
Submitted:
29 June 2023
Posted:
30 June 2023
You are already at the latest version
Abstract
The tumor microenvironment of colorectal cancer (CRC) is heterogenous; thus, it is likely that multiple immune-related and inflammatory markers are simultaneously expressed in the tumor. The aim of this study was to identify immune-related and inflammatory markers expressed in freshly frozen CRC tissues and to investigate whether they are related to the clinicopathological features and prognosis of CRC. Seventy patients with CRC who underwent curative surgical resection between December 2014 and January 2017 were included in this study. Tissue samples were obtained from tumor and non-tumor areas in the patients’ colons. The concentrations of immune-related markers (APRIL/TNFSF13, BAFF, LAG-3, PD-1, PD-L1, and CTLA-4) and inflammatory markers (CHIT, MMP-3, osteocalcin, pentraxin-3, sTNF-R1, and sTNF-R2) in the samples were measured using the Bio-plex Multiplex Immunoassay system. The concentrations of APRIL/TNFSF13, BAFF, and MMP-3 in the samples were significantly high; thus, we conducted analyses based on the cutoff values for these three markers. The high APRIL/TNFSH13 expression group showed a significantly higher rate of metastatic lesions than the low expression group, whereas the high MMP-3 expression group had higher CEA levels, more lymph node metastases, and more advanced disease stages than the low expression group. The five-year disease-free survival of the high MMP-3 expression group was significantly shorter than that of the low expression group (65.1% vs. 90.2%, p=0.033). This study provides evidence that the APRIL/TNFSF13, BAFF, and MMP-3 pathway is overexpressed CRC tissues and is associated with unfavorable clinicopathological features and poor prognosis in CRC patients. These markers could serve as diagnostic or prognostic biomarkers for CRC.
Keywords:
Colorectal neoplasm
; Biomarkers
; Bioplex
; Immune checkpoint proteins
1. Introduction
In recent years, immunotherapy using immune checkpoint inhibitors (ICIs) has been receiving increasing attention as an effective therapeutic option for the treatment of advanced, metastatic, and recurrent colorectal cancer (CRC) [1,2]. Immunotherapy using ICIs can reverse tumor immune escape by suppressing immune checkpoint pathways. Representative immune checkpoint target molecules include programmed cell death protein 1 (PD-1), programmed death ligand 1 (PD-L1), and cytotoxic T-lymphocyte-associated protein 4 (CTLA-4). The efficacy of ICI therapy for the treatment of various malignant tumors, such as melanoma, lung cancer, and prostate cancer, has been demonstrated [3,4,5,6]. For the treatment of CRC, ICI therapy has been partially proven to be effective and is used in clinical settings. Currently, ICIs are used on a limited basis for the treatment of patients with stage IV metastatic CRC and have been reported to have some effect in patients with the DNA mismatch repair-deficient (dMMR)/microsatellite instability-high (MSI-H) genetic phenotype. However, some patients do not respond to immunotherapy; therefore, its effect has not been clearly identified [7,8]. Additionally, ICIs are ineffective for the treatment of tumors with specific genetic phenotypes, such as the mismatch-repair-proficient (pMMR) and microsatellite-stable (MSS) phenotypes, or tumors with low levels of microsatellite instability (MSI-L) [9]. As tumors with the MSI-H phenotype account for only 5–15% of all CRC cases, development of immunotherapy for pMMR/MSS tumors with few genetic variants is urgently needed [10]. To do so, it is essential to discover not only MSI status but also novel immune-related markers that can predict the efficacy of immunotherapy for cancer treatment. Overexpression of various immune-related markers in tumors has been reported in several studies. However, to the best of our knowledge, there has been no clear conclusion that these markers are related to clinicopathological features and long-term outcomes [11,12,13].
Given the heterogeneous nature of the tumor microenvironment (TME), it is likely that multiple immune-related and inflammatory markers are simultaneously expressed in tumors, contributing to the complexity of tumor-immune interactions. Understanding the expression patterns and effects of these markers in the TME is critical for developing effective cancer therapies that harness the power of the immune system to fight cancer [14].
Therefore, the aim of this study was to identify immune-related and inflammatory markers expressed in CRC tissue that had been stored as freshly frozen samples and to investigate whether they are related to clinicopathological features and prognosis. In particular, rather than use a traditional enzyme-linked immunosorbent assay (ELISA), we attempted to efficiently identify these markers using the Bio-plex Multiplex immunoassay, which has not been used in previous studies.
2. Results
2.1. Patient Characteristics
Seventy patients were included in this study. The mean age of the patients was 69.6 years and 38 (54.3%) of them were male. Nineteen (27.1%) and 27 (25.7%) patients had right- and left-sided colon cancer, respectively, whereas 24 (34.3%) had rectal cancer. Fifty-five (78.6%) patients underwent minimally invasive surgery, including laparoscopic or robotic surgery. Thirty-one (44.3%) patients had stage III disease, which was the most common disease stage, and the average number of metastatic lymph nodes recorded was 2.2. Sixty-three (91%) patients had MSS (91%), four had MSI-H (5%), and three (4%) had unverifiable MSI information. Forty-six (65.7%) patients received postoperative chemotherapy, whereas only one (1.4%) patient received radiation treatment. During the follow-up period, 17 (24.3%) patients showed cancer recurrence, and five (7.1%) patients died. The patient characteristics are summarized in Table 1.
2.2. Immune-Related and Inflammatory Markers in Tumor Tissues
Table 2 shows the results of the multiplex immunoassay for immune-related and inflammatory markers in tumor tissues. Among the various markers identified in the tumor tissues, a proliferation-inducing ligand (APRIL/TNFSF13), B-cell activating factor (BAFF), and matrix metalloproteinase-3 (MMP-3) showed significantly high concentrations. Scatter plots that show the distribution of the immune marker levels are outlined in Figure 1.
2.3. Relationships between Immune-Related and Inflammatory Markers and Clinicopathologic Features
We set cut-off values for each of the three above-mentioned immune-related and inflammatory markers significantly high in tumor tissues and analyzed the differences in clinicopathological features between the low and high expression groups. APRIL/TNFSH13 and BAFF were grouped based on quartile 3 values of 806.4 and 664.0, respectively, whereas MMP-3 was grouped based on the quartile 1 value of 736.2. There were no differences in basic patient characteristics, such as age, body mass index, American Society of Anesthesiologists score, and medical history, between the subgroups. The high APRIL/TNFSH13 expression group showed a significantly higher rate of metastatic lesions (ML) than the low APRIL/TNFSH13 expression group (11.8% vs. 36.8%, P =0.03); therefore, the proportion of patients with stage IV disease was high. Additionally, neutrophil-lymphocyte ratio, one of the serologic markers, was significantly higher in the APRIL/TNFSH13 high expression group than the low APRIL/TNFSH13 expression group (4.1 vs. 2.7, respectively, p=0.04). The high BAFF expression group had a significantly higher five-year recurrence rate than the low BAFF expression group (12 [23.1%] vs. 5 [27.8%], p=0.03). Compared to the low expression group, the MMP-3 high expression group had more patients with a CEA level ≥5 (44.7% vs. 17.4%, p=0.04). In addition, the high MMP-3 expression group had a higher proportion of patients with T4 disease than the low MMP-3 expression group (15 [31.9%] vs. 1 [4.3%], p=0.01). Furthermore, the mean number of metastatic lymph nodes in the high MMP-3 expression group was 2.7, which was significantly higher than that of the low MMP-3 expression group, 1.1 (p=0.02), and there were many patients in advanced stages disease, such as stage 3 and 4 disease (p=0.04) (Table 3).
2.4. Relationships between Immune-Related and Inflammatory Markers and Long-Term Oncologic Outcomes
Of the three above-mentioned markers, only MMP-3 was associated with five-year disease-free survival (DFS). The five-year DFS of the high MMP-3 expression group was significantly lower than that of the low MMP-3 expression group (65.1% vs. 90.2%, p=0.033). In addition, there was no difference in five-year overall survival (OS) between the two groups (90.0% vs. 95.7%, p=0.489). For APRIL/TNFSH13 and BAFF, there was no difference between the survival curves of the high and low expression groups (Figure 2).
3. Discussion
In this study, we investigated the expression of immune-related and inflammatory markers in CRC tissue samples. The results indicated that APRIL/TNFSF13, BAFF, and MMP-3 are highly expressed in CRCs. Analyses performed according to expression levels of these markers confirmed that high expression of immune-related and inflammatory markers was associated with advanced clinicopathological features. In addition, the results revealed that high expression of MMP-3 was associated with elevated CEA levels, more lymph node metastases, and more advanced disease stages. Furthermore, the results indicated that MMP-3 expression level was associated with long-term prognoses, such as five-year DFS. Moreover, the high APRIL/TNFSH13 expression group showed a higher rate of metastatic lesions than the low APRIL/TNFSH13 expression group.
The MMPs are a family of at least 28 zinc-dependent enzymes. Their main function is catalyzing proteolytic activities and aiding the breakdown of the extracellular matrix. It is upregulated in response to inflammation and has been shown to be involved in the development and progression of several inflammatory and autoimmune diseases, as well as cancer. They induce tumor invasion, neoangiogenesis, and metastasis by degrading the connective tissues between cells and in the lining of blood vessels [15]. Several studies have demonstrated that MMPs are highly expressed in malignant tumors compared with normal tissue [12,16,17]. There are several subtypes of MMPs, and studies on the role of each subtype have been conducted [16,18]. Yu et al. [16] analyzed the mRNA expression levels of all 24 MMPs and their prognostic values in CRC. The authors suggested that the transcriptional levels of MMP1, MMP3, MMP7, MMP9–MMP12, and MMP14 are significantly upregulated in tumors. In addition, their analysis showed that upregulation of MMP11, MMP14, MMP17, and MMP19 is significantly associated with a more advanced tumor stage and worse long-term prognosis. Another study by Islekel et al.[11] demonstrated that the protein expression levels of MMP-3 in tumor tissues are higher than those in normal tissues, and that the expression level of MMP-3 is related to lymph node status. These findings are consistent with the results of the present study.
APRIL/TNFSF13 is a tumor necrosis factor (TNF) protein that plays an important role in the development of B cells, which are involved in immune function [19]. This protein is expressed by immune cells in bone marrow and peripheral tissues under normal physiological conditions. APRIL is produced by various types of tumor cells, including breast, gastric, bladder, and ovarian cancers [20,21,22,23]. Several studies have suggested that APRIL is overexpressed in CRC tissues, and that increased APRIL expression is associated with poor prognosis in patients with CRC [24,25,26]. Similar to the results of the present study, a study by Lascano et al. [24] demonstrated that distant metastasis is more frequent in patients that show high APRIL expression than in those that show low APRIL expression; however, APRIL expression level is not an independent factor for OS.
BAFF is a member of the TNF superfamily and is mainly produced by myeloid cells. BAFF plays a role in immune function regulating B cell survival, activation, and maturation. Previous studies have demonstrated that BAFF plays a role in neoplasm progression and aggressiveness [27,28]. In addition, both BAFF and APRIL signaling may increase tumor cell proliferation and enhance tumor cell viability in response to chemotherapeutic drugs for hematopoietic malignancies. Interestingly, elevated blood levels of BAFF and APRIL are associated with an advanced disease stage and invasiveness of cancers such as breast cancer, chronic lymphocytic leukemia, and pancreatic cancer [28,29]. However, the relationship between BAFF expression and disease progression is not consistent in all cancers [30]. A study has shown that the expression of BAFF in CRC tissues is higher than that in normal tissues; however, there has been no analysis of the association between BAFF expression and disease severity [13]. In the present study, high BAFF expression was observed; however, its correlations with clinicopathological features and long-term outcomes were not confirmed.
Taken together, the April/TNFSF13, BAFF/TNFSF13B, and MMP-3 pathway plays a critical role in the regulation of the immune system, and dysregulation of this pathway can lead to the development of cancer. Theoretically, these above-mentioned markers that were overexpressed in CRC tissues in the present study can be used as treatment targets. In fact, several studies have been conducted to evaluate the potential of these markers as therapeutic targets. MMP-3 has also been studied as a potential therapeutic target for CRC [31]. The results of an in vitro study by Wen et al. suggested that histone deacetylase 11 (HDAC11) inhibits the migration and invasion of CRC cells by downregulating MMP-3 expression. Additionally, the authors found that HDAC11 is downregulated in human CRC tissues, and that decreased HDAC11 level is correlated with advanced clinical stage and lymph node metastasis. Another in vivo and in vitro study suggested that APRIL knockdown is associated with the modulation of cell proliferation, as well as the reduction of cell migration and invasion in vitro. Moreover, APRIL-knockdown cells displayed markedly inhibited tumor growth and decreased liver metastasis in the study. The study also revealed that APRIL could regulate the expression of MMPs, suggesting a link between APRIL and MMPs [32]. Overall, these studies suggest that APRIL/TNFSF13 and MMP-3 may be potential targets for the development of new therapies for CRC. However, further research is required to fully understand the roles of these markers in the development and progression of CRC.
To assess the expression of immune-related and inflammatory markers in the present study, we utilized the Bio-plex Multiplex immunoassay system. This is a highly sensitive assay that is capable of simultaneously measuring multiple analytes in a single sample, making it an ideal tool for studying complex biological systems such as the TME [33]. The multiplex immunoassay is faster than the traditional ELISA and planar microarray, but with comparable and reliable diagnostic accuracy [34,35,36]. The mulitplex immunoassay has been used in a few studies to detect tumor-specific biomarkers in malignant tumors such as melanomas, ovarian cancer, and pancreatic cancer [37,38]. Calu et al. [13] used multiplex immunoassays to identify inflammatory molecules in CRC tissues.
This study has several limitations. First, the number of patients included in this study was relatively small. Second, as this study was conducted using data from a single institution, the characteristics of various types of patients may not have been included. Third, markers other than APRIL/TNFSF13, BAFF, and MMP-3 did not yield meaningful results because they reacted below our detection level; therefore, their effects could not be studied. Given that the TME is dynamic and subject to changes over time, we utilized freshly frozen tissue samples to capture the most current state of the tumor and its surrounding environment. It is possible that certain aspects of the microenvironment may not have been fully captured because the freeze-thaw process can alter the expression of certain biomolecules. However, the use of frozen tissue samples is a widely accepted method for studying gene expression and protein levels and has yielded reliable results in various research settings [39].
4. Materials and Methods
4.1. Study Ppulation
Patients with CRC who underwent curative surgical resection between December 2014 and January 2017 were included in this study. Patients who underwent bypass surgery without curative resection for palliative purposes, patients with cancers of other organs, and patients with a previous history of CRC were excluded from the study. Tumor tissues were prospectively obtained during the index surgical procedure. Clinical, hematological, and pathological information were extracted from the patients’ medical records. Informed consent to participate in this study was obtained from all patients. The study protocol was approved by the Institutional Review Board of Wonju Severance Medical Center (CR:318334), and the study was conducted in accordance with the tenets of the Declaration of Helsinki.
4.2. Tissue Sample Preparation
Tissue samples from both tumor and non-tumor areas of the resected specimen were collected and immediately placed in an ice-cold radioimmunoprecipitation assay buffer that contained protease inhibitor cocktails (Sigma Chemical Co., St. Louis, USA). The tissue samples were homogenized at 14000 rpm for 10 min and centrifuged for 5 min. The resultant supernatant was collected and stored at −80°C until it was ready for further analysis.
4.3. Bio-plex Multiplex Immunoassay System
The concentrations of immune-related markers (APRIL/TNFSF13, BAFF, LAG-3, PD-1, PD-L1, and CTLA-4) and inflammatory markers (CHIT, MMP-3, osteocalcin, pentraxin-3, sTNF-R1, and sTNF-R2) in colon tumor and non-tumor tissues were measured using the Milliplex® map human immuno-oncology checkpoint protein magnetic bead panel 96-well plate assay (Millipore Corporation, Billerica, USA), which is a luminex-based multiplex technology. The Bio-Plex assays (Bio-Rad, Hercules, CA, USA) contained standard concentrations of each analyte, and the calculated standard curves allowed for precise definition of the concentration of the protein of interest. The assay was performed according to the manufacturer’s instructions. Lyophilized cytokine standard was resuspended in standard diluents, and serial dilution of the standard (30 µL) was performed to generate the standard curves for each protein of interest. The bead mixture was added to the standard or sample and the plate was incubated overnight (16-18 h) at 4°C. The sample was washed three times with wash buffer/well using an automatic washer for magnetic beads. The detection antibody was then added to the plate and incubated at room temperature for 1 h. Streptavidin-phycoerythrin mix was added, and the sample was incubated at room temperature for 30 min. After washing, the assay buffer was added and analyzed using the Luminex 200 Bio-Plex instrument (Bio-Rad, Hercules, CA, USA).
4.4. Surgery and Pathological Examination
Complete mesocolic excision and total mesorectal excision, which are standard surgical approaches for colon and rectal cancer, respectively, were performed. The excised tissue was immediately transported to the pathology department, where a pathologist extracted normal and tumor tissue sections. Thorough histopathological examination was conducted following standardized guidelines, and the resulting histological data were recorded.
4.5. Statistical Analyses
Categorical variables were analyzed using the chi-square test and are described as frequencies and percentages. Fisher’s exact test was performed if the frequency of the data was <5. The normality of all continuous data was tested using the Shapiro-Wilk test. Continuous variables were analyzed using Student’s t-test and are expressed as mean values and standard deviations. Non-normally distributed data were analyzed using the Mann-Whitney U test and are described as medians and interquartile ranges. DFS was defined as the period from the date of the index surgery to the date of recurrence or death. OS was defined as the period from the date of the index surgery to the date of death. Survival analysis was performed using the Kaplan-Meier curve with the log-rank test. All statistical analyses were performed using R statistical software (version 4.1.0; R Foundation for Statistical Computing, Vienna, Austria). Statistical significance was set at p <0.05.
5. Conclusions
In conclusion, this study confirmed that various immune-related and inflammatory markers, such as APRIL/TNFSF13, BAFF, and MMP-3, are overexpressed in colorectal tumor tissues and are related to the unfavorable clinicopathological features and poor prognosis of CRC. The results of this study suggest that these markers could potentially serve as diagnostic or prognostic biomarkers for CRC.
Author Contributions
Conceptualization, S.A., K.K., H.J.B. and Y.K.; Design, S.A., K.K., and Y.K.; Supervision, S.A., K.K., H.J.B., and Y.K.; Methodology, S.A., K.K., H.J.B. and Y.K.; Data collection and processing, S.A., S.K.K., C.S.K., H.Y.K., H.D., B.K., K.K., H.J.B. and Y.K.; Analysis and interpretation, S.A., S.K.K., C.S.K., H.Y.K., H.D., B.K., K.K., H.J.B. and Y.K; Writing—original draft, S.A. and Y.K.; Writing—review and editing, S.A., K.K., and Y.K. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
This study was approved by the Institutional Review Board of Wonju Severance Christian Hospital (CR: 318334).
Informed Consent Statement
Written informed consent was obtained from all participants.
Data Availability Statement
Not applicable.
Acknowledgments
Not applicable.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Sahin, I.H.; Akce, M.; Alese, O.; Shaib, W.; Lesinski, G.B.; El-Rayes, B.; Wu, C. Immune checkpoint inhibitors for the treatment of msi-h/mmr-d colorectal cancer and a perspective on resistance mechanisms. Br. J. Cancer 2019, 121, 809–818. [Google Scholar] [CrossRef] [PubMed]
- Boukouris, A.E.; Theochari, M.; Stefanou, D.; Papalambros, A.; Felekouras, E.; Gogas, H.; Ziogas, D.C. Latest evidence on immune checkpoint inhibitors in metastatic colorectal cancer: A 2022 update. Crit. Rev. Oncol. Hematol. 2022, 173, 103663. [Google Scholar] [CrossRef] [PubMed]
- Carlino, M.S.; Larkin, J.; Long, G.V. Immune checkpoint inhibitors in melanoma. Lancet 2021, 398, 1002–1014. [Google Scholar] [CrossRef] [PubMed]
- Venkatachalam, S.; McFarland, T.R.; Agarwal, N.; Swami, U. Immune checkpoint inhibitors in prostate cancer. Cancers (Basel) 2021, 13, 2187. [Google Scholar] [CrossRef]
- Paz-Ares, L.; Ciuleanu, T.E.; Cobo, M.; Schenker, M.; Zurawski, B.; Menezes, J.; Richardet, E.; Bennouna, J.; Felip, E.; Juan-Vidal, O. , et al. First-line nivolumab plus ipilimumab combined with two cycles of chemotherapy in patients with non-small-cell lung cancer (checkmate 9la): An international, randomised, open-label, phase 3 trial. Lancet Oncol. 2021, 22, 198–211. [Google Scholar] [CrossRef] [PubMed]
- Hellmann, M.D.; Rizvi, N.A.; Goldman, J.W.; Gettinger, S.N.; Borghaei, H.; Brahmer, J.R.; Ready, N.E.; Gerber, D.E.; Chow, L.Q.; Juergens, R.A. , et al. Nivolumab plus ipilimumab as first-line treatment for advanced non-small-cell lung cancer (checkmate 012): Results of an open-label, phase 1, multicohort study. Lancet Oncol. 2017, 18, 31–41. [Google Scholar] [CrossRef] [PubMed]
- Le, D.T.; Uram, J.N.; Wang, H.; Bartlett, B.R.; Kemberling, H.; Eyring, A.D.; Skora, A.D.; Luber, B.S.; Azad, N.S.; Laheru, D. , et al. Pd-1 blockade in tumors with mismatch-repair deficiency. N. Engl. J. Med. 2015, 372, 2509–2520. [Google Scholar] [CrossRef]
- Overman, M.J.; McDermott, R.; Leach, J.L.; Lonardi, S.; Lenz, H.J.; Morse, M.A.; Desai, J.; Hill, A.; Axelson, M.; Moss, R.A. , et al. Nivolumab in patients with metastatic DNA mismatch repair-deficient or microsatellite instability-high colorectal cancer (checkmate 142): An open-label, multicentre, phase 2 study. Lancet Oncol. 2017, 18, 1182–1191. [Google Scholar] [CrossRef]
- San-Roman-Gil, M.; Torres-Jimenez, J.; Pozas, J.; Esteban-Villarrubia, J.; Albarran-Fernandez, V.; Alvarez-Ballesteros, P.; Chamorro-Perez, J.; Rosero-Rodriguez, D.; Orejana-Martin, I.; Martinez-Delfrade, I.; et al. Current landscape and potential challenges of immune checkpoint inhibitors in microsatellite stable metastatic colorectal carcinoma. Cancers (Basel) 2023, 15, 863. [Google Scholar] [CrossRef]
- Gatalica, Z.; Vranic, S.; Xiu, J.; Swensen, J.; Reddy, S. High microsatellite instability (msi-h) colorectal carcinoma: A brief review of predictive biomarkers in the era of personalized medicine. Fam. Cancer 2016, 15, 405–412. [Google Scholar] [CrossRef]
- Islekel, H.; Oktay, G.; Terzi, C.; Canda, A.E.; Fuzun, M.; Kupelioglu, A. Matrix metalloproteinase-9,-3 and tissue inhibitor of matrix metalloproteinase-1 in colorectal cancer: Relationship to clinicopathological variables. Cell Biochem. Funct. 2007, 25, 433–441. [Google Scholar] [CrossRef] [PubMed]
- Roeb, E.; Arndt, M.; Jansen, B.; Schumpelick, V.; Matern, S. Simultaneous determination of matrix metalloproteinase (mmp)-7, mmp-1, -3, and -13 gene expression by multiplex pcr in colorectal carcinomas. Int. J. Colorectal Dis. 2004, 19, 518–524. [Google Scholar] [CrossRef] [PubMed]
- Calu, V.; Ionescu, A.; Stanca, L.; Geicu, O.I.; Iordache, F.; Pisoschi, A.M.; Serban, A.I.; Bilteanu, L. Key biomarkers within the colorectal cancer related inflammatory microenvironment. Sci. Rep. 2021, 11, 7940. [Google Scholar] [CrossRef] [PubMed]
- Zou, W.; Wolchok, J.D.; Chen, L. Pd-l1 (b7-h1) and pd-1 pathway blockade for cancer therapy: Mechanisms, response biomarkers, and combinations. Sci. Transl. Med. 2016, 8, 328rv324. [Google Scholar] [CrossRef]
- Gialeli, C.; Theocharis, A.D.; Karamanos, N.K. Roles of matrix metalloproteinases in cancer progression and their pharmacological targeting. FEBS J. 2011, 278, 16–27. [Google Scholar] [CrossRef]
- Yu, J.; He, Z.; He, X.; Luo, Z.; Lian, L.; Wu, B.; Lan, P.; Chen, H. Comprehensive analysis of the expression and prognosis for mmps in human colorectal cancer. Front. Oncol. 2021, 11, 771099. [Google Scholar] [CrossRef]
- Baker, E.A.; Bergin, F.G.; Leaper, D.J. Matrix metalloproteinases, their tissue inhibitors and colorectal cancer staging. Br. J. Surg. 2000, 87, 1215–1221. [Google Scholar] [CrossRef]
- Gobin, E.; Bagwell, K.; Wagner, J.; Mysona, D.; Sandirasegarane, S.; Smith, N.; Bai, S.; Sharma, A.; Schleifer, R.; She, J.X. A pan-cancer perspective of matrix metalloproteases (mmp) gene expression profile and their diagnostic/prognostic potential. BMC Cancer 2019, 19, 581. [Google Scholar] [CrossRef]
- Nowacka, K.H.; Jabłońska, E. Role of the april molecule in solid tumors. Cytokine Growth Factor Rev. 2021, 61, 38–44. [Google Scholar] [CrossRef]
- Garcia-Castro, A.; Zonca, M.; Florindo-Pinheiro, D.; Carvalho-Pinto, C.E.; Cordero, A.; Gutierrez del Fernando, B.; Garcia-Grande, A.; Manes, S.; Hahne, M.; Gonzalez-Suarez, E. , et al. April promotes breast tumor growth and metastasis and is associated with aggressive basal breast cancer. Carcinogenesis 2015, 36, 574–584. [Google Scholar] [CrossRef]
- Zhi, X.; Tao, J.; Xiang, G.; Cao, H.; Liu, Z.; Yang, K.; Lv, C.; Ni, S. April induces cisplatin resistance in gastric cancer cells via activation of the nf-kappab pathway. Cell. Physiol. Biochem. 2015, 35, 571–585. [Google Scholar] [CrossRef] [PubMed]
- Mhawech-Fauceglia, P.; Allal, A.; Odunsi, K.; Andrews, C.; Herrmann, F.R.; Huard, B. Role of the tumour necrosis family ligand april in solid tumour development: Retrospective studies in bladder, ovarian and head and neck carcinomas. Eur. J. Cancer 2008, 44, 2097–2100. [Google Scholar] [CrossRef] [PubMed]
- Bat-Erdene, U.; Quan, E.; Chan, K.; Lee, B.M.; Matook, W.; Lee, K.Y.; Rosales, J.L. Neutrophil tlr4 and pkr are targets of breast cancer cell glycosaminoglycans and effectors of glycosaminoglycan-induced april secretion. Oncogenesis 2018, 7, 45. [Google Scholar] [CrossRef] [PubMed]
- Lascano, V.; Hahne, M.; Papon, L.; Cameron, K.; Roeder, C.; Schafmayer, C.; Driessen, L.; van Eenennaam, H.; Kalthoff, H.; Medema, J.P. Circulating april levels are correlated with advanced disease and prognosis in rectal cancer patients. Oncogenesis 2015, 4, e136. [Google Scholar] [CrossRef] [PubMed]
- Wang, F.; Ding, W.; Wang, J.; Jing, R.; Wang, X.; Cong, H.; Wang, Y.; Ju, S.; Wang, H. Identification of microrna-target interaction in april-knockdown colorectal cancer cells. Cancer Gene Ther. 2011, 18, 500–509. [Google Scholar] [CrossRef]
- Ding, W.; Wang, J.; Wang, F.; Wang, G.; Wu, Q.; Ju, S.; Cong, H.; Wang, H. Serum sapril: A potential tumor-associated biomarker to colorectal cancer. Clin. Biochem. 2013, 46, 1590–1594. [Google Scholar] [CrossRef]
- Moreaux, J.; Veyrune, J.L.; De Vos, J.; Klein, B. April is overexpressed in cancer: Link with tumor progression. BMC Cancer 2009, 9, 83. [Google Scholar] [CrossRef]
- Pelekanou, V.; Notas, G.; Athanasouli, P.; Alexakis, K.; Kiagiadaki, F.; Peroulis, N.; Kalyvianaki, K.; Kampouri, E.; Polioudaki, H.; Theodoropoulos, P. , et al. Bcma (tnfrsf17) induces april and baff mediated breast cancer cell stemness. Front. Oncol. 2018, 8, 301. [Google Scholar] [CrossRef]
- Koizumi, M.; Hiasa, Y.; Kumagi, T.; Yamanishi, H.; Azemoto, N.; Kobata, T.; Matsuura, B.; Abe, M.; Onji, M. Increased b cell-activating factor promotes tumor invasion and metastasis in human pancreatic cancer. PLoS One 2013, 8, e71367. [Google Scholar] [CrossRef]
- Warakomska, M.; Tynecka, M.; Lemancewicz, D.; Grubczak, K.; Dzieciol, J.; Moniuszko, M.; Eljaszewicz, A.; Bolkun, L. The effects of baff and april signaling on non-small cell lung cancer cell proliferation and invasiveness. Oncol. Lett. 2021, 22, 728. [Google Scholar] [CrossRef]
- Wen, Y.; Zhang, X.; Li, X.; Tian, L.; Shen, S.; Ma, J.; Ai, F. Histone deacetylase (hdac) 11 inhibits matrix metalloproteinase (mmp) 3 expression to suppress colorectal cancer metastasis. J. Cancer 2022, 13, 1923–1932. [Google Scholar] [CrossRef] [PubMed]
- Wang, G.; Wang, F.; Ding, W.; Wang, J.; Jing, R.; Li, H.; Wang, X.; Wang, Y.; Ju, S.; Wang, H. April induces tumorigenesis and metastasis of colorectal cancer cells via activation of the pi3k/akt pathway. PLoS One 2013, 8, e55298. [Google Scholar] [CrossRef]
- Huang, W.; Luo, S.; Burgess, R.; Yi, Y.H.; Huang, G.F.; Huang, R.P. New insights into the tumor microenvironment utilizing protein array technology. Int. J. Mol. Sci. 2018, 19, 559. [Google Scholar] [CrossRef]
- Fu, Q.; Zhu, J.; Van Eyk, J.E. Comparison of multiplex immunoassay platforms. Clin. Chem. 2010, 56, 314–318. [Google Scholar] [CrossRef]
- Song, J.; Merbs, S.L.; Sokoll, L.J.; Chan, D.W.; Zhang, Z. A multiplex immunoassay of serum biomarkers for the detection of uveal melanoma. Clin. Proteomics 2019, 16, 10. [Google Scholar] [CrossRef] [PubMed]
- Doseeva, V.; Colpitts, T.; Gao, G.; Woodcock, J.; Knezevic, V. Performance of a multiplexed dual analyte immunoassay for the early detection of non-small cell lung cancer. J. Transl. Med. 2015, 13, 55. [Google Scholar] [CrossRef]
- Yurkovetsky, Z.; Skates, S.; Lomakin, A.; Nolen, B.; Pulsipher, T.; Modugno, F.; Marks, J.; Godwin, A.; Gorelik, E.; Jacobs, I. , et al. Development of a multimarker assay for early detection of ovarian cancer. J. Clin. Oncol. 2010, 28, 2159–2166. [Google Scholar] [CrossRef] [PubMed]
- Song, J.; Sokoll, L.J.; Pasay, J.J.; Rubin, A.L.; Li, H.; Bach, D.M.; Chan, D.W.; Zhang, Z. Identification of serum biomarker panels for the early detection of pancreatic cancer. Cancer Epidemiol. Biomarkers Prev. 2019, 28, 174–182. [Google Scholar] [CrossRef]
- Shi, L.; Tong, W.; Su, Z.; Han, T.; Han, J.; Puri, R.K.; Fang, H.; Frueh, F.W.; Goodsaid, F.M.; Guo, L. , et al. Microarray scanner calibration curves: Characteristics and implications. BMC Bioinformatics 2005, 6(Suppl 2), S11. [Google Scholar] [CrossRef]
Figure 1.
Levels of immune-related and inflammatory markers in tumor tissues. Scatter plots showing the distribution of levels of twelve markers. APRIL/TNFSF13, A proliferation-inducing ligand/ Tumor necrosis factor lsuperfamily member 13; BAFF, B lymphocyte activating factor; CHIT, Chitinase 1; MMP-3, matrix metallopeptidase 3; sTNF-R, Soluble Tumor Necrosis Factor Receptor Type; LAG-3, Lymphocyte activation gene-3; PD-1, Programmed cell death protein 1; PD-L1, Programmed death-ligand 1; CTLA-4, Cytotoxic T-Lymphocyte Associated Protein 4.
Figure 1.
Levels of immune-related and inflammatory markers in tumor tissues. Scatter plots showing the distribution of levels of twelve markers. APRIL/TNFSF13, A proliferation-inducing ligand/ Tumor necrosis factor lsuperfamily member 13; BAFF, B lymphocyte activating factor; CHIT, Chitinase 1; MMP-3, matrix metallopeptidase 3; sTNF-R, Soluble Tumor Necrosis Factor Receptor Type; LAG-3, Lymphocyte activation gene-3; PD-1, Programmed cell death protein 1; PD-L1, Programmed death-ligand 1; CTLA-4, Cytotoxic T-Lymphocyte Associated Protein 4.
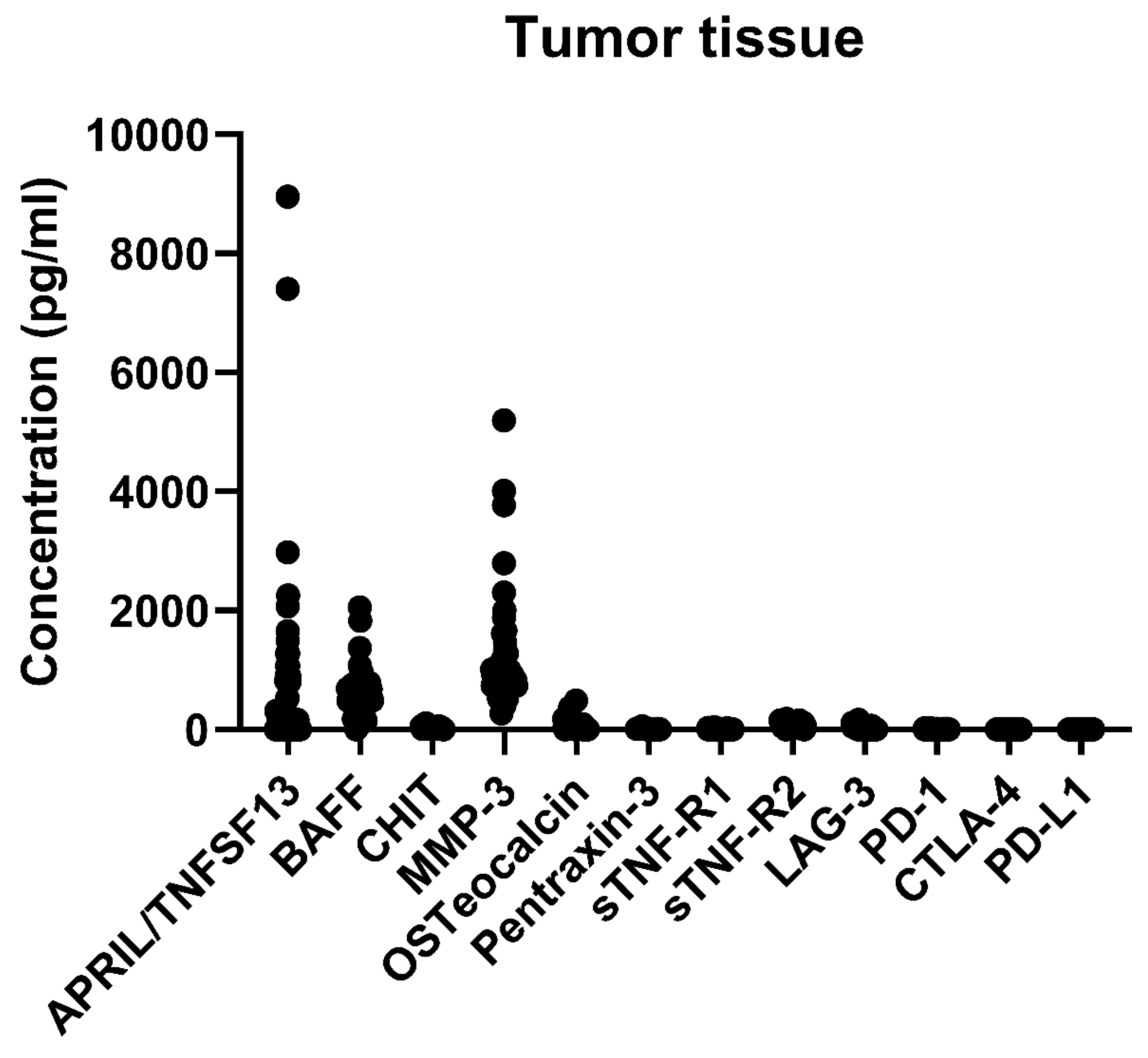
Figure 2.
Kaplan–Meier survival curves for disease-free survival (a) and overall survival (b) according to the expression level of MMP-3. MMP-3, matrix metallopeptidase 3.
Figure 2.
Kaplan–Meier survival curves for disease-free survival (a) and overall survival (b) according to the expression level of MMP-3. MMP-3, matrix metallopeptidase 3.
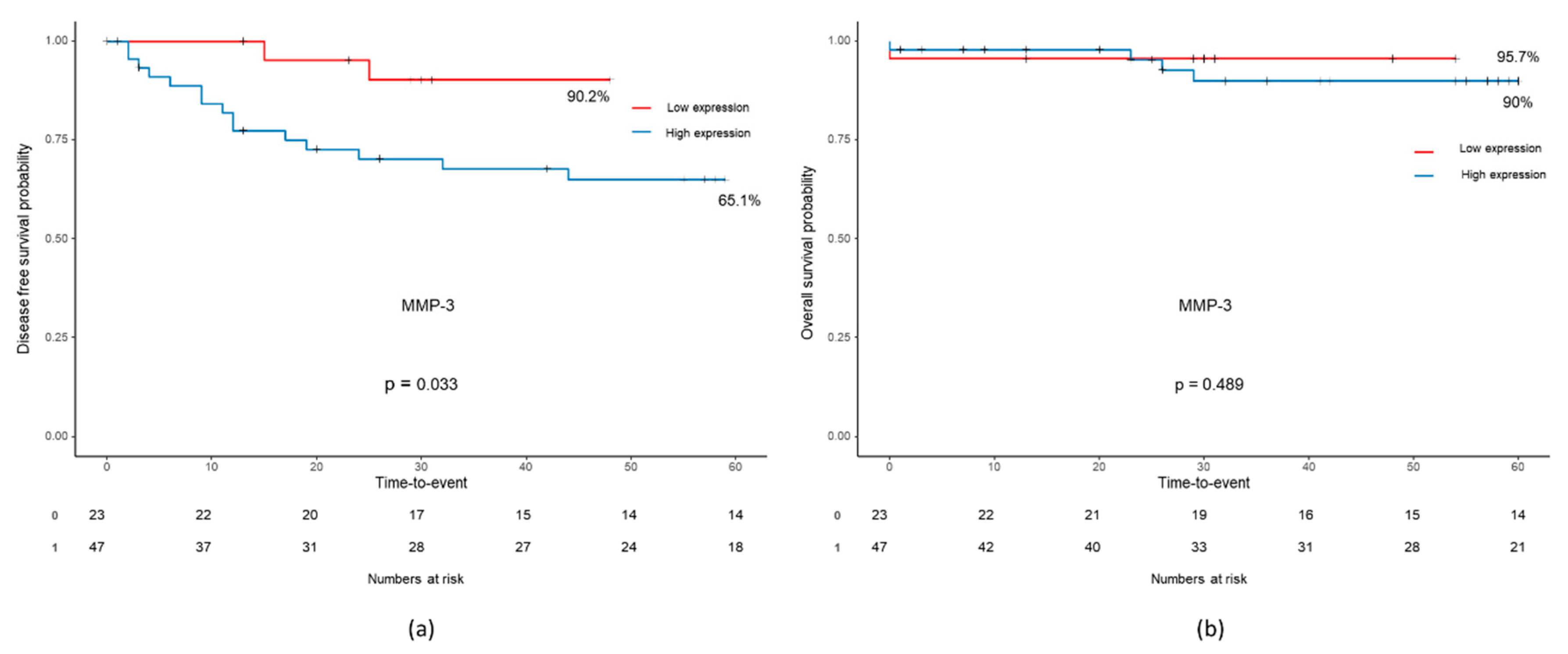

Table 1.
Baseline characteristics.
| Number of patients (%) (n=70) |
|
|---|---|
| Age, mean ± SD | 69.6 ± 10.8 |
| Gender | |
| Male | 38 (54.3) |
| Female | 32 (45.7) |
| Body mass index, mean ± SD | 23.4 ± 3.5 |
| ASA score | |
| II | 35 (50.0) |
| III | 35 (50.0) |
| Medical history | |
| None | 19 (27.1) |
| One | 18 (25.7) |
| Two or more | 33 (47.1) |
| Tumor location | |
| Right | 19 (27.1) |
| Left | 27 (38.6) |
| Rectum | 24 (34.3) |
| CEA | |
| <5 | 45 (64.3) |
| ≥5 | 25 (35.7) |
| Operation method | |
| Open | 15 (21.4) |
| MIS | 55 (78.6) |
| T stage | |
| Tis | 1 (1.4) |
| 3 | 53 (75.7) |
| 4 | 16 (22.9) |
| N stage | |
| 0 | 28 (40.0) |
| 1 | 28 (40.0) |
| 2 | 14 (20.0) |
| M stage | |
| 0 | 57 (81.4) |
| 1 | 13 (18.6) |
| TNM stage | |
| 0 | 1 (1.4) |
| 2 | 25 (35.7) |
| 3 | 31 (44.3) |
| 4 | 13 (18.6) |
| Metastatic lymph node, mean ± SD | 2.2 ± 3.6 |
| Harvested lymph node, mean ± SD | 24.8 ± 11.1 |
| Tumor differentiation | |
| Well differentiation | 13 (18.8) |
| Moderate differentiation | 53 (76.8) |
| Poorly differentiation | 1 (1.4) |
| Mucinous adenocarcinoma | 2 (2.9) |
| Tumor size (cm), mean ± SD | 5.0 ± 2.0 |
| Lymphatic invasion | |
| Negative | 38 (54.3) |
| Positive | 32 (45.7) |
| Venous invasion | |
| Negative | 63 (90.0) |
| Positive | 7 (10.0) |
| Perineural invasion | |
| Negative | 50 (71.4) |
| Positive | 20 (28.6) |
| EGFR | |
| Negative | 5 (7.6) |
| Positive | 61 (92.4) |
| MSI | |
| MSS | 63 (94.0) |
| MSI-H | 4 (6.0) |
| KRAS | |
| Wild | 39 (58.2) |
| Mutant | 28 (41.8) |
| NRAS | |
| Wild | 47 (92.2) |
| Mutant | 2 (3.9) |
| BRAF | |
| Wild | 62 (95.4) |
| Mutant | 3 (4.6) |
| Laboratory markers, mean ± SD | |
| WBC (103/μL) | 7.6 ± 3.1 |
| Hb (g/dL) | 11.9 ± 2.4 |
| PLT (103/μL) | 288.0 ± 100.3 |
| Neutrophil count (103/μL) | 5.4 ± 3.0 |
| Lymphocyte count (103/μL) | 1.5 ± 0.6 |
| NLR | 4.5 ± 4.9 |
| C-reactive protein (mg/dL) | 1.7 ± 2.7 |
| Albumin (g/dL) | 3.8 ± 0.6 |
| Chemotherapy | |
| No | 24 (34.3) |
| Yes | 46 (65.7) |
| Radiotherapy | |
| No | 69 (98.6) |
| Yes | 1 (1.4) |
| Recurrence | |
| No | 42 (60.0) |
| Yes | 17 (24.3) |
| Death | |
| No | 45 (64.3) |
| Yes | 5 (7.1) |
SD, standard deviation; ASA, American Society of Anesthesiologists; CEA, Carcinoembryonic antigen; MIS, minimally invasive surgery; EGFR, Epidermal growth factor receptor; MSI, Microsatellite instability; WBC, white blood cell; Hb, hemoglobin; PLT, platelet; NLR, neutrophil-lymphocyte ratio.
Table 2.
Immune-related and inflammatory markers in tumor tissues.
| Median [IQR] | Range | |
|---|---|---|
| APRIL/TNFSF13 | 166.02 [0, 806.4] | 0~8954.58 |
| BAFF | 485.6 [355.3, 664.0] | 0~2053.2 |
| CHIT | 21.3 [10.24, 31.24] | 0~101.19 |
| MMP-3 | 905.1 [736.2, 1106.9] | 270.5~5198.8 |
| Osteocalcin | 16.33 [2.37, 41.34] | 0~487.48 |
| Pentraxin-3 | 8.98 [7.41, 12.19] | 3.23~57.43 |
| sTNF-R1 | 6.67 [5.43, 7.87] | 2.28~36.20 |
| sTNF-R2 | 60.99 [35.78, 106.93] | 0~177.87 |
| LAG-3 | 0 [0, 11.46] | 0~164.96 |
| PD-1 | 5.3 [5.30, 10.84] | 0~21.77 |
| PD-L1 | 0 [0, 0.43] | 0~4.49 |
| CTLA-4 | 0 [0, 0] | 0~3.1 |
IQR, interquartile range; APRIL/TNFSF13, A proliferation-inducing ligand/ Tumor necrosis factor lsuperfamily member 13; BAFF, B lymphocyte activating factor; CHIT, Chitinase 1; MMP-3, matrix metallopeptidase 3; sTNF-R, Soluble Tumor Necrosis Factor Receptor Type; LAG-3, Lymphocyte activation gene-3; PD-1, Programmed cell death protein 1; PD-L1, Programmed death-ligand 1; CTLA-4, Cytotoxic T-Lymphocyte Associated Protein 4
Table 3.
Correlation of immunologic markers with clinicopathologic features.
| APRIL/TNFSF13 (806.4) | BAFF (664.0) | MMP-3 (736.2) | |||||||
|---|---|---|---|---|---|---|---|---|---|
| Low (N=51) | High (N=19) | p | Low (N=52) | High (N=18) | p | Low (N=23) | High (N=47) | p | |
| Age, mean ± SD | 69.8 ± 10.7 | 69.2 ± 11.0 | 0.82 | 69.4 ± 11.1 | 70.3 ± 10.1 | 0.74 | 70.7 ± 11.4 | 69.1 ± 10.5 | 0.59 |
| Gender | |||||||||
| Male | 27 (52.9) | 11 (57.9) | 0.92 | 25 (48.1) | 13 (72.2) | 0.13 | 15 (65.2) | 23 (48.9) | 0.30 |
| Female | 24 (47.1) | 8 (42.1) | 27 (51.9) | 5 (27.8) | 8 (34.8) | 24 (51.1) | |||
| BMI | 23.5 ± 3.7 | 23.1 ± 3.1 | 0.70 | 23.4 ± 3.7 | 23.4 ± 3.0 | 0.96 | 23.3 ± 3.6 | 23.4 ± 3.5 | 0.90 |
| ASA score | |||||||||
| II | 28 (54.9) | 7 (36.8) | 0.28 | 29 (55.8) | 6 (33.3) | 0.17 | 13 (56.5) | 22 (46.8) | 0.61 |
| III | 23 (45.1) | 12 (63.2) | 23 (44.2) | 12 (66.7) | 10 (43.5) | 25 (53.2) | |||
| Medical history | |||||||||
| None | 14 (27.5) | 5 (26.3) | 0.95* | 12 (23.1) | 7 (38.9) | 0.22* | 6 (26.1) | 13 (27.7) | 0.81 |
| One | 14 (27.5) | 4 (21.1) | 16 (30.8) | 2 (11.1) | 5 (21.7) | 13 (27.7) | |||
| T or more | 23 (45.1) | 10 (52.6) | 24 (46.2) | 9 (50.0) | 12 (52.2) | 21 (44.7) | |||
| Tumor location | |||||||||
| Right | 15 (29.4) | 4 (21.1) | 0.65 | 17 (32.7) | 2 (11.1) | 0.13* | 8 (34.8) | 11 (23.4) | 0.51 |
| Left | 20 (39.2) | 7 (36.8) | 20 (38.5) | 7 (38.9) | 7 (30.4) | 20 (42.6) | |||
| Rectum | 16 (31.4) | 8 (42.1) | 15 (28.8) | 9 (50.0) | 8 (34.8) | 16 (34.0) | |||
| CEA | |||||||||
| <5 | 34 (66.7) | 11 (57.9) | 0.68 | 34 (65.4) | 11 (61.1) | 0.96 | 19 (82.6) | 26 (55.3) | 0.04 |
| ≥5 | 17 (33.3) | 8 (42.1) | 18 (34.6) | 7 (38.9) | 4 (17.4) | 21 (44.7) | |||
| Operation method | |||||||||
| Open | 10 (19.6) | 5 (26.3) | 0.53* | 11 (21.2) | 4 (22.2) | 1* | 6 (26.1) | 9 (19.1) | 0.54* |
| MIS | 41 (80.4) | 14 (73.7) | 41 (78.8) | 14 (77.8) | 17 (73.9) | 38 (80.9) | |||
| T stage | |||||||||
| Tis | 0 (0.0) | 1 (5.3) | 0.29* | 0 (0.0) | 1 (5.6) | 0.09* | 0 (0.0) | 1 (2.1) | 0.01* |
| 3 | 40 (78.4) | 13 (68.4) | 42 (80.8) | 11 (61.1) | 22 (95.7) | 31 (66.0) | |||
| 4 | 11 (21.6) | 5 (26.3) | 10 (19.2) | 6 (33.3) | 1 (4.3) | 15 (31.9) | |||
| N stage | |||||||||
| 0 | 22 (43.1) | 6 (31.6) | 0.60* | 20 (38.5) | 8 (44.4) | 0.81* | 13 (56.5) | 15 (31.9) | 0.15* |
| 1 | 20 (39.2) | 8 (42.1) | 22 (42.3) | 6 (33.3) | 6 (26.1) | 22 (46.8) | |||
| 2 | 9 (17.6) | 5 (26.3) | 10 (19.2) | 4 (22.2) | 4 (17.4) | 10 (21.3) | |||
| M stage | |||||||||
| 0 | 45 (88.2) | 12 (63.2) | 0.03* | 45 (86.5) | 12 (66.7) | 0.08* | 21 (91.3) | 36 (76.6) | 0.19* |
| 1 | 6 (11.8) | 7 (36.8) | 7 (13.5) | 6 (33.3) | 2 (8.7) | 11 (23.4) | |||
| TNM stage | |||||||||
| 0 | 0 (0.0) | 1 (5.3) | 0.02* | 0 (0.0) | 1 (5.6) | 0.06* | 0 (0.0) | 1 (2.1) | 0.04* |
| 2 | 21 (41.2) | 4 (21.1) | 19 (36.5) | 6 (33.3) | 13 (56.5) | 12 (25.5) | |||
| 3 | 24 (47.1) | 7 (36.8) | 26 (50.0) | 5 (27.8) | 8 (34.8) | 23 (48.9) | |||
| 4 | 6 (11.8) | 7 (36.8) | 7 (13.5) | 6 (33.3) | 2 (8.7) | 11 (23.4) | |||
| Metastatic lymph node | 1.8 ± 3.3 | 3.2 ± 4.3 | 0.23 | 2.0 ± 3.3 | 2.8 ± 4.4 | 0.45 | 1.1 ± 1.7 | 2.7 ± 4.2 | 0.02 |
| Harvested lymph node | 24.4 ± 9.4 | 25.9 ± 14.9 | 0.68 | 25.3 ± 9.8 | 23.4 ± 14.4 | 0.62 | 27.1 ± 13.1 | 23.7 ± 9.9 | 0.27 |
| Tumor differentiation | |||||||||
| WD | 10 (19.6) | 3 (16.7) | 0.79* | 9 (17.3) | 4 (23.5) | 0.63* | 4 (17.4) | 9 (19.6) | 0.91* |
| MD | 39 (76.5) | 14 (77.8) | 41 (78.8) | 12 (70.6) | 19 (82.6) | 34 (73.9) | |||
| PD | 1 (2.0) | 0 (0.0) | 1 (1.9) | 0 (0.0) | 0 (0.0) | 1 (2.2) | |||
| Mucinous | 1 (2.0) | 1 (5.6) | 1 (1.9) | 1 (5.9) | 0 (0.0) | 2 (4.3) | |||
| Tumor size (cm), mean ± SD | 4.9 ± 2.2 | 5.2 ± 1.3 | 0.50 | 4.9 ± 2.2 | 5.1 ± 1.5 | 0.64 | 4.8 ± 2.0 | 5.0 ± 2.1 | 0.74 |
| Lymphatic invasion | |||||||||
| Negative | 28 (54.9) | 10 (52.6) | 1 | 28 (53.8) | 10 (55.6) | 1 | 11 (47.8) | 27 (57.4) | 0.61 |
| Positive | 23 (45.1) | 9 (47.4) | 24 (46.2) | 8 (44.4) | 12 (52.2) | 20 (42.6) | |||
| Venous invasion | |||||||||
| Negative | 47 (92.2) | 16 (84.2) | 0.37* | 47 (90.4) | 16 (88.9) | 1* | 21 (91.3) | 42 (89.4) | 1* |
| Positive | 4 (7.8) | 3 (15.8) | 5 (9.6) | 2 (11.1) | 2 (8.7) | 5 (10.6) | |||
| Perineural invasion | |||||||||
| Negative | 40 (78.4) | 10 (52.6) | 0.06 | 40 (76.9) | 10 (55.6) | 0.15 | 19 (82.6) | 31 (66.0) | 0.24 |
| Positive | 11 (21.6) | 9 (47.4) | 12 (23.1) | 8 (44.4) | 4 (17.4) | 16 (34.0) | |||
| EGFR | |||||||||
| Negative | 1 (2.1) | 4 (22.2) | 0.01* | 1 (2.0) | 4 (25.0) | 0.01* | 0 (0.0) | 5 (11.6) | 0.15* |
| Positive | 47 (97.9) | 14 (77.8) | 49 (98.0) | 12 (75.0) | 23 (100.0) | 38 (88.4) | |||
| MSI | |||||||||
| MSS | 46 (92.0) | 17 (100.0) | 0.56* | 47 (92.2) | 16 (100.0) | 0.56* | 21 (91.3) | 42 (95.5) | 0.60* |
| MSI-H | 4 (8.0) | 0 (0.0) | 4 (7.8) | 0 (0.0) | 2 (8.7) | 2 (4.5) | |||
| KRAS | |||||||||
| Wild | 27 (56.2) | 12 (63.2) | 0.80 | 29 (59.2) | 10 (55.6) | 1 | 12 (57.1) | 27 (58.7) | 1 |
| Mutant | 21 (43.8) | 7 (36.8) | 20 (40.8) | 8 (44.4) | 9 (42.9) | 19 (41.3) | |||
| NRAS | |||||||||
| Wild | 33 (97.1) | 14 (93.3) | 0.52* | 35 (97.2) | 12 (92.3) | 0.46* | 16 (100.0) | 31 (93.9) | 1* |
| Mutant | 1 (2.9) | 1 (6.7) | 1 (2.8) | 1 (7.7) | 0 (0.0) | 2 (6.1) | |||
| BRAF | |||||||||
| Wild | 45 (95.7) | 17 (94.4) | 1* | 45 (93.8) | 17 (100.0) | 0.56* | 19 (95.0) | 43 (95.6) | 1* |
| Mutant | 2 (4.3) | 1 (5.6) | 3 (6.2) | 0 (0.0) | 1 (5.0) | 2 (4.4) | |||
| Laboratory markers, median [IQR] | |||||||||
| WBC (103/μL) | 6.6 [5.4, 9.2] | 7.1 [6.5, 8.8] | 0.53 | 7.2 [5.5, 9.2] | 6.7 [5.9, 8.9] | 0.83 | 6.5 [4.9, 7.6] | 7.2 [5.9, 9.4] | 0.10 |
| Hb (g/dL) | 12.6 [10.4, 13.6] | 11.1 [9.7, 12.5] | 0.13 | 12.4 [10.2, 13.4] | 12.4 [9.8, 13.8] | 0.87 | 12.4 [10.1, 13.8] | 12.3 [10.2, 13.6] | 0.58 |
| PLT (103/μL) | 272.0 [209.5, 323.0] | 253.0 [231.0, 331.0] | 0.92 | 275.5 [212.2, 333.5] | 242.0 [224.5, 294.2] | 0.37 | 260.0 [193.0, 307.0] | 259.0 [222.5, 332.5] | 0.42 |
| Neutrophil (103/μL) | 4.7 [3.0, 6.4] | 5.1 [4.4, 7.1] | 0.17 | 4.7 [3.1, 6.9] | 4.9 [4.3, 6.8] | 0.38 | 3.6 [3.0, 5.8] | 4.9 [3.7, 7.1] | 0.08 |
| Lymphocyte (103/μL) | 1.6 [1.3, 1.9] | 1.3 [1.0, 1.8] | 0.20 | 1.5 [1.2, 1.9] | 1.3 [1.0, 1.8] | 0.49 | 1.4 [1.2, 1.7] | 1.6 [1.1, 1.9] | 0.48 |
| NLR | 2.7 [2.1, 4.2] | 4.1 [2.7, 6.0] | 0.04 | 2.7 [2.2, 4.4] | 3.9 [2.7, 5.4] | 0.15 | 2.5 [2.1, 4.1] | 3.6 [2.5, 5.2] | 0.16 |
| CRP (mg/dL) | 0.4 [0.3, 1.6] | 1.0 [0.3, 2.3] | 0.25 | 0.5 [0.3, 1.8] | 0.7 [0.3, 1.3] | 0.97 | 0.6 [0.3, 1.3] | 0.7 [0.3, 1.8] | 0.99 |
| Albumin (g/dL) | 3.9 [3.6, 4.3] | 3.7 [3.2, 4.0] | 0.07 | 3.9 [3.6, 4.2] | 3.8 [3.3, 4.2] | 0.58 | 3.8 [3.2, 4.2] | 3.9 [3.5, 4.3] | 0.31 |
| Chemotherapy | |||||||||
| No | 17 (33.3) | 7 (36.8) | 1 | 16 (30.8) | 8 (44.4) | 0.44 | 9 (39.1) | 15 (31.9) | 0.74 |
| Yes | 34 (66.7) | 12 (63.2) | 36 (69.2) | 10 (55.6) | 14 (60.9) | 32 (68.1) | |||
| Radiotherapy | |||||||||
| No | 50 (98.0) | 19 (100.0) | 1* | 51 (98.1) | 18 (100.0) | 1* | 22 (95.7) | 47 (100.0) | 0.32* |
| Yes | 1 (2.0) | 0 (0.0) | 1 (1.9) | 0 (0.0) | 1 (4.3) | 0 (0.0) | |||
| Recurrence | |||||||||
| No | 34 (66.7) | 8 (42.1) | 0.06* | 35 (67.3) | 7 (38.9) | 0.03* | 16 (69.6) | 26 (55.3) | 0.08* |
| Yes | 12 (23.5) | 5 (26.3) | 12 (23.1) | 5 (27.8) | 2 (8.7) | 15 (31.9) | |||
| Death | |||||||||
| No | 36 (70.6) | 9 (47.4) | 0.11* | 37 (71.2) | 8 (44.4) | 0.08* | 16 (69.6) | 29 (61.7) | 0.78* |
| Yes | 4 (7.8) | 1 (5.3) | 3 (5.8) | 2 (11.1) | 1 (4.3) | 4 (8.5) | |||
SD, standard deviation; ASA, American Society of Anesthesiologists; CEA, Carcinoembryonic antigen; MIS, minimally invasive surgery; EGFR, Epidermal growth factor receptor; MSI, Microsatellite instability; ; IQR, Interquartile range; WBC, white blood cell; Hb, hemoglobin; PLT, platelet; NLR, neutrophil-lymphocyte ratio.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



