Submitted:
20 June 2023
Posted:
21 June 2023
You are already at the latest version
Abstract
Classifications of AAFD/PCFD have evolved with an increased understanding of the pathology involved. A review of classification systems helps identify deficiencies and respective contributions to the evolution in understanding the classification of AAFD.
Using multiple electronic database searches (Medline, PubMed) and Google search, original papers classifying AAFD were identified. Nine original articles were identified that met the inclusion criteria.
Johnson's original classification and multiple variants provided a significant leap in understanding and communicating the pathology but remained tibialis posterior tendon focussed. Drawbacks of these classifications include the implication of causality, linearity of progression through stages, an over-simplification of stage 2 deformity and a failure to understand multiple tendons react, not just tibialis posterior. Later classifications, such as the PCFD classification, are deformity-centric. Early instability in non-cavus feet and all stages of cavus feet can present pain and instability with minor/no deformity. These may not be captured in deformity-based classifications biased to planus feet.' The authors developed the 'Triple Classification' (TC) understanding that primary pathology is a progressive ligament failure/instability that presents as tendon reactivity, deformity, and painful impingement. There is a variable manifestation dependent on starting foot morphology.
This review has identified deficiencies within classification systems used in AAFD/PCFD and, as a result, was used to help develop a more comprehensive 'Triple classification'. Advantages of the TC include representing foot types with no deformity, defining complex secondary instabilities, delinking of foot types, tendon reactivity/ligament instability and deformity to represent these independently in a more comprehensive classification system.
Keywords:
Forefoot deformities
; flatfoot syndrome
1. Introduction
Adult Acquired Flatfoot Syndrome (AAFD), or Progressive Collapsing Foot Deformity (PCFD), is an evolving complex subject. It remains a clinical diagnosis supported by radiological investigations. As shown in Figure 1, the clinical picture comprises a combination of ligament instability, deformity, reactive tendinopathy, joint stiffness and degeneration. Initial starting foot morphology varies significantly, masking or accentuating the clinical picture. Many classifications have emerged, with the most recent focusing on deformity.
Aims
To conduct a Scopus review that would help identify advantages and drawbacks of existing classification systems to develop thus a new approach to classifying AAFD based on deficiencies identified.
2. Methods
The literature search strategy was developed using medical subject headings (MeSH terms) and text words related to 'flatfoot pathology'. Studies were independently identified studies by searching Medline (PubMed interface). The search was conducted on 04/March/2023. A hand search of the reference lists from all preliminarily identified papers was also carried out.
The eligibility criteria for inclusion in this scoping review were new classifications for classifying flatfoot.
Exclusion criteria were publications (i) cadaveric-based studies, (ii) no English translation available, (iii) no human subjects, (iv) studies that were radiographic/ MRI descriptors only and (v) studies where only the abstract is available.
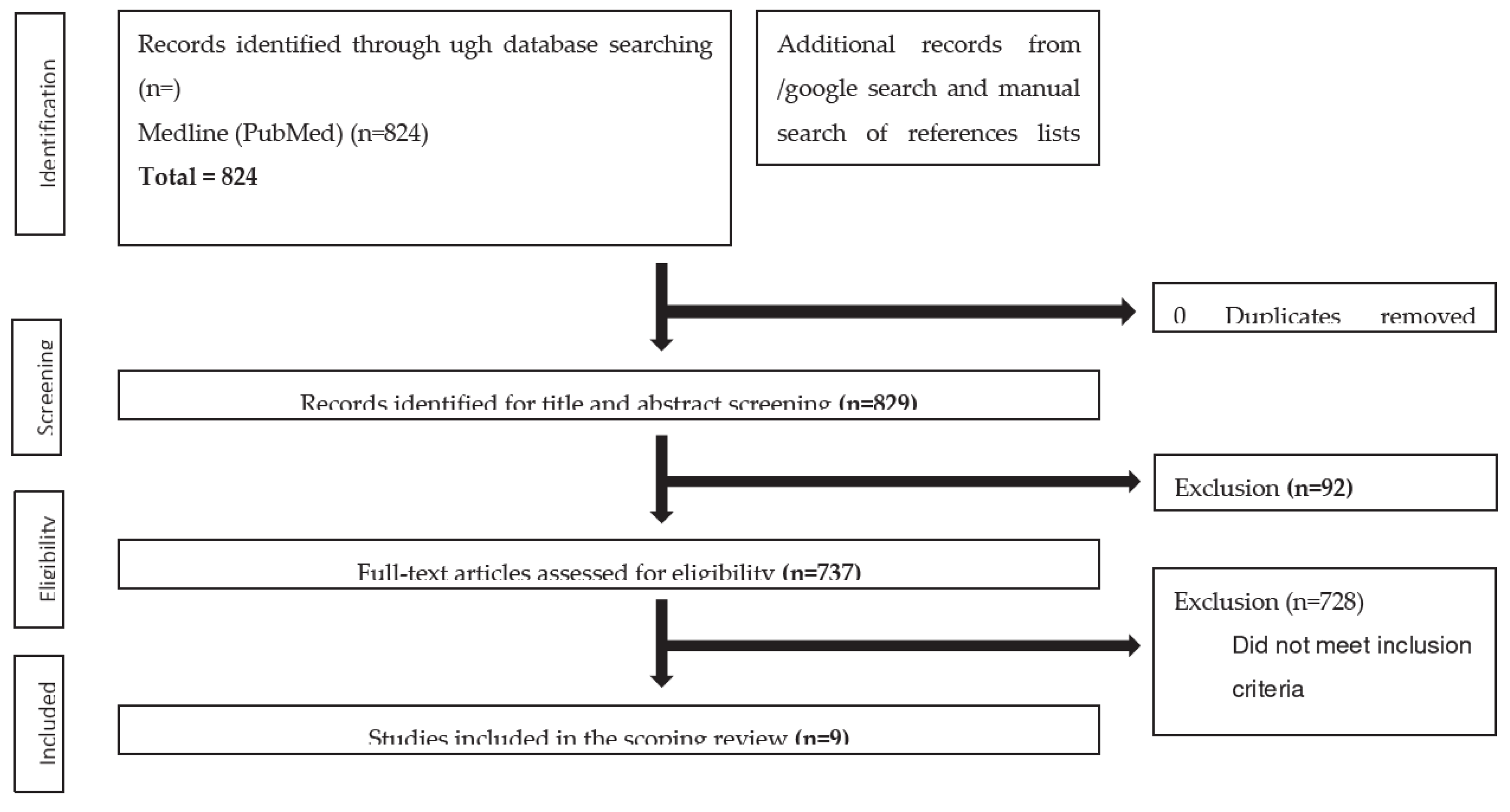
Figure 2.
PRISMA diagram showing the selection of papers for inclusion.
| Reason for exclusion | Number (From 737) |
| Review articles | 130 |
| Case reports | 24 |
| Not related to AAFD | 124 |
| Biomechanical studies | 60 |
| Other studies related to AAFD | 92 |
| All articles relating to surgical outcomes/techniques | 198 |
| Cadaver studies | 17 |
| Imaging/Radiology studies | 83 |
| New Classification Articles | 9 |
The senior author and co-author independently screened the titles and abstracts identified by the literature search for inclusion using the screening form (level 1 screening). There was 100% concordance in identifying original papers from the independent review process. The final studies found are shown in Table 1.
- Classifications Systems of AAFD/PCFD

Table 1.
Classification systems identified from the systematic review for AAFD/PCFD.
| Classification and Year | Article | Categories | |
|---|---|---|---|
| 1 | Johnson and Strom | 1989 | Original stage 1-3 classification |
| 2 | Myerson et al. | 1997 | Myerson modification of stages 1-4 |
| 3 | Weinraub and Heilala | 2002 | Stage 1-3 and grades (A, B, C) |
| 4 | Bluman et al. | 2007 | Stage 1-4 (A, B, C subtypes) |
| 5 | Deland | 2008 | Stages 1-4 (7 subtypes) |
| 6 | Parsons et al. | 2010 | Stage 1-4Stage 2 subtypes (A, B, C) |
| 7 | Raiken et al. | 2012 | RAM classificationThree categories and six subtypes |
| 8 | Pasapula et al. | 2017 | Stage 0-4 |
| 9 | Myerson et al. | 2020 | Stages 1-2 (242 subtypes) |
3. Results
3.1. A critical review of classifications
Initial understanding of AAFD was based on Johnson's Classification (1989) [1], which used clinical findings to communicate pathology. It erroneously assumed that primary synovitis/tears of the tibialis posterior (TP) tendon (Johnson stage 1) were causal rather than reactive, resulting in weakening of the medial arch, progressive collapse (Johnson stage 2) and fixed deformity (Johnson stage 3) [1]. Clinical, cadaver and computational modelling studies demonstrate that TP subtraction does not necessarily result in progression to unstable planovalgus (in AAFD) [2,3,4,5,6,7]. Finite element foot modelling demonstrates peroneal longus (PL) and TP tendon overload with simulated spring ligament (SL) laxity [8], reinforcing that tendon pain is reactive and not causal. The Johnson classification implies the foot starts in neutral posture and progresses to planus, yet many feet have pre-existing painless contralateral feet [9]. Controversy exists around the presence of Johnson's stage 1 AAFD [10]. This stage represents a crucial stage in some feet' natural history, alluding to the presence of midfoot ligament instability [SL/ superficial deltoid] with a stable first ray that resists planus [1,10,11]. It may present an opportunity to intervene early, before the onset of first ray instability (FRI) and to complex stage 2 deformities.
Initial classifications [1,11,12,45] implied progression between stages, which later classifications removed [10]. Progression rates between stages are not determined, and feet may not present at a specific stage or progress through all stages. Many feet are treated successfully with orthotics, remaining static if the tendon reactivity can be persuaded to settle.
Johnson's classification and its variants incorporated aspects of instability and stiffness [1,45, 11]. Later classifications used weight-bearing (WB) radiographs to account for talonavicular (TN) joint uncoverage [12], recognising the SL's role in stage 2 pathology but continued to focus on the TP tendon. Deltoid abnormalities were brought in later foot classifications in stage 3 [12] and into the RAM classification [42]. Myerson added to stage 4 to recognise deep deltoid rupture results in ankle valgus [44], further subclassified by Deland in 2008 [46]. Based on deformity location, the RAM classification implied that the TP tendon was the starting pathology in their stage 1 Rearfoot classification. Attempts to subclassify Johnson's stage 2 based on the degree of forefoot supination were made in the Truro classification [43]. Later, stage 0 was introduced [11] to define a stage of Talonavicular/spring ligament laxity and state this was the primary precipitating pathology, not the tibialis posterior, which can be clinically identified prior to first ray dorsiflexion failure. They believed this was the essential lesion in AAFD/PCFD development. Erroneously, these classifications remained 'deformity centric' with references to instability that continued to focus on the posterior tibialis.
In 2020 [10], Myerson proposed a new classification based on joint flexibility/rigidity and deformity location, as shown in Table 2. The consensus group of 9 mainly North American surgeons renamed the condition "Progressive Collapsing Foot Deformity" (PCFD). Some aspects did not reach 100% concordance.
Depending on associated clinical and radiograph findings, the system assesses deformity location and joint flexibility as stage I and rigidity as stage II.
This classification benefits from acknowledging that TP tendon reactivity is not the pathogenesis by removing it from its nomenclature. It removes the assumption of linearity of progression that Johnson's classification makes and the assumption that the foot starts in a normal attitude and progresses into planus through defined stages. The panel did not reach 100% consensus on using advanced modalities in the classification. It is primarily focused on classifying clinical deformity.
Drawbacks of this PCFD classification remain. Static weight-bearing imaging may miss or underestimate the associated dynamic instabilities and their severity, which requires clinical evaluation. Multiple tendon reactivity may be a significant presentation [14] and can present without deformity in the early stages of standard feet and any stage of collapsing cavus feet. As both 'deformity' and 'tendon reactivity' are secondary manifestations of progressive ligament instabilities, both need representation, not just deformity. Focussing on deformity detracts from representing feet with ligament instability in the absence of reactive deformities yet maybe/ maybe not progressively collapse. Two hundred forty-two subtypes make a comparative analysis and communication of different grades and stages difficult [15].
Further limitations of PCFD classification may arise from its reproducibility. There is good intra- observer reliability (Cohen kappa = 0.851, P < .001, 95% CI 0.777-0.926), however the interobserver reliability drops to moderate with a kappa value of (Fleiss kappa = 0.561, P < .001, 95% CI 0.528-0.594) [15,41]. Some PCFD subtypes only had a reliability of 0.07 / slight (class C) [15]. Collapsing planus feet constitute most and will be more expressive in their deformity [9]. Deformity-based classifications have an inherent bias in identifying deformity in planus feet with progressive instability. If a cohort of collapsing cavus feet is assessed, the classification may lack sensitivity in detecting deformity/pathology as they would naturally express deformity less. The degree of stiffness prior to becoming a fixed deformity is difficult to represent in classification systems. Li showed that the PCFD classification was not affected by the grade of the surgeon, but some aspects, such as peri talar subluxation, had a 26% misdiagnosis rate [13]. The abbreviations used are also not relatable [46]. Only nine surgeons were ultimately involved. Broadening the consensus with wider consultation of the professional field for future iterations of the PCFD classification may provide further insights and incorporate differential views [46].
3.2. Understanding the origin and identifying problems of AAFD classifications
- Deformity in AAFD is a variable expression of pre-existing foot posture and progressive instability arising from progressive ligament incompetence.
- Anteromedial deltoid instability, lateral column instability and significant subtalar instability/subluxation from interosseous ligament failure need representation.
- Overload reactivity of the plantar fascia [11] and the musculotendinous units [14,16] arise as a result of instability and changes to the subtalar axis (see below). Tendon overload and reactivity vary as the deformity progresses (PL and Tendoachilles), as they become offloaded and may not manifest in all AAFD stages.
- Cavus foot types with SL laxity and FRI may have no visible deformity yet have significant instability and tendon [TP and PL] overload pain [16].
- WB [axial gravitational force] stress joints in the axial plane. Many joints act perpendicular to the axial plane and, therefore, may not be expressive of the respective joint instability on weight-bearing radiographs. Joints whose motion acts perpendicular to the axial weight-bearing axis accentuate instability when forces are applied in the direction of their action. (TN joint: lateral plane/ ankle: anteroposterior motion instability and rotational ankle instability at the deltoid).
- Foot abduction stress radiographs exacerbate TN uncoverage, and ankle valgus stress views may accentuate deltoid instability. Both may be significantly underrepresented on weight-bearing radiographs.
| Name of classification | Year | Positive aspects of classification | Negative aspects of classification |
| Johnson and Strom | 1989 | 1. Original classification that classification systems are based upon 2. Linearity of progression demonstrated a basic understanding that more severe deformity with greater stage 3. Strong representation of early stages of AAFD where deformity can present with reactive TP |
1. No proven linearity of progression between stages 2. Fails to consider foot may not start in neutral 3. Focuses on the tibialis posterior as the prime driving force 4. Stage 2 is very under simplified 5. Very little on the validation of the classification system |
| Myerson | 1997 | 1. Modified Johnson and Strom classification to show deltoid instability occurs in stage 4 | 1. Still focussed on tibialis posterior as the prime cause 2. Failure to acknowledge that anteromedial ankle instability occurs prior to deltoid ligament failure 3. Assumed linearity of progression |
| Weinraub and Heilala | 2002 | 1. Understood that multiple factors determined the failure of the flatfoot 2. Recognised that the midtarsal joint played an important role in the stabilisation of flatfoot 3. Delinked deformity and tendon pathology |
1. Still primarily focussed upon the tibialis posterior tendon as the cause. 2. Based classification upon progressive inflammation/degenerative changes of the tendon |
| Bluman | 2007 | 1. Began to subclassify stage 2 and expand the different types 2. Graded level of deformity 3. Bluman classified a myriad of treatment options for all the subtypes |
1. Classification based upon the tibialis posterior in early stages 2. Implies progression of deformity through set stages 3. No discussion of the spring ligament and other ligaments that fail |
| Deland | 2008 | 1. Recognition of the Sl as a cause of potential instability | 2. Still focuses on the TP |
| Parsons | 2010 | 1. Began to subtype stage 2 into subtypes of A, B, C | 1. Still focuses on stage tibialis posterior as the cause of the flatfoot 2. Broadly based upon Johnson and Strom classification |
| Raiken | 2012 | 1. Previous classifications did not take into consideration the involvement of the mid-foot. 2. Classification was based on anatomic location, including the ankle, hindfoot, and mid-foot 3. Subgroups based on characteristic clinical and radiographic findings 4. Treatment algorithms then suggested based on these findings |
1. Several categories make communication more difficult 2. Still focused on tibialis posterior in early stages of the hindfoot |
| Pasapula | 2017 | 1. Introduced the concept of stage 0 2. Recognised that the tibialis posterior may or may not react despite the foot SL weakening and failing. |
Still used the Johnson and Strom classification Focuses on the tibialis posterior in stage 1 Continued to therefore simplify stage 2 |
| Myerson | 2020 | 1. Readdresses the pathology away from the tibialis posterior tendon 2. Several categories allow a more accurate representation of any one foot |
1. Static weight-bearing imaging may miss or underestimate the associated dynamic instabilities. 2. Multiple tendon reactivity may be a significant presentation [14] and can present without deformity, which needs representation. 3. Focussing on deformity detracts from representing feet with ligament instability. 4. 242 subtypes identified makes comparative analysis and communication of different grades and stages difficult. |
3.3. Key aspects to take into consideration in any new classification
3.3.1. The importance of the plantar fascia (PF) in protecting the SL and the effects of tight TA
An intact PF protects SL strain development [4]. Huang showed the plantar fascia confers a 56% relative contribution to arch stability [17]. Crary [4] demonstrated plantar fascia sectioning and cyclical cadaver foot loading leads to SL and long plantar ligament (LPL) strain and planus. PF is not represented in AAFD classification systems, but its role needs to be discussed. Non-rheumatological plantar fasciitis (NRPF) represents a potential early warning sign of foot progressive instability. SL/TN laxity has been shown in feet with NRPF, with ultrasound studies demonstrating SL thinning in feet with NRPF [18,19]. Symptomatic plantar fasciitis manifests as a reactive tensile overload of the PF [11]. Studies show in NRPF, altered radiographic foot alignment is present at the TN and subtalar joint articulations [20] and significant TN laxity, which reflects the short-term therapeutic effect of steroid injections in RCTs (3 months) and failure to address persistent biomechanical tensile overload [21].
The tendon Achilles / gastrocnemius tightness is the primary deforming factor or may develop secondary to the chronic valgus heel. Its presence is significant as a potential contributor to midfoot laxity. Tightness causes an early heel rise, prolonging inferomedial talar head pressure on the SL, causing strain and a midfoot break. Significant hindfoot valgus and internal rotation of the subtalar axis alters the TA pull and the heel strike ground reaction force vector to act lateral to the subtalar axis to augment hindfoot valgus. TA tightness prevents the reduction of the hindfoot to the neutral axis with ankle dorsiflexion.
3.3.2. The role of Musculotendinous units and their overload
Musculotendinous units decrease foot ligament stress [protective affect] [1], compensate for ligament failure [22] and have a dynamic role in contributing to foot arch stability [23]. Cadaver studies demonstrate increased subtalar joint internal rotation without TP without the plantar fascia and the SL [1]. Their loss does not necessarily lead to planus. Progressive ligament instability and deformity with biomechanical overload differentially overload tendons at different stages of deformity progression, which then act outside their physiological limit to manifest as reactive tendon pain (mainly medial retro-malleolar pain). EMG changes in intrinsic foot muscles, such as the abductor digiti minimi and the peroneus brevis, have been recorded [24]. Increased activity in the PL tendon [25], TP tendon and Achilles have been noted in collapsing planovalgus feet [14], reinforced by computational modelling [16,26].
3.3.3. Instability
AAFD classifications are large 'deformity centric', despite progressive ligament instability [primary pathology] manifesting as deformity, tendon reactivity and joint stiffness/degeneration. Determining the sequence of progressive ligament instability that develops in AAFD is important. Deformity as an expression of instability, depends on starting foot morphology, degree of ligament instability, joint stiffness/degeneration and the amount of axial load applied in the context of pain.
3.3.3.1. What's new about instability?
- Progressive instability is key to symptoms.
- Progressively collapse manifests as soft tissue reactivity and deformity, varying between individuals.
- Feet may not progress through all instability stages, and progression rates vary
- Some feet start with pre-existing laxity that has been physiologically normal for that foot. Increased instability progresses the foot to become symptomatic. Normal laxity for any foot may be gauged by contralateral foot comparison if unaffected, from serial foot assessment, or may never be ascertained if no pre-existing reference point exists.
- Lateral column instability, subtalar instability, and deltoid instability reflect a greater extent of foot ligament failure than the isolated failure of the medial column. Addressing the medial column alone (superficial deltoid/spring and first ray) may not restore all the foot instabilities that have developed completely.
3.3.3.2. Evidence for sequential/progressive instabilities in AAFD
Evidence for sequential instability comes from studies in several disciplines (cadaver/computational and clinical). Although multiple ligaments eventually progressively fail, the hallmark of AAFD requires some degree of SL component strain/dysfunction of the wider superficial deltoid-spring ligament complex [27], which would then allow inferomedial talar head subluxation and secondary/concomitant first ray destabilisation. Using a cadaver model, Jennings created deformities associated with AAFD in a 3-dimensional custom-loaded frame [29]. Significant rotational changes of the talus, navicular, and calcaneus occurred after SL sectioning that the loaded TP tendon could not restore, despite its incremental tensioning [30]. A functioning PF [4] acts as a tie beam for the medial longitudinal arch, and an intact superficial deltoid suspends the SL from the fixed medial malleolus. Their dysfunctions increase SL stress leading to its strain [31]. Early SL strain, not visible on WB radiographs, needs clinical evaluation [28]. The TN portion of the superficial deltoid also restrains TN abduction [32], and the tibiospring ligament suspends the SL from the medial malleolus.
There is a potential dichotomy of views regarding the superficial deltoid's structure. Dense condensations by some authors are thought to form individual ligament bands/fascicles [29]. The tibiotalocalcaneal ligament is consistently present, but other bundles have a variable presence [29]. The tibiotalocalcaneal ligament resists talus abduction [29]. Amaha demonstrated the internal morphology of the deltoid-spring ligament forms a single continuous structure that can be reflected as one from the medial malleolus [27]. Anteriorly it is composed of mainly fatty tissue, and medially fibrous tissue and inferiorly, the area known as the SL was recognised to be fibrocartilaginous. Injury to one area likely increases strain, given the same load in another area.
3.3.3.3. First Ray Instability and its classification
FRI develops concomitantly or after SL laxity [33], progressing the foot to an unstable planus [2, 31]. The stable first ray exerts an opposing supinating ground reaction force vector that resists foot pronation / inferomedial talar head subluxation with SL strain. The first ray eventually fails in dorsiflexion (failure of the plantar TMT ligaments and/or the plantar NC ligaments). Cyclical loading cadaver studies demonstrate a decrease in Meary's axis after SL/PF sectioning [33]. Deep deltoid rupture in ankle fractures demonstrates SL weakening [34] and Type 1 FRI (secondary to SL laxity, not hallux valgus [31]) that develops within six months post-injury [31]. Radiographic change in Meary's axis of 30 degrees has a high (100%) sensitivity for predicting intraoperative SL tears [30].
3.3.3.4. Lateral Column Instability
Lateral column instability develops in AAFD but is often not documented [4]. The mean increase in lateral column motion in feet with symptomatic AAFD is 5.5 mm [35]. SL laxity internally rotates the subtalar axis, lateralising forefoot load concerning the subtalar axis at toe-off. Medial column instability and gait alterations from a painful 2nd MTP joint further transfer load laterally to the middle and lateral foot columns straining the long plantar ligament and the plantar capsular ligaments.
3.3.3.5. Deltoid Instability
SL laxity affects superficial deltoid function (TN / tibiocalcaneal ligaments) and vice versa [31]. Abnormal talar kinematics most likely allows stress to transfer to the deep deltoid portion [1]. Forces from the valgus heel exacerbate talar head abduction forces that strain the superficial deltoid (TN / tibiocalcaneal). This contributes to deep deltoid strain and anteromedial ankle instability in AAFD, which is not represented in some classifications. Anteromedial ankle instability develops prior to deltoid rupture with ankle capsular failure/valgus ankle (Johnson stage 4). The gravitational external test and the external heel rotation test have been considered the gold standard [36,37] for detecting deep deltoid instability, prior to Johnson's stage 4 failure. Anteromedial gutter pain sensitivity is unknown as a sign of deep deltoid insufficiency in chronic anteromedial instability. The presence of anteromedial ankle instability in AAFD may change surgical management and maybe a persistent cause of PTT overload when counteracting this instability. This would be akin to peroneal pain with ankle instability. In our practice, patients with AAFD always have a positive lateral push test, often have a positive anteromedial draw test but sometimes have an external heel rotation test [37], suggesting multiple types of deltoid spring failures that have yet to be classified.
3.3.3.6. Subtalar Instability
The SL acts as a primary restraint to the hindfoot valgus. TN joint unlocking with SL laxity and secondary first ray instability allows non-physiological hindfoot valgus. Talonavicular joint laxity [SL laxity] and associated non-physiological heel valgus thrust negatively exacerbate each other with cyclical foot loading. Eventually, subtalar (interosseous) ligaments will strain with the hindfoot valgus [38], allowing subtalar instability. SL reconstruction may restore the TN joint axis but may not restore subtalar joint stability, or the subtalar axis if subtalar ligaments are compromised. Persistent subtalar instability and impingement (sinus tarsi and fibula) can still exist. Clinical examination aids diagnosis [28]. Sub-fibular/sinus tarsi impingement on WB radiographs and MRI subtalar ligament changes alludes to interosseous ligament instability [38]. Subtalar fusion as part of the treatment may restore stability and limit pain in this scenario. A good reference clinical test examination for subtalar/interosseous ligament instability assessment prior to lateral impingement after talonavicular reduction is still lacking [39,40].
4. Discussion
4.1. Foot Type and potential differential behaviour of cavus feet
Foot morphology is important. Given their biomechanical disadvantage, more planus feet destabilise/collapse [9]. Asymptomatic feet can start with normal, planus or cavus attitude and varying degrees of intrinsic stability. Scenarios with less deformity expression include collapsing cavus feet and feet with neutral foot attitude with SL laxity and first ray stability (early stages). FRI may not be radiographically expressed, given the starting plantarflexed position in cavus feet, yet act to overload the PLT and TP tendon. Deformity-based classifications may struggle to classify AAFD in these scenarios.
4.2. Triple classification: Foot Type/Stage of Instability / Zone of deformity
The 'Triple classification (TC)' delinks instability, which leads to deformity and degeneration in different foot types. In a highly evolving subject, addressing these entities independently enables a greater representation of stages and types of AAFD.
The 'backbone' of the TC is primarily stage feet, as shown in Figure 3, based on progressive instabilities, understanding deformity, degeneration and tendon/fascia overload are secondary consequences that are variably expressed. The secondary deformity can help anatomically localise instabilities. Early TC stages have instability with no deformity; later stages have more deformity, rigidity and degeneration, which can be zoned based on axial radiographs. Flexible stages have instabilities and deformities. Rigidity masks prior stages of ligament instability that have developed.
4.2.1. TC foot type
4.2.2. TC stage based on instability
Progressive ligament instabilities occur combined or discreetly through stages, as shown in Figure 4.
- TC stage 0:
-
Loss of SL integrity leads to TN abduction laxity (see above), allowing the potential for foot progression into planus (and development of secondary instabilities). SL integrity loss may arise primarily due to superficial deltoid or plantar fascia integrity loss. Assessing strain in these two structures may be more difficult to clinically ascertain. First, ray stability resists planus, and thus planus is not present on examination. This is the earliest isolated flatfoot lesion that can be clinically identified.
- -
- Neutral Heel lateral push test (NHLT) positive
- -
- The first ray is stable
- TC stage 1:
-
Reactive phase of the foot. Instability with biomechanical overload causes tendons and fascia to react prior to planus. SL laxity predisposes the foot to progressive collapse, but the stable first ray prevents planus. We believe the PF reactivity may represent an early warning sign. However, this stage of early foot reactivity may not be present in all feet with progressive collapse. Its presence alludes to the presence of instability
- -
- Above with tender reactive TP/PLT and plantar fascia
- TC stage 2:
-
First ray dorsal sagittal failure (TMT commonly and/or NC joints) secondary to SL laxity(type 1 FRI) is the hallmark of stage 2 pathology. Stability in this acts as a secondary stabiliser to planus. FRI with a lax/unlocking of the TN joint (SL laxity) progresses the foot into the planus. (a common stage/clinical scenario seen).
- -
- SL instability: Positive NHLT
- -
- FRI / dorsiflexion (Roots manoeuvre, Morton's test, Double dorsiflexion test)
- TC stage 3:
-
Secondary foot complex foot instabilities are present. Foot instability is no longer isolated to the TN joint and the first ray but begins to demonstrate more widespread instability at the ankle joint, the lateral column and/or the subtalar joint. Anteromedial ankle instability is secondary to superficial and deep deltoid failure, lateral column instability due to LPL strain [4] and subtalar instability from interosseous strain. These instabilities represent a more widespread foot ligament failure/involvement. Instabilities that have arisen beyond the medial column (SL and first ray inability) are explicitly stated, e.g. Stage 3 D (deltoid) or Stage 3DS(deltoid and subtalar).
- -
- [L] Lateral column ballottement compared to the contralateral side
- -
- [D] Anteromedial ankle draw test for deep deltoid
- -
- Heel external rotation test for deep deltoid instability
- -
- [S] Anterior draw for subtalar instability
- TC stage 4:
- Deep deltoid failure with capsular failure. The ankle progresses into the valgus. The assessment of instability is clinical and radiographic. Deformity helps anatomical localisation of ligament deficits.
Zoning deformity based on axial stress (weight bearing) radiographs further aids deformity localisation in stages 2,3,4 and alludes to foot type, as shown in Figure 5. Early stages of Type N and multiple stages of Type C feet may express no deformity and are classified as Zone U (deformity unidentified).
The role of advanced imaging modalities such as US, MRI, wb CT and stress views in staging ligament failure may be used but have not been incorporated in this iteration.
The deformity can be further subtyped into f,r, and d subtypes (flexible, rigid or with degenerative arthritis) within different zones where there may be a rigid hindfoot but a flexible first ray and vice versa.
4.3. Overview diagram of the Triple classification system
Based on everything we have discussed, feet can be classified based on Foot type, Stages of ligament instability and Zones of deformity, as shown in Figure 6.
5. Conclusions
AAFD/PCFD remains a clinical diagnosis with imaging modalities supportive serving to augment diagnosis. The fundamental pathology remains a sequential /combined failure of foot ligaments that start in the medial deltoid-spring ligament complex. Deformity assessment alone may not accurately diagnose stage 0 or complex stage 3 instabilities present in AAFD [Triple classification] and requires clinical with radiographic assessment. The TC is a more comprehensive classification system where Feet can be Typed, Deformity can be zoned, and instability can be staged. It also serves as a more comprehensive basis for future iterations as improved clinical assessment develops to diagnose more complex instabilities.
Funding
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors
References
- Johnson K, Strom D. Tibialis posterior tendon dysfunction. Clinical Orthopaedics and Related Research 1989;239. [CrossRef]
- Jeng C, Myerson M. The use of tendon transfers to correct paralytic deformity of the foot and ankle. Foot and Ankle Clinics 2004;9:319–37. [CrossRef]
- Cifuentes-De la Portilla C, Larrainzar-Garijo R, Bayod J. Analysis of the main passive soft tissues associated with adult acquired Flatfoot Deformity Development: A computational modelling approach. Journal of Biomechanics. 2019;84:183–90. [CrossRef]
- Crary JL, Hollis JM, Manoli A. The effect of plantar fascia release on strain in the spring and long plantar ligaments. Foot & Ankle International 2003;24:245–50. [CrossRef]
- Mizel MS, Temple HT, Scranton PE, Gellman RE, Hecht PJ, Horton GA, et al. Role of the Peroneal tendons in producing the deformed foot with posterior tibial tendon deficiency. Foot & Ankle International 1999;20:285–9. [CrossRef]
- Yeap JS, Birch R, Singh D. Long-term results of tibialis posterior tendon transfer for drop-foot. International Orthopaedics 2001;25:114–8. [CrossRef]
- Pecheva M, Devany A, Nourallah B, Cutts S, Pasapula C. Long-term follow-up of patients undergoing tibialis posterior transfer: Is acquired PES Planus a complication? The Foot 2018;34:83–9. [CrossRef]
- Cifuentes-De la Portilla C, Pasapula C, Larrainzar-Garijo R, Bayod J. Finite element analysis of secondary effect of midfoot fusions on the spring ligament in the management of adult acquired flatfoot. Clinical Biomechanics 2020;76:105018. [CrossRef]
- Dyal CM, Feder J, Deland JT, Thompson FM. PES planus in patients with posterior tibial tendon insufficiency: Asymptomatic versus symptomatic foot. Foot & Ankle International 1997;18:85–8. [CrossRef]
- Myerson MS, Thordarson DB, Johnson JE, Hintermann B, Sangeorzan BJ, Deland JT, et al. Classification and nomenclature: Progressive collapsing foot deformity. Foot & Ankle International 2020;41:1271–6. [CrossRef]
- Pasapula C, Cutts S. Modern theory of the development of adult acquired Flat Foot and an updated spring ligament classification system. Clinical Research on Foot & Ankle 2017;05. [CrossRef]
- Bluman EM, Title CI, Myerson MS. Posterior tibial tendon rupture: A refined classification system. Foot and Ankle Clinics 2007;12:233–49. [CrossRef]
- Li S, Zhu M, Gu W, Hamati M, Hunt KJ, de Cesar Netto C, et al. Diagnostic accuracy of the progressive collapsing foot deformity (PCFD) classification. Foot & Ankle International 2022;43:800–9. [CrossRef]
- Chiang CY, Lin KW, Yang WW, Chang YC, Chou LW. Changes in lower extremity biomechanics and muscle activity after six-minute fast-walk in individuals with flatfoot. Annals of Physical and Rehabilitation Medicine 2018;61. [CrossRef]
- Lalevée M, Barbachan Mansur NS, Lee HY, Ehret A, Tazegul T, de Carvalho KA, et al. A comparison between the bluman et al. and the progressive collapsing foot deformity classifications for flatfeet assessment. Archives of Orthopaedic and Trauma Surgery 2021. [CrossRef]
- Cifuentes-De la Portilla C, Pasapula C, Gutiérrez-Narvarte B, Larrainzar-Garijo R, Bayod J. Peroneus longus overload caused by soft tissue deficiencies associated with early adult acquired Flatfoot: A finite element analysis. Clinical Biomechanics 2021;86:105383. [CrossRef]
- Huang C-K, Kitaoka HB, An K-N, Chao EY. Biomechanical evaluation of Longitudinal Arch Stability. Foot & Ankle 1993;14:353–7. [CrossRef]
- Tanaka K, Kudo S. Functional assessment of the spring ligament using ultrasonography in the Japanese population. The Foot 2020;44:101665. [CrossRef]
- Pasapula C, Kiliyanpilakkil B, Khan DZ, Di Marco Barros R, Kim S, Ali AM, et al. Plantar fasciitis: Talonavicular instability/spring ligament failure as the driving force behind its histological pathogenesis. The Foot 2021;46:101703. [CrossRef]
- Graham ME, Kolodziej L, Kimmel HM. The Frequency of Association between Pathologic Subtalar Joint Alignment in Patients with Recalcitrant Plantar Fasciopathy-A Retrospective Radiographic Evaluation. Clinical Research on Foot & Ankle 2019;7:2. [CrossRef]
- McMillan AM, Landorf KB, Gilheany MF, Bird AR, Morrow AD, Menz HB. Ultrasound guided corticosteroid injection for plantar fasciitis: Randomised controlled trial. BMJ 2012;344. [CrossRef]
- Wong DW-C, Wang Y, Leung AK-L, Yang M, Zhang M. Finite element simulation on posterior tibial tendinopathy: Load transfer alteration and implications to the onset of PES Planus. Clinical Biomechanics 2018;51:10–6. [CrossRef]
- Robberecht J, Shah DS, Taylan O, Natsakis T, Vandeputte G, Vander Sloten J, et al. The role of medial ligaments and tibialis posterior in stabilising the medial longitudinal foot arch: A cadaveric gait simulator study. Foot and Ankle Surgery 2022;28:906–11. [CrossRef]
- Gatens PF, Saeed MA. Electromyographic findings in the intrinsic muscles of normal feet. Arch Phys Med Rehabil. 1982;63(7):317-318. [PubMed]
- Ringleb SI, Kavros SJ, Kotajarvi BR, Hansen DK, Kitaoka HB, Kaufman KR. Changes in gait associated with acute stage II posterior tibial tendon dysfunction. Gait & Posture 2007;25:555–64. [CrossRef]
- Cifuentes-De la Portilla C, Larrainzar-Garijo R, Bayod J. Biomechanical stress analysis of the main soft tissues associated with the development of adult acquired Flatfoot Deformity. Clinical Biomechanics 2019;61:163–71. [CrossRef]
- Amaha K, Nimura A, Yamaguchi R, Kampan N, Tasaki A, Yamaguchi K, et al. Anatomic study of the medial side of the ankle base on the joint capsule: An alternative description of the deltoid and spring ligament. Journal of Experimental Orthopaedics 2019;6. [CrossRef]
- Pasapula C, Devany A, Magan A, Memarzadeh A, Pasters V, Shariff S. Neutral heel lateral push test: The first clinical examination of Spring ligament integrity. The Foot 2015;25:69–74. [CrossRef]
- Jennings MM, Christensen JC. The effects of sectioning the spring ligament on rearfoot stability and posterior tibial tendon efficiency. The Journal of Foot and Ankle Surgery 2008;47:219–24. [CrossRef]
- Pate M, Hall J, Albright P, Bohay D, Anderson J, Roberts J. Increasing values of the lateral talar-first metatarsal angle preoperatively predict spring ligament attenuation in adult acquired flat foot deformity. Foot & Ankle Orthopaedics 2019;4. [CrossRef]
- Pasapula C, Ali AMS, Kiliyanpilakkil B, Hardcastle A, Koundu M, Gharooni A-A, et al. High incidence of spring ligament laxity in ankle fractures with complete deltoid ruptures and secondary first ray instability. The Foot 2021;46:101720. [CrossRef]
- Baxter JR, LaMothe JM, Walls RJ, Prado MP, Gilbert SL, Deland JT. Reconstruction of the medial talonavicular joint in simulated flatfoot deformity. Foot & Ankle International 2014;36:424–9. [CrossRef]
- Chu I-T, Myerson MS, Nyska M, Parks BG. Experimental flatfoot model: The contribution of dynamic loading. Foot & Ankle International 2001;22:220–5. [CrossRef]
- Wiegerinck JJ, Stufkens SA. Deltoid rupture in ankle fractures. Foot and Ankle Clinics 2021;26:361–71. [CrossRef]
- Chrastek D, Elmousili M, Al-Sukaini A, Austin I, Pasapula C. Quantiative assessment of dorsal sagittal lateral column instability in unilateral adult acquired Flatfoot Deformity (AAFD). British Orthopaedic Association Conference 2021. [CrossRef]
- Michelson JD, Varner KE, Checcone M. Diagnosing deltoid injury in ankle fractures. Clinical Orthopaedics and Related Research 2001;387:178–82. [CrossRef]
- Femino JE, Vaseenon T, Phistkul P, Tochigi Y, Anderson DD, Amendola A. Varus external rotation stress test for radiographic detection of deep deltoid ligament disruption with and without syndesmotic disruption. Foot & Ankle International 2013;34:251–60. [CrossRef]
- De Cesar Netto C, Saito GH, Roney A, Roberts L, Fansa A, Greditzer H, et al. Weightbearing CT and MRI findings of Stage II flatfoot deformity: Can we predict patients at high- risk for foot collapse? Foot & Ankle Orthopaedics 2019;4. [CrossRef]
- Michels F, Clockaerts S, Van Der Bauwhede J, Stockmans F, Matricali G. Does subtalar instability really exist? A systematic review. Foot and Ankle Surgery 2020;26:119–27. [CrossRef]
- Kato, T. The diagnosis and treatment of instability of the subtalar joint. J Bone Joint Surg Br. 1995;77(3):400-406. [PubMed]
- Lee HY, Barbachan Mansur NS, Lalevée M, Dibbern KN, Myerson MS, Ellis SJ, et al. Intra- and Interobserver reliability of the new classification system of progressive collapsing foot deformity. Foot & Ankle International 2021;43:582–9. [CrossRef]
- Raikin SM, Winters BS, Daniel JN. The RAM classification: a novel, systematic approach to the adult-acquired flatfoot. Foot and Ankle Clinics 2012;17:169–81. [CrossRef]
- Parsons S, Naim S, Richards PJ, McBride D. Correction and prevention of deformity in type II tibialis posterior dysfunction. Clinical Orthopaedics & Related Research 2010;468:1025–32. [CrossRef]
- Myerson, MS. Adult acquired flatfoot deformity: treatment of dysfunction of the posterior tibial tendon. Instr Course Lect. 1997;46:393-405.
- Weinraub GM, Saraiya MJ. Adult flatfoot/posterior tibial tendon dysfunction: Classification and treatment. Clinics in Podiatric Medicine and Surgery 2002;19:345–70. [CrossRef]
- Boakye LA, Uzosike AC, Bluman EM. Progressive collapsing foot deformity: Should we be staging it differently? Foot and Ankle Clinics 2021;26:417–25. [CrossRef]
- Deland, JT. Adult-acquired Flatfoot Deformity. Journal of the American Academy of Orthopaedic Surgeons 2008;16:399–406. [CrossRef]
Figure 1.
The clinical components of AAFD.

Figure 3.
Triple classification foot types.
Figure 4.
Triple classification stages.
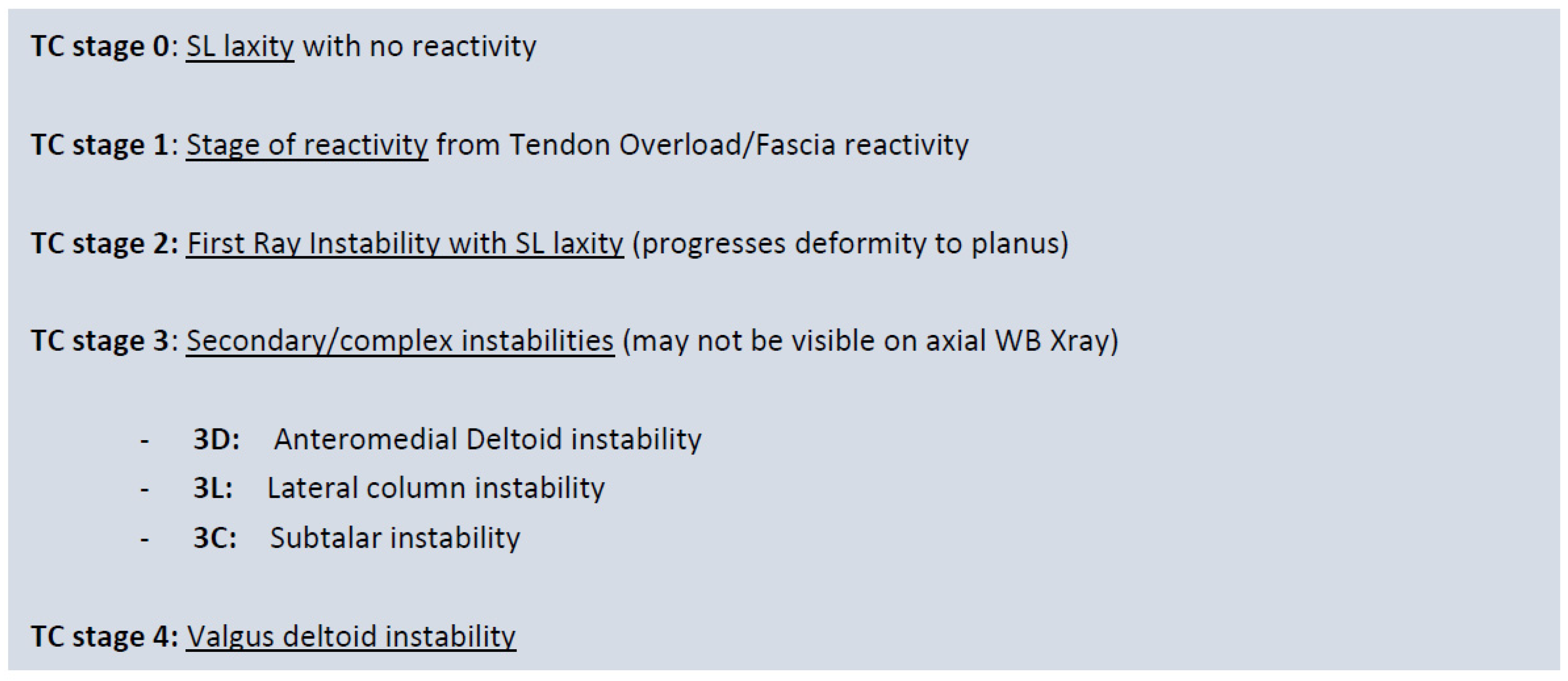
Figure 5.
Zonal classification is based on the anatomic location of the deformity.
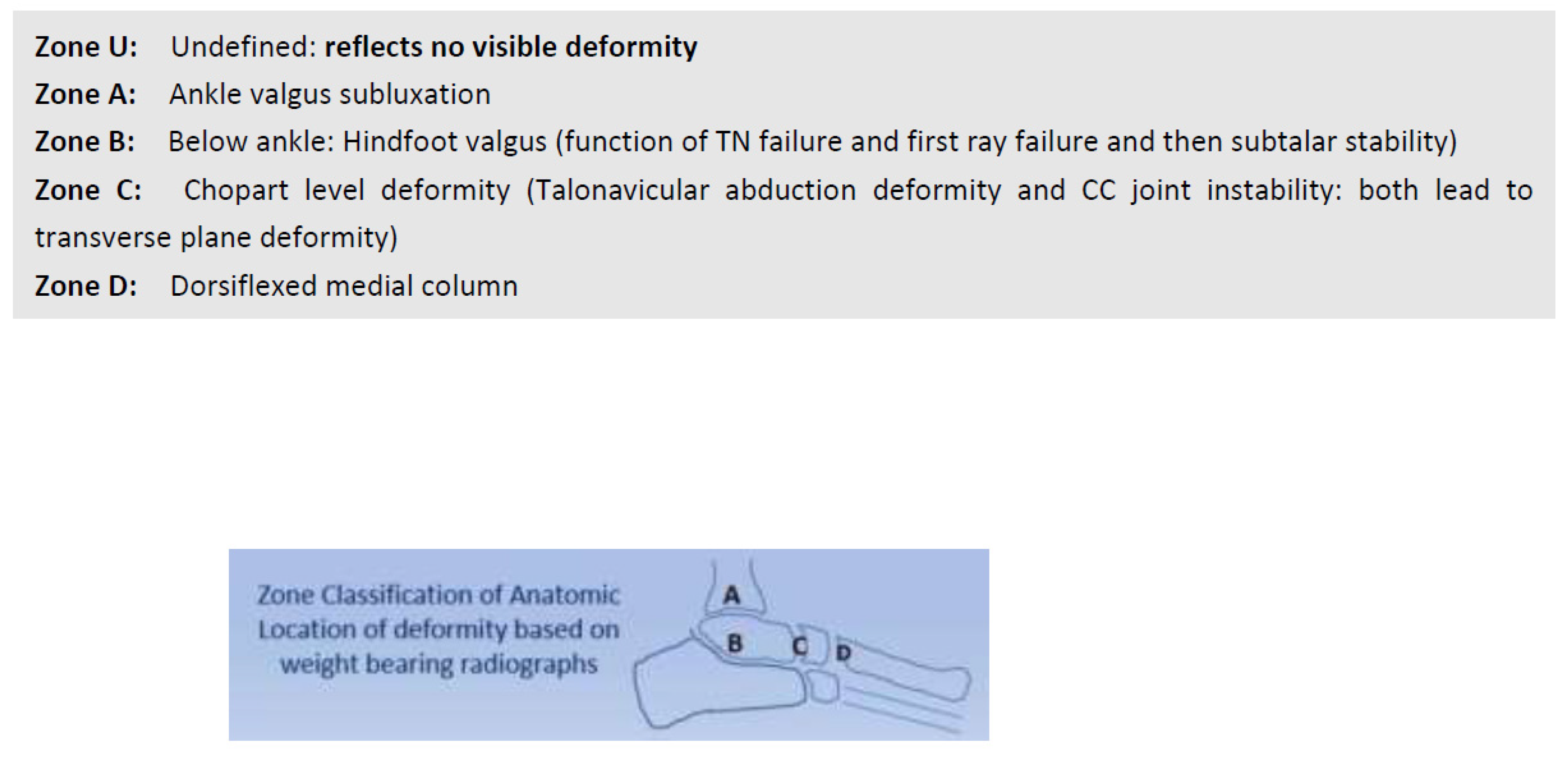
Figure 6.
Triple classification of AAFD.
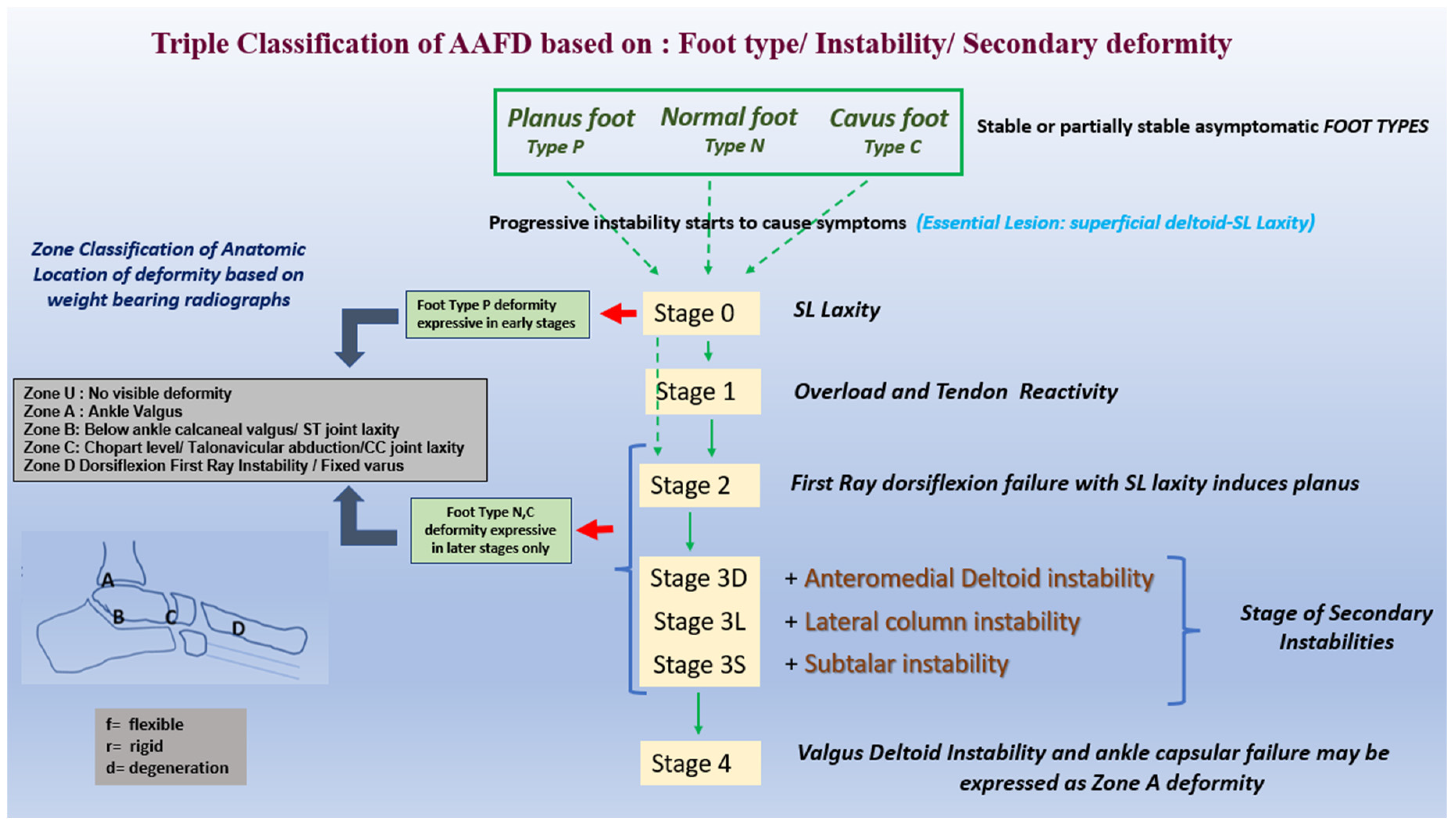
Table 2.
Myerson's classification of progressive collapsing foot deformity (PCFD).
| Stage of deformity | ||
|---|---|---|
| Stage I (flexible) or Stage II (rigid) | ||
| Type of deformity | ||
| Deformity type/location | Clinical/radiographic findings | |
| Class A | Hindfoot valgus deformity | Hindfoot valgus alignment Increased hindfoot moment arm, hindfoot alignment ankle, foot and ankle offset |
| Class B | Midfoot/forefoot abduction deformity | Decreased talar head coverage Increased talonavicular coverage angle Presence of sinus tarsi impingement |
| Class C | Forefoot varus deformity/medial column instability | Increased talus-first metatarsal angle Plantar gapping first tarsometatarsal (TMT) joint / naviculocuneiform (NC) joints Clinical forefoot varus |
| Class D | Peritalar subluxation/dislocation | Significant subtalar joint subluxation/sub-fibular impingement |
| Class E | Ankle instability | Valgus tilting of the ankle joint |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



