
Submitted:
30 June 2023
Posted:
30 June 2023
You are already at the latest version
Abstract
An analysis of the curve of Spee in relation to muscle activity, assessed by electromyographic analysis, on a group of 16 young adults with previous fixed orthodontic treatment is proposed as a pilot study.
Given the high incidence of this type of dental treatment, it is important to point out how, in this field of dentistry, there is a marked tendency to level and flatten this anatomical occlusal curve, as proposed by Andrews. If in orthodontics there is a standardized levelling of the curve of Spee, in the prosthetic and restorative field, the management of the curve of Spee requires greater attention and often even an individualized approach. The purpose of this study is to investigate what the levelling of the antero-posterior occlusal curve entails in terms of masticatory effectiveness and harmony. From the results obtained, it can be seen that in order to optimize the harmony of the stomatognathic apparatus, the curve of Spee is a parameter that requires individual attention: modifying it through standardized levelling has inevitable consequences.
Keywords:
curve of Spee
; electromyographic analysis
; young adults
1. Introduction
The curve of Spee is an anatomical curve described in 1890 by the German scholar Graf Von Spee, after whom it is named.
It is a curve that is described as ''an ideal line connecting the cusps, that is, the top of the natural teeth, starting from the canines and passing through the premolars to the molars of the same half of the mouth.'' [1]. Spee realized how this curved line could optimize tooth contact between elements on antagonistic arches.
The curve of Spee can be defined as a dental parameter determined by the mesio-distal inclinations of the latero-posterior elements of the mandibular dental arch [2]. As Osborn demonstrated, this arrangement allows a more efficient distribution of forces and masseter action [2].
It was this same scholar who noted that the inclination of the masseter was parallel to the long axis of the lower first molars [2].
The normal, everyday functions of the stomatognathic apparatus (chewing, swallowing and phonation) result in contacts between the antagonistic arches, and the consequent distribution of forces along the bone structure will differ between patients because of several variable parameters, including the Spee curve.
A similar sagittal arrangement of the dental elements maximizes muscle efficiency during chewing [2]. These different muscle forces and the direction of the fibre could contribute to the mandibular shape and, consequently, could influence the inclination of the occlusal plane [3]. The curve of Spee is thus a dental parameter that is likely to be affected and that will in turn influence the hard and soft tissues [4]. A similar curve in the sagittal plane is found in several mammalian taxa, including modern humans and fossil hominids. It went from a totally flat curve with wide retromolar space, found in Neanderthals and Australopithecus, to the progressive change in the hominid craniofacial structure, which also included the appearance and variation of the curve in Sapiens [5]. The presence/absence of this feature may be related to the functional variation of the masticatory apparatus and also to broader dentognathic spatial dynamics. It can be argued that this morphological relationship is probably due to the developmental and functional integration between the maxillary and mandibular dental arches [5]. Pathological situations, ethnicity, genetic components and age may also be part of the factors influencing the curve of Spee. This anatomical curve does not only vary in relation to evolution, but it also varies interpersonally, and even in the same individual depending on age: studies show how it varies according to the stage of dentition in which the subject is in. Marshall et al. noted how the occlusal plane is flat in full deciduous dentition [6]. Similar results were reported by Ash et al. [7], who suggested that deciduous dentition exhibits a curve of Spee that ranges from flat to slight, whereas dentition in adulthood exhibits a more pronounced Spee curve, which stabilizes and is maintained. Thus, if in deciduous dentition the flattened curve is physiological, the same cannot be said for the curve in adulthood. Often, however, there is a tendency to alter this curve, to reduce its depth or level it off, especially in the orthodontic school that follows Andrews, who believed that this curve should be reduced or eliminated so as to improve occlusal contact [8]. While that is true in static structures, it must nevertheless be remembered that the mandible is an organ that performs its functions primarily in movement. When designing dental treatment that is aimed at maintaining or restoring ideal functional harmony, not only must the centric movements of the mandible be taken into account, but also the eccentric and excursive components of mandibular movements. In fact, this curve favours the posterior disocclusion in protrusive movements [9]. As proof of this, a clinical examination that can be carried out is to ask patients to perform a protrusive movement by bringing the upper incisal margins into a head-to-head position with the lower ones. Subsequently, the amount of posterior disocclusion should be noted, as well as whether there is the presence of any precontact or contact that obstructs the movement. Dental extrusions can pathologically alter this curve and lead to a similarly altered occlusal plane [10], with the presence of posterior protrusive interference, which can cause abnormal activity – hyperactivity – in the mandibular elevator muscles, particularly the masseter and temporalis muscles [11], whose activity was examined in this study using electromyographic tracings. Excessive interference can also cause wear and tear, the fracture of restorations, and temporomandibular joint dysfunction. In confirmation of this, it has been seen that problems such as temporomandibular disorders are more prevalent in patients in whom the curve of Spee has been altered following orthodontic treatment [13]. Such complications can be avoided by reconstructing a curve of Spee that is in harmony with the subject's stomatognathic apparatus, and in particular with the structure of the mandibular condyle [12]. The purpose of this study is to investigate the curve of Spee in relation to muscle activity, assessed by electromyographic analysis, on a group of 16 young adults with previous fixed orthodontic treatment.
2. Materials and Methods
Digital imprints and electromyographic tracings of the anterior masseter and temporalis muscles were taken in a group of 16 subjects. The age of the subjects examined ranged between 20 and 25 years. All the subjects had Angle Class I occlusal relationships and had undergone previous fixed orthodontic treatment.
The study consists of three phases:
1-measurement of the curve of Spee on digital imprints and assessment of the extent of occlusal contact, using Dental Sirona software;
2-analysis of the electromyographic tracings obtained from the same subjects, study of the indices obtained from the electromyographic recordings and evaluation of the fit bite system of the Kinelock electromyograph software;
3-Correlation of the data obtained.
2.1. Materials
-intra oral scanner (Primescan Connect) and dedicated software (5.2.4) -Blender software (2023)
-Kinelock electromyograph
-disposable bipolar electrodes
-Cotton rollers with a diameter of 10 mm
-Latex gloves
-methylated spirit
-sterile gauze
-camera
2.2. Methods
Using the Primescan Connect intraoral scanner and the dedicated software 5.2.4, it was possible to take digital imprints of the subjects examined, thus obtaining digital models and visualizing the occlusal contacts and their extent in order to produce a colorimetric representation of the occlusal table through the digital survey. These digital readings were studied using computer graphics CAD software (Blended, version 2023).
Using these digital models, the curve of Spee was studied in the various subjects examined. Because it is a curve described in the lower arch, it is at this level that it is usually measured. In this study, the Spee curves were evaluated in both the right and left sides of the mandibular arch.
The maximum depth of the curve of Spee was measured in the mandibular arch as the greatest perpendicular distance between the tips of the buccal cusps of the mandibular teeth, and a plane of measurement that went from the canines to the tip of the distal cusp of the most posterior ipsilateral tooth of the same arch.
The maximum depth was studied by plotting several segments with the software, starting from the cusps of the latero-posterior elements perpendicular to the curve, and selecting the one having the greatest value as corresponding to the point of maximum depth of the curve.
The same subjects underwent electromyographic studies to assess the activity of the masticatory muscles: the anterior temporalis and the masseter.
The Kinelock electromyograph equipped with 8 channels, wirelessly connected to a dedicated PC, was used for the study. Bipolar Ag/Ag hydrochloride electrodes, with a diameter of 10mm and an interelectrode distance of 1 mm, were used for all the subjects and muscle surfaces, using a gelled surface treated with conductive paste and a reference electrode placed at the centre of the forehead on a silent area.
Before placing the electrodes on the skin, it was necessary to clean it with a cotton swab soaked in methylated spirit.
Electrodes were placed parallel to the muscle fibre.
For the anterior temporalis, they were placed vertically along the anterior margin of the muscle, just above the coronal suture, while for the masseter, they were placed parallel to the muscle fibre with the upper pole at the height of the intersection of the plane between the tragus and the angle of the lips and the plane between the gonion and the outer canthus of the eye.
For each subject, five acquisitions lasting 5 seconds each were performed in the position of maximum voluntary contraction (MVC).
During these tests, the subjects were verbally urged to clench as hard as possible. They were not shown the tracings during the test so as to avoid alterations due to visual biofeedback.
In order to simulate the subjects' muscular activities as closely as possible to reality, the assessments were made with visual correction means usually used by the subjects examined. For the first three recordings, the subjects were made to sit on a wooden chair, assuming a straight posture, with their feet resting on the ground and their hands resting on their knees, their gaze directed toward the horizon plane. The additional two acquisitions, on the other hand, were taken by asking the subjects to acquire an orthostatic posture, with their gaze toward the horizon and their arms along their sides. In the first survey, a neutralization of the occlusal contact through ''cotton clenching'' was performed: in subjects seated according to the arrangements described above, with their eyes open and looking straight at the horizon, two cotton rolls 10 mm in diameter were interposed between the arches, in the left and right premolar area, symmetrically. After cotton clenching, the cotton rollers were removed and the additional four recordings were made. The second recording was made with the subject sitting, eyes open. The third recording was made with the subject sitting, eyes closed; The fourth and fifth recordings, on the other hand, were made in the orthostatic position, with eyes open and then eyes closed, respectively. Thus, the electromyographic activity of the masseter muscles and the anterior temporalis muscles on both sides was recorded in the different positions with eyes open and closed, to study the possible influence of postural and visual proprioceptive inputs. From the electromyographic recordings it was possible to evaluate the raw and rds tracings, to study the POC MM, POC TA, IMPACT, BAR, and TORS indices, and to visualize the graphical representation of the subject's occlusal situation with the software's fit bite algorithm, which shows the areas where the occlusion should be modified, suggesting possible thickness modifications necessary to obtain better muscle activity.
3. Results
This study evaluated the influence of the arrangement of dental elements in sagittal view on the contractile activity of the masticatory muscles.
The subjects examined presented curves of Spee with mild depth, zero depth and in some cases had a negative curve (inverted concavity), probably caused by previous orthodontic treatment. The study shows that in the arches where the curve of Spee is more flattened and levelled, the maximum depths of the curve are often reached at the level of the distal buccal cusp of the first molar.
A further observation made concerns the differences in the depth of the curves in the two hemiarches, left and right, in the same subject.
It was noted that the curvatures of the two hemiarches are different, in a variably marked manner, and that the hemiarches in which the third molar is present are those with greater curvature. In fact, the presence of third molars in the arch causes a significant increase in the curve of Spee. The results show that the hemiarch in which the curvature is deepest is the hemiarch of the subject in which the occlusal contacts in maximum intercuspation are greater (as observed by colorimetric evaluations) and in which the stress resulting from occlusion in maximum intercuspation appears to be more distributed at the molar level and less localized at the premolar, canine and incisor levels. In contrast, in the arches or hemiarches in which the curve of Spee is flatter and almost level, stress appears to be more evenly distributed over both anterior, lateral and posterior elements.
With these curve depth values (reduced, zero, or reversed), an increased activity in the anterior temporalis was noted. The BAR index (occlusal centre of gravity) was found to vary in all subjects and be delocalized anteriorly in a variable manner in the 5 electromyographic recordings performed per participant. In addition to the BAR index, the electromyographic evaluations showed that IMPACT was another parameter which was often found to be lower than the normal value range. The system's fit bite algorithm indicated in these cases the need for shim additions in the posterior sectors (Figure 1). Changes in MVC activity recorded in muscle activity while seated and activity measured in orthostatism presented no significant differences; both the tracings and the indices were found to be similar, the slight differences presented being related to interpersonal variations. Visual inputs were found to be irrelevant in the muscle activity of the masticatory muscles examined. The slight differences in developed contractile activity (measured in microvolts, along the vertical y-axis of the ordinates of the electromyographic tracing) reoccurred and were reflected in slight, nonsignificant differences at the level of the indices evaluated.
Standing, eyes open
4. Discussion
The curve of Spee is in harmony with other factors that include the condylar guidance angle, the incisal guidance angle (overbite and overjet), and the occlusal plane angle. This harmony involves not only the dento-skeletal tissues, but also the soft tissues.
The reduced, zero or negative depth values of the curve of Spee assessed in the subjects examined imply a prevalence of anterior contacts (as visible in the colorimetric assessments) and correspond to an increased activity in the anterior temporalis, probably as a result of the reduced depth of the Spee curve.
This finding is confirmed by the BAR index (occlusal centre of gravity), which varied in all the subjects and was anteriorly delocalized in at least one of the 5 electromyographic recordings made per participant.
This observation can be correlated with the images of the colorimetric evaluations of occlusal contacts carried out by the intraoral scanner software. Above all, in cases of levelled curves of Spee, occlusal contacts in maximum intercuspation are observed to be well distributed along the arch, in a homogeneous way, even at the level of the anterior incisal region, where, however, there should be a 'grazing' contact and instead this contact is very much present, for guidance, during the protrusive excursive movements.
The alteration of the BAR index can be correlated with the change in the IMPACT index. The latter index corresponds to the DVO (distal vessel occlusion) of the subject: an increase in DVO correlatively produces an increase in IMPACT, which can be read as an index of chewing effectiveness [14].
The IMPACT value was found to be altered in almost all subjects: in most cases it was lower. In these cases, the system’s fit bite algorithm indicated the need for the addition of shims in the posterior sectors to restore an ideal curve of Spee, increasing its depth.
Information from the colorimetric analysis of occlusal contacts and from the fit bite software of the Kinelock electromyograph confirms the need for the addition of thickness at the posterior level.
If in the study it can be seen that a mild and flattened curve of Spee was generally correlated (when the other values were normal) to low IMPACT, with a need for increased posterior DVO and an increase in the Spee curve, it can be assumed that levelling has resulted in a reduction of this biological vertical dimension of occlusion in the individual and a consequent reduction in the effectiveness of the masticatory muscle activity.
On the other hand, it is also possible that levelling alters the DVO by increasing its values.
In a subject with increased DVO (e.g., because of levelling caused by excessive extrusion in the premolar/molar area), IMPACT will increase: the curve of Spee will have to be restored no longer by adding thickness and height to increase the posterior DVO, adding hard tissue or extruding and tilting the elements mesially, but by decreasing this DVO by selective intrusions or grinding.
Therefore, in the levelling of the curve of Spee, one of the issues that can arise is how to maintain a DVO that is in the ideal biological range for the subject and for the correct and most effective muscular and postural function. Levelling the curve of Spee could in fact cause an alteration in DVO, which may increase or decrease.
When the mandibular curve is convex, that is to say, with negative depth values, DVO is increased, as is IMPACT. On the other hand, the levelling of the curve of Spee in the other cases resulted in a reduction of DVO, with low IMPACT values, and the consequent need, as indicated by the fit bite algorithm, to add shims at the posterior level, increasing DVO at the molar level, along with IMPACT, thus achieving a restoration of the curve of Spee.
In addition, the fact that the maximum depth of the curve is often reached at the level of the distal buccal cusp of the first molar highlights how the mesio-distal inclination of these elements is different from normal, where the maximum depth is generally reached at the level of the buccal cusp of the second molar or at the mesio-buccal cusp of the first molar, because of their mesio-distal inclination.
In the hemiarch in which the curve is deeper, the mesio-distal inclinations of the posterior elements are greater. In these cases, the occlusal stress is distributed more on these lateral-posterior dental elements and is less localized anteriorly. Moreover, the occlusal contact in the maximum intercuspation is greater. This arrangement of contacts and stress in the maximal intercuspation benefits the lateral and anterior elements, which are the ones assigned to bearing high occlusal loads, especially in movements with a greater vertical component (unlike the anterior and lateral elements, which are usually used more in movements in which the horizontal component predominates: the antero-posterior and the latero-lateral, respectively).
Conversely, in the arches or hemiarches in which the curve of Spee appears to be shallower, stress appears to be more evenly distributed on both the anterior, lateral, and posterior elements, thus making the anterior and lateral elements susceptible to stress arising from the centric component of mandibular movements, and the posterior ones susceptible to stress from the eccentric and excursive component of the same mandibular movements during chewing.
In confirmation of this, it can be seen from the electromyographic tracings that a deeper arch curve does not only correspond, as mentioned, to the arch in which the stronger occlusal contact occurs and is more localized at the molar level in maximum intercuspation, but it can be seen that it is also the arch in which a greater ipsilateral masseter activity occurs (within normal ranges). This is observed both by analysing the tracings and by analysing the indices of the respective electromyographic evaluations.
Limitations of the Study
To better assess muscle function as a function of occlusion, it is proposed that dynamic electromyographic evaluations be made in future studies, especially for protrusive movements, with the relative muscles involved, in which the curve of Spee has been seen to play an important role.
The present study focuses its attention on the curve of Spee. It would be interesting if the evaluation was also applied to the curve of Wilson for a complete three-dimensional analysis of the occlusal plane.
An additional limitation of the study is the reduced size of the group of young adults on whom the test was performed, from which Angle class II and III subjects were excluded.
In addition, since many of the subjects evaluated had had previous orthodontic treatment, it would have been interesting to evaluate the data not only after treatment was completed but also pre-treatment.
5. Conclusions
The curve of Spee represents a variable in medical dental treatments, both in the orthodontic field and in the conservative-prosthetic one, and must be taken into account in order to achieve maximum masticatory efficiency and muscular balance in the stomatognathic apparatus.
If in the orthodontic field the flattening of the curve of Spee is expected, in the restorative and prosthetic fields, such a compensatory curve plays an indispensable role in the positive outcome, success, stability and long-term prognosis of the element.
Its alteration or the production of a curve that is not in harmony with the balance, both static and dynamic, of the neuro-muscular-skeletal apparatus of the individual may lead to various problems. Proposing a treatment with an alteration of such a curve should raise questions, not only about the stability of the treatment, but also about the occlusal and overall harmony of the stomatognathic system.
Author Contributions
Conceptualization, GAS and IB; methodology, GAS, IB; validation, MIK and AM; formal analysis, IB; investigation, IB, GAS; data curation, IB; writing—original draft preparation, GAS; writing—review and editing, PM; visualization, AM, MIK; supervision, PM. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki, and approved by the Institutional Review Board (or Ethics Committee) of University of Palermo-Policlinico Paolo Giaccone.
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study
Data Availability Statement
We encourage all authors of articles published in MDPI journals to share their research data. In this section, please provide details regarding where data supporting reported results can be found, including links to publicly archived datasets analyzed or generated during the study. Where no new data were created, or where data is unavailable due to privacy or ethical restrictions, a statement is still required. Suggested Data Availability Statements are available in section “MDPI Research Data Policies” at https://www.mdpi.com/ethics.
Conflicts of Interest
The authors declare no conflict of interest.
References
- The gliding path of the mandible along the skull. Ferdinand Graf Spee (1855-1937), prosector at the Anatomy Institute of Kiel. J Am Dent Assoc. 1980 May;100(5):670-5.
- Osborn, JW. Orientation of the masseter muscle and the curve of Spee in relation to crushing forces on the molar teeth of primates. Am J Phys Anthropol. 1993 Sep;92(1):99-106.
- Ogawa T, Koyano K, Suetsugu T. The relationship between inclination of the occlusal plane and jaw closing path. J Prosthet Dent. 1996 Dec;76(6):576-80.
- Casazza E, Orthlieb JD, Giraudeau A, Ré JP. Balkwill's angle, occlusal plane, mandibular shape, and curve of Spee. Cranio. 2022 Jan 12:1-9.
- Laird MF, Holton NE, Scott JE, Franciscus RG, Marshall SD, Southard TE. Spatial determinants of the mandibular curve of Spee in modern and archaic Homo. Am J Phys Anthropol. 2016 Oct;161(2):226-36.
- Marshall SD, Caspersen M, Hardinger RR, Franciscus RG, Aquilino SA, Southard TE. Development of the curve of Spee. Am J Orthod Dentofacial Orthop. 2008 Sep;134(3):344-52.
- Ash, M. Wheeler's dental anatomy, physiology and occlusion. 7th ed. Philadelphia: W.B. Saunders; 1993.
- Andrews, LF. The six keys to normal occlusion. Am J Orthod. 1972 Sep;62(3):296-309.
- Okeson, JP. Gestione dei disturbi temporo-mandibolari e dell'occlusione. 5a ed. Stati Uniti: Mosby; 2003. pp. 127-46.
- Herbert, T. Shillingburg, Jr, DDS Sumiya Hobo, DDS, MSD, PhD Lowell D. Whitsett, DDS Richard Jacobi, DDS Susan E. Brackett, "Fundamentals of Fixed Prosthodontics Third Edition.
- Williamson EH, Lundquit DO. Anterior guidance: It's effect on electromyographic activity of the temporal and masseter muscle. J Prosthet Dent. 1983;49:816-23.
- Williamson EH, Lundquist DO. Anterior guidance: its effect on electromyographic activity of the temporal and masseter muscles. J Prosthet Dent. 1983 Jun;49(6):816-23.
- Kanavakis G, Mehta N. The role of occlusal curvatures and maxillary arch dimensions in patients with signs and symptoms of temporomandibular disorders. Angle Orthod. 2014 Jan;84(1):96-101.
- Pompa G, Di Carlo S, Mencio F, Mattei M, Shahi J. Determinazione della dimensione verticale in protesi su impianti tramite elettromiografia di superficie J.Stomat Occ. Med. 2012; 5:83-87.
Figure 1.
indices obtained from an electromyographic recording, with muscle activity graph and fit bite algorithm ( Kinelock electromyograph).
Figure 1.
indices obtained from an electromyographic recording, with muscle activity graph and fit bite algorithm ( Kinelock electromyograph).
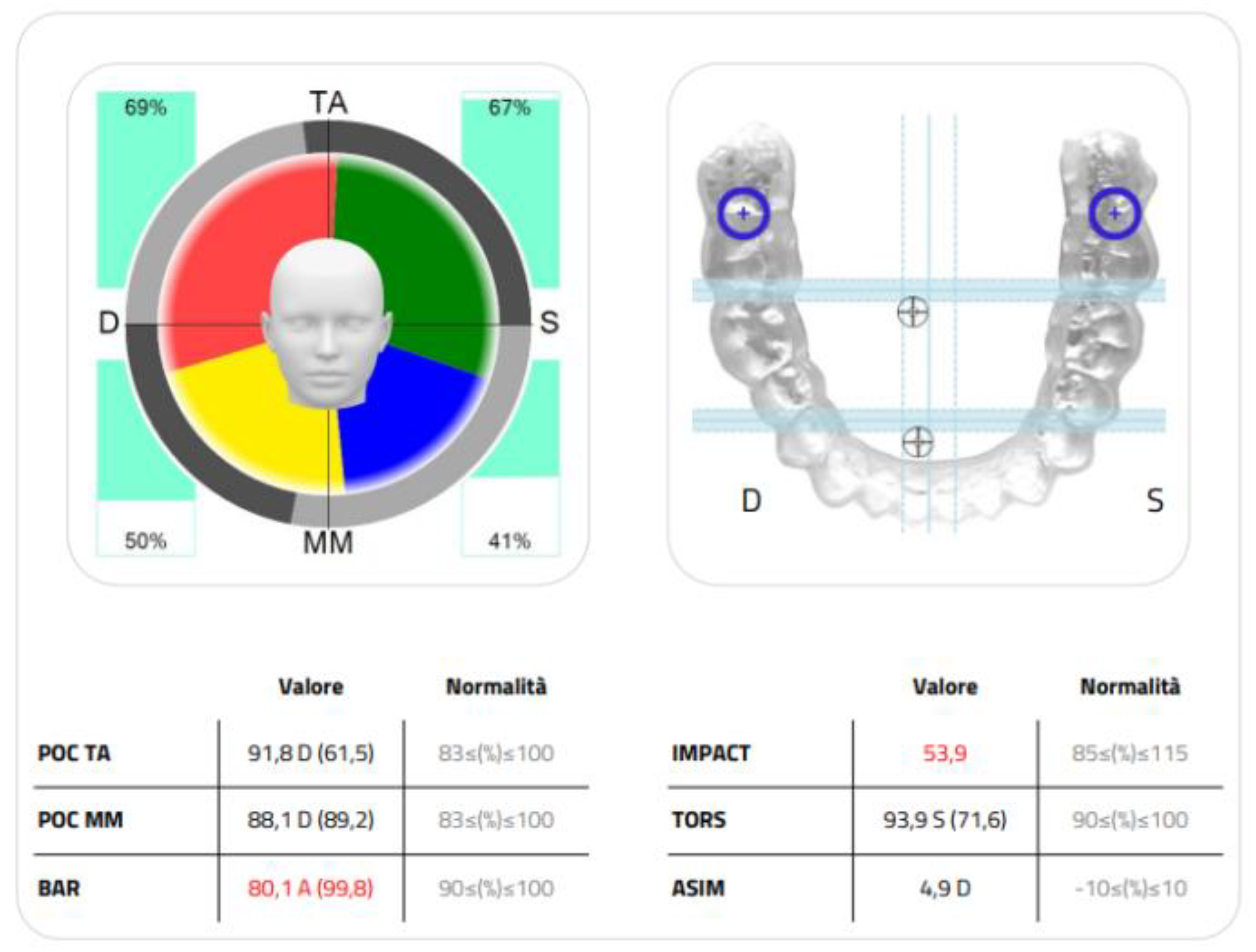
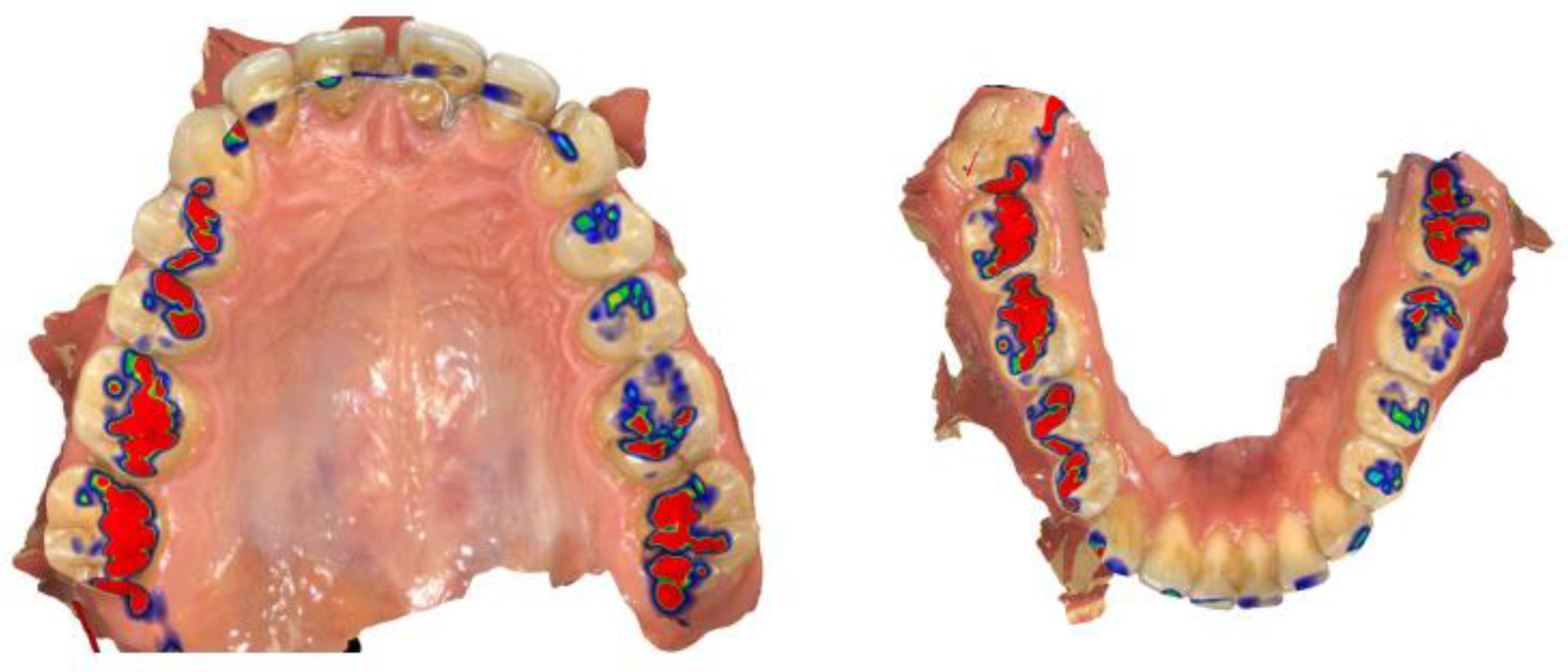
Figure 2.
colorimetric analysis of occlusal contacts.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



