
Submitted:
02 June 2023
Posted:
05 June 2023
You are already at the latest version
Abstract
Primary Health Care is crucial in the healthcare system, being the first level of contact with health services for users and patients to take action using the available resources. Patient care units are created to facilitate direct user participation through the circuit of complaints, grievances, and suggestions, allowing the analysis of the population's unmet expectations and needs. To study complaints and grievances regarding the treatment and information received by users in the Santiago and Barbanza healthcare area during the year 2022. A descriptive cross-sectional study was conducted, in which complaints filed by patients in the year 2022 in the Santiago and Barbanza healthcare area were analyzed. A total of 326 users who filed a total of 512 complaints were studied in the year 2022, with 358 (70.0%) related to treatment/information. The mean age was 33.5±16.2 years. 72.4% were women (n=236). A Pearson correlation was performed to establish whether there was a dependence between the number of healthcare visits in both primary care and hospital settings in 2022 and the number of complaints filed in the same year. Pearson correlation coefficient was 0.14; 95% CI (0.02 - 0.27), p=0.012. There is a correlation between the number of consultations and the number of complaints filed. Frequent users are more likely to file a complaint. However, there is no correlation between the number of consultations and the likelihood of filing a complaint regarding treatment/information. Therefore, there seems to be a good relationship between healthcare personnel and users, which impacts patient satisfaction.
Keywords:
primary care
; grievances
; complaints
; satisfaction
1. Introduction
Primary health care (PHC) is considered a fundamental part of the healthcare system, acting as the first point of contact for users and patients to access available health services [1,2]. This concept was defined during the First International Conference on Primary Health Care held in Alma-Ata, USSR, in 1978, which laid the foundation for the development of this level of care [3].
Building upon the Alma-Ata declaration, the World Health Organization (WHO) defines primary health care as "essential health care based on practical, scientifically sound, and socially acceptable methods and technologies, made universally accessible to individuals and families in the community through their full participation and at a cost that the community and country can afford" [3]. This definition was further ratified and complemented during the 2018 World Conference on Primary Health Care in Astana, Kazakhstan, as "a high-quality, safe, comprehensive, integrated, accessible, available, and affordable health service for all, delivered with compassion, respect, and dignity by well-trained, competent, motivated, and committed health professionals" [4].
These conferences and definitions emphasize the active participation of healthcare system users and health services as a tool for continuous improvement of processes at the primary care level. The success of this goal depends on several factors: (1) the development of knowledge and capabilities to ensure access for all, respecting their rights, needs, dignity, and autonomy; (2) health workforce, creating decent jobs with appropriate remuneration for all professionals, investing in education, training, development, and motivation; (3) technology, through advances in information systems, accountability, and performance monitoring in health systems; (4) financing, working towards financial sustainability and efficiency in national health systems [4].
In our country, user participation in the healthcare system is manifested through complaints and their management. Article 10 of the General Health Law (1986) guarantees the "right to make complaints, grievances, or suggestions regarding the functioning of health services." Apart from safeguarding one of the fundamental rights of citizens, complaints serve as a valuable source of information to understand both patient and user expectations, dissatisfaction reasons, and identify deficiencies in the healthcare system as a whole [5].
This is further reflected in the Law 16/2003 on Cohesion and Quality of the National Health System, which establishes cooperation and coordination among public health administrations, guaranteeing equity, quality, equality, and social participation in the national healthcare system [6].
Currently, the strategic plans of healthcare organizations should focus on user satisfaction. Customer orientation is a fundamental aspect of the EFQM (European Foundation for Quality Management) excellence model, and the assessment of user opinions is essential for total quality management. In this regard, patient care units are established to facilitate direct user participation through the circuit of complaints, grievances, and suggestions, enabling the analysis of unmet expectations and needs of the population served [7].
In our context, the Galician Health Law refers to the rights related to suggestions and complaints. It establishes the rights that influence the development of measures so that all centers, services, and healthcare facilities make suggestion and complaint forms available to users, as well as efficient procedures to receive written responses within established regulatory deadlines [8]. These measures have been reinforced in recent years by proposals for the development of local health plans as strategic planning instruments, which drive the transformation of primary health care. This model incorporates various principles: strengthening traditional values, community orientation, strengthening equity and the role of the patient, ensuring comparative leadership, and ensuring economic sufficiency and regulatory viability [9,10,11].
On the other hand, it is well known that complaints provide a partial approach to user opinions [12]. However, they offer complementary information and the advantage of easily accessible written records, enabling retrospective data analysis [13,14].
Complaints allow us to understand the impact of structural and organizational changes on users [15]. The Quality Plan of the National Health System (NHS) highlights the usefulness of analyzing complaints to identify improvement opportunities and drive organizational changes. For this purpose, evaluation and internal communication of results are crucial [16].
In recent years, there has been an increase in the number of complaints, with complaints regarding treatment/information being the most common [16]. In this context, our objective was to study complaints for this reason in the healthcare area of Santiago and Barbanza, Spain.
2. Materials and Methods
2.1. Study Design
A descriptive cross-sectional design was used to study complaints regarding treatment and information in primary care reported by users in the healthcare area of Santiago and Barbanza during the years 2020-2022. The following secondary objectives were defined: (1) Determine the prevalence and incidence of complaints regarding treatment and information received in primary care in the healthcare area of Santiago and Barbanza during the year 2022. (2) Identify the profile of complainants regarding complaints and grievances about treatment and information received in the year 2022. (3) Investigate whether there is a correlation between increased use of healthcare services and the likelihood of filing complaints or grievances about treatment and information received in the year 2022. (4) Identify the professional category with the highest prevalence of complaints and grievances about treatment and information in primary care in the healthcare area of Santiago and Barbanza in the year 2022. (5) Determine the healthcare centers with the highest incidence of complaints about treatment and information received in primary care in the healthcare area of Santiago and Barbanza in the year 2022.
Population and Sample
This study was conducted in the healthcare area of Santiago and Barbanza, which had a reference population for primary care of 442,618 citizens in the year 2022, distributed across 46 municipalities, with a total of 76 healthcare centers, including local clinics.
Assuming that a user of the healthcare system who files complaints regarding the received treatment is likely to file more than one complaint per year and that they are also frequent users (defined as those who have more than 12 visits per year) [17], we selected as the sample for the study the users who filed at least one complaint regarding treatment/information in 2022. During the year 2022, 326 users in the Santiago and Barbanza area filed complaints about treatment/information received in primary care. All these complaints will be studied in the present project. To determine whether the differences found in the bivariate analyses according to the objectives were significant, a significance level of 5% was established, with a confidence interval of 95% for estimating the parameter. Assuming an expected prevalence of complaints regarding treatment received of 18% [18], with a precision of 3%, this sample of 326 users provided us with a power greater than 90% for estimation. Users who were healthcare professionals or non-healthcare professionals in the primary care area and whose complaints did not concern a healthcare episode in which they were users as patients were excluded.
2.2. Procedure
To achieve the objectives of the study, all complaints filed regarding the treatment/information received by primary care users were included. Those classified as treatment/information received, from the years 2020 to 2022, were selected from the SERGAS application for complaint management.
All complaints and claims submitted by SERGAS users, regardless of the method of submission, were recorded and managed through an application called CONECTA. CONECTA is a unique and homogeneous management system for all of SERGAS, which allows for the collection, resolution, and reporting of complaints and suggestions related to service provision, as well as systematic analysis of the information derived from them in order to develop improvement actions. This application allows for the extraction of data collected from each complaint.
Based on this application, the complaints and claims management unit of the Santiago and Barbanza health area generates a dataset for analyzing each complaint and providing a response. Therefore, this unit maintains a data registry for care and management purposes, which is used to perform analyses of the unit's own activities, as well as continuous improvement work.
This data registry contains the following variables:
- Complaint/claim registration number
- Name and surname of the affected user
- SERGAS Identifying Care Number (NASI) of the affected user
- Gender of the affected user
- Age of the affected user
- Complaint submission date
- Center involved in the complaint
- Service involved
- Text of the complaint/claim
To determine the number of contacts made by users who were part of the sample, as well as the services and units, both in primary care and hospital settings, that they interacted with during the years 2020 to 2022, a query was made to the Complex Analysis Information System (SIAC) of SERGAS.
From the initial study data, a study database was generated, which included the following variables:
- Complaint/claim registration number
- Gender of the affected user
- Age of the affected user
- Complaint submission date
- Center involved in the complaint
- Service involved
- Number of contacts with the healthcare system per complaining user
- Services each complaining user interacted with
2.3. Statistical Analysis
A descriptive analysis of the collected variables was conducted to study the complaints/claims. Absolute and relative frequencies were calculated for qualitative variables. For the analysis of quantitative variables, mean ± standard deviation was used when they followed a normal distribution, or median and interquartile range when they did not. The normality of variables was tested using the Kolmogorov-Smirnov test. Exploratory bivariate analyses were carried out to detect potential dependencies between variables such as age, gender, service utilization, and the probability of filing complaints related to perceived treatment by the user. For this purpose, the Student's t-test or Wilcoxon rank-sum test was conducted when dichotomous qualitative variables were compared with continuous variables, depending on normality. When comparing qualitative variables, the Chi-square test or Fisher's exact test was used. A significance level of 5% was set for the bivariate analyses.
2.4. Ethical and Legal Aspects
The present study was evaluated and approved by the Santiago-Lugo Territorial Ethics Committee, with registration code 2023/192.
3. Results
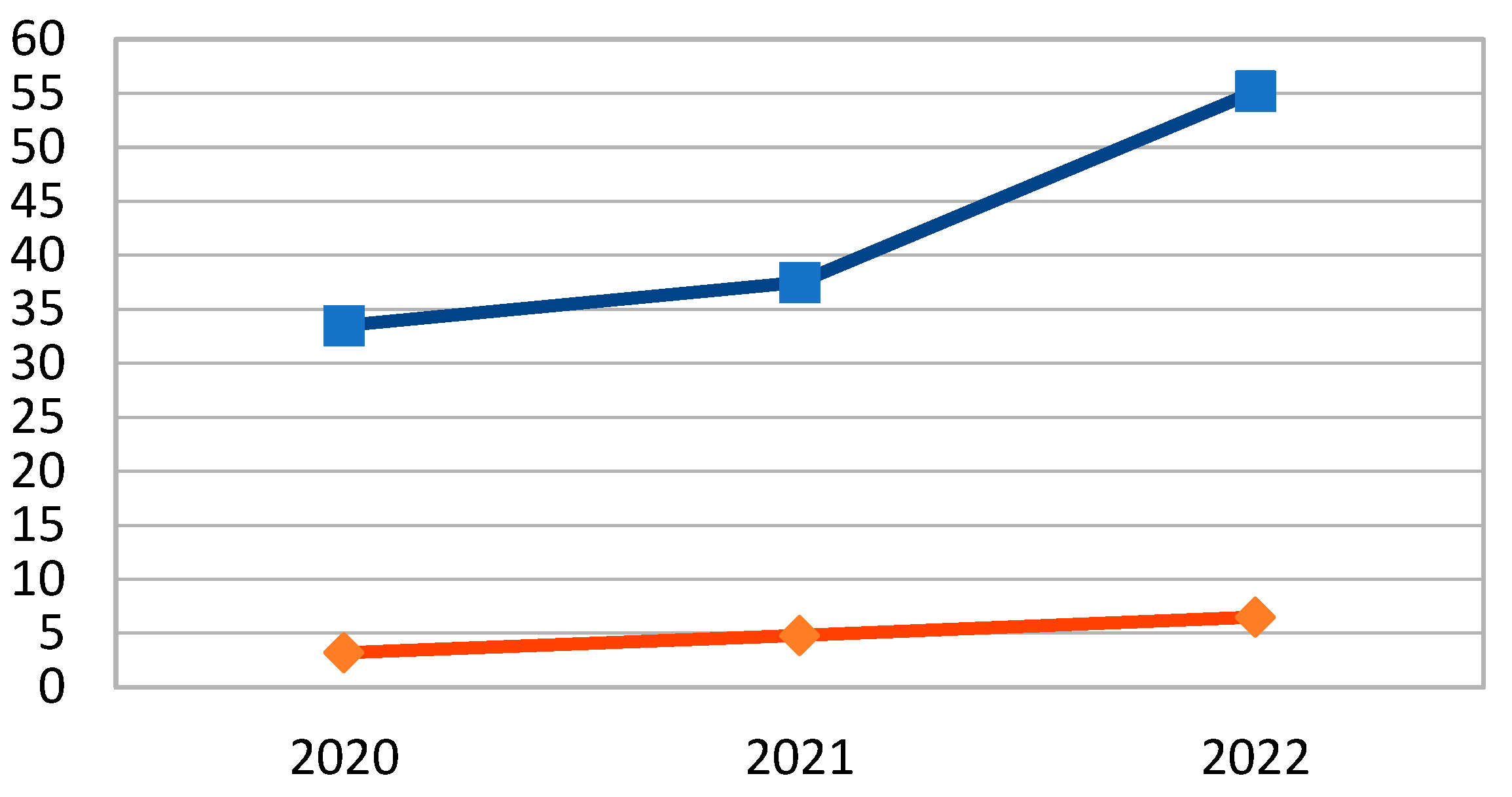
During the years 2020, 2021, and 2022, there were, respectively, 1,429, 2,127, and 2,858 complaints/claims filed in the primary care area. In those same years, a total of 4,271,095, 5,667,110, and 5,179,436 healthcare acts were generated, respectively. This represents a cumulative incidence (CCI) of 33.5 complaints per 100,000 healthcare acts in 2020; 37.5 in 2021, and 55.2 in 2022. Our complaint incidence rate (CIR), defined as the number of complaints/1,000 users/year, was 3.2 in 2020, 4.8 in 2021, and 6.5 in 2022.
Figure 1.
Evolution 2020-2021 of the CCI and CIR of claims.CCI: blue line. CIR: Red line.
The prevalence of complaints related to treatment/information in 2020, 2021, and 2022 was 10.7%, 13.6%, and 12.4%, respectively.
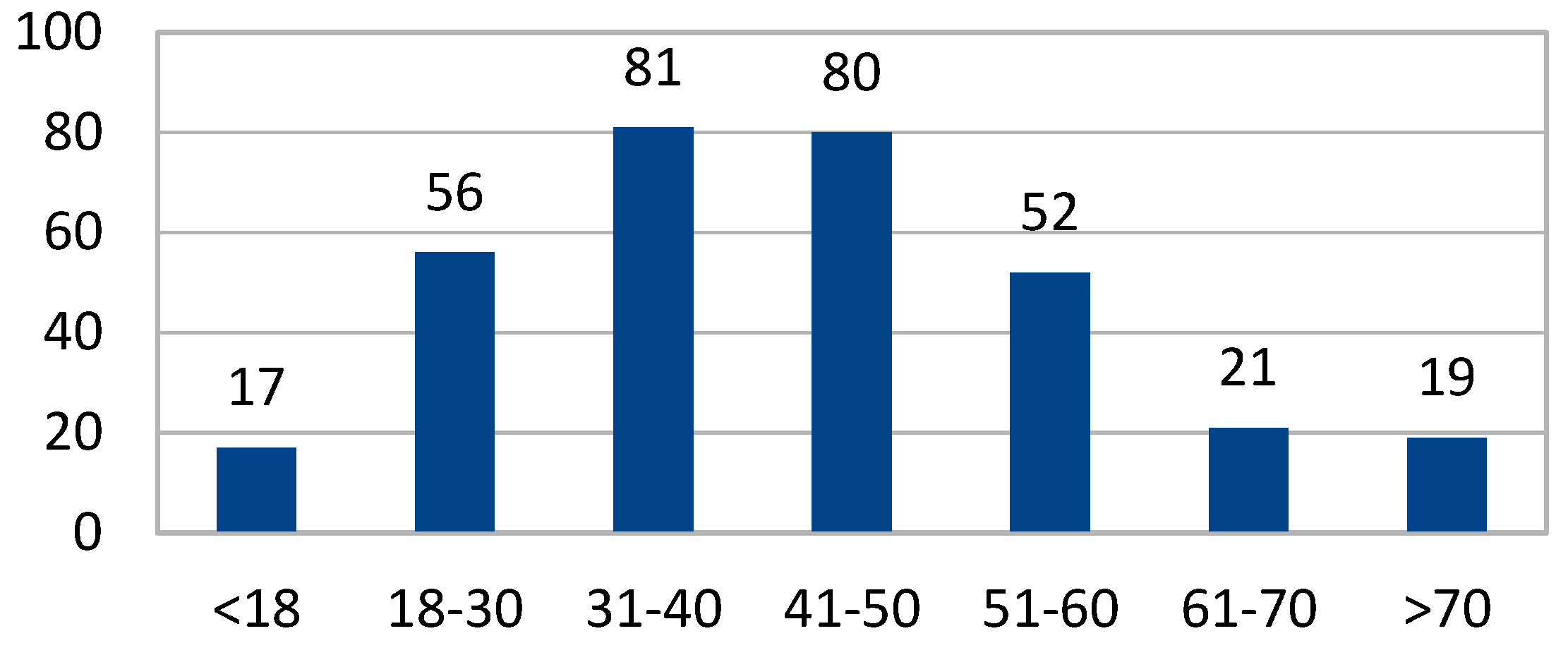
The study analyzed 326 users who had submitted at least one complaint/claim in primary care in 2022. These 326 users filed a total of 512 complaints/claims in 2022, with 358 (70.0%) related to treatment/information.
The mean age was 33.5 ± 16.2 years. 72.4% of the sample were women (n=236). The distribution of age categories was as follows:
Figure 2.
Distribution by age groups of the sample (n). n= number of participants into the age group.
Figure 2.
Distribution by age groups of the sample (n). n= number of participants into the age group.
We investigated if there were differences in the probability of filing a complaint based on gender. The mean number of complaints filed by women in 2022 was 1.6 ± 1.3, while for men it was 1.5 ± 1.1 (p=0.517). Regarding complaints related to treatment/information in 2022, there were no significant differences based on gender and the number of complaints filed. It was 1.1 ± 0.3 for women versus 1 ± 0.3 for men (p=0.673).
We assessed if gender could influence the probability of being a hyper-complainer, defined as a user who files more than 1 complaint per year (see Table 1).
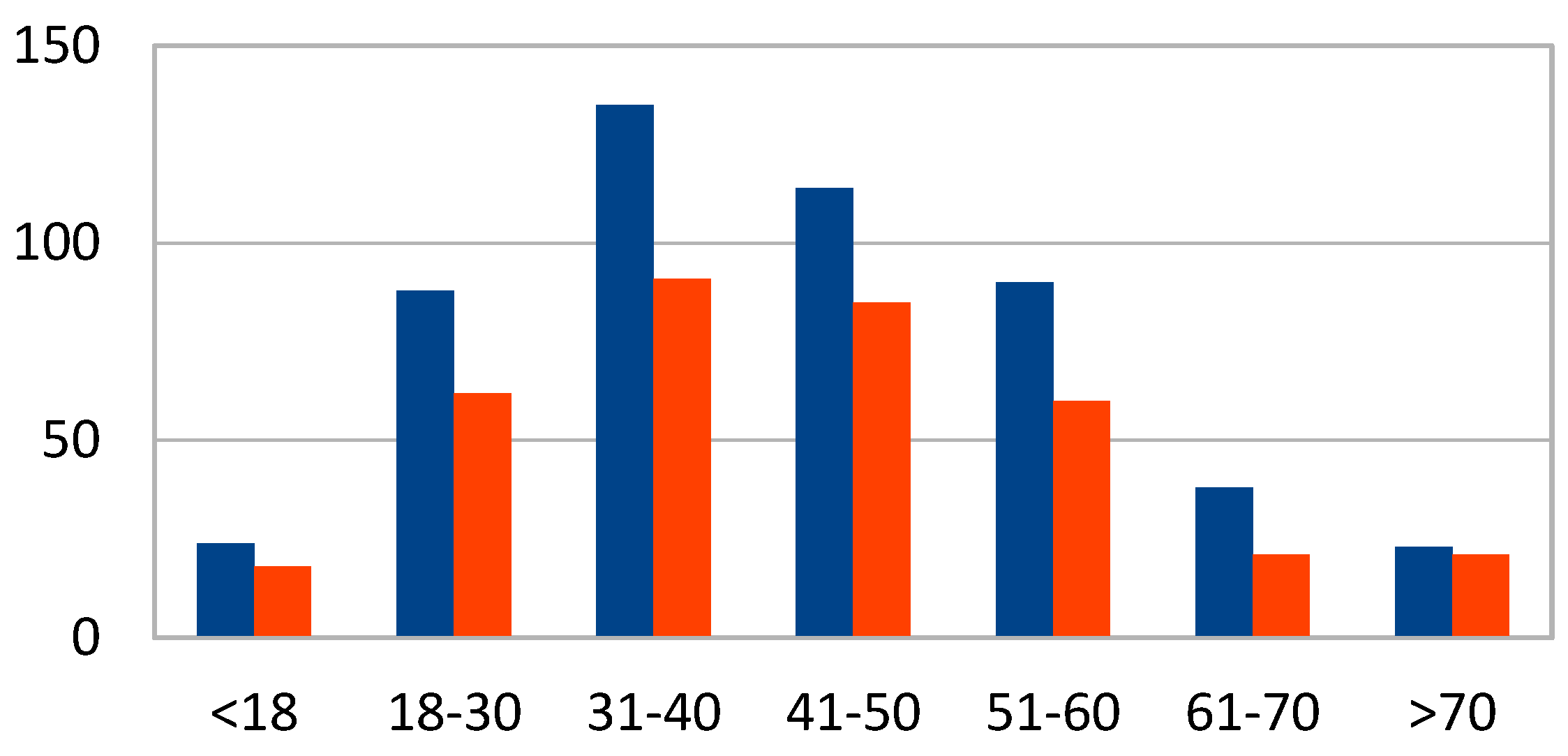
Figure 3.
Number of claims by age range. Year 2022. Total number of complaints: blue line. Number of complaints related to treatment/information: red line.
Figure 3.
Number of claims by age range. Year 2022. Total number of complaints: blue line. Number of complaints related to treatment/information: red line.
Regarding the services that received the most complaints about treatment, they can be observed in Figure 4.
The professional categories that received the most complaints related to treatment/information were as follows:
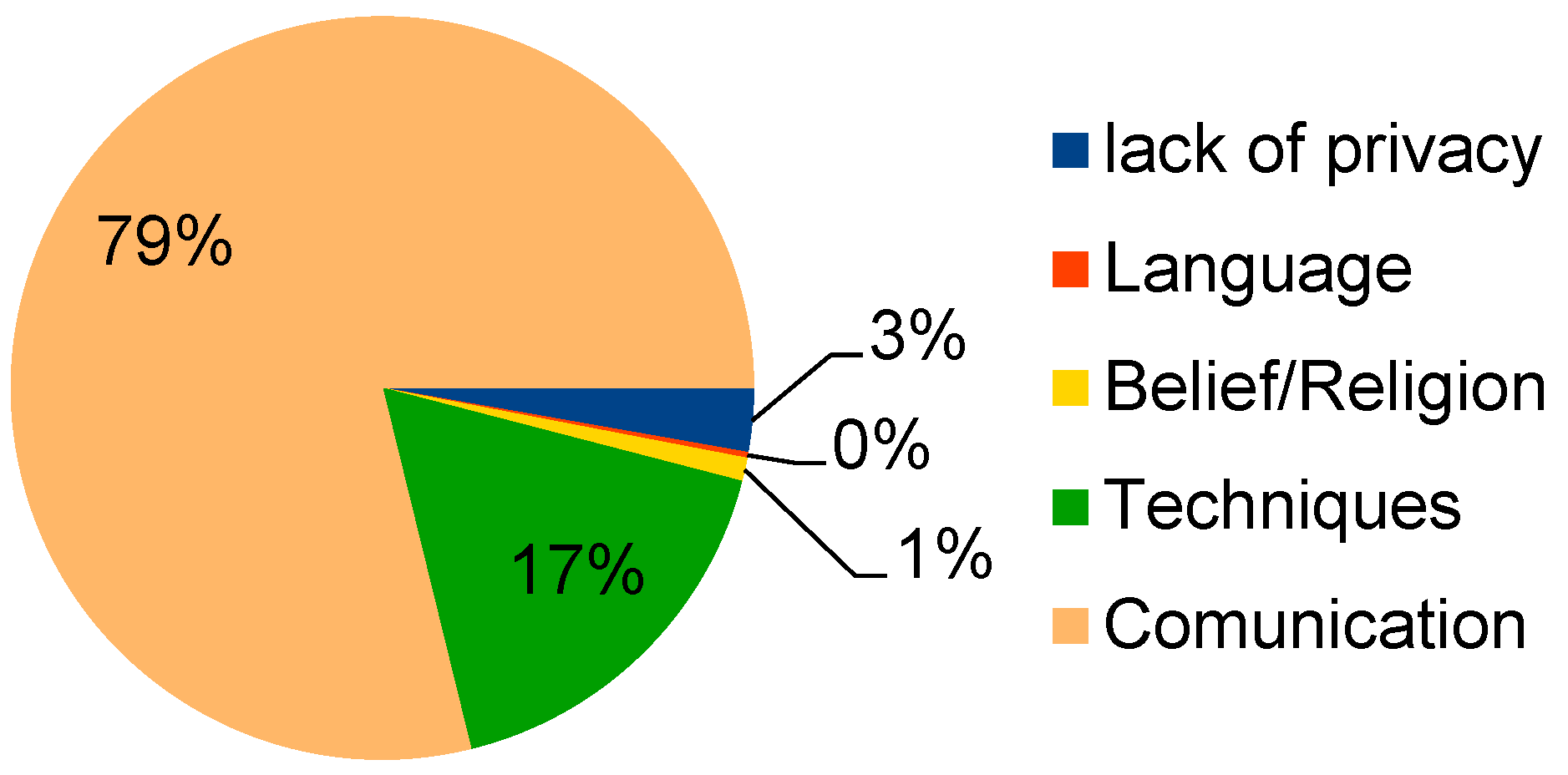
Figure 5.
Reasons for treatment/information complaints. Year 2022.
The professional categories that received the most complaints related to treatment/information were as follows (Figure 6):
The analyzed patients accumulated a total of 13,543 primary care consultations and 2,462 hospital consultations between 2020 and 2022. The mean number of consultations per year was as follows (see Table 2).
Out of the 326 analyzed patients, 170 were defined as hyperfrequenters (52.1%). There were marginally significant differences regarding being a hyperfrequenter and the probability of filing more than one complaint (hyper-complainer). 62.2% of hyperfrequenters filed more than one complaint related to treatment/information in 2022, compared to 37.8% of non-hyperfrequenters. OR = 1.5; 95% CI (0.9 - 2.4), p=0.06. No significant differences were observed regarding gender and the probability of being a hyper-complainer, OR = 1.2; 95% CI (0.7 - 2.0), p=0.340.
Figure 7.
Scatter plot and fit line of the Pearson correlation AP-AH care and number of claims in 2022.
Figure 7.
Scatter plot and fit line of the Pearson correlation AP-AH care and number of claims in 2022.
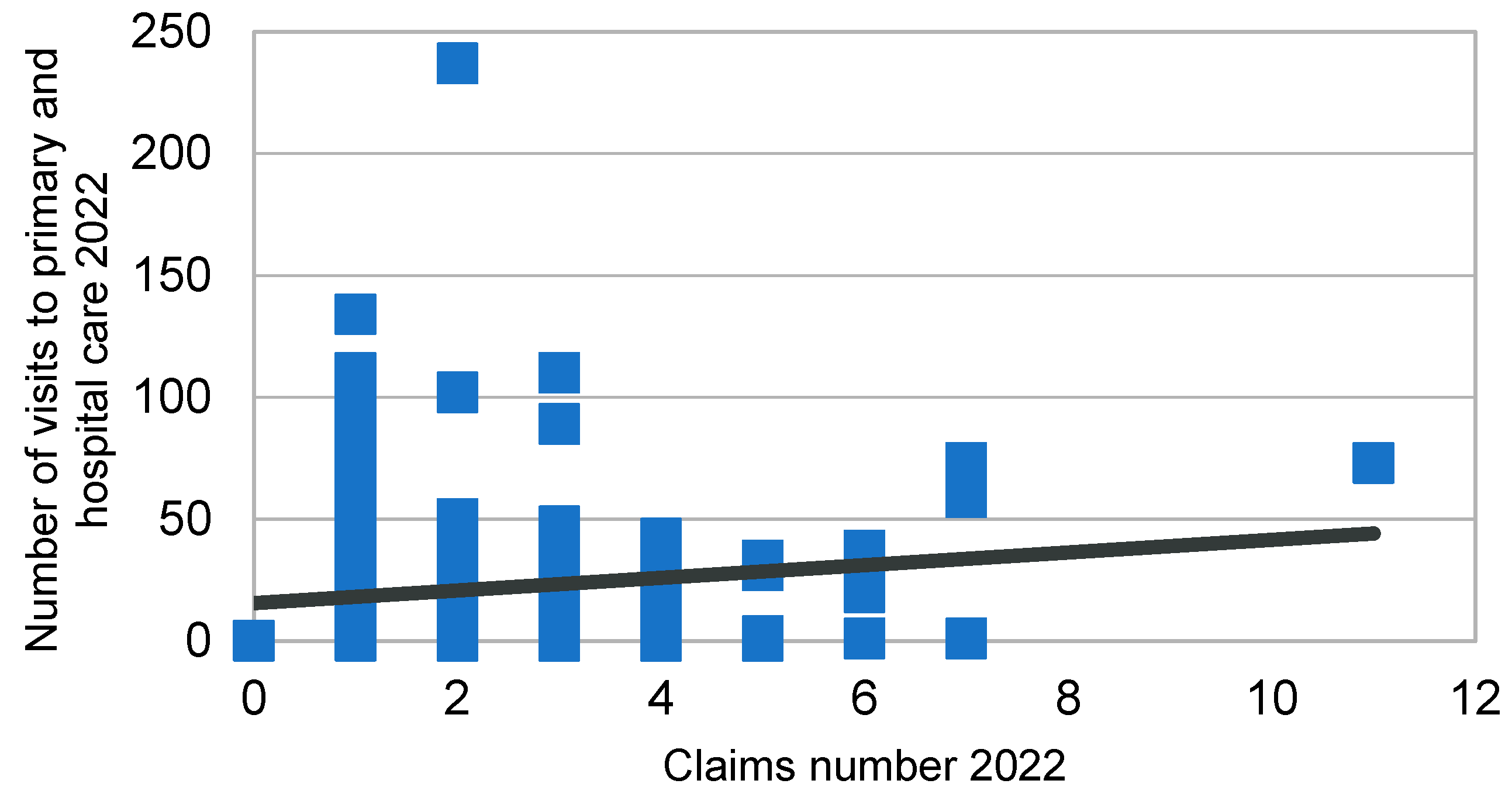
We conducted a Pearson correlation to determine if there was a relationship between the number of healthcare visits in both primary care and hospital settings in 2022 and the number of complaints filed in the same year. The Pearson correlation coefficient was 0.14; 95% CI (0.02 - 0.27), p=0.012. However, there is no dependency between the number of primary care and hospital visits in 2022 and the number of complaints related to treatment/information in that same year. The Pearson correlation coefficient was 0.02; 95% CI (-0.07 - 0.13), p=0.727.
4. Discussion
This study is, to our knowledge, the first one conducted in our setting that allows us to estimate the influence of the number of healthcare visits in a given year on the probability of filing a complaint.
Among the results we obtained, it is interesting to note that although the group that visits primary care centers the most consists of older individuals, the majority of complaints were filed by the middle-aged population (with 81% falling between the ages of 31 and 40). This demonstrates that older population tends to be more accepting of the services provided to them, while younger population demands greater efficiency and better treatment in healthcare.
Regarding gender distribution, a significant difference emerges between females and males, with women being the ones who file the most complaints. This finding aligns with information gathered from previous studies [19,20]. This is likely due to women being more frequent users of primary care centers, either as patients themselves or as accompanying individuals.
On the other hand, it is challenging to compare the most frequent classification of complaint reasons with other studies due to the lack of uniformity in classification. However, in various analyses, the top five most common reasons include choice of doctor or center, dissatisfaction with care, lack of staff, inappropriate treatment, and appointment scheduling [19,20,21].
In our study, the main reason was related to treatment/information between users, healthcare professionals, and non-medical staff. Communication emerged as the primary issue, accounting for 79% of the cases, followed by technical aspects at 17%. In contrast, previous research has highlighted other reasons such as administrative organization, delays in care, and disagreement with institutional norms [21].
Regarding the personnel or service targeted by the complaint, family physicians are the majority, which aligns with findings from other studies [19,20], followed by non-medical staff and nursing personnel. This may be due to the increased contact between family physicians and patients, leading to higher expectations placed on them.
This study highlights that complaints and grievances in general, particularly those related to treatment/information, have been increasing in recent years. This trend is likely associated with a rise in user demands and improved awareness of the complaint process, as well as growing confidence in its effectiveness. Increased user demands are related to high healthcare utilization, which influences the likelihood of filing a complaint [22]. One way to reduce the number of complaints or grievances regarding treatment/information is to improve doctor-patient communication, as well as communication among all healthcare professionals and users of the healthcare system. Previous studies have shown that as healthcare utilization increases, patients exert greater pressure on physicians, making communication more challenging [23].
Among the strengths of our study is the fact that analyzing the information provided by complaints and suggestions is one of the indirect methods that can be used to assess user satisfaction [19,20,24]. A rigorous and comprehensive analysis of these complaints can help identify issues related to the services provided in our centers, thereby promoting improvements to deliver the best possible service to our population.
As for limitations, it is important to note that our study focuses on complaints related to treatment/information received. We chose to do so because this type of complaint is generally the most common, as indicated by similar studies in our setting [20]. Additionally, when interpreting the results, it should be considered that the reliability and accuracy of data provided by primary care users can be influenced by significant subjectivity [25,26]. Furthermore, the classification of complaints depends on the individual criteria of the administrative professional evaluating and categorizing the complaint. This could potentially lead to confusion regarding the absolute number of complaints for the specific reasons analyzed in this study. This could be improved by implementing an IT tool that classifies complaints based on keywords contained within the complaint itself, as well as by creating protocols for complaint management that establish consistent criteria for proper classification of all complaints received [27].
Implications of this study include the promotion and implementation of continuous training innovations for primary care professionals to improve the relationship and communication between professionals and patients, thereby increasing patient satisfaction. Furthermore, further research should be conducted to deepen the assessment of complaints and grievances regarding treatment and information received, as well as to establish effective systems for resolving and responding to these complaints and grievances. It is also important to strengthen organizational and continuity of care aspects to establish more meaningful connections with users and create additional means, channels, and avenues to facilitate improved communication from patients and users.
5. Conclusions
Complaints and grievances serve as valuable sources of information regarding deficiencies identified by users accessing these services. There is a significant room for improvement in the analysis and management of these complaints and grievances.
Finally, based on this study, we can conclude that there is a correlation between the number of consultations and the number of complaints/grievances filed. High-frequency users are more likely to file a complaint. However, there is no correlation between the number of consultations and the likelihood of filing a complaint regarding treatment/information. Therefore, there appears to be a good relationship between healthcare personnel and users, which has an impact on patient satisfaction.
Author Contributions
Conceptualization, J.M.V-L.; M.G-P. and M.S-P.; methodology, J.M.V-L.; validation, J.M.V-L. and M.G-P.; formal analysis, J.M.V-L.; investigation, M.F.V-L; M.G-P. and M.S-P.; resources, M.F.V-L and M.G-P.; data curation, J.M.V-L.; writing—original draft preparation, J.M.V-L. and M.F.V-L.; writing—review and editing, J.M.V-L.; M.F.V-L., M.G-P. and M.S-P.; supervision, J.M.V-L.; and M.S-P.; project administration, J.M.V-L.; and M.S-P. All authors have read and agreed to the published version of the manuscript.
Funding
Please add: This research received no external funding.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Forrest CB, Starfield B. Entry into primary care and continuity: the effects of acces. Am J Public Health 1998; 88 (9):1330-1336.
- Starfield B. Primary care: concept, evaluation, policy. Oxford: Oxford University Press, 1992.
- World Health Organization. Declaration of Alma-Ata. International Conference on Primary Health Care, Alma-Ata: WHO; 1978. Available in: http://apps.who.int/iris/bitstream/handle/10665/39244/9243541358.pdf;jsessionid=E63236BFFAE019FFFB5485E7DC24FEE4?sequence=1. [Accessed on March 23, 2023].
- World Health Organization. Astana Declaration. International Conference on Primary Health Care, Astana: WHO; 2018. Available in: https://www.who.int/docs/default-source/primary-health/declaration/gcphc-declaration-sp.pdf. [Accessed on March 23, 2023].
- Ley 14/1986, de 25 de abril, General de Sanidad. BOE núm. 102, de 29/04/1986. Available in: https://www.boe.es/buscar/act.php?id=BOE-A-1986-10499. [Consultado el 23 de marzo de 2023].
- Ley 16/2003, de 28 de mayo, de cohesión y calidad del Sistema Nacional de Salud. BOE núm. 128, de 29/05/2003. Available in: https://www.boe.es/buscar/act.php?id=BOE-A-2003-10715. [Accessed on March 23, 2023].
- Corbacho MS, García-Mata JR, Blecua MJ, Equipo de Mejora para la atención al Usuario. La reclamación encubierta. Identificando problemas de calidad. Rev Calidad Asistencial 2001; 16:29-34.
- Ley 8/2008, de 10 de julio, de salud de Galicia. BOE núm. 202, de 21/08/2008. Available in: https://www.boe.es/buscar/act.php?id=BOE-A-2008-14134. [Consultado el 23 de marzo de 2023].
- Consellería de Sanidade, Servizo Galego de Saúde, Dirección Xeral de Asistencia Sanitaria. Plan Galego Atención Primaria 2019-2021. Santiago de Compostela: Xunta de Galicia; 2019. Available in: https://extranet.SERGAS.es/catpb/Docs/gal/Publicaciones/Docs/AtPrimaria/PDF-2760-ga.pdf. [Accessed on March 23, 2023].
- Abarca B, Armenteros del Olmo L, Carreras Viñas M, Clavería A, Domínguez-Sardiña M, Dono Días MA, et al. Por unha atención primaria vertebradora do sistema de saúde. Documento estratéxico e de xestión. Santiago de Compostela; 2019. Available in: https://www.SERGAS.es/Asistencia-sanitaria/Documents/1154/Por%20una%20atenci%C3%B3n%20primaria%20vertebradora%20del%20sistema%20de%20salud%20-%20WEB.pdf. [Accessed on March 23, 2023].
- Consellería de Sanidade, Servizo Galego de Saúde, Dirección Xeral de Asistencia Sanitaria. Plans Locais de Saúde para unha orientación comunitaria da Atención Primaria. Bases metodolóxicas para a súa elaboración. Santiago de Compostela: Xunta de Galicia; 2021. Available in: https://www.SERGAS.es/Asistencia-sanitaria/Documents/1398/Plan%20local%20de%20salud_DEF.pdf. [Accessed on March 23, 2023].
- Skär L, Söderberg S. Patients' complaints regarding healthcare encounters and communication. Nurs Open. 2018;5(2):224–232. doi:10.1002/nop2.132. [CrossRef]
- Almusawi MA, Radwan N, Mahmoud N, Alfaifi A, Alabdulkareem K. Analysis of patients' complaints in primary healthcare centres through the Mawid appl in Riyadh, Saudi Arabia; a cross-sectional study. Malays Fam Physician. 2023;18:17. [CrossRef]
- Schäfer WLA, Boerma WGW, Schellevis FG, Groenewegen PP. GP Practices as a One-Stop Shop: How Do Patients Perceive the Quality of Care? A Cross-Sectional Study in Thirty-Four Countries. Health Serv Res. 2018;53(4):2047-2063. [CrossRef]
- Padilla-Ruiz M, Hortas-Nieto ML, Toribio-Montero JC, Vallecillo Villalba A, Doncel-Molinero D, Rivas-Ruiz F. Patient participation through active listening. About the remodeling of an extractions service. Journal of Healthcare Quality Research 2022;37(6):415-422. [CrossRef]
- Ministerio de Sanidad y Consumo. Análisis y benchmarking del tratamiento de las reclamaciones y sugerencias en el Sistema Nacional de Salud. Madrid; 2008. Available in: https://www.sanidad.gob.es/organizacion/sns/planCalidadSNS/docs/InformelReclamaciones.pdf. [Accessed on March 23, 2023].
- Frequent attenders in general practice care: A literature review with special reference to methodological considerations. Public Health. 2005;119:118-37. [CrossRef]
- Alonso R, Llanes L. Control de calidad en la gestión de las reclamaciones de los usuarios del área sanitaria 10 de atención especializada de la comunidad de Madrid (2000-2005). Revista de Calidad Asistencial 2009;24(2):88-90.
- Añel-Rodríguez RM, Cambero-Serrano MI, Irurzun-Zuazabal E. Análisis de las reclamaciones de pacientes en Atención Primaria: una oportunidad para mejorar la seguridad clínica. Rev Calidad Asistencial 2015;30(5):220-225. [CrossRef]
- Lopez A, Ortiz H, de Miguel C. Análisis de las reclamaciones presentadas en un área de atención primaria. Rev Calidad Asistencial 2003; 18(3):153-8. [CrossRef]
- Gonzalez RM, Arrue B, Perez MJ, Sanchez E, Ansotegui JC, Letona J. La gestion de la información sobre quejas y reclamaciones en Osakidetza-Servicio Vasco de Salud. Rev Calidad Asistencial 2003; 18(7):591-7.
- Mira JJ, Carrillo I, Silvestre C, Pérez-Pérez P, Nebot C, Olivera G, González de Dios J, Aranaz Andrés JM. Drivers and strategies for avoiding overuse. A cross-sectional study to explore the experience of Spanish primary care providers handling uncertainty and patients' requests. BMJ Open. 2018;8(6):e021339. [CrossRef]
- O'Malley AS, Rich EC, Ghosh A, Palakal M, Rose T, Swankoski K, Peikes D, McCall N. Medicare beneficiaries with more comprehensive primary care physicians report better primary care. Health Serv Res. 2023;58(2):264-270. [CrossRef]
- Combalia A, Torà-Rocamora I, Diestre-Tomas A, Muñoz-Mahamud E, Grau- Cano J, Prat-Marín A. Influence of claims on the management of an orthopaedic surgery and traumatology service. Revista Española de Cirugía Ortopédica y Traumatología 2022;66(6):469-476. [CrossRef]
- Díaz Gorriti V, Añel Rodríguez RM. Contribución de los pacientes a la mejora de la calidad asistencial. Rev Calid Asist. 2015;30:47-48. [CrossRef]
- Crespo MI, Pérez J, Gonzales MP, Ballesteros AM. Más allá de la hoja de reclamaciones. Análisis cualitativo de las reclamaciones y sugerencias en atención primaria. Revista Enfermería CyL. 2019;11(1):5-11.
- Fernández Navascués AM. New technologies, new health organizations. An. Sist. Sanit. Navar. 2019; 42(2):133-138. doi:10.23938/ASSN.0716. [CrossRef]
Figure 4.
Number of claims for treatment/information per primary care service (n). Year 2022.
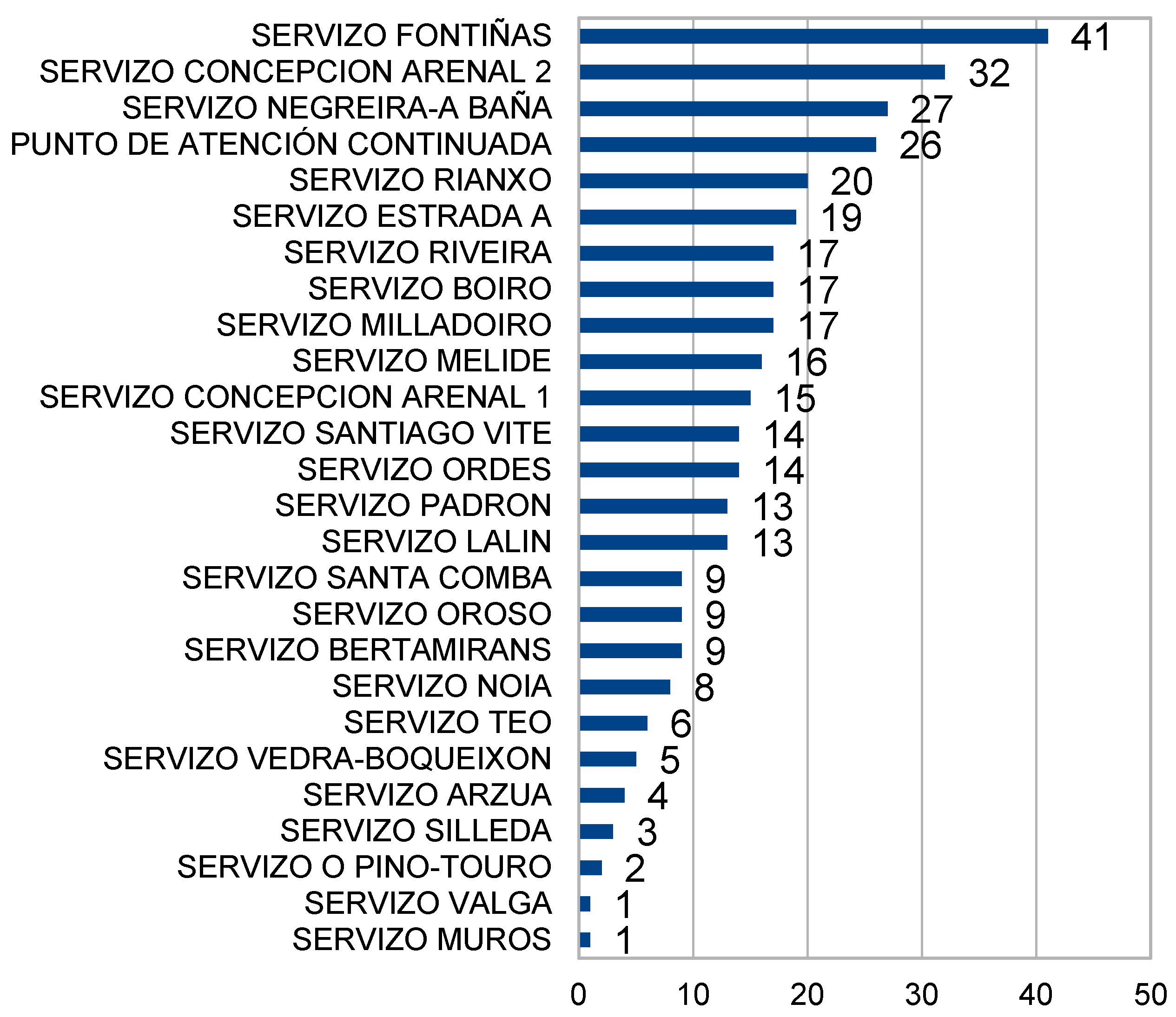
Figure 6.
Professional categories that receive the complaint for treatment (n). Year 2022.
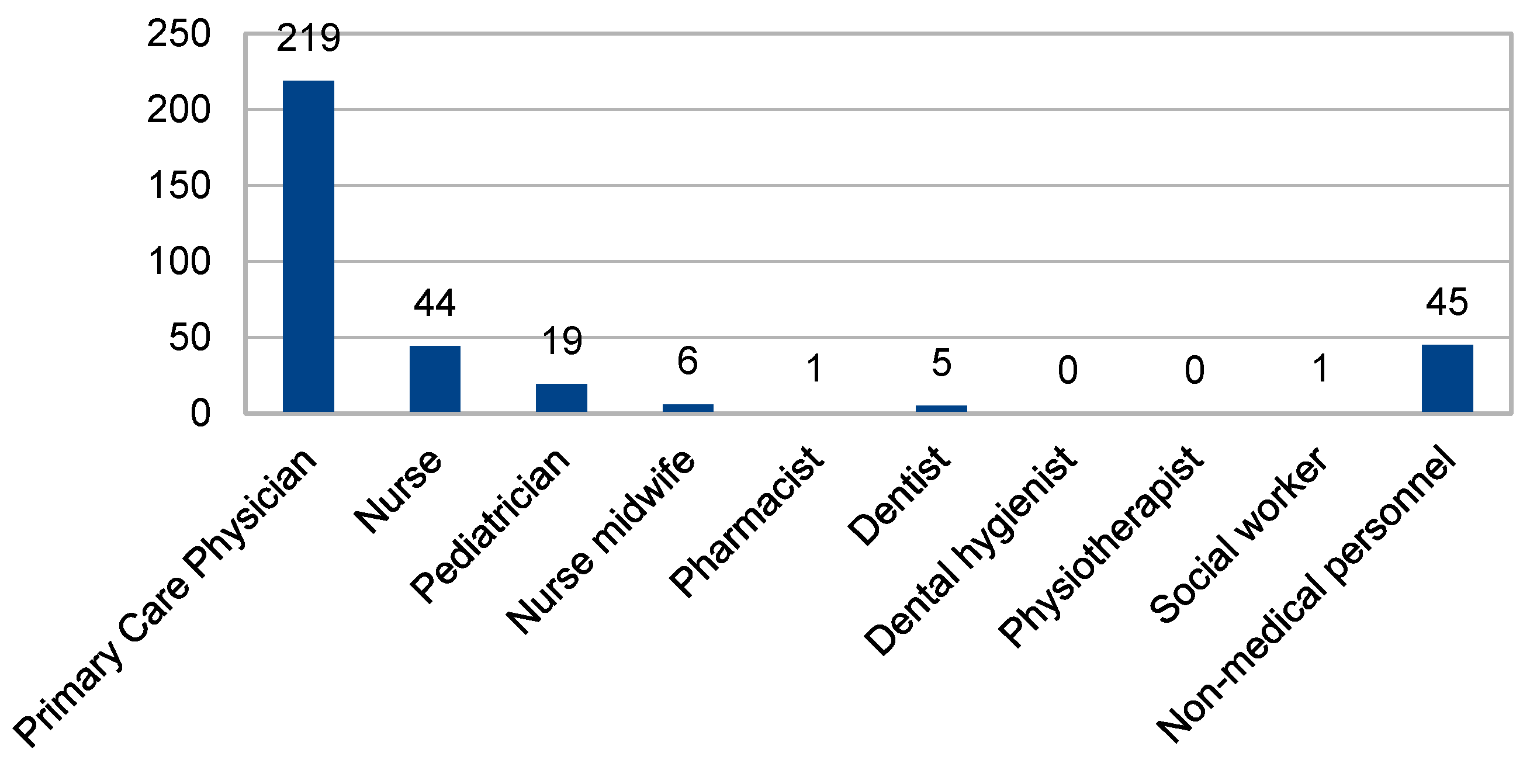

Table 1.
Chi-square analysis between gender and being or not hyperreclaiming.
| 1 Complaint | >1 Complaint | p-value | |
|---|---|---|---|
| Men | 65 (28.5%) | 25 (25.5%) | 0.34 |
| Women | 163 (71.5%) | 73 (74.5%) | |
| Total | 228 | 98 |
Table 2.
Distribution of the number of consultations in primary and hospital care (n). Years 2020-2022.
Table 2.
Distribution of the number of consultations in primary and hospital care (n). Years 2020-2022.
| Level of care and year | mean ± standard deviation |
|---|---|
| Primary care 2020 | 11,7 ± 20,4 |
| Primary care 2021 | 13,9 ± 16,9 |
| Primary care 2022 | 17,1 ± 20,6 |
| Hospital care 2020 | 2,3 ± 5,2 |
| Hospital care 2021 | 2,4 ± 4,4 |
| Hospital care 2022 | 3,1 ± 6,1 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



