Circulation. 2020;141(20):1648-1655. [CrossRef]
- Madjid M, Safavi-Naeini P, Solomon SD, Vardeny O. Potential Effects of Coronaviruses on the Cardiovascular System: A Review. JAMA Cardiol. 2020;5(7):831-840. [CrossRef]
- Klok FA, Kruip MJHA, van der Meer NJM, et al. Incidence of thrombotic complications in critically ill ICU patients with COVID-19. Thromb Res. 2020;191:145-147. [CrossRef]
- Bikdeli B, Madhavan M, v. Jimenez D, et al., COVID-19, and Thrombotic or Thromboembolic Disease: Implications for Prevention, Antithrombotic Therapy, and Follow-Up: JACC State-of-the-Art Review. J Am Coll Cardiol. 2020;75(23):2950-2973. [CrossRef]
- Bikdeli B, Madhavan M, v. Jimenez D, et al., COVID-19, and Thrombotic or Thromboembolic Disease: Implications for Prevention, Antithrombotic Therapy, and Follow-Up: JACC State-of-the-Art Review. J Am Coll Cardiol. 2020;75(23):2950-2973. [CrossRef]
- Goeijenbier M, van Wissen M, van de Weg C et al. Review: Viral infections and mechanisms of thrombosis and bleeding. J Med Virol. 2012;84(10):1680-1696. [CrossRef]
- Klok FA, Kruip MJHA, van der Meer NJM, et al. Incidence of thrombotic complications in critically ill ICU patients with COVID-19. Thromb Res. 2020;191:145-147. [CrossRef]
- Baccellieri, D., Bertoglio, L., Apruzzi, L., Ardita, V., D'Angelo, A., Bossi, M., Rinaldi, E., Bilman, V., Calvisi, S., Castagna, A., Galli, L., Landoni, G., Melissano, G., Querini, P. R., Tresoldi, M., De Cobelli, F., Zangrillo, A., Ciceri, F., & Chiesa, R. (2021). Incidence of deep venous thrombosis in COVID-19 hospitalized patients during the first peak of the Italian outbreak. Phlebology, 36(5), 375–383. [CrossRef]
- Loo, J., Spittle, D. A., & Newnham, M. (2021). COVID-19 immunothrombosis and venous thromboembolism: biological mechanisms. Thorax, 76(4), 412–420. [CrossRef]
- Erben, Y., Franco-Mesa, C., Gloviczki, P., Stone, W., Quinones-Hinojoas, A., Meltzer, A. J., Lin, M., Greenway, M. R. F., Hamid, O., Devcic, Z., Toskich, B., Ritchie, C., Lamb, C. J., De Martino, R. R., Siegel, J., Farres, H., Hakaim, A. G., Sanghavi, D. K., Li, Y., Rivera, C., … Meschia, J. F. (2021). Deep vein thrombosis and pulmonary embolism among hospitalized coronavirus disease 2019-positive patients predicted for higher mortality and prolonged intensive care unit and hospital stay in a multisite healthcare system. Journal of Vascular Surgery. Venous and lymphatic disorders, 9(6), 1361–1370.e1. [CrossRef]
- Ameri, P., Inciardi, R. M., Di Pasquale, M., Agostoni, P., Bellasi, A., Camporotondo, R., Canale, C., Carubelli, V., Carugo, S., Catagnano, F., Danzi, G., Dalla Vecchia, L., Giovinazzo, S., Gnecchi, M., Guazzi, M., Iorio, A., La Rovere, M. T., Leonardi, S., Maccagni, G., Mapelli, M., … Metra, M. (2021). Pulmonary embolism in patients with COVID-19: characteristics and outcomes in the Cardio-COVID Italy multicenter study. Clinical research in cardiology : official journal of the German Cardiac Society, 110(7), 1020–1028. [CrossRef]
- Fauvel, C., Weizman, O., Trimaille, A., Mika, D., Pommier, T., Pace, N., Douair, A., Barbin, E., Fraix, A., Bouchot, O., Benmansour, O., Godeau, G., Mecheri, Y., Lebourdon, R., Yvorel, C., Massin, M., Leblon, T., Chabbi, C., Cugney, E., Benabou, L., … Critical Covid-19 France Investigators (2020). Pulmonary embolism in COVID-19 patients: a French multicentre cohort study. European heart journal, 41(32), 3058–3068. [CrossRef]
- Poissy, J., Goutay, J., Caplan, M., Parmentier, E., Duburcq, T., Lassalle, F., Jeanpierre, E., Rauch, A., Labreuche, J., Susen, S., & Lille ICU Haemostasis COVID-19 Group (2020). Pulmonary Embolism in Patients With COVID-19: Awareness of an Increased Prevalence. Circulation, 142(2), 184–186. [CrossRef]
- Badr, O. I., Alwafi, H., Elrefaey, W. A., Naser, A. Y., Shabrawishi, M., Alsairafi, Z., & Alsaleh, F. M. (2021). Incidence and Outcomes of Pulmonary Embolism among Hospitalized COVID-19 Patients. International journal of environmental research and public health, 18(14), 7645. [CrossRef]
- Miró, Ò., Jiménez, S., Mebazaa, A., Freund, Y., Burillo-Putze, G., Martín, A., Martín-Sánchez, F. J., García-Lamberechts, E. J., Alquézar-Arbé, A., Jacob, J., Llorens, P., Piñera, P., Gil, V., Guardiola, J., Cardozo, C., Mòdol Deltell, J. M., Tost, J., Aguirre Tejedo, A., Palau-Vendrell, A., LLauger García, L., … Spanish Investigators on Emergency Situations TeAm (SIESTA) network (2021). Pulmonary embolism in patients with COVID-19: incidence, risk factors, clinical characteristics, and outcome. European heart journal, 42(33), 3127–3142. [CrossRef]
- Benito, N., Filella, D., Mateo, J., Fortuna, A. M., Gutierrez-Alliende, J. E., Hernandez, N., Gimenez, A. M., Pomar, V., Castellvi, I., Corominas, H., Casademont, J., & Domingo, P. (2020). Pulmonary Thrombosis or Embolism in a Large Cohort of Hospitalized Patients With Covid-19. Frontiers in medicine, 7, 557. [CrossRef]
- Franco-Moreno, A., Herrera-Morueco, M., Mestre-Gómez, B., Muñoz-Rivas, N., Abad-Motos, A., Salazar-Chiriboga, D., Duffort-Falcó, M., Medrano-Izquierdo, P., Bustamante-Fermosel, A., Pardo-Guimera, V., Ulla-Anés, M., Torres-Macho, J., & Infanta Leonor Thrombosis Research Group (2021). Incidence of Deep Venous Thrombosis in Patients With COVID-19 and Pulmonary Embolism: Compression Ultrasound COVID Study. Journal of ultrasound in medicine : official journal of the American Institute of Ultrasound in Medicine, 40(7), 1411–1416. [CrossRef]
- Cai, C., Guo, Y., You, Y., Hu, K., Cai, F., Xie, M., Yang, L., Ling, K., Ye, D., Misra, S., Wang, W., & Li, Y. (2020). Deep Venous Thrombosis in COVID-19 Patients: A Cohort Analysis. Clinical and applied thrombosis/hemostasis : official journal of the International Academy of Clinical and Applied Thrombosis/Hemostasis, 26, 1076029620982669. [CrossRef]
- Yu, Y., Tu, J., Lei, B., Shu, H., Zou, X., Li, R., Huang, C., Qu, Y., & Shang, Y. (2020). Incidence and Risk Factors of Deep Vein Thrombosis in Hospitalized COVID-19 Patients. Clinical and applied thrombosis/hemostasis : official journal of the International Academy of Clinical and Applied Thrombosis/Hemostasis, 26, 1076029620953217. [CrossRef]
- Xu, H., Martin, A., Singh, A., Narasimhan, M., Lau, J., Weinberg, M., Jauhar, R., & Rao, G. (2020). Pulmonary Embolism in Patients Hospitalized With COVID-19 (From a New York Health System). The American journal of cardiology, 133, 148–153. [CrossRef]
- Pereira de Godoy, J. M., Russeff, G. J. D. S., Costa, C. H., Sato, D. Y., Silva, D. F. D. F., Guerreiro Godoy, M. F., Pereira de Godoy, H. J., & Espada, P. C. (2021). Mortality of Patients Infected by COVID-19 with and without Deep-Vein Thrombosis. Medicines (Basel, Switzerland), 8(12), 75. [CrossRef]
- Fu, Z., Bai, G., Song, B., Wang, Y., Song, H., Ma, M., Zhu, J., Zhang, Z., & Kang, Q. (2022). Risk factors and mortality of pulmonary embolism in COVID-19 patients: Evidence based on fifty observational studies. Medicine, 101(45), e29895. [CrossRef]
- Ohsfeldt, R. L., Choong, C. K., Mc Collam, P. L., Abedtash, H., Kelton, K. A., & Burge, R. (2021). Inpatient Hospital Costs for COVID-19 Patients in the United States. Advances in therapy, 38(11), 5557–5595. [CrossRef]
- Madjid, M., Safavi-Naeini, P., Solomon, S. D., & Vardeny, O. (2020). Potential Effects of Coronaviruses on the Cardiovascular System: A Review. JAMA cardiology, 5(7), 831–840. [CrossRef]
- Giustino, G., Croft, L. B., Oates, C. P., Rahman, K., Lerakis, S., Reddy, V. Y., & Goldman, M. (2020). Takotsubo Cardiomyopathy in COVID-19. Journal of the American College of Cardiology, 76(5), 628–629. [CrossRef]
- Das, M., Bristow, M. R., & Chung, M. K. (2021). The Essential Vulnerability of Human Cardiac Myocytes to SARS-CoV-2. JACC. Basic to translational science, 6(4), 346–349. [CrossRef]
- Libby, P., Loscalzo, J., Ridker, P. M., Farkouh, M. E., Hsue, P. Y., Fuster, V., Hasan, A. A., & Amar, S. (2018). Inflammation, Immunity, and Infection in Atherothrombosis: JACC Review Topic of the Week. Journal of the American College of Cardiology, 72(17), 2071–2081. [CrossRef]
- Tersalvi, G., Vicenzi, M., Calabretta, D., Biasco, L., Pedrazzini, G., & Winterton, D. (2020). Elevated Troponin in Patients With Coronavirus Disease 2019: Possible Mechanisms. Journal of cardiac failure, 26(6), 470–475. [CrossRef]
- Majeed, H., Gangu, K., Sagheer, S., Garg, I., Khan, U., Shuja, H., Bobba, A., Chourasia, P., Shekhar, R., Avula, S. R., & Sheikh, A. B. (2022). COVID-19 and NSTEMI Outcomes among Hospitalized Patients in the United States and Racial Disparities in Mortality: Insight from National Inpatient Sample Database. Vaccines, 10(12), 2024. [CrossRef]
- Case, B. C., Yerasi, C., Forrestal, B. J., Shea, C., Rappaport, H., Medranda, G. A., Zhang, C., Satler, L. F., Ben-Dor, I., Hashim, H., Rogers, T., & Waksman, R. (2021). Comparison of Characteristics and Outcomes of Patients With Acute Myocardial Infarction With Versus Without Coronarvirus-19. The American journal of cardiology, 144, 8–12. [CrossRef]
- Rodriguez-Leor, O., Cid Alvarez, A. B., Pérez de Prado, A., Rossello, X., Ojeda, S., Serrador, A., López-Palop, R., Martin-Moreiras, J., Rumoroso, J. R., Cequier, A., Ibáñez, B., Cruz-González, I., Romaguera, R., & Moreno, R. (2021). In-hospital outcomes of COVID-19 ST-elevation myocardial infarction patients. EuroIntervention : journal of EuroPCR in collaboration with the Working Group on Interventional Cardiology of the European Society of Cardiology, 16(17), 1426–1433. [CrossRef]
- Choudry, F. A., Hamshere, S. M., Rathod, K. S., Akhtar, M. M., Archbold, R. A., Guttmann, O. P., Woldman, S., Jain, A. K., Knight, C. J., Baumbach, A., Mathur, A., & Jones, D. A. (2020). High Thrombus Burden in Patients With COVID-19 Presenting With ST-Segment Elevation Myocardial Infarction. Journal of the American College of Cardiology, 76(10), 1168–1176. [CrossRef]
- Saad, M., Kennedy, K. F., Imran, H., Louis, D. W., Shippey, E., Poppas, A., Wood, K. E., Abbott, J. D., & Aronow, H. D. (2021). Association Between COVID-19 Diagnosis and In-Hospital Mortality in Patients Hospitalized With ST-Segment Elevation Myocardial Infarction. JAMA, 326(19), 1940–1952. [CrossRef]
- Kite, T. A., Ludman, P. F., Gale, C. P., Wu, J., Caixeta, A., Mansourati, J., Sabate, M., Jimenez-Quevedo, P., Candilio, L., Sadeghipour, P., Iniesta, A. M., Hoole, S. P., Palmer, N., Ariza-Solé, A., Namitokov, A., Escutia-Cuevas, H. H., Vincent, F., Tica, O., Ngunga, M., Meray, I., … International COVID-ACS Registry Investigators (2021). International Prospective Registry of Acute Coronary Syndromes in Patients With COVID-19. Journal of the American College of Cardiology, 77(20), 2466–2476. [CrossRef]
- Dadras, O., SeyedAlinaghi, S., Karimi, A., Shamsabadi, A., Qaderi, K., Ramezani, M., Mirghaderi, S. P., Mahdiabadi, S., Vahedi, F., Saeidi, S., Shojaei, A., Mehrtak, M., Azar, S. A., Mehraeen, E., & Voltarelli, F. A. (2022). COVID-19 mortality and its predictors in the elderly: A systematic review. Health science reports, 5(3), e657. [CrossRef]
- Stefanini, G. G., Montorfano, M., Trabattoni, D., Andreini, D., Ferrante, G., Ancona, M., Metra, M., Curello, S., Maffeo, D., Pero, G., Cacucci, M., Assanelli, E., Bellini, B., Russo, F., Ielasi, A., Tespili, M., Danzi, G. B., Vandoni, P., Bollati, M., Barbieri, L., … Chieffo, A. (2020). ST-Elevation Myocardial Infarction in Patients With COVID-19: Clinical and Angiographic Outcomes. Circulation, 141(25), 2113–2116. [CrossRef]
- Kaur, P., Patel, P., Singh, B., Guragai, N., Vasudev, R., Virk, H. S., Shamoon, F., & Bikkina, M. (2021). ST-Segment Elevation in Patients with COVID-19: A Late Complication. The American journal of the medical sciences, 361(3), 403–405. [CrossRef]
- Muñoz-Price, L. S., Nattinger, A. B., Rivera, F., Hanson, R., Gmehlin, C. G., Perez, A., Singh, S., Buchan, B. W., Ledeboer, N. A., & Pezzin, L. E. (2020). Racial Disparities in Incidence and Outcomes Among Patients With COVID-19. JAMA network open 3(9), e2021892. [CrossRef]
- Dai, C. L., Kornilov, S. A., Roper, R. T., Cohen-Cline, H., Jade, K., Smith, B., Heath, J. R., Diaz, G., Goldman, J. D., Magis, A. T., & Hadlock, J. J. (2021). Characteristics and Factors Associated With Coronavirus Disease 2019 Infection, Hospitalization, and Mortality Across Race and Ethnicity. Clinical infectious diseases : an official publication of the Infectious Diseases Society of America, 73(12), 2193–2204. [CrossRef]
- Bangalore, S., Sharma, A., Slotwiner, A., Yatskar, L., Harari, R., Shah, B., Ibrahim, H., Friedman, G. H., Thompson, C., Alviar, C. L., Chadow, H. L., Fishman, G. I., Reynolds, H. R., Keller, N., & Hochman, J. S. (2020). ST-Segment Elevation in Patients with Covid.
- A Case Series. The New England journal of medicine, 382(25), 2478–2480. [CrossRef]
- Hamadeh, A., Aldujeli, A., Briedis, K., Tecson, K. M., Sanz-Sánchez, J., Al Dujeili, M., Al-Obeidi, A., Diez, J. L., Žaliūnas, R., Stoler, R. C., & McCullough, P. A. (2020). Characteristics and Outcomes in Patients Presenting With COVID-19 and ST-Segment Elevation Myocardial Infarction. The American journal of cardiology, 131, 1–6. [CrossRef]
- Evbayekha E, Okorare O, Okobi O. A Year Retrospective Study on the Morbidity and Mortality Pattern of Covid-19 Patients in an Isolation Facility in Benin City, Nigeria -. IJSCIA. Published August 27, 2021. Accessed May 10, 2023. https://www.ijscia.com/full-text-volume-2-issue-4-jul-sep-2021-659-663/.
Figure 1.
Percentages of DVT and PE in the study population.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



