Submitted:
03 July 2023
Posted:
05 July 2023
You are already at the latest version
Abstract
Background: Lipoprotein lipase (LPL) deficiency is a genetic condition. Affected individuals typically develop symptoms before age 10 with severe hypertriglyceridemia. No pharmacological treatment has lowered triglyceride levels in LPL deficiency patients successfully. The purpose of this study is to report on clinical outcomes of patients with LPL deficiency who responded to dietary therapy with successful reduction of their triglyceride (TG) levels with a long-chain triglyceride (LCT)-restricted, medium-chain triglyceride (MCT)-supplemented diet.
Methods: A single-center retrospective case review study of LPL deficiency patients who met the inclusion criteria and were evaluated at the Hospital of Sick Children between January 2000 to December 2022. Data collected include demographic and clinical data, biochemical profiles at diagnosis and after dietary treatment initiation, and molecular results.
Results: The study included seven patients with a suspected diagnosis of LPL deficiency (hypertriglyceridemia > 20 mmol/L). Six patients had a confirmed molecular diagnosis of LPL deficiency, and one had a Glycogen storage disease 1a (GSD1a) diagnosis. After presenting with hypertriglyceridemia, an LCT-restricted and MCT-supplemented diet was initiated, resulting in immediate and sustained TG reduction in all LPL deficiency patients that adhered to the diet. Additionally, they all maintained excellent growth and development. LPL deficiency-related complications were not observed under the MCT-enriched diet, except for increased pancreatic enzymes in one patient after dietary error. As expected, the diet failed to treat hypertriglyceridemia in the GSD1 patient.
Conclusions: The dietary restriction of LCT in combination with MCT supplementation was feasible and effective in the long-term management of patients with LPL deficiency. In our experience, this treatment eliminated LPL-related complications and led to good clinical outcomes.
Keywords:
lipoprotein lipase deficiency
; MCT diet
; inborn errors of metabolism
Introduction
Lipoprotein lipase (LPL) deficiency is a rare autosomal recessive condition due to biallelic pathogenic variants in the LPL gene that disrupts the postabsorptive conversion of alimentary fats (Gaudet et al., 2014). The lipoprotein metabolism, especially metabolization of chylomicrons and very-low-density lipoproteins relies on the function of the enzyme LPL. Consequence of enzyme dysfunction is the distinct rise of serum triglycerides (TGs).
LPL deficiency usually presents in childhood with episodes of abdominal pain, recurrent episodes of acute pancreatitis requiring hospitalization. Left untreated, pancreatitis can develop into a chronic condition with permeant destruction of the pancreatic cells that result in exocrine and endocrine pancreatic insufficiency. Additionally, patients with LPL deficiency may manifest eruptive cutaneous xanthomata, lipemia retinalis, and hepatosplenomegaly. Affected individuals typically develop signs and symptoms before age 10, with one-quarter having first symptoms at one year of age (de Pretis, Amodio, & Frulloni, 2018).
The primary long-term treatment for LPL (lipoprotein lipase) has traditionally been dietary modification, specifically a low-fat diet with a focus on reducing long-chain TGs (LCT). Other past and present treatment options include LPL gene therapies (alipogene tiparvovec), which involves introducing functional copies of the LPL gene using adeno-associated viral vector 1 (Gaudet et al., 2013), diacylglycerol acyl transferase 1 (Meyers et al., 2015), inhibitors of microsomal TG transfer protein (Sacks, Stanesa, & Hegele, 2014), angiopoietin-like protein 3 (Gryn & Hegele, 2015) and apoC-III (Gaudet et al., 2014). To date, these treatment options either have not been proven successful in lowering TG levels in LPL patients, have had to be discontinued for various reasons, or are still under investigation.
Treatment with medium chain TGs (MCT) has been proposed since MCT are not incorporated into chylomicron bodies and are absorbed directly from the portal vein (Williams et al., 2018). However, treatments of LPL patients with an MCT-enriched diet have not been reported to the best of our knowledge. It is known that provision of MCT is of particular importance for infants and children to ensure adequate fat intake for growth and development. Furthermore, the treatment of long-chain faty acid oxidation defects with an LCT-restricted/MCT-enriched diet has become a successful intervention that changes the natural course of the diseases (Van Calcar et al., 2020) and that is being practiced in all metabolic centers for inborn errors of metabolism in the world.
For more than a decade the metabolics service at the Hospital for Sick Children has success in treatment of LPL patients with an LCT-restricted/MCT-enriched diet. Currently, such dietary modifications are not standard of care for LPL deficiency or hypertriglyceridemia. This paper provides evidence that LPL patients can be successfully managed with this diet and we hope it paves the way to establish disease- specific dietary recommendations for patients with LPL deficiency.
Methods
In a single-center, retrospective, case review study patients with hypertriglyceridemia above 20 mmol/L, that have been or are still treated with an MCT-enriched diet by the metabolic service of the Hospital for Sick Children were included. After receiving parental consent, data were abstracted from medical records and recorded in the study database. The chart review included charts from 01 January 2000 to 01 December 2022 of male and female patients below 18 years of age.
We were able to enrol seven patients, six female, one male, with hypertriglyceridemia. We report the clinical manifestations and molecular findings in these patients. The response to LCT-restricted/MCT- enriched diet was monitored with respect to clinical course, disease-specific complications, and biochemical profile - specifically lipase (reference range 4 – 39 IU/L), amylase (reference range < 102 IU/L), TGs (reference range < 0.85 mmol/L (0-12 years), < 1.02 mmol/L (12 years and older)), cholesterol (reference range < 4.4 mmol/L), and essential faty acids (EFA).
The study was approved by the local ethics commitee (REB# 1000061520).
Red blood cell (RBC) total lipid faty acid profile
RBCs were separated from 1.5-3 mL EDTA blood, washed with phosphate-buffered saline, transferred to screw-capped plastic (low in phthalate) tubes such as NUNC micro screw-top freezer tubes and flushed with a stream of nitrogen for about 10 seconds before capping tightly and stored at -80°C. The samples were analyzed at the Peroxisomal Diseases Laboratory at the Kennedy Krieger Institute in Baltimore, Maryland. RBC membrane levels of faty acids (C8-C26) were determined using capillary gas chromatography-mass spectroscopy of pentafluorobenzyl bromide faty acid esters (Lagerstedt et al., 2001).
Patients
Patient 1
This girl is the first child of consanguineous parents of Indian descent with uneventful antenatal and perinatal history. At 40 days of age, she presented with a one-day history of persistent emesis, not tolerating her feeds. The abdominal ultrasound demonstrated a mass in the head of the pancreas, for which she was transferred to a tertiary pediatric center for further management.
Laboratory results at admission revealed a significant elevation of TGs 276 mmol/L, cholesterol 27 mmol/L, and lipase >1,200 U/L. A complete blood cell count, electrolytes, transaminases, and liver synthetic function tests were within normal limits. She was admited to the general pediatrics ward for pancreatitis secondary to hypertriglyceridemia, raising suspicion of a genetic dyslipidemia disorder. Upon admission, oral intake was stopped, and she was managed with I.V. fluids that led to normalization of TGs. Re-establishing enteral nutrition caused a significant rise of TGs to 117 mmol/L and lipase of 694 U/L. On examination, she had increased muscle tone. Due to the concern of blood hyper-viscosity, a brain MRI showed no evidence of infarction or clots, she was transferred to the PICU, where she received two days of plasmapheresis until normalization of TGs.
Initial suspicion of pancreatic mass was ruled out as abdominal MRI showed pancreatic inflammation consistent with pancreatitis.
After the discontinuation of plasmapheresis, the metabolic service was consulted, and she started on MCT-enriched formula (Lipistart) with a down trending and stable TGs below 10 mmol/L until discharge.
Targeted genetic testing confirmed the LPL diagnosis due to a homozygous pathogenic variant in the LPL
gene (c. 1014 C>A, p. Tyr338*). Both parents were heterozygous for the familial variant in
After discharge, she was maintained on an MCT diet with good tolerance. She was fed Lipistart® (Vitaflow, USA) exclusively for the first six months of life. Regular blood work over four years showed stable TGs within our target range for LPL patients < 10 mmol/L. In addition, she has excellent weight
gain, linear growth, up-to-age developmental milestones, and no further episodes of pancreatitis or
other LPL deficiency-related complications.
Patient 2-I
The girl is the first child of consanguineous, healthy parents of Pakistani descent. Pre-, peri-, and postnatal periods were unremarkable. At 3 ½ months of age, isolated splenomegaly was noted at a routine well-baby check-up. Blood work unmasked significant hypertriglyceridemia of > 50 mml/L; thus, she was referred to our center. Repeat labs confirmed hypertriglyceridemia of 29 mmol/L, normal cholesterol, amylase, and lipase. She was started on LCT-restricted/MCT-enriched formula with Lipistart® and Portagen® (Mead Johnson, USA). Molecular testing confirmed LPL deficiency with a homozygous pathogenic variant in the LPL gene (c.784C>T, p.Q262X) that segregated with the parents.
By 18 months of age, she was growing and developing well. TG levels up to this age were between 15-18 mmol/L, which we considered protective against pancreatitis, but rose to 20 mmol/L at 30 months of life. Changes were made, including discontinuing the Portagen® formula, increasing MCT provision by adding MCT Procal® (Vitaflow, USA) to Lipistart® and adding MCT oil to food. Moreover, EFA provision intake was suboptimal, for which the walnut oil dose was increased. Despite the changes, her TGs remained in the twenties, and her weight gain dropped. Turns out, the unsatisfactory metabolic control and failure to thrive were related to unhealthy feeding habits. She was followed up by a pediatric psychiatrist expert for feeding challenges, after which feeding habits improved and weight gain stabilized. TGs continued to fluctuate but lowered to 12-20 mmol/L. Until now, there have been no LPL deficiency-related complications.
Patient 2-II
The child, the third of consanguineous healthy parents of Pakistani descent and sibling of patient 2-I, was diagnosed due to positive family history. After delivery she was admited to an outside NICU for feeding intolerance secondary to a cleft palate. Given the positive family history, she was tested for TGs on day two and six of life. TGs were 30 mmol/L confirming her diagnosis of LPL deficiency. She was started on LCT-restricted/MCT-enriched formula (Lipistart®) on day 7 of life. By three months of age, she was noted to have severe global developmental delays, horizontal nystagmus, and facial dysmorphism. At the age of 4 years, she was diagnosed with an autistic spectrum disorder. Given consanguinity, a second genetic condition was suspected; therefore, referred for genetic service for assessment. An extensive genetic workup including a trio whole exome sequencing was done which confirmed the diagnosis of LPL deficiency with the same homozygous variant as her sister and a homozygous variant of uncertain significance in NAA25 gene which is a candidate gene with a potential relationship to her disease phenotype; however, this requires further evaluation.
From a metabolic perspective, since birth, she has been doing very well, tolerating her LCT- restricted/MCT-enriched diet. She has not had any LPL related complications. Her TG levels have been mostly in the treatment target range of <10 mmol/L. She continues to gain weight and grow along the usual percentiles.
Patient 3
This girl is the second child of consanguineous parents of Pakistani descent. Pregnancy was notable for fetal growth restriction. She was delivered at 41 weeks with a birth weight of 2.4 kg. She was noted to have poor weight gain during the neonatal period despite adequate nutrition. In addition, she had a positive newborn screening for congenital hypothyroidism, for which she was followed by Endocrinology.
Given a positive family history of a first-degree cousin with LPL deficiency (patient 2-I), she was assessed by the metabolic team at our center at seven weeks of age. Blood workup revealed elevated TGs 116 mmol/L and cholesterol of 19 mmol/L leading to admission for further evaluation and initiation of dietary treatment. Amylase was normal, with no signs of pancreatitis. She was successfully switched from breast milk to LCT-restricted/MCT-enriched formula (Lipistart) with a slow but persistent drop of TG. LPL diagnosis was confirmed with a homozygous pathogenic variant in the LPL gene ((c.784 C>T, p.Q262X), the same as in her cousins. Both parents were heterozygous for the familial variant in LPL. After discharge, she continued to have excellent tolerance to the MCT-based formula and TGs well withing our treatment target range <10 mmol/L.
By six months of age, she was noted to have failure to thrive, despite receiving appropriate calories for age and adequate metabolic control, which was out of proportion to what was known for LPL deficiency. Furthermore, she was noted to have a global developmental delay.
At the age of 7 months, given the clinical symptoms and the persistent elevation of TSH at around 10 mIU/L (reference range 0.5-4.77) despite of normal FT4 13.1 pmol/L (reference range 10-23) and adequate metabolic control, she was diagnosed with thyroid hormone resistance and was started on L- thyroxine, initially with 25 µIU/day, later increased to 50 µIU/day. That led to significantly improved growth and catch up in development.
The girl had one episode of pancreatitis. At four years of age, after eating lots of ice cream few days prior to her presentation, her lipase was 289 U/L, TGs were 14 mmol/L at time of presenting in clinic, but likely much higher the days before. After this, she has continued to do very well with her MCT diet and maintained TGs within the treatment target range <10 mmol/L. There were no other LPL deficiency related complications and no further concerns regarding weight gain and growth. She also continues to make appropriate gains from a developmental perspective.
Considering the complexity of the clinical presentation, the consanguinity and appreciation of some distinct facial features, the genetics service initiated further workup. Microarray and brain MRI were normal. Whole exome sequencing revealed a homozygous variant of unknown significance in IGF1R in addition to the already known LPL variant.
Patient 4
She is the product of a consanguineous union between first cousins of Pakistani descent. She was doing well until the age of 20 days, when she presented to the emergency department with history of lethargy, poor feeding, irritability, and abdominal distension. Blood taken at this visit was noted to be creamy.
Abdominal ultrasound showed splenomegaly. The initial lipid profile showed elevated cholesterol at 7.65 and a TGs of 45.5 mmol/L. She was started on LCT-restricted/MCT-enriched diet consisting of Portagen®, Enfamil® (Mead Johnson, USA) plus added walnut oil, creating a 60% MCT mixture. TGs improved quickly. By day 4 of admission, the TGs were 1.34 mmol/L. Diagnosis of LPL deficiency was confirmed by molecular testing, which showed a homozygous variant in the LPL gene (c.472G>A, p.A158T). At 18 months, the family moved to the Middle East but returned for yearly follow ups to our center until the last follow-up at 17 years of age. Since diagnosis, she has followed the MCT-enriched diet. Her TG levels fluctuated over the years, with most readings between 13-17 mmol/L. Parents atributed the fluctuation to difficulty in adherence to the diet, given that she spends much time with the extended family. At the age of 10 years and 17years, she had a high TG level of 33 and 25 mmol/L, respectively, atributed to dining out and eating high-fat food. Fortunately, she remained stable with no signs of pancreatitis. TGs improved immediately after resuming the MCT diet. Since birth, she has achieved appropriate developmental milestones and has grown appropriately. She has not had any LPL deficiency related complications.
Patient 5
The boy is the product of a consanguineous union between first cousins of Pakistani descent. At two weeks of age, he presented for a circumcision, when blood work was done, and high TGs were found. Not much is known about further details. However, at that time, the family in Pakistan was told to avoid high-fat food. The family history is remarkable in that both parents had hyperlipidemia and the father had bypass surgery by the age of 60 years. One paternal uncle has hyperlipidemia and is on medications but has no cardiovascular complaints. The family moved to Canada in 2006 when he was six years old. He was followed up in the cardiology lipid clinic at Hospital for Sick Children. His initial lipid profile showed elevated TG; he was started on a fat restricted diet and fibrate medication (Lipidil®). Diagnosis of LPL deficiency was confirmed by molecular testing which showed a homozygous nonsense mutation in the LPL gene (Q262X, c.784C>T). The family’s compliance with the diet was insufficient. He continued to have extremely elevated TG levels with a range of 45 mml/L which ultimately affected his growth and development significantly. By seven years of age, he developed eruptive xanthomata spreading over his body, ears, forearms, and legs. He had no previous history of hospitalization with acute pancreatitis; however, he had frequent episodes of headache and abdominal pain related to eating faty food.
At the age of 14 years, he was referred to our metabolic clinic, and his diet was adjusted to LCT- restricted/MCT-enriched diet. Since implementing the dietary changes, his TGs and clinical status have improved. Specifically, his growth, weight gain, and head circumference improved, crossing percentiles. However, compliance with the MCT diet remained an issue until adulthood, which is reflected in his TG readings and growth parameters.
Patient 6
She is the product of a non-consanguineous union of healthy parents of European descent. She was reportedly in good health until five months of age, when she began to experience growth failure. At nine months, her length was just above the 3rd percentile while her weight was tracking along the 50th percentile. At that time, her weight started decreasing, she began to experience increased work of breathing and had tachypnea. Work up revealed a significantly elevated TGs 113 mmol/L, cholesterol of 14.43 mmol/L, elevated lactate, elevated transaminases, and high anion gap metabolic acidosis. Abdominal ultrasound showed significant hepatomegaly.
As the differential diagnosis for her highly elevated TGs included LPL deficiency, she was managed with LCT-restricted/MCT-enriched diet; however, due to slow improvement in the TGs, she required intravenous fluids and parenteral nutrition for five days before significant improvement in TG and lactate. She remained clinically well with no evidence of pancreatitis. Once the TGs were below 40 mmol/L, oral feeding was re-started with MCT formula (Lipistart®) and TGs were down trending. Subsequent observation of recurrent hypoglycemia and pathognomonic lactate trends in response to fasting/feeding led to the suspicion of glycogen storage disease type1 (GSD1). Consequently, our treatment plan was changed to manage both LPL and GSD1 until genetic diagnosis. She was discharged home on frequent feeds, Lipistart® formula, and cornstarch for glucose homeostasis. Her glycaemic control with this regimen was reasonable. She was gaining weight and making good developmental progress. Her metabolic control improved, with TGs below 10 mmol/L, normal lactate, and uric acid. After molecular confirmation of GSD1A deficiency through segregating compound heterozygous pathogenic variants in G6PC (c.980_982del p. Phe327del / c.563-3C>G p.?), the Lipistart® formula was stopped, while GSD management continued.
Diet Principles
The diet restricts LCT to a level alike the restriction for a severe long-chain faty acid oxidation defect (Van Calcar et al., 2020). We aim to provide approximately 10-15% of energy in the diet from LCT and 20-30% of energy from MCT, depending on the age of the child and the fat intake required to sustain growth and weight gain. Total faty acid needs are higher for infants and therefore total energy from fat, or the % energy from MCT is higher in the neonatal period. The diet aims to provide only enough LCT to prevent deficiency in the essential faty acids and ensure the diet is tolerable.
Sources of MCT in the infant diet are MCT-enriched formulas such as Monogen® (Nutricia) or Lipistart® (Vitaflo). Our patients are typically maintained on the MCT-enriched formula into childhood, as it is also an important source of vitamins and minerals, some of which are at risk of deficiency in a diet low in LCT. In childhood, or when the MCT-enriched formula is no longer tolerated, MCT is provided in the diet across the diet in the form of medical-grade MCT oil (Nestle) added to cooking or foods, or a MCT supplement, such as Liquigen® (Nutricia) or MCT Procal® (Vitaflo) - added to a fat-free beverage or food.
LCT are provided from a source of essential faty acids in the infantile period and then, once the infant begins to eat food, in minimal amounts from food. Food choices are either fat-free or very low in fat. Parents are often advised to count grams of fat from food and not exceed a limit recommended by the dietitian.
The essential faty acids, linoleic acid and alpha-linolenic acid cannot be made by the body and therefore must be included in the diet in the minimum amounts reported to be required (Spiekerkoeter et al., 2009; Van Calcar et al., 2020). The inclusion of breastfeeding in the diet for infants is difficult due to the very high fat content of breastmilk, which is mostly LCT.
Results
Our results showed that patients with hypertriglyceridemia > 20 mmol/L can be managed with MCT- enriched diet. This study reviews a 23-year period with a total of 7 cases enrolled. The follow-up after treatment start was 7.1, 4.3-15.5 years (median, range) excluding patient # 7 who had a diagnosis of GSD and MCT-enriched diet stopped after the diagnosis.
Parents of all six cases with LPL deficiency were consanguine couples. 50% (3 cases) had family history of similar condition. Five cases of LPL deficiency were females and 1 case was male (Table 1).
Presentation
The initial presentation was very early during the neonatal/early infantile period. The median age at presentation was 30 days. The initial presentation for 2 cases (P1, P4) was poor feeding, lethargy, and abdominal distension. In P1, abdominal distension was initially thought to be due to a pancreatic mass, ruled out after an abdominal MRI, showed changes suggestive of pancreatitis. Abdominal US in P4 showed splenomegaly. Two patients (P 2-I, P5) were picked up during a routine checkup. Of these (P 2-I) was found to have isolated splenomegaly, and the other was found to have elevated TGs in a routine blood work. Given the family history of LPL deficiency in 2 cases (P2-II, P3), they were screened for LPL deficiency during the neonatal period (Table 1).
Treatment
The LCT-restricted/MCT-enriched diet in our patients is summarises in Table 2.
Biochemical characteristics
The median plasma TG concentration at presentation, excluding patients #5 (we do not have the reading at presentation), was 45.8 mmol/L. Our Diet was initiated immediately after the initial presentation for four (P2-I, P2-II, P3, P4) of the 6 cases. P1 was managed initially by the pediatric team. She underwent plasmapheresis, and our Diet was started four days after her presentation. P5 was followed initially by the cardiology lipid clinic. They tried Diet and other interventions but could not lower TGs after which he was referred to our service at the age of 13 years and five months and started on the MCT-enriched Diet. All six patients had an immediate response and improvement in their TG level. Four (P1, P2-II, P3, P4) of the six patients demonstrated plasma TG levels < 10 mmol/L within five days of treatment or less (Figure 1). Due to unclear causes in P2-I, we could not establish TGs below 10; however, most of her readings were below 20 mmol/L, with no evidence of pancreatitis. In P5, routine blood work after initiating the MCT-enriched diet showed a significant decrease in TGs compared to the previous levels. Nonetheless, his readings were mainly around 20 mmol/L due to diet adherence issues.
Furthermore, amylase and lipase were recorded in patients charts during follow up visits for all six patients except for P4 where we did not have lipase historically (Figure 1). We could not establish clear correlation between lipase, amylase, and TG levels. Lipase was elevated in two patients who were symptomatic and presented with acute pancreatitis (P1, P3). One child (P2-I) always had two times higher baseline lipase than the other cases. However, she did not have any documented acute pancreatitis episode (Figure 1).
Complications
To study the effect of long-term dietary intervention on TG, we compiled plasma TG data for each patient during the observation period (Figure 1). During the study period, one patient (P3) had a documented episode of acute pancreatitis, presenting with abdominal discomfort after eating a big portion of ice cream (lipase 289 IU/L). Her TG concentration was in the treatment range when she reassumed MCT- enriched diet the next day. She recovered without sequelae. Her metabolic control was excellent before and after the acute pancreatitis with most readings within the treatment target range of < 10 mmol/L.
Due to the uncontrolled TG levels preceding the initiation of the MCT-enriched diet, P5 developed eruptive xanthoma in many parts of his body (ears, forearms, and legs). After initiation of the MCT- enriched diet, his xanthomas abated over time, and there were no other documented LPL-related complications (Table 1).
We have not observed lipidemia retinalis, xanthomata, and organomegaly in any patient after initiation of the LCT-restricted/CT-enriched diet.
Growth and EFF
To assess the safety of the dietary intervention growth, development, and EFA levels for all six cases were followed very closely over the observation period (Figure 2). No persistent adverse effects on weight gain, linear growth, or pubertal development were seen in our patients. P5 had a catch-up growth after starting the MCT-enriched diet. In P3 growth failure initially was caused by hypothyroidism and was not diet related. Once thyroxine supplementation was started growth and development improved.
Genetic variants
Genetic analysis was performed in all 7 cases. All LPL patients had homozygous pathogenic variants in LPL gene. Four were homozygous for the same pathogenic variant (p.Q262X). One patient was homozygous for p.Tyr338*, and one was homozygous for p.A158T (Table 1). We could not establish any genotype-phenotype correlation. Five of the pathogenic variants were missense and one was a nonsense mutation (Table 1). Two pathogenic variants in the G6PC gene (c.980_982del p. Phe327del / c.563-3C>G p.?) segregating with the parents were identified in patient 6 with GSD1a.
Imaging
Abdominal ultrasound was performed in 4 cases (P1, P3, P2-I, P4). In two of them (P1, P4), abdominal ultrasound was conducted as part of the workup for the initial presentation. In one patient (P2-I), a follow-up abdominal ultrasound was done as a routine check-up suspected splenomegaly in the physical examination. Lastly, in P3, ultrasound was done after she presented to the hospital with abdominal distention and elevated lipase. Routine abdominal ultrasounds were not done during the observation period. Abdominal and Brain MRI was completed for P1 at initial presentation due to suspicion of an abdominal mass in the ultrasound and abnormal neurological examination. In patients P2-II and P3, brain MRI was performed as part of the genetic workup of the medical complexity (Table 1).
Discussion
Lipoprotein lipase deficiency (LPL) is a rare autosomal recessive disorder characterized by impaired TG metabolism due to a mutation in the lipoprotein lipase gene. In this retrospective chart review, we present the clinical characteristics and management outcomes of seven children presenting with hypertriglyceridemia >20 mmol/L who were treated with an LCT-restricted/MCT-supplemented diet.
The clinical presentations of the patients in this study were consistent with the typical features of LPL deficiency. Some experienced episodes of abdominal pain and recurrent acute pancreatitis, a common LPL deficiency complication. The elevated serum TG levels observed in these patients are a hallmark of the disorder and can lead to various complications if left untreated, such as lipemia retinalis, eruptive cutaneous xanthomata, and hepatosplenomegaly. An association of LPL deficiency with increased risk of cardiovascular disease is still controversial. The current literature does not consistently support an increased risk of cardiovascular disease in patients with LPL deficiency (Benlian et al., 1996; Clee et al., 2000; Hokanson, Brunzell, Jarvik, Wijsman, & Austin, 1999; Kobayashi & Mabuchi, 2015). In one study, in four patients peripheral or coronary atherosclerosis, or both were observed before age 55 despite good metabolic control (Benlian et al., 1996). Hokanson et al. reported an increased risk of atherosclerosis with specific genotypes (Asp9Asn and Gly188Glu) and cardioprotective effect with others (S447X) (Hokanson et al., 1999). None of our patients had the high-risk genotypes described by Hokanson et al. (Hokanson et al., 1999). Additionally, no cardiovascular disease or cardiac symptoms were observed during the observation period. Therefore, we did not routinely perform cardiovascular monitoring in our patients. Nevertheless, we can not exclude the long-term risk of cardiovascular disease in those individuals with LPL deficiency that maintain TG levels between 10-20 mmol/L. Long-term studies in adults would be necessary to assess the cardiovascular disease risk associated with TGs in this range.
LPL deficiency is the primary differential diagnosis to consider in case of severe hypertriglyceridemia, i.e., TGs above 20 mmol/L. The clinical presentation of LPL can overlap with other conditions characterized by hypertriglyceridemia, such as uncontrolled diabetes mellitus, hypothyroidism, specific medications like thiazide diuretics and estrogen-containing contraceptives, as well as excessive alcohol consumption.
Once a diagnosis of LPL deficiency is confirmed, it is crucial to avoid these secondary causes to effectively manage the condition (Paragh, Nemeth, Harangi, Banach, & Fulop, 2022). In addition to LPL and apoC-II, other less common gene defects can cause monogenic chylomicronemia. APOC2 ranks as the third most observed cause of monogenic chylomicronemia, while pathogenic variants in other genes like APOA5, LMF1, LPL/LMF1, LPL/ApoA5, and GPIHBP1 are much rarer (Brahm & Hegele, 2015).
Additionally, it is worth discussing the differential diagnosis of LPL deficiency considering the case of patient 6, who was ultimately diagnosed with GSD1a. GSD1 is a rare autosomal recessive disorder due to impaired glucose-6-phosphatase activity and leading to the accumulation of glycogen in various tissues, including the liver and kidneys. Clinical features of GSD1 include hypoglycemia, hepatomegaly, growth retardation, and lactic acidosis. Some GSD1 patients may also present with hypertriglyceridemia (Olgac, Okur, Biberoglu, Ezgu, & Tumer, 2021) which can obviously mimic LPL deficiency. Pre-prandial lactic acidosis is not part of the clinical spectrum in LPL deficiency, but it is obligatory in GSD1. If clinical features do not align with LPL deficiency consideration of alternate diagnoses is imperative since therapeutic strategies may differ.
The diagnosis of LPL deficiency in our patients, five children from four families, was confirmed through targeted genetic testing and revealed homozygous pathogenic variants in the LPL gene in all of them. The high rate of homozygosity highlights the importance of genetic counseling about the increased likelihood conceiving a child with the disorder in consanguineous couples with a family history of LPL deficiency.
The primary treatment goal in LPL deficiency is lowering serum TG levels to prevent pancreatitis. In 2012, gene therapy was developed for a subset of patients with LPL deficiency who were at increased risk for pancreatitis (Wierzbicki, Hardman, & Viljoen, 2012). The therapy showed promising initial results, including improved overall quality of life and decreased risk of pancreatitis (Kassner et al., 2018).
However, despite the positive outcomes, the therapy was discontinued reportedly due to low demand.
Currently, there is no pharmacological treatment available for LPL deficiency, making dietary modification the mainstay of long-term therapy. An LCT-restricted/MCT-supplemented diet has been successfully employed for over a decade at our institution. The success of the MCT diet can be atributed to several factors. MCTs are rapidly absorbed and metabolized, bypassing the impaired lipoprotein lipase function in LPL patients. This allows for efficient utilization of dietary fats and prevents the accumulation of TGs in the bloodstream. The use of an MCT-enriched formula led to a significant drop in TGs, with values consistently maintained below 20 mmol/L in all cases and some achieving the target range of 10 mmol/L, indicating that MCTs, which are not incorporated into chylomicrons in the small intestine but absorbed directly into the portal vein, can be effectively metabolized as a source for faty acids without exacerbating hypertriglyceridemia. The LCT restriction component of the diet limits the intake of LCT that would require functional LPL for processing. Technically that is achieved by replacing LCT with MCT while keeping the total caloric contribution of nutritional fat constant. This treatment approach is used in the management of patients with inherited long-chain faty acid oxidation defects and has been proven effective and safe (Van Calcar et al., 2020).
It is important to note that adherence to the prescribed diet plays a crucial role in achieving optimal outcomes. Patients who deviated from the diet or had difficulty maintaining dietary compliance experienced fluctuations in TG levels, emphasizing the need for ongoing education and support for patients and their families. Our patients were all closely monitored and supported by a registered dietitian to help execute the dietary principles in a practical and acceptable manner to the child and family, while adjusting the diet through changes in dietary requirements across infancy and childhood. Strategies to support dietary adherence include adjusting the MCT-supplement to the taste-preferences of the child, education on recipes and low-fat cooking techniques, education on the fat-content of foods and meal planning. In our experience, it is paramount to address dietary compliance with counseling, education, and close monitoring by a multidisciplinary team.
Since the principle of the LCT-restricted/MCT-enriched diet is the same as the ones for the treatment of inherited long-chain faty acid oxidation defects (Van Calcar et al., 2020), metabolic dietitians are proficient in calculating and directing the diet for neonates, children, and adults. Special atention is paid to avoiding deficiency of essential faty acids (Spiekerkoeter et al., 2009; Van Calcar et al., 2020). In our experience regular monitoring of faty acids in the lipid fraction of the erythrocyte membrane helps to identify deficiencies. Dietary adjustments include the supplementation of some plant oils like walnut oil that have a desirable ratio of both essential faty acids (Burns-Whitmore, Froyen, Heskey, Parker, & San Pablo, 2019).
The significance of a well-balanced diet is exemplified in the clinical course of patient 5. Diagnosed with elevated TGs in infancy and treated with fat restriction between age 6 and 12, the patient faced challenges in adhering to the low-fat diet. TGs were persistently elevated, he developed eruptive xanthomata, and had poor growth and development. After switching to the LCT-restricted/MCT-enriched diet, his metabolic control improved, his eruptive xanthomata resolved, and he had catch-up growth, emphasizing the potential of the LCT-restricted/MCT-enriched diet in managing LPL-related complications, controlling TG levels, and supporting healthy growth.
Limitations of the study include its retrospective nature, the small sample size and specifics of the patient population limiting generalizability of the findings, and the lack of a control group. Future studies with larger sample sizes, prospective designs, and longer follow-up periods would provide more robust evidence regarding the efficacy and long-term effects of an LCT-restricted/MCT-enriched diet in treatment of LPL deficiency. Despite these limitations, our findings contribute to the growing body of evidence supporting the use of dietary interventions, specifically the LCT-restricted/MCT-supplemented diet, as a viable treatment strategy for LPL deficiency.
While the MCT-based diet appears promising, it is important to recognize the challenges associated with long-term adherence. Dietary modifications can significantly impact patients’ lifestyles and may require ongoing support and education to ensure compliance. Moreover, individual variations in response to the diet may exist, as observed in patient 2-I who experienced fluctuating TG levels despite dietary intervention. This highlights the need for personalized approaches, close monitoring, and regular follow- up to optimize management outcomes.
In conclusion, the LCT-restricted/MCT-supplemented diet used in this study has been employed for over a decade at our institution and has led to good outcomes in our LPL patients. Our findings demonstrate that one can manage LPL deficiency with the diet and that one can prevent the complications associated with hypertriglyceridemia. Furthermore, the patients in achieving appropriate weight gain, linear growth, and developmental milestones indicates that dietary management supports overall health and well-being. While the MCT-based diet appears promising, it is important to recognize the challenges associated with long-term adherence. Dietary modifications can significantly impact patients’ lifestyles and may require ongoing support and education to ensure compliance. Moreover, individual variations in response to the diet may exist, as observed in patient 2-I who experienced fluctuating TG levels despite dietary intervention. It highlights the need for personalized approaches, close monitoring, and regular follow-up to optimize management outcomes. Notably, all patients in this study presented very early in life and exhibited significant elevations in TGs. That emphasizes the opportunity for early diagnosis and intervention to optimize outcomes in LPL deficiency.
Funding
LA was supported by a trainee research grant from the Garrod Association, Canada.
Abbreviations
| EFA - essential |
| faty acids |
| LCT - long-chain |
| triglycerides |
| Lipoprotein |
| Lipase - LPL |
| MCT - medium chain |
| triglycerides |
| RBC - Red blood cells |
| TG(s) – triglyceride(s) |
References
- Benlian, P.; De Gennes, J.L.; Foubert, L.; Zhang, H.; Gagne, S.E.; Hayden, M. Premature atherosclerosis in patients with familial chylomicronemia caused by mutations in the lipoprotein lipase gene. N Engl J Med 1996, 335, 848–854. [Google Scholar] [CrossRef] [PubMed]
- Brahm, A.J.; Hegele, R.A. Chylomicronaemia—Current diagnosis and future therapies. Nat Rev Endocrinol 2015, 11, 352–362. [Google Scholar] [CrossRef] [PubMed]
- Burns-Whitmore, B.; Froyen, E.; Heskey, C.; Parker, T.; San Pablo, G. Alpha-Linolenic and Linoleic Faty Acids in the Vegan Diet: Do They Require Dietary Reference Intake/Adequate Intake Special Consideration? Nutrients 2019, 11, 2365. [Google Scholar] [CrossRef] [PubMed]
- Clee, S.M.; Bissada, N.; Miao, F.; Miao, L.; Marais, A.D.; Henderson, H.E.; Steures, P.; McManus, J.; McManus, B.; LeBoeuf, R.C.; et al. Plasma and vessel wall lipoprotein lipase have different roles in atherosclerosis. J Lipid Res 2000, 41, 521–531. [Google Scholar] [CrossRef] [PubMed]
- de Pretis, N.; Amodio, A.; Frulloni, L. Hypertriglyceridemic pancreatitis: Epidemiology, pathophysiology and clinical management. United European Gastroenterol J 2018, 6, 649–655. [Google Scholar] [CrossRef] [PubMed]
- Gaudet, D.; Brisson, D.; Tremblay, K.; Alexander, V.J.; Singleton, W.; Hughes, S.G.; Geary, R.S.; Baker, B.F.; Graham, M.J.; Crooke, R.M.; et al. Targeting APOC3 in the familial chylomicronemia syndrome. N Engl J Med 2014, 371, 2200–2206. [Google Scholar] [CrossRef] [PubMed]
- Gaudet, D.; Méthot, J.; Déry, S.; Brisson, D.; Essiembre, C.; Tremblay, G.; Tremblay, K.; de Wal, J.; Twisk, J.; van den Bulk, N.; et al. Efficacy and long-term safety of alipogene tiparvovec (AAV1-LPLS447X) gene therapy for lipoprotein lipase deficiency: An open-label trial. Gene Ther 2013, 20, 361–369. [Google Scholar] [CrossRef] [PubMed]
- Gryn, S.E.; Hegele, R.A. Novel therapeutics in hypertriglyceridemia. Curr Opin Lipidol 2015, 26, 484–491. [Google Scholar] [CrossRef] [PubMed]
- Hokanson, J.E.; Brunzell, J.D.; Jarvik, G.P.; Wijsman, E.M.; Austin, M.A. Linkage of low-density lipoprotein size to the lipoprotein lipase gene in heterozygous lipoprotein lipase deficiency. Am J Hum Genet 1999, 64, 608–618. [Google Scholar] [CrossRef] [PubMed]
- Kassner, U.; Hollstein, T.; Grenkowitz, T.; Wuhle-Demuth, M.; Salewsky, B.; Demuth, I.; Dippel, M.; Steinhagen-Thiessen, E. Gene Therapy in Lipoprotein Lipase Deficiency: Case Report on the First Patient Treated with Alipogene Tiparvovec Under Daily Practice Conditions. Hum Gene Ther 2018, 29, 520–527. [Google Scholar] [CrossRef] [PubMed]
- Kobayashi, J.; Mabuchi, H. Lipoprotein lipase and atherosclerosis. Ann Clin Biochem 2015, 52 Pt 6, 632–637. [Google Scholar] [CrossRef]
- Lagerstedt, S.A.; Hinrichs, D.R.; Bat, S.M.; Magera, M.J.; Rinaldo, P.; McConnell, J.P. Quantitative determination of plasma c8-c26 total faty acids for the biochemical diagnosis of nutritional and metabolic disorders. Mol Genet Metab 2001, 73, 38–45. [Google Scholar] [CrossRef] [PubMed]
- Meyers, C.D.; Tremblay, K.; Amer, A.; Chen, J.; Jiang, L.; Gaudet, D. Effect of the DGAT1 inhibitor pradigastat on triglyceride and apoB48 levels in patients with familial chylomicronemia syndrome. Lipids Health Dis 2015, 14, 8. [Google Scholar] [CrossRef] [PubMed]
- Olgac, A.; Okur, I.; Biberoglu, G.; Ezgu, F.S.; Tumer, L. A Case of Glycogen Storage Disease Type 1a Mimicking Familial Chylomicronemia Syndrome. Balkan J Med Genet 2021, 24, 103–106. [Google Scholar] [CrossRef] [PubMed]
- Paragh, G.; Nemeth, A.; Harangi, M.; Banach, M.; Fulop, P. Causes, clinical findings and therapeutic options in chylomicronemia syndrome, a special form of hypertriglyceridemia. Lipids Health Dis 2022, 21, 21. [Google Scholar] [CrossRef] [PubMed]
- Sacks, F.M.; Stanesa, M.; Hegele, R.A. Severe hypertriglyceridemia with pancreatitis: Thirteen years’ treatment with lomitapide. JAMA Intern Med 2014, 174, 443–447. [Google Scholar] [CrossRef] [PubMed]
- Spiekerkoeter, U.; Lindner, M.; Santer, R.; Grotzke, M.; Baumgartner, M.R.; Boehles, H.; Das, A.; Haase, C.; Hennermann, J.B.; Karall, D.; et al. Treatment recommendations in long-chain faty acid oxidation defects: Consensus from a workshop. J Inherit Metab Dis 2009, 32, 498–505. [Google Scholar] [CrossRef] [PubMed]
- Van Calcar, S.C.; Sowa, M.; Rohr, F.; Beazer, J.; Setlock, T.; Weihe, T.U.; Pendyal, S.; Wallace, L.S.; Hansen, J.G.; Stembridge, A.; et al. Nutrition management guideline for very-long chain acyl-CoA dehydrogenase deficiency (VLCAD): An evidence- and consensus-based approach. Mol Genet Metab 2020, 131, 23–27. [Google Scholar] [CrossRef]
- Wierzbicki, A.S.; Hardman, T.C.; Viljoen, A. New lipid-lowering drugs: An update. Int J Clin Pract 2012, 66, 270–280. [Google Scholar] [CrossRef] [PubMed]
- Williams, L.; Rhodes, K.S.; Karmally, W.; Welstead, L.A.; Alexander, L.; Suton, L. families living with.
- Williams, L.; Rhodes, K.S.; Karmally, W.; Welstead, L.A.; Alexander, L.; Sutton, L. Familial chylomicronemia syndrome: Bringing to life dietary recommendations throughout the life span. J Clin Lipidol 2018, 12, 908–919. [Google Scholar] [CrossRef]
Figure 1.
Triglycerides and Pancreatic Enzymes in 6 patients with lipoprotein lipase deficiency. Implementation of LCT-reduced / MCT-enriched diet (black arrows). Please note exceptional events in Pts 3, 4, and 5 (empty arrows).
Figure 1.
Triglycerides and Pancreatic Enzymes in 6 patients with lipoprotein lipase deficiency. Implementation of LCT-reduced / MCT-enriched diet (black arrows). Please note exceptional events in Pts 3, 4, and 5 (empty arrows).
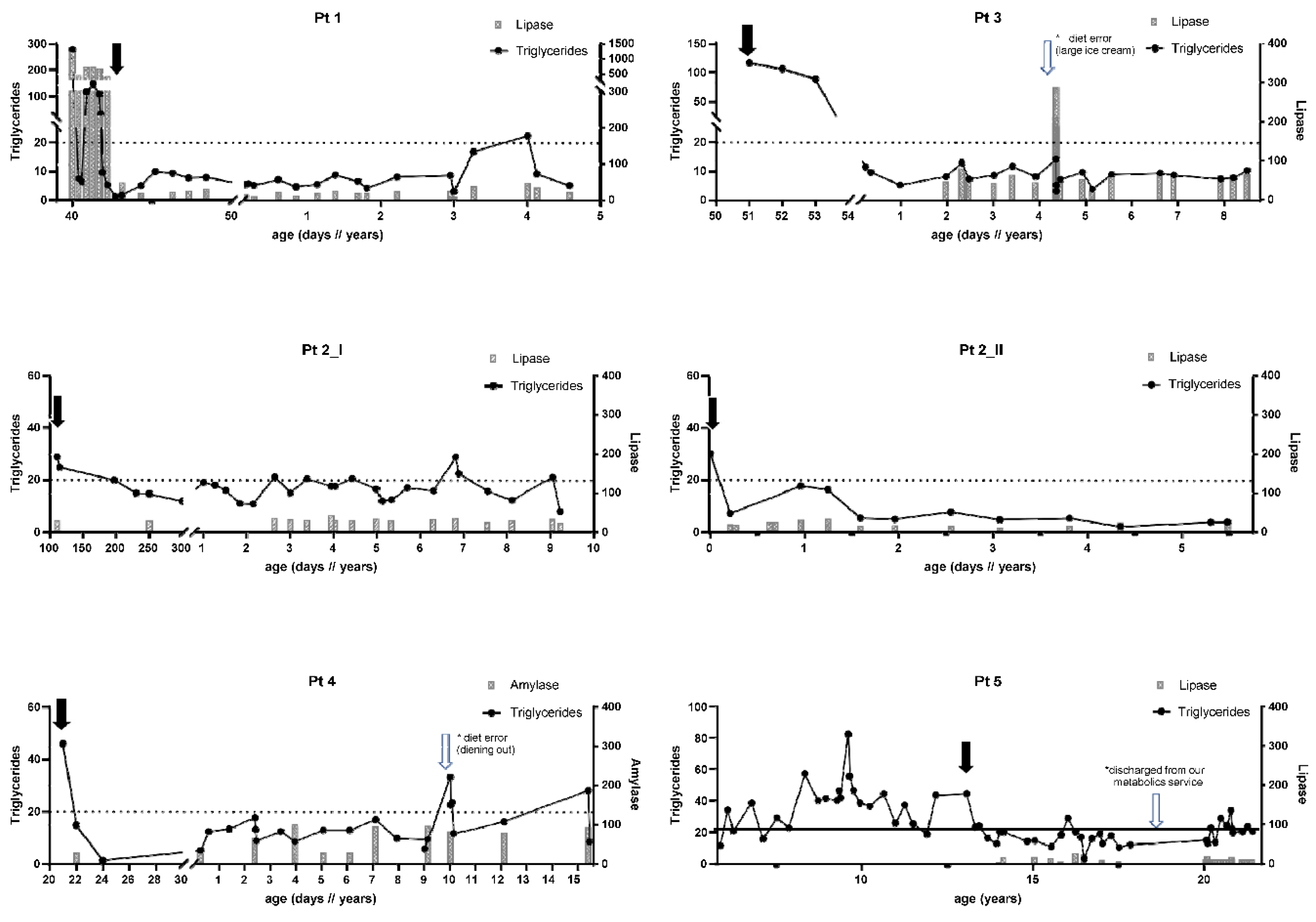
Figure 2.
Growth parameter in 6 patients with lipoprotein lipase deficiency. Growth recordings begin in patients 1-4 at the time of initiation of the LCT-restricted/MCT-enriched diet. Start of diet in patient 5 is marked with the white arrow.
Figure 2.
Growth parameter in 6 patients with lipoprotein lipase deficiency. Growth recordings begin in patients 1-4 at the time of initiation of the LCT-restricted/MCT-enriched diet. Start of diet in patient 5 is marked with the white arrow.
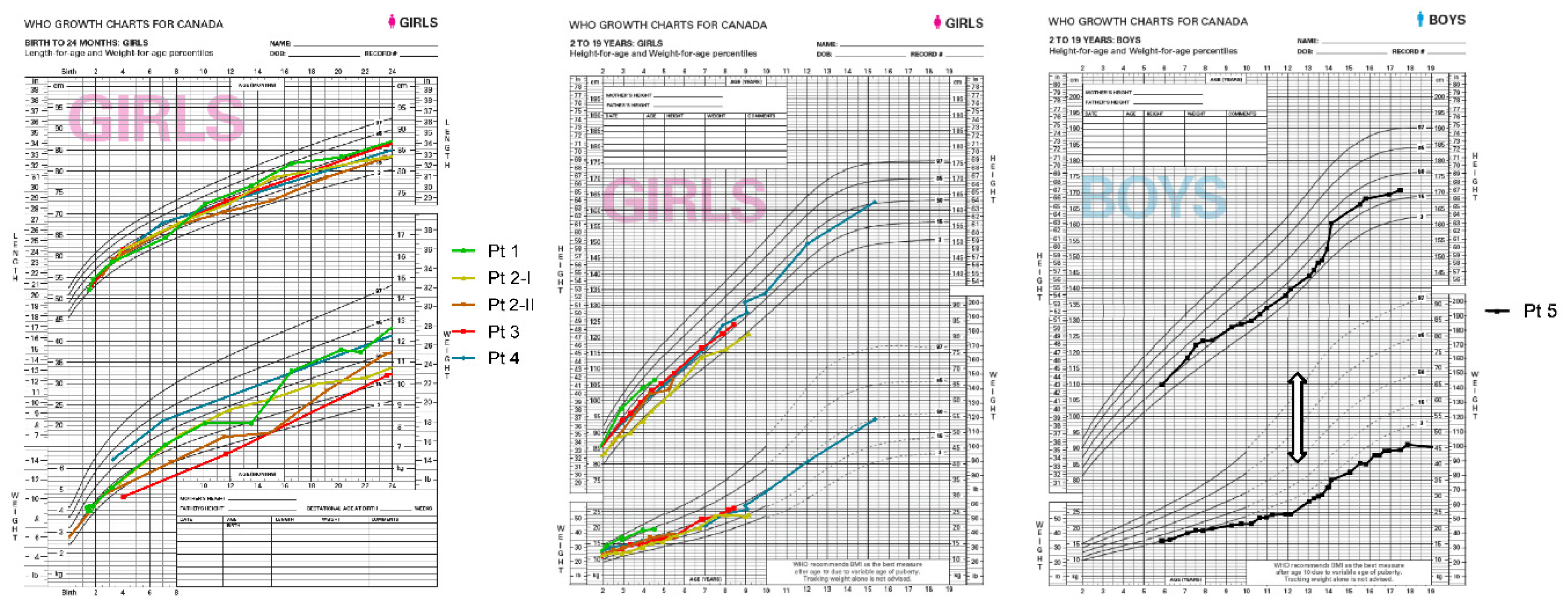

Table 1.
Demographics and Clinical Findings.
| Gender | Initial Presentation | Age at presentation |
TG at presentation |
Pancreatitis | Eruptive xanthoma |
Lipemia retinalis |
Genetics | Abdominal Ultra Sound | MRI | |
|---|---|---|---|---|---|---|---|---|---|---|
| [days] | [mmol/L] | |||||||||
| P1 | female | Vomiting, diarrhea, irritability and abdominal distension |
39 | 276 | At presentation* | No | No | LPL : c.1014 C>A, p.Tyr338* // c.1014 C>A, p.Tyr338* | Demonstrated a mass in the head of the pancreas | Abdomial MRI: Pancreatic inflammation consistent with pancreatitis. Brain MRI: No evidence of infarction or clots |
| P3 | female | Positive family history | 51 | 116 | One episode due to diet failure | No | No | LPL : c.784 C>T, p.Q262X // c.784 C>T, p.Q262X | Normal | Brain MRI: Normal |
| P2-I | female | Isolated splenomegaly was noted at a routine well-baby check-up | 110 | 29 | No | No | No | LPL : c.784 C>T, p.Q262X // c.784 C>T, p.Q262X | Splenomegaly, resolved after initiating diet | Not done |
| P2-II | female | Positive family history | 7 | 30 | No | No | No |
LPL : c.784 C>T, p.Q262X //c.784 C>T, p.Q262X ROBO3 : c.1193_1196del, p.T398Sfs*43 // c.1193_1196del, p.T398Sfs*43 |
Normal | Brain MRI: Brainstem malformation, in keeping with known ROBO3 defect Spinal MRI: Scoliosis |
| P4 | female | Lethargy, poor feeding, irritability, and abdominal distension. | 21 | 46 | No | No | No | LPL : c.472 G>A, p.A158T // c.472 G>A, p.A158T | Splenomegaly, resolved after initiating diet | Not done |
| P5 | male | Routine workup for circumcision | 14 | unknown | Chronic pancreatitis* |
Yes* | No | LPL : c.784 C>T, p.Q262X // c.784 C>T, p.Q262X | Renal US for bilateral hydronephrosis: normal | Not done |
| P6 | female | Growth failure, hepatomegaly and respiratory distress | 270 | 113 | No | No | No |
LPL : no variants G6PC : c.980_982del, p. F327del // c.563-3 C>G, p.?) |
Hepatomegaly | Not done |
*not since start of the MCT-enriched diet.
Table 2.
LCT-restricted/MCT-enriched diet in LPL patients.
| Age | MCT | LCT | LA | ALA | EER | LA | ALA | DHA | ||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| [days] | [% of total energy] |
[% of total energy] |
[% of total energy] |
[% of total energy] |
[% of EER] |
[% of total lipid fatty acid] |
[% of total lipid fatty acid] |
[% of total lipid fatty acid] |
||||||
| mean ± SD (range) |
9.47 ± 1.04 (7.39-11) |
0.097 ± 0.035 (0.027-0.167) |
3.35 ± 1.03 (1.29-5.41) |
|||||||||||
| P1 | 41 | < 6 months: Lipistart 6 months-2 years: Lipistart, MCT oil > 2 years MCT oil, MCT Procal |
Vit D | Walnut oil - since 8 months of age | 19.4 | 8.4 | 2.5 | 0.44 | 98 | 8.42 | 0.17 | 4.63 | ||
| P3 | 51 | < 1.5 years: Lipistart and Portagen 1.5-5 years: Lipistart and MCT Prolcal > 5 years: MCT Procal, MCT oil, Liquigen |
< 5 years: Phlexy vits > 5 years: Vit D and Calcium |
Walnut oil - since 8 months of age | 24.0 | 8.0 | 2.7 | 0.42 | 106 | 9.38 | 0.21 | 3.28 | ||
| P2-I | 110 | < 1.5 years: Lipistart > 1.5 years: Lipistart, MCT Procal/MCT oil/Liquigen |
< 2 years: Vit D >2 years: Phlexy vits |
Walnut oil - since 2 years of age | 22.7 | 5.5 | 2.5 | 0.40 | 104 | 7.06 | 0.12 | 3.75 | ||
| P2-II | 7 | < 12 months: Lipistart > 12 months- currently: Lipistart, MCT oil, MCT Procal |
Calcium, Vit D | Walnut oil - since 8 months of age | 22.3 | 6.6 | 2.7 | 0.41 | 100 | 6.77 | 0.09 | 4.14 | ||
| P4 | 21 | < 2 years portagen, MCT oil, > 8 years stopp portagen switch to MCT Procal |
Calcium, Vit D | Walnut oil - since 2 years of age | 11.4 | 11.8 | 2.1 | 0.33 | 103 | 8.34 | 0.41 | 3.11 | ||
| P5 | 13.4 years | 13.5-18 years: MCT Procal, Portagen, Boost Fruit Beverage | Calcium, Vit D, Iron | Walnut oil - since 13.5 years of age | 17.2 | 9.4 | 1.4 | 0.34 | 101 | 9.09 | 0.36 | 2.29 |
*Red Blood Cell Membrane Total Lipid Fatty Acid Profile. Controls: age 8.7 ± 4.6, 0-16 years (mean ± SD, range), n=44. Abbreviations: TG - triglycerides, MCT - medium chain triglycerides, LCT - long-chain triglycerides, LA - linoleic acid, ALA - alpha-linolenic acid, EER - estimated energy requirement.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



