Submitted:
07 July 2023
Posted:
10 July 2023
You are already at the latest version
Abstract
In infectious disease and clinical microbiology, rarely encountered species are often of special concern simply by virtue of their unfamiliarity, especially in settings of complicated underlying disease. This is all the more so when the infectious agent has an appearance that distinguishes it from most commonly encountered organisms, making it a mystery that must be explained. In this context, it is rare for histopathologists to be more familiar with a bacterial species than clinical microbiologists but Sarcina ventriculi is one such example. Infrequently seen in tissue and even less often in culture, we here report a case of Sarcina ventriculi in the GI tract of a geriatric patient with complex underlying history. A brief discussion of the history, clinical presentation, treatment, and culture conditions of this organism is provided, along with clarification of nomenclature, which has changed and could otherwise be a source of additional confusion in this rarely encountered bacterium.
Keywords:
sarcina
; bundles
; tetrads
; Micrococcus
; Zymosarcina
; Clostridia
Introduction
In infectious disease and clinical microbiology, rarely encountered species are often of special concern simply by virtue of their unfamiliarity, especially in settings of complicated underlying disease. This is all the more so when the infectious agent has an appearance that distinguishes it from most commonly encountered organisms, making it a mystery that must be explained. In this context, it is rare for histopathologists to be more familiar with a bacterial species than clinical microbiologists but Sarcina ventriculi is one such example. Infrequently seen in tissue and even less often in culture, we here report a case of Sarcina ventriculi in the GI tract of a geriatric patient with complex underlying history. A brief discussion of the history, clinical presentation, treatment, and culture conditions of this organism is provided, along with clarification of nomenclature, which has changed and could otherwise be a source of additional confusion in this rarely encountered bacterium.
Case Description
The patient is an 80-year-old female with a complex past medical history who presented with a small-bowel obstruction in the setting of multiple prior GI surgeries, impaired GI motility secondary to known hollow visceral myopathy, stercoral proctitis, and a chronic enterocutaneous fistula. Her initial CT scan was notable for severe fluid-filled dilation of the distal esophagus, stomach, duodenum, and proximal jejunum with gradual transition point in the left hemiabdomen. The gastroenterology service was initially consulted in the setting of hematemesis. The patient’s first esophagogastroduodenoscopy (EGD) showed active bleeding in the distal esophagus and she underwent subsequent clipping. She then developed coffee-ground emesis prompting a second EGD where 1.5 liters of dark liquid was suctioned from the stomach revealing nodular, erythematous, friable mucosa of unclear etiology. A biopsy from the stomach fundus was obtained for histological workup but culture was not pursued. Post biopsy, the patient received seven days of empiric antibiotic treatment with metronidazole and cefepime to cover the possibility of bacterial colitis. Further antibiotic treatment was not pursued following release of the biopsy results described below.
Case Analysis
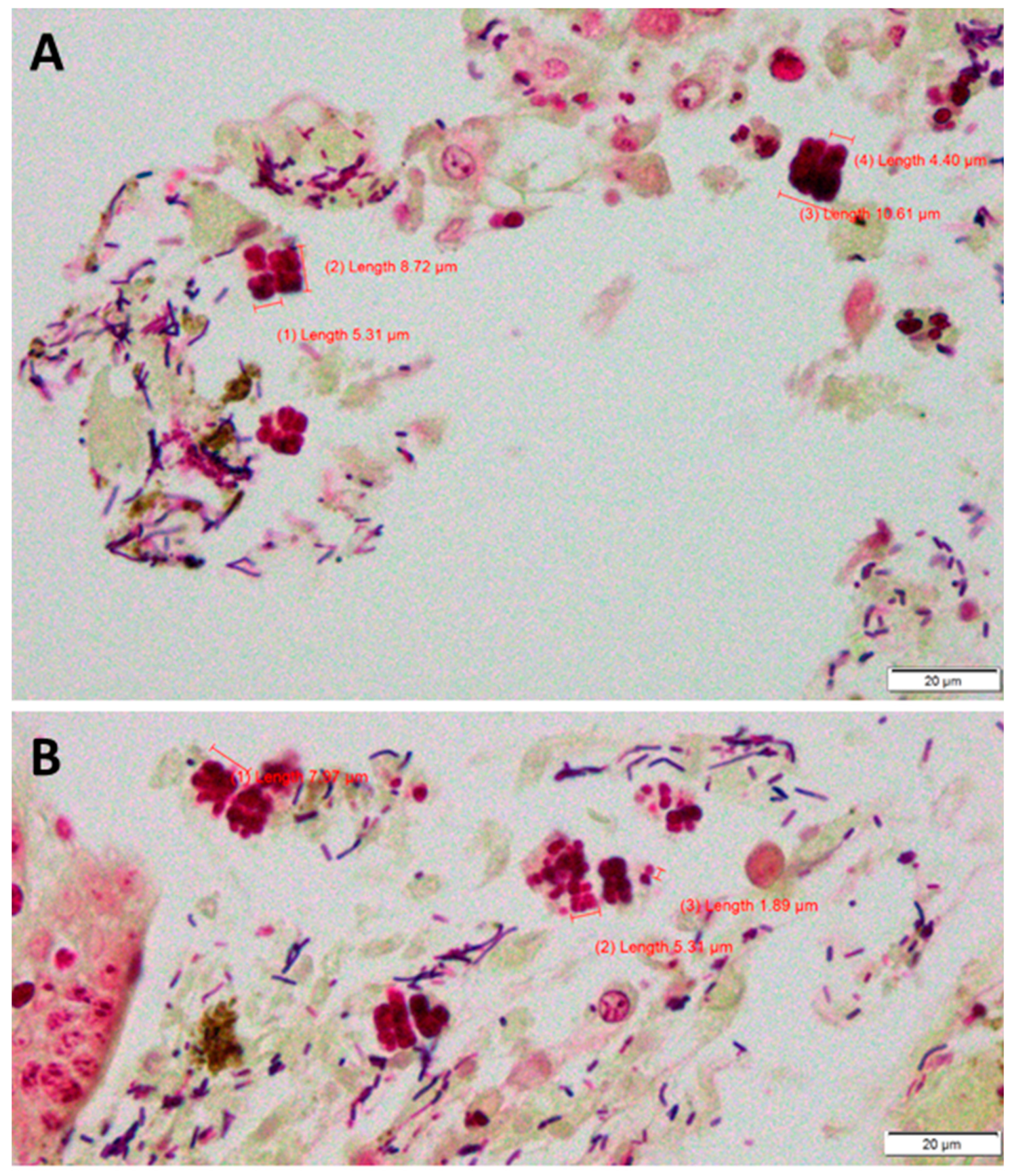
Tissue staining, including with hematoxylin-eosin (H&E; Figure 1) and Brown-Brenn (tissue Gram stain; Figure 2), revealed the presence of two bacterial morphologies. The first was Gram-positive rods approximately 1-2µm in length that were not further characterized (Figure 2). The second was large Gram-variable cocci arranged in multiples of four, reminiscent of four-leaf clovers. Single cells in these structures measured 1.5-3 µm in diameter (Figure 2B) [1,2] and frequently seen two-by-two cell arrangements were consequently ~3.5-7 µm on a side (Figure 1 and Figure 2). There were also higher-order multimers made from stacks of these smaller units; these multimers were typically 7-12 µm along a side, with the largest measuring ~20 µm along a side (Figure 1A). Given the particular arrangement of these cocci, their large size, and the specimen source, the differential was limited to Sarcina ventriculi.
Sarcina ventriculi was first described by John Goodsir in 1842 who observed and reported its presence in the stomach contents of a patient who presented with vomiting [3]. This organism is most often found in patients with conditions that cause gastroesophageal content stasis, such as gastric outlet mechanical obstruction, gastroparesis, or delayed gastric emptying [4]. It is primarily identified in the stomach, followed by the esophagus and duodenum. The typical symptoms of S. ventriculi infection include epigastric pain, nausea, and vomiting. The severity of the infection can vary, ranging from asymptomatic cases to life-threatening situations. In severe cases, complications such as hemodynamic instability secondary to emphysematous gastritis and gastric perforation can occur [5]. About two-thirds of reported cases suffered from at least one comorbidity [6]. While most cases have been identified in gastrointestinal biopsies, there have been very rare reports of this organism being isolated from blood, urine, and the respiratory tract [4,6,11].
Antimicrobial susceptibility data are scarce but a literature review of 66 cases found the most frequently reported empirical treatment regimen was metronidazole (as given in our case) in combination with ciprofloxacin [6]. Overall, the literature is consistent with Sarcina infection being more the effect of underlying gastrointestinal conditions than the cause, especially given its propensity to be seen in patients with multiple comorbidities. Treatment of underlying conditions may influence outcome more than treating Sarcina itself.
Reports from the veterinary field solidify the association of Sarcina species with intestinal morbidity. For example, the organism has been implicated as a causative agent in gastric bloat in livestock [7,8]. Candidatus S. troglodytae is associated with a highly lethal disease called “epizootic neurologic and gastroenteric syndrome” in chimpanzees [9]. Environmental sampling has recovered S. ventriculi from varied source material, including animals, plants, soil and water [10], supporting the conclusion that it is ubiquitous in nature.
S. ventriculi is known among surgical pathologists but is rarely identified in clinical microbiology laboratories. Indeed, most clinical microbiology textbooks do not include any information on S. ventriculi due to a scarcity of culture or susceptibility information. The organism grows anaerobically and requires 48 hours of incubation. Growth has been reported on CDC agar but not kanamycin/vancomycin-laked blood agar or phenylethyl alcohol agar [1]. S. ventriculi is often described as Gram-positive but, like many species in the family Clostridiaceae, it often stains poorly and can be more properly thought of as Gram-variable (Figure 2A).
S. ventriculi is known to form tetrads and cuboid clusters composed of eight individual cells, which are called sarcinae (“bundle” or “package” in Latin). What makes this organism distinctive from other bacteria that tend to form tetrads and sarcinae is the size of the clusters: with cell size ranging from 1.5-3 µm, S. ventriculi is significantly larger than Staphylococcus (also recoverable from stomach; cells arranged in disorganized clusters) and Micrococcus species (which are often seen in isolated tetrads), for example, and the characteristic higher-order cell clusters can reach 20 µm along a side, as is seen in this case (Figure 1A). As a colonizer of the stomach and upper intestinal tract, S. ventriculi is well adapted to low-pH conditions. The characteristic square and cuboid cell arrangements are seen at low pH; in high-pH environments, distorted cell shapes and cell arrangements appear and sporulation is induced [12]. While S. ventriculi is currently not included in standard MALDI-TOF databases, 16S rRNA sequencing can be used for definitive identification.
Note that there is some confusion with correctly naming this species. In addition to two historical species names, S. ventriculi [3] and Zymosarcina ventriculi [13], recent literature often refers to this species as Clostridium ventriculi due to a proposed reclassification based on 16S rRNA phylogeny [14,15]. However, the proposal was ultimately rejected [16], so as of 2023, the correct name for this bacterial species remains Sarcina ventriculi [17,18].
Conclusion
In the field of pathology, it is usually impossible to directly identify an organism to the species level when microbiological entities are seen only in stained specimens (e.g. Gram stain, H&E, etc), as growth properties, biochemical properties, and (sometimes) molecular techniques are very informative and usually required for distinguishing among similar-looking organisms. Sarcina ventriculi is the notable exception, owing to its unique large cell size and their arrangement in cuboid cell clusters. Mainly found in the GI tract, this anaerobic species is highly associated with pre-existing comorbidities, often including abnormal gastric function, the resolution of which may be more important than direct treatment of this bacterium itself. The lack of culture and susceptibility data, combined with the absence of Sarcina from MALDI-TOF databases, mean that visual detection remains the best method for identification of this bacterial species.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Elvert, J.L.; El Atrouni, W.; Schuetz, A.N. Photo Quiz: A Bacterium Better Known by Surgical Pathologists than by Clinical Microbiologists. J. Clin. Microbiol. 2018, 56, e01335–17. [Google Scholar] [CrossRef] [PubMed]
- Elvert, J.L.; El Atrouni, W.; Schuetz, A.N. Answer to Photo Quiz: Sarcina ventriculi. J. Clin. Microbiol. 2018, 56, e01335–17. [Google Scholar] [CrossRef] [PubMed]
- Goodsir, J.; Wilson, G. History of a Case in Which a Fluid Periodically Ejected from the Stomach Contained Vegetable Organisms of an Undescribed Form. Edinb. Med Surg. J. 1842, 57, 430–443. [Google Scholar] [CrossRef] [PubMed]
- Lam-Himlin D, Tsiatis AC, Montgomery E; et al. Sarcina organisms in the gastrointestinal tract: a clinicopathologic and molecular study. Am J Surg Pathol. 2011, 35, 1700–1705. [Google Scholar] [CrossRef] [PubMed]
- Marcelino, L.P.; Valentini, D.F.; Machado, S.M.d.S.; Schaefer, P.G.; Rivero, R.C.; Osvaldt, A.B. Sarcina ventriculi a rare pathogen. Autops. Case Rep. 2021, 11, e2021337. [Google Scholar] [CrossRef] [PubMed]
- Tartaglia, D.; Coccolini, F.; Mazzoni, A.; Strambi, S.; Cicuttin, E.; Cremonini, C.; Taddei, G.; Puglisi, A.G.; Ugolini, C.; Di Stefano, I.; et al. Sarcina Ventriculi infection: a rare but fearsome event. A Systematic Review of the Literature. Int. J. Infect. Dis. 2022, 115, 48–61. [Google Scholar] [CrossRef] [PubMed]
- Debey, B.M.; Blanchard, P.C.; Durfee, P.T. Abomasal bloat associated with Sarcina-like bacteria in goat kids. J. Am. Veter- Med Assoc. 1996, 209, 1468–1469. [Google Scholar]
- Vatn, S.; Gunnes, G.; Nybø, K.; Juul, H.M. Possible Involvement of Sarcina ventriculi in Canine and Equine Acute Gastric Dilatation. Acta Veter- Scand. 2000, 41, 333–337. [Google Scholar] [CrossRef] [PubMed]
- Owens, L.A.; Colitti, B.; Hirji, I.; Pizarro, A.; Jaffe, J.E.; Moittié, S.; Bishop-Lilly, K.A.; Estrella, L.A.; Voegtly, L.J.; Kuhn, J.H.; et al. A Sarcina bacterium linked to lethal disease in sanctuary chimpanzees in Sierra Leone. Nat. Commun. 2021, 12, 763. [Google Scholar] [CrossRef]
- 07 June. Available online: https://bacdive.dsmz.de/strain/164000#ref69479(retrieved on 07 June 2023).
- Al Rasheed, M.R.H.; Senseng, C.G. Sarcina ventriculi: Review of the Literature. Arch. Pathol. Lab. Med. 2016, 140, 1441–1445. [Google Scholar] [CrossRef]
- E Lowe, S.; Pankratz, H.S.; Zeikus, J.G. Influence of pH extremes on sporulation and ultrastructure of Sarcina ventriculi. J. Bacteriol. 1989, 171, 3775–3781. [Google Scholar] [CrossRef]
- Smit, J. Die Gärungssarcinen. Eine Monographie. Pflanzenforschung 1930, 14, 1–59. [Google Scholar]
- Willems, A.; Collins, M.D. Phylogenetic Placement of Sarcina ventriculi and Sarcina maxima within Group I Clostridium, a Possible Problem for Future Revision of the Genus Clostridium: Request for an Opinion. Int. J. Syst. Evol. Microbiol. 1994, 44, 591–593. [Google Scholar] [CrossRef] [PubMed]
- Lawson, P.A.; Rainey, F.A. Proposal to restrict the genus Clostridium Prazmowski to Clostridium butyricum and related species. Int. J. Syst. Evol. Microbiol. 2016, 66, 1009–1016. [Google Scholar] [CrossRef] [PubMed]
- Tindall, B.J. Priority of the genus name Clostridium Prazmowski 1880 (Approved Lists 1980) vs Sarcina Goodsir 1842 (Approved Lists 1980) and the creation of the illegitimate combinations Clostridium maximum (Lindner 1888) Lawson and Rainey 2016 and Clostridium ventriculi (Goodsir 1842) Lawson and Rainey 2016 that may not be used. Int. J. Syst. Evol. Microbiol. 2016, 66, 4890–4894. [Google Scholar] [CrossRef] [PubMed]
- Wiegel J, Family I. 2009. Clostridiaceae Pribram 1933, 90 AL. In: De Vos P, Garrity GM, Jones D, Krieg NR, Ludwig W, Rainey FA, K.-H. S, Whitman WB (eds), Bergey’s Manual of Systematic Bacteriology, volume 3, The Firmicutes, Springer, New York, p. 738-848.
- 07 June. Available online: https://lpsn.dsmz.de/species/sarcina-ventriculi(retrieved on 07 June 2023).
Figure 1.
H&E stain of stomach tissue. Sarcina ventriculi cells appear purple or pink. Size measurements of various Sarcina cell arrangements are shown in all three panels.
Figure 1.
H&E stain of stomach tissue. Sarcina ventriculi cells appear purple or pink. Size measurements of various Sarcina cell arrangements are shown in all three panels.
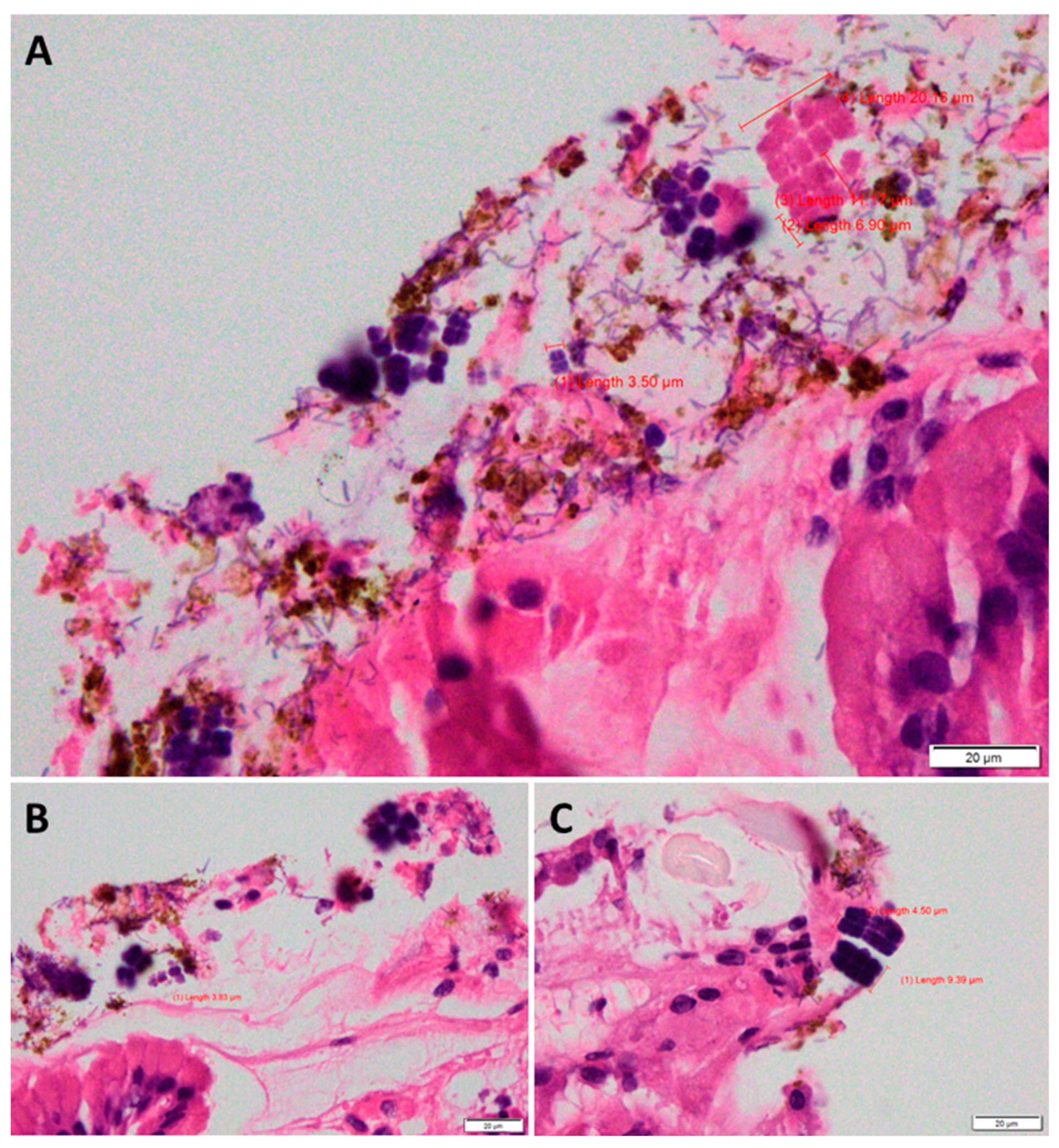
Figure 2.
Brown-Brenn (tissue Gram) stain of stomach tissue. Sarcina ventriculi cells appear as square packets of multiples of four. Their Gram variability is very apparent in Panel A. Sizes of various S. ventriculi structures are indicated. Gram-positive rods are also visible in both panels.
Figure 2.
Brown-Brenn (tissue Gram) stain of stomach tissue. Sarcina ventriculi cells appear as square packets of multiples of four. Their Gram variability is very apparent in Panel A. Sizes of various S. ventriculi structures are indicated. Gram-positive rods are also visible in both panels.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



