Submitted:
12 July 2023
Posted:
14 July 2023
You are already at the latest version
Abstract
Background - Mandibular flexion (MF) is a complex biomechanical phenomenon, which involves a deformation of the mandible, due mainly to the contraction of the masticatory muscles, and can have numerous clinical effects. The main aim of the current systematic review is to highlight the different factors that can increase MF, to help clinicians, identify patients to whom they should pay more attention. As a secondary outcome, we wanted to analyze the preventive measures and suitable techniques to be adopted to minimize the negative effects of this phenomenon on oral fixed rehabilitations. Methods - The review, which was carried out in accordance with the “Preferred Reporting Items for Systematic reviews and Meta-Analyses” (PRISMA) flowchart, was recorded in the “International Prospective Register of Systematic Reviews” (PROSPERO). As research questions, “Patient/Population, Intervention, Comparison and Outcomes” (PICO) questions were employed. Using the ROBINS-I technique, the risk of bias in non-randomized clinical studies was evaluated. Results - The initial electronic search identified over 1300 potential articles, of which 54 studies were included in this systematic review. Information regarding the relationship between MF and individual factors, mandibular movements, impression-taking and fixed rehabilitations were obtained. Conclusions – The studies included in this systematic review showed that MF is greater during protrusive movements, in the posterior areas of the lower jaw, and in patients with brachial facial type, greater jaw length, small gonial angle and less density, length and bone surface of the symphysis. The biomechanical effects of mandibular flexion on fixed restorations are debated. Prospective clinical and radiological observational studies should be conducted to evaluate the potential short-, medium- and long-term consequences of MF.
Keywords:
mandibular flexure
; mandibular deformation
; fixed oral rehabilitation
; implant-supported full-arch
1. Introduction
All long bones in the body exhibit a complex biomechanical behaviour known as elastic-deformation under functional load and the human mandible is no exception [1]. This is mainly related to two different factors: the intricate structure of the bone, which is an elastic, anisotropic, and non-homogeneous tissue, and its anatomical horseshoe form, which is in close contact with the ligaments and muscles of the head and neck, particularly the masticatory ones [1,2,3,4,5]. The contraction of these structures results in pressure and tractional forces on the mandible, changing its shape. Median Mandibular Flexure (MMF) is the name for this multifactorial condition, which was first identified around 60 years ago. It more frequently happens when the mouth protrudes or opens, and less frequently when the mouth moves laterally [6,7,8]. Further studies have revealed that it also happens during clenching and bruxism, highlighting that mandibular flexion also occurs with muscular activity alone and not necessarily with jaw movements or when the occlusal load is placed on the jaw itself [9,10,11,12].
The bilateral contraction of the lateral or external pterygoid muscles (LPMs) is the primary source of this phenomenon: when the lower heads contract, they pull the condyles and condylar necks medially, forward and down, producing a buccolingual rotation of the mandibular arch [11]. However, measuring the force generated by the contraction of LPMs to ascertain this is quite difficult due to their size and position [13]. In addition to the lateral pterygoid muscles, the mylohyoid, platysma, superior pharyngeal constrictor and other jaw depressor muscles provide supplemental aid for its generation [11].
In the frontal plane, the distance between the right and left mandibular ramus narrows due to elastic flexion of the mandible, leading to a reduction in the width of the mandibular arch [6,7,8]. For increasing degrees of jaw opening, mandibular arch static amplitude analyses showed a gradual decrease in its medial-lateral diameter [10,14,15]. Furthermore, dynamic investigations have demonstrated an increase during mandibular retraction and a decrease during protrusion movements, owing to muscular contraction without tooth contact [1,9,11].
Hylander et al. recognized four mandibular deformation patterns during mandibular flexion: symphysis flexion, dorso-ventral shear, corporal rotation and antero-posterior shear [7]. From his research, it appeared that any of the postulated mandibular deformation patterns can provide compressive, tensile, or shear pressures, and that the highest symphyseal tension, which causes bending, was produced by the contraction of the medial component of the LPMs.
In addition to causing an alteration in the shape of the jaw with a reduction in the width of the arch from a few microns to 1 mm, with an average of 0.073 mm, MMF also affects the relative position of the teeth on the mandibular arch, producing lingual tipping [10,11,14,16,17]. The periodontal ligament reduces bone loss around teeth due to mandibular flexion in natural dentition by allowing the physiological movement of teeth [18,19]. According to Frost's mechanostatic theory, stress/strain levels are maintained within the bone's physiological adaptation window by avoiding an excessive rise in stress [20,21]. In the case of edentulous jaws restored with implant-supported full-arch prostheses, a rigid structure is created that connects the various implants, forming a single functional unit [22]. By doing this, not only is there no longer the protective effect of the periodontal ligament, but it facilitates the creation of flexural forces that modify and/or increase bone stress around the implants, resulting in resorption [8,23,24]. Mandibular flexion was found to be the main factor contributing to posterior implant failure in mandibular full-arch fixed prostheses with solidarized implants by Miyamoto et al. [25]. In fixed implant restorations, the biomechanical effect of the mandible's functional flexibility might result in crestal bone loss surrounding the implant head. Moreover, several clinical and experimental research have demonstrated that mandibular bending can negatively impact the proper fit of fixed and removable prostheses, lead to denture decementation, and cause fracture of porcelain, screws, or implants [6,17,26,27,28]. Once more, the accuracy of the impression can be impacted by the lingual tipping of the teeth that happens when the mouth is opened for impression-taking, creating a series of flaws that could result in treatment failure [15].
As the deformation of the lower jaw caused by mandibular flexion is generally very small, it is often overlooked and considered irrelevant from a clinical point of view by many authors, especially taking into account the large size of the mandible in relation to the lateral pterygoid muscle [27]. However, it should be important to remember that MMF has a multifactorial aetiology and that there are many variables that can affect it and cause increasing deformity up to non-negligible levels. These parameters include facial type, mandibular structure and symphysis characteristics of bone density, length and surface area [29,30,31,32,33,34].
This is the background to the present review, the main aim of which is to highlight the different factors that can increase mandibular flexure, to help clinicians, identify patients to whom they should pay more attention [35]. As a secondary outcome, we wanted to analyse the preventive measures and suitable techniques to be adopted to minimise the negative effects of this phenomenon on oral fixed rehabilitations. More emphasis was placed on the different types of fixed full-arch implant-supported rehabilitations. This is intended to facilitate the success of dental therapies aimed at preserving the health of periodontal and peri-implant tissues and achieving long-term outcomes.
2. Materials and Methods
2.1. Study protocol
The study protocol was developed in compliance with the Preferred Reporting Items for Systematic Reviews and Meta-analyses (PRISMA) statement before the literature search, data extraction, and analysis and was registered on the “International Prospective Register of Systematic Reviews” (PROSPERO) (ID 438105).
The research question was formulated according to the Population, Intervention, control or Comparison, Outcome (PICO) strategy.
The clinical question in "PICO" format was: Is there a significant difference in mandibular flexion values based on several factors that may influence fixed oral rehabilitations and what are the preventive measures and suitable techniques to be adopted to minimise the negative effects of this phenomenon on fixed oral rehabilitations?
P (Population): subjects with mandibular oral fixed oral rehabilitations;
I (Intervention): mandibular oral fixed rehabilitations;
C (Comparison): subjects without oral fixed rehabilitations;
O (Outcome): factors that can increase mandibular flexure and the preventive measures and suitable techniques to be adopted to minimise the negative effects of this phenomenon on fixed oral rehabilitations.
2.2. Search Strategy
Studies published in the English language concerning factors that can influence mandibular flexure and the influence of MF on oral fixed rehabilitations were electronically searched without date restrictions till 1st May 2023.
An electronic search was conducted through several databases: MEDLINE/PubMed, Google Scholar, BioMed Central, and the Cochrane Library databases, by two independent reviewers (D.G. and A.A.).
The search was performed using the following keywords with Boolean operators:
(“deformation’’ OR “flexion” OR “median flexion” OR “flexure” OR “median flexure”)
AND
(“mandibular” OR “mandible”).
The following filters were applied:
-English language on the MEDLINE/PubMed database;
No filters were employed on BioMed Central database, Google Scholar and on the Cochrane library.
2.3. Study Selection and Eligibility Criteria
The inclusion and exclusion criteria that were established before the start of the search and adhered to when selecting studies are shown below.
Inclusion Criteria:
- -
- Studies published in English language;
- -
- In vivo and in vitro studies;
- -
- Studies examining the effects of mandibular flexion on fixed rehabilitations and the factors influencing it;
- -
- Studies highlighting suitable clinical techniques to be adopted to minimise the negative effects of mandibular flexion.
Exclusion Criteria:
- -
- Studies not published in English language;
- -
- Reviews, systematic reviews and case reports;
- -
- Studies about the mandibular flexure along with any other physiological or pathological problems;
- -
- Articles that review removable prosthodontic treatments.
Collected citations were recorded, duplicates were eliminated through the Zootero reference manager tool, and the remaining titles were screened by two independent reviewers (D.G. and M.C.). The same two reviewers subsequently screened relevant abstracts of obtained studies.
Full texts of those potentially eligible abstracts were obtained, and full texts were independently reviewed by the same authors (D.G. and F.D.A.). Any disagreement was solved by discussing and a third Author (A.A.) was consulted in case of doubts.
The bibliography of the selected articles was examined for relevant titles and the subsequent study screening was performed as already described.
No restrictions regarding the date of publication or number of studies were applied.
2.4. Data Extraction and Collection
Data were independently extracted in duplicate by two authors (D.G. and F.D.A.) on a standardized data extraction form developed from the models proposed for intervention reviews on RCTs and non-RCTs before data extraction; a third author (A.A.) was involved in case of disagreement. From each studies included in the present umbrella review, the following data criteria were recorded:
- -
- Author(s), year and journal of publication, and kind of the study;
- -
- Type of rehabilitation, and sample size;
- -
- Factors that can increase mandibular flexure;
- -
- Preventive measures and suitable techniques to be adopted to minimise the negative effects of this phenomenon on oral rehabilitations.
2.5. Data Synthesis
The characteristics and main findings of the included studies are presented in tabular form and summarized through a narrative synthesis.
Data from included studies were qualitatively synthesized through descriptive statistical analysis using the Microsoft Excel software 2019 (Microsoft Corporation, Redmond, WA, USA).
The main aim of which is to highlight the different factors that can increase mandibular flexure, to help clinicians, identify patients to whom they should pay more attention. As a secondary outcome, we wanted to analyse the preventive measures and suitable techniques to be adopted to minimise the negative effects of this phenomenon on oral rehabilitations.
2.6. Quality Assessment
The risk of bias of the non-randomized clinical trials was highlighted by the ROBINS-I (“Risk Of Bias In Non-randomized Studies - of Interventions”) tool (Sterne JA et al.2016).
In this tool different bias are underline: biases due to confounding, bias due to selection of participants, biases due to classification of interventions, biases due to deviations from intended interventions, bias due to missing data, biases in measurement of outcomes and biases due to selection of the reported result (Sterne JA et al. 2016).
The risk of bias assessment was categorized into four levels:
- -
- Low risk of bias: the study is judged to be at low risk of bias for all domains.
- -
- Moderate risk of bias: the study is judged to be at low or moderate risk of bias for all domains.
- -
- Serious risk of bias: the study is judged to be at serious risk of bias in at least one domain, but not at critical risk of bias in any domain.
- -
- Critical risk of bias: the study is judged to be at critical risk of bias in at least one domain.
The response options for the bias are: Yes (Y), Probably yes (PY), Probably no (PN), No (N) and No information(NI). “Y” indicate low risk of bias, “PY” indicate a moderate risk of bias; “PN” indicate a serious risk, “N” indicate a critial risk of bias and “NI” indicate that are no informations.
3. Results
3.1. Study Selection
The initial electronic search identified over 1300 potential articles. In particular, 991 records were found using MEDLINE/PubMed, 56 records were found using Google Scholar, 185 records were found using BioMed Central and 156 records were found using Cochrane Library databases. By manual search, a further 23 articles were identified. Once duplicates were removed, of the 1141 title abstracts identified, only 71 title abstracts were screened. Of these 71 title abstracts, only 61 abstracts were useful for the present systematic review, in accordance with the inclusion criteria. Of these 61 records, their full texts were obtained and screened, and 7 articles were excluded, as shown in Table 1. The table includes author names, years of publication of the study, reference and motivation for exclusion of their studies from the present review. A total of 54 studies met the eligibility criteria and were included in the review (Figure 1 and Table 2).
3.2. Study characteristics
The main features of the included studies are summarized in Table 2.
3.3. Data Extraction and Synthesis
Detailed findings related the presence or absence of a significant correlation between mandibular flexion (MF) and various individual factors, and the values of MMF according to different types of mandibular movements are respectively synthesized in Table 3 and Table 4. The tables include also information about the author(s), the year of publication and the reference of the articles where these topics are discussed, as well as the type of rehabilitation and the sample size.
The articles concerning the different frameworks of implant-supported full-arch rehabilitations are summarised in Table 5. The table presents information about the author, year of publication and reference of the articles focused on the topic, type of rehabilitation, sample size, and results in favour of divided (D) or undivided (U) frameworks.
3.4. Quality Assessment of the Included Studies
The evaluation of the risk of bias of the studies included in this systematic review was conducted using the “Risk Of Bias In Non-randomised Studies - of Interventions” tool (ROBINS-I), which identifies various sources of bias that can potentially affect the validity and reliability of study findings.
4. Discussion
All of the studies included in the present review established that mandibular bending exists and most of them focused on calculations and measurements of mandibular deformation during various jaw movements.
4.1. Measurement of mandibular flexion
Due to the wide variability in jaw size and bone density between individuals, the assessment of mandibular biomechanical characteristics is challenging. In addition, the contraction of the masticatory muscles can generate a wide range of mandibular movements and forces that play a key role in the genesis of MMF. It is extremely difficult to measure the force that the superficial muscles of mastication, such as the masseters, exert on the mandible, and even more so regarding the deep muscles, such as the lateral pterygoid muscles, due to their position and size.
The range of mandibular flexure measurements is a few micrometres to around 1 mm, with an average value of 0.073 mm [11,12,14,16,17,39,43,65,70,76,77].
Such a large range can be justified by several factors affecting the measurements:
- -
- Individual factors: facial type, mandibular structure, gonial angle and symphysis characteristics (density, length, and bone surface). Some authors have also proposed age, gender, maximum occlusal force (MOF), height, weight, BMI, muscle pain, bruxism and tooth wear as parameters that may influence mandibular flexion values.
- -
- Measurement techniques: in vivo or in vitro.
- -
- Type of movement performed during measurement: protrusion, mouth opening, laterality and retrusion.
- -
- Area of the mandible where the measurement is performed: incisor-canine, premolar and molar area.
- -
- Clinical condition of the mandible: jaw with teeth or edentulous.
4.1.1. Individual factors
There are three different patterns of facial types:
- -
- Brachifacial: is characterised by a reduced angle of the mandibular plane, reduced vertical facial height and a horizontal growth pattern, with maximum muscle anchorage. Brachifacial patients present a short and wide face, a square jaw and strong muscle chains.
- -
- Mesofacial: is characterised by a medium mandibular plane angle, medium vertical facial height, and a mixed growth pattern, with medium muscle anchorage. Mesofacial patients are referred to as “neutral subjects” because no skeletal or muscular features prevail in them, showing a harmonious balance of the vertical and horizontal components of the face.
- -
- Dolichofacial: is characterised by a high mandibular plane angle, high vertical facial height and a vertical growth pattern, with minimal muscle anchorage. Dolichofacial patients have a long, narrow face with a convex profile [78].
From an epidemiological point of view, 70% of the population is mesofacial, while the remaining 30% is divided more or less evenly between brachifacial and dolichofacial types [79]. Since the brachifacial patient has stronger masticatory muscles, it has been hypothesised that they have a higher MMF, followed by the mesofacial and dolichofacial types. This hypothesis has been supported by numerous studies relating facial type to mandibular flexion, all of which were initially conducted on natural dentition [23,26,29,30,34,80]. Nevertheless, Shinkai et al. ruled out a significant influence of facial type on MMF, arguing that, given the small size and not excessive strength of the lateral pterygoid muscle, muscular strength plays a secondary role with respect to the resistance of the bone structure to mandibular deformation [33]. The recent study by Gao J. et al. evaluated for the first time the morphological-functional response to mandibular flexion of implant-supported prostheses in different facial types, showing that not only is mandibular deformation greater in brachial patients, but that different clinical arrangements are required than in meso- and dolicho- patients [75].
Mandibular flexion is directly correlated with the length of the mandibular structure: the longer the mandible, the greater the mandibular flexion. Furthermore, it has been shown that the gonial angle, which represents mandibular inclination, when reduced, statistically affects the increase in mandibular flexion, even if to a limited extent [12].
Parameters of considerable influence on MMF are the symphysis characteristics, such as height and length, surface area and bone density. Several in vivo studies have shown that symphyses with increased length and height, large surface area and high bone density are more resistant to mandibular deformation, reducing it [7,17,26,30].
On the other hand, older edentulous individuals are more inclined to experience higher mandibular deformation because they have less thick skeletons due to an increased risk of osteoporosis and smaller symphyses as a result of bone resorption after edentulousness [24,43,46,47,49]. However, no age difference was identified in the MMF evaluation between the two groups in the research by Gülsoy et al., where the average age of the edentulous individuals was 63 years and that of the dentate participants was 29 years (P >.05) [74]. Even though the age-mandibular flexion correlation has not been proven in numerous articles with statistically significant results, the studies showing its interdependence can be explained by the connection between age-related consequences (lower bone density and smaller symphysis structure) and mandibular deformation [72].
Regarding the relationship between sex and mandibular flexion, multiple studies have found that women exhibit more mandibular flexion than males, albeit this difference is not statistically significant [12,30,34,65,76]. A predictability of 32-95.6% was discovered after several research investigated the potential forecasting of sex from mandibular flexion ranges and different mandibular characteristics. The predictive accuracy of mandibular flexion for sex determination was found to be smaller in women than in males by Balci et al. and Shinkai et al. [33,55]; this is probably because women exhibit a greater variability in mandibular arch width. Kemkes-Grottenthaler et al. claim that measurements of the gonial angle, mandibular flexion, and length and width of the ramus can be precise and predictable criteria for morphological identification [51]. However, age and edentulousness may substantially diminish these markers' accuracy. In the study by Gülsoy et. al., in which no statistically significant difference was found between the sexes in terms of MMF values in both edentulous and dentate patients, the mean MMF values were slightly higher in edentulous males [74]. This is probably due to women experience three times the amount of bone resorption in postmenopausal than men do, and their trabecular bone mineral density decreases more dramatically than men's does [60].
According to Canabarro and Shinkai et al., R. S. Shinkai et al. and Chen et al. evaluations, there was no statistically significant correlation between MMF and other parameters such as maximum occlusal force (MOF), height, weight, BMI, muscle pain, bruxism, and tooth wear. It is highly probable that MOF is unrelated to jaw flexion since anthropometric factors (height, weight, and BMI), muscular soreness, bruxism, and tooth wear have a direct proportionality connection with MOF but do not affect mandibular flexion. However, more research is required.
4.1.2. Measurement techniques
In vitro and in vivo intra- and extra-oral measuring techniques were utilized in the various investigations to analyze the degree of mandibular deformation.
Diagnostic models made from imprints obtained at various phases of the mandibular opening were frequently used to make in vivo extra-oral measurements, as were photos that monitored the movement of the mandibles [10,15,30,72].
On the other hand, strain gauges, calipers, and transducers connected to surfaces or implants were used to make in-vivo intra-oral measurements [9,10,14,39,43,76,81].
In vitro measurements to assess the distribution of deformations in the mandibular body were conducted initially using photoelastic models and subsequently by means of FEA, i.e. finite element analysis, which simulates three-dimensional models [74,82,83,84].
However, each of these measuring techniques has disadvantages and limitations. For instance, the strain gauge method can only be used to measure exact strain values at the locations where the strain gauge is placed, whereas the use of photoelastic models has significant numerical data limitations but provides excellent qualitative data on the distribution and concentration of stresses [85]. On the other hand, the finite element method (FEA) can provide detailed quantitative data at any point in the mathematical model. However, in order to obtain accurate results, the modelling must be performed accurately and must look like the real structure [86]. Moreover, modelling biological tissues has several of drawbacks and difficulties, and bone structure can vary both within and between people [74,87]. Compared to models created by scanning traditional impressions, digital models created by intra-oral scanning have been shown to have higher dimensional accuracy: this is mainly related to the fact that, with oral scanning, errors that can arise from an incorrect water/dust ratio of the plaster material and deformation of the impression material are eliminated [88,89,90]. Furthermore, the pressure used to press down on the jaw when obtaining an imprint using conventional techniques may affect mandibular flexibility [70].
4.1.3. Type of movement performed during measurement
According to Omar & Wise, there is no change in the mandibular arch width up to a mouth opening of 28% [11]; however, after that point, the decrease is proportionate to the degree of mouth opening, with an average loss of 0.093 mm and a range of 0.012-0.164 mm. The results from this study are comparable to those obtained in the research of Goodkind & Heringlake and Regli & Kelly, where the deformation ranges from 0.0316 mm to 0.0768 mm and 0.03 mm to 0.09 mm respectively, depending on the degree of mouth opening [9,10]. Fischman et al. also obtained similar values of mandibular bending, i.e. 0.0711 mm at mouth opening [15]. The values obtained by Chen et al. (2000) on a larger sample (62 volunteers as opposed to Fishman's 10) are, on the other hand, slightly larger, at 0.145 mm MMF [30].
Gates e Nicholls demonstrated that mandibular flexion was greater during protrusion movements than during mouth opening movements. In their work, the distortion values found during opening ranged from 0 to 0.3 mm, in line with the studies of Osborne et al., Bowman et al. and Goodkind & Heringlake, but lower than the ranges 0.2-1.4 mm and 0.6-1.5 mm, found by McDowell & Regli and De Marco & Paine, respectively [6,9,14,41,42]. Whereas, strain values during protrusion range from 0.1 to 0.5 mm, in line with the results obtained by Osborne et al., but lower than the 0.2-1.2 and 0.2-1.5 mm ranges of Bowman et al. and McDowell & Regli, respectively. Several other clinical and biomechanical studies highlighted the increased mandibular deformation and stress/strain during protrusion movements [57,58,59,68,71]. The lack of involvement of the anterior digastric muscles in mandibular flexion during mouth opening may be the cause of this. From a therapeutic perspective, parafunctions like grinding or incisal-incisal margin contact can greatly be influenced by this, while for the mastication, where protrusive motions are uncommon, is less significant.
As demonstrated by Burch and Borchers, also lateral movements can cause the mandibular arch decrease [43]. In the right lateral position, the average amplitude of the reduction was 0.243 mm, and in the left lateral position, it was 0.257 mm. Due to the activation of only one lateral pterygoid muscle rather than both, the mandibular flexion values in lateral motions are lower than those in protrusion (0.61 mm MMF) and mouth opening (0.438 mm MMF). The same author then conducted research with a larger sample size (25 participants as opposed to 10 in the prior study) and same results were validated [1].
4.1.4. Area of the mandible where the measurement is performed
Asadzadeh et al.'s study was the first to examine the potential for various mandibular deformation levels across different mandibular regions [76]. Prior to this investigation, mandibular bending was usually measured at the level of the first or second molar in the posterior intermolar areas. On 35 female volunteers with teeth, Asadzadeh et al. measured MMF using digital calipers in the area of the canines and second molars. In the molar area (0.1894 mm), the mandibular flexure measured greater values than in the canine region (0.1671 mm). This can be explained by the closer proximity of the posterior sectors to the LPMs muscle insertions; as one moves toward the anterior sectors from them, mandibular flexion reduces more and more. The recent study by Gülsoy, Tuna, and Pekkan confirmed this hypothesis by taking measurements in seven different regions, starting from the anterior to the posterior region, in dentate and edentulous individuals [74]. To standardize the landmarks in the edentulous individuals, the markers of the dentate persons were employed. In both the toothed and the edentulous specimen, it was shown that the symphyseal region serves as the center of rotation and that the degree of deformation increases linearly from anterior to posterior locations. The measurements taken on the dentate specimen were 0.048 mm, 0.138 mm, 0.224 mm, 0.324 mm, 0.391 mm, 0.470 mm, and 0.630 mm, whereas the measurements taken on the edentulous specimen were 0.089 mm, 0.162 mm, 0.239 mm, 0.343 mm, 0.452 mm, 0.552 mm, and 0.710 mm. The differences in the MMF values in the molar region of this study compared to past studies can be explained by taking into account individual factors in the sample and variations related to measurement techniques.
Last but not least, a study by Angel Alvarez Arena revealed that during mouth opening, flexion was greatest at the level of the condyles, slightly less at the level of the body of the mandible, and virtually nonexistent in the area of the symphysis, whereas during protrusion, flexion was greatest at the level of the angle of the mandible [32].
4.1.5. Clinical condition of the mandible
Following tooth loss, which frequently occurs brought on by aging, alveolar bone resorbs, and the mineral content and density of cortical and trabecular bone decrease [91]. Mandibular flexion is typically enhanced in low bone density patients. However, due to a loss in collagen fibers with age, bone tissue's elasticity also declines [92]. In light of all of these factors, it follows that mandibular flexion is not significantly different in dentate and edentulous people, nor is it different with age. The study by Gülsoy, Tuna, and Pekkan found no statistically significant difference in the MMF values of the same mandibular areas in dentate and edentulous patients [74].
4.2. Clinical effects of MMF
This review revealed a very wide range of mandibular flexion values, from a few micrometres to about 1 mm, with an average of 0.073 mm. Since it is often relatively little, it is frequently disregarded and viewed as useless from a therapeutic perspective. However, more so in protrusive movements and to a lesser extent in mouth-opening movements, in the posterior areas of the mandible and in the presence of individual factors, such as brachi- facial type, long mandibular structure, small gonial angle, and lower symphysis bone density, length, and surface area, the results of the numerous reviewed articles consistently show higher MMF values, which cannot be clinically neglected to preserve periodontal and peri-implant tissue health and achieve long-term outcomes [6,7,12,17,26,30,74,75,76]. Mandibular flexure may affect the precision of the many processes of various prosthetic treatments, especially fixed ones, which might result in failure. It can result in peri-implant bone resorption, distortion of the impression, improper fit of removable or fixed prostheses, fracture of implant screws or porcelain prosthetic crowns, and chewing pain by altering the distribution of masticatory stresses and increasing their intensity in implant-supported prostheses, abutments, and surrounding bone [93]. As a consequence, it's crucial to implement therapeutic modifications and preventative measures to lessen the negative effects of this phenomena on oral rehabilitations [23,27,94,95,96,97,98,99,100,101,102].
4.2.1. MMF and impression-taking
This review clearly showed that, during mouth opening movements, mandibular flexion results in a reduction of the mandibular arch and a lingual tipping of the teeth. All impression-taking methods include a certain amount of mouth opening; hence it is inevitable that the effects of MMF be taken into consideration while creating an impression. Generally, the imperfect fit of dentures was attributed to the variability of dental procedures, not considering the influence of MMF, which can alter the precision of the master model and compromise the prosthesis [9,15]. The prosthesis created from the impression taken with the mouth open wide may not fit the jaw precisely when it is at rest because it is built on a limited arch and has teeth that are not only more lingual but also rotated lingually. This may lead to pressure on the teeth and surrounding structures, pain, gingival inflammation, tooth mobility and bone loss. The areas generally subject to most pain are located below the lower denture, at the level of the mylohyoid ridge, where the greatest stress occurs during mandibular flexion [39,44]. In implant-supported full-arch prostheses, it is even more important that impressions are accurate to allow a passive fit of the superstructure on rigidly connected implants [23,103]. Consequently, in order to minimise deformation when taking traditional impressions for the lower jaw, it has been suggested that impressions should be made with a minimum mouth opening, as close to the upper jaw as possible and ideally no more than 20 mm, so as to involve minimal activation of the masticatory muscles [15]. In addition, any protrusive movement should be avoided and, while hardening the impression, the dentist should avoid touching the patient's jaw, pushing it up or down [40]. The extent of minimisation is uncertain, however, given the limited literature on the subject. For impressions intended for fixed prosthetic rehabilitations, the use of vinyl polysiloxane (PVS), which has greater dimensional stability than other impression materials, and the use of individual impression posts should be preferred.
4.2.2. MMF and fixed teeth-supported rehabilitation
By allowing physiological movement of the dental elements, the periodontal ligament (PDL) absorbs most of the stress created by mandibular flexion, preventing bone loss around them [18,19]. However, in fixed teeth-supported rehabilitations, the use of rigid connectors and long spans limits the movement of the dental components and, as a result, increases stress at the PDL level, which may outcome in bone resorption, as well as at the level of the prosthesis itself, which may end up in porcelain fractures. It is preferable to utilize flexible connections and divide the span into many portions to prevent such unfavorable effects, especially in the case of periodontal patients. Additionally, it is not advised to utilize porcelain for bigger restorations [10,15,45,52].
4.2.3. MMF and implant-supported full-arch fixed rehabilitations
By changing the distribution of stresses at the bone/implant interface and at the level of the prosthetic structure itself, mandibular flexure has the potential to affect the accuracy of several phases of implant rehabilitations, including osseointegration and the creation of implant-supported prostheses. This can result in peri-implant bone resorption, material fracture, and pain during function.
The main goal of implant-supported fixed restorations is to determine an adequate biomechanical distribution both at the level of the prosthetic superstructure and at the level of the implant [68].
In order to achieve this, it is necessary to make assessments on three different parameters:
- -
- Type of prosthesis: single or segmented structure
- -
- Material of the superstructure
- -
- Number and position of implants
Type of prosthesis: single or segmented structure
The results that have emerged from the literature are somewhat contradictory regarding the necessity or not of splitting the superstructure, separating doctors into two separate schools of thinking. For some authors, division of the superstructure at the level of the symphysis is recommended to reduce the increased stresses occurring at that level [53,61,63]. This indication was also supported by Fischman and McCartney, who highlighted how a single, continuous and rigid structure can subject both the implant/bone interface and the prosthetic structure to dangerous concentrations of stress, increasing the rate of screw loosening and fracture [15,102]. Other studies favour the undivided superstructure because it can evenly distribute stresses between the splinted implants and its inherent rigidity can provide additional resistance to mandibular bending [56,68]. In any case, all studies agree that it is preferable to divide the structure into two segments at the level of the symphysis rather than three or more segments. Finally, a study by Gao et al. related facial type to prosthetic superstructure [75]. It was found that a one-piece prosthesis is preferable for the brachifacial type, whereas in the case of the mesofacial or dolichofacial type there is more freedom of choice, with the single structure being preferred if the patient's other individual factors are correlated with bigger mandibular flexion values.
Material of the superstructure
The material of the superstructure could also influence mandibular bending. Suedam et al. found that materials with a lower modulus of elasticity, and thus more flexible, reduce stress to a greater extent, while stiffer materials are more resistant to bending forces [99]. Consequently, they recommended a high modulus of elasticity for the superstructure. This indication was later confirmed by the subsequent work of Favot et al. and rejected by that of Marin et al. [31,38]. Other studies, however, stated that the stiffness of the material used for the prosthesis does not affect mandibular flexion as much as other parameters [46,63,100].
Number and position of implants
Over the years, several protocols have been proposed for implant-supported fixed rehabilitation of mandibular totally edentulous patients. Brånemark's initial technique for the rehabilitation of totally edentulous patients involved the use of 5 implants for the mandible and 6 for the maxilla arranged in parallel and distributed in the inter-foraminal region for anatomical and surgical reasons, such as the location of the alveolar nerve and the quantity and quality of bone [105]. In agreement with the aim of modern dentistry, which is to develop minimally invasive rehabilitations that guarantee functionality, aesthetics, comfort and cost containment, Malò and Rangert introduced the All-on-4 technique in 2003, as an alternative to much more expensive and invasive methods for the rehabilitation of patients with severe posterior bone atrophy. This technique consisted of the insertion of two axial implants in the lateral incisor/canine area and two implants just mesial to the chin foramen inclined distally at about 30° to the occlusal plane with the implant plate near the second premolar and prosthetic superstructure with distal cantilevers [106]. However, several clinical and virtual studies, using finite element analysis (FEA), have shown that restorations with distal cantilevers can lead to detrimental biomechanical stress on the peri-implant bone, due to unfavourable lever arms [107,108,109]. Shackleton et al., White et al., Lindquist et al., Naert et al. confirmed the potential negative effects of distal cantilevers, showing a lower success rate and peri-implant bone loss [97,110,111,112]. Fenton & Zarb interpreted these results, suggesting the placement of multiple implants to achieve an even distribution of stresses and avoid long cantilevers [113]. On this line of thought, Agliardi et al. proposed the All-on-6 technique [114].
To date, there is no uniformity of thought on either the precise number of implants or their positioning in the arch for ideal rehabilitation. Over the years, several studies have been conducted to evaluate the effects of mandibular flexion on individual implants in different types of rehabilitation. From the reviewed articles, a controversy has arisen regarding the placement of implants mesial or distal to the chin foramen: some scholars, including Zarone et al., prefer their placement more mesial, allowing for less pressure on the implants; others, including Nokar et al., recommend placing implants also more distal, demonstrating that peri-implant bone stress is less in this position [53,63]. The lack of unanimity of results may be due to the large number of parameters influencing mandibular flexion in implant-supported restorations.
5. Conclusions
Mandibular flexion is greater during protrusive movements, in the posterior areas of the lower jaw, and in patients with brachial facial type, greater jaw length, small gonial angle and less density, length and bone surface of the symphysis. The various articles reviewed showed no statistically significant difference in the extent of mandibular flexion between the right and left hemiarch, between edentulous and toothless patients, and when parameters such as age, gender, maximum occlusal force (MOF), height, weight, BMI, muscle pain, bruxism and tooth wear were varied.
To minimise its negative effect and achieve long-term outcomes, certain preventive measures and suitable techniques must be adopted during the different phases of oral rehabilitations.
The literature suggests that the impression of the lower jaw should be taken with a minimum mouth opening, as close to the upper jaw as possible and ideally no more than 20 mm, to involve minimal activation of the masticatory muscles. In addition, any protrusive movement should be avoided and, while hardening the impression, the dentist should avoid touching the patient's jaw by pushing it up or down. Finally, digital scans showed minimal mandibular flexion and more effective results than traditional impressions.
About fixed dento-supported rehabilitations, it is advisable to use non-rigid connectors and to divide the span into several sections, even more so in the case of periodontal patients. Furthermore, the use of porcelain in larger restorations is not recommended.
The biomechanical effects of mandibular flexion on fixed implant-supported restorations are debated. Considering the inhomogeneity of results with regard to the number and position of implants, the segmentation or non-segmentation of the superstructure and its material of construction, further prospective clinical and radiological observational studies should be conducted to evaluate the potential short-, medium- and long-term consequences of mandibular flexure on implant-supported full-arch restorations.
Author Contributions
Conceptualization, M.C. and F.G.; methodology, M.C. and F.D.A; software, A.A.; validation, F.D.A and F.G.; investigation, D.G.; data curation, A.A.; writing—original draft preparation, A.A and F.D.A.; writing—review and editing, M.C and A.A.; visualization, F.G.; supervision, F.G.; All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Data Availability Statement
All data generated or analyzed during this study are included in this article.
Acknowledgments
None.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Burch, J.G. Patterns of Change in Human Mandibular Arch Width during Jaw Excursions. Arch Oral Biol 1972, 17, 623–631. [Google Scholar] [CrossRef] [PubMed]
- Wall, J.C.; Chatterji, S.K.; Jeffery, J.W. The Influence That Bone Density and the Orientation and Particle Size of the Mineral Phase Have on the Mechanical Properties of Bone. J Bioeng 1978, 2, 517–526. [Google Scholar] [PubMed]
- Bonfield, W. Elasticity and Viscoelasticity of Cortical Bone. In Natural and Living Biomaterials; CRC Press, 1984 ISBN 978-1-351-07490-2.
- Ashman, R.B.; Van Buskirk, W.C. The Elastic Properties of a Human Mandible. Adv Dent Res 1987, 1, 64–67. [Google Scholar] [CrossRef] [PubMed]
- Katz, J.L.; Meunier, A. The Elastic Anisotropy of Bone. J Biomech 1987, 20, 1063–1070. [Google Scholar] [CrossRef]
- Gates, G.N.; Nicholls, J.I. Evaluation of Mandibular Arch Width Change. J Prosthet Dent 1981, 46, 385–392. [Google Scholar] [CrossRef]
- Hylander, W.L. Stress and Strain in the Mandibular Symphysis of Primates: A Test of Competing Hypotheses. Am J Phys Anthropol 1984, 64, 1–46. [Google Scholar] [CrossRef]
- van Eijden, T.M. Biomechanics of the Mandible. Crit Rev Oral Biol Med 2000, 11, 123–136. [Google Scholar] [CrossRef]
- Goodkind, R.J.; Heringlake, C.B. Mandibular Flexure in Opening and Closing Movements. J Prosthet Dent 1973, 30, 134–138. [Google Scholar] [CrossRef]
- Regli, C.P.; Kelly, E.K. The Phenomenon of Decreased Mandibular Arch Width in Opening Movements. J Prosthet Dent 1967, 17, 49–53. [Google Scholar] [CrossRef]
- Omar, R.; Wise, M.D. Mandibular Flexure Associated with Muscle Force Applied in the Retruded Axis Position. J Oral Rehabil 1981, 8, 209–221. [Google Scholar] [CrossRef]
- Canabarro, S. de A.; Shinkai, R.S.A. Medial Mandibular Flexure and Maximum Occlusal Force in Dentate Adults. Int J Prosthodont 2006, 19, 177–182.
- Röhrle, O.; Pullan, A.J. Three-Dimensional Finite Element Modelling of Muscle Forces during Mastication. J Biomech 2007, 40, 3363–3372. [Google Scholar] [CrossRef] [PubMed]
- De Marco, T.J.; Paine, S. Mandibular Dimensional Change. J Prosthet Dent 1974, 31, 482–485. [Google Scholar] [CrossRef] [PubMed]
- Fischman, B. The Rotational Aspect of Mandibular Flexure. J Prosthet Dent 1990, 64, 483–485. [Google Scholar] [CrossRef] [PubMed]
- Linkow, L.I.; Ghalili, R. Ramus Hinges for Excessive Movements of the Condyles: A New Dimension in Mandibular Tripodal Subperiosteal Implants. J Oral Implantol 1999, 25, 11–17. [Google Scholar] [CrossRef] [PubMed]
- Shinkai, R.S.A.; Canabarro, S. de A.; Schmidt, C.B.; Sartori, E.A. Reliability of a Digital Image Method for Measuring Medial Mandibular Flexure in Dentate Subjects. J Appl Oral Sci 2004, 12, 358–362. [CrossRef]
- Wenzel, A.; Gröndahl, H.G. Direct Digital Radiography in the Dental Office. Int Dent J 1995, 45, 27–34. [Google Scholar]
- Borg, E.; Gröndahl, H.G. On the Dynamic Range of Different X-Ray Photon Detectors in Intra-Oral Radiography. A Comparison of Image Quality in Film, Charge-Coupled Device and Storage Phosphor Systems. Dentomaxillofac Radiol 1996, 25, 82–88. [Google Scholar] [CrossRef]
- Frost, H.M. Bone “Mass” and the “Mechanostat”: A Proposal. Anat Rec 1987, 219, 1–9. [Google Scholar] [CrossRef]
- Frost, H.M. A 2003 Update of Bone Physiology and Wolff’s Law for Clinicians. Angle Orthod 2004, 74, 3–15. [Google Scholar] [CrossRef]
- Pantaleo, G.; Acerra, A.; Giordano, F.; D’Ambrosio, F.; Langone, M.; Caggiano, M. Immediate Loading of Fixed Prostheses in Fully Edentulous Jaws: A 7-Year Follow-Up from a Single-Cohort Retrospective Study. Applied Sciences 2022, 12, 12427. [Google Scholar] [CrossRef]
- Hobkirk, J.A.; Havthoulas, T.K. The Influence of Mandibular Deformation, Implant Numbers, and Loading Position on Detected Forces in Abutments Supporting Fixed Implant Superstructures. J Prosthet Dent 1998, 80, 169–174. [Google Scholar] [CrossRef]
- Korioth, T.W.; Hannam, A.G. Deformation of the Human Mandible during Simulated Tooth Clenching. J Dent Res 1994, 73, 56–66. [Google Scholar] [CrossRef] [PubMed]
- Miyamoto, Y.; Fujisawa, K.; Takechi, M.; Momota, Y.; Yuasa, T.; Tatehara, S.; Nagayama, M.; Yamauchi, E. Effect of the Additional Installation of Implants in the Posterior Region on the Prognosis of Treatment in the Edentulous Mandibular Jaw. Clin Oral Implants Res 2003, 14, 727–733. [Google Scholar] [CrossRef] [PubMed]
- Hobkirk, J.A.; Schwab, J. Mandibular Deformation in Subjects with Osseointegrated Implants. Int J Oral Maxillofac Implants 1991, 6, 319–328. [Google Scholar] [PubMed]
- Horiuchi, M.; Ichikawa, T.; Noda, M.; Matsumoto, N. Use of Interimplant Displacement to Measure Mandibular Distortion during Jaw Movements in Humans. Arch Oral Biol 1997, 42, 185–188. [Google Scholar] [CrossRef] [PubMed]
- Paez, C.Y.; Barco, T.; Roushdy, S.; Andres, C. Split-Frame Implant Prosthesis Designed to Compensate for Mandibular Flexure: A Clinical Report. J Prosthet Dent 2003, 89, 341–343. [Google Scholar] [CrossRef]
- Custodio, W.; Gomes, S.G.F.; Faot, F.; Garcia, R.C.M.R.; Del Bel Cury, A.A. Occlusal Force, Electromyographic Activity of Masticatory Muscles and Mandibular Flexure of Subjects with Different Facial Types. J Appl Oral Sci 2011, 19, 343–349. [Google Scholar] [CrossRef] [PubMed]
- Chen, D.C.; Lai, Y.L.; Chi, L.Y.; Lee, S.Y. Contributing Factors of Mandibular Deformation during Mouth Opening. J Dent 2000, 28, 583–588. [Google Scholar] [CrossRef] [PubMed]
- Favot, L.-M.; Berry-Kromer, V.; Haboussi, M.; Thiebaud, F.; Ben Zineb, T. Numerical Study of the Influence of Material Parameters on the Mechanical Behaviour of a Rehabilitated Edentulous Mandible. Journal of Dentistry 2014, 42, 287–297. [Google Scholar] [CrossRef]
- Alvarez-Arenal, A.; Lasheras, F.S.; Fernández, E.M.; González, I. A Jaw Model for the Study of the Mandibular Flexure Taking into Account the Anisotropy of the Bone. Mathematical and Computer Modelling 2009, 50, 695–704. [Google Scholar] [CrossRef]
- Shinkai, R.S.; Lazzari, F.L.; Canabarro, S.A.; Gomes, M.; Grossi, M.L.; Hirakata, L.M.; Mota, E.G. Maximum Occlusal Force and Medial Mandibular Flexure in Relation to Vertical Facial Pattern: A Cross-Sectional Study. Head Face Med 2007, 3, 18. [Google Scholar] [CrossRef]
- Prasad, M.; Hussain, M.Z.; Shetty, S.K.; Kumar, T.A.; Khaur, M.; George, S.A.; Dalwai, S. Median Mandibular Flexure at Different Mouth Opening and Its Relation to Different Facial Types: A Prospective Clinical Study. J Nat Sci Biol Med 2013, 4, 426–430. [Google Scholar] [CrossRef]
- Scandurra, C.; Gasparro, R.; Dolce, P.; Bochicchio, V.; Muzii, B.; Sammartino, G.; Marenzi, G.; Maldonato, N.M. The Role of Cognitive and Non-Cognitive Factors in Dental Anxiety: A Mediation Model. Eur J Oral Sci 2021, 129, e12793. [Google Scholar] [CrossRef]
- de Oliveira, R.M.; Emtiaz, S. Mandibular Flexure and Dental Implants: A Case Report. Implant Dent 2000, 9, 90–95. [Google Scholar] [CrossRef] [PubMed]
- Law, C.; Bennani, V.; Lyons, K.; Swain, M. Mandibular Flexure and Its Significance on Implant Fixed Prostheses: A Review. J Prosthodont 2012, 21, 219–224. [Google Scholar] [CrossRef] [PubMed]
- Marin, D.O.M.; Dias, K. de C.; Paleari, A.G.; Pero, A.C.; Arioli Filho, J.N.; Compagnoni, M.A. Split-Framework in Mandibular Implant-Supported Prosthesis. Case Rep Dent 2015, 2015, 502394. [CrossRef]
- Sivaraman, K.; Chopra, A.; Venkatesh, S.B. Clinical Importance of Median Mandibular Flexure in Oral Rehabilitation: A Review. J Oral Rehabil 2016, 43, 215–225. [Google Scholar] [CrossRef]
- Mijiritsky, E.; Shacham, M.; Meilik, Y.; Dekel-Steinkeller, M. Clinical Influence of Mandibular Flexure on Oral Rehabilitation: Narrative Review. Int J Environ Res Public Health 2022, 19, 16748. [Google Scholar] [CrossRef]
- A Quantitative Analysis of the Decrease in Width of the Mandibular Arch during Forced Movements of the Mandible - James A. McDowell, Carl P. Regli, 1961. Available online: https://journals.sagepub.com/doi/abs/10.1177/00220345610400061201 (accessed on 20 May 2023).
- Osborne, J. Tomlin Medial Convergence of the Mandible. Br. Dental J. 1964, 117, 112–114. [Google Scholar]
- Burch, J.G.; Borchers, G. Method for Study of Mandibular Arch Width Change. J Dent Res 1970, 49, 463. [Google Scholar] [CrossRef] [PubMed]
- Novak, C.A. Mandibular Dimensional Change in the Various Jaw Positions and Its Effect upon Prosthetic Appliances. Dent Stud 1972, 50, 19. [Google Scholar] [PubMed]
- Fischman, B.M. The Influence of Fixed Splints on Mandibular Flexure. J Prosthet Dent 1976, 35, 643–647. [Google Scholar] [CrossRef] [PubMed]
- Ferrario, V.; Sforza, C. Biomechanical Model of the Human Mandible: A Hypothesis Involving Stabilizing Activity of the Superior Belly of Lateral Pterygoid Muscle. J Prosthet Dent 1992, 68, 829–835. [Google Scholar] [CrossRef] [PubMed]
- Hart, R.T.; Hennebel, V.V.; Thongpreda, N.; Van Buskirk, W.C.; Anderson, R.C. Modeling the Biomechanics of the Mandible: A Three-Dimensional Finite Element Study. J Biomech 1992, 25, 261–286. [Google Scholar] [CrossRef]
- Korioth, T.W.P.; Romilly, D.P.; Hannam, A.G. Three-Dimensional Finite Element Stress Analysis of the Dentate Human Mandible. American Journal of Physical Anthropology 1992, 88, 69–96. [Google Scholar] [CrossRef]
- Koolstra, J.H.; van Eijden, T.M. Biomechanical Analysis of Jaw-Closing Movements. J Dent Res 1995, 74, 1564–1570. [Google Scholar] [CrossRef]
- Abdel-Latif, H.H.; Hobkirk, J.A.; Kelleway, J.P. Functional Mandibular Deformation in Edentulous Subjects Treated with Dental Implants. Int J Prosthodont 2000, 13, 513–519. [Google Scholar]
- Kemkes-Grottenthaler, A.; Löbig, F.; Stock, F. Mandibular Ramus Flexure and Gonial Eversion as Morphologic Indicators of Sex. Homo 2002, 53, 97–111. [Google Scholar] [CrossRef]
- Jiang, T.; Ai, M. In Vivo Mandibular Elastic Deformation during Clenching on Pivots. J Oral Rehabil 2002, 29, 201–208. [Google Scholar] [CrossRef]
- Zarone, F.; Apicella, A.; Nicolais, L.; Aversa, R.; Sorrentino, R. Mandibular Flexure and Stress Build-up in Mandibular Full-Arch Fixed Prostheses Supported by Osseointegrated Implants. Clin Oral Implants Res 2003, 14, 103–114. [Google Scholar] [CrossRef]
- Choi, A.H.; Ben-Nissan, B.; Conway, R.C. Three-Dimensional Modelling and Finite Element Analysis of the Human Mandible during Clenching. Aust Dent J 2005, 50, 42–48. [Google Scholar] [CrossRef] [PubMed]
- Balci, Y.; Yavuz, M.F.; Cağdir, S. Predictive Accuracy of Sexing the Mandible by Ramus Flexure. Homo 2005, 55, 229–237. [Google Scholar] [CrossRef]
- Yokoyama, S.; Wakabayashi, N.; Shiota, M.; Ohyama, T. Stress Analysis in Edentulous Mandibular Bone Supporting Implant-Retained 1-Piece or Multiple Superstructures. Int J Oral Maxillofac Implants 2005, 20, 578–583. [Google Scholar]
- Al-Sukhun, J.; Helenius, M.; Lindqvist, C.; Kelleway, J. Biomechanics of the Mandible Part I: Measurement of Mandibular Functional Deformation Using Custom-Fabricated Displacement Transducers. J Oral Maxillofac Surg 2006, 64, 1015–1022. [Google Scholar] [CrossRef] [PubMed]
- Al-Sukhun, J.; Kelleway, J. Biomechanics of the Mandible: Part II. Development of a 3-Dimensional Finite Element Model to Study Mandibular Functional Deformation in Subjects Treated with Dental Implants. Int J Oral Maxillofac Implants 2007, 22, 455–466. [Google Scholar] [PubMed]
- El-Sheikh, A.M.; Abdel-Latif, H.H.; Howell, P.G.; Hobkirk, J.A. Midline Mandibular Deformation during Nonmasticatory Functional Movements in Edentulous Subjects with Dental Implants. Int J Oral Maxillofac Implants 2007, 22, 243–248. [Google Scholar]
- Gulsahi, A.; Yüzügüllü, B.; Imirzalioglu, P.; Genç, Y. Assessment of Panoramic Radiomorphometric Indices in Turkish Patients of Different Age Groups, Gender and Dental Status. Dentomaxillofac Radiol 2008, 37, 288–292. [Google Scholar] [CrossRef]
- Naini, R.B.; Nokar, S. Three-Dimensional Finite Element Analysis of the Effect of 1-Piece Superstructure on Mandibular Flexure. Implant Dent 2009, 18, 428–437. [Google Scholar] [CrossRef]
- Bellini, C.M.; Romeo, D.; Galbusera, F.; Taschieri, S.; Raimondi, M.T.; Zampelis, A.; Francetti, L. Comparison of Tilted versus Nontilted Implant-Supported Prosthetic Designs for the Restoration of the Edentuous Mandible: A Biomechanical Study. Int J Oral Maxillofac Implants 2009, 24, 511–517. [Google Scholar]
- Nokar, S.; Baghai Naini, R. The Effect of Superstructure Design on Stress Distribution in Peri-Implant Bone during Mandibular Flexure. Int J Oral Maxillofac Implants 2010, 25, 31–37. [Google Scholar] [PubMed]
- Zaugg, B.; Hämmerle, C.H.F.; Palla, S.; Gallo, L.M. Implant-Supported Mandibular Splinting Affects Temporomandibular Joint Biomechanics. Clin Oral Implants Res 2012, 23, 897–901. [Google Scholar] [CrossRef] [PubMed]
- Madani, A.S.; Asadzadeh, N.; Hosseini, S.H. Mandibular Flexure in Anterior-Posterior and Transverse Plane on Edentulous Patients in Mashhad Faculty of Dentistry. Journal of Dental Materials and Techniques 2012, 1, 24–28. [Google Scholar] [CrossRef]
- Law, C.; Bennani, V.; Lyons, K.; Swain, M. Influence of Implant Framework and Mandibular Flexure on the Strain Distribution on a Kennedy Class II Mandible Restored with a Long-Span Implant Fixed Restoration: A Pilot Study. J Prosthet Dent 2014, 112, 31–37. [Google Scholar] [CrossRef] [PubMed]
- Lin, C.; Jiao, B.; Liu, S.; Guan, F.; Chung, N.-E.; Han, S.-H.; Lee, U.-Y. Sex Determination from the Mandibular Ramus Flexure of Koreans by Discrimination Function Analysis Using Three-Dimensional Mandible Models. Forensic Sci Int 2014, 236, 191.e1-6. [Google Scholar] [CrossRef]
- Martin-Fernandez, E.; Gonzalez-Gonzalez, I.; deLlanos-Lanchares, H.; Mauvezin-Quevedo, M.A.; Brizuela-Velasco, A.; Alvarez-Arenal, A. Mandibular Flexure and Peri-Implant Bone Stress Distribution on an Implant-Supported Fixed Full-Arch Mandibular Prosthesis: 3D Finite Element Analysis. Biomed Res Int 2018, 2018, 8241313. [Google Scholar] [CrossRef]
- Shahriari, S.; Parandakh, A.; Khani, M.-M.; Azadikhah, N.; Naraghi, P.; Aeinevand, M.; Nikkhoo, M.; Khojasteh, A. The Effect of Mandibular Flexure on Stress Distribution in the All-on-4 Treated Edentulous Mandible: A Comparative Finite-Element Study Based on Mechanostat Theory. J Long Term Eff Med Implants 2019, 29, 79–86. [Google Scholar] [CrossRef]
- Wolf, L.; Bergauer, B.; Adler, W.; Wichmann, M.; Matta, R.E. Three-Dimensional Evaluation of Mandibular Deformation during Mouth Opening. Int J Comput Dent 2019, 22, 21–27. [Google Scholar]
- Tulsani, M.; Maiti, S.; Rupawat, D. Evaluation of Change In Mandibular Width During Maximum Mouth Opening and Protrusion. International Journal of Dentistry and Oral Science 2020. [Google Scholar] [CrossRef]
- Ebadian, B.; Abolhasani, M.; Heidarpour, A.; Ziaei, M.; Jowkar, M. Assessment of the Relationship between Maximum Occlusal Force and Median Mandibular Flexure in Adults: A Clinical Trial Study. J Indian Prosthodont Soc 2020, 20, 76–82. [Google Scholar] [CrossRef]
- Schmidt, A.; Klussmann, L.; Schlenz, M.A.; Wöstmann, B. Elastic Deformation of the Mandibular Jaw Revisited-a Clinical Comparison between Digital and Conventional Impressions Using a Reference. Clin Oral Investig 2021, 25, 4635–4642. [Google Scholar] [CrossRef]
- Gülsoy, M.; Tuna, S.H.; Pekkan, G. Evaluation of Median Mandibular Flexure Values in Dentulous and Edentulous Subjects by Using an Intraoral Digital Scanner. J Adv Prosthodont 2022, 14, 32–44. [Google Scholar] [CrossRef]
- Gao, J.; Li, X.; He, J.; Jiang, L.; Zhao, B. The Effect of Mandibular Flexure on the Design of Implant-Supported Fixed Restorations of Different Facial Types under Two Loading Conditions by Three-Dimensional Finite Element Analysis. Front Bioeng Biotechnol 2022, 10, 928656. [Google Scholar] [CrossRef]
- Asadzadeh, N.; Madani, A.S.; Mirmortazavi, A.; Sabooni, M.R.; Shibani, V. Mandibular Width and Length Deformation during Mouth Opening in Female Dental Students. Journal of Applied Sciences 2012, 12, 1865–1868. [Google Scholar] [CrossRef]
- Choi, A.H.; Conway, R.C.; Taraschi, V.; Ben-Nissan, B. Biomechanics and Functional Distortion of the Human Mandible. J Investig Clin Dent 2015, 6, 241–251. [Google Scholar] [CrossRef]
- Abu Alhaija, E.S.J.; Al Zo’ubi, I.A.; Al Rousan, M.E.; Hammad, M.M. Maximum Occlusal Bite Forces in Jordanian Individuals with Different Dentofacial Vertical Skeletal Patterns. Eur J Orthod 2010, 32, 71–77. [Google Scholar] [CrossRef]
- Sella Tunis, T.; May, H.; Sarig, R.; Vardimon, A.D.; Hershkovitz, I.; Shpack, N. Are Chin and Symphysis Morphology Facial Type-Dependent? A Computed Tomography-Based Study. Am J Orthod Dentofacial Orthop 2021, 160, 84–93. [Google Scholar] [CrossRef]
- Dahlin, D.C. Bone and Bones. Fundamentals of Bone Biology. American Journal of Clinical Pathology 1956, 26, 179. [Google Scholar] [CrossRef]
- Picton, D.C. Distortion of the Jaws during Biting. Arch Oral Biol 1962, 7, 573–580. [Google Scholar] [CrossRef]
- Standlee, J.P.; Caputo, A.A.; Ralph, J.P. Stress Trajectories within the Mandible under Occlusal Loads. J Dent Res 1977, 56, 1297–1302. [Google Scholar] [CrossRef]
- Mongini, F.; Calderale, P.M.; Barberi, G. Relationship between Structure and the Stress Pattern in the Human Mandible. J Dent Res 1979, 58, 2334–2337. [Google Scholar] [CrossRef]
- Ralph, J.P.; Caputo, A.A. Analysis of Stress Patterns in the Human Mandible. J Dent Res 1975, 54, 814–821. [Google Scholar] [CrossRef]
- Clelland, N.L.; Lee, J.K.; Bimbenet, O.C.; Brantley, W.A. A Three-Dimensional Finite Element Stress Analysis of Angled Abutments for an Implant Placed in the Anterior Maxilla. J Prosthodont 1995, 4, 95–100. [Google Scholar] [CrossRef]
- Brunski, J.B. Biomechanical Factors Affecting the Bone-Dental Implant Interface. Clin Mater 1992, 10, 153–201. [Google Scholar] [CrossRef]
- Cochran, D.L. The Scientific Basis for and Clinical Experiences with Straumann Implants Including the ITI Dental Implant System: A Consensus Report. Clin Oral Implants Res 2000, 11 (Suppl. S1), 33–58. [Google Scholar] [CrossRef] [PubMed]
- Quaas, S.; Rudolph, H.; Luthardt, R.G. Direct Mechanical Data Acquisition of Dental Impressions for the Manufacturing of CAD/CAM Restorations. J Dent 2007, 35, 903–908. [Google Scholar] [CrossRef] [PubMed]
- Flügge, T.V.; Schlager, S.; Nelson, K.; Nahles, S.; Metzger, M.C. Precision of Intraoral Digital Dental Impressions with ITero and Extraoral Digitization with the ITero and a Model Scanner. Am J Orthod Dentofacial Orthop 2013, 144, 471–478. [Google Scholar] [CrossRef] [PubMed]
- Anh, J.-W.; Park, J.-M.; Chun, Y.-S.; Kim, M.; Kim, M. A Comparison of the Precision of Three-Dimensional Images Acquired by 2 Digital Intraoral Scanners: Effects of Tooth Irregularity and Scanning Direction. Korean J Orthod 2016, 46, 3–12. [Google Scholar] [CrossRef] [PubMed]
- Tallgren, A. The Continuing Reduction of the Residual Alveolar Ridges in Complete Denture Wearers: A Mixed-Longitudinal Study Covering 25 Years. J Prosthet Dent 1972, 27, 120–132. [Google Scholar] [CrossRef] [PubMed]
- Atkinson, P.J.; Woodhead, C. Changes in Human Mandibular Structure with Age. Arch Oral Biol 1968, 13, 1453–1464. [Google Scholar] [CrossRef]
- D Ambrosio, F.; Caggiano, M.; Acerra, A.; Pisano, M.; Giordano, F. Is Ozone a Valid Adjuvant Therapy for Periodontitis and Peri-Implantitis? A Systematic Review. J Pers Med 2023, 13, 646. [Google Scholar] [CrossRef] [PubMed]
- Yang, H.S.; Lang, L.A.; Felton, D.A. Finite Element Stress Analysis on the Effect of Splinting in Fixed Partial Dentures. J Prosthet Dent 1999, 81, 721–728. [Google Scholar] [CrossRef]
- Watanabe, F.; Uno, I.; Hata, Y.; Neuendorff, G.; Kirsch, A. Analysis of Stress Distribution in a Screw-Retained Implant Prosthesis. Int J Oral Maxillofac Implants 2000, 15, 209–218. [Google Scholar]
- Torsello, F.; di Torresanto, V.M.; Ercoli, C.; Cordaro, L. Evaluation of the Marginal Precision of One-Piece Complete Arch Titanium Frameworks Fabricated Using Five Different Methods for Implant-Supported Restorations. Clin Oral Implants Res 2008, 19, 772–779. [Google Scholar] [CrossRef] [PubMed]
- Lindquist, L.W.; Rockler, B.; Carlsson, G.E. Bone Resorption around Fixtures in Edentulous Patients Treated with Mandibular Fixed Tissue-Integrated Prostheses. J Prosthet Dent 1988, 59, 59–63. [Google Scholar] [CrossRef] [PubMed]
- Korioth, T.W.; Johann, A.R. Influence of Mandibular Superstructure Shape on Implant Stresses during Simulated Posterior Biting. J Prosthet Dent 1999, 82, 67–72. [Google Scholar] [CrossRef]
- Suedam, V.; Souza, E.A.C.; Moura, M.S.; Jacques, L.B.; Rubo, J.H. Effect of Abutment’s Height and Framework Alloy on the Load Distribution of Mandibular Cantilevered Implant-Supported Prosthesis. Clin Oral Implants Res 2009, 20, 196–200. [Google Scholar] [CrossRef]
- Skalak, R. Biomechanical Considerations in Osseointegrated Prostheses. J Prosthet Dent 1983, 49, 843–848. [Google Scholar] [CrossRef]
- Itoh, H.; Caputo, A.A.; Kuroe, T.; Nakahara, H. Biomechanical Comparison of Straight and Staggered Implant Placement Configurations. Int J Periodontics Restorative Dent 2004, 24, 47–55. [Google Scholar] [CrossRef]
- McCartney, J.W. Cantilever Rests: An Alternative to the Unsupported Distal Cantilever of Osseointegrated Implant-Supported Prostheses for the Edentulous Mandible. J Prosthet Dent 1992, 68, 817–819. [Google Scholar] [CrossRef]
- Jemt, T. In Vivo Measurements of Precision of Fit Involving Implant-Supported Prostheses in the Edentulous Jaw. Int J Oral Maxillofac Implants 1996, 11, 151–158. [Google Scholar] [PubMed]
- Schmidt, A.; Wöstmann, B.; Schlenz, M.A. Accuracy of Digital Implant Impressions in Clinical Studies: A Systematic Review. Clin Oral Implants Res 2022, 33, 573–585. [Google Scholar] [CrossRef] [PubMed]
- Bra-nemark, P.-I.; Zarb, G.A.; Albrektsson, T.; Rosen, H.M. Tissue-Integrated Prostheses. Osseointegration in Clinical Dentistry. Plastic and Reconstructive Surgery 1986, 77, 496. [Google Scholar] [CrossRef]
- Maló, P.; Rangert, B.; Nobre, M. “All-on-Four” Immediate-Function Concept with Brånemark System Implants for Completely Edentulous Mandibles: A Retrospective Clinical Study. Clin Implant Dent Relat Res 2003, 5 (Suppl. S1), 2–9. [Google Scholar] [CrossRef] [PubMed]
- Apicella, A.; Masi, E.; Nicolais, L.; Zarone, F.; de Rosa, N.; Valletta, G. A Finite-Element Model Study of Occlusal Schemes in Full-Arch Implant Restoration. J Mater Sci Mater Med 1998, 9, 191–196. [Google Scholar] [CrossRef]
- Tashkandi, E.A.; Lang, B.R.; Edge, M.J. Analysis of Strain at Selected Bone Sites of a Cantilevered Implant-Supported Prosthesis. J Prosthet Dent 1996, 76, 158–164. [Google Scholar] [CrossRef]
- van Zyl, P.P.; Grundling, N.L.; Jooste, C.H.; Terblanche, E. Three-Dimensional Finite Element Model of a Human Mandible Incorporating Six Osseointegrated Implants for Stress Analysis of Mandibular Cantilever Prostheses. Int J Oral Maxillofac Implants 1995, 10, 51–57. [Google Scholar]
- Shackleton, J.L.; Carr, L.; Slabbert, J.C.; Becker, P.J. Survival of Fixed Implant-Supported Prostheses Related to Cantilever Lengths. J Prosthet Dent 1994, 71, 23–26. [Google Scholar] [CrossRef]
- White, S.N.; Caputo, A.A.; Anderkvist, T. Effect of Cantilever Length on Stress Transfer by Implant-Supported Prostheses. J Prosthet Dent 1994, 71, 493–499. [Google Scholar] [CrossRef]
- Naert, I.; Quirynen, M.; van Steenberghe, D.; Darius, P. A Study of 589 Consecutive Implants Supporting Complete Fixed Prostheses. Part II: Prosthetic Aspects. J Prosthet Dent 1992, 68, 949–956. [Google Scholar] [CrossRef]
- Fenton, A.H.; Zarb, G.A. Research Status of Prosthodontic Procedures. Int J Prosthodont 1993, 6, 137–144. [Google Scholar] [PubMed]
- Agliardi, E.L.; Francetti, L.; Romeo, D.; Del Fabbro, M. Immediate Rehabilitation of the Edentulous Maxilla: Preliminary Results of a Single-Cohort Prospective Study. Int J Oral Maxillofac Implants 2009, 24, 887–895. [Google Scholar] [PubMed]
Figure 1.
PRISMA flowchart depicting the article selection process.
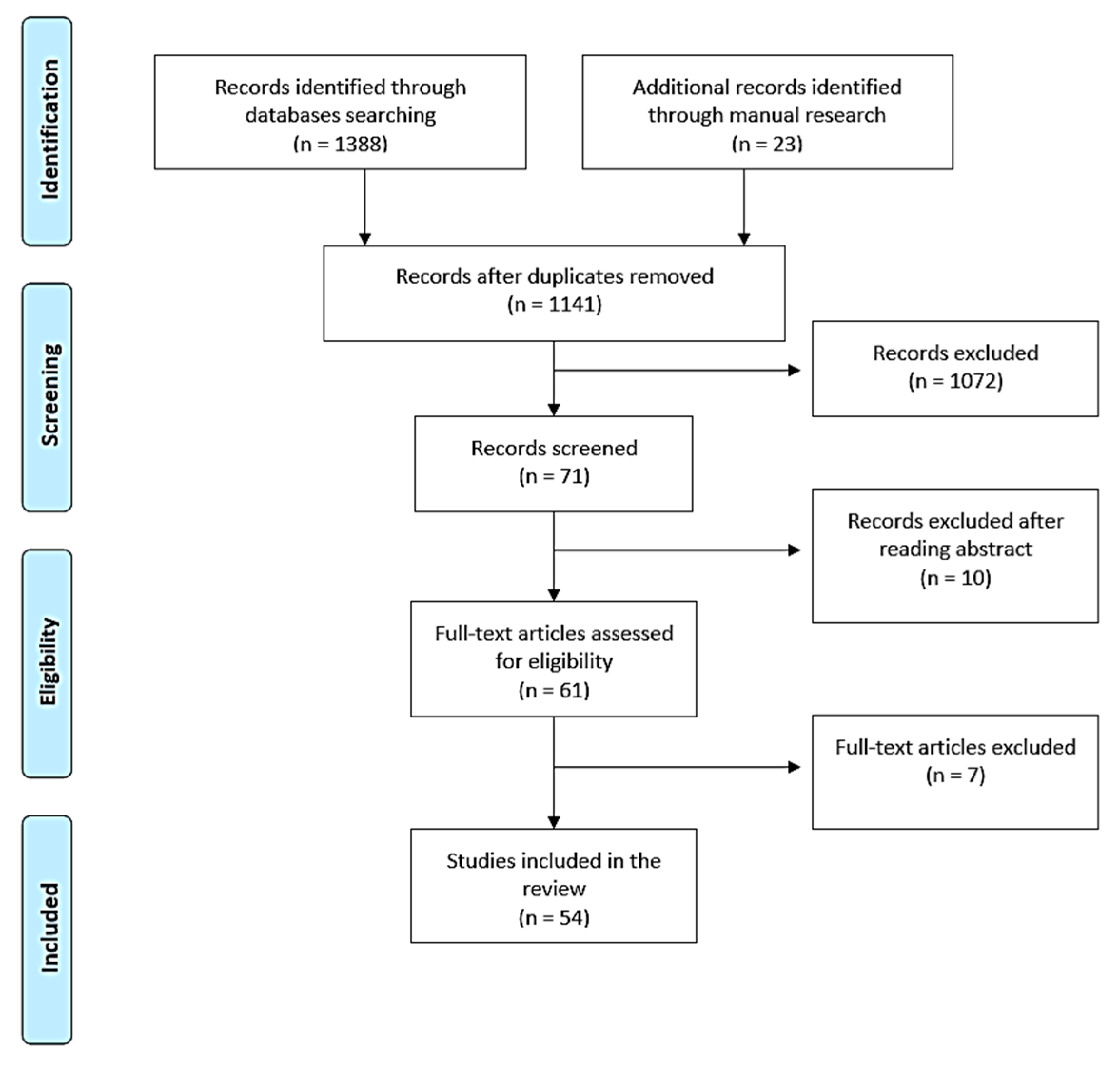

Table 1.
Studies excluded along with reasons for exclusion.
| Author, year of publication and reference | Reason for exclusion |
|---|---|
| Van Eijden TM, 2000 [8] | It’s a review |
| de Oliveira RM, 2000 [36] | It’s a case report |
| Paez CY, 2003 [28] | It’s a case report |
| Law C, 2012 [37] | It’s a review |
| Marin DO, 2015 [38] | It’s a case report |
| Sivaraman K, 2016 [39] | It’s a review |
| Mijiritsky E, 2022 [40] | It’s a narrative review |
Table 2.
Characteristics of the studies included in the present systematic review: author, year of publication and reference; journal of publication; study design; outcome. Mandibular flexion (MF).
Table 2.
Characteristics of the studies included in the present systematic review: author, year of publication and reference; journal of publication; study design; outcome. Mandibular flexion (MF).
| Author, year of publication and reference | Journal of publication | Study design | Outcome |
|---|---|---|---|
| McDowell JA, 1961 [41] | Journal of Dental Research | Clinical trial | Influence of mandibular movements on MF values |
| Osborne J, 1964 [42] | Br Dent J | Clinical trial | MF measurement |
| Regli CP, 1967 [10] | J Prosthet Dent. | Clinical trial | MF measurement |
| Burch JG, 1970 [43] | J Dent Res. | Clinical trial | Influence of mandibular movements and individual factors on MF values |
| Novak CA, 1972 [44] | Dent Stud. | Clinical trial | MF measurement |
| Burch JG, 1972 [1] | Arch Oral Biol. | Clinical trial | Influence of mandibular movements on MF values |
| Goodkind RJ, 1973 [9] | J Prosthet Dent. | Clinical trial | MF measurement |
| De Marco TJ, 1974 [14] | J Prosthet Dent. | Clinical trial | MF measurement |
| Fischman BM, 1976 [45] | J Prosthet Dent. | Clinical trial | MF reduces when fixed splints are present in natural dentition |
| Gates GN, 1981 [6] | J Prosthet Dent. | Clinical trial | Influence of mandibular movements on MF values |
| Omar R, 1981 [11] | J Oral Rehabil. | Clinical trial | Influence of MF on impression-taking |
| Hylander WL, 1984 [7] | Am. J. Phys. Anthropol. | Clinical trial | Influence of individual factors on MF values |
| Fischman B, 1990 [15] | J Prosthet Dent. | Clinical trial | MF measurement |
| Hobkirk JA, 1991 [26] | Int J Oral Maxillofac Implants | Clinical trial | Influence of individual factors on MF values |
| Ferrario V, 1992 [46] | J Prosthet Dent. | Clinical trial | Influence of individual factors on MF values |
| Hart RT, 1992 [47] | Journal of Biomechanics | Clinical trial | Influence of individual factors on MF values |
| Korioth TW, 1992 [48] | Am J Phys Anthropol | Clinical trial | Influence of individual factors on MF values |
| Koolstra JH, 1995 [49] | J Dent Res. | Clinical trial | Influence of individual factors on MF values |
| Horiuchi M, 1997 [27] | Arch Oral Biol. | Clinical trial | Influence of mandibular movements on MF values |
| Hobkirk JA, 1998 [23] | The Journal of Prosthetic Dentistry | Clinical trial | Influence of individual factors on MF values |
| Chen DC, 2000 [30] | J Dent. | Clinical trial | Influence of individual factors on MF values |
| Abdel-Latif HH, 2000 [50] | Int J Prosthodont. | Clinical trial | MF measurement |
| Kemkes-Grottenthaler A, 2002 [51] | Homo | Clinical trial | Influence of individual factors on MF values |
| Jiang T, 2002 [52] | J Oral Rehabil. | Clinical trial | Influence of MF on connected prosthesis supported by natural tooth and implants |
| Zarone F, 2003 [53] | Clin Oral Implants Res. | Clinical trial | Influence of MF on implants and superstructures in different fixed full-arch rehabilitations |
| Shinkai R, 2004 [17] | Journal of Applied Oral Science | Clinical trial | Influence of individual factors on MF values |
| Choi AH, 2005 [54] | Aust Dent J. | Clinical trial | Influence of mandibular movements on MF values |
| Balci Y, 2005 [55] | Homo | Clinical trial | Influence of individual factors on MF values |
| Yokoyama S, 2005 [56] | Int J Oral Maxillofac Implants | Clinical trial | Influence of MF on different superstructures in fixed full-arch rehabilitations |
| Canabarro Sde A, 2006 [12] | Int J Prosthodont. | Clinical trial | Influence of mandibular movements and individual factors on MF values |
| Al-Sukhun J, 2006 [57] | J Oral Maxillofac Surg. | Clinical trial | Influence of mandibular movements on MF values |
| Al-Sukhun J, 2007 [58] | Int J Oral Maxillofac Implants. | Clinical trial | Influence of mandibular movements on MF values |
| Shinkai RS, 2007 [33] | Head Face Med. | Clinical trial | Influence of individual factors on MF values |
| El-Sheikh AM, 2007 [59] | Int J Oral Maxillofac Implants | Clinical trial | Influence of mandibular movements on MF values |
| Gulsahi A, 2008 [60] | Dentomaxillofac Radiol. | Clinical trial | Influence of individual factors on MF values |
| Alvarez-Arenal A, 2009 [32] | Mathematical and Computer Modelling | Clinical trial | Influence of mandibular movements and individual factors on MF values |
| Naini RB, 2009 [61] | Implant Dent | Clinical trial | Influence of MF on different superstructures in fixed full-arch rehabilitations |
| Bellini CM, 2009 [62] | Int J Oral Maxillofac Implants | Clinical trial | Influence of MF on tilted and nontilted implant |
| Nokar S, 2010 [63] | Int J Oral Maxillofac Implants | Clinical trial | Influence of MF on different superstructures in fixed full-arch rehabilitations |
| Custodio W, 2011 [29] | J Appl Oral Sci. | Clinical trial | Influence of individual factors on MF values |
| Zaugg B, 2012 [64] | Clinical Oral Implants Research | Clinical trial | MF values in oral rehabilitation with posterior implants and natural teeth in anterior mandible |
| Madani AS, 2012 [65] | Journal of Dental Materials and Techniques | Clinical trial | Influence of individual factors on MF values |
| Prasad M, 2013 [34] | J Nat Sci Biol Med. | Clinical trial | Influence of individual factors on MF values |
| Law C, 2014 [66] | J Prosthet Dent. | Clinical trial | Influence of MF on the strain distribution in unilateral distal edentulisms |
| Lin C, 2014 [67] | Forensic Sci Int. | Clinical trial | Influence of individual factors on MF values |
| Favot LM, 2014 [31] | J Dent. | Clinical trial | MF values with different superstructure’s material and cortical bone thickness |
| Martin-Fernandez E, 2018 [68] | Biomed Res Int. | Clinical trial | Influence of superstructure type and different mandibular movements on MF in fixed implant rehabilitations |
| Shahriari S, 2019 [69] | J Long Term Eff Med Implants | Clinical trial | Influence of MF on tilted and nontilted implant |
| Wolf L, 2019 [70] | Int J Comput Dent. | Clinical trial | Influence of mandibular movements and individual factors on MF values |
| Tulsani M, 2020 [71] | International Journal of Dentistry and Oral Science | Clinical trial | Influence of mandibular movements on MF values |
| Ebadian B, 2020 [72] | J Indian Prosthodont Soc. | Clinical trial | Influence of individual factors on MF values |
| Schmidt A, 2021 [73] | Clin Oral Investig. | Clinical trial | Influence of MF on different techniques of impression-taking |
| Gülsoy M, 2022 [74] | J Adv Prosthodont. | Clinical trial | Influence of individual factors on MF values |
| Gao J, 2022 [75] | Front Bioeng Biotechnol. | Clinical trial | Influence of individual factors on MF values |
Table 3.
Summary of studies included in the current review regarding the existence of significant correlation (+) or not (-) between MF (Mandibular Flexion) and individual factors*. * Age, sex, facial type, gonial angle, length of the mandibular structure, symphysis characteristics, MOF (Maximum Occlusal Force) and parameters that modify it (height, weight, BMI, muscle pain, bruxism, and tooth wear).
Table 3.
Summary of studies included in the current review regarding the existence of significant correlation (+) or not (-) between MF (Mandibular Flexion) and individual factors*. * Age, sex, facial type, gonial angle, length of the mandibular structure, symphysis characteristics, MOF (Maximum Occlusal Force) and parameters that modify it (height, weight, BMI, muscle pain, bruxism, and tooth wear).
| Author, year of publication and reference | Type of rehabilitation | Sample size | Correlation between MF and individual factors* |
|---|---|---|---|
| Burch JG, 1970 [43] | Natural dentition | 10 | Age + |
| Hylander WL, 1984 [7] | Natural dentition | 6 macaca fascicularis | Symphysis characteristics + |
| Hobkirk JA, 1991 [26] | Natural dentition | 3 | Facial type + Symphysis characteristics + |
| Ferrario V, 1992 [46] | Natural dentition | 3D FEM | Age + |
| Hart RT, 1992 [47] | Natural dentition | 3D FEM | Age + |
| Korioth TW, 1992 [48] | Natural dentition | 3D FEM | Age + |
| Koolstra JH, 1995 [49] | Natural dentition | 3D FEM | Age + |
| Hobkirk JA, 1998 [23] | Natural dentition | 3 | Facial type + |
| Chen DC, 2000 [30] | Natural dentition | 62 | Facial type + Gonial angle + Symphysis characteristics + Sex – MOF and parameters that modify it - |
| Kemkes-Grottenthaler A, 2002 [51] | Forensic mandibles and archaeological mandibles | 153 forensic mandibles and 80 archaeological mandibles | Sex + |
| Shinkai R, 2004 [17] | Natural dentition | 7 | Symphysis characteristics + |
| Balci Y, 2005 [55] | Forensic mandibles | 120 mandibles from forensic cases | Sex + |
| Canabarro Sde A, 2006 [12] | Natural dentition | 80 | Gonial angle + Length of the mandibular structure + Sex – Age - MOF and parameters that modify it - |
| Shinkai RS, 2007 [33] | Natural dentition | 51 | Facial type – Sex + MOF and parameters that modify it - |
| Gulsahi A, 2008 [60] | Edentulous, partially and full dentate patients | 1.863 | Sex + |
| Custodio W, 2011 [29] | Natural dentition | 78 | Facial type + |
| Madani AS, 2012 [65] | Natural dentition and edentulous | 50 and 70 | Age - |
| Prasad M, 2013 [34] | Natural dentition | 60 | Facial type + Sex - |
| Lin C, 2014 [67] | Natural dentition | 3D FEM | Sex + |
| Wolf L, 2019 [70] | Natural dentition | 40 | Sex - |
| Ebadian B, 2020 [72] | Natural dentition | 90 | Age + Sex – MOF and parameters that modify it - |
| Gülsoy M, 2022 [74] | Natural dentition and edentulous | 56 and 35 | Age - Sex - |
| Gao J, 2022 [75] | Implant-supported fixed restorations | 3D FEM | Facial type + |
Table 4.
Summary of studies included in the current review regarding the values of MMF according to different types of mandibular movements*. *Mouth opening, protrusion, and lateral movements.
Table 4.
Summary of studies included in the current review regarding the values of MMF according to different types of mandibular movements*. *Mouth opening, protrusion, and lateral movements.
| Author, year of publication and reference | Type of rehabilitation | Sample size | Type of movement* and values of MMF |
|---|---|---|---|
| McDowell JA, 1961 [41] | Natural dentition | 20 | Mouth opening 0.4 mm Protrusion 0.5 mm |
| Osborne J, 1964 [42] | Natural dentition | 18 | Mouth opening 0.07 mm |
| Regli CP, 1967 [10] | Natural dentition | 62 | Mouth opening 0.03-0.09 mm |
| Burch JG, 1970 [43] | Natural dentition | 10 | Mouth opening 0.438 mm Protrusion 0.61 mm Lateral movements 0.243/0.257 mm |
| Novak CA, 1972 [44] | Natural dentition | 50 | Mouth opening 1.00 mm |
| Burch JG, 1972 [1] | Natural dentition | 25 | Mouth opening 0.224 mm Protrusion 0.432 mm Lateral movements 0.112/0.105 mm |
| Goodkind RJ, 1973 [9] | Natural dentition | 40 | Mouth opening 0.031-0.076 mm |
| De Marco TJ, 1974 [14] | Natural dentition | 25 | Mouth opening 0.78 mm |
| Gates GN, 1981 [6] | Natural dentition | 10 | Mouth opening 0-0.3 mm Protrusion 0.1-0.5 mm |
| Omar R, 1981 [11] | Natural dentition | 10 | Mouth opening 0.012-0.164 mm |
| Fischman B, 1990 [15] | Natural dentition | 10 | Mouth opening 0.0711 mm |
| Horiuchi M, 1997 [27] | Natural dentition | 4 | Mouth opening 0.016 mm Protrusion 0.010-0.037 mm |
| Chen DC, 2000 [30] | Natural dentition | 62 | Mouth opening 0.145 mm |
| Shinkai R, 2004 [17] | Natural dentition | 7 |
Mouth opening 0.21-0.44 mm |
| Choi AH, 2005 [54] | Edentulous mandible with implants | 3D FEM | Mouth opening 0.168 mm in the first molar region and 0.256 mm in the second molar region |
| Canabarro Sde A, 2006 [12] | Natural dentition | 80 | Mouth opening 0.146 mm Protrusion 0.15 mm |
| Al-Sukhun J, 2006 [57] | Edentulous patients with implants | 12 | Mouth opening 0.011–0.052 mm Protrusion 0.025-0.057 mm |
| Al-Sukhun J, 2007 [58] | Edentulous patients with implants | 12 | Mouth opening 0.8 mm Protrusion 1.07 mm Lateral movements 1.1/0.9 mm |
| El-Sheikh AM, 2007 [59] | Edentulous patients with implants | 5 | Mouth opening 0.025-0.042 mm Protrusion 0.018-0.053 mm Lateral movements 0.010-0.021 mm |
| Madani AS, 2012 [65] | Natural dentition and edentulous | 50 and 70 | Mouth opening 0.078-0.751 mm |
| Wolf L, 2019 [70] | Natural dentition | 40 | Mouth opening 0.011-0.232 mm |
| Tulsani M, 2020 [71] | Natural dentition | 140 | Mouth opening 0.363 mm Protrusion 0.973 mm |
Table 5.
Summary of studies included in the current review regarding different type of superstructure of full-arch implant-supported rehabilitation. 1 D: division of the superstructure; U: undivided framework.
Table 5.
Summary of studies included in the current review regarding different type of superstructure of full-arch implant-supported rehabilitation. 1 D: division of the superstructure; U: undivided framework.
| Author, year of publication and reference | Type of rehabilitation | Sample size | Results in favour of D/U1 |
|---|---|---|---|
| Zarone F, 2003 [53] | Full-arch 6-implants-supported rehabilitation | 1 | D |
| Naini RB, 2009 [61] | Full-arch 5-implants-supported rehabilitation | 3D FEM | D |
| Nokar S, 2010 [63] | Full-arch 6-implants-supported rehabilitation | 3D FEM | D |
| Yokoyama S, 2005 [56] | Full-arch 8-implants-supported rehabilitation | 3D FEM | U |
| Martin-Fernandez E, 2018 [68] | Full-arch 6-implants-supported rehabilitation | 3D FEM | U |
| Gao J, 2022 [75] | Full-arch implants-supported rehabilitation | 3D FEM | U |
Table 6.
Risk of bias of the studies included in the systematic review. The response options for the bias are: Yes (Y), Probably yes (PY), Probably no (PN), No (N) and No information (NI). “Y” indicate low risk of bias, PY indicate a moderate risk of bias; PN indicate a serious risk, N indicate a critical risk of bias and NI indicate that are no informations.
Table 6.
Risk of bias of the studies included in the systematic review. The response options for the bias are: Yes (Y), Probably yes (PY), Probably no (PN), No (N) and No information (NI). “Y” indicate low risk of bias, PY indicate a moderate risk of bias; PN indicate a serious risk, N indicate a critical risk of bias and NI indicate that are no informations.
| Studies | Bias due to confounding |
Bias in selection of participants | Bias in measurement classification of interventions | Bias due to deviations from intended interventions |
Bias due to missing data | Bias in measurement of outcomes | Bias due to selection of the reported result |
|---|---|---|---|---|---|---|---|
| McDowell JA, 1961 [41] | Y / PY / PN / N |
Y / PY / PN / N/ NI |
Y / PY / PN / N/ NI |
Y / PY / PN / N/ NI |
Y / PY / PN / N/ NI |
Y / PY / PN / N/ NI |
Y / PY / PN / N/ NI |
| Osborne J, 1964 [42] | Y/ PY / PN / N |
Y / PY / PN / N/ NI |
Y / PY / PN / N/ NI |
Y / PY / PN / N/ NI |
Y / PY / PN / N/ NI |
Y / PY / PN / N/ NI |
Y / PY / PN / N/ NI |
| Regli CP, 1967 [10] | Y / PY / PN /N |
Y / PY / PN /N/ NI |
Y / PY / PN / N/ NI |
Y / PY / PN / N/ NI |
Y / PY / PN / N/ NI |
Y / PY / PN / N/ NI |
Y / PY / PN / N/ NI |
| Burch JG, 1970 [43] | Y / PY / PN / N |
Y / PY / PN/N/NI |
Y / PY / PN / N/ NI |
Y / PY / PN / N/ NI |
Y / PY / PN / N/ NI |
Y / PY / PN / N/ NI |
Y / PY / PN / N/ NI |
| Novak CA, 1972 [44] | Y / PY / PN / N |
Y / PY / PN / N/ NI |
Y / PY / PN / N/ NI |
Y / PY / PN / N/ NI |
Y / PY / PN / N/ NI |
Y / PY / PN / N/ NI |
Y / PY / PN / N/ NI |
| Burch JG, 1972 [1] | Y / PY / PN / N |
Y / PY / PN / N/ NI |
Y / PY / PN / N/ NI |
Y / PY / PN / N/ NI |
Y / PY / PN / N/ NI |
Y / PY / PN / N/ NI |
Y / PY / PN / N/ NI |
| Goodkind RJ, 1973 [9] | Y / PY / PN / N |
Y / PY / PN / N/ NI |
Y / PY / PN / N/ NI |
Y / PY / PN / N/ NI |
Y / PY / PN / N/ NI |
Y / PY / PN / N/ NI |
Y / PY / PN / N/ NI |
| De Marco TJ, 1974 [14] | Y / PY / PN / N |
Y / PY / PN / N/ NI |
Y / PY / PN / N/ NI |
Y / PY / PN / N/ NI |
Y / PY / PN / N/ NI |
Y / PY / PN / N/ NI |
Y / PY / PN / N/ NI |
| Fischman BM, 1976 [45] | Y / PY / PN / N |
Y / PY / PN / N/ NI |
Y / PY / PN / N/ NI |
Y / PY / PN / N/ NI |
Y / PY / PN / N/ NI |
Y / PY / PN / N/ NI |
Y / PY / PN / N/ NI |
| Gates GN, 1981 [6] | Y / PY / PN / N |
Y / PY / PN / N/ NI |
Y / PY / PN / N/ NI |
Y / PY / PN / N/ NI |
Y / PY / PN / N/ NI |
Y / PY / PN / N/ NI |
Y / PY / PN / N/ NI |
| Omar R, 1981 [11] | Y / PY / PN / N |
Y / PY / PN / N/ NI |
Y / PY / PN / N/ NI |
Y / PY / PN / N/ NI |
Y / PY / PN / N/ NI |
Y / PY / PN / N/ NI |
Y / PY / PN / N/ NI |
| Hylander WL, 1984 [7] | Y / PY / PN / N |
Y / PY / PN / N/ NI |
Y / PY / PN / N/ NI |
Y / PY / PN / N/ NI |
Y / PY / PN / N/ NI |
Y / PY / PN / N/ NI |
Y / PY / PN / N/ NI |
| Fischman B, 1990 [15] | Y / PY / PN / N |
Y / PY / PN / N/ NI |
Y / PY / PN / N/ NI |
Y / PY / PN / N/ NI |
Y / PY / PN / N/ NI |
Y / PY / PN / N/ NI |
Y / PY / PN / N/ NI |
| Hobkirk JA, 1991 [26] | Y / PY / PN / N |
Y / PY / PN / N/ NI |
Y / PY / PN / N/ NI |
Y / PY / PN / N/ NI |
Y / PY / PN / N/ NI |
Y / PY / PN / N/ NI |
Y / PY / PN / N/ NI |
| Ferrario V, 1992 [46] | Y / PY / PN / N |
Y / PY / PN / N/ NI |
Y / PY / PN / N/ NI |
Y / PY / PN / N/ NI |
Y / PY / PN / N/ NI |
Y / PY / PN / N/ NI |
Y / PY / PN / N/ NI |
| Hart RT, 1992 [47] | Y / PY / PN / N |
Y / PY / PN / N/ NI |
Y / PY / PN / N/ NI |
Y / PY / PN / N/ NI |
Y / PY / PN / N/ NI |
Y / PY / PN / N/ NI |
Y / PY / PN / N/ NI |
| Korioth TW, 1992 [48] | Y / PY / PN / N |
Y / PY / PN / N/ NI |
Y / PY / PN / N/ NI |
Y / PY / PN / N/ NI |
Y / PY / PN / N/ NI |
Y / PY / PN / N/ NI |
Y / PY / PN / N/ NI |
| Koolstra JH, 1995 [49] | Y / PY / PN / N |
Y / PY / PN / N/ NI |
Y / PY / PN / N/ NI |
Y / PY / PN / N/ NI |
Y / PY / PN / N/ NI |
Y / PY / PN / N/ NI |
Y / PY / PN / N/ NI |
| Horiuchi M, 1997 [27] | Y / PY / PN / N |
Y / PY / PN / N/ NI |
Y / PY / PN / N/ NI |
Y / PY / PN / N/ NI |
Y / PY / PN / N/ NI |
Y / PY / PN / N/ NI |
Y / PY / PN / N/ NI |
| Hobkirk JA, 1998 [23] | Y / PY / PN / N |
Y / PY / PN / N/ NI |
Y / PY / PN / N/ NI |
Y / PY / PN / N/ NI |
Y / PY / PN / N/ NI |
Y / PY / PN / N/ NI |
Y / PY / PN / N/ NI |
| Chen DC, 2000 [30] | Y / PY / PN / N |
Y / PY / PN / N/ NI |
Y / PY / PN / N/ NI |
Y / PY / PN / N/ NI |
Y / PY / PN / N/ NI |
Y / PY / PN / N/ NI |
Y / PY / PN / N/ NI |
| Abdel-Latif HH, 2000 [50] | Y / PY / PN / N |
Y / PY / PN / N/ NI |
Y / PY / PN / N/ NI |
Y / PY / PN / N/ NI |
Y / PY / PN / N/ NI |
Y / PY / PN / N/ NI |
Y / PY / PN / N/ NI |
| Kemkes-Grottenthaler A, 2002 [51] | Y / PY / PN / N |
Y / PY / PN / N/ NI |
Y / PY / PN / N/ NI |
Y / PY / PN / N/ NI |
Y / PY / PN / N/ NI |
Y / PY / PN / N/ NI |
Y / PY / PN / N/ NI |
| Jiang T, 2002 [52] | Y / PY / PN / N |
Y / PY / PN / N/ NI |
Y / PY / PN / N/ NI |
Y / PY / PN / N/ NI |
Y / PY / PN / N/ NI |
Y / PY / PN / N/ NI |
Y / PY / PN / N/ NI |
| Zarone F, 2003 [53] | Y / PY / PN / N |
Y / PY / PN / N/ NI |
Y / PY / PN / N/ NI |
Y / PY / PN / N/ NI |
Y / PY / PN / N/ NI |
Y / PY / PN / N/ NI |
Y / PY / PN / N/ NI |
| Shinkai R, 2004 [17] | Y / PY / PN / N |
Y / PY / PN / N/ NI |
Y / PY / PN / N/ NI |
Y / PY / PN / N/ NI |
Y / PY / PN / N/ NI |
Y / PY / PN / N/ NI |
Y / PY / PN / N/ NI |
| Choi AH, 2005 [54] | Y / PY / PN / N |
Y / PY / PN / N/ NI |
Y / PY / PN / N/ NI |
Y / PY / PN / N/ NI |
Y / PY / PN / N/ NI |
Y / PY / PN / N/ NI |
Y / PY / PN / N/ NI |
| Balci Y, 2005 [55] | Y / PY / PN / N |
Y / PY / PN / N/ NI |
Y / PY / PN / N/ NI |
Y / PY / PN / N/ NI |
Y / PY / PN / N/ NI |
Y / PY / PN / N/ NI |
Y / PY / PN / N/ NI |
| Yokoyama S, 2005 [56] | Y / PY / PN / N |
Y / PY / PN / N/ NI |
Y / PY / PN / N/ NI |
Y / PY / PN / N/ NI |
Y / PY / PN / N/ NI |
Y / PY / PN / N/ NI |
Y / PY / PN / N/ NI |
| Canabarro Sde A, 2006 [12] | Y / PY / PN / N |
Y / PY / PN / N/ NI |
Y / PY / PN / N/ NI |
Y / PY / PN / N/ NI |
Y / PY / PN / N/ NI |
Y / PY / PN / N/ NI |
Y / PY / PN / N/ NI |
| Al-Sukhun J, 2006 [57] | Y / PY / PN / N |
Y / PY / PN / N/ NI |
Y / PY / PN / N/ NI |
Y / PY / PN / N/ NI |
Y / PY / PN / N/ NI |
Y / PY / PN / N/ NI |
Y / PY / PN / N/ NI |
| Al-Sukhun J, 2007 [58] | Y / PY / PN / N |
Y / PY / PN / N/ NI |
Y / PY / PN / N/ NI |
Y / PY / PN / N/ NI |
Y / PY / PN / N/ NI |
Y / PY / PN / N/ NI |
Y / PY / PN / N/ NI |
| Shinkai RS, 2007 [33] | Y / PY / PN / N |
Y / PY / PN / N/ NI |
Y / PY / PN / N/ NI |
Y / PY / PN / N/ NI |
Y / PY / PN / N/ NI |
Y / PY / PN / N/ NI |
Y / PY / PN / N/ NI |
| El-Sheikh AM, 2007 [59] | Y / PY / PN / N |
Y / PY / PN / N/ NI |
Y / PY / PN / N/ NI |
Y / PY / PN / N/ NI |
Y / PY / PN / N/ NI |
Y / PY / PN / N/ NI |
Y / PY / PN / N/ NI |
| Gulsahi A, 2008 [60] | Y / PY / PN / N |
Y / PY / PN / N/ NI |
Y / PY / PN / N/ NI |
Y / PY / PN / N/ NI |
Y / PY / PN / N/ NI |
Y / PY / PN / N/ NI |
Y / PY / PN / N/ NI |
| Alvarez-Arenal A, 2009 [32] | Y / PY / PN / N |
Y / PY / PN / N/ NI |
Y / PY / PN / N/ NI |
Y / PY / PN / N/ NI |
Y / PY / PN / N/ NI |
Y / PY / PN / N/ NI |
Y / PY / PN / N/ NI |
| Naini RB, 2009 [61] | Y / PY / PN / N |
Y / PY / PN / N/ NI |
Y / PY / PN / N/ NI |
Y / PY / PN / N/ NI |
Y / PY / PN / N/ NI |
Y / PY / PN / N/ NI |
Y / PY / PN / N/ NI |
| Bellini CM, 2009 [62] | Y / PY / PN / N |
Y / PY / PN / N/ NI |
Y / PY / PN / N/ NI |
Y / PY / PN / N/ NI |
Y / PY / PN / N/ NI |
Y / PY / PN / N/ NI |
Y / PY / PN / N/ NI |
| Nokar S, 2010 [63] | Y / PY / PN / N |
Y / PY / PN / N/ NI |
Y / PY / PN / N/ NI |
Y / PY / PN / N/ NI |
Y / PY / PN / N/ NI |
Y / PY / PN / N/ NI |
Y / PY / PN / N/ NI |
| Custodio W, 2011 [29] | Y / PY / PN / N |
Y / PY / PN / N/ NI |
Y / PY / PN / N/ NI |
Y / PY / PN / N/ NI |
Y / PY / PN / N/ NI |
Y / PY / PN / N/ NI |
Y / PY / PN / N/ NI |
| Zaugg B, 2012 [64] | Y / PY / PN / N |
Y / PY / PN / N/ NI |
Y / PY / PN / N/ NI |
Y / PY / PN / N/ NI |
Y / PY / PN / N/ NI |
Y / PY / PN / N/ NI |
Y / PY / PN / N/ NI |
| Madani AS, 2012 [65] | Y / PY / PN / N |
Y / PY / PN / N/ NI |
Y / PY / PN / N/ NI |
Y / PY / PN / N/ NI |
Y / PY / PN / N/ NI |
Y / PY / PN / N/ NI |
Y / PY / PN / N/ NI |
| Prasad M, 2013 [34] | Y / PY / PN / N |
Y / PY / PN / N/ NI |
Y / PY / PN / N/ NI |
Y / PY / PN / N/ NI |
Y / PY / PN / N/ NI |
Y / PY / PN / N/ NI |
Y / PY / PN / N/ NI |
| Law C, 2014 [66] | Y / PY / PN / N |
Y / PY / PN / N/ NI |
Y / PY / PN / N/ NI |
Y / PY / PN / N/ NI |
Y / PY / PN / N/ NI |
Y / PY / PN / N/ NI |
Y / PY / PN / N/ NI |
| Lin C, 2014 [67] | Y / PY / PN / N |
Y / PY / PN / N/ NI |
Y / PY / PN / N/ NI |
Y / PY / PN / N/ NI |
Y / PY / PN / N/ NI |
Y / PY / PN / N/ NI |
Y / PY / PN / N/ NI |
| Favot LM, 2014 [31] | Y / PY / PN / N |
Y / PY / PN / N/ NI |
Y / PY / PN / N/ NI |
Y / PY / PN / N/ NI |
Y / PY / PN / N/ NI |
Y / PY / PN / N/ NI |
Y / PY / PN / N/ NI |
| Martin-Fernandez E, 2018 [68] | Y / PY / PN / N |
Y / PY / PN / N/ NI |
Y / PY / PN / N/ NI |
Y / PY / PN / N/ NI |
Y / PY / PN / N/ NI |
Y / PY / PN / N/ NI |
Y / PY / PN / N/ NI |
| Shahriari S, 2019 [69] | Y / PY / PN / N |
Y / PY / PN / N/ NI |
Y / PY / PN / N/ NI |
Y / PY / PN / N/ NI |
Y / PY / PN / N/ NI |
Y / PY / PN / N/ NI |
Y / PY / PN / N/ NI |
| Wolf L, 2019 [70] | Y / PY / PN / N |
Y / PY / PN / N/ NI |
Y / PY / PN / N/ NI |
Y / PY / PN / N/ NI |
Y / PY / PN / N/ NI |
Y / PY / PN / N/ NI |
Y / PY / PN / N/ NI |
| Tulsani M, 2020 [71] | Y / PY / PN / N |
Y / PY / PN / N/ NI |
Y / PY / PN / N/ NI |
Y / PY / PN / N/ NI |
Y / PY / PN / N/ NI |
Y / PY / PN / N/ NI |
Y / PY / PN / N/ NI |
| Ebadian B, 2020 [72] | Y / PY / PN / N |
Y / PY / PN / N/ NI |
Y / PY / PN / N/ NI |
Y / PY / PN / N/ NI |
Y / PY / PN / N/ NI |
Y / PY / PN / N/ NI |
Y / PY / PN / N/ NI |
| Schmidt A, 2021 [73] | Y / PY / PN / N |
Y / PY / PN / N/ NI |
Y / PY / PN / N/ NI |
Y / PY / PN / N/ NI |
Y / PY / PN / N/ NI |
Y / PY / PN / N/ NI |
Y / PY / PN / N/ NI |
| Gülsoy M, 2022 [74] | Y / PY / PN / N |
Y / PY / PN / N/ NI |
Y / PY / PN / N/ NI |
Y / PY / PN / N/ NI |
Y / PY / PN / N/ NI |
Y / PY / PN / N/ NI |
Y / PY / PN / N/ NI |
| Gao J, 2022 [75] | Y / PY / PN / N |
Y / PY / PN / N/ NI |
Y / PY / PN / N/ NI |
Y / PY / PN / N/ NI |
Y / PY / PN / N/ NI |
Y / PY / PN / N/ NI |
Y / PY / PN / N/ NI |
| Risk of bias judgements | MODERATE | SERIOUS | MODERATE | LOW | MODERATE | MODERATE | MODERATE |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



