
Submitted:
29 June 2023
Posted:
30 June 2023
You are already at the latest version
Abstract
This study aimed to explore the effects of raloxifene (Rx) and estradiol (E2) on prothrombin time (PT), partial thromboplastin time (APTT), coagulation factors (VII, X, XI), and fibrinogen concen-trations in rats. Rats were ovariectomized 11 days prior to starting the treatment. Then they re-ceived Rx or E2 (1 to 1000 µg/Kg) or propylene glycol (0.3 ml; vehicle, V) subcutaneously for three consecutive days. Plasmas were collected to measure the hemostatic parameters. Rx significantly increased PT (8%, at 1000 µg/Kg; p<0.05) and APTT at all doses evaluated (32, 70, 67, 30%; p<0.05, respectively). Rx (1 to 1000 µg/Kg) decreased the activity of factor VII by -20, -40, -37, and -17% (p<0.05), respectively, while E2 increased it by 9, 34, 52, and 29%; Rx reduced factor X activity at 10 and 100 µg/kg doses (-30, and -30% p<0.05), while E2 showed an increment of 24% with 1000 µg/kg dose only; Rx (1-100 µg/Kg) diminished FXI activity (-71, -62, -66; p<0.05), while E2 (1 and 10 µg/Kg) diminished it in -60 and -38, respectively (p<0.05); Rx (1000 µg/Kg) produced an increment of 29% (p<0.05) in fibrinogen concentration, but not E2. Our findings suggest that raloxifene has a pro-tective effect on hemostasis in rats.
Keywords:
raloxifene
; 17β-Estradiol
; hemostasis
; ovariectomized rats
; thrombosis
1. Introduction
Raloxifene (Rx, Optruma®—Eli Lilly or Evista®—Daiichi Sankyo) currently has FDA-approval to be used for the treatment and profilaxis of postmenopausal osteoporosis [1]. Rx is a structural analogue of tamoxifen and belongs to the second generation selective benzothiophene group of selective estrogen receptor modulators (SERMs). Rx is a non-steroidal compound that acts as an ER ligand and has the unique characteristic of behaving as a selective agonist or antagonist depending on the function of certain tissues and the biological context in which they act. Like 17ꞵ-estradiol (E2), Rx is capable of crossing the cytoplasmic and nuclear membranes; once Rx is located in the nucleus, the benzothiophene ring can bind to the ER with an affinity equivalent to E2 [2,3]. The dual activity of the drug on the receptor is tissue specific, either acting as an estrogenic agonist (bone, lipid metabolism) or as an antagonist (uterus and breast), attributing this quality to some of the beneficial effects related to these signaling pathways, reporting a low incidence and severity of adverse effects [2,3].
Rx is rapidly absorbed after oral administration and is extensively bound to plasma proteins, having a wide distribution, and detected in most tissues minutes after ingestion, with the lowest concentration detected in the brain due to difficulty crossing the blood-brain barrier [4]. It undergoes first-pass effect and hepatic metabolism with formation of glucuronide conjugates; finally, it is eliminated mainly in the feces [4]. Although there is a low incidence of reported side effects, some of the known adverse effects of Rx are antithrombotic and vascular actions, involving suppression of oxidative stress, vasorelaxation, and regulation of endothelial reaction to trauma, a predictive indicator for vascular disease [5,6,7]. Despite its beneficial effects on preventing bone loss and reducing fracture risk, Rx therapy is significantly associated with an increased risk (2- to -3-fold) of deep venous thrombosis and pulmonary embolism. This increment might be due to its estrogenic effects on the coagulation and fibrinolytic systems [8,9]. In one report, Rx therapy in postmenopausal women induced a procoagulant state, observing higher plasma level of factor VIII, XI, and XII as well as a diminished APC sensitivity [10]. However, the mechanisms involved are not fully understood and further study is needed to explain Rx effects on the hemostasis and specific hemostatic parameters.
A useful model for the study of the effects of Raloxifene is through the use of ovariectomized (OVX) rats. The procedure of ovariectomizing a rat entails the surgical removal of the ovaries, thus removing the primary organ of estrogen biosynthesis, resulting in a reduction of the circulating levels of estradiol. Estrogens are involved in various physiological processes, and estradiol as well as SERMs can exert effects over distinct tissues such as bone, uterine, serum cholesterol, adipose tissues and on the hematological system [5,11], specifically OVX has been shown to cause a prothombotic state [5]. Therefore, many studies use this method to limit the effect of the internal production of estradiol when investigating the effects of these hormones on the coagulation system [11,12,13].
Estrogens are shown to be intricately involved in the regulation of the balance between a the procoagulant and anticoagulant activity in the blood, and the use of hormone replacement therapy or of treatment with SERMs has been shown to have diverse effects over this system [14]. It should be noted that the effects of raloxifene on the coagulation systems have mixed findings. In a randomized control trial of breast cancer prevention in postmenopausal women, treatment with Rx had a 3-fold increase in the risk for venous thrombosis [15]. Similarly, the current use of raloxifene in women with breast cancer was associated with a 7-fold increase in the risk for idiopathic venous thromboembolism in the absence of any other risk factors [16]. Moreover, in OVX pigs, Rx treatment increased the production of proaggregatory prostanoids [17].
On the other hand, Rx has also demonstrated beneficial homeostatic effects, preventing thrombotic events, as shown by Abu-Fanne et al. in OVX mice, where Rx reduced intravascular thrombosis and increased the expression of cyclooxygenase-2 and suppressing the adhesion of platelets [5]. Rx has also been suggested to reduce the risk of thrombosis through the effects directly on the vascular tissue. In aortic strips from OVX rats, Rx treatment has been shown to inhibit platelet aggregation, the direct effect over the vascular tissue increased the production of nitric oxide, preventing the formation of blood clots [13]. However, in another study there was no change in NO production in OVX rats treated with Rx, but the levels of von Willebrand factor were lowered and plasminogen activator inhibitor 1 (PAI-1) was increased compared to the control group [12]. These discrepancies may be due to variations in study design, dosage regimens, species, and specific parameters assessed.
To explore that area, we evaluated the effects of Rx on female ovariectomized rats, and we compared them with the effects of 17ß-estradiol (E2), the classic agonist estrogenic compound.
2. Materials and Methods
Materials
Raloxifene (hydrochloride [6-hydroxy-2-(4-hydroxyphenyl)-1-benzothiophen-3-yl]-[4-(2-piperidin-1-ylethoxy) phenyl] methanone), 17ß-estradiol (E2) (1,3,5(10)-estratrien-3,17ß-diol), tert-amyl alcohol, 2,2,2-tribromoethanol, and propyleneglycol were purchased from Sigma-Aldrich (St. Louis, MO, USA). Thromboplastin C plus, Actin FS, coagulation factors deficient plasmas (FVII, FX, FXI), bovine thrombin, standard human plasma, veronal, and imidazole buffer solution were purchased from Dade® Behring® (Marburg, Germany). Vacutainer blood collection tubes with buffer sodium citrate and Safety-LokTM collection sets were purchased from Becton, Dickinson, and Co. (Franklin Lakes, NJ, USA).
Animals
The experiments were carried out under the approval of the ethics and research committee of the Faculty of Medicine of the National Autonomous University of Mexico and under the standards of the official Mexican norm (NOM-062-ZOO-1999). Adult Wistar rats (Ratuss Norvegicus) weighing 200 to 225 g from the Faculty of Medicine's vivarium were used. The animals were kept under controlled light and dark conditions of cycles of 12 h, humidity of 40 %, temperature of 22 °C to 24 °C, and were kept in polypropylene boxes (4 rats per box). They received purified water and lab diet 5001. All testing were made in rigorous accordance with the international regulations of the National Institutes of Health Guide for the Care and Use of Laboratory Animals (NIH publication N0. 80–23 revised in 1996).
Ovariectomy
The rats were ovariectomized (surgical removal of the ovaries), implying that they are in a state of estrogen deficiency. Ovariectomy models have significantly contributed to our understanding of the role of raloxifene and estrogen in the context of hemostasis and thrombosis [12]. Rats were ovariectomized under anesthesia with 0.2 g/kg tribromoethanol/tert-amyl alcohol, through intraperitoneal administration. After ovarian tubal ligation, the ovaries were removed from the uterine horns by a dorsal section, the uteri were tied with chromic gut surgical suture 4-0 and the dorsal incisions were closed. The animals were placed in clean cages in a warm environment for recovery.
Experimental design
After 11 days of recovery, ovariectomized rats were distributed into nine groups according to their body weight, four rats were assigned to each group. The first group was the control group which received the vehicle propylene glycol (0.3 ml). The second to fifth group received Rx (1, 10, 100, or 10000 µg/Kg). The sixth to ninth group received E2 (1, 10, 100, or 1000 µg/Kg). All doses were administered subcutaneously for three consecutive days and the experiment was performed in triplicate.
Blood and plasma collection
In research studies involving ovariectomized rats, blood and plasma collection are common procedures performed to analyze hematological parameters [12]. A day after the last injection, the rats in all groups fasted overnight with ad libitum access to water, then they were anesthetized and euthanized with Avertin (ip, 250 mg/kg, tert-amyl alcohol/2,2,2-tribromoethanol) through intraperitoneal administration. Blood samples were collected from the iliac artery using a Vacutainer® system into citrated (0.105 M) tubes (Dickinson and Company, Franklin Lakes, NJ, USA) as an anticoagulant. Each sample was centrifuged at 20-22°C during 10 minutes at 800 g (3000 rpm) and plasma was separated. All samples were stored at -20°C util assays. It's important to follow appropriate animal handling and ethical guidelines while performing blood and plasma collection in ovariectomized rats. This includes using aseptic techniques, ensuring proper anesthesia, and minimizing stress or discomfort to the animals.
Determination of Prothrombin time (PT) and activated partial thromboplastin time (APTT)
Prothrombin Time (PT) and Activated Partial Thromboplastin Time (APTT) are two common laboratory tests used to evaluate the clotting ability of blood and assess the functionality of the coagulation system. These tests are standard tools useful for the diagnosis and monitoring of various bleeding and clotting disorders. PT and APTT were determined in a semiautomatic coagulometer, according to Quick [18], and Proctor and Rapaport methods [19], respectively. To activated PT, we added thromboplastin C plus. Samples (50 µl) were incubated for 60 s at 37° C, then thromboplastin C plus (37° C) was added. For APTT determinations, 50 µl of the sample was added and mixed with actin (50 µl) and incubated for 120 s at 37° C. The samples were activated by adding CaCl2 (50 µl).
The standardization of coagulation factors VII, X, and XI was done in accordance with García-Manzano [20]. Briefly, samples (50 µl) were incubated (37° C), with the plasma free of coagulation factors (50 µl) (VII, X, or XI). Samples were incubated at 37° C during 60s, and thromboplastin (50 µl) was added to activate the clot in factors VII and X. For factor XI determination, samples were mixed with actin (50 µl) and incubated at 37° C for 120 s and the clot was activate with the addition of CaCl2 (50 µl). It's worth noting that the PT and APTT tests are often performed together, along with other coagulation tests, to provide a comprehensive evaluation of the clotting system.
Standard curve of fibrinogen
The determination of fibrinogen levels in a blood sample can be performed using the Clauss methods [21]. This method is widely used and established for fibrinogen determination. It involves the measurement of the clotting time of fibrinogen in the presence of excess thrombin. The principle is based on the conversion of fibrinogen to fibrin by thrombin, resulting in the formation of a clot. The clotting time is inversely proportional to the fibrinogen concentration in the sample. In the Clauss method, a blood sample is collected in a citrate anticoagulant tube to prevent clotting. The plasma is then separated by centrifugation. To initiate clot formation, a standardized thrombin reagent is added to the plasma. The clotting time is measured using a coagulation analyzer or a manual method, and it is compared to a calibration curve or standard to determine the fibrinogen concentration. Plasma concentrations (mg/dl) were prepared with a veronal buffer as follows: 500 (4.4 s), 375 (5.9 s), 250 (8.4 s), 187 (9.1 s), 125 (23.7 s). Each sample was incubated for 120 s at 37°C and activated with diluted thrombin 1:2 (100 IU) [21].
Effects of Raloxifene and Estradiol on blood coagulation factors VII, X, and XI
To establish if both raloxifene and estradiol could have an effect over the blood coagulation factors VII, X, and XI in ovariectomized rats, you would typically follow a research study design specific to this animal model. The ovariectomized rats were randomly divided into different treatment groups, this included a control group (placebo or untreated), a raloxifene-treated group, and an estradiol-treated group. After the respective treatments with Rx and E2, the blood samples were obtained and centrifuged to obtain the plasma. Each sample were diluted with imidazole buffer. The dilution with imidazole buffer for factors VII and X (extrinsic and common pathway) was 1:20, whereas samples for factor XI determinations (intrinsic pathway), were diluted with imidazole buffer 1:5.
To determinate FVII and X activities, the samples (50 µl) were incubated at 37°C with plasma free of FVII or FX, for 60 s. To activate each factor thromboplastin was added (50 µl). For determination of FXI activity, we used samples treated with the compounds. Each sample (50 µl), was mixed with factor XI deficient plasma (50 µl), and actin (50 µl) and incubated during 120 s. The reaction was activated with the addition of CaCl2 (100 µl) prewarmed. All data obtained were extrapolated in the standard curve of each factor. Vehicle data were considered as 100%. These effects on coagulation factors should be considered in the context of overall hemostasis and thrombotic risk.
Determination of the effects of raloxifene and estradiol on fibrinogen concentrations
The effects of raloxifene and estradiol on fibrinogen concentrations in ovariectomized rats can be investigated through experimental studies. Randomly divide the ovariectomized rats into different treatment groups. This may include a control group (placebo or untreated), a raloxifene-treated group, and an estradiol-treated group. Fibrinogen was quantified with samples diluted 1:10 through the Clauss method [21]. Samples were incubated for 120 s at 37°C and activated with 100 µl of thrombin 1:2 (100 IU/ml). The data obtained in seconds were extrapolated to obtain the concentration.
Statistical methods
The differences in the response between the treated and control groups were evaluated through parametric tests: a one-way analysis of variance (ANOVA) followed by Dunnett's test ANOVA. Statistical significance was set at P values lower than 0.05 (p<0.05) bimarginally. All data were presented as percentage ± standard error of the mean (SEM). The vehicle was considered as 100 %. In all experiments, the value for n “15” corresponds to a different animal and all experiments were done in triplicate and analyzed with SigmaPlot 10 (Systat Software, San Jose, CA, USA).
3. Results
3.1.1. Raloxifene and estradiol effects on PT and APTT screening tests
We determined the effect of raloxifene and estradiol on the PT (Prothrombin Time) and APTT (Activated Partial Thromboplastin Time) screening tests, which are commonly used to evaluate the coagulation status of an individual. To evaluate differences between PT and APTT due to Rx and E2, we measured these parameters in blood serum. Figure 1A shows how Rx administered (1000 µg/Kg) significantly increased PT (8%; p<0.05), while the administration of E2 had no significant effect. Figure 1B shows that Rx (1, 10, 100 and 1000 µg/Kg) produced a significant increment (p<0.05) in APTT (32, 70, 67, 30%, respectively), whereas E2 did not show any effect on this parameter. Rx showed an important increased on APTT which is a marker of the intrinsic pathway of coagulation. It's important to note that the effects of raloxifene and estradiol on PT and APTT tests can be influenced by many factors, including the dosage, and duration of treatment.
3.1.2. Raloxifene and estradiol effects on extrinsic factor VII and common pathway factor X
Both raloxifene and estradiol can have effects on extrinsic factor VII and common pathway factor X, which are important components of the coagulation cascade. Figure 2A shows that Rx administration (1, 10, 100, and 1000 µg/Kg) significantly decreased the activity of factor VII by -20, -40, -37, and -17 % (p<0.05) respectively, whereas the administration of E2 produced a significant increment of 9, 34, 52, and 29% with all doses evaluated. Figure 2B shows that administration of 10 and 100 µg/Kg doses of Rx (p<0.05) produced a significant decrease of the activity of factor X by -30%, while a 1000 µg/Kg dose of E2 showed an increment of 24%. Rx decreased activity of both factors, as opposed to the effect with E2; however, their effects may differ due to their distinct mechanisms of action and interactions with estrogen receptors.
3.1.3. Raloxifene and estradiol effects on intrinsic factor XI and fibrinogen concentration
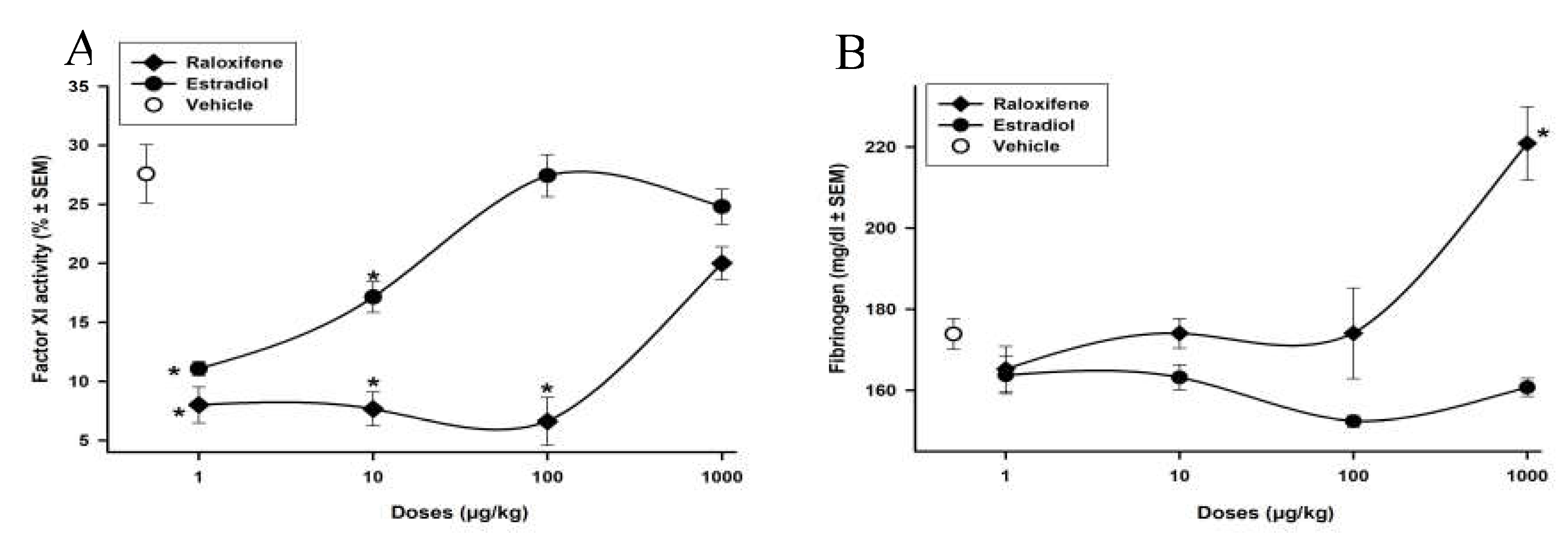
Studies investigating the effects of raloxifene and estradiol on intrinsic factor XI and fibrinogen in rats that have undergone ovariectomy (OVX) are limited. Our studies show in Figure 3A shows Rx and E2 effects on coagulation factor XI. The administration of Rx (1, 10, 100, and 1000 µg/Kg) produced a diminution in factor XI activity (-71, -62, -66 %; p<0.05), whereas E2 administration (1 and 10 µg/Kg) diminished factor XI activity in -60 and -38 % respectively (p<0.05). In this case, both compounds diminished intrinsic factor XI. Figure 3B shows the effect of Rx and E2 on fibrinogen concentrations. The administration of Rx (1000 µg/Kg) produced a significant increment 29% (p<0.05) in fibrinogen concentration. The administration of E2 produced a modest yet not significant decrease in fibrinogen concentration.
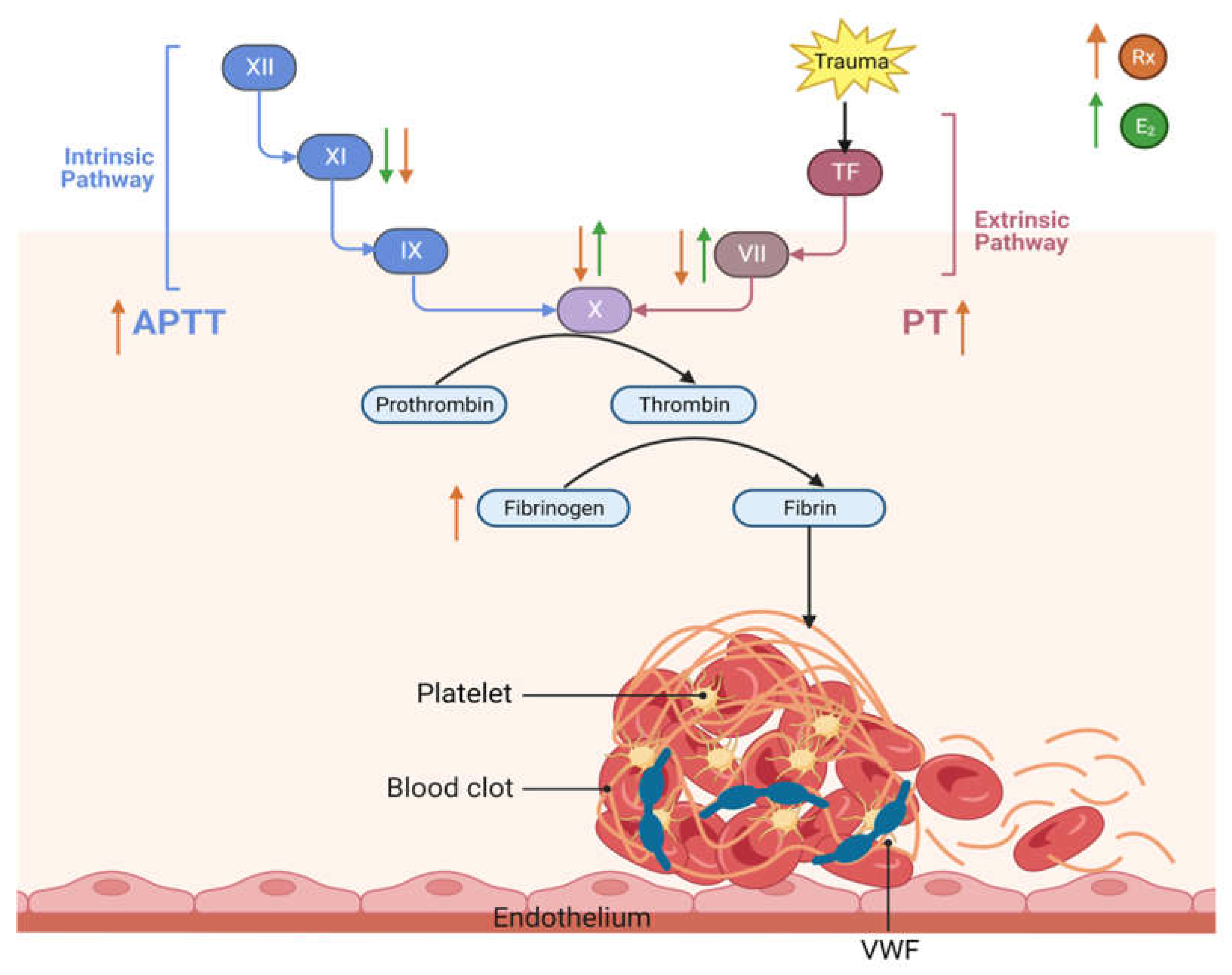
3.1.4. This diagram illustrates our current understanding of the effect of raloxifene and estrogen on hemostasis and thrombosis.
Figure 4.
Raloxifene and estradiol have contrasting effects on hemostasis and thrombosis due to their interactions with estrogen receptors and their impact on various components of the coagulation system. The orange arrows represent the effect of raloxifene while the green represent the effect of estradiol. Raloxifene showed an increased-on PT, APTT and Fibrinogen and produced a diminution in factor VII, X and XI activity. E2 induced an increment of factor VII and X activity and lowered factor XI, whereas it did not show any effect in PT and APTT.
Figure 4.
Raloxifene and estradiol have contrasting effects on hemostasis and thrombosis due to their interactions with estrogen receptors and their impact on various components of the coagulation system. The orange arrows represent the effect of raloxifene while the green represent the effect of estradiol. Raloxifene showed an increased-on PT, APTT and Fibrinogen and produced a diminution in factor VII, X and XI activity. E2 induced an increment of factor VII and X activity and lowered factor XI, whereas it did not show any effect in PT and APTT.
4. Discussion
This study reveals that Rx, a specific type of estrogen receptor modulator, affects three different hemostasis pathways in rats: the extrinsic, intrinsic, and common pathways. When it comes to the extrinsic pathway, the highest dosage of Rx led to an increase in prothrombin time and a notable decrease in factor VII activity, it could especially benefit patients at risk of venous thromboembolism as an alternative to estradiol and merits further study. On the other hand, E2 resulted in an increase in FVII activity. These results are in line with previous findings that suggest that a mid-term treatment with Rx in postmenopausal women who have endothelial dysfunction and ischemic heart disease does not affect their endothelial function. Even though the understanding of the effects of estrogen on the hemostasis and thrombosis systems is still incomplete, it has been shown to affect multiple variables that influence the balance between the procoagulant and anticoagulant properties. The effects of estrogen should especially be taken into consideration in patients that have other risk factors for thrombosis (e.g., age, smoking, obesity, comorbidities, genetic predisposition), especially when considering hormonal replacement therapy, and perhaps could benefit from a SERM alternative [22].
According to Roqué et al., raloxifene (Rx) had varying effects on hemostasis and thrombotic risk in postmenopausal women with ischemic heart disease. The study found that mid-term treatment with Rx did not have a significant effect on endothelial function in this group of women [23].
Interestingly, the effects of Rx seem to be associated with a chronological influence, in postmenopausal women treated with 60 mg daily of Rx in the morning for 12 months had higher plasma concentrations of plasminogen activated inhibitor (PAI)-1 in comparison with the group receiving the evening treatment. No additional changes were observed in other coagulation factors. It should be noted that elevated PAI-1 levels are associated with a risk of venous thromboembolism and should be considered when prescribing Rx [24]. In another study, hormone therapy in postmenopausal women with either Rx or tibolone for 12 weeks, in the group with a history of venous thrombosis there was an increase in sex hormone binding globulin (SHBG), which in turn was associated with a change in APC resistance, proposing that SHBG can be used as a biomarker to identify an increased risk in venous thrombosis in hormone therapy [25].
Regarding hemostasis, the study showed that Rx affected the extrinsic, intrinsic, and common pathways in rats. In particular, the highest dose of Rx produced an increment in prothrombin time and a significant inhibitory effect in factor VII activity, which is associated with increased thrombotic risk. However, the same study reported that Rx treatment did not have any effect on fibrinolytic activity, which is involved in the breakdown of blood clots and can help prevent thrombotic events. It is important to note that our findings with Raloxifene had similar results. In our study with rats, we also observed that Raloxifene had varying effects on hemostasis and thrombotic risk. Specifically, the highest dose of Raloxifene resulted in an increase in prothrombin time and a significant inhibitory effect in factor VII activity, which suggests an increased thrombotic risk. However, we did not find any significant effect of Raloxifene on fibrinolytic activity, which is involved in the breakdown of blood clots and can help prevent thrombotic events [23].
It has been found that there are distinct differences in the effects of raloxifene and estrogen on coagulation factors, indicating that plasma levels of coagulation factors are regulated by independent mechanisms. One significant difference between raloxifene and estrogen is that only raloxifene decreased the levels of coagulation factors VII, X, and XI. In the intrinsic pathway, raloxifene led to a notable increase in activated partial thromboplastin time. Both raloxifene and estrogen reduced the activity of factor XI, but only at low doses. In terms of the common pathway, raloxifene decreased the activity of factor X, whereas estrogen showed the opposite effect. These findings suggest that raloxifene and estrogen have varying effects on different coagulation factors and pathways, highlighting the importance of careful consideration when prescribing these medications for patients with a history of thrombotic events or other relevant medical conditions [26].
Only the highest dose of Rx produced a significant increase in fibrinogen concentrations. Fibrinogen is an independent risk factor of initial cardiovascular events related to venous and arterial thrombosis [27,28]. In 2001, Cushman reported that Rx appears to have more positive effects than hormone replacement therapy in fibrinogen lowering [29]. Therefore, when Rx is prescribed to postmenopausal women with osteoporosis it is fundamental to take into consideration the dosing times in order for plasma levels not to increase until a concentration where the cardioprotective effect is lost [30]. Our findings support past reports in mice that stated that 4 months of treatment with Rx attenuates intravascular thrombosis. They showed that the antithrombotic effect was be associated with by an improved expression of cyclooxygenase-2 (COX2) and inhibition of platelet surface adhesion [5].
In contrast to our findings, Cosman's research demonstrated that estrogen, tamoxifen, and raloxifene have pro-coagulation effects and impair anticoagulation in postmenopausal women, differing subtly from the effects of estrogen. Overall, our findings suggest that raloxifene can positively impact coagulation markers related to cardiovascular risk, and we observed a protective effect of raloxifene in the acute treatment of hemostasis in rats.
5. Conclusions
This present study supports evidence the hemostatic effects of raloxifene in ovariectomized rats. The results demonstrated that treatment with raloxifene modulates key aspects in both the extrinsic and intrinsic pathways of coagulation, as observed by the significant increment in both the prothrombin time and activated partial thromboplastin time. This effect of raloxifene was caused by regulating the activity of coagulation factors VII and XI, while increasing fibrinogen concentration. These findings suggest that raloxifene modify coagulation parameters, decrease the risk of thrombosis in ovariectomized rats thereby showcasing its potential as a therapeutic option for conditions such as osteoporosis, especially in patients with a risk of venous thrombosis. It is important to note that the exact hemostatic effects of raloxifene may vary depending on the dosage, duration of treatment, and individual characteristics of the experimental models. However, further studies are necessary to elucidate the underlying mechanisms of Rx's hemostatic effects and to evaluate its safety profile in human subjects.
Author Contributions
D.A.C.H. conceived and performed the experiments, analyzed the results, and writing—original draft preparation. M.S.N., and E.F.S., contributed to the literature search, performed the experiments, data curation, review and editing the manuscript R.J., conceived and designed the study, drafted the initial manuscript, analyzed the data, revised the manuscript for important intellectual content and funding acquisition. All authors have read and approved to the published version final of the manuscript.
Funding
This study was supported by grants from the Dirección General de Asuntos del Personal Académico (PAPIIT-DGAPA, IN224211-2 and IN224120) and Department of Pharmacology grants and carried out at Facultad de Medicina, Universidad Nacional Autónoma de México.
Institutional Review Board Statement
All experiments were conducted according to the Mexican official standard which indicates the methodological specifications for the production, care, and use of lab animals (NOM-062-ZOO-1999). The Ethics Committee in research and animal care of the Faculty of Medicine approved the protocol.
Informed Consent Statement
Not applicable.
Acknowledgments
The authors would like to thank Josefina Bolado and Brenda Sandoval Meza, part of the Scientific Paper Translation Department at the Research Division, for editing the English-language version of this manuscript; to Ana María García-Maynez, Isabel Arce Camacho, Rubén González-Alfaro, Rosa Rubí García-Gómez, Israel Zarate-Trejo and Ma. Concepción Limón-Rodríguez for their technical assistance, at Facultad de Medicina, Universidad Nacional Autónoma de México.
Conflicts of Interest
The authors declare no conflict of interest or personal relationships that could have influenced the data reported in this paper.
References
- Berman, H.; Henrick, K.; Nakamura, H. Announcing the worldwide Protein Data Bank. Nat Struct Biol 2003, 10, 980. [Google Scholar] [CrossRef] [PubMed]
- Hernández, E.; Valera, R.; Alonzo, E.; Bajares-Lilue, M.; Carlini, R.; Capriles, F.; Martinis, R.; Bellorin-Font, E.; Weisinger, J.R. Effects of raloxifene on bone metabolism and serum lipids in postmenopausal women on chronic hemodialysis. Kidney In. 2003, 63, 2269–2274. [Google Scholar] [CrossRef]
- Lewis, J.S.; Jordan, V.C. Selective estrogen receptor modulators (SERMs): mechanisms of anticarcinogenesis and drug resistance. Mutat Res 2005, 591, 247–263. [Google Scholar] [CrossRef]
- Ang, Z.; He, X.; Zhang, Y. The determination of raloxifene in rat tissue using HPLC. Biomed Chromatogr 2007, 21, 229–233. [Google Scholar] [CrossRef] [PubMed]
- Abu-Fanne, R.; Brzezinski, A.; Golomb, M.; Grad, E.; Foldes, A.J.; Shufaro, Y.; Varon, D; Brill, A. ; Lotan, C.; Danenberg, H.D. Effects of estradiol and raloxifene on arterial thrombosis in ovariectomized mice. Menopause 2008, 15, 98–104. [Google Scholar] [CrossRef] [PubMed]
- Ferretti, G.; Bacchetti, T.; Simental-Mendía, L.E.; Reiner, Z.; Banach, M.; Sahebkar, A. Raloxifene lowers plasma lipoprotein(a) concentrations: A systemic review and meta-analysis of randomized placebo-controlled trials. Cardiovasc Drugs Ther 2017, 31, 197–208. [Google Scholar] [CrossRef]
- Meyer, M.R.; Barton, M. Estrogens and coronary artery disease: New clinical perspectives. Adv Pharmacol 2016, 77, 307–360. [Google Scholar]
- Barrett-Connor, E.; Mosca, L.; Collins, P.; Geiger, M.J.; Grady, D.; Kornitzer, M.; McNabb, M.A.; Wenger, N.K. Effects of raloxifene on cardiovascular events and breast cancer in postmenopausal women. N Engl J Med 2006, 355, 125–137. [Google Scholar] [CrossRef]
- Gizzo, S.; Saccardi, C.; Patrelli, T.S.; Berretta, R.; Capobianco, G.; Di Gangi, S.; Vacilotto, A.; Bertocco, A.; Noventa, M.; Ancona, E. Update on raloxifene: mechanism of action, clinical efficacy, adverse effects, and contraindications. Obstet Gynecol Surv 2013, 68, 467–481. [Google Scholar] [CrossRef]
- Azevedo, G.D.; Franco, R.F.; Baggio, M.S.; Maranhao, T.M.; Ferriani, M.F.; Silva de Sa, M.F. Effects of raloxifene therapy on the anticoagulant system in postmenopausal women. Climacteric 2003, 6, 140–145. [Google Scholar] [CrossRef]
- Sato, M.; Rippy, M. K.; Bryant, H. U. Raloxifene, tamoxifen, nafoxidine, or estrogen effects on reproductive and nonreproductive tissues in ovariectomized rats. FASEB journal: official publication of the Federation of American Societies for Experimental Biology 1996, 10, 905–912. [Google Scholar] [CrossRef]
- Gao, H.; Xi, S.; Xu, L. [Effects of raloxifene combined with conjugated equine estrogen on prothrombotic state in ovariectomized rats]. Zhonghua Fu Chan Ke Za Zhi 2013, 48, 935–938. [Google Scholar]
- Polini, N.; Rauschemberger, M. B.; Mendiberri, J.; Selles, J.; Massheimer, V. Effect of genistein and raloxifene on vascular dependent platelet aggregation. Molecular and cellular endocrinology 2007, 267, 55–62. [Google Scholar] [CrossRef] [PubMed]
- Rosendaal, F. R.; Helmerhorst, F. M.; Vandenbroucke, J. P. Female Hormones and Thrombosis. Arteriosclerosis, Thrombosis, and Vascular Biology 2002, 22, 201–210. [Google Scholar] [CrossRef] [PubMed]
- Cummings, S. R.; Eckert, S.; Krueger, K. A.; Grady, D.; Powles, T. J.; Cauley, J. A.; Norton, L.; Nickelsen, T.; Bjarnason, N. H.; Morrow, M.; Lippman, M. E.; Black, D.; Glusman, J. E.; Costa, A.; Jordan, V. C. The effect of raloxifene on risk of breast cancer in postmenopausal women: results from the MORE randomized trial. Multiple Outcomes of Raloxifene Evaluation. JAMA 1999, 281, 2189–2197. [Google Scholar] [CrossRef] [PubMed]
- Meier, C. R.; Jick, H. Tamoxifen and risk of idiopathic venous thromboembolism. British journal of clinical pharmacology 1998, 45, 608–612. [Google Scholar] [CrossRef]
- Lewis, D. A.; Avsar, M.; Labreche, P.; Bracamonte, M.; Jayachandran, M.; Miller, V. M. Treatment with raloxifene and 17beta-estradiol differentially modulates nitric oxide and prostanoids in venous endothelium and platelets of ovariectomized pigs. Journal of cardiovascular pharmacology 2006, 48, 231–238. [Google Scholar] [CrossRef]
- Quick, A.J. Normal values for coagulation test. N Engl J Med 1954, 290, 751. [Google Scholar]
- Proctor, R.R.; Rapaport, S. The partial thromboplastin time with kaolin. A simple screening test for first stage plasma clotting factor deficiencies. Am J Clin Pathol 1961, 36, 212–219. [Google Scholar] [CrossRef]
- García-Manzano, A.; González, LJ.; Lemini, C.; Rubio-Póo, C. Standardization of rat blood clotting tests with reagents used for humans. Proc West Pharmacol Soc 2001, 44, 153–155. [Google Scholar]
- Clauss, A. Coagulation fast method for the determination of fibrinogen. Acta Hematol 1957, 17, 237–240. [Google Scholar] [CrossRef]
- Abou-Ismail, M. Y. , Citla Sridhar, D., & Nayak, L. Estrogen and thrombosis: A bench to bedside review. Thrombosis research 2020, 192, 40–51. [Google Scholar] [PubMed]
- Roqué, M.; Sitges, M.; Sala, J.; Delgado, V.; Morales, M.; Marrugat, J.; Vila, J.; Subirana, I.; Tàssies, D.; Reverter, J.C. Effects of raloxifene on endotelial function and hemostasis in women with ischemic heart disease. Rev Esp Cardiol 2011, 64, 572–578. [Google Scholar] [CrossRef]
- Ando, H.; Otoda, T.; Ookami, H.; Nagai, Y.; Inano, A.; Takamura, T.; Ushijima, K.; Hosohata, K.; Matsushita, E.; Saito, T.; Kaneko, S. : Fujimura, A. Dosing time-dependent effect of raloxifene on plasma plasminogen activator inhibitor-1 concentrations in post-menopausal women with osteoporosis. Clinical and experimental pharmacology & physiology 2013, 40, 227–232. [Google Scholar]
- Eilertsen, AL.; Dahm, AEA. ; Høibraaten, E.; Lofthus, CM.; Mowinckel, MC.; Sandset, PM. Relationship between sex hormone binding globulin and blood coagulation in women on postmenopausal hormone treatment. Blood coagulation & fibrinolysis: an international journal in haemostasis and thrombosis 2019, 30, 17–23. [Google Scholar]
- Cosman, F.; Baz-Hecht, M.; Cushman, M.; Vardy; M. D.; Cruz, J.D.; Nieves, J.W.; Zion, M.; Lindsay, R. Short-term effects of estrogen, tamoxifen and raloxifene on hemostasis: a randomized-controlled study and review of the literature. Thrombosis Res 2005, 116, 1–13. [Google Scholar] [CrossRef]
- Kannel, W. Influence of fibrinogen on cardiovascular disease. Drugs 1997, 54, 32–40. [Google Scholar] [CrossRef]
- De la Serna, G. Fibrinogen: a new major risk factor for cardiovascular disease. A review of the literature. J Fam Pract 1994, 39, 468–477. [Google Scholar] [PubMed]
- Cushman, M. Effects of estrogen and selective estrogen receptor modulators on hemostasis and inflammation. Ann N Y Acad Sci 2001, 949, 175–180. [Google Scholar] [CrossRef]
- Tsuruoka, S.; Hasegawa, G.; Kaneda, T.; Maeda, A.; Fujimura, A. Dosing time-dependent effect of raloxifene on plasma fibrinogen concentration in ovariectomized rats. Chronobiol Int 2008, 25, 808–818. [Google Scholar] [CrossRef]
Figure 1.
Raloxifene (⧫) an estradiol (•) on prothrombin (A) and thromboplastin (B) time. Each point represents the mean ± SEM of 15 determinations. * P<0.05 vs vehicle (o) Dunnett´s test.
Figure 1.
Raloxifene (⧫) an estradiol (•) on prothrombin (A) and thromboplastin (B) time. Each point represents the mean ± SEM of 15 determinations. * P<0.05 vs vehicle (o) Dunnett´s test.
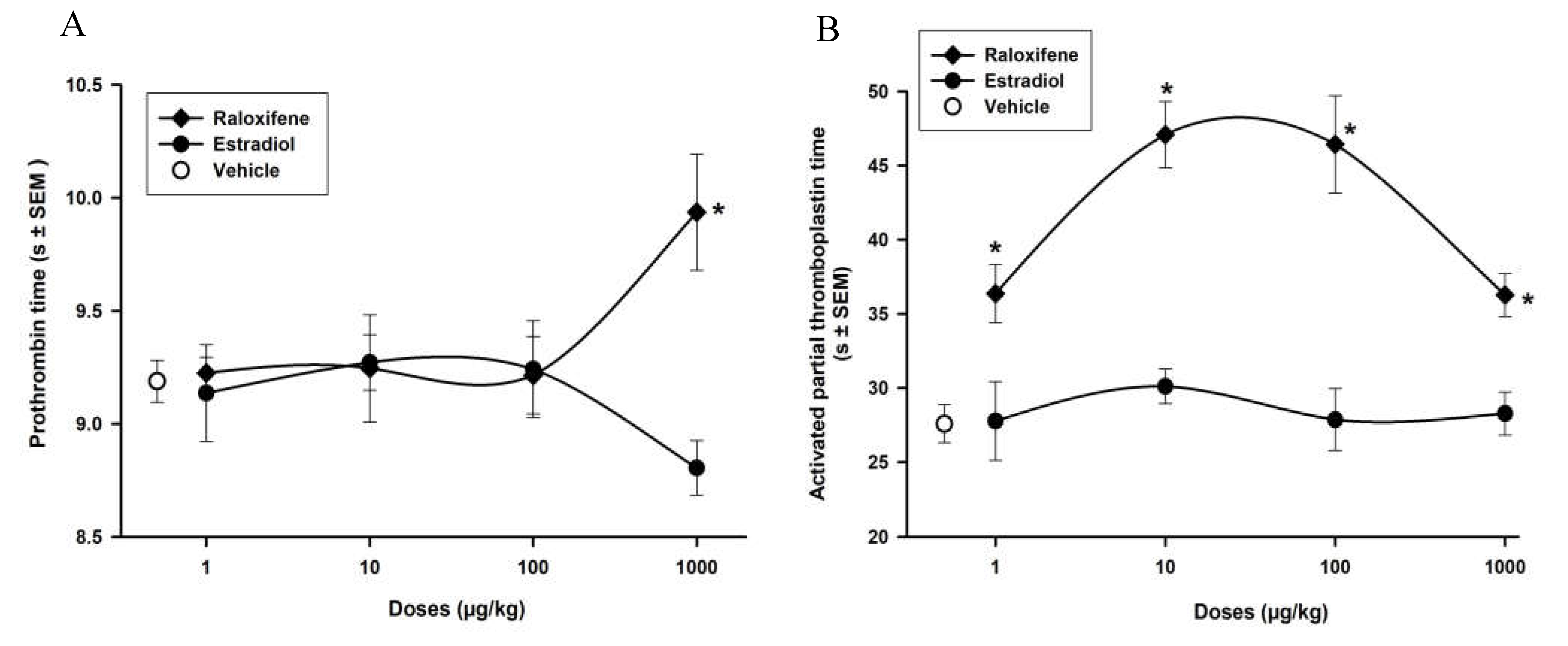
Figure 2.
Raloxifene (⧫) an estradiol (•) on activity of coagulation factor VII (A) and X (B). Each point represents the mean ± SEM of 15 determinations. * P<0.05 vs vehicle (o) Dunnett´s test.
Figure 2.
Raloxifene (⧫) an estradiol (•) on activity of coagulation factor VII (A) and X (B). Each point represents the mean ± SEM of 15 determinations. * P<0.05 vs vehicle (o) Dunnett´s test.
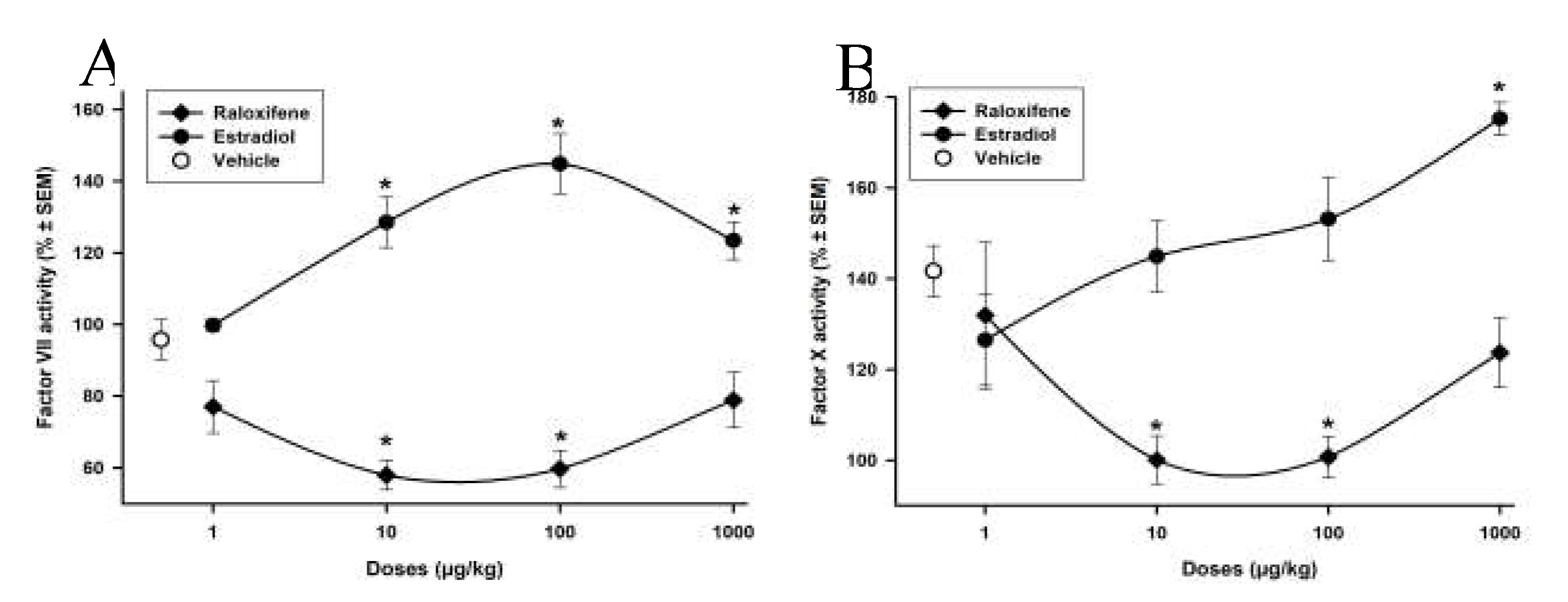
Figure 3.
Raloxifene (⧫) an estradiol (•) on activity of coagulation factor VII (A) and fibrinogen concentrations (B). Each point represents the mean ± SEM of 15 determinations. * P<0.05 vs vehicle (o) Dunnett´s test.
Figure 3.
Raloxifene (⧫) an estradiol (•) on activity of coagulation factor VII (A) and fibrinogen concentrations (B). Each point represents the mean ± SEM of 15 determinations. * P<0.05 vs vehicle (o) Dunnett´s test.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions, or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



