Submitted:
22 June 2023
Posted:
23 June 2023
You are already at the latest version
Abstract
TBI is one of the most common causes of death and long term damage to health worldwide. The approved guidelines for patients with TBI include standards of treatment. However, there is lack of guidelines for monitoring or neuroprotective treatment. Cerebrolysin is a drug with a proven beneficial effect on treatment outcome in patients with TBI. There are also reports of the beneficial effect of Amantadine. Studies on the use of additional neuromonitoring are also published with increasing frequency. We decided to investigate how the result of treatment changed with the administration of Cerebrolysin and Amantadine and with additional neuromonitoring. In an observational study, we collected data on 56 patients. After the statistical analysis, it could be shown, that Cerebrolysin monotherapy increases Glasgow Outcome Scale (GOS) among our patients and it was found to interact significantly with Amantadine and neuromonitoring approach in the group of severe TBI. In conclusion, it is worth considering a multimodal approach to the treatment and monitoring of patients with TBI. However, more randomized studies are needed to confirm the method of monitoring or conducting neuroprotective therapy in patients with TBI.
Keywords:
TBI
; Cerebrolysin
; Amantadine
; neuromonitoring
; NIRS
; ONDS
; ICP
; SjO2
1. Introduction
TBI (Traumatic Brain Injury) is associated with one of the highest rates of death and failure in return to life in society [1]. The need for rapid medical intervention and rehabilitation in the treatment of patients with TBI is particularly emphasized in the latest reports in the medical literature [2]. One of the milestones in the treatment of TBI was the introduction of the Brain Trauma Foundation (BTF) guidelines [3]. If followed they reduce mortality rates of patients significantly [4]. However, it still remains at a high level and new consensuses are needed for further improvements like the recent report from the Seattle conference in 2020 [5]. Most algorithms concern standards of neurological, intensive and surgical treatment. However, there is no consensus regarding neuroprotective treatment and neuromonitoring.
TBI is a heterogeneous disease. The mechanism of injury, pathophysiology and location can be radically different in different cases [6]. Across the world, TBI main causes vary by population. From elderly patients after falls in Singapore to TBI-related suicides, injuries or motor collisions USA [7,8]. The approach to monitoring and treatment of patients differs around the world as well and because of this, an increasing number of publications suggest multimodal approaches to treatment and diagnosis [6,9]. The aim of this study was to test the hypothesis that Cerebrolysin in combination with Amantadine and neuromonitoring has a positive additive effect on treatment, evaluated by i.e. GOS.
Cerebrolysin is a low molecular weight neuropeptide and free amino acid solution obtained from purified porcine brain proteins. Its beneficial influence on the outcome of patients diagnosed with TBI, stroke, Alzheimer’s disease has been proven [10].
It has been shown to have neuroproptective properties both in vitro and in vivo conditions. From the molecular point of view Cerebrolysin influences glutamatergic, GABAergic, and cholinergic transmission by acting on different targets. It influences also the antiapoptotic reactions by modulating the sonic Hedgehog pathways. It modulates and directs the nervous anti-inflammatory response by mimicking the neurotrophic factors [10]. In animal studies Cerebrolysin shows its anti-inflammatory long distance influence by reducing astrogliosis and stimulating neurogenesis [11]. In TBI models results of introducing Cerebrolysin improves BBB barrier, enhances tight junction protein levels, and decreases pro inflammatory cytokines [12], demonstrated in in vitro studies as well [13].
Amantadine is another neuroprotective drug. It is a synthetic, tricyclic amine of the adamantanes. It could be administrated both: orally and intravenously. Since its origin, it had different roles in the treatment of influenza, Parkinson’s disease and off label in many others pathologies especially with movement disorders [14]. Recently it has also been researched according to few reports on its potentially beneficial role during the COVID infection [15,16]. Several trials of its use in patients with TBI diagnosis have also been published. Latest meta analysis results showed that Amantadine could be beneficial but further long term observational trials are needed [17]. Although Amantadine is used for nearly 100 years its exact mechanism of action is not clear until now. Amantadine multi directionally participates in the intensification of dopaminergic transmission. It affects the synthesis, turnover, uptake, and synaptic release in animal studies and synthesis in human studies. It plays a role in the modification of both pre- and post-synaptic transmission. Amantadine is a low-affinity, non-competitive antagonist of NMDA receptors, which makes it have a remarkable effect on glutamatergic transmission. The balance of the latter is the basis for regulating dyskinesia in the course of neurodegenerative diseases. The effects on Acetylcholine, Serotonin, Norepinephrine and phosphodiesterase activity, which are involved in modulating inflammation, remain unclear [15,18].
The golden standard of neuromonitoring is apart from clinical neurological examination the intracranial pressure (ICP) measurement. According to the BTF and Seattle Guidelines is it advised to target the treatment for a specific ICP value, cerebral perfusion pressure (CPP) [3,5]. Without these measurements clinicians can only observe mean arterial pressure (MAP). In recent years more research concerning other kinds of monitoring, especially non invasive methods, were published but most of them are not included in official guidelines. The reason to that is a lack of randomized studies using non-invasive techniques. The trends of non-invasive monitoring results can tell more about the patients condition and often correspond to an increase in ICP [19].
Near-infrared spectroscopy (NIRS) is a bedside, non invasive technique. Two electrodes are simply placed on the patients forehead and give the information about regional oxygenation of brain tissue. NIRS is using Beer-Lambert law, according to which absorption is directly proportional to concentration of absorbing material. In this case it detects the wavelengths from 700 to 1000 nm. The differences between detection of oxygenated and deoxygenated hemoglobin is most likely to detect in this wavelength. The regional oxygen saturation is reflected by the differences in light absorption and reflection. It is a very sensitive tool for which the levels of 60-75% seem to be correct and the deviations need further medical assessment and actions [19,20]. NIRS parameters could predict ischemia and with MAP and ICP could give information about the auto regulation of the brain circulation [19]. The SafeBoosC II randomized trial with 166 newborns proved that changes in NIRS followed by changes in treatment drove to stabilization of the brain damage markers levels in the blood. This makes the technique worth considering for neuromonitoring [21]. Using NIRS does not require additional training. Putting electrodes on patients forehead and managing the monitor is quite intuitive. The method however need additional expense in the form of electrodes.
Optic Nerve Sheath Diameter (ONSD) is another bedside non invasive technique. It is save and requires only basic ultrasound equipment and trained personnel. It does not require additional costs. It also corresponds with elevated ICP and can predict its elevation [22]. The greatest correspondence with elevated ICP confirmed by Computed Tomography (CT) scans are the values of ONSD higher than 0,58 cm [22,23].
Electroencephalography (EEG) is especially important in patients with TBI. Tissue destruction and extravasated blood can be epileptogenic. In the terms of constant intensive care and patient sedation the cases of non convulsive status epilepticus could remain undiagnosed. The misdiagnosed cases could be even up to 15% of all patients [19]. That is why it is so important to repeatedly examine the patient every day, but also to monitor them, preferably continuously with the use of EEG. The method is simply, bedside but it requires additional electrodes, that are places on the forehead so is associated with additional costs. Each seizure is a nerve cell-destroying attack. Therefore, early diagnosis of epilepsy and anti epileptic treatment introduction helps to improve the prognosis of patients with seizure. EEG is recommended by the Seattle consesnsus [5].
Concerning the invasive methods : the Jugular Venous Oxygen Saturation (Sjv02) is one of the bedside attached solutions. Measuring the saturation of blood collected from jugular bulb gives us information about delivery and extraction of oxygen in the brain tissues. The saturation gives information about the global oxygenation of the brain. A catheter is placed in jugular vein in the same technique as in placing it normally for central venous pressure (CVP) measurement but in the opposite direction. In most of cases an X ray is done to confirm that the tip of catheter is in the bulb directly. Blood samples for the laboratory analysis could be taken as often as they are needed. The common complications that could occur are heamatomas, artery puncture, pneumothorax, thrombosis, infection. The values between below 50% indicates ischemia and more than 75% hyperemia. Inadequate results can be obtained by too fast drawing of a blood sample, so it is very important to have a trained personnel. This method is mentioned in the Brain Trauma Guidelines [19].
The golden standard for neuromonitoring of patients after TBI is the ICP direct measurement. It is mentioned both in Brain Trauma Foundation guidelines but also in Seattle Consensus where we are provided with algorithm including special treatment tiers and targets [2,5]. This is an invasive method and the catheter is placed in the brain parenchyma or in lateral ventricles. In latest reports the ventricle catheters are associated with a higher rate of infection, however, the mortality rate of patients and the general outcome remain the same as in parenchymal patients [24 volvovic]. Based on the measurements and ICP values, we can determine the CPP, which should be above 60mmHg [5]. The method is invasive and the most common complications are bleeding, infection, and incorrect placement of the catheter, which causes misreadings [24].
In the literature so far there are no references concerning observational studies examining the influence of Cerebrolysin, additional neuroprotective treatment and neuromonitoring. It therefore seemed reasonable to investigate this correlation in presented research.
2. Materials and Methods
2.1. Design of the Study and Participants
The study was conducted with patients diagnosed with TBI and admitted do University Hospital no.1 in Szczecin, Poland.
The inclusion criteria were:
- -
- age >18 years old
- -
- TBI diagnosis
- -
- Admission to ICU
The exclusion criteria were:
- -
- age <18 years
- -
- history of allergy to Cerebrolysin
- -
- acute renal failure
- -
- pregnancy
- -
- multi organ trauma
- -
- death within 48 hours after admission.
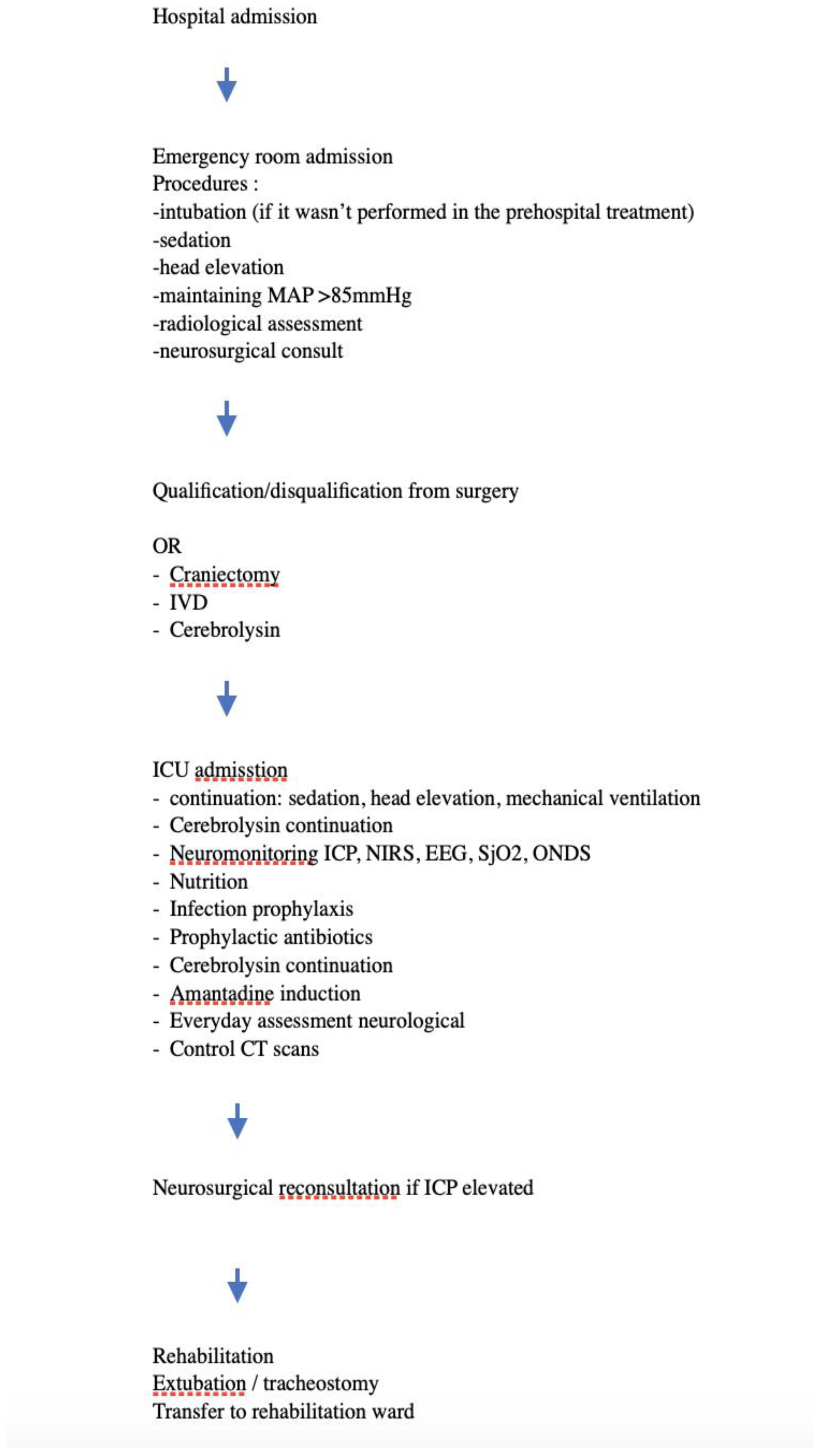
The patients were admitted to hospital, then assessed at the emergency room and after the radiological evaluation qualified or disqualified from immediate neurosurgery procedure. The next step was admission to ICU and following the basic guidelines for TBI within the ICU. Some of the patients received Cerebrolysin in the dosage 30ml - 50ml as soon as possible - the latest within 24 hours after the injury. During the patients stay in the ICU Cerebrolysin was continued. Also additional neuromonitoring was applied in the form of : ICP, NIRS, EEG, SjO2 or ONDS. After further hospitalization if the patients status was improving, they have been extubated and transferred to rehabilitation wards to continue the treatment route.
The Flowchart below on Figure 1 illustrates the patients pathway during the hospitalization.
Figure 1.
Flowchart of patients inclusion.
2.2. Clinical Management
After the admission to ICU the patients were treated with general ICU rules. The patients were assessed with Glasgow Coma Scale (GCS) initially. We used the GCS as descried in 1974 by Teasdale & Jennet [25]. Additionally patients with severe TBI (GCS <8) were included in severe-TBI subgroup and patients with mild and moderate TBI (GCS >8) were included in non-severe TBI subgroup.
The patients were sedated in most cases with propofol and fentanyl in continuous infusion. Routinely, several times a day a neurological assessment was performed in order to assess if the neurological reflexes are stable. Additional neuromonitoring was applied in the form of : ICP, NIRS, EEG, SjO2 or ONDS. Invasive osmotic therapy was performed under the control of osmolarity either calculated or assessed through laboratory tests. The patients were ventilated invasively with the intubating tube initially applying to the rules of protective lung ventilation. The Positive End Expiratory Pressure (PEEP) didn’t exceed 8 mmHg in all cases. After several failures to extubate the patients with preserved consciousness, a tracheostomy was performed, ditto in patients with consciousness disturbances.
During the first period of acute post trauma phase the MAP in patients without ICP monitoring, was kept above 85mmHg. To keep it within the range the amino catecholamines : norepinephrine and, or vasopressin analogues were used. The patient monitored with ICP were treated according to CPP targeting. In these cases the threshold of 60mmHg was kept
Nutrition was introduced on the next day after admission through nasogastric tube. Patients in vegetative state at the end of the treatment or with swallowing disturbances had a percutaneous gastrostomy was performed via a minimally invasive endoscopic approach.
2.3. Outcomes
For the primary outcome the GOS (Glasgow Outcome Scale) was used [26]. The secondary ones were length of stay (LOS) and mortality.
2.4. Statistical Analysis
The statistical analyses were performed with the use of Med Calc statistical software version 20.210 (Ostend, Belgium). Two-sided p < 0.05 indicated a statistically significant difference. Continuous variables conforming to normal distribution were expressed as mean ± standard deviation (SD). Continuous variables that were not normally distributed were defined as median and interquartile range [IQR)]. Nonparametric tests, Mann-Whitney or Kruskall-Wallis, as appropriate, compared differences between groups. Categorical data were expressed as numbers (percentages) and compared using chi-square or Fisher’s exact test. At the same time, the Bonferroni correction was used for correction. Because of relatively unequal sample sizes after the division according to severity of TBI (mild, moderate, severe) subgroups were grouped into : severe and non-severe patients. To find the interaction between Cerebrolysin treatment and other intervention with well-established efficacy, two-way Anova was used. I this case, the Levene’s test was used for conforming the equality of variances.
2.5. Ethical statement:
The research was carried out on the basis of the decision number : KB-0012/88/16, established by Pomeranian Medical University Bioethical Committee.
2.6. Clinical trials registry number: NCT05807503
3. Results
3.1. Patient characteristics:
Finally, we included data of 56 patients (19 females; 34.5%) allocated to Cerebrolysin (n=25) or no-Cerebrolysin (n=31) group. Concerning the GCS variable: mild TBI (GCS 13-15) was diagnosed in 6 patients (10,9%), moderate (GCS 9-12 ) in 8 patients (14,5%) and severe TBI was diagnosed in 41 patients (74,5%). The mean age in these groups were severe: 59.39±17.08 and not severe: 58.5±17.09 (p=0.749). There were no differences in regards to gender (p=0.59).
The severity of TBI was at admission in 10% mild, 14% moderate and 74% severe according do GCS. To make the statistical analysis more accurate we divided the patients into 2 groups : severe 74% and non-severe (moderate and mild pooled) 25% as listed in the Table 1 and Table 2 below.

Table 1.
GCS according to division on mild, moderate and severe.
| GCS | GCS | % |
|---|---|---|
| Mild | 6 | 10,90% |
| Moderate | 8 | 14,50% |
| Severe | 42 | 74,50% |
Table 2.
GCS according to division on severe- non severe.
| GCS | Severe/ not severe | ||
|---|---|---|---|
| <8 | Severe | 41 | 74,5 |
| >8 | Not severe | 14 | 25,5 |
3.2. Patients treatment efficacy.
Amantadine was administered in 10 patients (17,9%) .Neurosurgical craniotomy was performed in 53 patients (94,6%).
The patients were monitored additionally with the use of ICP catheter (2; 3,6%), NIRS (7;12,5%), NIRS, ONDS, SJO2 (1;1,8%), ONDS 2 (n; 3,6%), SJ02 (3; 5,4%), SJ02, ONDE (1; 1,8%), Sjo2, NIRS (1; 1,8%). Additional monitoring was overall used in 18 patients (32,1%). These characteristics in regards to GCS groups are presented in Table 3. There were no significant differences between tested variables.
Table 3.
Treatment in TBI patients.
| Amantadine | |||
| GCS_qualitatively | NO | YES | p |
| not severe | 11 | 3 | 0.55 |
| severe | 35 | 6 | |
| Cerebrolysin | |||
| GCS_qualitatively | NO | YES | p |
| not severe | 9 | 5 | 0.49 |
| severe | 22 | 19 | |
| Cerebrolysin | |||
| GCS_qualitatively | NO | YES | p |
| not severe | 0 | 14 | 0.40 |
| severe | 2 | 39 | |
| Monitoring | |||
| GCS_qualitatively | NO | YES | p |
| not severe | 10 | 4 | 0.82 |
| severe | 28 | 13 | |
3.3. Data analysis
The mean GOS score for all patients severe and non-severe was 2.48±0.95 whilst LOS 15.02±16.52.
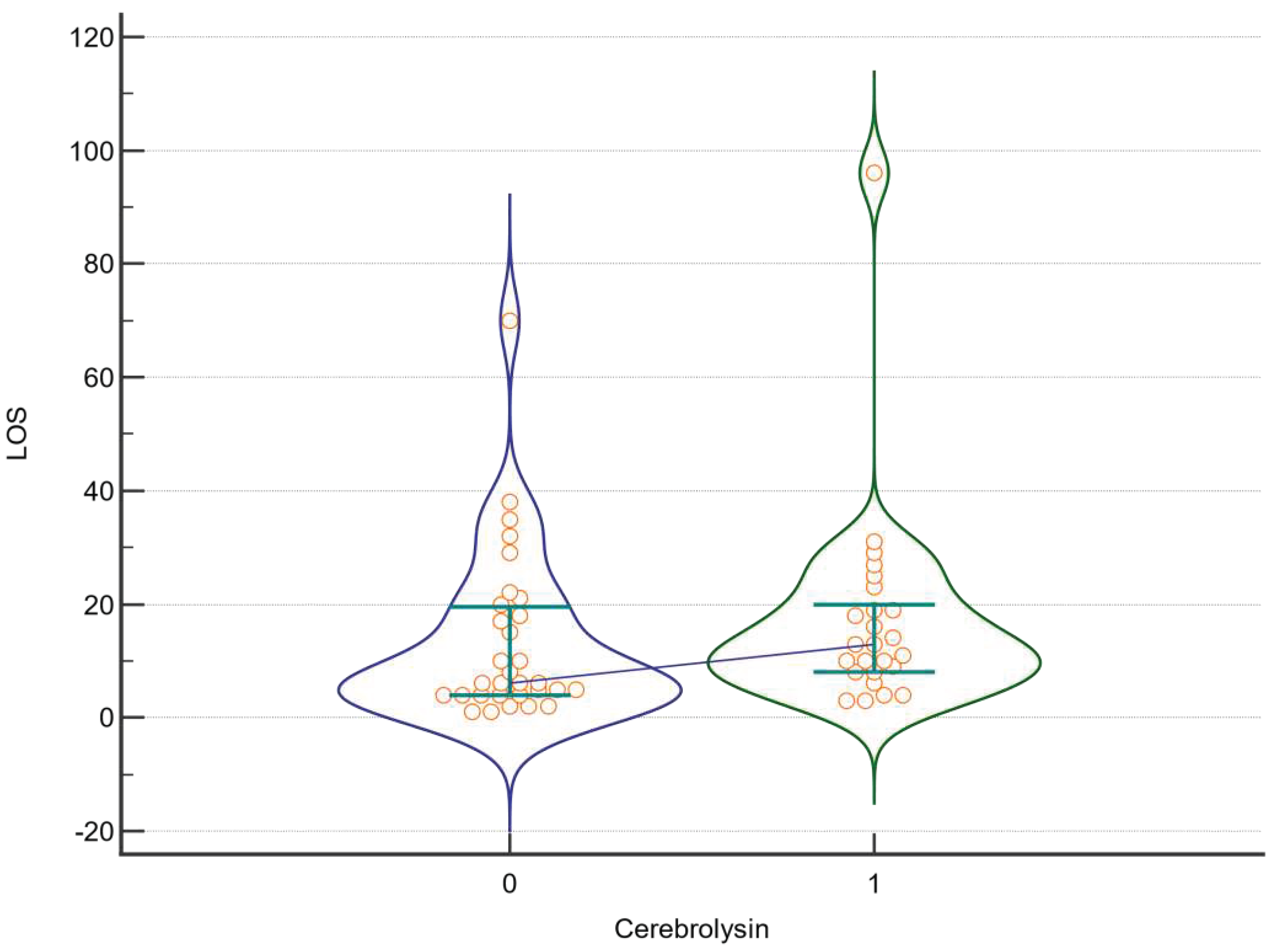
In the first set of analyses we assessed whether Cerebrolysin affected the raw value of GOS in all patients without dividing them into severe and non-severe group. We found no significant results (p=0.197). Similar results were obtained for LOS (p=0.11; Figure 2 and Figure 3).
Figure 2.
GOS in regards to Cerebrolysin treatment. A violin plot depicting medians and IQR. Orange circles represent individual cases. Blue horizontal line connects medians.
Figure 2.
GOS in regards to Cerebrolysin treatment. A violin plot depicting medians and IQR. Orange circles represent individual cases. Blue horizontal line connects medians.
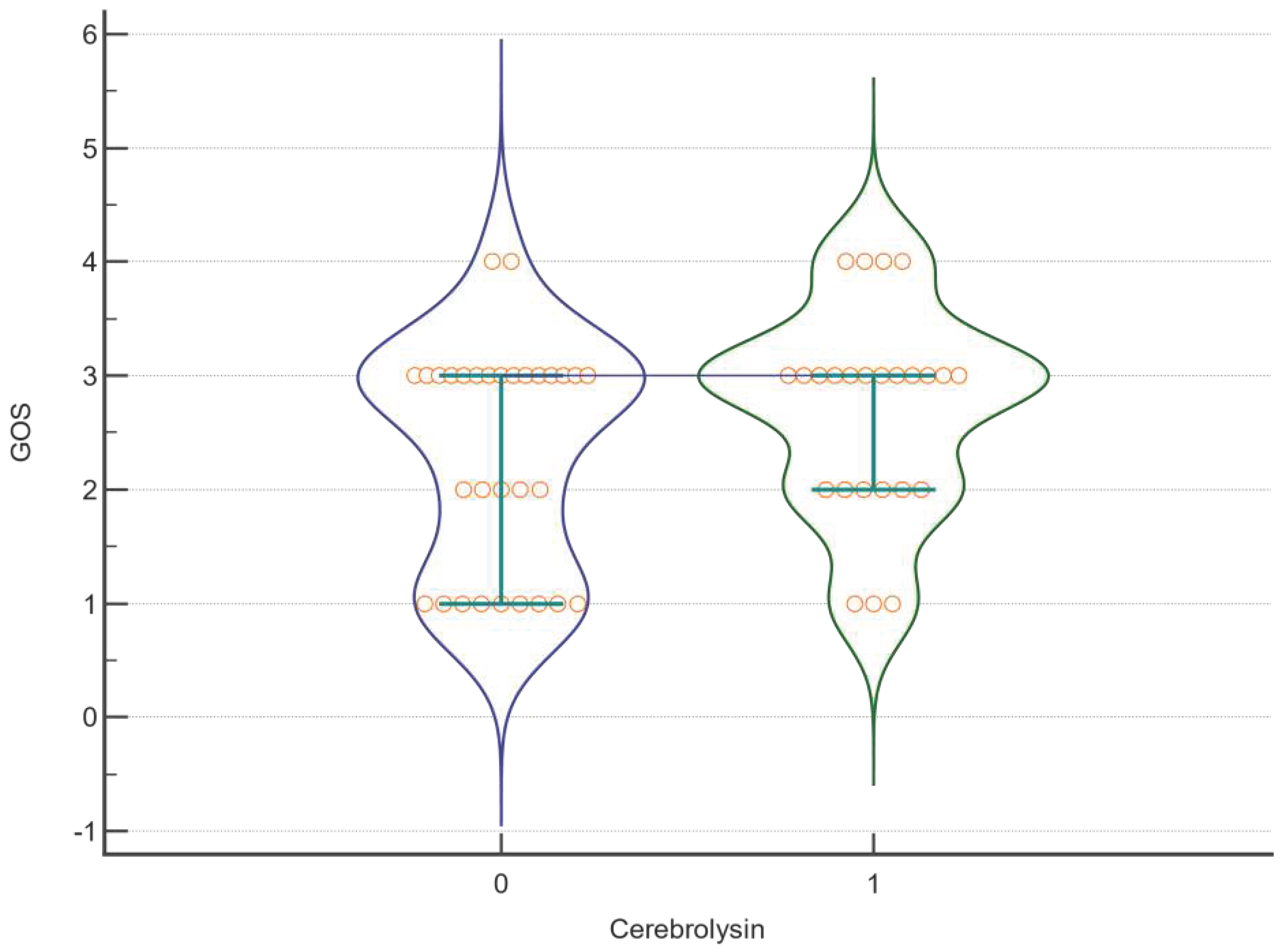
Figure 3.
LOS in regards to Cerebrolysin treatment. A violin plot depicting medians and IQRs. Orange circles represent individual cases. Blue horizontal line connects medians.
Figure 3.
LOS in regards to Cerebrolysin treatment. A violin plot depicting medians and IQRs. Orange circles represent individual cases. Blue horizontal line connects medians.
Despite the fact that there were no significant differences in regards to GCS scores expressed qualitatively between the intervention and control group (p=0.4928), we aimed to assess whether this parameter would affect the Cerebrolysin mode of action in severe and non-severe patients separately. Also, as other interventions (e.g. Amantadine, craniectomy, neuromonitoring) might affect the efficacy of Cerebrolysin, we adopted two-way Anova with primary outcomes (LOS, GOS) for these two subgroups (severe and non-severe) in regard to GCS scale and Cerebrolysin treatment. Results are shown in Table 4.
Table 4.
The efficacy of Cerebrolysin along with Amantadine, craniectomy and neuromonitoring on LOS and GOS in regard to severe patients.
Table 4.
The efficacy of Cerebrolysin along with Amantadine, craniectomy and neuromonitoring on LOS and GOS in regard to severe patients.
| Factor | DF | F | P |
|---|---|---|---|
| GOS | |||
| Cerebrolysin | 1 | 0,795 | <0,001 |
| Amantadine | 1 | 0,000945 | <0,001 |
| Cerebrolysin *Amantadine | 1 | 0,341 | <0,001 |
| Cerebrolysin | 1 | 0,0391 | <0,001 |
| Craniectomy | 1 | 0,722 | <0,001 |
| Cerebrolysin *Craniectomy | 1 | 0,0391 | <0,001 |
| Cerebrolysin | 1 | 0,745 | <0,001 |
| Monitoring | 1 | 0,3 | <0,001 |
| Cerebrolysin *Monitoring | 1 | 2,048 | <0,001 |
| LOS | |||
| Cerebrolysin | 1 | 0,657 | 0,421 |
| Amantadine | 1 | 0,074 | 0,787 |
| Cerebrolysin *Amantadine | 1 | 0,105 | 0,748 |
| Cerebrolysin | 1 | 0,00753 | 0,931 |
| Craniectomy | 1 | 0,176 | 0,677 |
| Cerebrolysin *Craniectomy | 1 | 0,555 | 0,46 |
| Cerebrolysin | 1 | 0,0523 | 0,82 |
| Monitoring | 1 | 0,147 | 0,703 |
| Cerebrolysin *Monitoring | 1 | 0,345 | 0,56 |
DF - degrees of freedom.
We were able to show that in severe group Cerebrolysin affected the GOS results positively and this parameter was found to significantly interact with the administration of Amantadine, craniectomy and neuromonitoring - see Table 7 below. Such associations were not confirmed in regard to LOS.
In non-severe patients, Cerebrolysin affected the GOS positively as well, as evidenced in two-way Anova approach (Table 5). However it didn’t interact with additional Amantadine and neuromonitoring as in group of severe-TBI.
Table 5.
The efficacy of Cerebrolysin along with Amantadine, craniectomy and neuromonitoring on LOS and GOS in regard to non severe patients.
Table 5.
The efficacy of Cerebrolysin along with Amantadine, craniectomy and neuromonitoring on LOS and GOS in regard to non severe patients.
| Factor | DF | F | P |
|---|---|---|---|
| GOS | |||
| Cerebrolysin | Not estimable | ||
| Amantadine | |||
| Cerebrolysin *Amantadine | |||
| Cerebrolysin | |||
| Craniectomy | |||
| Cerebrolysin *Craniectomy | |||
| Cerebrolysin | 1 | 5,908 | 0,035 |
| Monitoring | 1 | 4,73 | 0,055 |
| Cerebrolysin *Monitoring | 1 | 0,0164 | 0,901 |
| LOS | |||
| Cerebrolysin | Not estimable | ||
| Amantadine | |||
| Cerebrolysin *Amantadine | |||
| Cerebrolysin | |||
| Craniectomy | |||
| Cerebrolysin *Craniectomy | |||
| Cerebrolysin | 1 | 2,793 | 0,126 |
| Monitoring | 1 | 2,65 | 0,135 |
| Cerebrolysin *Monitoring | 1 | 0,0796 | 0,784 |
At last, we found that Cerebrolysin did not affect the mortality in either severe or not severe patients. See Table 6 below.
Table 6.
Cerebrolysin and other interventions efficacy in severe and not severe TBI patients.
| Variable | Whole group | Severe | Not severe | ||||||
|---|---|---|---|---|---|---|---|---|---|
| Cerebrolysin | NO | YES | p | NO | YES | p | NO | YES | p |
| ALIVE | 22 | 22 | 0.12 | 16 | 16 | 0.38 | 6 | 5 | 0.16 |
| DEAD | 9 | 3 | 6 | 3 | 3 | 0 | |||
| Amantadine | NO | YES | p | NO | YES | p | NO | YES | p |
| ALIVE | 35 | 9 | 0.33 | 27 | 5 | 0.73 | 8 | 3 | 0.32 |
| DEAD | 11 | 1 | 8 | 1 | 3 | 0 | |||
| Craniectomy | NO | YES | p | NO | YES | p | NO | YES | p |
| ALIVE | 3 | 41 | 0.36 | 2 | 30 | 0.44 | 0 | 11 | n.e. |
| DEAD | 0 | 12 | 0 | 9 | 0 | 3 | |||
| Neuromonitoring | NO | YES | p | NO | YES | p | NO | YES | p |
| ALIVE | 29 | 15 | 0.55 | 21 | 11 | 0.49 | 8 | 3 | 0.84 |
| DEAD | 9 | 3 | 7 | 2 | 2 | 1 | |||
4. Discussion
Achieving a good treatment result for TBI patients depends on many factors. Every part of medical treatment, starting from the injury onset, through quick pre-medical assistance, quick and accurate decisions regarding treatment and diagnosis at hospital, to rehabilitation seems to be essential. Each element of this chain of medical treatment is extremely important and can influence the success of the final outcome. In the literature reports on multimodal treatment methods of TBI patients can be found [20,27]and can affect many aspects of therapy and diagnosis [27]. Previous treatment standards utilizing isolated treatments are increasingly replaced by multimodal approaches [19].
In the context of neuroprotective treatment, there is no golden standard yet published in the available literature. Cerebrolysin is a drug with a proven positive effect on the treatment outcome (GOS, mRankin scale) in patients with TBI. The Captain II and CAPTAIN Meta-analysis studies confirmed a positive impact of Cerebrolysin on global outcome, cognition, attention and depression symptoms [28,29]. In our study we found that Cerebrolysin has a positive influence on GOS and this effect interacts positively with additional neuroprotective treatment (Amantadine) and neuromonitoring.
There is also evidence pointing the mode of action of the drug in regards to improved outcome. It turned out that. at the cellular level, Cerebrolysin increases the number of neuroblasts and led to the promotion of neurogenesis in the dentate gyrus and also a reduced astrogliosis in the corpus callosum, cortex, dentate gyrus, CA1 and CA3 Regions [12]. In updated guidelines, Cerebrolysin has been recommended for use in early motor rehabilitation after acute ischemic stroke by the European Academy of Neurology and European Federation of Neurorehabilitation Societies [30]. Recently it is also elaborated in Evidence-Based Review concerning research data up to 2020 as an agent that could be used to achieve better cognition effects after ABI [31]
In our study we found that Cerebrolysin interacts with Amantadine to work efficiently in severe TBI patients. Indeed, Amantadine is an antagonist for NMDA receptor and agonist for dopamine receptor acting for dopamine releasing and re- uptaking. It has a positive effect on cognition in patients with TBI in the intermediate-term [18]. We can also find the first reports of a positive additive effect of Amantadine and Cerebrolysin used together in patients with acquired brain injury [32]. The synergic effect of two different pharmacological agents could be explained by working with different receptors target. Cerebrolysin acts more like neurotrophic agent by mimicking the NTF and Amantadine influences the NMDA and dopamine pathways. Those two different activities are involved in TBI pathology in early and late states of reconvalensce. Cerebrolysin and Amantadine have proven positive influence on TBI cognitive outcome also in the post acute phase of the trauma [33,34]. Lee et al reported the retrospective case-control study describing 84 patients with TBI treated in 2 groups: Amantadine only and Cerebrolysin plus Amantadine. After 4 weeks of follow up the group with combined treatment presented greater increase in Coma Recovery Scale-Revised (CRS-R) assessment [32].
The golden standard for monitoring patients with TBI today is ICP measurement. SjO2 is also mentioned in the guidelines of BTF [3,5]. However, due to the invasiveness of these procedures and possible complications, more attention is given to non-invasive methods. According to the current state of multimodal consensus - non-invasive methods are not included as the golden standard of TBI treatment. However, they may correspond to elevated ICP and some of these methods anticipate the deterioration of the clinical condition of patients. It is worth using several of these methods in order to observe the trends of a given patient more closely [35].
TBI is a heterogeneous condition. From the moment of injury to the patient’s convalescence, each element of treatment has a significant impact on the final effect. Both mistakes and proper decisions at every stage can determine the success or failure of therapy. In pre-hospital care, the most important are quick decisions, airway protection and proper ventilation, avoiding hypotension and the basics of anti-edematous treatment. In hospital care, the most important from the very beginning are quick radiological diagnoses and decisions concerning possible surgical interventions. During the treatment in intensive care units, the basics of treatment: sedation, ventilation, maintaining proper parameters of the circulatory system are decisive for the patient’s survival. The multimodal approach to patient treatment includes not only the basics, but also an attempt to extend to all the accessible methods [36]. Concerning monitoring it could be an attempt to evaluate several parameters and trends to guide a more personalized therapy. In multimodal treatment, it is worth mentioning pharmacotherapy with different target points. And no less of important the intensive rehabilitation in the period after secondary injury. By using as many methods as possible to improve the patients care, it may be possible to affect as many treatment targets as possible. Multimodal approach could help to achieve a better effect not only in terms of mortality but also in terms of cognitive outcome [37].
In our research, we confirmed the positive effect of Cerebrolysin used alone on the treatment outcome GOS of severe and non-severe TBI patients. We also confirmed additive effects of Amantadine and Cerebrolysin on GOS in the group of severe-TBI. We found the additive correlation between Cerebrolysin and additional neuromonitoring - invasive or non-invasive on GOS in severe TBI patients. Because of the observational character of our study there is a great need for further research in this matter with prospective trials. It seems reasonable to use Cerebrolysin in patients with TBI and attempt to combine it with a multimodal approach in monitoring, diagnosing and treating patients.
5. Conclusions
Cerebrolysin positively affected GOS in severe and non-severe TBI patients. The efficacy of Cerebrolysin interacted positively with other interventions : Amantadine, neuromonitoring in severe TBI patients. This topic requires more data and further research especially regarding randomized prospective trials with more participants involved.
Author Contributions
Conceptualization, K.J. and K.K.; methodology, K.J.; software, A.A..; validation, J.S-P., A.J.; formal analysis, K.K.; investigation, A.A.; resources, K.J.; data curation, K.K.; writing—original draft preparation, K.K.; writing—review and editing, K.J.; visualization, K.J.; supervision, A.J.; project administration, J.S-P.; funding acquisition, A.J.. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki, and approved by the Pomeranian Medical University Bioetical Committee - No. KB-0012/88/16.
Informed Consent Statement
Written informed consent has been obtained from the patients to publish this paper.
Data Availability Statement
all the data are to be shared after directly contacting with corresponding author.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Badhiwala, J.H.; Wilson, J.R.; Fehlings, M.G. Global burden of traumatic brain and spinal cord injury. Lancet Neurol. 2019, 1, 24–25. [Google Scholar] [CrossRef]
- Ng, S.Y.’ Lee, A.Y.W. Traumatic Brain Injuries: Pathophysiology and Potential Therapeutic Targets. Front Cell Neurosci. 2019, 13, 528. [CrossRef]
- Carney, N.; Totten, A.M.; O’Reilly, C.; Ullman, J.S.; Hawryluk, G.W.; Bell, M.J.; Bratton, S.L.; Chesnut, R.; Harris, O.A.; Kissoon, N.; Rubiano, A.M.; Shutter, L.; Tasker, R.C.; Vavilala, M.S.; Wilberger, J.; Wright, D.W.; Ghajar, J. Guidelines for the Management of Severe Traumatic Brain Injury, Fourth Edition. Neurosurg. 2017, 1, 6–15. [Google Scholar] [CrossRef] [PubMed]
- Gerber, L. M.; Chiu, Y.; , et al. Marked reduction in mortality in patients with severe traumatic brain injury. J. Neurosurg 2013, 119, 1583–1590. [CrossRef]
- Hawryluk, G.W.J.; Aguilera, S.; et al. A management algorithm for patients with intracranial pressure monitoring: the Seattle International Severe Traumatic Brain Injury Consensus Conference (SIBICC). Intensive Care Med 2019, 45, 1783–1794. [Google Scholar] [CrossRef] [PubMed]
- Brazinova, A.; Rehorcikova, V.; et al. Epidemiology of Traumatic Brain Injury in Europe: A Living Systematic Review. J. Neurotrauma 2021, 38, 1411–1440. [Google Scholar] [CrossRef]
- Lui, S.K.; Fook-Chong, S.; Teo, Q.Q. Demographics of traumatic brain injury and outcomes of continuous chain of early rehabilitation in Singapore. Proc. Singapore Healthc. 2020, 29, 33–41. [Google Scholar] [CrossRef]
- Daugherty, J.; Waltzman, D.; Sarmiento, K.; Xu, L. Traumatic Brain Injury-Related Deaths by Race/Ethnicity, Sex, Intent, and Mechanism of Injury - United States. Morb Mortal Wkly Rep. 2019, 22, 1050–1056. [Google Scholar] [CrossRef]
- Feng, J.; van Veen, E.; et al. Comparison of care system and treatment approaches for patients with traumatic brain injury in China versus Europe: a CENTER-TBI survey study. Journal of neurotrauma 2020, 37, 1806–1817. [Google Scholar] [CrossRef]
- Fiani, B.; Covarrubias, C.; Wong, A.; et al. Cerebrolysin for stroke, neurodegeneration, and traumatic brain injury: review of the literature and outcomes. Neurol Sci 2021, 42, 1345–1353. [Google Scholar] [CrossRef]
- Zhang, Y.M.S.; Chopp, M.; Zheng, G.Z.; Zhang, Y.; Zhang, L.; Lu, M.; Zhang, T.M.S.; Winter, S.; Doppler, E.; Brandstaetter, H.; Mahmood, A.; Xiong, Y. Cerebrolysin Reduces Astrogliosis and Axonal Injury and Enhances Neurogenesis in Rats After Closed Head Injury. Neurorehabilitation and Neural Repair 2019, 33, 15–26. [Google Scholar] [CrossRef]
- Lu, W.; Zhu, Z.; Shi, D.; Li, X.; Luo, J.; Liao, X. Cerebrolysin alleviates early brain injury after traumatic brain injury by inhibiting neuroinflammation and apoptosis via TLR signaling pathway. Acta Cir. Bras. 2022, 37. [Google Scholar] [CrossRef] [PubMed]
- Teng, H.; Li, C.; Zhang, Y.; Lu, M.; Chopp, M.; Zhang, Z.G.; Melcher-Mourgas, M.; Fleckenstein, B. Therapeutic effect of Cerebrolysin on reducing impaired cerebral endothelial cell permeability. Neuroreport. 2021, 32, 359–366. [Google Scholar] [CrossRef]
- Rascol, O.; Fabbri, M.; Poewe, W. Amantadine in the treatment of Parkinson’s disease and other movement disorders. Lancet Neurol 2021, 20, 1048–1056. [Google Scholar] [CrossRef]
- Barczyk, A.; Czajkowska-Malinowska, M.; Farnik, M.; Barczyk, M.; Boda, Ł.; Cofta, S.; Dulawa, J.; Dyrbus, M.; Harat, R.; Huk, M.; Kotecka, S.; Nahorecki, A.; Nasiłowski, J.; Naumnik, W.; Przybylski, G.; Słabon-Willand, M.; Skoczynski, S.; Wita, K.; Zioło, G.; Kuna, P. Efficacy of oral amantadine among patients hospitalised with COVID-19: A randomised, double-blind, placebo-controlled, multicentre study. Respir Med. 2023, 212, 107198. [Google Scholar] [CrossRef] [PubMed]
- Bodnar, W.; Aranda-Abreu, G.; Slabon-Willand, M.; Kotecka, S.; Farnik, M.; Bodnar, J. The ecacy of amantadine hydrochloride in the treatment of COVID-19 - a single-center observation study. Research Square 2021. [CrossRef]
- Mohamed, Mona. Salah.; El Sayed, I.; Zaki, A.; Abdelmonem, S. Assessment of the effect of amantadine in patients with traumatic brain injury: A meta-analysis. J. Trauma Acute Care Surg 2022, 92, 605–614. [CrossRef]
- Andrea, Loggini.; Ruth, Tangonan.; Faten, E.l.A.; Ali, Mansour.; Fernando, D.; Goldenberg, C.L.; Kramer, C.L. The role of amantadine in cognitive recovery early after traumatic brain injury: A systematic review. Clin Neurol Neurosurg. 2020, 194.
- Ruhatiya, R.S.; Adukia, S.A.; Manjunath, R.B.; Maheshwarappa, H.M. ; Current Status and Recommendations in Multimodal Neuromonitoring. Indian J Crit Care Med. 2020, 24, 353–360. [Google Scholar]
- Roldán, M.; Kyriacou, P.A. Near-Infrared Spectroscopy (NIRS) in Traumatic Brain Injury (TBI). Sensors 2021, 21, 1586. [Google Scholar] [CrossRef]
- Plomgaard, A. M., van Oeveren, W., Petersen, T. H., Alderliesten, T., Austin, T., van Bel, F., Benders, M., Claris, O., Dempsey, E., Franz, A., Fumagalli, M., Gluud, C., Hagmann, C., Hyttel-Sorensen, S., Lemmers, P., Pellicer, A., Pichler, G., Winkel, P., & Greisen, G. The SafeBoosC II randomized trial: treatment guided by near-infrared spectroscopy reduces cerebral hypoxia without changing early biomarkers of brain injury. Pediatric research 2016, 79, 528–535.
- Du, J.; Deng, Y.; Li, H.; Qiao, S.; Yu, M.; Xu, Q.; Wang, C. Ratio of Optic Nerve Sheath Diameter to Eyeball Transverse Diameter by Ultrasound Can Predict Intracranial Hypertension in Traumatic Brain Injury Patients: A Prospective Study. Neurocritical care 2020, 32, 478–485. [Google Scholar] [CrossRef] [PubMed]
- Munawar, K.; Khan, M. T.; Hussain, S. W.; Qadeer, A.; Shad, Z. S.; Bano, S.; Abdullah, A. Optic Nerve Sheath Diameter Correlation with Elevated Intracranial Pressure Determined via Ultrasound. Cureus 2019, 11, 4145. [Google Scholar] [CrossRef] [PubMed]
- Volovici, V.; Huijben, J. A.; Ercole, A.; Stocchetti, N.; Dirven, C. M. F.; van der Jagt, M.; Steyerberg, E. W.; Lingsma, H. F.; Menon, D. K.; Maas, A. I. R.; Haitsma, I. K. Ventricular Drainage Catheters versus Intracranial Parenchymal Catheters for Intracranial Pressure Monitoring-Based Management of Traumatic Brain Injury: A Systematic Review and Meta-Analysis. Journal of neurotrauma. 2019, 36, 988–995. [Google Scholar] [CrossRef]
- Teasdale, G.; Jennet, B. Assessment of coma and impaired consciousness. Lancet 1974, 81–84. [Google Scholar] [CrossRef] [PubMed]
- McMillan, T.; Wilson, L.; Ponsford, J.; et al. The Glasgow Outcome Scale — 40 years of application and refinement. Nat Rev Neurol 2016, 12, 477–485. [Google Scholar] [CrossRef]
- Kurtz, P.; Rocha, E.E.M. Nutrition Therapy, Glucose Control, and Brain Metabolism in Traumatic Brain Injury: A Multimodal Monitoring Approach. Frontiers in neuroscience. 2020, 14, 190. [Google Scholar] [CrossRef]
- Muresanu, D.F.; Florian, S.; et al. Efficacy and safety of cerebrolysin in neurorecovery after moderate-severe traumatic brain injury: results from the CAPTAIN II trial. Neurol Sci 2020, 41, 1171–1181. [Google Scholar] [CrossRef]
- Vester, J.C.; Buzoianu, A.D.; et al. Cerebrolysin after moderate to severe traumatic brain injury: prospective meta-analysis of the CAPTAIN trial series. Neurol Sci 2021, 42, 4531–4541. [Google Scholar] [CrossRef]
- Beghi, E.; Binder, H.; Birle, C.; Bornstein, N.; Diserens, K.; Groppa, S.; Homberg, V.; Lisnic, V.; Pugliatti, M.; Randall, G.; Saltuari, L.; Strilciuc, S.; Vester, J.; Muresanu, D. European Academy of Neurology and European Federation of Neurorehabilitation Societies guideline on pharmacological support in early motor rehabilitation after acute ischaemic stroke. European journal of neurology. 2021, 28, 2831–2845. [Google Scholar] [CrossRef]
- Marshall, S,; Harnett, A,; Welch-West, P,; Ferri, C.; Janzen, S.; Togher, L.; Teasell, R.; Attention, Concentration and Information Processing Post Acquired Brain Injury. In Teasell R, Cullen N, Marshall S, Bayley M, Harnett A editors. Evidence-Based Review of Moderate to Severe Acquired Brain Injury. 2021, Version 14.0: p1-64. [CrossRef]
- Lee, S.; Haeng, L. H.; Lee, Y.; Lee, J. Additive effect of cerebrolysin and amantadine on disorders of consciousness secondary to acquired brain injury: A retrospective case-control study. Journal of Rehabilitation Medicine. 2020, 52, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Álvarez, X. A.; Sampedro, C.; et al. Positive effects of Cerebrolysin on electroencephalogram slowing, cognition and clinical outcome in patients with postacute traumatic brain injury: an exploratory study. Int. Clin. Psychopharmacol. 2003, 18, 271–278. [Google Scholar] [CrossRef] [PubMed]
- Giacino, J.T.; Whyte, J.; Bagiella, E.; Kalmar, K.; Childs, N.; Khademi, A.; Eifert, B.; Long, D.; Katz, D.I.; Cho, S.; Yablon, S.A.; Luther, M.; Hammond, F.M.; Nordenbo, A.; Novak, P.; Mercer, W.; Maurer-Karattup, P.; Sherer, M.; et al. Placebo-Controlled Trial of Amantadine for Severe Traumatic Brain Injury. N Engl J Med 2012, 366, 819–826. [Google Scholar] [CrossRef]
- Lindblad, C.; Raj, R.; Zeiler, F.A. Current state of high-fidelity multimodal monitoring in traumatic brain injury. Acta Neurochir 2020, 164, 3091–3100. [Google Scholar] [CrossRef]
- Ball, J. Protecting the brain from long term damage in Critical Care London. 2015, 13, 135–157. [Google Scholar] [CrossRef]
- Smith, M. Multimodality Neuromonitoring in Adult Traumatic Brain Injury: A Narrative Review. Anesthesiology 2018, 128, 401–415. [Google Scholar] [CrossRef] [PubMed]
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



