
Submitted:
05 June 2023
Posted:
05 June 2023
You are already at the latest version
Abstract
Streptococcus intermedius is frequently associated with brain and liver abscesses, while pleuropulmonary infections are considered rarer. Even less frequent is the association of lung and brain abscess due to this agent with left heart endocarditis. We describe the case of a 40-year-old man with a brain abscess due to S. intermedius and concomitant lung abscess and aortic native valve endocarditis. He was treated with surgical drainage of the brain abscess and a 4-week course of intravenous ceftriaxone, followed by oral amoxicillin/clavulanate, obtaining healing of the lesions without relapse of the infection.
Keywords:
Streptococcus intermedius
; brain abscess
; lung abscess
; endocarditis
1. Introduction
Streptococcus intermedius is a gram positive, catalase-negative coccus belonging to the Streptococcus anginosus group (SAG), which is often referred to as the Streptococcus milleri group, including S. intermedius, S. anginosus, and S. constellatus. SAG bacteria have been detected in the mouth, the gastrointestinal and upper respiratory tract, and the vagina [1,2].
Streptococcus intermedius is frequently associated with brain and liver abscesses, while pleuropulmonary infections are considered rarer [3]. Even less frequent is the association of lung and brain abscess due to this agent with left heart endocarditis. We describe the case of a 40-year-old man with a brain abscess due to S. intermedius and concomitant lung abscess and aortic native valve endocarditis.
2. Case presentation
The patient was a 40-year-old male of Egyptian origin, residing in Italy for about 15 years. He denied allergies, previous hospitalizations, or surgical interventions. For about 20 days he experienced persistent cough, asthenia, intermittent fever, intense headache, and worsening back and lumbar pain partially responsive to therapy with paracetamol and non-steroidal anti-inflammatory drugs. Due to the worsening of these symptoms, he went to the Emergency Department (ED) of a peripheral Hospital, where his vital signs were as follows: blood pressure 140/80 mmHg, heart rate 105 bpm, respiratory rate 17 breaths per minute, oxygen saturation 97% in room air, body temperature 38°C, and Glasgow Coma Scale 15. There were no focal neurological deficits, no meningeal signs, no positive covid antigen tests. Blood tests showed neutrophilic leukocytosis (white blood cells 12,900/mmc; neutrophils 77.7%) and a slight increase in C-reactive protein (1.2 mg/dL). A non-contrast cranial computed tomography (CT) scan revealed a necrotic-colliquative expansive lesion measuring 36 mm in diameter in the left subcortical occipital area, with an associated perilesional oedema. The patient started treatment with ceftriaxone 2 g intravenously (IV) and methylprednisolone 4 mg.
He was then transferred to the ED of a second level Center with Neurosurgical facilities, where a contrast-enhanced chest CT scan showed a pleural-based consolidative lesion in the left lung lower lobe measuring 63 mm in diameter, associated with a 16 mm internal cavity (Figure 1). The patient was admitted to the Oncologic Pneumology department. After an Infectious Diseases consultation, the antibiotic therapy was modified to include meropenem 2 g three times/day (TID) and vancomycin 500 mg four times/day. QuantiFERON-TB (QTF) Gold Plus and blood cultures resulted negative. A nuclear magnetic resonance (NMR) scan (Figure 2) confirmed the abscess nature of the brain lesion and revealed its communication with the trigone of the left lateral ventricle, along with perilesional oedema.
He was then transferred to the Neurosurgery department, where a bronchial aspiration was performed for direct microscopic examination, culture and DNA testing for Mycobacterium tuberculosis complex, non-tuberculous mycobacteria, and Aspergillus. A full spine NMR scan was also conducted but resulted negative for focal lesions. Pending microbiologic results, considering the possible tubercolar etiology of the disease, empirical combination therapy with linezolid 600 mg two times/daily, meropenem 2 g TID, rifampicin 600 mg once daily (QD), isoniazid 300 mg QD, ethambutol 1200 mg QD, levofloxacin 750 mg QD, and dexamethasone 6 mg TID was initiated.
Subsequently, a left occipital parasagittal craniotomy procedure was performed, resulting in drainage of the abscess and partial removal of the abscess capsule, along with sampling of biological material. The culture of the cerebral abscess samples resulted positive for Streptococcus intermedius sensitive to ampicillin, ceftriaxone, clindamycin, teicoplanin, and vancomycin. Thus, the patient started targeted therapy with ceftriaxone 2 g IV BID and dexamethasone 12 mg IV BID. Following the QTF and PCR results, which tested negative for mycobacteria and fungi, the previous anti-tubercular therapy was discontinued.
The patient was then transferred to our Infectious Diseases Center in stable conditions and afebrile. During the hospitalization, a transesophageal color Doppler echocardiography revealed aortic valve thickening with a prolapsing attitude of the right cusp, and a nodular hyperechogenic image between the right and left cusps, along with mild valve insufficiency. Due to the presence of multiple carious lesions, a dental CT scan was performed, showing periapical bone resorption at tooth 14 in the upper arch and a large carious lesion of tooth 36, accompanied by an inflammatory periapical bone resorption area.
The patient received a four-week course of ceftriaxone 2 g IV BID, resulting in progressive improvement of his clinical, laboratory, and radiological findings (Figure 3). He was discharged in good general conditions, with instructions to continue oral therapy with amoxicillin/clavulanate 875 mg TID for further 10 days and a program of cardiological, neurosurgical and dental outpatient visits. After a three-month follow-up the patient is still in good health with no signs of infection relapse.
3. Discussion
Pleuropulmonary infections due to Streptococcus intermedius are considered uncommon [4]; however, in recent years their importance has been increasingly recognized. We reviewed the available medical literature by PubMed with the keywords “Streptococcus intermedius” AND “lung abscess”, “pleural effusion”, “pleural empyema” from 1993 to 2023, published in English. We found 34 articles meeting the inclusion criteria (Table 1), of which 4 described concomitant brain and lung abscesses, but none reported the presence of lung and brain abscess due to S. intermedius associated with left heart endocarditis [1,2,3,4,5,6,7,8,9,10,11,12,13,14,15,16,17,18,19,20,21,22,23,24,25,26,27,28,29,30,31,32,33,34]. Only one paper [14] described the case of lung and brain abscess associated with Chiari network endocarditis in the right heart.
Streptococcus intermedius is a Gram-positive, catalase-negative, nonmotile and facultative anaerobe coccus that colonize the mouth and the upper respiratory tract [2,26]. SAG streptococci are oral bacteria and may be unable to grow significantly on ordinary aerobic cultures; as a consequence, conventional cultivation may underestimate the role of these pathogens [25] in respiratory infections. The significance of anaerobes and oral bacteria in patients with community-acquired pneumonia and pleuritis has previously been reported [35,36]. In some cases, a 16S rRNA gene sequencing analysis of bronchoalveolar or pleural effusion specimens was able to identify pathogens that are generally difficult to isolate using ordinary cultivation methods [25].
Risk factors for S. intermedius pleuropulmonary disease include smoking, alcoholism, dental diseases, chronic obstructive pulmonary disease, malignant neoplasms, liver cirrhosis, and diabetes [3]. Our patient had dental lesions that could have caused bacteremia and aortic valve endocarditis with brain abscess as a haematogenous spread complication. The lung abscess could have been caused by aspiration or haematogenous spread. Teramoto et al. [37] reported that aspiration may contribute to the pathogenesis of pneumonia in elderly patients, and that an increased age is associated with the risk of developing aspiration pneumonia. Given the young age of our patient, the aspiration in this case is less likely, whereas the haematogenous spread could have caused the lung abscess. Bacteraemic venous blood following the venous draining system to the right ventricle of the heart is pumped into the pulmonary arteries, until the capillary network of alveoli and parts of the visceral pleura. Indeed, several works described the simultaneous occurrence of brain abscess and lung abscess or pleural empyema [22]. In their recent work, Dyrhovden and coll. suggest that facultative and anaerobic oral bacteria, able to spread by deoxygenated venous blood to establish purulent infections in brain tissue, could also be able to reach and establish pyogenic infections in the lung parenchyma or pleural cavity [22].
S. intermedius is reported as a causative pathogen in only 2-5% of cases of bacterial pneumonia, but in 13-44% of pulmonary abscesses/empyema [21]. S. intermedius infections are commonly associated with abscess development. Virulence factors contributing to tissue invasion and abscess formation by this agent have recently been described by Issa and coll. [38] and include antigens I/II surface proteins; hydrolytic enzymes such as hyaluronidase, chondroitin sulfatase, and deoxyribonuclease; biofilm formation and defensive genes to oppose the human immune system, such as superantigens that cause lymphocyte apoptosis; the polysaccharidic capsule formation; the genes of the Streptococcus Invasion locus system; the intermedilysin, which initiates pore complex formation in host cell membranes, and the sialidase A that contributes to pathogenicity by controlling interbacterial communication and host-bacterial interactions. Abscess drainage and surgery should be considered, on a case by case basis, in order to successfully achieve an adequate source control of the infection.
4. Conclusions
In summary, we described a case of brain abscess caused by S. intermedius, associated with lung abscess and aortic valve endocarditis, in a young patient with dental disorders. In addition to being a well known cause of brain abscess, S. intermedius is increasingly recognised as a causative agent of pleuropulmonary disease.
Author Contributions
each Author have made substantial contributions to the conception of the work, to the acquisition of data and to the revision of the paper; each Author has approved the submitted version and agrees to be personally accountable for the Author’s own contributions and for ensuring that questions related to the accuracy or integrity of any part of the work, even ones in which the Author was not personally involved, are appropriately investigated, resolved, and documented in the literature. Conceptualization, F.G. and P.C.; Data Curation, G.C. and G.O.; Methodology: A.C. and F.T.; Writing – Original Draft Preparation, P.C. and G.G.; Writing – Review & Editing, S.A.M and E.C.; Supervision, F.T. and P.C.
Funding
This research received no external funding.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Written informed consent for publication was obtained from the patient for the case report and imaging.
Data Availability Statement
The data presented in this study are available on request from the corresponding author.
Conflicts of Interest
F.T. received grants from Tillots, MSD, Menarini, Angelini, Gilead. All other Authors: no conflict.
References
- Shinzato, T.; Saito, A. The Streptococcus milleri group as a cause of pulmonary infections. Clin. Infect. Dis. 1995, 21 Suppl 3, S238-43. [CrossRef]
- Noguchi, S.; Yatera, K.; Kawanami, T.; Yamasaki, K.; Naito, K.; Akata, K.; Shimabukuro, I.; Ishimoto, H.; Yoshii, C.; Mukae, H. The clinical features of respiratory infections caused by the Streptococcus anginosus group. BMC Pulm. Med. 2015, 15, 133. [CrossRef]
- Bueno, C.O.P.; Trillos, S.J.G.; Rosales, D.J.C.; García, E.A.B. Lung abscess due to Streptococcus intermedius associated with SARS CoV-2 infection in pregnancy: Unusual presentation and complication of a commensal bacteria during pregnancy. Clin. Case Rep. 2023, 11, e6763. [CrossRef]
- Erne, B.V.; Exner, C.; Frauenfelder, T.; Schmid, S.; Weder, W. A curious case of convulsion. Lancet 2010, 375, 2050. [CrossRef]
- Jerng, J.S.; Hsueh, P.R.; Teng, L.J.; Lee, L.N.; Yang, P.C.; Luh, K.T. Empyema thoracis and lung abscess caused by viridans streptococci. Am. J. Respir. Crit. Care Med. 1997, 156, 1508-14. [CrossRef]
- Chandy, B.; Todd, J.; Stucker, F.J.; Nathan, C.O. Pott's puffy tumor and epidural abscess arising from dental sepsis: a case report. Laryngoscope 2001, 111, 1732-4. [CrossRef]
- May, A.M.; Riede, F.N.; Riede, U.N. Acute subepicardial infarction associated with severe septic shock--insight in myocardial perfusion. Pathol Res Pract. 2010, 206, 401-4. [CrossRef]
- van Laren, M.; van Walree, N.C.; Kluytmans, J.A. Multiple lung abscesses secondary to a uterine empyema caused by an intrauterine device. Infection 2011, 39, 385-7. [CrossRef]
- de Kruif, M.D.; van Gorp, E.C.; Bel, E.H.; Gerlag, D.M.; Kunst, P.W. Streptococcal lung abscesses from a dental focus following tocilizumab: a case report. Clin. Exp. Rheumatol. 2012, 30, 951-3.
- Trabue, C.; Pearman, R.; Doering, T. Pyogenic brain and lung abscesses due to Streptococcus intermedius. J. Gen. Intern. Med. 2014, 29, 407. [CrossRef]
- Maeda, S.; Sado, T.; Sakurada, A.; Okada, Y.; Kondo, T. Successful closure of an open-window thoracostomy wound by negative-pressure wound therapy: report of a case. Surg. Today 2012, 42, 295-8. [CrossRef]
- Armendariz-Guezala, M.; Undabeitia-Huertas, J.; Samprón-Lebed, N.; Michan-Mendez, M.; Ruiz-Diaz, I.; Úrculo-Bareño, E. Absceso cerebral actinomicótico en paciente inmunocompetente [Actinomycotic brain abscess in immunocompetent patient]. Cir. Cir. 2017, 85 Suppl 1, 103-107.
- Sakurai, M.; Nagasawa, H.; Takeuchi, I.; Yanagawa, Y. A Case of an 80-Year-Old Man with Empyema and Psoas Abscess. Case Rep. Emerg. Med. 2020, 24, 2020:8895785. [CrossRef]
- Carrena, O.; Oluoha, O.; Wahba, A.; Eshun, D.; Endsley, M.; Okafor, H. Complicated Infective Endocarditis Limited to a Chiari Network. Case Rep. Cardiol. 2018, 26, 2018:3837825. [CrossRef]
- Fujihara, T.; Itoh, N.; Yamamoto, S.; Kurai, H. Lateral thoracic artery aneurysm with lung abscess and empyema caused by Streptococcus intermedius. J. Gen. Fam. Med. 2021, 22, 296-297. [CrossRef]
- Tasleem, A.; Mahmood, A.; Sharma, R. Streptococcus intermedius Pleuropulmonary Disease: A Not So Commonly Seen Radiological Picture. Cureus 2021, 13, 17385. [CrossRef]
- Manasrah, N.; Nanja Reddy, S.; Al Sbihi, A.; Hafeez, W. Streptococcus intermedius: unusual presentation and complication of lung abscess. BMJ Case Rep. 2021, 14, e245675. [CrossRef]
- Nakagawa, Y.; Otake, S.; Oue, T.; Ryu, H.; Kasai, M. Case of infant invasive Streptococcus intermedius infection suggesting the need for anaerobic cultures. J. Infect. Chemother. 2022, 28, 437-439. [CrossRef]
- Christensen, P.J.; Kutty, K.; Adlam, R.T.; Taft, T.A.; Kampschroer, B.H. Septic pulmonary embolism due to periodontal disease. Chest 1993, 104, 1927-9. [CrossRef]
- Patail, H.; Patail, H.; Ahmad, S. A Man in His 30s Presenting With Shortness of Breath and Productive Cough After a Recent Pneumonia. Chest 2020, 157, e91-e93.
- Takahashi, S.; Ishitsuka, T.; Namatame, K.; Nakamura, M. A false-positive pneumococcal rapid urinary antigen test in Streptococcus intermedius infection. Respirol. Case Rep. 2019, 7, e00466. [CrossRef]
- Dyrhovden, R.; Nygaard, R.M.; Patel, R.; Ulvestad, E.; Kommedal, Ø. The bacterial aetiology of pleural empyema. A descriptive and comparative metagenomic study. Clin. Microbiol. Infect. 2019, 25, 981-986. [CrossRef]
- Cobo, F.; Sampedro, A.; Rodríguez-Granger, J.; Aliaga-Martínez, L.; Navarro-Marí, J.M. Clinical and microbiologic characteristics of pleuro-pulmonary infection due to Streptococcus intermedius. Rev. Esp. Quimioter. 2018, 31, 146-151.
- Crespo Valadés, E.; Fernández Blanco, J.M.; Troya García, J.; Malmierca Corral, M. Absceso subfrencio izquierdo primario por Streptoccocus intermedius [Primary left subphrenic abscess due to Streptococcus intermedius]. An. Med. Interna 2005, 22, 202-3.
- Noguchi, S.; Yatera, K.; Kawanami, T.; Yamasaki, K.; Fukuda, K.; Naito, K.; Akata, K.; Nagata, S.; Ishimoto, H.; Taniguchi, H.; Mukae, H. Pneumonia and empyema caused by Streptococcus intermedius that shows the diagnostic importance of evaluating the microbiota in the lower respiratory tract. Intern. Med. 2014, 53, 47-50. [CrossRef]
- Hannoodi, F.; Ali, I.; Sabbagh, H.; Kumar, S. Streptococcus intermedius Causing Necrotizing Pneumonia in an Immune Competent Female: A Case Report and Literature Review. Case Rep. Pulmonol. 2016, 2016, 7452161. [CrossRef]
- Mautner, G.H.; Lu, I.; Ort, R.J.; Grossman, M.E. Transverse leukonychia with systemic infection. Cutis 2000, 65, 318-20.
- Huang, M.; Li, S.; Wu, X.; Xu, D.; Tang, L.; Chen, Z. An isolated pulmonary nodule secondary to Streptococcus intermedius infection in an otherwise healthy 10-year-old boy: A case report and literature review. Front. Pediatr. 2022, 10, 921258. [CrossRef]
- Kurkowski, S.C.; Thimmesch, M.J.; Jha, P.; Abdelgadir, Y.H. Streptococcus intermedius Bacteremia and Pyogenic Liver Abscess in a Patient With No Risk Factors. Cureus 2022, 14, e26786. [CrossRef]
- Jud, P.; Fink-Neuboeck, N.; Lindenmann, J. Massive ventilator-associated pleural empyema. Korean J. Intern. Med. 2019, 34, 942-943. [CrossRef]
- Lescan, M.; Lepski, G.; Steger, V.; Schlensak, C.; Walker, T. Rapidly progressive paraplegia and pleural empyema: how does that correlate? Gen. Thorac. Cardiovasc. Surg. 2013, 61, 640-2.
- Stelzmueller, I.; Berger, N.; Wiesmayr, S.; Eller, M.; Tabarelli, W.; Fille, M.; Margreiter, R.; Bonatti, H. Group milleri streptococci: significant pathogens in solid organ recipients. Transpl. Int. 2007, 20, 51-6. [CrossRef]
- Iskandar, S.B.; Al Hasan, M.A.; Roy, T.M.; Byrd, R.P. Jr. Streptococcus intermedius: an unusual cause of a primary empyema. Tenn. Med. 2006, 99, 37-9.
- Lau, S.K.; Woo, P.C.; Chan, B.Y.; Fung, A.M.; Que, T.L.; Yuen, K.Y. Haemophilus segnis polymicrobial and monomicrobial bacteraemia identified by 16S ribosomal RNA gene sequencing. J. Med. Microbiol. 2002, 51, 635-640. [CrossRef]
- Kawanami, T.; Fukuda, K.; Yatera, K.; Kido, M.; Mukae, H.; Taniguchi, H. A higher significance of anaerobes: the clone library analysis of bacterial pleurisy. Chest 2011, 139, 600-608.
- Yamasaki, K.; Kawanami, T.; Yatera, K.; Fukuda, K.; Noguchi, S.; Nagata, S.; Nishida, C.; Kido, T.; Ishimoto, H.; Taniguchi, H.; Mukae, H. Significance of anaerobes and oral bacteria in community-acquired pneumonia. PLoS One 2013, 8, :e63103. [CrossRef]
- Teramoto, S.; Fukuchi, Y.; Sasaki, H.; Sato, K.; Sekizawa, K.; Matsuse, T.; Japanese Study Group on Aspiration Pulmonary Disease. High incidence of aspiration pneumonia in community- and hospital-acquired pneumonia in hospitalized patients: a multicenter, prospective study in Japan. J. Am. Geriatr. Soc. 2008, 56, 577-9.
- Issa, E.; Salloum, T.; Tokajian, S. From Normal Flora to Brain Abscesses: A Review of Streptococcus intermedius. Front. Microbiol. 2020, 11, 826.
Figure 1.
Chest CT scan showing consolidated area with thick-walled cavity lesion in the left lung lower lobe.
Figure 1.
Chest CT scan showing consolidated area with thick-walled cavity lesion in the left lung lower lobe.

Figure 2.
A) First axial contrast-enhanced T1-weighted NMR showing an oval-shaped enhanced lesion in the left occipital lobe with ipsilateral ventricular communication. B) T2 weighted NMR showing ventricular communication of the lesion with T2 hyperintense fluid collection. C) T1-weighted sagittal view of the abscess.
Figure 2.
A) First axial contrast-enhanced T1-weighted NMR showing an oval-shaped enhanced lesion in the left occipital lobe with ipsilateral ventricular communication. B) T2 weighted NMR showing ventricular communication of the lesion with T2 hyperintense fluid collection. C) T1-weighted sagittal view of the abscess.
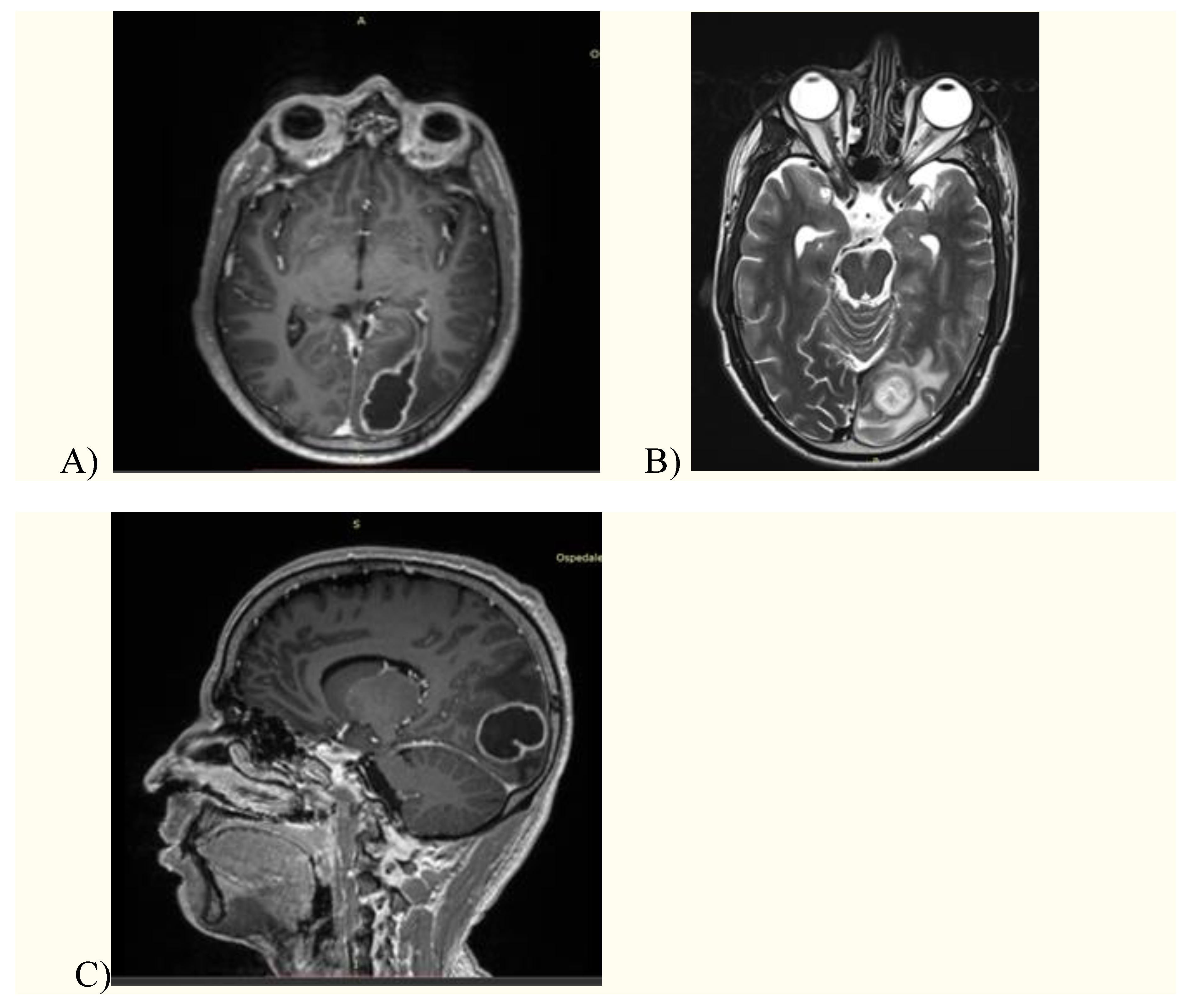
Figure 3.
A) follow-up CT scan showing the reduction of the left lung lesion after a 4- week antibiotic course. B) Follow-up T1-weighted brain NMR after a 4-week antibiotic course. C) Follow-up T2-weighted brain NMR after a 4-week antibiotic course.
Figure 3.
A) follow-up CT scan showing the reduction of the left lung lesion after a 4- week antibiotic course. B) Follow-up T1-weighted brain NMR after a 4-week antibiotic course. C) Follow-up T2-weighted brain NMR after a 4-week antibiotic course.

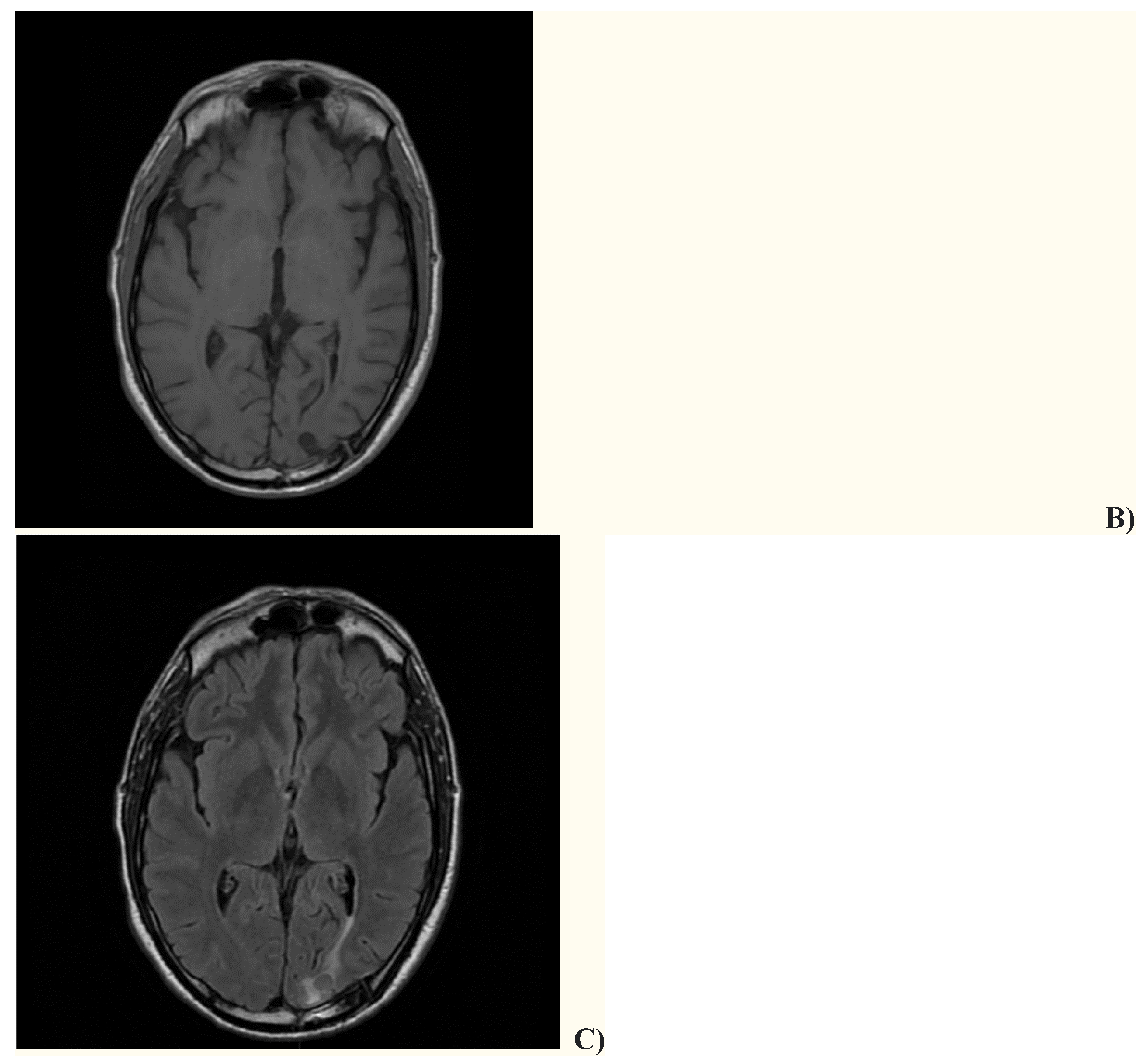

Table 1.
Articles describing lung abscesses and/or pleural infections due to S. intermedius.
| Article | n. of patients |
Gender | Age (y) | Infection site | Outcome |
|---|---|---|---|---|---|
| Shinzato et al.1, 1995 | 9 | M=8 F=1 |
Mean 61.3 | Lung, pleura | NA |
| Noguchi et al.2, 2015 | 14 | M=10 F=4 |
Mean 77.3 | Lung/pleura | Recovered=12 Death=2 |
| Bueno et al.3, 2023 | 1 | F | 25 | Lung | Recovered |
| Erne et al.4, 2010 | 1 | M | 61 | Lung, brain | Recovered |
| Jerng et al.5, 1997 | 17 | NA | NA | Lung/pleura | NA |
| Chandy et al.6, 2001 | 1 | M | 21 | Blood, lung, frontal sinus, epidural abscess | Recovered |
| May et al.7, 2010 | 1 | M | 53 | Lung | Death |
| Van Laren et al.8, 2011 | 1 | F | 29 | Blood, lung, genital | Recovered |
| De Cruif et al.9, 2012 | 1 | F | 63 | Lung, dental abscess | Recovered |
| Trabue et al.10, 2014 | 1 | M | 36 | Lung, brain | NA |
| Maeda et al.11, 2012 | 1 | F | 46 | Chest wall abscess, pleura | Recovered |
| Armendariz-Guezala et al.12, 2017 | 1 | M | 33 | Brain, lung | Recovered |
| Sakurai et al.13, 2020 | 1 | M | 80 | Pleura, iliopsoas abscess | Recovered |
| Carrena et al.14, 2018 | 1 | M | 61 | Lung, brain, Chiari network endocarditis | Recovered |
| Fujihara et al.15, 2021 | 1 | M | 64 | Lung, pleura | Death |
| Tasleem et al. 16, 2021 | 1 | M | 54 | Lung, pleura | Death |
| Manasrah et al.17, 2021 | 1 | M | 54 | Lung, pleura, vertebrae and discitis | Recovered |
| Nakagawa et al.18, 2022 | 1 | M | 6 mo | Lung, pleura | Recovered |
| Christensen et al.19, 1993 | 1 | M | 56 | Lung | Recovered |
| Patail et al.20, 2020 | 1 | M | 30 | Lung, pleura | NA |
| Takahashi et al.21, 2019 | 1 | F | 83 | Pleura | Recovered |
| Dyrhovden et al.22, 2019 | 16 | NA | NA | Pleura | NA |
| Cobo et al.23, 2018 | 9 | M=7 F=2 |
Mean 63.9 | Lung, pleura | Recovered=8 Death=1 |
| Crespo Valades et al.24, 2005 | 1 | M | 60 | Pleural effusion, subphrenic abscess | Recovered |
| Noguchi et al.25, 2014 | 1 | M | 79 | Lung, pleura | Recovered |
| Hannoodi et al.26, 2016 | 1 | F | 52 | Lung, pleura | Recovered |
| Mautner et al.27, 2000 | 1 | M | 80 | Lung, pleura | Recovered |
| Huang et al.28, 2022 | 1 | M | 10 | Lung, pleura | Recovered |
| Kurkowski et al.29, 2022 | 1 | M | 39 | Liver, pleura, blood | Recovered |
| Jud et al.30, 2019 | 1 | M | 59 | Lung, pleura | Recovered |
| Lescan et al.31, 2013 | 1 | M | 74 | Lung, pleura, epidural abscess | Recovered |
| Stelzmueller et al.32, 2006 | 2 | NA | NA | Pleural empyema | Recovered |
| Iskandar et al.33, 2006 | 1 | NA | NA | Pleural empyema | NA |
| Lau et al.34, 2002 | 1 | M | 32 | Pleural empyema, blood | Recovered |
NA: not available
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



