
Submitted:
02 July 2023
Posted:
04 July 2023
You are already at the latest version
Abstract
Background: This systematic review aims to investigate whether percutaneous transhepatic gallbladder drainage (PTGDB), as definitive treatment, is superior to emergency cholecystectomy (EC) in high-risk patients with acute cholecystitis (AC).
Material and methods: A systematic literature search was performed until December 2022 using Scopus, Medline/PubMed and Web of Science databases in order to compare PTGDB as definitive treatment vs EC in AC.
Results: Seventeen studies (1 Randomized Control Trials and 16 observational studies) have been included with a total of 783,672 patients (32,634 treated with PTGDB vs 4,663 who underwent laparoscopic cholecystectomy, 343 who underwent open cholecystectomy and 746,032 who underwent cholecystectomy, but without laparoscopic or open approach being specified). The quality assessment (ROBINS-I) of the not randomized studies showed a serious risk, differently the evaluation of the randomized study (RoB 2) showed a low risk of bias. Analysis of the results shows that PTGDB, despite being minimally invasive, do not have different incidence of complications than EC (RR 0.77 95% CI [0.44 to 1.34]; I2 = 99%; P=0.36). A lower postoperative mortality was reported in patients who underwent EC (2.37%) than in PTGDB group (13.78 %) (RR 4.21; 95% CI [2.69 to 6.58]; P < 0.00001), furthermore the risk of hospital readmission for biliary complications (RR 2.19 95% CI [1.72 to 2.79]; I2 = 48 %; P<0.00001) and hospital stay (MD 4.29 95% CI [2.40 to 6.19]; P<0.00001) were lower in EC group.
Conclusions: No advantage in using PTGDB as a definitive treatment over EC in the management of critically ill patients with AC has been demonstrated; the results of our systematic review and meta-analysis suggest using EC as the treatment of first choice, even for very high-surgical-risk patient in which PTGDB should be reserved. The major limitation of this systematic review and meta-analysis is associated to a low quality of evidence for the serious bias in the not randomized studies. For this reason, new high powered and well-designed clinical trials are needed to recommend PTGDB as definitive treatment in patients unfit for surgery or those who refuse to undergo surgery.
Keywords:
acute cholecystitis
; percutaneous cholecystectomy
; cholecystectomy
INTRODUCTION
Acute cholecystitis (AC), typically due to gallstone obstruction of the cystic duct, affects about 200,000 people in the United States each year [1]. For more than a century, open cholecystectomy (OC) was the gold standard [2], while laparoscopic cholecystectomy was introduced in the 1980s [3] and is now the worldwide accepted gold standard [4]. Its success was due to its advantages of less postoperative pain, better cosmetic results and shorter hospital stay with respect to the open approach [5].
In the common clinical practice, early laparoscopic cholecystectomy, performed within three days of diagnosis, is the first line of treatment for AC [6,7,8,9,10]. Recently, the WSES (World Society of Emergency Surgery) guidelines suggested performing a laparoscopic cholecystectomy “as soon as possible, within 7 days from hospital admission and within 10 days from the onset of symptoms” [11].
Nowadays, the choice of treatment is still a dilemma in patients with high risk for severe underlying disease or acutely poor general conditions [12]. In these cases, a percutaneous transhepatic gallbladder drainage (PTGBD) is a minimally invasive technique allowing an immediate drain and decompression of the gallbladder, with a prompt clinical response and few procedure-related complications [13]. In the common clinical practice, PTGBD can be preferred as a bridge to surgery over emergency upfront surgery in unfit patients with AC [14,15], but PTGBD as definitive treatment in extremely high-risk patients is still matter for debate [16]. Therefore, for each case, a tailored and shared decision-making process is mandatory [17].
However, up until now, few studies managed to compare the results of both approaches, leaving open the discussion of which is the best solution.
This systematic review and meta-analysis of the literature aims to compare two treatment options, PTGBD as definitive treatment vs EC, comparing their efficacy and safety in the management of a high-risk surgical patients with AC.
MATERIALS AND METHODS
The protocol for this systematic review and meta-analysis was registered (CRD42021126286) on the PROSPERO repository (http://www.crd.york.ac.uk/prospero). The search of the scientific literature was performed until 15 December 2022, in accordance with the updated PRISMA guidelines for reporting systematic reviews and meta-analyses [18].
Relevant Literature comparing definitive PTGBD vs EC in AC was searched using the Scopus, Medline/PubMed and Web of Science (Web of Science Category: Surgery) databases. The studies comparing PTGBD vs conservative medical treatment, those using percutaneous cholecystostomy as a “bridge” to cholecystectomy, and those analyzing the outcomes of only one of the two approaches were excluded. In these steps, randomized controlled trials (RCTs), retrospective comparative studies (RCSs), prospective controlled studies (PCSs), and studies from administrative databases (SAD) were selected. All articles were included irrespective of the language. The references of all included studies were checked to identify other relevant papers.
The following keywords were used for Literature search: “acute cholecystitis OR severe cholecystitis OR cholecystectomy OR laparoscopic cholecystectomy OR open cholecystectomy AND cholecystostomy OR percutaneous cholecystostomy OR gall bladder drain OR gallbladder tube OR transhepatic gallbladder drain OR transhepatic gallbladder tube OR cholecystostomy tube.” Two Authors (R.C. and G.B.) independently reviewed the included studies in accordance with the updated PRISMA guidelines for systematic reviews.
To minimize retrieval bias, a manual search was performed through the Google Scholar database.
The search for ongoing clinical studies was performed on ClinicalTrials.gov.
The following data were extracted from the studies:
The following data were extracted from the studies:
- authors and year of publication
- type of study
- countries and facilities involved
- timing of treatments
- number of patients included
-
characteristics of patients included:
- age;
- gender;
- comorbidities;
- BMI (“body mass index”);
- ASA (“American Society of Anesthesiologists physical status”);
- diagnostic criteria used for acute cholecystitis;
-
type of percutaneous cholecystostomy:
- transperitoneal drainage;
- transhepatic drainage;
-
type of surgical treatment:
- laparoscopic cholecystectomy;
- open cholecystectomy.
The primary endpoints were the following:
- postoperative mortality;
- emergency surgical treatment;
- readmission for biliary complications.
The secondary endpoints were:
- overall postoperative complications;
- major postoperative complications;
- emergency reinterventions;
- length of hospital stay.
The statistical analysis of data was conducted with the Review Manager software (RevMan version 5.4.1) (Copenhagen: The Nordic Cochrane Center, The Cochrane Collaboration, 2018).
The results of the first analysis were examined by evaluating the Risk Ratio for dichotomous variables, while weighted mean differences (WDM) were considered for continuous variables. The statistical model used for the meta-analysis was the random-effects Mantel-Haenszel method, and the results were summarized using Forest Plots. Heterogeneity of the studies was measured by the Cochran’s Q test of heterogeneity and was quantified by Higgins’ index (I2) with 95% confidence intervals.
The risk of bias of the included studies was performed by the Authors (G.B. and R.C.). Methodological assessment of the included studies was performed with a revised tool for assessing risk of bias in randomized trials (RoB 2) [19] and the Risk of Bias in Non-randomized Studies of Interventions (ROBINS-I) assessment tool [20]. Finally, the GRADE was utilized to perform analysis of the evidence (GRADEpro GDT. McMaster University and Evidence Prime Inc, 2021).
RESULTS
Literature search
The results of the systematic review of literature are reported in the Supplementary Figure 1. The initial search yielded 2079 potentially relevant articles and 13 articles from additional papers were identified through other sources (grey literature). After removing duplicates and analyzing the remaining titles, abstracts and additional articles, 31 studies remained for full-text analysis. Of these, 14 were excluded because of lack of data; therefore, only 17 articles were included: 1 RCT [21]; 2 PCS [22,23]; 8 RCS [24,25,26,27,28,29,30,31] and 6 SAD [32,33,34,35,36,37].
Characteristics of the included studies. The characteristics of the included studies are summarized in Table 1.
The total number of patients included was 783,672:
- -
- 32,634 treated with percutaneous drainage;
- -
- 4,663 underwent laparoscopic cholecystectomy,
- -
- 343 underwent open cholecystectomy,
- -
Characteristics of included participants. The characteristics of included cases are reported in the ssupplementary Table 1.
All studies, excluding Abi Hadair’s, provided information on the gender of included patients, showing prevalence of male subjects [24]. All the 17 studies reported the age of the patients, but this variable was not comparable. As a matter of fact, the Authors used either mean or median age, that are not comparable. However, the patients who underwent percutaneous drainage had an older age with respect to those who had EC. BMI has been assessed by few studies [21,24,25,29]; La Greca et al. reported that the BMI was analyzed, but they did not provide further data in this regard [27]. Surgical risk was assessed in all studies, but different classifications of surgical risk were used. The most common was the ASA scale. In the study by Melloul et al., the Authors preferred the SAPS II [28], Loozen et al. used the APACHE [21], Latif et al. reported both ASA and APACHE, while others did not specify how they assigned patients into a high surgical risk class [30].
Diagnostic parameters. The findings of the diagnostic pathways for acute cholecystitis are reported in supplementary Table 2. Nine of seventeen studies used the diagnostic criteria given by the Tokyo guidelines [15]; while SAD used ICD-9 as the database to search for patients with acute cholecystitis. The study by Smith et al. generically indicates that they based the diagnosis on clinical and laboratory and radiological data but provides no further details [31], while the study by Garcés-Albir et al. does not specify how they selected patients [26].
Type of percutaneous drainage technique performed. The type of percutaneous gallbladder drainage technique performed is reported in Table 2:
- -
- in 7 studies transhepatic access was used;
- -
- in 2 studies the access was transperitoneal;
- -
- in the study by Loozen et al.[21] , both techniques were used;
- -
- 7 studies did not specify the preferred technique.
After the procedure, the PTGBD was removed after a heterogeneous length of time. In actual facts, there is no clear standard for this. I n the included studies, the time of PTGBD removal was highly variable, ranging from two to nine weeks. All studies indicated that they removed the catheter after the patients’ clinical condition stabilized. Only the RCT by Loozen et al.[21] suggested that an anterograde cholangiography be performed before catheter removal to assess duodenal reflux and cystic duct patency.
Quality assessment of RCTs. The RCT by Loozen et al.[21] (supplementary Figure 2) reported a low risk in the evaluation of random sequence generation. The study reports allocation concealment and blinding of outcome assessment and thereby has lower risk of bias.
Quality assessment of non-RCTs. According to the ROBINS-I tool, risk-of-bias judgement may be identified as few, moderate, serious or critical (supplementary Figure 3). Regarding bias due to confounding, five studies were evaluated to have a moderate risk; on the other hand, seven studies have a severe risk and three a critical risk of bias due to confounding. The most common conditions were a higher Charlson Co-morbidity Index and severity of ASA in the PTGBD group. Analyzing the bias in the selection of participants, eight of ten reviews were evaluated as serious risk, in fact the patients’ characteristics were not homogeneous; the patients recruited in the PTGBD group were older than the patients in the EC group. In some studies, a significant difference in BMI was reported. Bias in classifying interventions was severe in seven studies, as they do not report the type of percutaneous access. The length of time associated with percutaneous drainage was not reported in several studies. The bias due to deviation from intended intervention was serious in all studies. The bias from missing data related to acute cholecystitis was moderate in 6 studies and serious in 10. The bias in measurement of outcomes was moderate in 6 studies and serious in 10.
Analysis of results: Primary outcomes
Postoperative mortality. This outcome was evaluated in sixteen studies with a total of 776,706 patients. There was a reduction in the incidence of postoperative mortality in the group undergoing cholecystectomy (2.37% (17,716/747,283)) compared to the value found in the group undergoing percutaneous drainage (13.78 % (4,057/29,423)). The result was statistically significant (RR 4.21; 95% CI [2.69 to 6.58]; P < 0.00001). Heterogeneity was extremely high in the overall analysis (I2= 99%) (Figure 1).
The analysis of the different type of studies reported a higher heterogeneity value in the SAD type (I2 = 100%), and very low in the other study types: prospective cohort studies (0%) and retrospective cohort studies (37%).
All studies reported lower postoperative mortality in the group undergoing EC:
- RCT: PTGBD group 8.82% (6/68) vs EC group 3.03% (2/66) (RR 2.91; 95% CI [0.61 to 13.91]; P 0.18).
- Prospective cohort studies: PTGBD group 13.95% (6/43) vs 0 (0/40) of EC group; this result was not statistically significant (RCTs: RR 2.91 95% CI [0.61 to 13.91]; P=0.18).
- Retrospective cohort: there was an advantage of the EC group (1.45%) (14/966) over the PTGBD group (8.35%) (56/870), but in this case the result was statistically significant (RR 4.59 95% CI [2.11 to 9.96]; P=0.0001).
- Studies from administrative databases: the mortality was 2.37% in the group undergoing cholecystectomy vs 13.92% in the group undergoing PTGBD, and this difference was statistically significant (RR4.10 95%CI [2.29 to 7.33]; P<0.00001).
Risk of bias was unclear, as studies report general “postoperative mortality” but not 30-day mortality specifically.
The subgroup analysis of laparoscopic EC was performed in eight studies (1,162 patients) and reported an advantage of laparoscopy with a mortality of 1.98% (12/604) compared to 7.34% (41/558) in the PTGBD group. The result was statistically significant (RR 3.00, 95% CI [1.61 to 5.60]; P=0.0005).
Overall postoperative complications. Eleven studies analyzed this outcome (746,810 patients). The incidence of postoperative complications was similar between the two groups: 11.15% (3,090/27,707) PTGBD compared with 9.06% (65,167/719,103) in the EC, but the result did not reach statistical significance (RR 0.77 95% CI [0.44 to 1.34]; I2 = 99%; P=0.36). The analysis of different types of studies reported a higher heterogeneity value in SAD (I2 = 100%) and retrospective cohort studies (I2=89%) while it was moderate in prospective cohort studies (64%). Only the analysis of prospective studies reported an advantage of the PTGBD group (20.93%, 9/43) over the EC group (35%, 14/40), but statistical significance was not reached (RR 0.45, 95% CI [0.08 to 2.59]; P=0.37) (Figure 2). In the analysis of the retrospective group (40.41% in PTGBD group (97/240) vs 58.1% in EC group (208/358) and SAD (10.88% (2,984/27,424) in PTGBD group vs 9.03% (64,945/718. 705) in the EC group), the rates were very similar, but statistical significance was reached only in the SAD (RR 0.8 95% CI [0.42 to 1.55]) P=0.52 for the retrospective group, (RR 0.88; 95% CI [0.34 to 2.25]) P<0.00001 for the SAD). The risk of bias was found to be unclear; in fact, the Authors report only “postoperative complications” and do not report 30-day mortality specifically.
Subgroup analysis of five LC studies (419 patients) showed a lower rate of complications in the PTGBD group (27.09%) compared to the LC group (48.14%) but the result was not statistically significant (RR 0.59 95% CI [0.27 to 1.29]; P=0.19).
Emergency reinterventions. This outcome was analyzed in five different studies with a total of 630 patients. The rate of emergency reintervention was lower in the EC group (2.93%) than in the PTGBD group (12.54%) but the result obtained did not reach statistical significance (RR 3.75 95%CI [0.92 to 15.33]; I2 = 63%; P=0.07) (Figure 3).
Subgroup analysis of three studies with laparoscopic surgery (368 patients) showed similar results: 5.18% with laparoscopic EC compared with 8.57% with the PTGBD. However, the result did not reach statistical significance (RR 1.36 95% CI [0.64 to 2.87]; P=0.42)
Abdominal Abscess. Two studies evaluated this outcome (238 patients). The result shows a lower incidence of abdominal abscess in the PTGDB group 0.94% (1/107) compared with 1.53% (2/131) in the EC group (RR 0.70, 95% CI [0.09 to 5.52]; I2 = 0%; P 0.73) (Supplementary Figure 4).
Analysis of results: Secondary outcomes
Major postoperative complications. Four studies reported this endpoint for a total of 485 patients. The incidence of major postoperative complications was higher (30.76%) in the PTGBD group, compared with the surgical group (11.15%), but did not reach statistical significance (RR 1.60 CI 95% [0.44 to 5.84]; I2 = 86%; P=0.47) (Supplementary Figure 5).
The study by Loozen et al. [21] reported a significant advantage for the EC group with a complication rate of 12.12% compared to 64.7% found in the PTGBD group (RR 5.34 CI 95% [2.72 to 10.46] P<0.00001). While retrospective cohort studies that analyzed this outcome reported an advantage for the PTGBD group but did not demonstrate statistical significance.
The subgroup analysis of LC studies is comparable to the one of the overall study analyses.
Length of hospital stay. Twelve studies have reported this outcome (780,111 patients). Length of hospital stay was statistically lower in the EC group than in the PTGBD group (MD 4.29 95% CI [2.40 to 6.19]; P<0.00001) (Supplementary Figure 6). In the overall analysis, heterogeneity was extremely high (I2=100%); subgroup analysis reported a higher heterogeneity value in SAD (I2 = 100%), while it was very low in the analysis of prospective cohort studies (0%) and retrospective cohort studies (52%). The analysis of the randomized controlled trial and retrospective cohort studies reported a shorter length of hospital stay in the group that underwent cholecystectomy; however, the result was not statistically significant. In contrast, the analysis of prospective cohort studies and SAD showed a shorter length of hospital stay in the surgical group than in the group undergoing percutaneous drainage, reaching statistical significance.
Subgroup analysis of five LC studies (361 patients) favor the laparoscopic access, and the result reached statistical significance (MD 3.30, 95% CI [1.05 to 5.56]; P=0.004).
Hospital readmission for biliary complications. Seven studies reported this outcome (8,863 patients). The result shows a significant increase in the incidence of postoperative complications in the PTGBD group: 21.56% (918/4256) compared with 10.96% (505/4,607) in the EC group (RR 2.19 95% CI [1.72 to 2.79]; I2 = 48 %; P<0.00001) (Figure 4).
In addition, subgroup analysis of four studies with a total of 717 patients favors of laparoscopic access with a readmission rate of 4.27% compared with 20.69% in the PTGBD group, and again, the result reached statistical significance (RR 4.33, 95% CI [2.64 to 7.10] P<0.00001).
Results of GRADE (Grading of Recommendations, Assessment, Development, and Evaluations) analysis. Overall evidence of the four critical outcomes (post-operative 30-day mortality, overall post-operative complications, intra-abdominal abscess and emergency re-intervention) was evaluated with GRADE (Figure 5) and the quality of evidence was low in all analyzed outcomes. For this reason, PTGBD as definitive treatment should not be used in the treatment of AC for its lower benefit ratio compared to EC; we suggested that PTGBD as definitive treatment could be used only in critically ill patients for whom surgery is at very high risk (strength of recommendation “weakly positive “).
DISCUSSION
In cases of AC in patients with high surgical risk, the Tokyo 2018 guidelines mention PTGBD as an alternative to EC [15]. There are few studies comparing the two different treatment approaches and, to date, only one randomized clinical trial [21]. The studies supporting PTGBD as a definitive treatment are almost all retrospective, dated or based on a limited number of cases [22,23,24,25,26,27,28,29,30,31,32,33,34,35,36,37]; therefore, it can be stated that the current medical literature does not provide solid evidence of the benefits of PTGBD.
This systematic review and meta-analysis were conducted to analyze the advantages and disadvantages of PTGBD as a definitive treatment compared with EC in the management of the critically ill patient with AC. Seventeen studies with a total of 783,672 patients were analyzed.
The study showed that EC is superior to PTGBD in the treatment of high risk patients with acute cholecystitis. In fact, significant benefits of cholecystectomy were found in terms of lower postoperative mortality (2.37% in the EC compared with 13.78% in PTGBD) (RR 4.21; 95% CI [2.69 to 6.58]; P < 0.00001), decreased incidence of hospital readmission for biliary complications (10.96% in the EC group compared with 21.56% in the PTGBD group) (RR 2.19 95% CI [1.72 to 2.79]; I2 = 48 %; P<0.00001), and shorter length of hospital stay (MD 3.30, 95% CI [1.05 to 5.56]; P=0.004). The analysis of other endpoints favor EC, in the absence of statistically significant values; in fact, a trend towards fewer overall postoperative complications (9.06% vs 11.15%) (RR 0.77 95% CI [0.44 to 1.34]; I2 = 99%; P=0.36), fewer major postoperative complications (11.15 vs 30.76%) (RR 1.60 CI 95% [0.44 to 5.84]; I2 = 86%; P=0.47) and fewer emergency reinterventions (2.93% vs 12.54%) (RR 3.75 95%CI [0.92 to 15.33]; I2 = 63%; P=0.07) were demonstrated in the group undergoing EC compared with the PTGBD group.
The controversies about the use of PTGBD are due to the fact that studies conducted up until now on the subject led to conflicting conclusions. Several observational studies have demonstrated a high short-term success rate of PTGBD in high-risk patients with AC. According to Griniatsos et al. [38], it is possible to perform PTGBD as definite treatment in 100% of the 24 patients included in the study, procedure-related mortality was only 4% while improvement of the clinical and laboratory picture as well as resolution of sepsis occurred in 90.5% of cases within 72 hours of PTGBD. McKay et al. [39] conducted a retrospective study published in 2012 using a larger sample: of the 68 patients included, the acute episode of AC was successfully treated in 58 patients (85%), while 10 patients (15%) died in the hospital. The results of a 10-year experience of PTGBD use in Denmark showed that the procedure-related mortality rate was 4.7 percent, and 234 patients out of the total of 278 were discharged without complications, considering them adequately treated with cholecystostomy [40].
Some Authors even suggest PTGBD as a first-line treatment in all high-risk patients with acute cholecystitis [28,32,41,42,43].
However, it is crucial to consider that in support of PTGBD there are mostly retrospective studies, with small sample sizes, and without control group (i.e., a group of patients undergoing EC). In addition, many patients who have PTGBD need definitive cholecystectomy at some point after the procedure, because of recurrence of biliary symptoms if the drainage is removed, resulting in morbidity and mortality rates that are generally difficult to monitor and document over time [44,45].
These data suggest that real PTGBD-related mortality may likely be higher than it as reported in the above studies.
Furthermore, when compared to EC, cholecystostomy seems to be related to a higher mortality rate: 10.8% in PTGBD compared to 0.9% in the cholecystectomy [46] and this difference was statistically significant.
A systematic literature review of 53 studies published in 2009, defines cholecystostomy as a minimally invasive procedure with a high success rate (85.6%) and low related mortality (0.36%); however, 30-day mortality is high (15.4%), in contrast to the one related to cholecystectomy (4.5%) [47].
Our systematic review and meta-analysis demonstrate that EC is a safer treatment than PTGBD in critically ill patients.
Another interesting finding is about the rate of hospital readmission for biliary complications, which is significantly higher in the PTGBD than in the EC (21.56% vs 10.96%) (RR 2.19 95% CI [1.72 to 2.79]; I2 = 48 %; P<0.00001). Previous studies showed that performing upfront cholecystectomy on elderly patients prevents further episodes of gallstone-related disease, reduces readmission rates, and is associated with lower overall healthcare costs [48,49,50,51,52].
According to the study by Riall et al. [53], patients who did not undergo cholecystectomy experience gallstone disease-related hospital readmissions within 2 years more frequently than those who underwent cholecystectomy (38% vs 4%).
A meta-analysis of 32 studies [54], 9 of them randomized controlled trials, published in 2022, confirmed that the results of the group undergoing cholecystectomy after PTGBD were superior to those of the EC group in terms of postoperative complications (RCTs: RR 0.28, 95% CI 0.14 to 0.56, I2 = 63%). The incidence of intra-abdominal abscess, blood loss, conversion to laparotomy, partial cholecystectomy, operative time and wound infection was also lower in the PTGBD group than in the EC group.
If the patients in the present study had undergone elective cholecystectomy after percutaneous drain placement, it is possible that the rate of biliary complications and the risk of hospital readmission would be reduced. On the other hand, one of the advantages of PTGBD is to avoid surgery-related complications, which is why several Authors still suggest that patients at high surgical risk should not undergo elective cholecystectomy after percutaneous drainage [38,43,55,56].
According to our experience, only patients particularly at risk for recurrent biliary disease (acute cholecystitis, choledocholithiasis, pancreatitis) should undergo cholecystectomy. Unfortunately, up until now there is no evidence of any clinical, biochemical or radiological predictor of the risk of biliary complications in those patients. Antegrade cholangiography could aid in the selection of patients for elective surgery, but prospective studies on this topic are yet to come.
This meta-analysis, despite the very large number of patients, has limitations that must be acknowledged.
First, some Authors, in a large number of patients, did not mention whether an open or laparoscopic surgery was performed.
Second, the selection bias is arising directly from the inclusion of eight retrospective cohort studies. In fact, the higher mortality rate found in patients undergoing cholecystostomy may be due to the fact that PTGBD is usually considered in elderly and severely comorbid patients.
Moreover, there are critical issues related to the use of administrative databases determined mainly by the incompleteness and/or inadequacy of clinical information such as age, gender, BMI or lifestyle information of patients. These confounding factors were not always reported correctly and thus could not be analyzed.
Furthermore, as highlighted in the results, the included studies are heterogenous regarding the criteria used to establish the diagnosis and severity of acute cholecystitis (Tokyo guideline criteria, ICD-9, clinical, laboratory and radiological data). Surgical risk was also estimated using different classification systems (ASA-PS, APACHE II, SAPS II). These are key factors that contributed to the heterogeneity of the meta-analysis.
A further concern is about the selection of patients to be treated with PC. This approach was reserved to subjects considered to be at a higher operative risk, elderly, comorbid, or with high-grade cholecystitis; this may account for the greater bias in the data collected.
TG18 recommends that PTGBD followed by Lap-C should be performed first in high-risk patients for emergency surgical treatment. That is, it is recommended to perform PTGBD as a bridge to elective surgery. Successively some surgeons suggest considering PTGBD as definitive treatment in high-risk patients [15]. However, more recent evidence show that those guidelines may have overestimated the role of PTGBD and that these patients would get a larger benefit from cholecystectomy [21,46]. It must be considered that the only randomized trial publish until now on this topic is the CHOCOLATE study by Loozen et al.[21] , which showed that laparoscopic cholecystectomy is better than percutaneous drainage in high-risk patients with acute cholecystitis. The aforementioned study demonstrated that LC was associated to lower postoperative mortality (3% vs 9%), lower rate of major complications (12% vs 65%), lower incidence of cholecystitis-related reinterventions (12% vs 66%), lower recurrence of biliary disease (5% v 53%), and also shorter hospital stay including readmissions (5 days vs 9 days) [21].
PTGBD may be an acceptable treatment choice when surgery is absolutely contraindicated, i.e., recent myocardial infarction (MI) (<6 weeks) or acute cerebrovascular accident.
In view of the detected bias of the published studies and the results obtained in the present systematic review, it is clear that further studies with stricter criteria are needed to evaluate clinical, biochemical, and/or radiological factors which are predictive of failure of the percutaneous drainage in acute cholecystitis. Strong evidence-based guidelines are most needed on the real indications for PTGBD, specifying the timing with respect to the onset of symptom, the route of catheter insertion (transhepatic or transperitoneal), and the length of time the catheter should remain in place. At the moment, it is also extremely difficult to compare the results of PTGBD from different centers. On the contrary, indications, technique and follow-up of PTGBD should be standardized, so that it would be possible to select patients who could truly benefit from this treatment and those who, on the contrary, could be candidate to upfront emergency cholecystectomy.
CONCLUSIONS
In this systematic review the majority of studies have very low-quality evidence and more RCTs are needed; furthermore, the meta-analysis reported that PTGBD is inferior in the treatment of AC in high-risk patients and does not demonstrate any advantage in using PTGBD as a definitive treatment over EC in the management of critically ill patients with acute cholecystitis. The definition of high-risk patients is important in interpreting the results, but the methods of assessment and definitions differ between studies. The analysis of our results shows that PTGBD, despite being minimally invasive, is burdened with a higher incidence of complications with respect to EC. The lower postoperative mortality, lower risk of hospital readmission for biliary complications and shorter hospital stay times suggest considering upfront cholecystectomy as the treatment of choice, even for patients at high surgical risk.
Probably, the inferiority of PTGBD versus early LC for high-risk patients may likely be related to an association of various patient-side factor conditions and the severity of acute cholecystitis. Nowadays, percutaneous cholecystostomy should be reserved only to patients with very poor general conditions on whom surgery is not feasible or appropriate, or as a bridge to elective surgery in patients whose general conditions can be improved after an initial damage control procedure.
Acknowledgments
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors. All authors substantially contributed to the manuscript. All authors read and approved the final version of the manuscript. No funding was received for the present study. For this clinical case: no ethics commission has met.
References
- Gallaher JR, Charles A. Acute Cholecystitis: A Review. JAMA. 2022; 327(10):965-975. [CrossRef]
- Carvalho GL, Lima DL, Shadduck PP, de Góes GHB, Alves de Carvalho GB, Cordeiro RN, Calheiros EMQ, Cavalcanti Dos Santos D. Which Cholecystectomy do Medical Students Prefer? JSLS. 2019; 23(1):e2018.00086 [CrossRef]
- Blum CA, Adams DB. Who did the first laparoscopic cholecystectomy? J Minim Access Surg. 2011; 7(3):165- 8. [CrossRef]
- McSherry CK. Cholecystectomy: the gold standard. Am J Surg. 1989; 158(3):174-8. [CrossRef]
- Keus F, de Jong JA, Gooszen HG, van Laarhoven CJ. Laparoscopic versus open cholecystectomy for patients with symptomatic cholecystolithiasis. Cochrane Database Syst Rev. 2006 Oct 18;(4):CD006231. [CrossRef]
- Ansaloni L, Pisano M, Coccolini F, et al. 2016 WSES guidelines on acute calculous cholecystitis. World J Emerg Surg. 2016 Jun 14; 11:25. [CrossRef]
- Gurusamy KS, Davidson C, Gluud C, Davidson BR. Early versus delayed laparoscopic cholecystectomy for people with acute cholecystitis. Cochrane Database Syst Rev. 2013;30(6):CD005440. [CrossRef]
- Zhou MW, Gu XD, Xiang JB, Chen ZY. Comparison of clinical safety and outcomes of early versus delayed laparoscopic cholecystectomy for acute cholecystitis: a meta-analysis. Sci World J. 2014. [CrossRef]
- Wu XD, Tian X, Liu MM, Wu L, Zhao S, Zhao L. Meta-analysis comparing early versus delayed laparoscopic cholecystectomy for acute cholecystitis. Br J Surg. 2015; 102:1302–1313. [CrossRef]
- Cao AM, Eslick GD, Cox MR. Early Cholecystectomy is superior to delayed cholecystectomy for acute cholecystitis: a meta-analysis. J Gastrointest Surg. 2015;19:848–857. [CrossRef]
- Pisano M, Allievi N, Gurusamy K, et al. 2020 World Society of Emergency Surgery updated guidelines for the diagnosis and treatment of acute calculus cholecystitis. World J Emerg Surg. 2020 Nov 5;15(1):61. [CrossRef]
- Schuster KM, Holena DN, Salim A, Savage S, Crandall M. American Association for the Surgery of Trauma emergency general surgery guideline summaries 2018: acute appendicitis, acute cholecystitis, acute diverticulitis, acute pancreatitis, and small bowel obstruction. Trauma Surg Acute Care Open. 2019; 4(1):e000281 [CrossRef]
- Elsharif M, Forouzanfar A, Oaikhinan K, Khetan N. Percutaneous cholecystostomy… why, when, what next? A systematic review of past decade. Ann R Coll Surg Engl. 2018 Oct 5;100(8):1-14. [CrossRef]
- Stanek A, Dohan A, Barkun J, et al. Percutaneous cholecystostomy: A simple bridge to surgery or an alternative option for the management of acute cholecystitis? Am J Surg. 2018 Sep;216(3):595-603. [CrossRef]
- Okamoto K, Suzuki K, Takada T, et al. Tokyo Guidelines 2018: flowchart for the management of acute cholecystitis. J Hepatobiliary Pancreat Sci. 2018 Jan;25(1):55-72. [CrossRef]
- Malik A, Seretis C. Use of percutaneous cholecystostomy for complicated acute lithiasic cholecystitis: solving or deferring the problem? Pol Przegl Chir. 2021; 93(0):7-12. [CrossRef]
- Filiberto AC, Efron PA, Frantz A, Bihorac A, Upchurch GR Jr, Loftus TJ. Personalized decision-making for acute cholecystitis: Understanding surgeon judgment. Front Digit Health. 2022; 4:845453. [CrossRef]
- Page MJ, McKenzie JE, Bossuyt PM, et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. BMJ. 2021; 372: 71. [CrossRef]
- Sterne JA, Savović J, Page MJ, et al. RoB 2: a revised tool for assessing risk of bias in randomised trials. BMJ. 2019 Aug 28;366:l4898. [CrossRef]
- Sterne JA, Hernán MA, Reeves BC, Savović J, Berkman ND, Viswanathan M, et al. ROBINS-I: a tool for assessing risk of bias in non-randomised studies of interventions. BMJ. 2016;355:i4919.
- Loozen CS, van Santvoort HC, van Duijvendijk P, et al. Laparoscopic cholecystectomy versus percutaneous catheter drainage for acute cholecystitis in high risk patients (CHOCOLATE): multicentre randomised clinical trial. BMJ. 2018; 363:k3965. [CrossRef]
- Rodríguez-Sanjuán JC, Arruabarrena A, Sánchez-Moreno L, González-Sánchez F, Herrera LA, Gómez-Fleitas M. Acute cholecystitis in high surgical risk patients: percutaneous cholecystostomy or emergency cholecystectomy? Am J Surg. 2012; 204(1):54-9. [CrossRef]
- Somuncu E, Kara Y, Kızılkaya MC, et al. Percutaneous cholecystostomy instead of laparoscopy to treat acute cholecystitis during the COVID-19 pandemic period: single center experience. Ulus Travma Acil Cerrahi Derg. 2021; 27(1):89-94. [CrossRef]
- Abi-Haidar Y, Sanchez V, Williams SA, Itani KM. Revisiting percutaneous cholecystostomy for acute cholecystitis based on a 10-year experience. Arch Surg. 2012;147(5):416-22. [CrossRef]
- El Hadidi A, Negm A, Halim MA, Basheer M, Samir M, Attia MS. Cholecystectomy versus percutaneous cholecystostomy drainage in critically ill patients with acute calculous syndrome: a comparative study. Egypt J Surg 2019; 38:46-5. [CrossRef]
- Garcés-Albir M, Martín-Gorgojo V, Perdomo R, et al. Acute cholecystitis in elderly and high-risk surgical patients: is percutaneous cholecystostomy preferable to emergency cholecystectomy? J Gastrointest Surg. 2020; 24(11):2579-2586. [CrossRef]
- La Greca A, Di Grezia M, Magalini S, et al. Comparison of cholecystectomy and percutaneous cholecystostomy in acute cholecystitis: results of a retrospective study. Eur Rev Med Pharmacol Sci. 2017; 21(20): 4668-4674.
- Melloul E, Denys A, Demartines N, Calmes JM, Schäfer M. Percutaneous drainage versus emergency cholecystectomy for the treatment of acute cholecystitis in critically ill patients: does it matter? World J Surg. 2011 Apr;35(4):826-33. [CrossRef]
- Zehetner J, Degnera E, Olasky J, Mason RA, Drangsholt S, Moazzez A, et al. Percutaneous cholecystostomy versus laparoscopic cholecystectomy in patients with acute cholecystitis and failed conservative management: a matched-pair analysis. Surg Laparosc Endosc Percutan Tech. 2014; 24(6):523-7. [CrossRef]
- Latif J, Kushairi A, Thurley P, Bhatti I, Awan A. Laparoscopic cholecystectomy versus percutaneous cholecystostomy: suitability of APACHE-II Score, ASA Grade, and Tokyo Guidelines 18 Grade as predictors of outcome in patients with acute cholecystitis. Surg Laparosc Endosc Percutan Tech. 2022 Jun 1;32(3):342-349. [CrossRef]
- Smith TJ, Manske JG, Mathiason MA, Kallies KJ, Kothari SN. Changing trends and outcomes in the use of percutaneous cholecystostomy tubes for acute cholecystitis. Ann Surg. 2013; 257(6):1112-5. [CrossRef]
- Anderson JE, Chang DC, Talamini MA. A nationwide examination of outcomes of percutaneous cholecystostomy compared with cholecystectomy for acute cholecystitis, 1998-2010. Surg Endosc. 2013; 27(9):3406-11 [CrossRef]
- Anderson JE, Inui T, Talamini MA, Chang DC. Cholecystostomy offers no survival benefit in patients with acute acalculous cholecystitis and severe sepsis and shock. J Surg Res. 2014; 190(2):517-21. [CrossRef]
- Fleming MM, DeWane MP, Luo J, Liu F, Zhang Y, Pei KY. A propensity score matched comparison of readmissions and cost of laparoscopic cholecystectomy vs percutaneous cholecystostomy for acute cholecystitis. Am J Surg. 2019; 217(1):83-89.
- Schlottmann F, Gaber C, Strassle PD, Patti MG, Charles AG. Cholecystectomy vs. cholecystostomy for the management of acute cholecystitis in elderly patients. J Gastrointest Surg. 2019 Mar;23(3):503-509. [CrossRef]
- Simorov A, Ranade A, Parcells J, Shaligram A, Shostrom V, Boilesen E, Goede M, Oleynikov D. Emergent cholecystostomy is superior to open cholecystectomy in extremely ill patients with acalculous cholecystitis: a large multicenter outcome study. Am J Surg. 2013 Dec;206(6):935-40. [CrossRef]
- Lu P, Chan CL, Yang NP, Chang NT, Lin KB, Lai KR. Outcome comparison between percutaneous cholecystostomy and cholecystectomy: a 10-year population-based analysis. BMC Surg. 2017;17(1):130. [CrossRef]
- Griniatsos J, Petrou A, Pappas P, et al. Percutaneous cholecystostomy without interval cholecystectomy as definitive treatment of acute cholecystitis in elderly and critically ill patients. South Med J 2008; 101:586-90. [CrossRef]
- McKay A, Abulfaraj M, Lipschitz J. Short- and long-term outcomes following percutaneous cholecystostomy for acute cholecystitis in high-risk patients. Surg Endosc 2012; 26:1343-51. [CrossRef]
- 40. Horn T, Christensen SD, KirkegaÃärd J, Larsen LP, Knudsen AR, Mortensen FV. Percutaneous cholecystostomy is an effective treatment option for acute calculous cholecystitis: a 10-year experience. HPB (Oxford) 2015; 17:326-31. [CrossRef]
- Zerem E, Omerovic S. Can percutaneous cholecystostomy be a defnitive management for acute cholecystitis in high-risk patients? Surg Laparosc Endosc Percutan Tech 2014; 24:187–191. [CrossRef]
- Chang YR, Ahn YJ, Jang JY, et al. Percutaneous cholecystostomy for acute cholecystitis in patients with high comorbidity and re-evaluation of treatment efficacy. Surgery 2014 155:615–622. [CrossRef]
- hok KS, Chu FS, Cheung TT, et al. Results of percutaneous transhepatic cholecystostomy for high surgical risk patients with acute cholecystitis. ANZ J Surg 2010; 80:280-3. [CrossRef]
- 44. Boules M, Haskins IN, Farias-Kovac M, et al. What is the fate of the cholecystostomy tube following percutaneous cholecystostomy? Surg Endosc 2017; 31:1707–1712. [CrossRef]
- Loftus TJ, Collins EM, Dessaigne CG, et al. Percutaneous cholecystostomy: prognostic factors and comparison to cholecystectomy. Surg Endosc 2017; 31:4568–4575. [CrossRef]
- Hall BR, Armijo PR, Krause C, Burnett T, Oleynikov D. Emergent cholecystectomy is superior to percutaneous cholecystostomy tube placement in critically ill patients with emergent calculous cholecystitis. Am J Surg 2018; 216:116–119. [CrossRef]
- Winbladh A, Gullstrand P, Svanvik J, Sandström P. Systematic review of cholecystostomy as a treatment option in acute cholecystitis. HPB (Oxford) 2009; 11(3):183–93. [CrossRef]
- McArthur P, Cuschieri A, Shields R, et al. Controlled clinical trial comparing early with interval cholecystectomy for acute cholecystitis. Proc R Soc Med 1975; 68:676–678.
- Norrby S, Herlin P, Holmin T, et al. Early or delayed cholecystectomy in acute cholecystitis? A clinical trial. Br J Surg 1983; 70:163–165. [CrossRef]
- Shikata S, Noguchi Y, Fukui T. Early versus delayed cholecystectomy for acute cholecystitis: a metaanalysis of randomized controlled trials. Surg Today 2005; 35:553–560. [CrossRef]
- Siddiqui T, MacDonald A, Chong PS, et al. Early versus delayed laparoscopic cholecystectomy for acute cholecystitis: a meta-analysis of randomized clinical trials. Am J Surg 2008; 195:40–47. [CrossRef]
- Jia B, Liu K, Tan L, Jin Z, Liu Y. Percutaneous transhepatic gallbladder drainage combined with laparoscopic cholecystectomy versus emergency laparoscopic cholecystectomy in acute complicated cholecystitis: comparison of curative efficacy. Am Surg 2018; 84:438–442.
- Riall TS, Zhang D, Townsend CM Jr, Kuo YF, Goodwin JS. Failure to perform cholecystectomy for acute cholecystitis in elderly patients is associated with increased morbidity, mortality, and cost. J Am Coll Surg. 2010; 210(5): 668-77. [CrossRef]
- Cirocchi R, Cozza V, Sapienza P, et al. Percutaneous cholecystostomy as bridge to surgery vs surgery in unfit patients with acute calculous cholecystitis: A systematic review and meta-analysis. Surgeon. 2022: S1479-666X(22)00138-X. [CrossRef]
- Granlund A, Karlson BM, Elvin A, Rasmussen I. Ultrasound-guided percutaneous cholecystostomy in high-risk surgical patients. Langenbecks Arch Surg 2001; 386:212-7. [CrossRef]
- Leveau P, Andersson E, Carlgren I, Willner J, Andersson R. Percutaneous cholecystostomy: a bridge to surgery or definite management of acute cholecystitis in high-risk patients? Scand J Gastroenterol 2008; 43:593-6 [CrossRef]
Figure 1.
Forest plot of postoperative mortality rates of PTGBD vs EC.
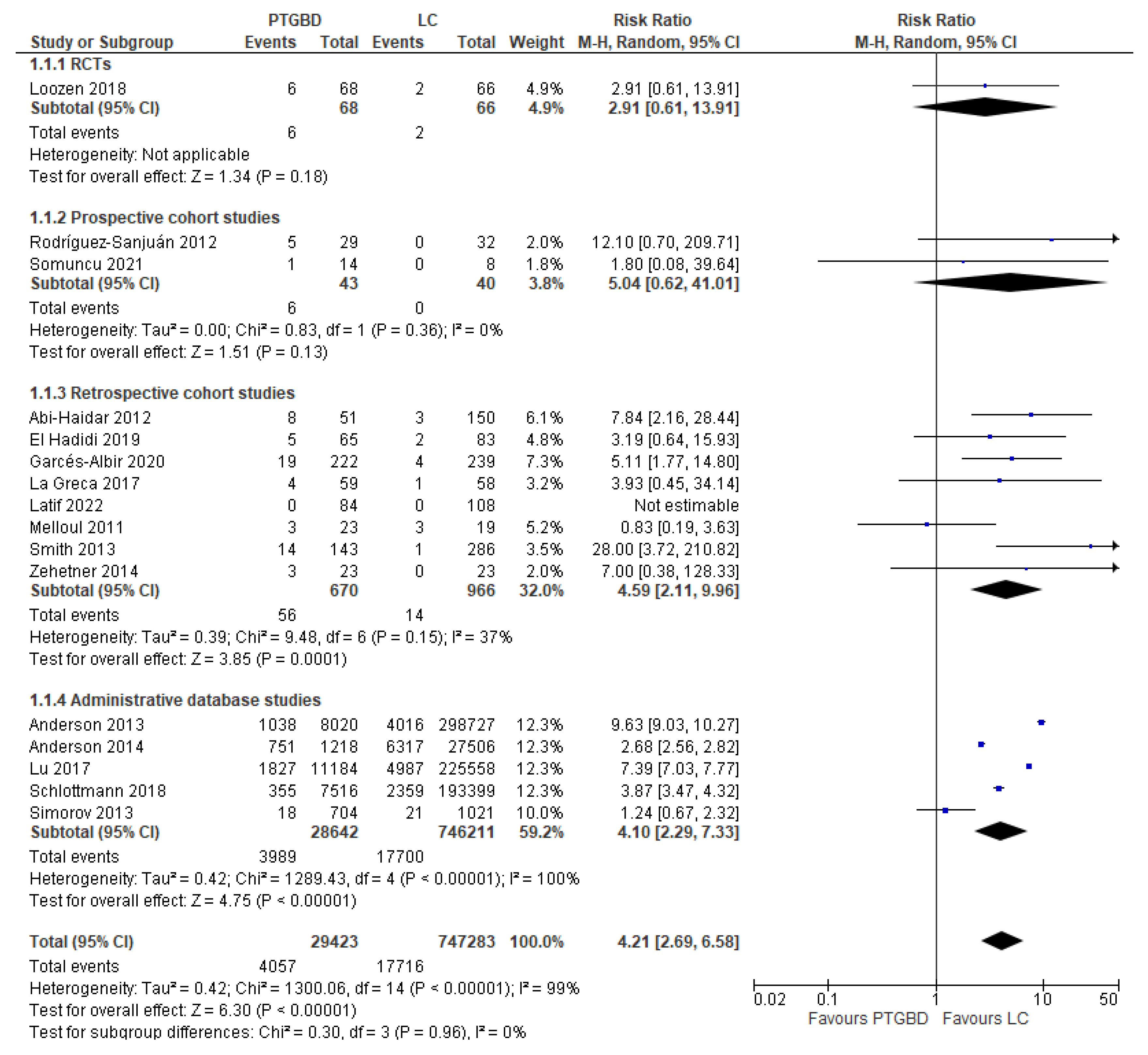
Figure 2.
Forest plot of overall postoperative complications between PTGBD vs EC.
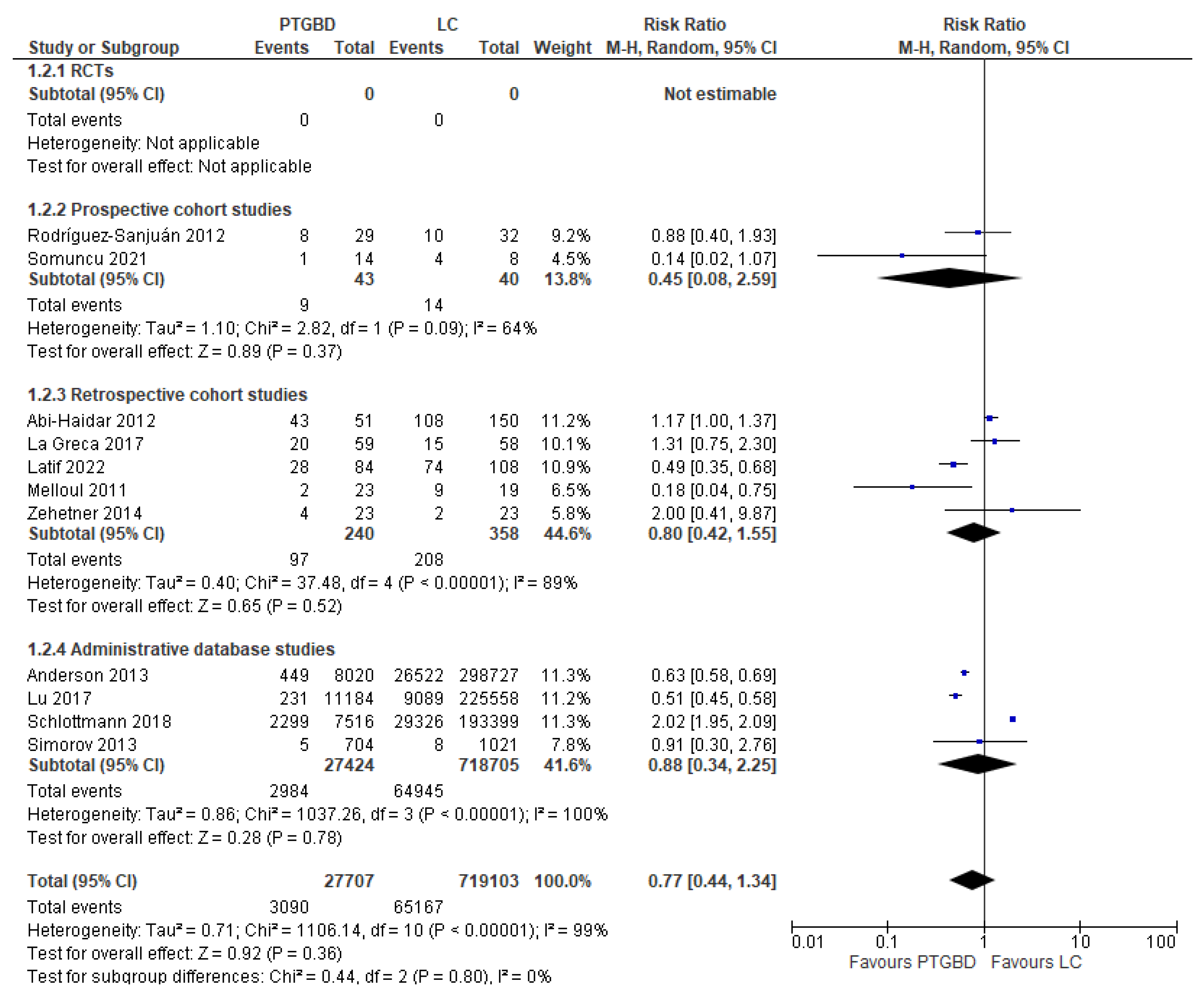
Figure 3.
Forest plot of emergency reinterventions between PTGBD vs EC (emergency conventional cholecystectomy).
Figure 3.
Forest plot of emergency reinterventions between PTGBD vs EC (emergency conventional cholecystectomy).
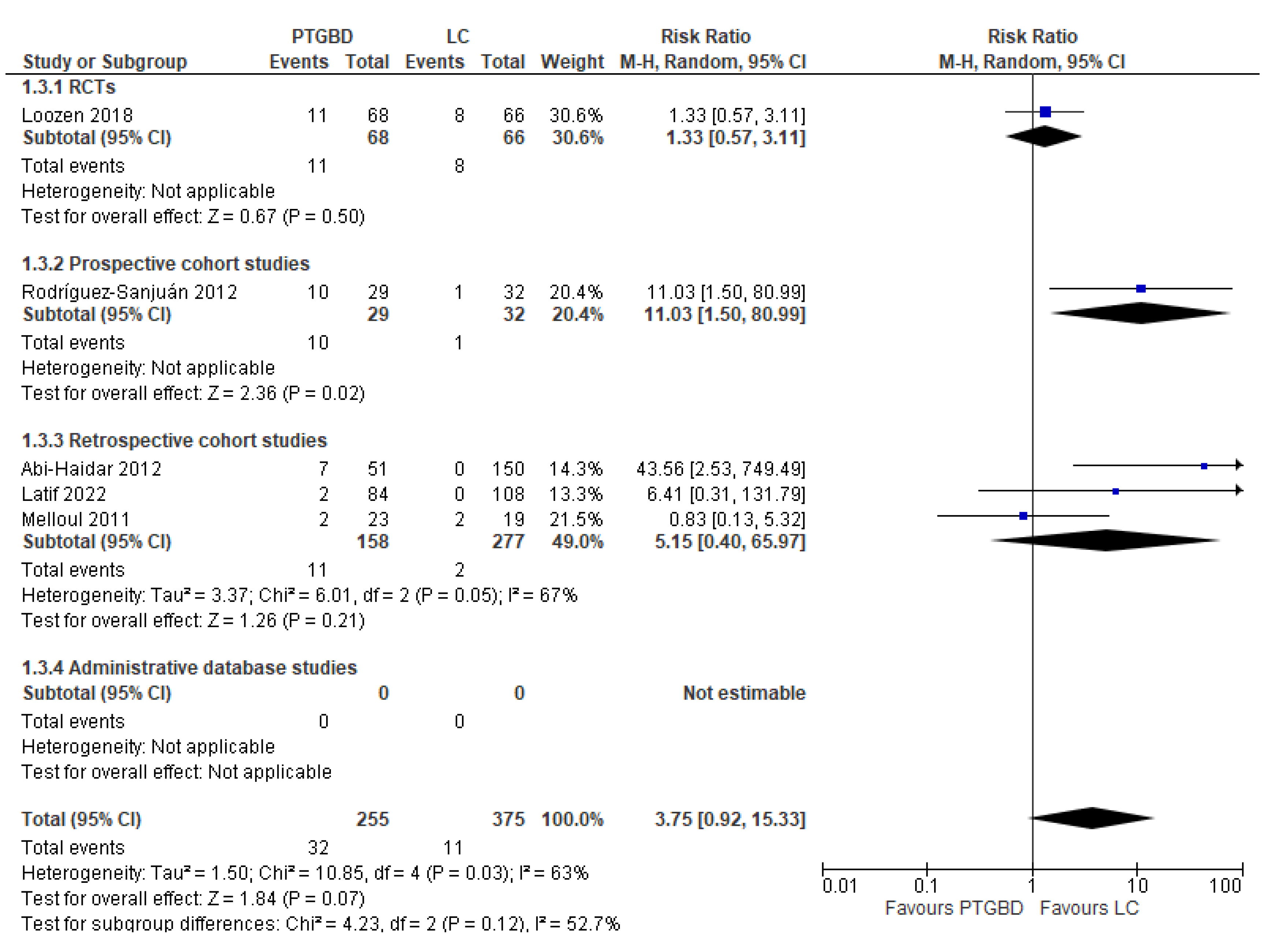
Figure 4.
Forest plot of hospital readmission for biliary complications between PTGBD vs EC.
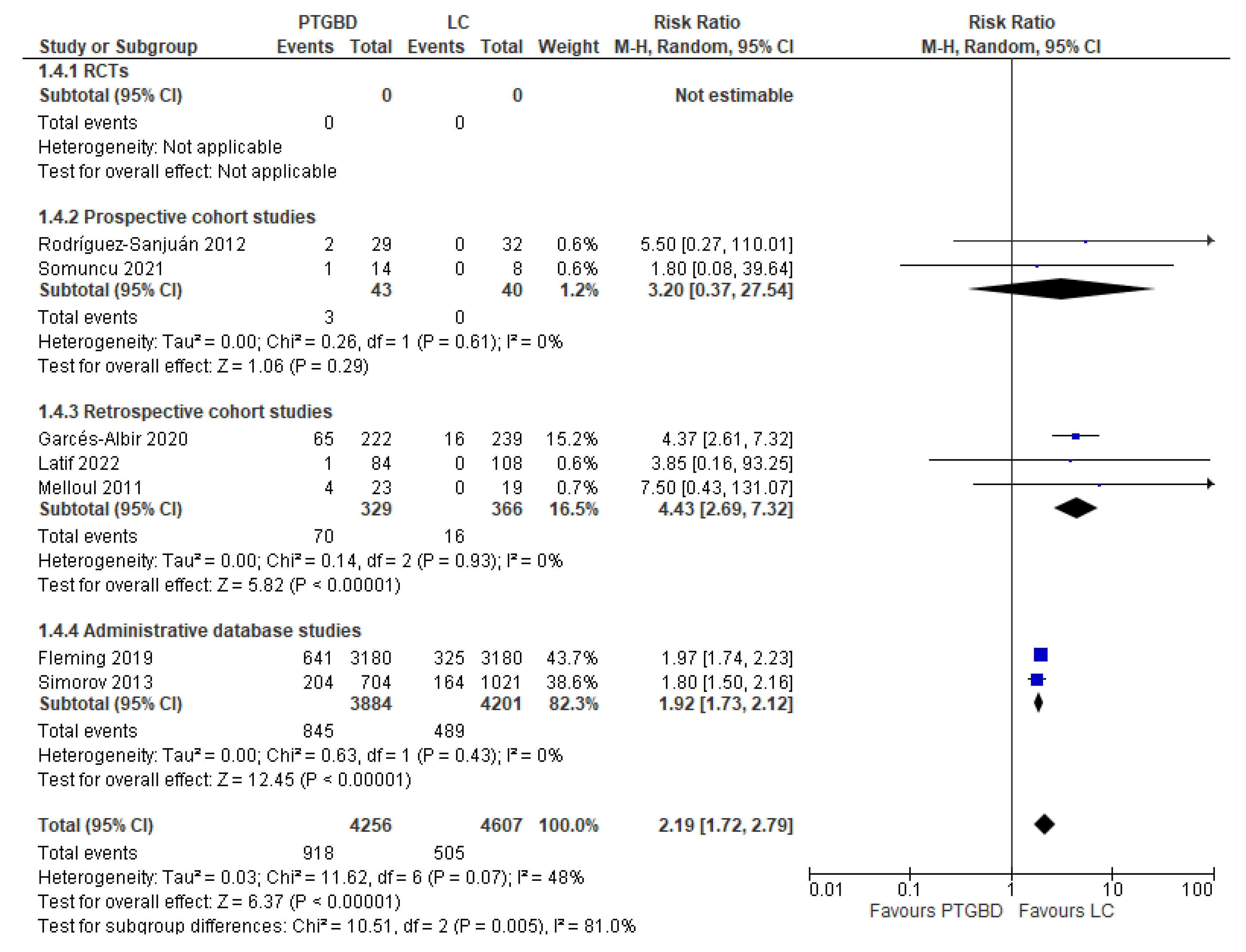

Table 1.
Characteristics of the included studies.
| Author and year of publication | Nation | Type of study | N. of patients included | Time of enrolment | PTGBD group | LC in control group | OC | NR | |||
|---|---|---|---|---|---|---|---|---|---|---|---|
| N. of patients | Timing | N. of patients | Timing | N. of patients | Timing | N. of patients | |||||
| Latif et al. 2022 |
United Kingdom | RCS | 192 | 2016 to 2018 | 84 | NR | 108 | After >48 of conservative management | 0 | NR | 0 |
| Somuncu et al. 2021 | Turkey | PCS | 22 | March 2020 to June 2020 | 14 | NR | 8 | NR | 0 | NR | 0 |
| Garcés Albir et al. 2020 | Spain-Uruguay | RCS | 461 | January 2005 to December 2016 | 222 | NR | 239 | NR | 0 | NR | 0 |
| El Hadidi et al. 2019 | Egypt | RCS | 225 | February 2014 a September 2017 | 65 | NR | 83 | NR | 77 | NR | 0 |
| Fleming et al. 2019 | USA | Administrative database studies | 6360 | 2013 to 2014 | 3180 | NR | 3180 | NR | 0 | 0 | 0 |
| Loozen et al. 2018 | Netherlands | RCT | 134 | February 2011 to January 2016 | 68 | Within 24h after randomization | 66 | Within 24h after randomization | 0 | 0 | 0 |
| Schlottmann et al. 2018 | USA- Argentina | Administrative database studies | 200915 | January 2000 to December 2014 | 7516 | NR | NR | NR | NR | NR | 193399 |
| La Greca et al. 2017 | Italy | RCS | 646 | August 2009 to March 2016 | 90 | NR | NR | NR | NR | NR | 556 |
| Lu et al. 2017 |
Taiwan | Administrative database studies | 236742 | 2003 to 2012 | 11184 | NR | NR | NR | NR | NR | 225558 |
| Anderson et al. 2014 | USA | Administrative database studies | 28724 | 1995 to 2009 | 1218 | NR | NR | NR | NR | NR | 27506 |
| Zehetner et al. 2014 | USA | RCS | 46 | January 1999 to October 2010 | 23 | NR Presence of symptoms for 72h |
23 | NR Presence of symptoms for 72h |
0 | 0 | 0 |
| Anderson et al. 2013 | USA | Administrative database studies | 306747 | 1998 to 2010 | 8020 | NR | NR | NR | NR | NR | 298727 |
| Simorov et al. 2013 | USA | Administrative database studies | 1725 | October 2007 to June 2011 | 704 | NR | 822 | NR | 199 | NR | 0 |
| Smith et al. 2013 |
USA | RCS | 432 | April 1998 to December 2009 | 143 | NR | NR | NR | NR | NR | 286 |
| Abi-Haidar et al. 2012 | USA | RCS | 201 | January 2001 to December 2010 | 51 | NR | 110 | During 24h of admission = 32 Later than 24h after admission = 33 Elective procedure = 45 |
40 | During 24h of admission = 26Later than 24h after admission = 7 Elective procedure = 3 Emergency procedure after discharged = 4 |
0 |
| Rodrìguez-Sanjuàn et al. 2012 | Spain | PCS | 61 | January 2005 to December 2010 | 29 | NR | 14 | First 72hours from AC onset | 18 | First 72hours from AC onset | 0 |
| Melloul et al. 2011 | Switzerland | RCS | 42 | 2001 to 2007 | 23 | 12-24h | 10 | 12-24h | 9 | 12-24h | 0 |
| Total | 783.672 | 32.634 | 4.663 | 343 | 746.032 | ||||||
Table 2.
Type of percutaneous drainage technique performed.
| Transhepatic route | Transperitoneal route | Not Reported |
|---|---|---|
| Latif et al. 2022 | Loozen et al. 2018 | Fleming et al. 2019 |
| Somuncu et al. 2021 | La Greca et al. 2017 | Schlottmann et al. 2018 |
| Garcés Albir et al. 2020 | Smith et al. 2013 | Lu et al. 2017 |
| El Hadidi et al. 2019 | Anderson et al. 2014 | |
| Loozen et al. 2018 | Zehetner et al. 2014 | |
| Melloul et al. 2011 | Anderson et al. 2013 | |
| Abi-Haidar et al. 2012 | Simorov et al. 2013 | |
| Rodriguez-Sanjuàn et al. 2012 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



