Submitted:
08 June 2023
Posted:
12 June 2023
You are already at the latest version
Abstract
Choroid plexus insufficiency or glymphatic stasis are often classified as prequels to harmful accretion of toxic proteins in neurodegenerative disease. Cognitive decline and memory loss subsequently become cardinal features of Alzheimer’s disease (AD), typically progressing with amyloid-ß and tau protein accumulation. For Parkinson’s disease (PD), α-synuclein deposits and dopamine depletion are linked to impaired movement, resting tremor, and rigidity. Importantly, both diagnoses are accompanied by hyperinflammation and intrathecal cytokine changes. Thus far, numerous clinical trials for investigational drugs have produced nothing effective for AD or PD, yet the anti-inflammatory and regenerative potential of platelet-rich plasma (PRP) remains largely unexamined in this context. This report explores a proposed Phase I study on intrathecal condensed plasma growth factors processed from autologous thrombin-activated PRP as monotherapy for AD or PD. The concept gains support from related work where cytokines of platelet origin successfully lowered inflammation, corrected background fibrosis, deactivated abnormal cells, and recovered local tissue function—all desirable outcomes in AD and PD. PRP-mediated effects on membrane potentials, electrolyte balance, and water clearance are less well characterized, but experimental evidence suggests these pathways could likewise influence glymphatic drainage to ameliorate proteinopathies. As a well-tolerated ‘orthobiologic’ with no hypersensitivity risk, intrathecal PRP and its derivatives bring advantages distinct from synthetic pharmaceuticals. If age-associated neuroinflammation in AD and PD is an upstream event contributing to neural disruption, then dampening local oxidative stress by a patient’s own platelet cytokines (as already proven in other tissues) could offer therapeutic relevance to these neurodegenerative conditions as well.
Keywords:
Alzheimer’s disease
; Parkinson’s disease
; condensed cytokines
; intrathecal
; PRP
1. Introduction
The need to provide a cure for chronic neurodegenerative diseases has never been more acute. Despite decades of uninterrupted international scientific efforts, clinical trials for Alzheimer’s disease (AD) have scored the lowest yield of almost any medical research endeavor [1]. Forecasts for breakthroughs in Parkinson’s disease (PD) are similarly bleak [2]. And as global incidence of neurodegenerative diseases is expected to increase three-fold by 2050 [3,4] the socioeconomic importance of this public health concern is outpacing the medical research meant to check them.
While the poor return on AD and PD research has been discussed by others [2,5], against this busy background one path to cure still remains largely untraveled: Intrathecal platelet-rich plasma (PRP). Considering novel recombinants synthesized to alter production of specified brain proteins, autologous PRP risks being discounted as simplistic by comparison. However, in addition to platelet-derived growth factor (PDGF), fibroblast growth factor (FGF), insulin-like growth factor-1 (IGF-1), vascular endothelial growth factor (VEGF) and other better-known PRP constituents, activated platelet (PLT) releasate also includes nerve growth factor (NGF), brain-derived neurotrophic factor (BDNF), and neurotrophin-3 (NT3), plus other potent neurotrophic signals [6,7]. Notwithstanding animal data on inflammatory myelin damage in multiple sclerosis showing recovery after intrathecal PRP [8], a literature search intersecting ‘intrathecal’ and ‘platelet-rich plasma’ identifies only seven publications—and none specifically address AD or PD. While the paucity of published data on intrathecal PRP for neurodegenerative conditions is notable, more worrisome is a survey of registered clinical trials on this topic, where no investigations are currently underway or planned [9]. This means that not only is scant knowledge available on this point now, the research pipeline is extremely unlikely to deliver anything of relevance going forward. Accordingly, this account puts intrathecal PRP under fresh scrutiny as an alternative anti-inflammatory, regenerative, disease-modifying option in AD and PD.
2. Cerebrospinal fluid and neurodegenerative pathology
Substantial neuronal loss occurs in both AD and PD. For both conditions, diagnosis depends on clinical tests where detection of early-stage disease is far from ideal. Indeed, at initial presentation the stage of neurodegeneration may already be quite advanced [10]. A recent study of noradrenaline, 3-methoxy-4-hydroxyphenylglycol, and noradrenaline transport availability for both conditions found that PD shows markedly lower levels of noradrenaline and 3-methoxy-4-hydroxyphenylglycol in cerebrospinal fluid (CSF), as well as poor hypothalamic noradrenaline transport availability [11]. In AD, profoundly reduced amyloid-β clearance is observed compared to healthy controls yet production quantity is unchanged [12]. While there is disagreement on how much time must pass before these changes will manifest, the relation highlights the role of disordered brain clearance systems [13,14] where resident microglia and peripheral mononuclear phagocytes somehow exhaust their governance over cerebral deposition of amyloid-β [15,16].
Cellular water handling is also relevant to CSF dynamics, and the aquaporin (AQP) family has been extensively studied with at least 12 different AQPs operating in specific cell types. While function of transmembrane channels is subject to resting voltage potentials [17], how PLT cytokines influence cell portal operation is only now being investigated. Loss of membrane integrity from inflammation is often reversible, and ongoing work should extend recent discoveries concerning how gap junctions are targets for selected PLT cytokines [18]. If this also applies to the main aquaporin in neural tissue (AQP4), then PLT cytokines may actuate this transmembrane gate to mediate amyloid-β clearance [19] and manage extracellular volume during synaptic action [20]. Moreover, this proposal incorporates PLT activation by thrombin [21] rather than calcium chloride or calcium gluconate [22], to minimize risk of electrolyte upset.
When CSF cytokines in AD patients were referenced against healthy controls, eotaxin, IL-1ra, IL-4, IL-7, IL-8, IL-9, IL-10, IL-15, GCSF, monocyte chemotactic protein 1, PDGF, and TNF-alpha were all elevated [16]. Of note, a negative correlation was observed between disease progression and IL-1β, IL-4, IL-6, IL-9, IL-17A, FGF, GCSF, GMCSF, interferon gamma, and macrophage inflammatory protein-1β [16]. By contrast, CSF features in PD include α-synuclein (αSyn) levels which are often much lower than expected in normal health [23]. This diminished αSyn could be explained by passage of this protein from CSF into adjacent tissues [24,25], precipitates which could be worsened by slower circulation secondary to local inflammation. Oxidative stress is central to both cause and course of PD pathology, typified by mitochondrial dysfunction, excitotoxicity, and loss of dopaminergic action [26,27]. Since CSF biomarkers have discriminatory value for these neurogenerative conditions [11] this becomes a plausible route for cytokine normalization, enabling a directed therapeutic purpose, as proposed here.
3. Neural targets, intrathecal access
Effective therapy for neurodegenerative conditions, mass lesions, infections, or refractory pain relies on direct drug delivery to bypass the blood-brain barrier [28], explaining why many systemically administered agents never achieve therapeutic levels in brain tissue [29]. The current design extends prior work where drug delivery was via transdermal adhesive patch placed dorsally on the neck [30], by intranasal insufflation [31], or similar techniques [32,33]. Access to cerebrospinal and intraventricular space by intrathecal dosing [34] has the benefit of placing PLT cytokines in close proximity to glymphatic control sites most likely affected by oxidative stress, inflammation, or fibrosis [35,36,37].
The glymphatic system is a perivascular network for CSF transport connecting distally to the dural/meningeal lymphatic system. As the chief efflux channel for brain tissue [38], the glymphatic network clears metabolic products to prevent pathologic accretion in brain parenchyma and interstitial fluid [39]. Produced at a rate of 500-700 mL/d, total average CSF volume is ~140mL in healthy adults [40,41]. While there is broad consensus that CSF originates from choroid plexus in humans, anatomical exit routes beyond arachnoid granulations are less well characterized [42].
A standard intrathecal/lumbar catheter inserted at L3-L5 permits safe injection of volumes ranging from 0.5 to 5mL. While the concept of intrathecal therapy for neurodegenerative disease is underdeveloped, placement of blood products here is not: For spinal headache, needle access near a lumbar puncture site is often used to inject an autologous ‘blood patch’ to reduce symptoms and promote dural healing [43,44].
The 2009 priority paper outlining intrathecal dosing of conventional PRP in the management of AD and PD may be attributed to Shen et al [7]. Their insight was predicated not necessarily on anti-inflammatory properties (see Figure 1), but on the observed neurotrophic capacity of PLT growth factors which, individually or in concert, could ameliorate neurodegenerative diseases. Interventions to remove biochemical residue to assuage neurodegenerative loss gained momentum from animal research, where glymphatic dysfunction was noted after traumatic brain injury or stroke as well as animal models for normal aging and AD [45,46,47,48]. These findings helped frame workable ways to assure proper physiologic elimination of waste solutes [48,49]. Downshifting tau production would be another logical process to address AD pathology, and favorable results from a first-in-human Phase Ib clinical trial described a tau-targeting antisense oligonucleotide given intrathecally for this purpose [50]. While devices adapted to alleviate neurodegenerative symptoms are in preclinical development [51], using fresh autologous condensed PLT cytokines in this context represents an application not previously considered. Indeed, recent laboratory and clinical gains in PLT processing include better preparations of plasma cytokine samples and their delivery—including cell-free substrates following PLT subtraction. But might intrathecal use of an autologous PLT product have efficacy in AD or PD?
4. ‘Orthobiologic’ activity in AD/PD
AD and PD are characterized by dysregulated, excessive inflammation causing tissue damage, morbidity, and death. How specific brain tissues respond to these stresses is difficult to predict, although cellular changes observed in AD include neurofibrillary tangles/tau protein variants as signature features. These findings were originally considered the defect responsible for the AD phenotype, although further research has reexamined the disease sequence such that the observed tangles may be but one part of a compensatory response initiated by local inflammation, kinase activation, and subsequent tau phosphorylation [52]. Such neurofibrillary changes can confer protection against redox damage in neurons [53], explaining the apparent paradox of tangles occurring without disease where such neurons can function well for many years [52,53]. While there is no consensus on how these related structures lead to AD, there is closer agreement on inflammation being the inciting stress eventually culminating in neurodegenerative pathology.
PLTs enter the therapeutic roster perhaps best known for contributions to hemostasis, but this designation has since broadened to include serving other roles. Specifically, upon activation PLTs expel a suite of cytokines and soluble growth factors which communicate with varied targets to modulate inflammation, normalize cellular metabolism, and organize tissue healing [54]. Thus, to reestablish quiescence in a hyperinflammatory background, intrathecal PLT-derived cytokines would be a well-suited ‘orthobiologic’ [55,56,57,58]. Indeed, diffuse neural tissue inflammation [59] can be attenuated by hepatocyte growth factor (HGF) transforming growth factor-β (TGF-β), insulin-like growth factor 1 (IGF-1), interleukin (IL)-1 receptor antagonist, IL-4, IL-6, IL-10, IL-11, or IL-13 [55,60,61,62,63], all of which are components of the activated PLT releasate.
Nerve growth factor (NGF), brain-derived neurotrophic factor (BDNF), and neurotrophin-3 (NT3) are also discharged from activated PLTs and control neuron survival, development, and function via Trk-p75 NTR receptors, including suspension of programmed cell death [64,65,66]. First isolated in brain tissue, BDNF is now known to be stored in PLTs at concentrations 100 to 1000-fold greater than neurons and plays a major role in synaptic plasticity and neuron development [64]. Importantly for this clinical trial, these signals also promote progenitor cell differentiation to induce formation of replacement neurons—most notably involving the hippocampal dentate gyrus and subventricular zone [4,67]. While additional PLT releasate constituents (i.e., EGF, IGF-1, and TGF-β) exhibit neurotrophic potential, the widefield effects of these signals are only partially known (see Figure 2). Chen et al (2018) were among the first to describe intrathecal PRP placed into rat spinal cords where microglia and astrocyte activation was observed with PDGF-B and ICAM-1 expression [69]. Their intrathecal PRP protocol for SCI successfully recovered locomotor function with white matter sparing, and interestingly, ongoing treatment at reduced levels yielded therapeutic effects superior to single-dose PRP [69]. Remarkably, this axonal regeneration evoked by PLT growth factors persisted even after an extended interval between injury and treatment.
These encouraging results agree with those reported from others working in a cat model, where intrathecal PRP given 14d post-spinal cord injury produced significant benefits on hindlimb motor function, sometimes as early as d20. On MRI exam, lesion size was also significantly reduced after PRP treatment, while histopathology comparisons showed PRP fostered significant remyelination with improved structure and organization of white matter [8]. Brain atrophy in AD or PD may sometimes overshadow equally important spinal cord involvement. As the spinal cord sends and receives sensorimotor signals involving cortex and periphery, these motor pathways often undergo abnormal rewiring even before cognitive decline [70]. This would explain why fine motor impairment and deteriorating handwriting are common preludes to dementia in AD. Thus, degenerative atrophy may extend beyond hippocampus and temporal lobes with AD spinal cord changes akin to spinal atrophy present in multiple sclerosis [71,72]. Notably, intrathecal PRP recovered functional recovery, remyelination, oligodendrogenesis, and lowered inflammation in an animal model for multiple sclerosis [73].
As PLT cytokines also regulate heat shock protein expression by oligodendrocytes in human glial cell cultures and other fibroblasts [74,75] when acting near abnormal brain tissue, they may also influence local unfolded protein responses [76]. For example, heat shock proteins under cytokine control drives apoptosis to deactivate abnormal cells, slowing progress of inflammation and associated neurodegeneration [77]. Even for mechanical hyperalgesia and induced inflammation, intrathecal PRP tested in a mammal model gave a post-treatment response of higher pain threshold, inhibited astrocyte activation, diminished aerobic glycolysis, and lower PKM2 expression [78].
5. Conclusions
As with all early investigations, it is impossible to predict if intrathecal autologous condensed plasma cytokines/PRP can become a disease-modifying agent for AD or PD. Given the long history of prior interventions aspiring to manage these conditions, the odds are not especially favorable. Most PRP applications tend to support tissue regeneration, although some authors are more reserved [79,80]. Notwithstanding the growing interest in PRP and its derivatives in new domains [81], nonuniform sample preparations [82,83] have made randomized controlled trials difficult to standardize and almost impossible to interpret. While any diffuse hyperinflammation corrected by PLT cytokine use is welcome, numerous CNS signal pathways are impacted upon PLT activation to facilitate tissue repair, angiogenesis and neurogenesis [84]. This work therefore expands prior descriptions of PRP treatment for CNS disorders [7] given its recuperative effects in SCI and peripheral nerve damage documented elsewhere [68,85]. This approach also extends earlier PRP use in kidney disease, which balanced difficulties of treating an encapsulated solid organ with the need to dose PRP locally [86]. Because a generic PRP-based clinical trial entails no FDA new drug clearance and requires few resources to establish the study program, the project joins the AD/PD research discourse as an outlier. Under assessment by an institutional review board, repurposing PLT-derived cytokines represents a readily available, relatively inexpensive, low risk, and underutilized therapy for intrathecal use in AD/PD. This concept should contribute to AD/PD treatment options by opening renewed appreciation for this therapeutic paradigm.
Conflicts of Interest
The author has been awarded U.S. Trademark #88505430 for specified process and method using autologous platelet cytokines.
References
- Moutinho, S. The long road to a cure for Alzheimer's disease is paved with failures. Nat Med 2022;28(11):2228-31. [CrossRef]
- Mari Z, Mestre TA. The disease modification conundrum in Parkinson's disease: Failures and hopes. Front Aging Neurosci 2022;14:810860. [CrossRef]
- Dorsey ER, Sherer T, Okun MS, Bloem BR. The emerging evidence of the Parkinson pandemic. J Parkinsons Dis 2018;8:S3–S8. [CrossRef]
- Triaca V, Imbimbo BP, Nisticò R. Editorial: Neurotrophins biodelivery to CNS: Innovative approaches for disease-modifying therapy. Front Neurosci 2022;16:916563. [CrossRef]
- Cummings JL, Goldman DP, Simmons-Stern NR, Ponton E. The costs of developing treatments for Alzheimer's disease: A retrospective exploration. Alzheimers Dement 2022;18(3):469-77. [CrossRef]
- Swift MJ, Greene JA, Welch ZR. Concentration of neurotransmitter and neurotrophic factors in platelet-rich plasma. Blood 2006;108(11):3914. [CrossRef]
- Shen YX, Fan ZH, Zhao JG, Zhang P. The application of platelet-rich plasma may be a novel treatment for central nervous system diseases. Med Hypotheses 2009;73(6):1038-40. [CrossRef]
- Farid MF, Abouelela YS, Yasin NAE, Mousa MR, Ibrahim MA, Prince A, et al. A novel cell-free intrathecal approach with PRP for the treatment of spinal cord multiple sclerosis in cats. Inflamm Regen 2022;42(1):45. [CrossRef]
- U.S. National Library of Medicine/NIH. Clinical trial registry (clinicaltrials.gov) https://clinicaltrials.gov/ct2/results?cond=Neurodegenerative+Diseases&term=intrathecal%3B+platelet-rich+plasma&cntry=&state=&city=&dist=&Search=Search [site accessed 1 June 2023].
- Domínguez-Fernández C, Egiguren-Ortiz J, Razquin J, Gómez-Galán M, De Las Heras-García L, Paredes-Rodríguez E, et al. Review of technological challenges in personalised medicine and early diagnosis of neurodegenerative disorders. Int J Mol Sci 2023;24(4):3321. [CrossRef]
- Lancini E, Haag L, Bartl F, Rühling M, Ashton NJ, Zetterberg H, et al. Cerebrospinal fluid and positron-emission tomography biomarkers for noradrenergic dysfunction in neurodegenerative diseases: A systematic review and meta-analysis. Brain Commun 2023;5(3):fcad085. [CrossRef]
- Mawuenyega KG, Sigurdson W, Ovod V, Munsell L, Kasten T, Morris JC, et al. Decreased clearance of CNS beta-amyloid in Alzheimer's disease. Science 2010;330(6012):1774. [CrossRef]
- Jessen NA, Munk AS, Lundgaard I, Nedergaard M. The glymphatic system: A beginner's guide. Neurochem Res 2015;40(12):2583-99. [CrossRef]
- Tadayon E, Pascual-Leone A, Press D, Santarnecchi E; Alzheimer's Disease Neuroimaging Initiative. Choroid plexus volume is associated with levels of CSF proteins: Relevance for Alzheimer's and Parkinson's disease. Neurobiol Aging 2020;89:108-17. [CrossRef]
- Sochocka M, Diniz BS, Leszek J. Inflammatory response in the CNS: Friend or foe? Mol Neurobiol 2017;54:8071e8089. [CrossRef]
- Taipa R, das Neves SP, Sousa AL, Fernandes J, Pinto C, Correia AP, et al. Proinflammatory and anti-inflammatory cytokines in the CSF of patients with Alzheimer's disease and their correlation with cognitive decline. Neurobiol Aging 2019;76:125-32. [CrossRef]
- Bulling A, Brucker C, Berg U, Gratzl M, Mayerhofer A. Identification of voltage-activated Na+ and K+ channels in human steroid-secreting ovarian cells. Ann NY Acad Sci 1999;868:77-9. [CrossRef]
- Sassoli C, Garella R, Chellini F, Tani A, Pavan P, Bambi F, et al. Platelet-rich plasma affects gap junctional features in myofibroblasts in vitro via vascular endothelial growth factor (VEGF)-A/VEGF receptor. Exp Physiol 2022;107(2):106-21. [CrossRef]
- Ozawa Y, Toda E, Kawashima H, Homma K, Osada H, Nagai N, et al. Aquaporin-4 suppresses neural hyperactivity and synaptic fatigue and finetunes neurotransmission to regulate visual function in the mouse retina. Mol Neurobiol 2019;56(12):8124-35. [CrossRef]
- Haj-Yasein NN, Jensen V, Østby I, Omholt SW, Voipio J, Kaila K, et al. Aquaporin-4 regulates extracellular space volume dynamics during high-frequency synaptic stimulation: A gene deletion study in mouse hippocampus. Glia 2012;60(6):867-74. [CrossRef]
- Xu Y, Wang X, Liu W, Lu W. Thrombin-activated platelet-rich plasma enhances osteogenic differentiation of human periodontal ligament stem cells by activating SIRT1-mediated autophagy. Eur J Med Res 2021;26(1):105. [CrossRef]
- Sills ES, Rickers NS, Li X, Palermo GD. First data on in vitro fertilization and blastocyst formation after intraovarian injection of calcium gluconate-activated autologous platelet rich plasma. Gynecol Endocrinol 2018;34(9):756-60. [CrossRef]
- Kang JH, Irwin DJ, Chen-Plotkin AS, Siderowf A, Caspell C, Coffey CS, et al. Association of cerebrospinal fluid β-amyloid 1-42, T-tau, P-tau181, and α-synuclein levels with clinical features of drug-naive patients with early Parkinson disease. JAMA Neurol 2013;70(10):1277-87. [CrossRef]
- Mollenhauer B, Locascio JJ, Schulz-Schaeffer W, Sixel-Döring F, Trenkwalder C, Schlossmacher MG. α-Synuclein and tau concentrations in cerebrospinal fluid of patients presenting with parkinsonism: A cohort study. Lancet Neurol 2011;10(3):230-40. [CrossRef]
- Hall S, Surova Y, Öhrfelt A, Zetterberg H, Lindqvist D, Hansson O. CSF biomarkers and clinical progression of Parkinson disease. Neurology 2015;84(1):57-63. [CrossRef]
- Chakrabarti S, Bisaglia M. Oxidative stress and neuroinflammation in Parkinson's disease: The role of dopamine oxidation products. Antioxidants (Basel) 2023;12(4):955. [CrossRef]
- Huang P, Zhang LY, Tan YY, Chen SD. Links between COVID-19 and Parkinson's disease/Alzheimer's disease: Reciprocal impacts, medical care strategies and underlying mechanisms. Transl Neurodegener 2023;12(1):5. [CrossRef]
- Yi X, Manickam DS, Brynskikh A, Kabanov AV. Agile delivery of protein therapeutics to CNS. J Control Release 2014;190:637-63. [CrossRef]
- Xie H, Chung JK, Mascelli MA, McCauley TG. Pharmacokinetics and bioavailability of a therapeutic enzyme (idursulfase) in cynomolgus monkeys after intrathecal and intravenous administration. PLoS One 2015;10(4):e0122453. [CrossRef]
- Lehrer S, Rheinstein PH. Transspinal delivery of drugs by transdermal patch back-of-neck for Alzheimer's disease: a new route of administration. Discov Med 2019;27(146):37-43. https://pubmed.ncbi.nlm.nih.gov/30721650/.
- Lehrer, S. Nasal NSAIDs for Alzheimer's disease. Am J Alzheimers Dis Other Demen 2014;29(5):401-3. [CrossRef]
- Slavc I, Cohen-Pfeffer JL, Gururangan S, Krauser J, Lim DA, Maldaun M, et al. Best practices for use of intracerebroventricular drug delivery devices. Mol Genet Metab 2018;124(3):184-8. [CrossRef]
- Muschol N, Koehn A, von Cossel K, Okur I, Ezgu F, Harmatz P, et al. A phase I/II study on intracerebroventricular tralesinidase-alfa in patients with Sanfilippo syndrome type B. J Clin Invest 2023;133(2):e165076. [CrossRef]
- Manuel MG, Tamba BI, Leclere M, Mabrouk M, Schreiner TG, Ciobanu R, et al. Intrathecal pseudodelivery of drugs in the therapy of neurodegenerative diseases: Rationale, basis and potential applications. Pharmaceutics 2023;15(3):768. [CrossRef]
- Prineas JW, Parratt JD, Kirwan PD. Fibrosis of the choroid plexus filtration membrane. J Neuropathol Exp Neurol 2016;75(9):855-67. [CrossRef]
- Hsu SJ, Zhang C, Jeong J, Lee SI, McConnell M, Utsumi T, et al. Enhanced meningeal lymphatic drainage ameliorates neuroinflammation and hepatic encephalopathy in cirrhotic rats. Gastroenterology 2021;160(4):1315-29.e13. [CrossRef]
- Buccellato FR, D'Anca M, Serpente M, Arighi A, Galimberti D. The role of glymphatic system in Alzheimer's and Parkinson's Disease pathogenesis. Biomedicines 2022;10(9):2261. [CrossRef]
- Nedergaard, M. Neuroscience. Garbage truck of the brain. Science 2013;340(6140):1529-30. [CrossRef]
- Sepehrinezhad A, Stolze Larsen F, Ashayeri Ahmadabad R, Shahbazi A, et al. The glymphatic system may play a vital role in the pathogenesis of hepatic encephalopathy: A narrative review. Cells 2023;12(7):979. [CrossRef]
- Seehusen DA, Reeves MM, Fomin DA. Cerebrospinal fluid analysis. Am Fam Physician 2003;68(6):1103-9. https://www.aafp.org/pubs/afp/issues/2003/0915/p1103.html.
- Hrishi AP, Sethuraman M. Cerebrospinal fluid (CSF) analysis and interpretation in neurocritical care for acute neurological conditions. Indian J Crit Care Med 2019;23(Suppl 2):S115-9. [CrossRef]
- Astara K, Pournara C, de Natale ER, Wilson H, Vavougios GD, Lappas AS, et al. A novel conceptual framework for the functionality of the glymphatic system. J Neurophysiol 2023;129(5):1228-36. [CrossRef]
- Epstein NE, Agulnick MA. Perspective: Early direct repair of recurrent postoperative cerebrospinal fluid leaks: No good evidence epidural blood patches work. Surg Neurol Int 2023;14:120. [CrossRef]
- Beckman SP, Proctor C, Toms JB. Management of recurrent post-myelography lumbar pseudomeningocele with epidural blood patch. Cureus 2023;15(2):e35600. [CrossRef]
- Peng W, Achariyar TM, Li B, Liao Y, Mestre H, Hitomi E, et al. Suppression of glymphatic fluid transport in a mouse model of Alzheimer's disease. Neurobiol Dis 2016;93:215-25. [CrossRef]
- Rasmussen MK, Mestre H, Nedergaard M. The glymphatic pathway in neurological disorders. Lancet Neurol 2018;17(11):1016-24. [CrossRef]
- Jiang H, Wei H, Zhou Y, Xiao X, Zhou C, Ji X. Overview of the meningeal lymphatic vessels in aging and central nervous system disorders. Cell Biosci 2022;12(1):202. [CrossRef]
- Butler T, Zhou L, Ozsahin I, Wang XH, Garetti J, Zetterberg H, et al. Glymphatic clearance estimated using diffusion tensor imaging along perivascular spaces is reduced after traumatic brain injury and correlates with plasma neurofilament light, a biomarker of injury severity. Brain Commun 2023;5(3):fcad134. [CrossRef]
- Benveniste H, Liu X, Koundal S, Sanggaard S, Lee H, Wardlaw J. The glymphatic system and waste clearance with brain aging: A review. Gerontology 2019;65(2):106-19. [CrossRef]
- Mummery CJ, Börjesson-Hanson A, Blackburn DJ, Vijverberg EGB, De Deyn PP, Ducharme S, et al. Tau-targeting antisense oligonucleotide MAPTRx in mild Alzheimer's disease: A phase 1b, randomized, placebo-controlled trial. Nat Med 2023 Apr 24. [CrossRef]
- BioMarin Pharmaceutical Inc. NIH registered clinical trial NCT02754076—A treatment study of Mucopolysaccharidosis Type IIIB: https://clinicaltrials.gov/ct2/show/NCT02754076 [site accessed 1 June 2023].
- Bonda DJ, Castellani RJ, Zhu X, Nunomura A, Lee HG, Perry G, et al. A novel perspective on tau in Alzheimer's disease. Curr Alzheimer Res 2011;8(6):639-42. [CrossRef]
- Lee HG, Perry G, Moreira PI, Garrett MR, Liu Q, Zhu X, et al. Tau phosphorylation in Alzheimer's disease: pathogen or protector? Trends Mol Med 2005;11(4):164-9. [CrossRef]
- Scherlinger M, Richez C, Tsokos GC, Boilard E, Blanco P. The role of platelets in immune-mediated inflammatory diseases. Nat Rev Immunol 2023:1-16. [CrossRef]
- Abdul Ameer LA, Raheem ZJ, Abdulrazaq SS, Ali BG, Nasser MM, Khairi AWA. The anti-inflammatory effect of the platelet-rich plasma in the periodontal pocket. Eur J Dent 2018;12(4):528-31. [CrossRef]
- Kumar V, Talwar J, Rustagi A, Krishna LG, Sharma VK. Comparison of clinical and functional outcomes after platelet-rich plasma injection and corticosteroid injection for the treatment of de Quervain's tenosynovitis. J Wrist Surg 2022;12(2):135-42. [CrossRef]
- Rodeo, SA. Orthobiologics: Current status in 2023 and future outlook. J Am Acad Orthop Surg 2023;31(12):604-13. [CrossRef]
- Wongjarupong A, Pairuchvej S, Laohapornsvan P, Kotheeranurak V, Jitpakdee K, Yeekian C, et al. Platelet-rich plasma epidural injection an emerging strategy in lumbar disc herniation: A randomized controlled trial. BMC Musculoskelet Disord 2023;24(1):335. [CrossRef]
- Tarkowski E, Andreasen N, Tarkowski A, Blennow K. Intrathecal inflammation precedes development of Alzheimer's disease. J Neurol Neurosurg Psychiatry 2003;74(9):1200-5. [CrossRef]
- Opal SM, DePalo VA. Anti-inflammatory cytokines. Chest 2000;117(4):1162-72. [CrossRef]
- Zhang J, Middleton KK, Fu FH, Im HJ, Wang JH. HGF mediates the anti-inflammatory effects of PRP on injured tendons. PLoS One 2013;8(6):e67303. [CrossRef]
- Southworth TM, Naveen NB, Tauro TM, Leong NL, Cole BJ. The use of platelet-rich plasma in symptomatic knee osteoarthritis. J Knee Surg 2019;32(1):37-45. [CrossRef]
- Ziegler CG, Van Sloun R, Gonzalez S, Whitney KE, DePhillipo NN, Kennedy MI, et al. Characterization of growth factors, cytokines, and chemokines in bone marrow concentrate and platelet-rich plasma: A prospective analysis. Am J Sports Med 2019;47(9):2174-87. [CrossRef]
- Boukhatem I, Fleury S, Welman M, Le Blanc J, Thys C, Freson K, et al. The brain-derived neurotrophic factor prompts platelet aggregation and secretion. Blood Adv 2021;5(18):3568-80. [CrossRef]
- Mitsiadis TA, Pagella P. Expression of nerve growth factor (NGF), TrkA, and p75(NTR) in developing human fetal teeth. Front Physiol 2016;7:338. [CrossRef]
- Burk, K. The endocytosis, trafficking, sorting and signaling of neurotrophic receptors. Prog Mol Biol Transl Sci 2023;196:141-65. [CrossRef]
- Park H, Poo MM. Neurotrophin regulation of neural circuit development and function. Nat Rev Neurosci 2013;14:7-23. [CrossRef]
- Su LN, Song XQ, Wei HP, Yin HF. Identification of neuron-related genes for cell therapy of neurological disorders by network analysis. J Zhejiang Univ Sci B 2017;18(2):172-82. [CrossRef]
- Chen NF, Sung CS, Wen ZH, Chen CH, Feng CW, Hung HC, et al. Therapeutic effect of platelet-rich plasma in rat spinal cord injuries. Front Neurosci 2018;12:252. [CrossRef]
- Fu L, Liu L, Zhang J, Xu B, Fan Y, Tian J. Brain network alterations in Alzheimer's disease identified by early-phase PIB-PET. Contrast Media Mol Imaging 2018;2018:6830105. [CrossRef]
- Azodi S, Nair G, Enose-Akahata Y, Charlip E, Vellucci A, Cortese I, et al. Imaging spinal cord atrophy in progressive myelopathies: HTLV-I-associated neurological disease (HAM/TSP) and multiple sclerosis. Ann Neurol 2017;82(5):719-28. [CrossRef]
- Lorenzi RM, Palesi F, Castellazzi G, Vitali P, Anzalone N, Bernini S, et al. Unsuspected Involvement of Spinal Cord in Alzheimer Disease. Front Cell Neurosci 2020;14:6. [CrossRef]
- Borhani-Haghighi M, Mohamadi Y. The therapeutic effect of platelet-rich plasma on the experimental autoimmune encephalomyelitis mice. J Neuroimmunol 2019;333:476958. [CrossRef]
- D'Souza SD, Antel JP, Freedman MS. Cytokine induction of heat shock protein expression in human oligodendrocytes: An interleukin-1-mediated mechanism. J Neuroimmunol 1994;50(1):17-24. [CrossRef]
- Hasan RJ, Ameredes BT, Calhoun WJ. Cytokine mediated regulation of heat shock protein 90 (Hsp90) and steroid receptor function. J Allergy Clin Immunol 2008;121(2 Suppl 1):S120. [CrossRef]
- Tao SC, Yuan T, Rui BY, Zhu ZZ, Guo SC, Zhang CQ. Exosomes derived from human platelet-rich plasma prevent apoptosis induced by glucocorticoid-associated endoplasmic reticulum stress in rat osteonecrosis of the femoral head via the Akt/Bad/Bcl-2 signal pathway. Theranostics 2017;7(3):733-50. [CrossRef]
- Terrab L, Wipf P. Hsp70 and the unfolded protein response as a challenging drug target and an Inspiration for probe molecule development. ACS Med Chem Lett 2020;11(3):232-6. [CrossRef]
- Wei X, Jin XH, Meng XW, Hua J, Ji FH, Wang LN, et al. Platelet-rich plasma improves chronic inflammatory pain by inhibiting PKM2-mediated aerobic glycolysis in astrocytes. Ann Transl Med 2020;8(21):1456. [CrossRef]
- Filardo G, Kon E. PRP: More words than facts. Knee Surg Sports Traumatol Arthrosc 2012;20(9):1655-6. [CrossRef]
- Hamid MS, Yusof A, Mohamed Ali MR. Platelet-rich plasma (PRP) for acute muscle injury: A systematic review. PLoS One 2014;9(2):e90538. [CrossRef]
- Sills ES, Wood SH. Epigenetics, ovarian cell plasticity, and platelet-rich plasma: Mechanistic theories. Reprod Fertil 2022;3(4):C44-C51. [CrossRef]
- Andia I, Maffulli N. A contemporary view of platelet-rich plasma therapies: Moving toward refined clinical protocols and precise indications. Regen Med 2018;13(6):717-28. [CrossRef]
- Rickers NS, Sills ES. Is autologous platelet activation the key step in ovarian therapy for fertility recovery and menopause reversal? Biomedicine (Taipei) 2022;12(4):1-8. [CrossRef]
- Padilla S, Orive G, Anitua E. Shedding light on biosafety of platelet rich plasma. Expert Opin Biol Ther 2017;17(8):1047-8. [CrossRef]
- Sánchez M, Anitua E, Delgado D, Sanchez P, Prado R, Orive G, et al. Platelet-rich plasma, a source of autologous growth factors and biomimetic scaffold for peripheral nerve regeneration. Expert Opin Biol Ther 2017;17(2):197-212. [CrossRef]
- Martín-Solé O, Rodó J, García-Aparicio L, Blanch J, Cusí V, Albert A. Effects of platelet-rich plasma on a model of renal ischemia-reperfusion in rats. PLoS One 2016;11(8):e0160703. [CrossRef]
Figure 1.
Anti-inflammatory sequence for processed platelet (PLT) rich plasma and its soluble mediators (blue), discharged after thrombin (T) activation. After PLT subtraction, these cytokines include: Brain-derived neurotrophic factor (BDNF), supports neuron survival and induces differentiation of de novo neurons and synapses; Epidermal growth factor (EGF), a central element in cellular proliferation, differentiation, and survival; Fibroblast growth factor (bFGF), a mediator with broad mitogenic and survival actions; Hepatocyte growth factor (HGF), stimulates mitogenesis, cell motility, and matrix invasion with a key role in angiogenesis and tissue regeneration; Insulin like growth factors (IGFs) are required for cell stimulation and response to local microclimate; Interleukin-1β (IL-1β), a central inflammatory mediator involved in cell proliferation, differentiation, and apoptosis; Interleukin-2 (IL-2), an inducer of T-helper 1 (Th1) and Th2 cell differentiation and antagonist to inflammatory Th17 cells; Interleukin-6 (IL-6), a metabolic regulator and promoter of hypothalamic PGE2; Interleukin-8 (IL-8, or ‘neutrophil chemotactic factor’) coordinates local angiogenesis; Interleukin-10 (IL-10) suppresses Th1 cytokines and MHC class II antigens and regulates the JAK-STAT signaling network; Ligand of CD40 (CD-40L), an inflammatory organizer of PLTs, leukocytes, and dendrites; Macrophage inflammatory protein 1-alpha (MIP-1α), a conditional trigger for cell migration, survival, and proliferation; Platelet derived growth factor (PDGF), modulates mitogenesis and mesenchymal proliferation; Platelet factor 4 (PF4), a chemotactic protein involved in PLT aggregation; Regulated after Activation of Normal T-cell Expressed and Secreted (RANTES), a monocyte attractant; Transforming growth factor beta (TGF-β), an activator of multiple downstream substrates involved in tissue repair; Tumor necrosis factor (TNF), highly diverse actions with multiple cross-talk nodes balancing cell proliferation and apoptosis; and Vascular endothelial growth factor (VEGF), a promoter of vascular development for improved perfusion. In addition to recorded changes in selected CSF parameters, post-program serum C-reactive protein (CRP) is measured to estimate systemic anti-inflammatory effect.
Figure 1.
Anti-inflammatory sequence for processed platelet (PLT) rich plasma and its soluble mediators (blue), discharged after thrombin (T) activation. After PLT subtraction, these cytokines include: Brain-derived neurotrophic factor (BDNF), supports neuron survival and induces differentiation of de novo neurons and synapses; Epidermal growth factor (EGF), a central element in cellular proliferation, differentiation, and survival; Fibroblast growth factor (bFGF), a mediator with broad mitogenic and survival actions; Hepatocyte growth factor (HGF), stimulates mitogenesis, cell motility, and matrix invasion with a key role in angiogenesis and tissue regeneration; Insulin like growth factors (IGFs) are required for cell stimulation and response to local microclimate; Interleukin-1β (IL-1β), a central inflammatory mediator involved in cell proliferation, differentiation, and apoptosis; Interleukin-2 (IL-2), an inducer of T-helper 1 (Th1) and Th2 cell differentiation and antagonist to inflammatory Th17 cells; Interleukin-6 (IL-6), a metabolic regulator and promoter of hypothalamic PGE2; Interleukin-8 (IL-8, or ‘neutrophil chemotactic factor’) coordinates local angiogenesis; Interleukin-10 (IL-10) suppresses Th1 cytokines and MHC class II antigens and regulates the JAK-STAT signaling network; Ligand of CD40 (CD-40L), an inflammatory organizer of PLTs, leukocytes, and dendrites; Macrophage inflammatory protein 1-alpha (MIP-1α), a conditional trigger for cell migration, survival, and proliferation; Platelet derived growth factor (PDGF), modulates mitogenesis and mesenchymal proliferation; Platelet factor 4 (PF4), a chemotactic protein involved in PLT aggregation; Regulated after Activation of Normal T-cell Expressed and Secreted (RANTES), a monocyte attractant; Transforming growth factor beta (TGF-β), an activator of multiple downstream substrates involved in tissue repair; Tumor necrosis factor (TNF), highly diverse actions with multiple cross-talk nodes balancing cell proliferation and apoptosis; and Vascular endothelial growth factor (VEGF), a promoter of vascular development for improved perfusion. In addition to recorded changes in selected CSF parameters, post-program serum C-reactive protein (CRP) is measured to estimate systemic anti-inflammatory effect.
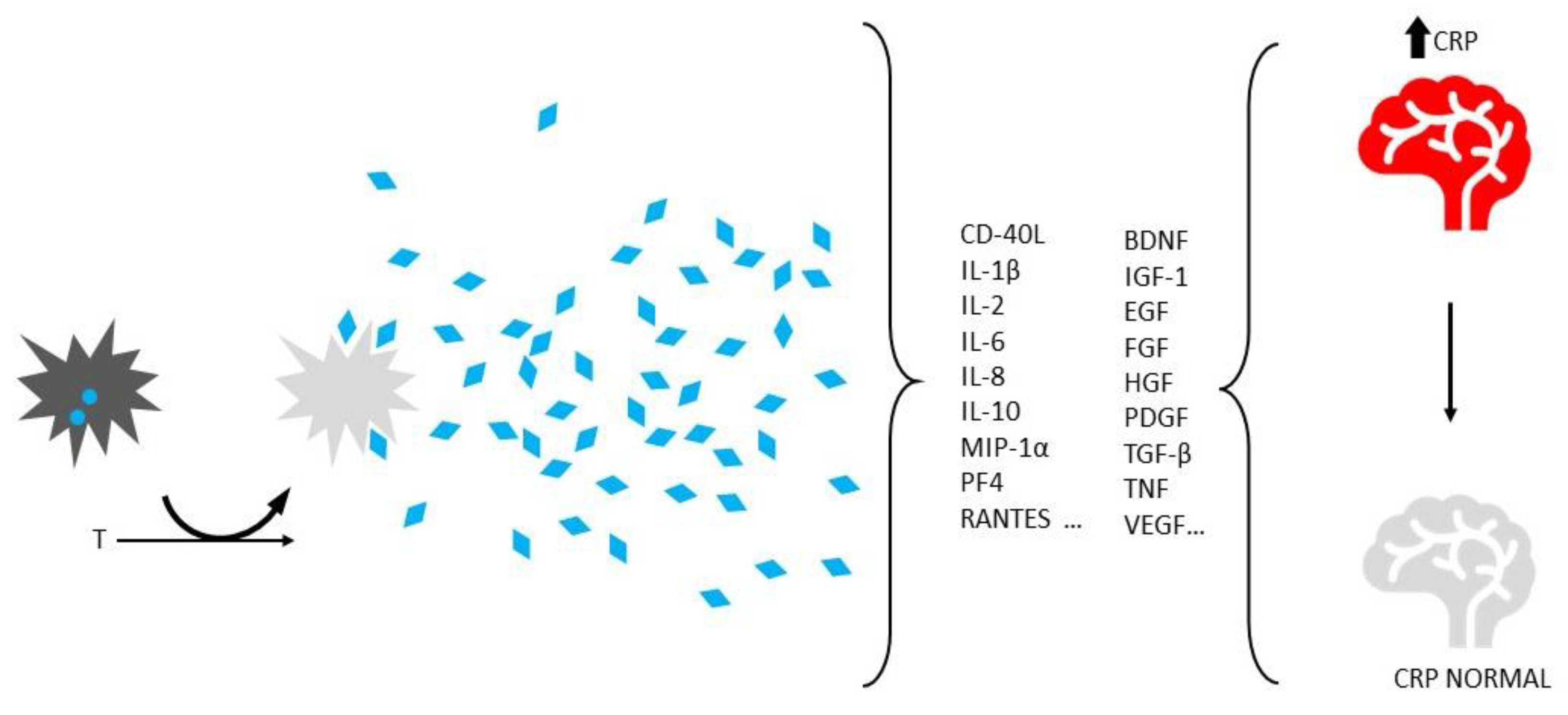
Figure 2.
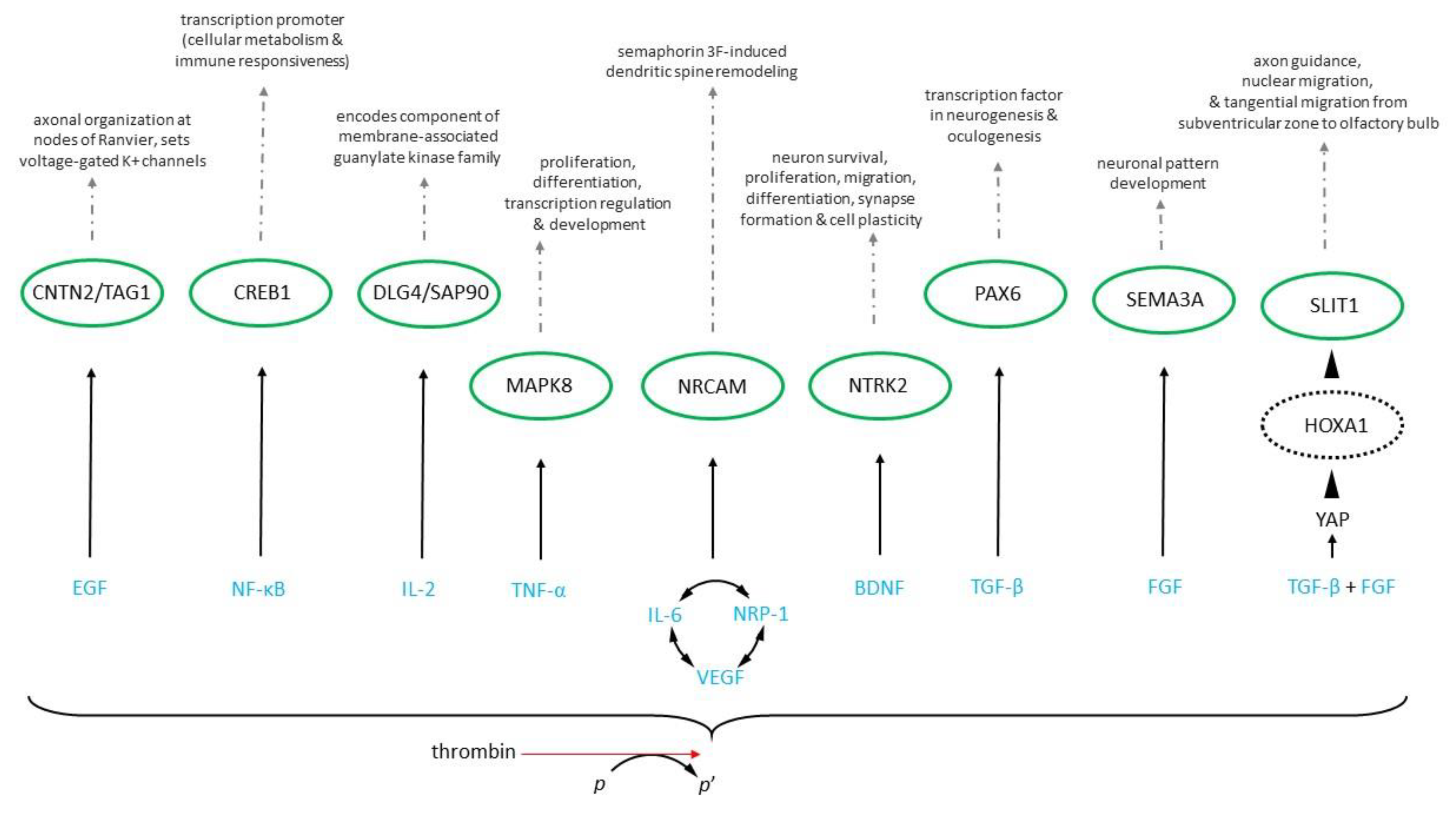
Gene ontology functional schematic from representative cytokines (blue) discharged after thrombin activation of autologous platelets (p, p’) shown with modulated intermediate (dashed) and hub gene (green) targets associated with neuronal differentiation and downstream tissue effects (top). Where: CNTN2 = Contactin-2, CREB = cAMP responsive element binding protein-1, DLG4 = Discs large MAGUK scaffold protein-4, HOXA1 = Homeobox A1, MAPK8 = Mitogen-activated protein kinase-8, NRCAM = Neuronal cell adhesion molecule, NTRK2 = Neurotrophic receptor tyrosine kinase-2, PAX6 = Paired box protein-6 (aniridia type II protein), SEMA3A = Semaphorin-3A, SLIT1 = Slit guidance ligand-1, YAP = Yes-associated protein. Modified from [68]. Condensed plasma cytokines: BDNF = Brain derived neurotrophic factor, EGF = Epidermal growth factor, FGF = Fibroblast growth factor, IL-2 = Interleukin-2, IL-6 = Interleukin-6, NF-kB = Nuclear factor kappa-light-chain-enhancer of activated B cells, NRP-1 = Neuropilin-1, TGF-β = Transforming growth factor-β, TNF-α = Tumor necrosis factor-alpha, VEGF = Vascular endothelial growth factor.
Figure 2.
Gene ontology functional schematic from representative cytokines (blue) discharged after thrombin activation of autologous platelets (p, p’) shown with modulated intermediate (dashed) and hub gene (green) targets associated with neuronal differentiation and downstream tissue effects (top). Where: CNTN2 = Contactin-2, CREB = cAMP responsive element binding protein-1, DLG4 = Discs large MAGUK scaffold protein-4, HOXA1 = Homeobox A1, MAPK8 = Mitogen-activated protein kinase-8, NRCAM = Neuronal cell adhesion molecule, NTRK2 = Neurotrophic receptor tyrosine kinase-2, PAX6 = Paired box protein-6 (aniridia type II protein), SEMA3A = Semaphorin-3A, SLIT1 = Slit guidance ligand-1, YAP = Yes-associated protein. Modified from [68]. Condensed plasma cytokines: BDNF = Brain derived neurotrophic factor, EGF = Epidermal growth factor, FGF = Fibroblast growth factor, IL-2 = Interleukin-2, IL-6 = Interleukin-6, NF-kB = Nuclear factor kappa-light-chain-enhancer of activated B cells, NRP-1 = Neuropilin-1, TGF-β = Transforming growth factor-β, TNF-α = Tumor necrosis factor-alpha, VEGF = Vascular endothelial growth factor.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



