Submitted:
24 May 2023
Posted:
26 May 2023
You are already at the latest version
Abstract
It is yet unknown how the formation of aneurysm inside the human body occurs. Thus, the understanding and analysis of the Coanda effect will result in a better overview of the overall fluid mechanics that develops inside such a structure, leading not only to better treatment plans, but also to diminished postoperative risks.
This paper presents how the fluid behaves in this situation, and takes into consideration how this physical phenomenon influences the hemodynamics inside numerous anatomical regions, located in the central nervous system, where aneurysms usually develop.
Analyzing the three main areas in which cerebral aneurysms form the Coanda effect can potentially lead to the rupture of the aneurysm, by changing the blood flow trajectory, it should be taken into consideration when choosing a treatment plan, especially in postoperative care. In addition, there are other factors that can influence the evolution of an aneurysm such as shape, size, localization and the patient’s health condition.
Understanding and analysis of the Coanda effect will result in a better overview of the overall fluid mechanics that develops inside such a structure, leading not only to better treatment plans, but also to diminished postoperative risks.
Keywords:
Coanda Effect
; aneurysm
; hemodynamics
; Willis Polygon
; pathology
1. General data
1.1. Historical facts
Henri Coanda was born in Bucharest on the 7th of June 1886. His early education consisted mostly of military training due to the fact that his father was a general in the Romanian Army. At just 19 years of age he constructed his first prototype of a rocket-airplane. Later that decade, Henri Coanda created the “Coanda 1910”, an airplane without propeller, following his graduation from “ Institut Supérieur de l’Aéronautique et de l’Espace”.
Through the years he invented other aircrafts following “Coanda 1911”, “Bristol-Coanda”, both with propellers and “Coanda 1916” which he invented while working at “Saint-Chamond” in Saint Denis.
Coanda’s inventions not only had a great impact on the further discoveries in the aeronautical domain, which were used in the First World War, but also in fields such as medicine, architecture, transports, construction and others.
In 1930 (1), he obtained a French patent for the observation and description of “Coanda Effect”, a physical phenomenon that, besides medicine, has numerous appliances in fields such as aeronautics, fluids, and meteorology. Henri Coanda died on the 25th of November 1972.
1.2. The physics of the Coanda Effect
Coanda effect is a physical phenomenon that describes the tendency of a fluid or gas to attach to a surface after passing through an asymmetrical narrowing, exerting force on neighboring fluid or gas. We believe the Coanda effect is overlooked when taking into consideration the formation and development of numerous types of aneurysms, and also the postsurgical events that can happen after clipping an aneurysm. This physical phenomenon is of great importance both when the blood passes through a narrowing of the lumen, as well as when the blood goes through an arterial passage that is physiological or pathologically enlarged in comparison to the rest of the artery.
From a medical standpoint, a narrowing inside the body develops, for example, when a cholesterol plaque is created. In addition, being a protuberance (convex structure), it will divert the blood flow on the opposite side of the artery, creating a pressure gradient between the blood jet and the rest of the lumen. The phenomenon develops itself and the blood flow will become adherent to the wall, creating further pressure on the afferent wall while also recruiting adjacent liquid particles into the stream. It is important to mention that the Coanda effect occurs for Reynold’s number as small as 50, meaning that it is present both in laminar and turbulent flow. Also, the Coanda effect is viable for both high and extremely low pressure (2). It is important to note that if the narrowing of the vessel is developed close to a junction of an artery, the blood flow will tend to become asymmetrical, thus creating a flux gradient between the two ramifications. The effect on the boundary wall makes the blood tend to stick to the wall and create a pressure gradient, the jet adhering more to a ramification, resulting in the possibility of some blood joining the ramification where the pressure is higher, creating a retrograde flow.
Image 1.
P- Protuberance, A- point of junction, A1- artery 1, A2- artery 2.
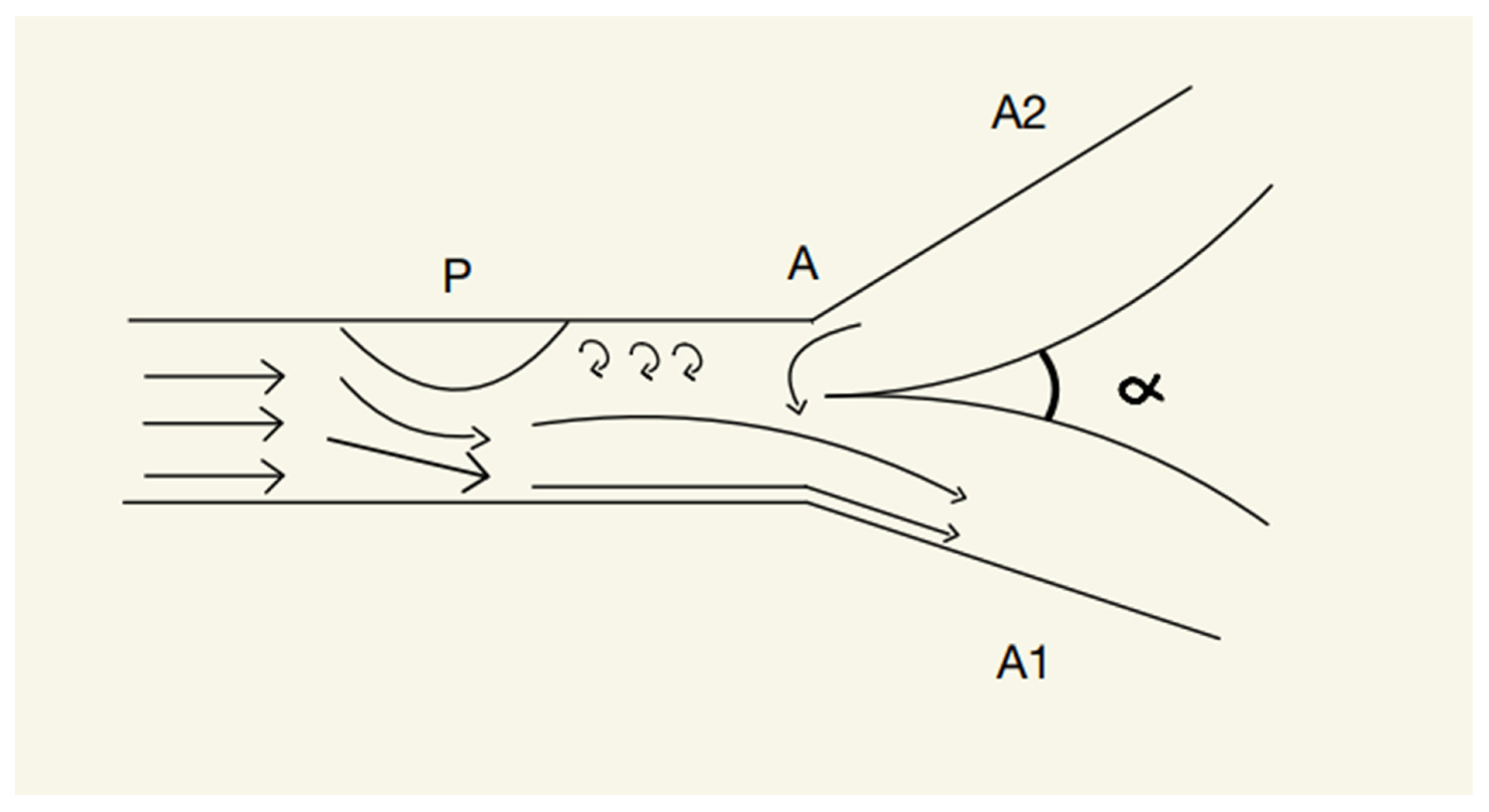
According to (2), the protuberance will create an asymmetry inside the blood vessel, resulting in the jet being diverted to the opposite wall; Thus, the jet will create, according to the Coanda effect, a pressure gradient that will cause retrograde flow from the A2 artery to the A1 artery, phenomenon which can lead to dangerous ischemic damage.
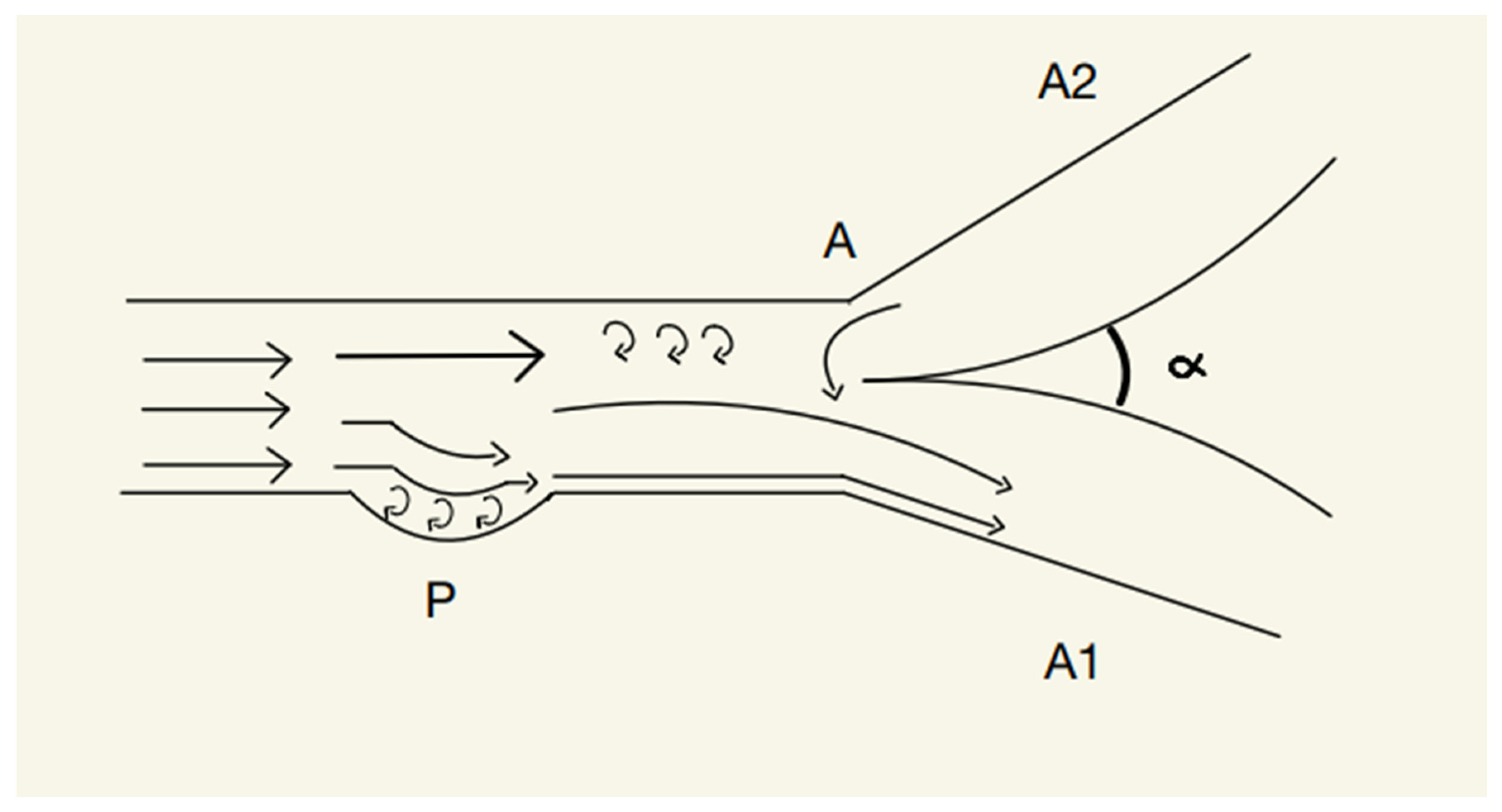
However, when a surface of the blood vessel is concave, the phenomenon will become opposite to the one previously described. The blood jet will tend to attach to the concave surface due to the low pressure inside the pit, thus creating small scale swirls that will exert pressure on the arterial wall. This event will divert the blood flow on the wall with the concavity, and, according to the Coanda effect, will determine neighboring liquid to join the newly created jet. This will, once again, result in an asymmetry of the blood flow if this event happens before a junction.
Image 2.
P- Concavity, A- point of junction, A1- artery 1, A2- artery 2.
2. Typical aneurysms
An aneurysm is a vascular structure that implies a weakening of a blood vessel (with all its layers) that can be localized along the route of both arteries and veins. It takes form as a dilatation of the blood vessel and can be classified based on various factors such as location (abdominal, thoracic, cerebral or peripheral), shape (fusiform, saccular), size (small, large, giant) and cause (congenital, infectious, gained, tumorous, dissecting, traumatic). A special classification of aneurysms is based on the association with the surrounding vessels that proves to be useful in treating cerebral aneurysms.(3)
3. Typical form of cranial aneurysms
Regarding the cranial aneurysms based on their form they can be either fusiform or saccular.
Fusiform- This type of intracranial aneurysms are represented by cylindrical dilatations formed on a relatively short distance on the vessel and are usually associated with atherosclerosis and high blood pressure (4).
Coanda effect in fusiform aneurysm-In this case, Coanda effect appears on the blood vessel wall due to the presence of the concavities. This physical phenomenon will determine the stream to behave in a certain way: a part of the jet will be bound to one wall, another part will be bound to the other side and a part of the jet will flow through the center of the blood vessel (in case of bilateral fusiform aneurysm). The quantity of the stream that will be bound to a side or another can be influenced by a number of factors such as the variation of the pressure, more specific the level of the contraction force of the walls, the number of particles involved, the temperature of the environment, flow rate, viscosity of the blood and also the size and shape of the aneurysm (5). Inside these types of concavities, micro swirls will be created, applying continuous pressure upon the vessel’s walls. In time, this will lead to an overall increase in the size of the aneurysm.
Another important factor is how the aneurysm is clipped intraoperative; if the aneurysm is clipped too tight or the placement is not perfect the Coanda effect will determine a deviation of the jet and an asymmetrical blood flow. This effect causes the blood to follow the curved walls of the vessel contributing to increase the pressure inside the blood vessel (2),as a result it will progressively expand and can lead to a potential rupture. The vascular complications are caused not only by increasing the pressure but also because the Coanda effect determines a blood stagnation in certain parts of the aneurysm resulting in the formation of thrombi. In addition to the progression of the aneurysm, taking the Coanda effect into consideration can change the treatment approach especially while using the endovascular techniques. In this case, the catheter is guided by this physical phenomenon on the wall and can be used to direct the blood flow away from the aneurysm. This way, the risk of rupture is lowered and the normal jet stream is restored(6).
Saccular-This type of intracranial aneurysms are represented by a small sac-like dilatations of an artery that are usually associated with weakening of the blood vessel wall based on the growth of the hemodynamic pressure as well as the distension of the artery(7). It can also be associated with tumorous structures or with infections such as tuberculosis (8).
Coanda effect in saccular aneurysm-
Our understanding of saccular aneurysms develops from convex structures inside the blood vessels. As mentioned before, convex structures appear inside the body when, for example, a cholesterol plaque forms inside an artery. The blood will interact with the convex structure and stick to the opposite wall of the artery, according to the Coanda Effect. Subsequently, the resistance of the afferent wall decreases and, in time, will lead to the formation of a concavity. As previously stated, due to the Coanda effect, a concavity will determine the blood flow to adhere to it, a vicious cycle that will in time lead to the formation of a saccular aneurysm.
It is mandatory to perform surgery on an aneurysm under conditions of hypotension, thus, after clipping an aneurysm, if the clip is placed too tightly and too close to the base of the aneurysm, post operatory we may identify a protrusion inside the vessel, generating other life threatening complications.
4. Special type of brain aneurysm and how it gets affected by the Coanda effect
Serpentine (Giant)- This type of aneurysm is a giant aneurysm that is formed by evolving a saccular or fusiform type. It has a complex form and a sinuous vascular channel. From an angiographic perspective the features presented by a serpentine aneurysm are: a diameter greater than 25mm, it has an undulating intra-aneurysmal vascular channel and it usually is associated with partial thrombosis(9). The Coanda effect appears when the blood jet flows through the aneurysm and can cause the stream to bind to the walls of the blood vessel. As a result, areas of stagnating blood will appear increasing the risk of blood clots to form within the aneurysm. The micro swirls that form within the environment of the blood vessel will also contribute to increasing the pressure of the jet stream and to deviate on the opposite wall from the one where the aneurysm is situated. There are a number of techniques that address the Coanda effect in serpentine aneurysms such as surgical clipping or using stents to redirect the blood flow and minimizing the risk of blood clots to appear, this methods are very relevant considering the increased risk of stroke compared to other types of aneurysms.
5. Coanda effect inside the main aneurysmal areas of the Willis Polygon
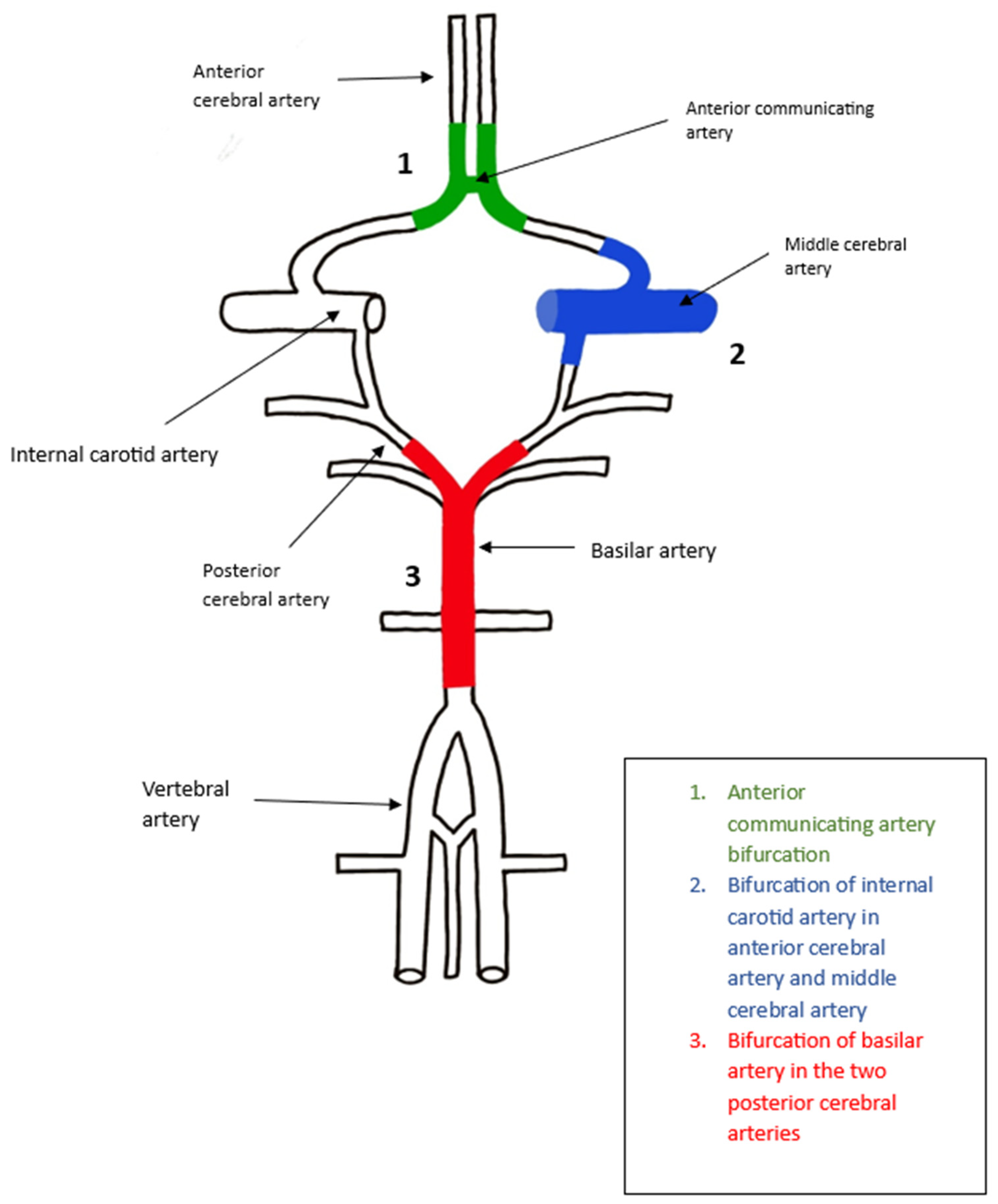
- Anterior communicating artery
Aneurysms appear commonly at the junction between the anterior communicating artery, pericallosal artery and the anterior cerebral artery. Recent studies (10) show that for these types of aneurysms the most indicated approach is clipping, because endovascular treatment is often too inefficient being performed in this segment. Parallel clipping of these types of aneurysms will determine the formation of a protuberance in the walls of the anterior cerebral artery, protuberance that will divert the majority of the flow either through the pericallosal artery, either through the anterior communicating artery, into the opposite pericallosal artery. Therefore, the Coanda effect can lead to serious ischemic damage in postoperative care.
- 2.
- Bifurcation of Internal Carotid artery in Anterior Cerebral artery and Middle Cerebral artery
ICA aneurysm is a type of cerebral aneurysm that develops in the internal carotid artery which is one of the main arteries that supplies blood to the brain and is mostly saccular considering the shape. The junction in this region is formed by the internal carotid artery, anterior cerebral artery and the middle cerebral artery forming a T-shape, the alpha angle being approximately 180 degrees. The constriction of the wall appears on the internal carotid artery but it has to be on a very high level in order for the Coanda effect to appear but if it appears the blood flow will adhere to the opposite wall of the artery and will be lead to the anterior cerebral artery(2). The main risk is represented by the progression of the aneurysm that can lead to rupture as well as the risk of blood clots to form inside the aneurysm therefore, localization of the aneurysm at this bifurcation is relevant and can influence the form treatment. Lower aneurysm can be clipped with any technique while higher ones need to be clipped at the right angle, otherwise, the Coanda effect can appear leading to other treatment plans needing to be addressed in order to minimize the risk that come with the apparition of this phenomenon and also to deviate the blood flow. Other factors that can influence the manifestation of fluid mechanics disturbances as well as the Coanda effect are the size, location, and shape of the aneurysm, as well as the patient’s age, overall health state, and other medical conditions.
- 3.
- Bifurcation of Basilar artery in the two Posterior Cerebral arteries
Basilar artery aneurysm is a type of cerebral aneurysm that appears in the basilar artery which is a large blood vessel inside the brain and supplies the brainstem and the cerebellum. They are extremely rare and are mostly saccular. The junction in this region is Y-shaped, which makes it a textbook case of Coanda effect, which causes the blood flow to deviate to the opposite wall of the aneurysm into the posterior cerebral artery. In this case, the Coanda effect plays a most significant part in determining the blood stream’s trajectory change as well as the progression of the aneurysm. Treatment options include clipping, flow diversion and endovascular coiling reducing the main risk of rupture in this area. In some cases, for example, after clipping, a convection can appear below the clipping area which can determine the apparition of another aneurysm, in this instance, multiple treatment plans should be applied. The treatment plan also can depend on other factors such as the shape or size of the aneurysm, the patient’s health condition and the risk of rupture.
6. Discussion
It is of great importance, when looking at the human body as a whole, to take into consideration all the physical phenomena that occur naturally inside it. The tendency of the fluid to attach to a part of the artery can lead a deviation of the blood flow, resulting in serious ischemic damage in absence of thrombosis(11). This effect can explain both how the aneurysms are created, and also how they develop. Using actual methods such as Doppler echocardiography, computing tomography and magnetic resonance imaging we can detect the Coanda effect and use different treatment plans in order to minimize the risks that can occur.
In conclusion, understanding how the Coanda effect influences hemodynamics will result in a more cautious approach to aneurysm surgical clipping and postoperative treatment.
References
- Coanda H. Procédé de propulsion dans un fluide. Brevet Invent Gr Cl. 1932;2.
- Robinson JL, Roberts A. Operative treatment of aneurysms and Coanda effect: a working hypothesis. Journal of Neurology, Neurosurgery & Psychiatry [Internet]. 1972 Dec 1;35(6):804. Available from: http://jnnp.bmj.com/content/35/6/804.abstract.
- Pritz MB. Cerebral Aneurysm Classification Based on Angioarchitecture. Journal of Stroke and Cerebrovascular Diseases [Internet]. 2011 Mar 1;20(2):162–7. [CrossRef]
- Echiverri HC, Rubino FA, Gupta SR, Gujrati M. Fusiform aneurysm of the vertebrobasilar arterial system. Stroke [Internet]. 1989 Dec 1;20(12):1741–7. [CrossRef]
- Camuffo D. Microclimate and Atmospheric Variables. In 2019. p. 3–14.
- Barletta EA, Ricci RL, Silva RDG, Gaspar RHML, Araújo JFM, Neves MWF, et al. Fusiform aneurysms: A review from its pathogenesis to treatment options. Surg Neurol Int. 2018;9(1). [CrossRef]
- Frösen J, Tulamo R, Paetau A, Laaksamo E, Korja M, Laakso A, et al. Saccular intracranial aneurysm: pathology and mechanisms. Acta Neuropathol [Internet]. 2012;123(6):773–86. [CrossRef]
- Foutrakis GN, Yonas H, Sclabassi RJ. Saccular Aneurysm Formation in Curved and Bifurcating Arteries. American Journal of Neuroradiology [Internet]. 1999 Jul 1;20(7):1309. Available from: http://www.ajnr.org/content/20/7/1309.abstract.
- Christiano LD, Gupta G, Prestigiacomo CJ, Gandhi CD. Giant serpentine aneurysms. Vol. 26, Neurosurgical Focus. 2009. p. 1–11.
- Chen J, Li M, Zhu X, Chen Y, Zhang C, Shi W, et al. Anterior Communicating Artery Aneurysms: Anatomical Considerations and Microsurgical Strategies. Vol. 11, Frontiers in Neurology. Frontiers Media S.A.; 2020.
- Guntheroth W, Miyaki-Hull C. Coanda effect on ductal flow in the pulmonary artery. Journal of Ultrasound in Medicine [Internet]. 1999;18(3):203–6. Available from: https://onlinelibrary.wiley.com/doi/abs/10.7863/jum.1999.18.3.203.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



