Submitted:
31 May 2023
Posted:
01 June 2023
You are already at the latest version
Abstract
The oncological outcomes are improving in gastrointestinal cancer with advancement in systemic therapies, and there is notable potential in combining immunotherapy and radiation therapy (RT)to allow for further improvements in outcomes. Various preclinical and early phase II studies have shown promising synergy with immunotherapy and RT in gastrointestinal cancer. Consolidative nivolumab in esophageal cancer after neoadjuvant chemoradiation (CRT) and complete resection has recently been approved as standard treatment after improved disease free survival in phase III study. Immunotherapy has shown promising results in hepatocellular carcinoma and colorectal cancer as well. We have reviewed the published and ongoing studies of the combinations of immunotherapy and RT in gastrointestinal cancers.
Keywords:
Immunotherapy
; Radiation
1. Introduction
The incidence of gastrointestinal (GI) cancers is increasing worldwide, with diverse epidemiological factors and genetic and epigenetic abnormalities contributing to their development. These cancers are very common globally, and are often associated with high mortality rates[1]. Typically, patients are diagnosed at advanced stages, which poses a challenge for treatment. Although conventional treatments such as chemotherapy, radiation therapy (RT), and surgery are available, they often result in suboptimal outcomes due to local relapses and distant metastases[2]. Therefore, the exploration of innovative therapies, including immunotherapy, has great potential in treating these diseases.
Immunotherapeutic agents have a targeted effect on malignant cells by interacting with immunogens (neoantigens) presented on them, either promoting or inhibiting immune responses[3]. A variety of immunotherapeutic modalities have been used experimentally to treat gastrointestinal (GI) cancers, including immune checkpoint inhibitors (ICI), adoptive cell transfer, chimeric antigen receptor (CAR)-T cell therapy, cancer vaccines, and/or their combinations. Immune checkpoint blockade is a widely used approach that targets various critical molecular targets. The predominant clinically utilized drugs target programmed death-ligand 1 (PD-L1) found on cancer cells and antigen-presenting cells (APCs), programmed cell death protein (PD-1) present on the surface of lymphocytes, and cytotoxic T-lymphocyte associated protein-4 (CTLA-4) found on regulatory T cells (Tregs) or on activated T cells.
Various preclinical, phase II and one phase III studies have shown promising results with ICI in GI cancers in the setting of radiation therapy. We reviewed the present status and future directions of combination of ICI and RT in GI cancers.
2. Mechanism of radiation in combination with immune checkpoint inhibitors
The main premise for checkpoint inhibition involves inducing an immune response when pre-existing T-cells are blocked by PD-1 or CTLA-4 signaling. The programmed cell death 1 (PD-1) receptor and cytotoxic T lymphocyte-associated protein 4 (CTLA-4) are key guardians of immune checkpoints and are mainly expressed in T cells. Both were demonstrated to have a potent inhibitory role in regulating T cell responses[4]. Cancer cells detect that they are under attack from T cells by recognizing IFN-gamma, which leads to the expression of PD-L1 on the surface of cancer cells and in turn inactivates antitumor T cell response by binding to PD-1 (CD279). CTLA-4 (CD152) is a negative regulator of co-stimulation of CD28 that is required for the activation of an antitumor T cell in a lymph node upon recognition of its specific tumor antigen, which is presented by an APC[5].
Radiation is a key modality of antitumor therapy and can modulate the tumor and host immuno-microenvironments[6]. Response to radiation includes the upregulation of the MHC class I expression in tumor cells, and this enhances antigen recognition of cytotoxic CD8 T cells[7]. Dendritic cells play a key role in antigen presentation to T cells. RT can activate dendritic cells through the secretion of pro-inflammatory cytokines including type I and II interferons, interleukin 1 and 2, and tumor necrosis factor-alpha[8]. Co-stimulatory molecules including CD86 and CD70 on the surface of dendritic cells are upregulated by radiation[9]. These radiation-primed pro-inflammatory reactions induce cancer cell death and facilitates presentation of neoantigens, and this subsequently leads to improved priming and activation of dendritic cells and T cells as well[10].
The pro-inflammatory effect of radiation provides a rationale for combining radiation with immune checkpoint inhibitors (ICIs) which block the interaction between PD-1 and PD-L1 or CTLA-4 and B7-1 (CD80)/B7-2 (CD86) resulting in the activation of anti-tumorigenic T cells[11,12]. ICIs are antibodies binding to cell receptors and are not cytotoxic in and of themselves. RT combined with ICIs may increase T cell-mediated cytotoxicity through enhancing antigen presentation and recognition, the release of pro-inflammatory cytokines, and the development of tumor antigens or neoantigens[13].
There are some potential barriers to optimal therapeutic efficacy of RT and ICI which are being explored in future studies. These factors are intrinsic tissue sensitivity to RT, complexities of interferon, TREX1 (DNA exonuclease) expression and differences in abscopal effects[14]
3. Gastroesophageal Cancer
Programmed death-ligand 1 (PD-L1) is expressed in up to 45% and 38% of esophageal and gastric cancers, respectively (at the 1% staining level) [15]. Mouse studies showed that the addition of anti-PD1 to radiation provided the greatest tumor control (both primary and contralateral non-irradiated tumor) compared to anti-PD1 with chemotherapy by increasing the ratio of CD8 T cells to Treg cells and decreasing T cell exhaustion in both the primary and contralateral implanted tumors in mice with esophageal cancers[16]. It also has been reported that RT combined with ICIs can greatly improve anti-tumor activities in radiotherapy-insensitive gastric tumor mouse models by priming the tumor microenvironment[17]. These promising results from preclinical studies led to the initiation of multiple clinical studies testing the combination of RT with ICIs in patients with gastroesophageal cancers (GECs).
- Phase I/II Studies
In a phase I study involving 19 patients with inoperable locally advanced ESCC unsuitable for chemoradiation (CRT), Zhang et al. showed that RT combined with camrelizumab, an anti-PD-1 antibody, was associated with a median overall survival (OS) of 16.7 months and progression-free survival (PFS) of 11.7 months. Patients received 60 Gy RT in 30 fractions over 5 weeks with camrelizumab (200 mg every 2 weeks) starting with RT and continuing for 32 weeks[18]. Peri-operative avelumab in combination with neoadjuvant CRT in 22 patients with stage II/III resectable esophageal and gastroesophageal junction cancers was shown to be well tolerated with no unexpected toxicities in a phase I/II study by Uboha et al. [19]. Zhu et al. in a Phase Ib/II trial involving 31 patients with cT1-3N0-3M0 gastroesophageal junction (GEJ) adenocarcinoma investigated Pembrolizumab-containing trimodality therapy including neoadjuvant pembrolizumab-containing CRT followed by surgical resection and adjuvant pembrolizumab. This study showed acceptable tolerability and 7/31 (22.6%) patients achieved pCR [20]. A Single-arm Phase II Feasibility Trial (PERFECT, n=40) investigating neoadjuvant chemoradiotherapy (nCRT) combined with atezolizumab for resectable esophageal adenocarcinoma showed 83% of patients completed all five cycles of atezolizumab and proceeded to surgery. The pathologic complete response rate was 25% [21]. Wang et al. recently presented an interim analysis of an ongoing prospective study of consolidative camrelizumab following concurrent CRT in unresectable locally advanced ESCC. The majority of patients (11/12) had stable disease with manageable toxicities[22]
- Retrospective Studies
Wie and colleagues evaluated the addition of ICI to CRT in inoperable advanced esophageal cancer patients after first line treatment failure in a small retrospective study. CRT plus PD-1 inhibitor was given in 26 patients and had superior OS as compared with CRT alone in 22 patients (HR 0.19, 95% CI 0.069–0.509, and p = 0.001), with similar PFS[23].
A retrospective study by Nie et al. using propensity score matching for patients with Stage II or higher esophageal cancer who received induction chemotherapy with ICI showed that sequential RT resulted in better PFS (15.7 vs. 5.7 months, p=0.002) and OS (15.7 vs. 12 months, p=0.036) than no RT [24]. Most patients received at least 4 cycles of chemotherapy and ICI (carmelizumab or pembrolizumab). RT with ICI was given in 55 patients and consisted of 60 Gy in 30 fractions. Peng et al. presented a retrospective study of 137 patients with unresectable locally advanced esophageal squamous cell carcinoma and found that induction ICI plus chemotherapy followed by definitive CRT yielded more favorable median OS (not reached vs. 25.2 months) and PFS (28.8 vs. 15.9 months, p=0.128) compared with definitive CRT alone[25].
- Phase III Study
CheckMate-577 (n=794) showed adjuvant nivolumab increased the median DFS to 22.4 months as compared to 11.0 months (HR 0.69, p<0.001) in esophageal/ gastroesophageal cancer after neoadjuvant CRT and R0 resection with residual disease at time of surgery[26]. The risk of distant recurrence or death was 26% lower and distant metastasis–free survival was 10.7 months longer with adjuvant nivolumab than with placebo.
- Ongoing Studies
An ongoing Phase II study (NCT03257163) is evaluating pre-operative pembrolizumab followed by adjuvant immunotherapy and CRT in Mismatch-Repair Deficient (dMMR), Epstein - Barr virus positive and PD-L1 positive gastric cancers. Another ongoing phase II/III study (EA2174) is evaluating preoperative nivolumab with CRT vs pre-op CRT alone in locally advanced esophageal GEC adenocarcinoma followed by post-surgery adjuvant ICI (nivolumab vs nivolumab/ipilimumab).
Published studies of combination of ICI and RT in gastroesophageal cancers are summarized in Table 1, and selected ongoing studies are summarized in Table 2. Representative pre-treatment and post-treatment positron emission tomography (PET) images of a patient (high PDL1) who received neoadjuvant CRT (carbopaltin/ paclitaxel/ RT) with concurrent nivolumab is shown in Figure 1. This patient had a pCR after surgery.
4. Hepatocellular carcinoma (HCC)
Hepatocellular carcinoma (HCC) is the most prevalent primary liver cancer globally [27]. Surgical resection or liver transplant in the early stages of HCC results in 5-year OS rates of 50% to 80%[28]. However, most patients are not eligible for surgical treatment due to advanced disease, poor hepatic reserve, or medical contraindications. In cases where the disease is confined to the liver, liver-directed therapies such as transarterial radioembolization (TARE) or chemoembolization (TACE), radiofrequency ablation (RFA), microwave ablation (MWA), or stereotactic body RT (SBRT) or hypofractionated RT can be used as a definitive treatment, bridging therapy, or to downstage to transplant eligibility [28]. Fractionated RT has yielded a response rate of 50-90% with 1-year OS of 50-100%, which has improved with modern SBRT regimens and techniques to a 2-year local control of 70-95% [29].
Although there are various liver-directed therapies available, the survival rates for patients with unresectable HCC remain low. Furthermore, in advanced disease, multitarget tyrosine kinase inhibitors (TKI), such as sorafenib and lenvatinib, have an OS of approximately 1 year or less [30].
- ICI alone studies in HCC
In cases of advanced or unresectable HCC, ICI has shown improved results when compared to TKI. IMbrave150 demonstrated 1-yr OS of 67.2% with atezolizumab plus the anti-angiogenic, bevacizumab compared to 54.6% with sorafenib [31]. Median PFS was 6.8 months with atezolizumab-bevacizumab and 4.3 months with sorafenib (HR 0.59, p<0.001). The Himalaya 3-arm trial compared tremelimumab (anti–CTLA-4)/ durvalumab (anti-PDL1) combination to durvalumab monotherapy or sorafenib alone in unresectable HCC. Most patients had Child Pugh A (approx. 98%) grade and BCLC C (approx. 80%) stage. Objective response rates were higher in combination ICI arm as compared to sorafenib arm (20% vs 5%). The 3-yr OS with combination of limited-dose tremelimumab (anti–CTLA-4) and durvalumab (anti-PDL1) was significantly superior to sorafenib alone (30.7% vs 20.2%; HR 0.78, p=0.0035) [32]. Therefore, the combination of local and systemic therapies for HCC is a subject of great research interest aimed at achieving better outcomes.
- RT with TKI in HCC
RTOG 1112 investigated the impact of adding SBRT (27.5- 50Gy in 5 fractions) to sorafenib in advanced HCC, however, the accrual was closed early as the standard of care systemic therapy changed. The results of the accrued patients showed that adding SBRT improved OS (15.8 vs 12.3 months, HR 0.77, p=0.0554) and PFS (9.2 vs 5.5 months, HR 0.55, 2-sided p=0.0001) in patients with advanced HCC, compared to sorafenib alone. The OS was statistically significantly improved for the SBRT/sorafenib arm after adjusting for variables such as performance status, Child Pugh score and degree of vascular invasion (HR=0.72, 2-sided Cox p=0.042). The addition of SBRT did not increase treatment related grade 3+ adverse events [33].
- RT with ICI in HCC: Phase I study
Studies combining RT with ICIs are limited. A Phase 1 randomized trial in 14 patients with advanced or unresectable HCC compared liver SBRT (40 Gy in 5 fractions) followed by either nivolumab alone or nivolumab plus ipilimumab. All patients had Child Pugh A grade, 4 had extra-hepatic disease and 4 had tumor thrombus. Two patients had received prior systemic therapy with TKI and 2 had received prior liver directed therapy. The median radiated target lesion size was 6.8 cm (range, 1.5-13.6 cm). The nivolumab plus ipilimumab arm had better overall response (23-87% vs 0-39%), median PFS (11.6 vs 2.7 months) and median OS (41.6 vs 4.7 months), not statistically significant. The 3-year OS with combination immunotherapy was 57%. Dose-limiting toxicities within 6 months occurred in 1 of 6 patients in the nivolumab arm and 1 of 7 patients in the nivolumab plus ipilimumab arm. The Grade 3 hepatotoxicity was seen in 3 patients in combination immunotherapy arm and 1 patient in nivolumab alone arm. The results showed that multimodal therapy was safe with favorable outcomes in patients with SBRT with nivolumab plus ipilimumab [34].
- RT with ICI in HCC: Retrospective Data
SBRT followed by nivolumab in unresectable HCC in a retrospective case series of 5 patients by Chiang et al. demonstrated 2 complete responses and 3 partial responses and no tumor progression after a median follow-up of 14.9 months [35]. In a follow-up study of 16 patients by the same group, the use of SBRT in combination with nivolumab demonstrated 1-year PFS of 93.3% and 1 year OS of 93.8% [36].
- RT with ICI in HCC: Ongoing studies
Other ongoing trials include NCT03482102, a single-arm phase 2 trial of durvalumab and tremelimumab with SBRT, and NCT03316872, a single-arm phase 2 study of pembrolizumab with SBRT and NCT05366829, a phase 2 study of hypofractionated RT followed by tislelizumab. The published results and ongoing trials are summarized in Table 3 and Table 4, respectively.
- TARE with ICI in HCC
TARE with Y-90 (Yttrium - 90) induces both local and systemic immune activation that corresponded to the sustained response[37]. Rivoltini et al showed that a significant proportion of Y- 90 induced CD4+ and CD8+ T cells expressed high levels of the inhibitory checkpoints markers PD-1[38] . A phase 2 study of 42 patients with unresectable HCC treated with TARE followed by nivolumab showed 41.5% objective response rates (ORR) with median time to progression (TTP) of 8.8 months and median OS of 20.9 months[39]. A similar phase 2 study of 40 patients of advanced HCC treated with TARE followed by nivolumab by Tai et al showed ORR of 30.6%[40]. Currently undergoing ROWAN study is a prospective, multicentric, randomized, Phase 2 study to assess the durability of local tumor control in HCC patients who receive TARE followed by durvalumab and tremelimumab, compared to those who receive TARE alone in HCC patients not eligible for or who have declined treatment with resection and/or ablation or liver transplant.
5. Cholangiocarcinoma (CCA)
Adjuvant RT (45-54 Gy in 1.8-2.0 Gy per fractions) may be used in Cholangiocarcinoma (CCA) following surgery with positive margins and is considered for >T3 or lymph node positive disease [41,42]. The role of RT (37.5 Gy – 67.5 Gy in 15 fractions) is currently being investigated in locally advanced CCA following chemotherapy as part of the NRG GI 001 trial .
- ICI in advanced CCA
In advanced-stage CCA, the addition of durvalumab to gemcitabine/cisplatin (GC) chemotherapy followed by maintenance durvalumab showed improved 2-year OS (24.9% vs 10.4%; HR 0.8, p = 0.021) as compared to GC chemotherapy with placebo in the TOPAZ-1 (n=685) clinical trial [43]. The objective response rates were increased in the durvalumab + GC arm to 26.7% as compared to 18.7% in the GC alone arm. Thus, the addition of RT to systemic therapy (including ICI) is an interesting prospect in advanced CCA and has been explored in case reports [44,45].
- RT with ICI in CCA: Phase II Studies
Currently, there are a few phase II clinical trials aimed at assessing the effectiveness and safety of combination of RT and ICI. The CORRECT trial is comparing radiation (SBRT or IMRT) plus ICI (camrelizumab) in the first line against standard chemotherapy, GC in unresectable intrahepatic CCA (NCT03898895). Another trial is underway to investigate the combination of tislelizumab and RT (using either IMRT or SBRT) in the second line settings post chemotherapy and no ICI (NCT04866836). Both of these trials were designed prior to the TOPAZ-1 trial, and there is now a need for new trials to compare RT plus ICI with GC/durvalumab or post-ICI therapy. The ongoing studies are tabulated in Table 5.
6. Pancreas cancer
Pancreatic cancer is the third most common cause of cancer mortality in the United States [27]. Advancements have been made over the years in the management of pancreatic cancer, including improvements in both systemic and local therapies, along with dose escalation with IMRT and SBRT. Neoadjuvant therapy may be employed in cases of resectable pancreas cancer (RPC). For borderline resectable pancreas cancer (BRPC), neoadjuvant therapy is given to enhance resection rates, achieve negative margin status and ensure receipt of therapy, as 40% of patients do not complete adjuvant therapy after surgical resection (SWOG S1505)[46]. However, the resection rate stands at approximately 60-75% after neoadjuvant therapy, with negative margins being achieved in 60-80% of resected patients [46,47]. The addition of ICI to neoadjuvant CRT has been explored in a few small studies.
- RT with ICI in RPC and BRPC
Rahma et al. conducted a phase II study of 37 patients with RPC and BRPC. Patients were randomized to receive either CRT alone prior to resection or concurrent pembrolizumab with CRT (50.4 Gy in 28 fractions plus Capecitabine) [48]]. After neoadjuvant therapy, 9/24 (37.5%) patients in the ICI arm had unresectable disease compared to 4/13 (30.8%) patients in the control arm with similar median OS (27.8 vs 24.3 months, p = 0.68). The most common grade 3+ toxicities were lymphopenia (29% vs. 31%) and diarrhea (8% vs. 0%). The initial findings indicate that the combination of CRT and Pembrolizumab was well-tolerated, but its impact on the densities of TILs and other immune cell populations within the tumor was minimal. Currently, larger prospective phase II trials are being conducted to gain a better understanding of the potential benefits of combining immunotherapy with chemotherapy and RT in the neoadjuvant setting.
- RT with ICI in LAPC
There are various challenges in delivering radiation in patients with locally advanced pancreatic cancer (LAPC) due to factors such as tumor size, location, invasion into adjacent bowel, inability to control internal motion, and limited access to on-board imaging or adaptive RT. The role of immunotherapy in combination with RT is also an active area of investigation in LAPC. Zhu et al. conducted a phase II randomized trial on 170 patients with locally recurrent pancreatic cancer after resection and adjuvant chemotherapy. There was an OS benefit in patients who received SBRT (40 Gy in 5 fractions), pembrolizumab, and trametinib in comparison to those who underwent SBRT (40 Gy in 5 fractions) in combination with gemcitabine. The median OS was 14.9 vs. 12.8 months (HR = 0.69, p = 0.02) [49]].
There are other ongoing clinical trials examining the safety and efficacy of combination immunotherapy with RT in pancreas cancer, as shown in Table-6.

Table 6.
Ongoing studies in Pancreas cancer.
| NCT Number | Disease status | Interventions | Outcome Measures | Phase |
|---|---|---|---|---|
| NCT04098432 | Locally Advanced Unresectable Pancreatic Adenocarcinoma | SBRT + Nivolumab | Safety | 1/2 |
| NCT04247165 | Pancreatic Cancer. | SBRT + Ipilimumab + Nivolumab | PFS | 1/2 |
| NCT04390399 | Locally Advanced or Metastatic Pancreatic Cancer | SBRT + Chemo +/- IT | PFS/ ORR | 2 |
| NCT04361162 | MSS Pancreatic Cancer | RT + Nivolumab + Ipilimumab | ORR | 2 |
| NCT03563248 | Localized Pancreatic Cancer | FOLFIRINOX + SBRT + Surgery +/- Nivolumab +/- Losartan | R0 Resection | 2 |
| NCT05116917 | Pancreatic Cancer. | SBRT + Nivolumab + Influenza Vaccine | ORR | 2 |
| NCT03161379 | Borderline Resectable Pancreatic Cancer | SBRT + Nivolumab + GVAX Pancreas Vaccine | ORR | 2 |
7. Colorectal Cancer
Colorectal cancer (CRC) is the fourth most frequently diagnosed cancer and the second leading cause of cancer death in the United States [27]. Around 5% of patients with metastatic CRC have either germline or somatic mutations in DNA mismatch repair (MMR) genes[50]. The occurrence of mismatch repair deficiency (dMMR) or Microsatellite instability-high (MSI-H) is linked to DNA repair deficiency leading to a higher mutational load. Tumors that exhibit dMMR/MSI-H have demonstrated a significant response to ICI treatment, as opposed to proficient MMR (pMMR) or microsatellite-stable (MSS) tumors due to the large number of neoantigens they express [51]. Based on the Checkmate 142 trial, the combinational therapy of nivolumab with ipilimumab is approved for metastatic CRC with dMMR/MSI-H [52]. Pembrolizumab has been demonstrated to improve outcomes in advanced metastatic CRC as first-line setting for dMMR/MSI-H (KEYNOTE – 177) [53]. The positive outcomes of ICI in mCRC have led to its exploration in non-metastatic settings as well.
- ICI alone in CRC: Phase II Studies
The NICHE study is a Phase II study which investigated neoadjuvant ipilimumab and nivolumab for CRC with dMMR/MSI-H or pMMR/MSS. Forty patients with 21 dMMR and 20 pMMR tumors were treated with a single dose of ipilimumab and two doses of nivolumab before surgery. Out of the 20 dMMR tumors, all of them showed pathological responses, with 19 demonstrating major pathological responses (MPR) and 12 showing pathological complete responses (pCR). In the case of pMMR tumors, only 4 out of 15 exhibited pathological responses, with 3 MPR and 1 partial response [54]. NICHE-2 study investigated the same neoadjuvant immunotherapy regimen of ipilimumab and nivolumab in 112 patients with non-metastatic dMMR advanced colon cancer. Most (89%) of patients has stage III disease with 77% as high-risk stage III, and 64% had T4 tumors. Recently presented results showed MPR in 95%, including pCR in 67% of patients. At a median follow-up of 13 months (range 1-57), none of the patients had disease recurrence [55].
Cercek et al. conducted a phase II study on patients with dMMR/MSI-H stage II or III rectal cancer to explore the efficacy of neoadjuvant therapy with dostarlimab [56]. As part of the trial, the patients were treated with dostarlimab for a period of six months, followed by chemoRT and surgery for those with residual disease. All (n=12) patients who participated in the trial achieved a complete clinical response to dostarlimab, and none of them required CRT or surgery at minimum 6 month follow up (range 6-25 months).
- RT with ICI in CRC: Phase I/II Studies
In pre-clinical studies, xenograft models of CRC have demonstrated excellent synergy between RT and ICI [57,58]. Patients with locally advanced rectal cancer were treated with CRT (50.4 Gy in 28 fractions) with capecitabine followed by nivolumab as part of the Phase I/II VOLTAGE trial. Among the patients with pMMR/MSS, 30% achieved pCR, while 60% of the dMMR/MSI-H patients achieved pCR [59].
The NRG-GI002 trial is currently awaiting final results. It is a randomized phase II study that examines the effects of total neoadjuvant therapy (TNT) with FOLFOX treatment followed by concurrent CRT (50.4 Gy in 28 fractions) with capecitabine. In the experimental arms, pembrolizumab or veliparib was added to CRT (NCT02921256). The addition of pembrolizumab for a non-biomarker-selected group of rectal cancer patients was associated with improved 3-year OS (95% vs 87%; HR 0.35, p =0.04) with similar 3-year DFS of 64%. Veliparib did not improve 3 year outcomes [60].
- RT with ICI in CRC: Ongoing Studies
An intriguing study (NCT04304209) is currently underway to investigate the impact of sintilimab on locally advanced rectal cancer, based on MMR/MSI status. In cohort A, patients with dMMR/MSI-H will receive neoadjuvant sintilimab and undergo surgery or observation and adjuvant therapy, while in cohort B, patients with pMMR/MSS will receive neoadjuvant CRT (45-50 Gy in 25 fractions) ± sintilimab and undergo surgery or observation and adjuvant therapy.
Neo-adjuvant nivolumab/ipilimumab combination with short course pelvic RT (SCRT) 25 Gy in 5 fractions is currently under investigation in locally advanced rectal cancer in phase II EOCG-ACRIN 2201 study (NCT04751370), whereas another phase II clinical trial (NCT04109755) is studying the impact of combining pembrolizumab with SCRT (25 Gy in 5 fractions) in the neo-adjuvant treatment of localized dMMR/MSI RC. The outcomes of these forthcoming clinical trials will provide insight into the role of radio-immunotherapy in the management of RC (Table 7).
8. Anal Cancer
Anal cancer accounts for approximately 3% of all GI cancers in United States [27]. Standard CRT (42 – 54 Gy in 28-30 fractions) is highly curative in treating early and locally advanced anal cancer, but about 30% of patients experience relapse or persistent disease [61]. Because of the association of HPV with anal cancer, as it is with head and neck cancer and cervical cancer, the use of ICI in locally advanced and metastatic anal cancer is being investigated [61].
Promising results have been obtained in patients with metastatic and surgically unresectable recurrent anal cancer who have received ICI treatment. In a multicentric phase 2 trial by Morris et al., previously treated patients with unresectable metastatic anal cancer achieved a 24% objective response rate with nivolumab, and no serious adverse events were reported [62]. Pembrolizumab was investigated in a phase 2 study, KEYNOTE-158, as a treatment for previously treated advanced anal squamous cell carcinoma. The study showed that 11% of patients had an objective response, with 15% of patients with PD-L1-positive tumors and 3% of patients with PD-L1-negative tumors responding positively. Additionally, 18% of patients experienced grade 3-4 adverse events [63]]
The positive outcomes observed in patients with advanced anal squamous cell carcinoma have resulted in clinical trials that assess the potential of ICI in these patients. A completed phase III trial ECOG-ACRIN 2165 is assessing the role of nivolumab after CRT (45-54 Gy in 30 fractions) in patients with high-risk stage II-IIIB anal cancer (NCT03233711). Patients were randomized to up to 6 months of adjuvant nivolumab vs. observation after CRT with the primary endpoint of DFS. Results are awaited for this study. The currently ongoing studies are shown in Table 8
9. Limitations
The combination of RT and ICI in GI cancer is still evolving. The duration of therapy, sequencing of therapy and treatment for recurrence after ICI is still under investigation. There should be awareness of immune mediated complications, especially colitis in patients receiving RT and ICI for GI cancer, and early intervention is needed to avoid high grade toxicities. There are some potential barriers to optimal therapeutic efficacy of RT and ICI which are being explored in future studies. The collection of quality of life (QOL) data is also ongoing.
10. Conclusions
The combination of radiation therapy and immune checkpoint inhibitors is increasingly being tested to improve oncological outcomes in gastrointestinal cancers. The available published studies show encouraging results with acceptable toxicity profiles. The optimal timing of RT and ICI is still evolving. Currently, ICI after RT has shown the most benefit, as in Checkmate 577 in esophageal cancer. There is an increasing interest in RT and ICI in dMMR/MSI-H CRC and gastric cancers, as well in the neoadjuvant or pre-operative setting. The results of the ongoing prospective studies will determine the role of combination of ICI and RT in GI cancers.
Supplementary Materials
None
Author Contributions
“Conceptualization, SKJ, RK JK; writing—original draft preparation, SKJ, RK, JK ; writing—review and editing, all authors; supervision, SJ, MD, HH; All authors have read and agreed to the published version of the manuscript.”
Funding
This research received no external funding
Conflicts of Interest
The authors declare no conflict of interest related to this review article.
References
- Lu, L.; Mullins, C.S.; Schafmayer, C.; Zeißig, S.; Linnebacher, M. A Global Assessment of Recent Trends in Gastrointestinal Cancer and Lifestyle-Associated Risk Factors. Cancer Commun (Lond) 2021, 41, 1137–1151. [Google Scholar] [CrossRef] [PubMed]
- Siegel, R.L.; Miller, K.D.; Fuchs, H.E.; Jemal, A. Cancer Statistics, 2022. CA Cancer J Clin 2022, 72, 7–33. [Google Scholar] [CrossRef] [PubMed]
- Kraehenbuehl, L.; Weng, C.-H.; Eghbali, S.; Wolchok, J.D.; Merghoub, T. Enhancing Immunotherapy in Cancer by Targeting Emerging Immunomodulatory Pathways. Nat Rev Clin Oncol 2022, 19, 37–50. [Google Scholar] [CrossRef] [PubMed]
- Ribas, A.; Wolchok, J.D. Cancer Immunotherapy Using Checkpoint Blockade. Science 2018, 359, 1350–1355. [Google Scholar] [CrossRef] [PubMed]
- Seidel, J.A.; Otsuka, A.; Kabashima, K. Anti-PD-1 and Anti-CTLA-4 Therapies in Cancer: Mechanisms of Action, Efficacy, and Limitations. Front Oncol 2018, 8, 86. [Google Scholar] [CrossRef] [PubMed]
- Burnette, B.; Weichselbaum, R.R. Radiation as an Immune Modulator. Semin Radiat Oncol 2013, 23, 273–280. [Google Scholar] [CrossRef]
- Park, B.; Yee, C.; Lee, K.-M. The Effect of Radiation on the Immune Response to Cancers. Int J Mol Sci 2014, 15, 927–943. [Google Scholar] [CrossRef]
- Van Limbergen, E.J.; De Ruysscher, D.K.; Olivo Pimentel, V.; Marcus, D.; Berbee, M.; Hoeben, A.; Rekers, N.; Theys, J.; Yaromina, A.; Dubois, L.J.; et al. Combining Radiotherapy with Immunotherapy: The Past, the Present and the Future. Br J Radiol 2017, 90, 20170157. [Google Scholar] [CrossRef]
- Gupta, A.; Probst, H.C.; Vuong, V.; Landshammer, A.; Muth, S.; Yagita, H.; Schwendener, R.; Pruschy, M.; Knuth, A.; van den Broek, M. Radiotherapy Promotes Tumor-Specific Effector CD8+ T Cells via Dendritic Cell Activation. J Immunol 2012, 189, 558–566. [Google Scholar] [CrossRef]
- Wang, Y.; Deng, W.; Li, N.; Neri, S.; Sharma, A.; Jiang, W.; Lin, S.H. Combining Immunotherapy and Radiotherapy for Cancer Treatment: Current Challenges and Future Directions. Front Pharmacol 2018, 9, 185. [Google Scholar] [CrossRef]
- Sharabi, A.B.; Lim, M.; DeWeese, T.L.; Drake, C.G. Radiation and Checkpoint Blockade Immunotherapy: Radiosensitisation and Potential Mechanisms of Synergy. Lancet Oncol 2015, 16, e498–509. [Google Scholar] [CrossRef] [PubMed]
- Sharabi, A.B.; Nirschl, C.J.; Kochel, C.M.; Nirschl, T.R.; Francica, B.J.; Velarde, E.; Deweese, T.L.; Drake, C.G. Stereotactic Radiation Therapy Augments Antigen-Specific PD-1-Mediated Antitumor Immune Responses via Cross-Presentation of Tumor Antigen. Cancer Immunol Res 2015, 3, 345–355. [Google Scholar] [CrossRef]
- Germino, E.A.; Govindarajan, A.; Sedrak, M.S.; Li, D.; Amini, A. Multimodality Treatment with Radiotherapy and Immunotherapy in Older Adults: Rationale, Evolving Data, and Current Recommendations. Semin Radiat Oncol 2022, 32, 142–154. [Google Scholar] [CrossRef] [PubMed]
- Pointer, K.B.; Pitroda, S.P.; Weichselbaum, R.R. Radiotherapy and Immunotherapy: Open Questions and Future Strategies. Trends Cancer 2022, 8, 9–20. [Google Scholar] [CrossRef]
- Badiyan, S.; Kaiser, A.; Eastman, B.; Forsthoefel, M.; Zeng, J.; Unger, K.; Chuong, M. Immunotherapy and Radiation Therapy for Gastrointestinal Malignancies: Hope or Hype? Transl Gastroenterol Hepatol 2020, 5, 21. [Google Scholar] [CrossRef] [PubMed]
- Oh, P.; Du, K.L.; Leichman, L.; Aifantis, I. PD-1 Blockade Enhances the Efficacy of Chemoradiation in a Mouse Model of Esophageal Cancer. International Journal of Radiation Oncology*Biology*Physics 2016, 96, S127–S128. [Google Scholar] [CrossRef]
- Hong, S.; Bi, M.; Yu, H.; Yan, Z.; Wang, H. Radiation Therapy Enhanced Therapeutic Efficacy of Anti-PD1 against Gastric Cancer. J Radiat Res 2020, 61, 851–859. [Google Scholar] [CrossRef]
- Zhang, W.; Yan, C.; Gao, X.; Li, X.; Cao, F.; Zhao, G.; Zhao, J.; Er, P.; Zhang, T.; Chen, X.; et al. Safety and Feasibility of Radiotherapy Plus Camrelizumab for Locally Advanced Esophageal Squamous Cell Carcinoma. Oncologist 2021, 26, e1110–e1124. [Google Scholar] [CrossRef]
- Uboha, N.V.; Eickhoff, J.C.; Maloney, J.D.; McCarthy, D.; DeCamp, M.; Deming, D.A.; LoConte, N.K.; Matkowskyj, K.A.; Patel, M.A.; Hurst, N.; et al. Phase I/II Trial of Perioperative Avelumab in Combination with Chemoradiation (CRT) in the Treatment of Stage II/III Resectable Esophageal and Gastroesophageal Junction (E/GEJ) Cancer. JCO 2022, 40, 4034–4034. [Google Scholar] [CrossRef]
- Zhu, M.; Chen, C.; Foster, N.R.; Hartley, C.; Mounajjed, T.; Salomao, M.A.; Fruth, B.F.; Beamer, S.E.; Kim, Y.; Harrington, S.M.; et al. Pembrolizumab in Combination with Neoadjuvant Chemoradiotherapy for Patients with Resectable Adenocarcinoma of the Gastroesophageal Junction. Clin Cancer Res 2022, 28, 3021–3031. [Google Scholar] [CrossRef]
- van den Ende, T.; de Clercq, N.C.; van Berge Henegouwen, M.I.; Gisbertz, S.S.; Geijsen, E.D.; Verhoeven, R.H.A.; Meijer, S.L.; Schokker, S.; Dings, M.P.G.; Bergman, J.J.G.H.M.; et al. Neoadjuvant Chemoradiotherapy Combined with Atezolizumab for Resectable Esophageal Adenocarcinoma: A Single-Arm Phase II Feasibility Trial (PERFECT). Clin Cancer Res 2021, 27, 3351–3359. [Google Scholar] [CrossRef] [PubMed]
- Wang, J.; Cheng, Y.; Wu, Y.; Cao, F.; Liu, Q.; Gao, G. Efficacy and Safety of Consolidative Camrelizumab Following Definitive Concurrent Chemoradiotherapy in Patients with Locally Advanced Esophageal Squamous Cell Cancer. Annals of Oncology 2022, 33, S1124. [Google Scholar] [CrossRef]
- Wei, T.; Ti, W.; Song, Q.; Cheng, Y. Study of PD-1 Inhibitors in Combination with Chemoradiotherapy/Chemotherapy in Patients with Esophageal Squamous Carcinoma. Curr Oncol 2022, 29, 2920–2927. [Google Scholar] [CrossRef] [PubMed]
- Nie, Y.; Yao, G.; Li, L.; Feng, A.; Zhang, W.; Xu, X.; Li, Q.; Yang, Z. Effects of Radiotherapy on Survival of Esophageal Cancer Patients Receiving Immunotherapy: Propensity Score Analysis and Nomogram Construction. Cancer Manag Res 2022, 14, 2357–2371. [Google Scholar] [CrossRef]
- Peng, F.; Lian, H.M.; Niu, S.Q.; Liufu, W.J.; Yu, T.T.; Bao, Y. Induction Anti-PD-1 Immunotherapy plus Chemotherapy Followed by Definitive Chemoradiation Therapy in Locally Advanced Esophageal Squamous Cell Carcinoma: A Real-World Retrospective Study. International Journal of Radiation Oncology*Biology*Physics 2022, 114, e165. [Google Scholar] [CrossRef]
- Kelly, R.J.; Ajani, J.A.; Kuzdzal, J.; Zander, T.; Van Cutsem, E.; Piessen, G.; Mendez, G.; Feliciano, J.; Motoyama, S.; Lièvre, A.; et al. Adjuvant Nivolumab in Resected Esophageal or Gastroesophageal Junction Cancer. N Engl J Med 2021, 384, 1191–1203. [Google Scholar] [CrossRef]
- Sung, H.; Ferlay, J.; Siegel, R.L.; Laversanne, M.; Soerjomataram, I.; Jemal, A.; Bray, F. Global Cancer Statistics 2020: GLOBOCAN Estimates of Incidence and Mortality Worldwide for 36 Cancers in 185 Countries. CA Cancer J Clin 2021, 71, 209–249. [Google Scholar] [CrossRef]
- Benson, A.B.; D’Angelica, M.I.; Abbott, D.E.; Anaya, D.A.; Anders, R.; Are, C.; Bachini, M.; Borad, M.; Brown, D.; Burgoyne, A.; et al. Hepatobiliary Cancers, Version 2.2021, NCCN Clinical Practice Guidelines in Oncology. J Natl Compr Canc Netw 2021, 19, 541–565. [Google Scholar] [CrossRef] [PubMed]
- Sayan, M.; Yegya-Raman, N.; Greco, S.H.; Gui, B.; Zhang, A.; Chundury, A.; Grandhi, M.S.; Hochster, H.S.; Kennedy, T.J.; Langan, R.C.; et al. Rethinking the Role of Radiation Therapy in the Treatment of Unresectable Hepatocellular Carcinoma: A Data Driven Treatment Algorithm for Optimizing Outcomes. Front Oncol 2019, 9, 345. [Google Scholar] [CrossRef]
- Falette Puisieux, M.; Pellat, A.; Assaf, A.; Ginestet, C.; Brezault, C.; Dhooge, M.; Soyer, P.; Coriat, R. Therapeutic Management of Advanced Hepatocellular Carcinoma: An Updated Review. Cancers (Basel) 2022, 14, 2357. [Google Scholar] [CrossRef]
- Finn, R.S.; Qin, S.; Ikeda, M.; Galle, P.R.; Ducreux, M.; Kim, T.-Y.; Kudo, M.; Breder, V.; Merle, P.; Kaseb, A.O.; et al. Atezolizumab plus Bevacizumab in Unresectable Hepatocellular Carcinoma. N Engl J Med 2020, 382, 1894–1905. [Google Scholar] [CrossRef] [PubMed]
- Abou-Alfa, G.K.; Lau, G.; Kudo, M.; Chan, S.L.; Kelley, R.K.; Furuse, J.; Sukeepaisarnjaroen, W.; Kang, Y.-K.; Van Dao, T.; De Toni, E.N.; et al. Tremelimumab plus Durvalumab in Unresectable Hepatocellular Carcinoma. NEJM Evidence 2022, 1. [Google Scholar] [CrossRef]
- Dawson, L.A.; Winter, K.; Knox, J.; Zhu, A.X.; Krishnan, S.; Guha, C.; Kachnic, L.A.; Gillin, M.T.; Hong, T.S.; Craig, T.; et al. NRG/RTOG 1112: Randomized Phase III Study of Sorafenib vs. Stereotactic Body Radiation Therapy (SBRT) Followed by Sorafenib in Hepatocellular Carcinoma (HCC) (NCT01730937). International Journal of Radiation Oncology*Biology*Physics 2022, 114, 1057. [Google Scholar] [CrossRef]
- Juloori, A.; Katipally, R.R.; Lemons, J.M.; Singh, A.K.; Iyer, R.; Robbins, J.R.; George, B.; Hall, W.A.; Pitroda, S.P.; Arif, F.; et al. Phase 1 Randomized Trial of Stereotactic Body Radiation Therapy Followed by Nivolumab plus Ipilimumab or Nivolumab Alone in Advanced/Unresectable Hepatocellular Carcinoma. Int J Radiat Oncol Biol Phys 2023, 115, 202–213. [Google Scholar] [CrossRef] [PubMed]
- Chiang, C.-L.; Chan, A.C.Y.; Chiu, K.W.H.; Kong, F.-M.S. Combined Stereotactic Body Radiotherapy and Checkpoint Inhibition in Unresectable Hepatocellular Carcinoma: A Potential Synergistic Treatment Strategy. Front Oncol 2019, 9, 1157. [Google Scholar] [CrossRef]
- Chiang, C.L.; Chan, A.C.Y.; Chiu, W.H.K.; Kong, F.M. Combined Stereotactic Body Radiotherapy and Immunotherapy (SBRT-IO) vs. TACE in Locally Advanced Hepatocellular Carcinoma (HCC): Propensity Score Matching Analysis. International Journal of Radiation Oncology*Biology*Physics 2021, 111, e35–e36. [Google Scholar] [CrossRef]
- Chew, V.; Lee, Y.H.; Pan, L.; Nasir, N.J.M.; Lim, C.J.; Chua, C.; Lai, L.; Hazirah, S.N.; Lim, T.K.H.; Goh, B.K.P.; et al. Immune Activation Underlies a Sustained Clinical Response to Yttrium-90 Radioembolisation in Hepatocellular Carcinoma. Gut 2019, 68, 335–346. [Google Scholar] [CrossRef]
- Rivoltini, L.; Bhoori, S.; Camisaschi, C.; Bergamaschi, L.; Lalli, L.; Frati, P.; Citterio, D.; Castelli, C.; Mazzaferro, V. Y90-Radioembolisation in Hepatocellular Carcinoma Induces Immune Responses Calling for Early Treatment with Multiple Checkpoint Blockers. Gut 2023, 72, 406–407. [Google Scholar] [CrossRef]
- de la Torre-Aláez, M.; Matilla, A.; Varela, M.; Iñarrairaegui, M.; Reig, M.; Lledó, J.L.; Arenas, J.I.; Lorente, S.; Testillano, M.; Márquez, L.; et al. Nivolumab after Selective Internal Radiation Therapy for the Treatment of Hepatocellular Carcinoma: A Phase 2, Single-Arm Study. J Immunother Cancer 2022, 10, e005457. [Google Scholar] [CrossRef]
- Tai, D.; Loke, K.; Gogna, A.; Kaya, N.A.; Tan, S.H.; Hennedige, T.; Ng, D.; Irani, F.; Lee, J.; Lim, J.Q.; et al. Radioembolisation with Y90-Resin Microspheres Followed by Nivolumab for Advanced Hepatocellular Carcinoma (CA 209-678): A Single Arm, Single Centre, Phase 2 Trial. Lancet Gastroenterol Hepatol 2021, 6, 1025–1035. [Google Scholar] [CrossRef]
- Gkika, E.; Hawkins, M.A.; Grosu, A.-L.; Brunner, T.B. The Evolving Role of Radiation Therapy in the Treatment of Biliary Tract Cancer. Front Oncol 2020, 10, 604387. [Google Scholar] [CrossRef] [PubMed]
- Ben-Josef, E.; Guthrie, K.A.; El-Khoueiry, A.B.; Corless, C.L.; Zalupski, M.M.; Lowy, A.M.; Thomas, C.R.; Alberts, S.R.; Dawson, L.A.; Micetich, K.C.; et al. SWOG S0809: A Phase II Intergroup Trial of Adjuvant Capecitabine and Gemcitabine Followed by Radiotherapy and Concurrent Capecitabine in Extrahepatic Cholangiocarcinoma and Gallbladder Carcinoma. J Clin Oncol 2015, 33, 2617–2622. [Google Scholar] [CrossRef] [PubMed]
- Oh, D.-Y.; Ruth He, A.; Qin, S.; Chen, L.-T.; Okusaka, T.; Vogel, A.; Kim, J.W.; Suksombooncharoen, T.; Ah Lee, M.; Kitano, M.; et al. Durvalumab plus Gemcitabine and Cisplatin in Advanced Biliary Tract Cancer. NEJM Evidence 2022, 1. [Google Scholar] [CrossRef]
- Liu, X.; Yao, J.; Song, L.; Zhang, S.; Huang, T.; Li, Y. Local and Abscopal Responses in Advanced Intrahepatic Cholangiocarcinoma with Low TMB, MSS, PMMR and Negative PD-L1 Expression Following Combined Therapy of SBRT with PD-1 Blockade. J Immunother Cancer 2019, 7, 204. [Google Scholar] [CrossRef] [PubMed]
- Zhao, Q.; Chen, Y.; Du, S.; Yang, X.; Chen, Y.; Ji, Y.; Zeng, Z. Integration of Radiotherapy with Anti-PD-1 Antibody for the Treatment of Intrahepatic or Hilar Cholangiocarcinoma: Reflection from Four Cases. Cancer Biol Ther 2021, 22, 175–183. [Google Scholar] [CrossRef] [PubMed]
- Ahmad, S.A.; Duong, M.; Sohal, D.P.S.; Gandhi, N.S.; Beg, M.S.; Wang-Gillam, A.; Wade, J.L.; Chiorean, E.G.; Guthrie, K.A.; Lowy, A.M.; et al. Surgical Outcome Results From SWOG S1505: A Randomized Clinical Trial of MFOLFIRINOX Versus Gemcitabine/Nab-Paclitaxel for Perioperative Treatment of Resectable Pancreatic Ductal Adenocarcinoma. Ann Surg 2020, 272, 481–486. [Google Scholar] [CrossRef] [PubMed]
- Versteijne, E.; Suker, M.; Groothuis, K.; Akkermans-Vogelaar, J.M.; Besselink, M.G.; Bonsing, B.A.; Buijsen, J.; Busch, O.R.; Creemers, G.-J.M.; van Dam, R.M.; et al. Preoperative Chemoradiotherapy Versus Immediate Surgery for Resectable and Borderline Resectable Pancreatic Cancer: Results of the Dutch Randomized Phase III PREOPANC Trial. J Clin Oncol 2020, 38, 1763–1773. [Google Scholar] [CrossRef]
- Rahma, O.; Katz, M.; Bauer, T.; Wolpin, B.; Stucky, C.-C.; Bekaii-Saab, T.; Elias, R.; Dias-Costa, A.; Nowak, J.; Patrick, L.; et al. Randomized Multicenter Study of Neoadjuvant Chemoradiation Therapy (CRT) Alone or in Combination with Pembrolizumab in Patients with Resectable or Borderline Resectable Pancreatic Cancer. J Immunother Cancer 2021, 9, A1010–A1010. [Google Scholar] [CrossRef]
- Zhu, X.; Cao, Y.; Liu, W.; Ju, X.; Zhao, X.; Jiang, L.; Ye, Y.; Jin, G.; Zhang, H. Stereotactic Body Radiotherapy plus Pembrolizumab and Trametinib versus Stereotactic Body Radiotherapy plus Gemcitabine for Locally Recurrent Pancreatic Cancer after Surgical Resection: An Open-Label, Randomised, Controlled, Phase 2 Trial. Lancet Oncol 2022, 23, e105–e115. [Google Scholar] [CrossRef]
- Koopman, M.; Kortman, G. a. M.; Mekenkamp, L.; Ligtenberg, M.J.L.; Hoogerbrugge, N.; Antonini, N.F.; Punt, C.J.A.; van Krieken, J.H.J.M. Deficient Mismatch Repair System in Patients with Sporadic Advanced Colorectal Cancer. Br J Cancer 2009, 100, 266–273. [Google Scholar] [CrossRef]
- Lumish, M.A.; Cercek, A. Immunotherapy for the Treatment of Colorectal Cancer. J Surg Oncol 2021, 123, 760–774. [Google Scholar] [CrossRef] [PubMed]
- Lenz, H.-J.; Van Cutsem, E.; Luisa Limon, M.; Wong, K.Y.M.; Hendlisz, A.; Aglietta, M.; García-Alfonso, P.; Neyns, B.; Luppi, G.; Cardin, D.B.; et al. First-Line Nivolumab Plus Low-Dose Ipilimumab for Microsatellite Instability-High/Mismatch Repair-Deficient Metastatic Colorectal Cancer: The Phase II CheckMate 142 Study. J Clin Oncol 2022, 40, 161–170. [Google Scholar] [CrossRef] [PubMed]
- Diaz, L.A.; Shiu, K.-K.; Kim, T.-W.; Jensen, B.V.; Jensen, L.H.; Punt, C.; Smith, D.; Garcia-Carbonero, R.; Benavides, M.; Gibbs, P.; et al. Pembrolizumab versus Chemotherapy for Microsatellite Instability-High or Mismatch Repair-Deficient Metastatic Colorectal Cancer (KEYNOTE-177): Final Analysis of a Randomised, Open-Label, Phase 3 Study. Lancet Oncol 2022, 23, 659–670. [Google Scholar] [CrossRef]
- Chalabi, M.; Fanchi, L.F.; Dijkstra, K.K.; Van den Berg, J.G.; Aalbers, A.G.; Sikorska, K.; Lopez-Yurda, M.; Grootscholten, C.; Beets, G.L.; Snaebjornsson, P.; et al. Neoadjuvant Immunotherapy Leads to Pathological Responses in MMR-Proficient and MMR-Deficient Early-Stage Colon Cancers. Nat Med 2020, 26, 566–576. [Google Scholar] [CrossRef] [PubMed]
- Chalabi, M.; Verschoor, Y.L.; van den Berg, J.; Sikorska, K.; Beets, G.; Lent, A.V.; Grootscholten, M.C.; Aalbers, A.; Buller, N.; Marsman, H.; et al. LBA7 Neoadjuvant Immune Checkpoint Inhibition in Locally Advanced MMR-Deficient Colon Cancer: The NICHE-2 Study. Annals of Oncology 2022, 33, S1389. [Google Scholar] [CrossRef]
- Cercek, A.; Lumish, M.; Sinopoli, J.; Weiss, J.; Shia, J.; Lamendola-Essel, M.; El Dika, I.H.; Segal, N.; Shcherba, M.; Sugarman, R.; et al. PD-1 Blockade in Mismatch Repair-Deficient, Locally Advanced Rectal Cancer. N Engl J Med 2022, 386, 2363–2376. [Google Scholar] [CrossRef]
- Deng, L.; Liang, H.; Burnette, B.; Beckett, M.; Darga, T.; Weichselbaum, R.R.; Fu, Y.-X. Irradiation and Anti-PD-L1 Treatment Synergistically Promote Antitumor Immunity in Mice. J Clin Invest 2014, 124, 687–695. [Google Scholar] [CrossRef]
- Dovedi, S.J.; Adlard, A.L.; Lipowska-Bhalla, G.; McKenna, C.; Jones, S.; Cheadle, E.J.; Stratford, I.J.; Poon, E.; Morrow, M.; Stewart, R.; et al. Acquired Resistance to Fractionated Radiotherapy Can Be Overcome by Concurrent PD-L1 Blockade. Cancer Res 2014, 74, 5458–5468. [Google Scholar] [CrossRef]
- Yoshino, T.; Bando, H.; Tsukada, Y.; Inamori, K.; Yuki, S.; Komatsu, Y.; Homma, S.; Uemura, M.; Kato, T.; Kotani, D.; et al. Voltage: Investigator-Initiated Clinical Trial of Nivolumab Monotherapy and Subsequent Radical Surgery Following Preoperative Chemoradiotherapy in Patients with Microsatellite Stable Locally Advanced Rectal Cancer. JCO 2019, 37, 3606–3606. [Google Scholar] [CrossRef]
- George, T.J.; Yothers, G.; Rahma, O.E.; Hong, T.S.; Russell, M.M.; You, Y.N.; Parker, W.; Jacobs, S.A.; Lucas, P.C.; Colangelo, L.H.; et al. Long-Term Results from NRG-GI002: A Phase II Clinical Trial Platform Using Total Neoadjuvant Therapy (TNT) in Locally Advanced Rectal Cancer (LARC). JCO 2023, 41, 7–7. [Google Scholar] [CrossRef]
- Eng, C.; Ciombor, K.K.; Cho, M.; Dorth, J.A.; Rajdev, L.N.; Horowitz, D.P.; Gollub, M.J.; Jácome, A.A.; Lockney, N.A.; Muldoon, R.L.; et al. Anal Cancer: Emerging Standards in a Rare Disease. J Clin Oncol 2022, 40, 2774–2788. [Google Scholar] [CrossRef] [PubMed]
- Morris, V.K.; Salem, M.E.; Nimeiri, H.; Iqbal, S.; Singh, P.; Ciombor, K.; Polite, B.; Deming, D.; Chan, E.; Wade, J.L.; et al. Nivolumab for Previously Treated Unresectable Metastatic Anal Cancer (NCI9673): A Multicentre, Single-Arm, Phase 2 Study. Lancet Oncol 2017, 18, 446–453. [Google Scholar] [CrossRef] [PubMed]
- Marabelle, A.; Cassier, P.A.; Fakih, M.; Kao, S.; Nielsen, D.; Italiano, A.; Guren, T.K.; van Dongen, M.G.J.; Spencer, K.; Bariani, G.M.; et al. Pembrolizumab for Previously Treated Advanced Anal Squamous Cell Carcinoma: Results from the Non-Randomised, Multicohort, Multicentre, Phase 2 KEYNOTE-158 Study. Lancet Gastroenterol Hepatol 2022, 7, 446–454. [Google Scholar] [CrossRef] [PubMed]
Figure 1.
Pre-treatment (1a &1b) and post-treatment (1c & 1d) PET images of a patient with cT2N1 adenocarcinoma of lower esophagus with PDL1 30% (White arrow shows the site of esophageal disease with insert showing magnified image). Patient received neoadjuvant chemoradiation (Carboplatin/ Paclitaxel/ RT) with concurrent nivolumab in view of high PDL1. Esophagectomy showed complete response in esophageal primary and nodes. .
Figure 1.
Pre-treatment (1a &1b) and post-treatment (1c & 1d) PET images of a patient with cT2N1 adenocarcinoma of lower esophagus with PDL1 30% (White arrow shows the site of esophageal disease with insert showing magnified image). Patient received neoadjuvant chemoradiation (Carboplatin/ Paclitaxel/ RT) with concurrent nivolumab in view of high PDL1. Esophagectomy showed complete response in esophageal primary and nodes. .
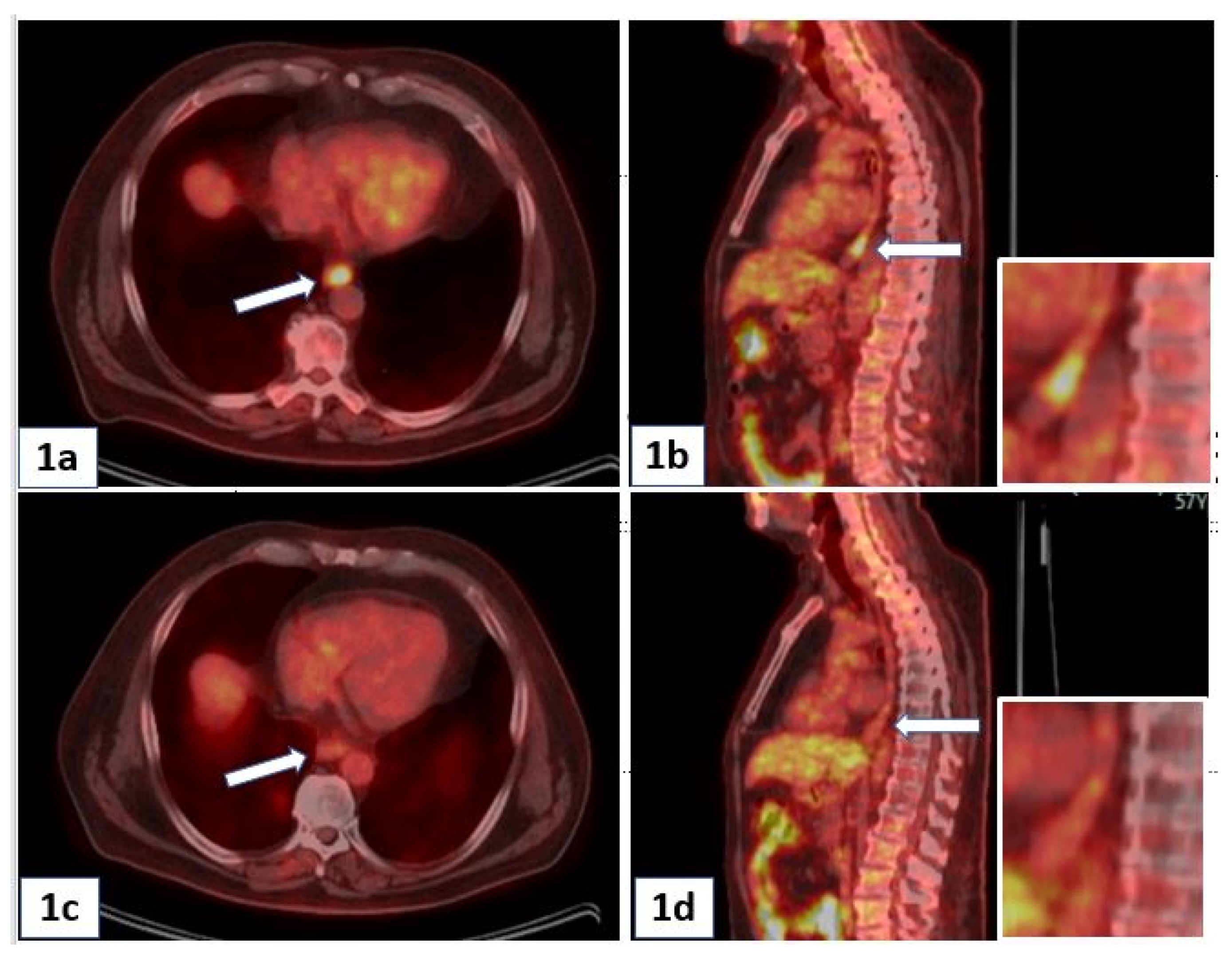
Table 1.
Gastro-esophageal Cancer (Published Studies).
| Author/Study | Type of study | Number (n) | Disease status | ICI | Intervention | Results |
|---|---|---|---|---|---|---|
| Zhang[18] | Phase 1 | 19 | Locally advanced | Camrelizumab | RT-ICI f/b ICI | PFS 11.7 months OS 16.7 months |
| Zhu[20] | Phase 1/2 | 31 | Resectable (Stage II/III) |
Pembrolizumab | CRT-ICI f/b Surgery f/b adjuvant ICI | pCR in 22.6% |
| PERFECT[21] | Phase 2 | 40 | Resectable | Atezolizumab | CRT-ICI f/b Surgery | pCR in 25% |
| Wang[22] | Phase 2 | 12 | Locally advanced | Camrelizumab | Definitive CRT f/b consolidative ICI (n=12) | 11/12 patients had SD |
| Wie[23] | Retrospective | 55 | Inoperable | Camrelizumab Tislelizumab Sintilimab |
CRT-ICI (n=26) CRT alone (n= 29) |
Improved OS with CRT-ICI |
| Nie[24] | Retrospective | 134 | Locally advanced | Carmelizumab Pembrolizumab |
CHT- ICI f/b RT(n=55) CHT- ICI (n= 79) |
PFS (15.7 vs. 5.7 m) OS (15.7 vs. 12 m) |
| Peng[25] | Retrospective | 62 | Locally advanced | ---- | CHT-ICI f/b definitive CRT | PFS 28.8 months |
| CheckMate 577[26] | Phase 3 | 794 | Resectable | Nivolumab | NA-CRT f/b Surgery +/-adjuvant ICI (n= 532 vs 262) | DFS 24.4 vs 11 months |
Table 2.
Gastro-esophageal Cancer (Ongoing Studies).
| NCT Number | Interventions | Primary outcome | Phase |
|---|---|---|---|
| NCT05650216 | Camrelizumab + CRT | Safety, pCR | 2 |
| NCT05043688 | Camrelizumab + CRT | pCR | 2 |
| NCT04229459 | Nivolumab + CRT | pCR | 2 |
| NCT03777813 | Durvalumab +CRT vs. CRT | PFS | 2 |
| NCT05520619 | Tislelizumab + CRT | PFS | 2 |
| NCT05387681 | Envafolimab + CRT | pCR | 2 |
| NCT04929392 | Pembrolizumab + CRT | pCR | 2 |
| NCT04888403 | Toripalimab + CRT | pCR | 2 |
| NCT03257163 | Pembrolizumab → Surgery → adj CHT and CRT with Pembrolizumab | DFS | 2 |
| NCT04973306 | Tislelizumab + CRT vs. CRT | pCR, OS | 2,3 |
| NCT03604991 | Pre-op Nivolumab + CRT vs Pre-op CRT with post-surgery adjuvant (Nivo vs Nivo/Ipi) | pCR, DFS, OS | 3 |
| NCT04404491 | Camrelizumab + RT vs. RT + CHT | AE, PFS | 3 |
| NCT04821843 | Nimotuzumab + CRT vs. Nimotuzumab + CHT | OS | 3 |
| NCT04821778 | Nimotuzumab + CRT vs CRT | OS | 3 |
| NCT05244798 | Sintilimab + CHT vs. Sintilimab + CRT vs. CRT | pCR | 3 |
| NCT04807673 | Pembrolizumab + CRT | Event Free Survival (EFS) | 3 |
Table 3.
HCC Published results.
| Author | Type of study | Patient characteristics | Intervention | Results |
|---|---|---|---|---|
| Chiang | Case series | N = 5 Unresectable HCC |
SBRT + Nivolumab | CR: 2/5 PR: 3/5 |
| Chiang | Retrospective | N = 16 | SBRT + Nivolumab | CR: 50% PR: 37.5% |
| Juloori | Prospective Phase 1 RCT | N = 14 | SBRT + Nivolumab (n = 6) | PR—12.5% SD—37.5% PD—50% |
| SBRT + Ipilimumab + nivolumab (n = 8) | PR—50% SD—37.5% PD—12.5% |
Table 4.
HCC (Ongoing Studies).
| NCT Number | Interventions | Outcome Measures | Phase |
|---|---|---|---|
| NCT05488522 | SBRT + atezolizumab and bevacizumab | PFS | 1 |
| NCT03817736 | TACE followed by SBRT followed by Avelumab | Response Rate/ Amenable to surgery | 2 |
| NCT04913480 | SBRT + Durvalumab (1 yr) | PFS | 2 |
| NCT04988945 | TACE followed by SBRT followed by Durvalumab + Tremelimumab | Response Rate/ Amenable to surgery | 2 |
| NCT04611165 | Hypofractionated radiation (10 fractions) + Nivolumab | PFS | 2 |
| NCT04430452 | Hypofractionated radiation + Durvalumab +/- Tremelimumab | Response Rate | 2 |
| NCT03316872 | SBRT + Pembrolizumab | Response Rate | 2 |
| NCT05366829 | RT + Tislelizumab | PFS | 2 |
| NCT04167293 | SBRT + Sintilimab | PFS | 2/3 |
Table 5.
CCA Ongoing Studies.
| NCT Number | Interventions | Outcome Measures | Phase |
|---|---|---|---|
| NCT04708067 | RT + Bintrafusp Alfa | Response | 1 |
| NCT04866836 | RT + Tislelizumab | Response | 2 |
| NCT03898895 (CORRECT) |
RT + Camrelizumab | PFS | 2 |
Table 7.
Rectal Cancer Ongoing Studies.
| NCT Number | Phase | Stage | ARM | Interventions | Outcome Measures |
|---|---|---|---|---|---|
| NCT03127007 (R-IMMUNE) |
Phase 1/2 | LARC | A | LC CRT + Atezolizumab → TME | AE, pCR |
| B | LC CRT → TME | ||||
| NCT02948348 | Phase 1/2 | LARC | -- | LC CRT + Nivo → TME | pCR |
| NCT05245474 | Phase 2 | LARC | A | LC CRT + Concurrent Tislelizumab → TME | pCR |
| B | LC CRT + Sequential Tislelizumab → TME | ||||
| C | LC CRT → TME | ||||
| NCT05576480 | Phase 2 | LARC | -- | SCRT → Penpulimab + CAPEOX → TME | pCR |
| NCT05086627 | Phase 2 | LARC | A | SCRT → Tislelizumab + CAPEOX → TME → CAPEOX | pCR |
| B | SCRT → CAPEOX → TME → CAPEOX | ||||
| NCT04621370 (PRIME-RT) |
Phase 2 | LARC | A | SCRT + Durvalumab → FOLFOX | pCR, cCR |
| B | LCRT + Durvalumab → FOLFOX | ||||
| NCT05507112 | Phase 2 | LARC | A | LC CRT + Concurrent Tislelizumab → TME | pCR |
| B | LC CRT → TME | ||||
| NCT04503694 | Phase 2 | LARC | -- | Regorafenib + Nivolumab → SCRT → Regorafenib + Nivolumab → TME → +/- adjuvant Chemo | pCR |
| NCT04751370 | Phase 2 | LARC | -- | Nivo/Ipi → SCRT → Nivo/Ipi → TME | pCR |
| NCT03921684 | Phase 2 | LARC | -- | LC CRT → FOLFOX + Nivolumab → TME | pCR |
| NCT04124601 | Phase 2 | LARC | A | LC CRT | AE, Response |
| B | LC CRT → Nivo/Ipi | ||||
| NCT03299660 | Phase 2 | LARC | -- | LC CRT → Avelumab → TME | pCR |
| NCT03854799 | Phase 2 | LARC | -- | LC CRT → Avelumab → TME | pCR |
| NCT03503630 | Phase 2 | LARC | -- | SCRT → Avelumab + FOLFOX → TME | pCR |
| NCT04293419 (DUREC) |
Phase 2 | LARC | -- | FOLFOX + Durvalumab → LCCRT → TME | pCR |
| NCT05009069 | Phase 2 | LARC | A | LC CRT + Atezolizumab + Tiragolumab → TME | pCR |
| NCT05484024 | Phase 2/3 | LARC | A | SCRT → NACT + Sintilimab → W/W or TME | pCR, DFS |
| B | SCRT → NACT → W/W or TME |
Table 8.
Anal Cancer Ongoing Studies.
| NCT Number | Phases | Stage | Interventions | Outcome Measures |
|---|---|---|---|---|
| NCT04046133 (CORINTH) |
Phase 1 | LA III A/B |
CRT + Pembrolizumab | AE, Response |
| NCT04230759 (RADIANCE) |
Phase 2 | LA IIB-IIIC |
CRT (with 5FU/ MMC) | DFS |
| CRT (with 5FU/ MMC/ Durvalumab) | ||||
| NCT04929028 | Phase 2 | Low Risk HIV | CRT (with 5FU/ MMC) | AE, DFS |
| High Risk HIV | CRT (with 5FU/ MMC/ Nivolumab) | |||
| NCT05661188 (TIRANUS) |
Phase 2 | I - IIIB | CRT (with 5FU/ MMC/ Tiraglolumab/ Atezolizumab) | cCR |
| NCT03233711 | Phase 3 | LA II-IIIB |
CRT | DFS |
| CRT → Nivolumab | ||||
| NCT05374252 | Phase 3 | LA III |
CRT (with 5FU/ MMC) | PFS, OS, cCR |
| CRT (with 5FU/ MMC/ Sintilimab) → Adjuvant Sintilimab |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



