
Submitted:
10 July 2023
Posted:
11 July 2023
You are already at the latest version
Abstract
The aim of our study was to assess the relationship between the concentration/activity of salivary stress biomarkers (cortisol, α-amylase) and the psychological profile of patients with oral lichen planus (OLP) and primary burning mouth syndrome (BMS). A total of 160 subjects participated in this cross-sectional study: 60 patients with OLP; 60 patients with primary BMS; 40 control subjects. Unstimulated whole saliva (UWS) was collected between 9 and 10 am. Salivary biomarkers were analyzed by enzyme-linked immunosorbent assay (ELISA). Psychological assessment was evaluated with the Depression, Anxiety, and Stress Scale (DASS-21). Patients with primary BMS had higher salivary cortisol concentrations and α-amylase activity (0.52 vs. 0.44 µg/dl; 160531 vs. 145804 U/L) compared with patients with OLP. Patients with primary BMS had statistically significantly higher scores for depression, anxiety, and stress compared with patients with OLP and control subjects (p <0.001, Kruskal-Wallis test). There was a strong positive correlation between anxiety and depression, stress and depression, stress and anxiety in patients with OLP and BMS (p <0.001 and p <0.001, respectively). There was a good positive correlation between symptom intensity (pain/burning) and psychological profile (depression, anxiety, stress) in patients with primary BMS (r=0.373, p=0.003; r=0.515, p <0.001; r=0.365, p= 0.004, respectively). Patients with BMS show a stronger association with mental disorders compared to patients with OLP. However, an interdisciplinary psychoneuroimmunological approach is equally important in both patient groups (OLP and BMS), regardless of whether mental disorders are the cause or the consequence.
Keywords:
Alpha-Amylase
; Biomarkers
; Burning Mouth Syndrome
; Cortisol
; Oral Lichen Planus
; Saliva.
1. Introduction
Oral lichen planus (OLP) is considered a chronic inflammatory autoimmune disease of unknown etiology that has phases of remission and relapse. There is a genetic predisposition for the occurrence of this disease and evidence of human leukocyte antigen (HLA): A3, A8, B5, B7, B8. A number of possible triggers and contributing factors for OLP have been proposed: 1) local and systemic triggers of cell-mediated hypersensitivity; 2) stress; 3) autoimmune response to epithelial antigens; and 4) microorganisms [1]. The role of psychological stress is not clear, nor is the causal relationship between stress and the occurrence of OLP [2,3,4].
Burning mouth syndrome (BMS) is a complex chronic pain disorder characterized by spontaneous unpleasant sensations (burning, pain) of the clinically healthy oral mucosa, excluding all local and systemic causes [5]. The etiology is multifactorial and possible etiologic factors include: local, systemic, psychological, neurological, and idiopathic [6]. Psychological disorders are more frequently described in patients with BMS and may trigger the onset of the disease, although studies have not confirmed the cause-effect relationship [7,8,9,10,11]. It remains unclear whether psychological factors underlie BMS or are its consequence.
The measured concentration of salivary cortisol is an indicator of the level of free cortisol or biologically active cortisol in human serum [12]. It remains an open question whether the hypothalamic-pituitary-adrenal (HPA) axis is hyperactive or hypoactive in response to acute stress when a person is exposed to chronic stress. Studies show that regulation of the HPA axis is impaired in the context of psychopathology, as evidenced by decreased fluctuations in salivary cortisol production [13]. In addition to cortisol, the central nervous system (CNS), which produces catecholamines, epinephrine, and norepinephrine, also plays an important role in stressful situations. The CNS regulates the activity of salivary α-amylase [14]. There are few studies on the relationship between chronic psychological stress (e.g., depression) and salivary amylase levels. The results suggest that salivary amylase may be a useful indicator of physiological changes during long-term exposure to stressful circumstances [15].
Therefore, the aim of our study is to assess the relationship between the concentration/activity of salivary stress biomarkers (cortisol, α-amylase) and the psychological profile of patients with OLP and BMS.
2. Materials and Methods
2.1. Study design and subjects
A total of 160 subjects, divided into three groups, participated in this cross-sectional study: 60 patients with a clinically and histopathologically confirmed diagnosis of OLP; 60 patients diagnosed with primary BMS; 40 control subjects. The group of patients with OLP was composed of 40 patients with an erosive form of the disease and 20 patients with a non-erosive form. The control group consisted of randomly selected patients who came to the Department of Diagnostic Radiology, Dental Clinic Split, Split, Croatia. The study protocol was explained to each subject and after signing the informed consent form they were enrolled in the study. The study lasted two years and was conducted with the approval of the Ethics Committee of the Dental Clinic Split, the teaching base of the School of Medicine, Study of Dental Medicine, University of Split, Split, Croatia (approved on July 24, 2020) and the School of Dental Medicine, University of Zagreb, Zagreb, Croatia (05-PA-30-XIX-9/2020) (approved on September 10, 2020). The study was conducted in accordance with the principles of the Declaration of Helsinki (1964) and its subsequent amendments.
Medical history data, a list of medications, and disease duration (months) were obtained from all subjects. The same oral medicine specialist performed a clinical oral examination of all subjects and an incisional biopsy of the oral cavity mucosa in the patients with OLP. Local and systemic factors were removed in patients with primary BMS by determining whole saliva (sialometry test), complete blood count (CBC), serum iron (Fe), folic acid, vitamin B12, and blood glucose levels [16]. Blood pressure was measured in all subjects before participation in the study to exclude the possible influence of hypertension on the HPA axis and autonomic nervous system (ANS). Patients with inflammatory oral diseases (gingivitis, periodontitis) were also excluded from the study. All subjects who did not understand the nature and purpose of the study and the content of the informed consent form were excluded from the study.
Inclusion criteria for OLP was:
1. patients with a clinically and histopathologically confirmed diagnosis of OLP according to the modified WHO criteria [17].
The exclusion criteria for OLP were:
1. patients with long-term systemic diseases [diabetes mellitus (DM), cardiovascular disease (CVD), renal dysfunction, liver disease] and/or autoimmune diseases and/or cancer, pregnant women;
2. patients who have received corticosteroid, immunosuppressive, psychoactive therapy (anxiolytics, anticonvulsants, antidepressants) three months ago, hormone therapy;
3. patients with harmful habits such as betel nut or tobacco chewing and smoking;
4. cutaneous lichen planus (LP).
The five main inclusion criteria for primary BMS according to Scala A et al. were [18]:
1. a diffuse and usually bilateral burning sensation in the oral mucosa,
2. a constant and usually bilateral burning sensation that worsens during the day,
3. a burning sensation in the oral mucosa that has persisted for at least four to six months,
4. a burning sensation that does not interfere with the patient's sleep,
5. a burning sensation that does not worsen with eating and drinking, and possible relief of discomfort with eating and drinking.
The exclusion criteria for primary BMS were:
- Fe, folic acid, vitamin B12 deficiency; DM;
- treatment with antihypertensive drugs (ACE inhibitors), taking drugs with xerostomic effect or drugs that make the oral cavity susceptible to the development of oral candidiasis (corticosteroids, antibiotics), taking antineoplastic, psychoactive and neurological therapies in the last three months, hormone therapy;
- smoking;
- oral mucosal disease (candidiasis); head and neck cancer; head and neck radiation; thyroid, liver, and kidney disease; allergies; gastroesophageal reflux disease (GERD); Sjögren's disease (SjD); pregnant women; breastfeeding.
2.2. Saliva sampling
Three days before saliva collection, all subjects were asked to refrain from intense physical activity and mental stress. All subjects were asked to refrain from eating, drinking, and brushing their teeth 90 minutes before sampling. Unstimulated whole saliva (UWS) was collected between 9 and 10 am to avoid diurnal variation. The systematic review and meta-analysis by Fernández-Agra M et al. showed that studies in which both types of whole saliva [UWS and stimulated (SWS)] were collected yielded similar results in salivary biomarkers. They conclude that UWS is suitable for salivary biomarker detection and can serve as a reference for future studies [19]. UWS was collected from fertile women during the follicular phase of the menstrual cycle. Subjects were instructed to sit comfortably and tilt their head slightly forward. Immediately before collecting the saliva sample, all subjects rinsed their oral cavity with water to avoid contamination from other sources and then waited 10 minutes for the sample to be collected. They were instructed to swallow the saliva just before sampling began. Approximately 2.00 to 2.50 ml of saliva was collected from the subjects with OLP, BMS, and the control subjects in graduated tubes (Salivette) (ref. 51. 1534.500, SARSTEDT AG & Co. KG, Nümbrecht, Germany) using the "spit method.“ In the "spit method“, all subjects collected saliva in their mouths for 60 seconds and then spat it out into a graduated tube. The procedure was repeated for an additional 10 minutes. Subjects did not use any materials to stimulate secretion.
The samples were delivered to the Department of Medical Laboratory Diagnostics, Clinical Hospital Center Split, Split, Croatia, and then centrifuged at 1,500 x g for five minutes. The pad was then discarded in the infectious waste and the Salivettes were stored at -20°C until used for study purposes. The frozen samples were first stored at room temperature for 30 minutes to determine salivary cortisol concentration and salivary α-amylase activity. Then the samples were centrifuged at 1,500 x g for five minutes. Salivary cortisol concentration was analyzed by the immunochemical method of enzyme-linked immunosorbent assay (ELISA) using reagents from EUROIMMUN [Medizinische Labordiagnostika AG, Lübeck (Germany)]. The lower sensitivity limit of salivary cortisol concentration tested by the manufacturer is 0.15 ng/ml; linearity ranges from 0.10 to 28.30 ng/ml. The coefficient of variation in the series was 3.70; 4.20; 3.20 for the concentrations 0.60; 2.10; 13.40 ng/ml, and between series 9.70; 7.90; 4.70 for the concentrations 1.30; 2.80; 13.90 ng/ml. Saliva samples were analyzed using the Elysis Duo instrument (Human, Wiesbaden, Germany). Salivary α-amylase activity was measured by the kinetic colorimetric method on the Roche/Hitachi cobas c 701/702 Systems instrument with reagents from the same manufacturer.
After collection of UWS for analysis of salivary cortisol concentration, serum samples were taken from the subjects to exclude hypercortisolemia of other cause. Serum samples were collected one day after the collection of UWS to avoid the influence of the HPA axis on cortisol concentration during blood collection. The concentration of serum cortisol was measured by the immunochemical method of electrochemiluminescence (ECLIA) on the Roche/Hitachi cobas c e801 Systems instrument with reagents from the same manufacturer at the Department of Medical Laboratory Diagnostics, Clinical Hospital Center Split, Split, Croatia. The reference values for serum cortisol measured by this test are 171 - 536 nmol/L and refer to the morning test period.
2.3. Instruments
2.3.1. Visual Analogue Scale (VAS)
The VAS (from 0 to 100 mm) was used to assess the intensity of pain and/or burning (0 = no pain/burning, 100 = worst possible pain/burning) in patients with OLP and BMS.
2.3.2. Depression, Anxiety and Stress Scale (DASS-21)
The psychological evaluation of each subject was assessed with the Depression, Anxiety and Stress Scale (DASS-21 – Depression, Anxiety and Stress Scale, Lovibond & Lovibond, 1995a; Croatian adaptation Jokić-Begić, Jakšić, Ivezić and Surányi, 2012). The same researcher collected the data through interviews to ensure that all subjects understood each question correctly. The scale consists of 21 statements and has a three-factor structure in the original, consisting of the subscales Depression, Anxiety, and Stress, each containing seven statements. They attempt to assess three negative emotional states, i.e. the degree of depression, anxiety, and stress in the past week. The reliability coefficients for the above subscales are 0.90 for the depression subscale, 0.89 for the anxiety subscale, and 0.91 for the stress subscale. The items are formulated as statements that are rated on a four-point Likert scale. The scale ranges from 0 - does not apply to me at all, to 3 - applies to me almost completely or most of the time. The score for the subscales is calculated by adding the scores for the seven statements and multiplying by the number two. The maximum score for each subscale is 42, i.e. a higher score for each subscale means a higher level of depression, anxiety, and stress [22].
2.4. Statistical analysis
All statistical analyzes were performed with MedCalc software (MedCalc Software, Os-tend, Belgium, version 22.007.). All graphical figures were made using SigmaPlot for Windows® software (Systat Software Inc, San Jose, CA, USA, version 14.0). Quantitative data were presented as mean ± standard deviation or median and interquartile range (IQR), while qualitative data were presented as whole number and percentage. Normality of the distribution was estimated using the Kolmogorov–Smirnov test. Student’s t-test for independent samples and Mann–Whitney U test were used for comparison of quantitative variables between two groups. The chi-square (χ2) test was used for comparison of qualitative variables between groups. The correlations were estimated using Spearman correlation. The comparison of quantitative variables between three groups was performed using the one-way ANOVA with Scheffe’s post hoc test or the Kruskal-Wallis test with Dunn’s post hoc test. The level of statistical significance was set at p <0.05.
3. Results
3.1. Study subjects
The sample of OLP patients consisted of 60 subjects ranging in age from 22 to 86 years, median 63.0 (IQR 51.5 to 70.5). The sample of BMS patients consisted of 60 subjects aged 27 to 86 years, median 66.0 (IQR 57.0 to 72.0). The control group consisted of 40 subjects aged 41 to 80 years, median 61.0 (IQR 52.0 to 65.0). In all three groups, the majority of respondents were women (75.0% vs. 81.7% vs. 82.5%). There was no statistically significant difference between the groups in regard of age and gender (p=0.10, p=0.57) (Table 1).
Mean disease duration was 18.5 months (9.0-36.5) in patients with OLP, while it was 15.0 months (8.0-36.0) in patients with BMS (p=0.76, Mann-Whitney U test). Patients with primary BMS had statistically significantly higher VAS scores compared to patients with OLP (7.0 vs. 3.5) (p <0.001, Mann-Whitney U test).
3.2. Salivary biomarkers
Patients with primary BMS had higher salivary cortisol concentrations and α-amylase activity (0.52 vs. 0.44 µg/dl; 160531 vs. 145804 U/L) compared with patients with OLP. The concentration/activity of salivary cortisol and α-amylase showed no statistically significant difference between patients with OLP (N=60), patients with primary BMS (N=60) and control subjects (N=40) (p=0.31; p=0.54) (Figure 1 and Figure 2).
3.3. Psychological profile
Patients with primary BMS had statistically significantly higher scores for depression, anxiety, and stress compared with patients with OLP and control subjects (p <0.001, Kruskal-Wallis test) (Table 2). Stress was the leading mental disorder in patients with OLP and primary BMS, and stress scores were twice as high in patients with primary BMS as in patients with OLP. Patients with primary BMS had ten times higher depression scores compared to patients with OLP.
There was no correlation between the concentration/activity of salivary biomarkers (cortisol, α-amylase) and the psychological profile of patients with OLP and patients with primary BMS. There was a strong positive correlation between anxiety and depression (r=0.643, p <0.001), stress and depression (r=0.720, p <0.001), stress and anxiety (r=0.696, p <0.001) in patients with OLP (Table 3). There was a strong positive correlation between anxiety and depression (r=0.652, p <0.001), stress and depression (r=0.793, p <0.001), stress and anxiety (r=0.705, p <0.001) in patients with primary BMS (Table 4).
There was a positive correlation between disease duration and salivary cortisol concentration in patients with OLP (r=0.253, p=0.05). There was no correlation between disease duration and psychological profile in patients with OLP. There was no correlation between disease duration and concentration/activity of salivary biomarkers (cortisol, α-amylase) and psychological profile in patients with primary BMS (Table 5).
There was no correlation between symptom intensity (pain/burning) and concentration/activity of salivary biomarkers (cortisol, α-amylase) and psychological profile in patients with OLP. There was no correlation between symptom intensity (pain/burning) and the concentration/activity of salivary biomarkers (cortisol, α-amylase) in patients with primary BMS. There was a good positive correlation between symptom intensity (pain/burning) and psychological profile (depression, anxiety, stress) in patients with primary BMS (r=0.373, p=0.003; r=0.515, p <0.001; r=0.365, p= 0.004, respectively) (Table 6).
3.4. Erosive and non-erosive form of OLP
There was no difference in the concentration/activity of salivary stress biomarkers (cortisol, α-amylase) and the psychological profile of patients with erosive and non-erosive forms of OLP (Table 7).
4. Discussion
OLP and primary BMS are two oral diseases whose etiopathogenetic mechanism is complex and not fully elucidated, i.e. psychoneuroimmunoendocrinological. Therefore, in this study, we observed the concentration/activity of salivary stress biomarkers (cortisol, α-amylase) and the psychological profile of patients with OLP, patients with primary BMS and control subjects.
Salivary cortisol concentration showed no statistically significant difference between patients with OLP, patients with primary BMS, and control subjects (p=0.51). The results of the different studies on salivary cortisol concentration in patients with OLP are contradictory. The meta-analysis by Lopez-Jornet P et al. analyzed salivary cortisol concentrations in patients with OLP in six studies. All studies were of high quality (according to the Newcastle-Ottawa quality assessment scale). This meta-analysis showed a statistically significant difference in salivary cortisol concentrations (ELISA) in the Indian population of patients with OLP compared with control subjects (5.33 ng/ml, p <0.0001), but not in studies conducted in the Middle East and Europe [23]. A systematic review by Humberto JSM et al. included five studies that analyzed salivary cortisol concentrations (ELISA) in patients with OLP [24]. Three of them showed increased salivary cortisol concentrations in patients with OLP compared with control subjects [25,26,27]. Most studies in this systematic review had a low level of evidence and a weak level of recommendation (level 3b/grade B) [24]. Rödström PO et al., Girardi C et al., Nosratzehi T et al., and Pippi R et al. found no difference in salivary cortisol concentration between patients with OLP and control subjects [28,29,30,31]. Their findings are consistent with the results of our study. The absence of a difference in salivary cortisol concentration between patients with OLP and control subjects in our study may be explained by: ethnicity (Europe), different waking times of subjects, different timing of sample collection, and different diagnostic inclusion criteria of OLP. We made a small contribution to reducing bias by comparing only studies in which salivary cortisol concentration was determined by the ELISA technique.
In our study, there was no statistically significant difference in salivary cortisol concentration between patients with erosive and non-erosive forms of OLP (0.45 ± 0.31 vs. 0.41 ± 0.23 µg/dl, p=0.69). The study included twice as many patients with the erosive form of OLP compared to the non-erosive form. Our results are consistent with those of Lopez-Jornet P et al. and Mansourian A et al. who found no statistically significant difference in salivary cortisol concentration between the different clinical forms of OLP [32,33].
The etiology of primary BMS is multifactorial, and alteration of cortisol concentration is thought to play a possible role [34]. The results of the studies performed are contradictory. A systematic review by Aitken-Saavedra J et al. showed increased salivary cortisol concentrations in patients with primary BMS [35]. The systematic review and meta-analysis by Fernández-Agra M et al. included studies with low heterogeneity that analyzed 54 different biomarkers in patients with BMS. However, salivary cortisol was the only biomarker included in the meta-analysis and the results showed a statistically significant higher salivary cortisol concentration in patients with BMS compared to control subjects (mean 0.39, p=0.003) [19]. López-Jornet P et al., Nakagawa A et al., Nosratzehi T et al., and de Souza FTA et al. showed no statistically significant difference in salivary cortisol concentration between patients with primary BMS and control subjects [14,36,37,38]. Their results are consistent with the results of our study. The differences in the obtained results could be due to the different waking time of subjects (which we could not influence), different timing of sample collection, and different diagnostic inclusion criteria of BMS. The experts of the working group of the World Workshop in Oral Medicine VII pointed out the great heterogeneity of the definition and diagnostic criteria of BMS in clinical trials [39].
The absence of a statistically significant difference in salivary cortisol concentration between the three groups of subjects (patients with OLP, patients with primary BMS, control subjects) indicates impaired regulation of the HPA axis, i.e. its hypoactivity in these chronic diseases and painful conditions. Salivary cortisol concentration was higher in patients with OLP than in patients with BMS. In addition, there was a correlation between disease duration and salivary cortisol concentration in patients with OLP. This suggests a gradual recovery of the HPA axis and better adaptive coping mechanisms in stressful situations in patients with OLP compared with patients with BMS.
Salivary α-amylase activity showed no statistically significant difference between patients with OLP, patients with primary BMS and control subjects (p=0.81). There are few studies that have investigated salivary α-amylase activity in patients with OLP, and their results are contradictory. The results of the study by Simour JAdS et al. showed increased salivary α-amylase activity 30 minutes after awakening in patients with OLP (determined at three time points) [40]. Pippi R et al. showed no statistically significant difference in daily fluctuation and production of salivary α-amylase between patients with OLP and control subjects (determined at three time points) [14]. Their results are consistent with the results of our study. Moreover, there was no statistically significant difference in salivary α-amylase activity between patients with erosive and non-erosive forms of OLP in our study (100815 vs. 101035 U/L, p=0.55).
Most of the studies performed showed the association between salivary α-amylase and BMS. The systematic review by Aitken-Saavedra J et al. and the systematic review and meta-analysis by Fernández-Agra M et al. showed increased salivary α-amylase activity in patients with primary BMS [19,35]. Kim H-I et al. showed no difference in salivary α-amylase activity between patients with BMS and control subjects [41]. Their results are consistent with the results of our study. Discrepancies in the results of salivary α-amylase activity can be explained by the different wake-up times of the subjects and the different times of sample collection. The objective relationship between chronic stress and salivary α-amylase activity is still the subject of numerous studies. Because BMS belongs to chronic pain disorders, we did not demonstrate the association in our study. Salivary α-amylase activity was higher in patients with primary BMS compared with patients with OLP. This suggests that salivary α-amylase may be a better indicator of stress than salivary cortisol, which is also shown in the study by Nosratzehi T et al. [14].
Patients with primary BMS have a statistically significant worse psychological profile, i.e. higher scores for depression, anxiety, and stress compared with patients with OLP and control subjects (p <0.001). The results of the studies conducted on the association between psychological disorders and OLP are contradictory. Simoura JAdS et al. showed a significant correlation of depression, anxiety, stress, and OLP [40]. The systematic review and meta-analysis by De Porras-Carrique T et al. showed a strong association between OLP and mental disorders. It is important to note that this meta-analysis was of low methodological quality (according to AMSTAR2) [42]. Girardi C et al. did not find statistically significant higher stress scores between patients with OLP and control subjects [29]. Nevertheless, numerous studies support the association between OLP and mental disorders. This was also evident in our study, as depression, anxiety, and stress scores were higher in patients with OLP than in control subjects. There was no statistically significant difference in depression, anxiety and stress between patients with erosive and non-erosive forms of OLP (1.0 vs. 2.0, 3.0 vs. 5.0, 8.0 vs. 8.0, p=0.51, p=0.54, p=0.76, respectively). Our results are consistent with those of Shah B et al. and Ebrahimi H et al. [26,43].
Numerous studies have demonstrated a strong association between mental disorders and BMS. This was also confirmed by the results of our study. López-Jornet P et al., Koike K et al., de Pedro M et al. showed the association between depression, anxiety, stress and BMS [36,44,45]. Comparing the psychological profile of patients with OLP and primary BMS, we can conclude that the statistically significant higher scores of depression, anxiety, and stress in patients with primary BMS indicate a strong association between psychogenic factors and BMS. Patients with BMS had five times higher depression scores and two times higher stress scores compared with patients with OLP. Psychogenic factors are part of the multifactorial etiology of BMS. Discrepancies in the psychological profiles of patients with OLP and BMS can be explained by the use of different diagnostic tools to identify mental disorders and by the cultural differences of the subjects.
The results of our study suggest that depression, anxiety, and stress are a consequence of OLP rather than a cause (although this type of study cannot be determined). Disease duration showed no correlation with the psychological profile of patients with OLP and BMS. This indicates good adaptation mechanisms of these patients to chronic pain conditions. The results of our study showed no correlation between symptom intensity (pain/burning) and psychological profile in patients with OLP. In contrast, patients with primary BMS showed a good correlation between symptom intensity (pain/burning) and psychological profile, indicating a close relationship and a possible causal role. Because pain/burning symptoms are more prominent in patients with BMS, the DASS-21 could be an initial and useful tool for early detection of psychological disorders. Psychiatrists should be involved in diagnosing comorbidity in patients with OLP and primary BMS.
The advantage of our study is the sample size, which gives it strength. Our study is the first to compare the concentration/activity of salivary biomarkers in two oral psychoneuroimmunoendocrine diseases/disorders. Our study has several limitations. One of the limitations is that we determined the concentration/activity of salivary biomarkers at a single time point. In addition, the concentration/activity of salivary biomarkers was not corrected for the concentration of total proteins. One of the confounding factors is the different sensitivity of the kits, which certainly affected the results.
5. Conclusions
Salivary cortisol concentration and α-amylase activity were higher in patients with primary BMS than in patients with OLP. This suggests their importance as salivary stress biomarkers, considering the demonstrated stronger association between BMS and mental disorders. An interdisciplinary psychoneuroimmunological approach is necessary for chronic diseases/disorders such as OLP and BMS, as they are related to the psychological profile, regardless of whether mental disorders are a cause or a consequence.
References
- Lodi, G.; Scully, C.; Carrozzo, M.; Griffiths, M.; Sugerman, P.B.; Thongprasom, K. Current controversies in oral lichen planus: Report of an international consensus meeting. Part 2. Clinical management and malignant transformation. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 2005, 100, 164–178. [Google Scholar] [CrossRef] [PubMed]
- Rojo-Moreno, J.L.; Bagán, J.V.; Rojo-Moreno, J.; Donat, J.S.; Milián, M.A.; Jiménez, Y. Psychologic factors and oral lichen planus. A psychometric evaluation of 100 cases. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 1998, 86, 687–691. [Google Scholar] [CrossRef]
- McCartan, B.E. Psychological factors associated with oral lichen planus. J Oral Pathol Med 1995, 24, 273–275. [Google Scholar] [CrossRef] [PubMed]
- Eisen, D. The clinical features, malignant potential, and systemic associations of oral lichen planus: A study of 723 patients. J Am Acad Dermatol 2002, 46, 207–214. [Google Scholar] [CrossRef] [PubMed]
- Grushka, M.; Epstein, J.B.; Gorsky, M. Burning mouth syndrome. Am Fam Physician 2002, 65, 615–620. [Google Scholar]
- Kamala, K.A.; Sankethguddad, S.; Sujith, S.G.; Tantradi, P. Burning Mouth Syndrome. Indian J Palliat Care 2016, 22, 74–79. [Google Scholar] [CrossRef]
- Rogulj, A.A.; Richter, I.; Brailo, V.; Krstevski, I.; Boras, V.V. Catastrophizing in Patients with Burning Mouth Syndrome. Acta Stomatol Croat 2014, 48, 109–115. [Google Scholar] [PubMed]
- Scala, A.; Checchi, L.; Montevecchi, M.; Marini, I.; Giamberardino, M.A. Update on burning mouth syndrome: overview nad patient management. Crit Rev Oral Biol Med 2003, 14, 275–291. [Google Scholar] [CrossRef]
- Braud, A.; Boucher, Y. The relationship between the clinical features of idiopathic burning mouth syndrome and self-perceived quality of life. J Oral Sci 2016, 58, 475–481. [Google Scholar] [CrossRef]
- Davies, S.J.C.; Underhill, H.C.; Abdel-Karim, A.; Christmas, D.M.; Bolea-Alamanac, B.M.; Potokar, J.; Herrod, J.; Prime, S.S. Individual oral symptoms in burning mouth syndrome may be associated differentially with depression and anxiety. Acta Odontol Scand 2016, 74, 155–160. [Google Scholar] [CrossRef]
- Suarez, P.; Clark, G.T. Burning mouth syndrome: an update on diagnosis and treatment methods. J Calif Dent Assoc 2006, 34, 611–622. [Google Scholar] [CrossRef]
- Gaur, A.; Kumar, C.A.; Kumar, J.S.; Nair, G.K.R.; Agrawal, V.M. Estimation of Salivary Cortisol Level and Psychological Assessment in Patients with Oral Lichen Planus. J Indian Acad Oral Med Radiol 2018, 30, 14–17. [Google Scholar] [CrossRef]
- McEwen, B.S. Mood disorders and allostatic load. Biol Psychiatry 2003, 54, 200–207. [Google Scholar] [CrossRef]
- Nosratzehi, T.; Salimi, S.; Parvaee, A. Comparison of Salivary Cortisol and α-amylase Levels and Psychological Profiles in Patients with Burning Mouth Syndrome. Spec Care Dentist 2017, 37, 120–125. [Google Scholar] [CrossRef]
- Nater, U.M.; Rohleder, N. Salivary alpha-amylase as a non-invasive biomarker for the sympathetic nervous system: current state of research. Psychoneuroendocrinology 2009, 34, 486–496. [Google Scholar] [CrossRef] [PubMed]
- Wu-Wang, C.Y.; Patel, M.; Feng, J.; Milles, M.; Wang, S.L. Decreased levels of salivary prostaglandin E2 and epidermal growth factor in recurrent aphthous stomatitis. Arch Oral Biol 1995, 40, 1093–1098. [Google Scholar] [CrossRef] [PubMed]
- van der Meij, E.H.; van der Waal, I. Lack of clinicopathologic correlation in the diagnosis of oral lichen planus based on the presently available diagnostic criteria and suggestions for modifications. J Oral Pathol Med 2003, 32, 507–512. [Google Scholar] [CrossRef]
- Scala, A.; Checchi, L.; Montevecchi, M.; Marini, I.; Giamberardino, M.A. Update on burning mouth syndrome: overview nad patient management. Crit Rev Oral Biol Med 2003, 14, 275–291. [Google Scholar] [CrossRef]
- Fernández-Agra, M.; González-Serrano, J.; de Pedro, M.; Virto, L.; Caponio, V.C.A.; Ibáñez-Prieto, E.; Hernández, G.; López-Pintor, R.M. Salivary biomarkers in burning mouth syndrome: A systematic review and meta-analysis. Oral Dis 2022. Oral Dis Online ahead of print]. 2022. [Google Scholar] [CrossRef] [PubMed]
- Kang, J-H. ; Kho, H-S. Blood contamination in salivary diagnostics: Current methods and their limitations. Clin Chem Lab Med 2019, 57, 1115–1124. [Google Scholar] [CrossRef]
- Kamodyová, N.; Baňasová, L.; Janšáková, K.; Koborová, I.; Tóthová, Ľ.; Stanko, P.; Celec, P. Blood contamination in Saliva: Impact on the measurement of salivary oxidative stress markers. Dis Markers 2015, 2015, 479251. [Google Scholar] [CrossRef] [PubMed]
- Pačić-Turk, Lj.; Ćepulić, D-B.; Haramina, A.; Bošnjaković, J. The relationship of different psychological factors with the level of stress, anxiety and depression in health care workers during the COVID-19 pandemic in the Republic of Croatia. Suvremena psihologija 2020, 23, 35–53. [CrossRef]
- Lopez-Jornet, P.; Zavattaro, E.; Mozaffari, H.R.; Ramezani, M.; Sadeghi, M. Evaluation of the Salivary Level of Cortisol in Patients with Oral Lichen Planus: A Meta-Analysis. Medicina (Kaunas) 2019, 55, 213. [Google Scholar] [CrossRef] [PubMed]
- Humberto, J.S.M.; Pavanin, J.V.; da Rocha, M.J.A.; Motta, A.C.F. Cytokines, cortisol, and nitric oxide as salivary biomarkers in oral lichen planus: a systematic review. Braz Oral Res 2018, 32, e82. [Google Scholar] [CrossRef] [PubMed]
- Koray, M.; Dülger, O.; Ak, G.; Horasanli, S.; Uçok, A.; Tanyeri, H.; Badur, S. The evaluation of anxiety and salivary cortisol levels in patients with oral lichen planus. Oral Dis 2003, 9, 298–301. [Google Scholar] [CrossRef]
- Shah, B.; Ashok, L.; Sujatha, G.P. Evaluation of salivary cortisol and psychological factors in patients with oral lichen planus. Indian J Dent Res 2009, 20, 288–292. [Google Scholar] [CrossRef]
- Nadendla, L.K.; Meduri, V.; Paramkusam, G.; Pachava, K.R. Association of salivary cortisol and anxiety levels in lichen planus patients. J Clin Diagn Res 2014, 8, ZC01–03. [Google Scholar] [CrossRef] [PubMed]
- Rödström, P.O.; Jontell, M.; Hakeberg, M.; Berggren, U.; Lindstedt, G. Erosive oral lichen planus and salivary cortisol. J Oral Pathol Med 2001, 30, 257–263. [Google Scholar] [CrossRef] [PubMed]
- Girardi, C.; Luz, C.; Cherubini, K.; de Figueiredo, M.A.Z.; Nunes, M.L.T.; Salum, F.G. Salivary cortisol and dehydroepiandrosterone (DHEA) levels, psychological factors in patients with oral lichen planus. Arch Oral Biol 2011, 56, 864–868. [Google Scholar] [CrossRef]
- Nosratzehi, T.; Arbabi-Kalati, F.; Salimi, S.; Honarmand, E. The evaluation of psychological factor and salivary cortisol and IgA levels in patients with oral lichen planus. Zahedan J Res Med Sci 2014, 16, 31–34. [Google Scholar]
- Pippi, R.; Romeo, U.; Santoro, M.; Del Vecchio, A.; Scully, C.; Petti, S. Psychological disorders and oral lichen planus: matched case-control study and literature review. J Oral Dis 2016, 22, 226–234. [Google Scholar] [CrossRef]
- Lopez-Jornet, P.; Cayuela, C.A.; Tvarijonaviciute, A.; Parra-Perez, F.; Escribano, D.; Ceron, J. Oral lichen planus: salival biomarkers cortisol, immunoglobulin A, adiponectin. J Oral Pathol Med 2016, 45, 211–217. [Google Scholar] [CrossRef] [PubMed]
- Mansourian, A.; Najafi, S.; Nojoumi, N.; Parhami, P.; Moosavi, M-S. Salivary Cortisol and Salivary Flow Rate in Clinical Types of Oral Lichen Planus. Skinmed 2018, 16, 19–22. [Google Scholar] [PubMed]
- Jääskeläinen, SK. Pathophysiology of primary burning mouth syndrome. Clin Neurophysiol 2012, 123, 71–77. [Google Scholar] [CrossRef] [PubMed]
- Aitken-Saavedra, J.; Tarquinio, S.B.; Kinalski, M.; Haubman, D.; Martins, M.W.; Vasconcelos, A.C. Salivary characteristics in burning mouth syndrome: a systematic review. Minerva Dent Oral Sci 2022, 71, 233–241. [Google Scholar] [CrossRef]
- López-Jornet, P.; Camacho-Alonso, F.; Andujar-Mateos, M.P. Salivary cortisol, stress and quality of life in patients with burning mouth syndrome. J Eur Acad Dermatol Venereol 2009, 23, 1212–1213. [Google Scholar] [CrossRef]
- Nakagawa, A.; Yoshida, H.; Morita, S. Changes of salivary cortisol and chromogranin A levels in patients with burning mouth syndrome. J Osaka Dental Univ 2010, 44, 57–63. [Google Scholar]
- de Souza, F.T.A.; Kummer, A.; Silva, M.L.V.; Amaral, T.M.P.; Abdo, E.N.; Abreu, M.H.N.G.; Silva, T.A.; Teixeira, A.L. The association of openness personality trait with stress-related salivary biomarkers in burning mouth syndrome. Neuroimmunomodulation 2015, 22, 250–255. [Google Scholar] [CrossRef]
- Ariyawardana, A.; Chmieliauskaite, M.; Farag, A.M.; Albuquerque, R.; Forssell, H.; Nasri-Heir, C.; Klasser, G.D.; Sardella, A.; Mignogna, M.D.; Ingram, M.; Carlson, C.R.; Miller, C.S. World Workshop on Oral Medicine VII: Burning mouth syndrome: A systematic review of disease definitions and diagnostic criteria utilized in randomized clinical trials. Oral Dis 2019, 25 Suppl 1, 141–156. [Google Scholar] [CrossRef]
- Simoura, J.A.dS.; Pires, A.L.P.V.; Alves, L.D.B.; Arsati, F.; Lima-Arsati, Y.B.dO.; Dos Santos, J.N, Freitas, V.S. Psychological profile and α-amylase levels in oral lichen planus patients: A case-control preliminary study. Oral Dis 2023, 29, 1242–1249. [CrossRef]
- Kim, H-I.; Kim, Y-Y.; Chang, J-Y.; Ko, J-Y.; Kho, H-S. Salivary cortisol, 17β-estradiol, progesterone, dehydroepiandrosterone, and α-amylase in patients with burning mouth syndrome. Oral Dis 2012, 18, 613–620. [CrossRef]
- De Porras-Carrique, T.; González-Moles, M.A.; Warnakulasuriya, S.; Ramos-García, P. Depression, anxiety, and stress in oral lichen planus: a systematic review and meta-analysis. Clin Oral Investig 2022, 26, 1391–1408. [Google Scholar] [CrossRef] [PubMed]
- Ebrahimi, H.; Pourshahidi, S.; Tadbir, A.A. Evaluation of the Relationship between Oral Lichen Planus and Stress. J Dent (Shiraz) 2011, 12, 43–47. [Google Scholar]
- Koike, K.; Shinozaki, T.; Hara, K.; Noma, N.; Okada-Ogawa, A.; Asano, M.; Shinoda, M.; Eliav, E.; Gracely, R.H.; Iwata, K.; Imamura, Y. Immune and endocrine function in patients with burning mouth syndrome. Clin J Pain 2014, 30, 168–173. [Google Scholar] [CrossRef] [PubMed]
- de Pedro, M.; López-Pintor, R.M.; Casañas, E.; Hernández, G. Effects of photobiomodulation with low-level laser therapy in burning mouth syndrome: A randomized clinical trial. Oral Dis 2020, 26, 1764–1776. [Google Scholar] [CrossRef]
Figure 1.
Comparison of salivary cortisol concentration between patients with OLP (N=60), patients with primary BMS (N=60), and control subjects (N=40). * one-way analysis of variance (ANOVA) with post hoc Scheffe test. OLP: 0.44 ± 0.28; BMS: 0.52 ± 0.29; CONTROL: 0.44 ± 0.38. Abbreviations: BMS, burning mouth syndrome; OLP, oral lichen planus.
Figure 1.
Comparison of salivary cortisol concentration between patients with OLP (N=60), patients with primary BMS (N=60), and control subjects (N=40). * one-way analysis of variance (ANOVA) with post hoc Scheffe test. OLP: 0.44 ± 0.28; BMS: 0.52 ± 0.29; CONTROL: 0.44 ± 0.38. Abbreviations: BMS, burning mouth syndrome; OLP, oral lichen planus.
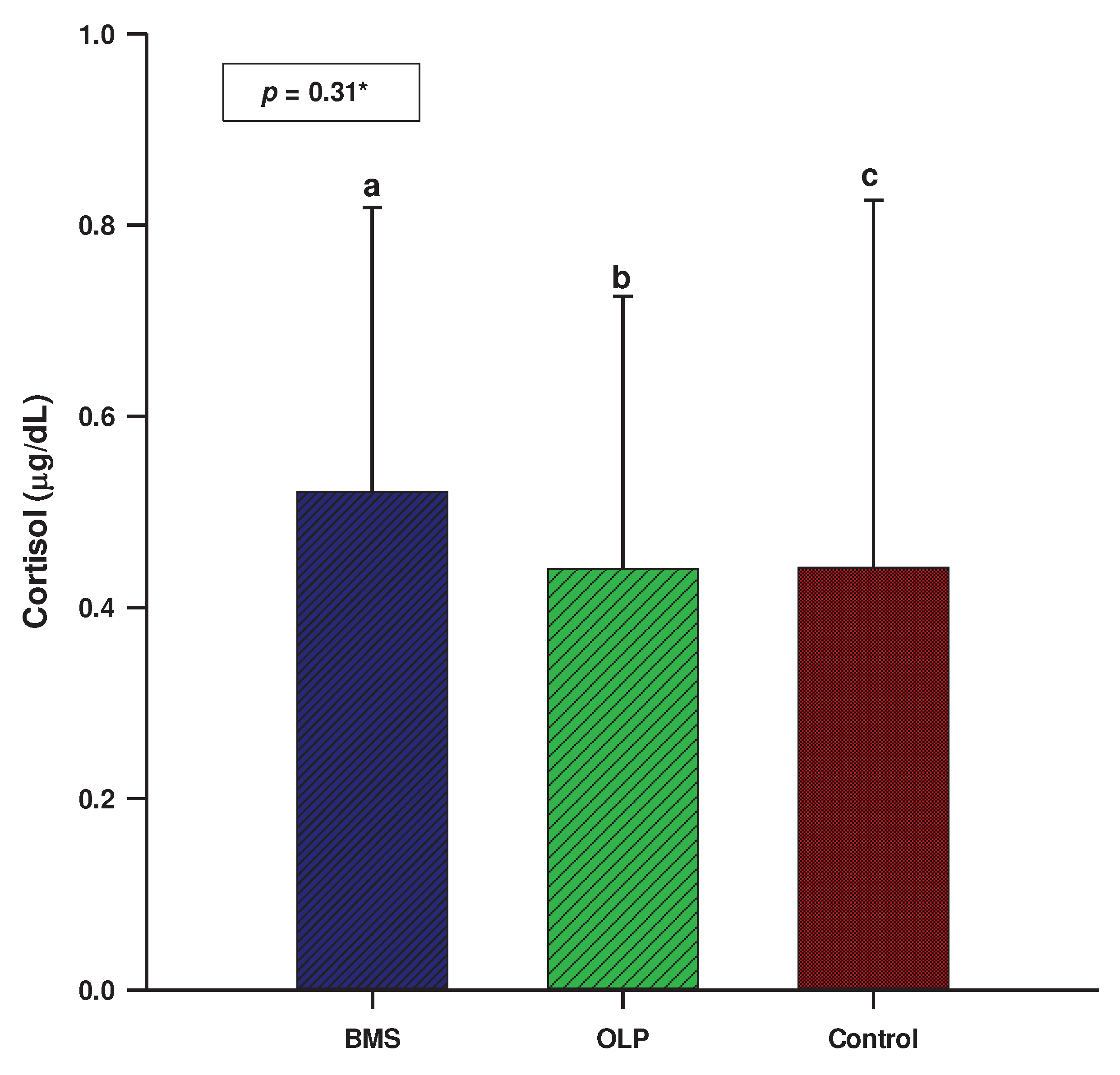
Figure 2.
Comparison of salivary α-amylase activity between patients with OLP (N=60), patients with primary BMS (N=60), and control subjects (N=40). * one-way analysis of variance (ANOVA) with post hoc Scheffe test; OLP: 145804 ± 111087; BMS: 160531 ± 148806; CONTROL: 179107 ± 182639; Abbreaviations: BMS, burning mouth syndrome; OLP, oral lichen planus.
Figure 2.
Comparison of salivary α-amylase activity between patients with OLP (N=60), patients with primary BMS (N=60), and control subjects (N=40). * one-way analysis of variance (ANOVA) with post hoc Scheffe test; OLP: 145804 ± 111087; BMS: 160531 ± 148806; CONTROL: 179107 ± 182639; Abbreaviations: BMS, burning mouth syndrome; OLP, oral lichen planus.
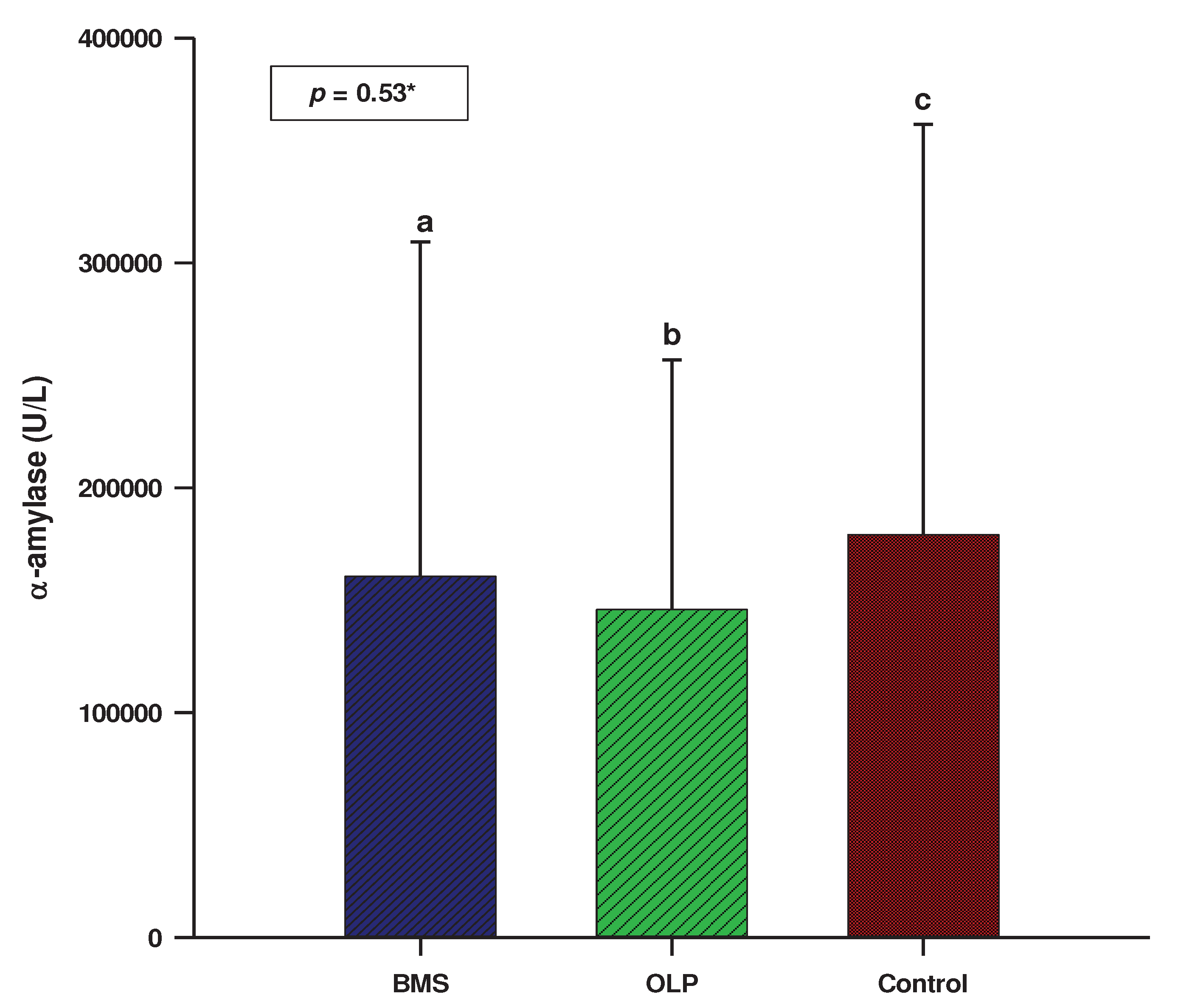

Table 1.
Demographic data.
| Sample N=160 |
OLP group N=60 |
BMS group N=60 |
Control group N=40 |
p | |
|---|---|---|---|---|---|
|
Gender (N, %) Men Women |
33 (20.6) 127 (79.4) |
15 (25.0) 45 (75.0) |
11 (18.3) 49 (81.7) |
7 (17.5) 33 (82.5) |
0.57* |
| Age (years) | 63.0 (52.0-70.0) |
63.0 (51.5-70.5) |
66.0 (57.0-72.0) |
61.0 (52.0-65.0) |
0.10# |
All data are presented as whole numbers (percentage) or median (interquartile range). * chi-square test # Kruskal-Wallis test with post hoc Dunn test, Abbreviations: BMS, burning mouth syndrome; OLP, oral lichen planus.
Table 2.
Psychological profile of patients with OLP, primary BMS, and control subjects.
| OLP group N=60 |
BMS group N=60 |
Control group N=40 |
p* | |
|---|---|---|---|---|
| Depression | 1.0 (0.0-8.0) | 10.0 (4.0-18.0) | 2.0 (0.0-4.0) | <0.001ab |
| Anxiety | 4.0 (0.0-8.0) | 7.0 (4.0-16.0) | 2.0 (0.0-5.0) | <0.001ab |
| Stress | 8.0 (2.0-14.0) | 16.0 (8.0-28.0) | 4.0 (2.0-14.0) | <0.001ab |
* Kruskal-Wallis test with post hoc Dunn's test. a BMS vs. OLP; p <0.05. b BMS vs. control; p <0.05. c OLP vs. control; p <0.05. Abbreviations: BMS, burning mouth syndrome; OLP, oral lichen planus.
Table 3.
Correlation of concentration/activity of salivary biomarkers (cortisol, α-amylase) and psychological profile in patients with OLP (N=60).
Table 3.
Correlation of concentration/activity of salivary biomarkers (cortisol, α-amylase) and psychological profile in patients with OLP (N=60).
| Depression | Anxiety | Stress | Cortisol | α-amylase | |
|---|---|---|---|---|---|
| Depression | 1.0 | ||||
| Anxiety | 0.643* | 1.0 | |||
| Stress | 0.720* | 0.696* | 1.0 | ||
| Cortisol | -0.011 | -0.016 | -0.077 | 1.0 | |
| α-amylase | -0.037 | 0.050 | 0.053 | 0.039 | 1.0 |
* p <0.001, Spearman's correlation.
Table 4.
Correlation of concentration/activity of salivary biomarkers (cortisol, α-amylase) and psychological profile in patients with primary BMS (N=60).
Table 4.
Correlation of concentration/activity of salivary biomarkers (cortisol, α-amylase) and psychological profile in patients with primary BMS (N=60).
| Depression | Anxiety | Stress | Cortisol | α-amylase | |
|---|---|---|---|---|---|
| Depression | 1.0 | ||||
| Anxiety | 0.652* | 1.0 | |||
| Stress | 0.793* | 0.705* | 1.0 | ||
| Cortisol | 0.083 | 0.028 | 0.122 | 1.0 | |
| α-amylase | 0.048 | -0.218 | -0.024 | 0.008 | 1.0 |
* p <0.001; Spearman's correlation.
Table 5.
Correlation of disease duration with concentration/activity of salivary biomarkers (cortisol, α-amylase) and psychological profile in patients with OLP (N=60) and primary BMS (N=60).
Table 5.
Correlation of disease duration with concentration/activity of salivary biomarkers (cortisol, α-amylase) and psychological profile in patients with OLP (N=60) and primary BMS (N=60).
| OLP | BMS | |||
|---|---|---|---|---|
| r* | p | r* | p | |
| Cortisol | 0.253 | 0.05 | -0.089 | 0.50 |
| α-amylase | 0.038 | 0.77 | 0.076 | 0.56 |
| Depression | -0.078 | 0.55 | -0.007 | 0.96 |
| Anxiety | -0.035 | 0.79 | -0.033 | 0.80 |
| Stress | -0.023 | 0.86 | -0.026 | 0.84 |
*Spearman's correlation coefficient; Abbreviations: BMS, burning mouth syndrome; OLP, oral lichen planus.
Table 6.
Correlation of symptom intensity (pain/burning) with concentration/activity of salivary biomarkers (cortisol, α-amylase) and psychological profile of patients with OLP (N=60) and patients with primary BMS (N=60).
Table 6.
Correlation of symptom intensity (pain/burning) with concentration/activity of salivary biomarkers (cortisol, α-amylase) and psychological profile of patients with OLP (N=60) and patients with primary BMS (N=60).
| OLP | BMS | |||
|---|---|---|---|---|
| r* | p | r* | p | |
| Cortisol | 0.006 | 0.96 | -0.230 | 0.08 |
| α-amylase | 0.079 | 0.55 | -0.004 | 1.10 |
| Depression | 0.109 | 0.41 | 0.373 | 0.003 |
| Anxiety | 0.081 | 0.54 | 0.515 | <0.001 |
| Stress | 0.089 | 0.50 | 0.365 | 0.004 |
*Spearman's correlation coefficient; Abbreviations: BMS, burning mouth syndrome; OLP, oral lichen planus.
Table 7.
Comparison of concentration/activity of salivary biomarkers (cortisol, α-amylase) and psychological profile between patients with erosive and non-erosive forms of OLP.
Table 7.
Comparison of concentration/activity of salivary biomarkers (cortisol, α-amylase) and psychological profile between patients with erosive and non-erosive forms of OLP.
| Erosive OLP | Non-erosive OLP | ||
|---|---|---|---|
| N=40 | N=20 | p | |
| Cortisol | 0.45 ± 0.31 | 0.41 ± 0.23 | 0.69† |
| α-amylase | 100815 (67160-257030) | 101035 (74825-142870) | 0.55* |
| Depression | 1.0 (0.0-5.0) | 2.0 (0.0-10.0) | 0.51* |
| Anxiety | 3.0 (0.0-6.0) | 5.0 (0.0-13.0) | 0.54* |
| Stress | 8.0 (2.0-12.0) | 8.0 (1.0-16.0) | 0.76* |
* Mann-Whitney U test; † independent t-test. Abbreviation: OLP, oral lichen planus.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



