Submitted:
20 May 2023
Posted:
23 May 2023
You are already at the latest version
Abstract
Mucosal healing (MH) is the main treatment target in ulcerative colitis and Crohn’s disease, and it is defined by a combination of complete endoscopic and histologic remission. Indeed, the complete resolution of mucosal inflammation should be confirmed at histology. Neutrophil infiltration represents the unique histological marker in discriminating the active vs quiescent phase of disease, also including crypt injuries (cryptitis and crypt abscesses), erosions and ulcerations. Basal plasmacytosis do not qualify by itself the remission in inflammatory bowel diseases (IBD), but it represents a diagnostic clue, mostly at onset. Several histological scoring systems have been developed to evaluate therapeutic efficacy, even though they often resulted tricky and subjective. Moreover, these scores listed a heterogeneous group of histological features as parameters. The recently proposed simplified histological score on MH was based on neutrophils and their distribution in the gut mucosa was also considered, aiming to provide a simple, time-sparing and reproducible tool to be applied to the routinary diagnostic practice. The artificial intelligence could be a promising tool both in evaluating and standardizing the histological assessment of disease activity in IBD. Moreover, novel molecules involved in the inflammatory dynamics in the gut could be employed in supporting the diagnostic practice in IBD.
Keywords:
ulcerative colitis
; Crohn’s disease
; scoring system
; histological mucosal healing
1. Introduction
The assessment of disease activity is the cornerstone of modern management of inflammatory bowel diseases (IBD), shaping its clinical management. Endoscopy represents the gold standard in the assessing of IBD activity, especially in ulcerative colitis (UC). In the past few decades, remission has been considered to be achieved by symptomatic relief. However, residual foci of subtle inflammation were found to remain at histology in a subset of cases, raising the bar about the treatment goals and mucosal healing (MH) [1]. MH is usually defined by a combination of complete endoscopic and histological remission. Several scoring systems have been introduced to grade inflammation in the gut mucosa [2,3]. The Mayo endoscopic score represents the most suitable tool for grading the mucosal injuries at endoscopy, and it defines remission as the disappearance of visible inflammation or ulceration (Mayo Score 0 to 1) [4,5]. Endoscopic remission has been found to be associated with a better long-term clinical outcome, including the reduced need for glucocorticoid administration, the lower rate of relapse, hospitalization and surgical resection. The occurrence of IBD associated colorectal neoplasia was also found to be reduced in long-lasting remission [6,7,8,9]. However, the endoscopic remission do not stands for histological remission, since the 14-40% of patients showed evidence of mucosal active inflammation at histology, even though the endoscopic findings were unremarkable [10,11,12]. Early reports by Truelove et al [13] showed the 37% of patients with normal sigmoidoscopy to display a persistence of active inflammation at histology. Thus, the therapeutic target is currently focused on the achievement of the histological MH . The histological evidence of active inflammation is a stronger predictor of relapse in UC, less responsiveness to first-line treatment (e.g. NSAIDs and Mesalazine), and hospitalization [1,10]. In remitting UC at endoscopy, the histological evidence of active inflammation was found to be associated to an increased relapse rate [14], as well as to an increased risk of developing colorectal neoplasia [15]. According to these evidences, the Food and Drug Administration of the US Department of Health and Human Services recommended that clinical trials should have been conducted with histological assessment paired to the endoscopic evaluation of UC activity [16]. The role of histology as predictor of treatment response is less clear in Crohn’s disease (CD), since both the trans-mural involvement and the patchy distribution of disease limit the role of the mucosal biopsy in assessing the MH [17]. Nonetheless, the histological MH was found to correlate with a lesser relapse rate and glucocorticoid administration in remitting CD ileitis, whereas the endoscopic MH did not [18].
2. Histopathological features of IBD
UC usually affects the colorectum and it is characterized by a continuous distribution of inflammation and mucosal injuries . CD can potentially affects all the gastrointestinal (GI) tract, from the anus to the mouth with a discontinuous pattern of inflammation. The terminal ileum is the most common site of onset, followed by the colon, whereas the upper GI location is rare.
The diagnosis of IBD is based on the identification of specific histological features [19]. Among them, the histological hallmarks of UC are represented by the increased density in inflammatory infiltration in the lamina propria, including plasma cells and eosinophils. Particularly, the raised plasma cells (3 or more of them) are most commonly located at the base of the crypts or in the lower third of the inter-cryptic space in the lamina propria. Such a feature known as basal plasmacytosis, is of critical diagnostic importance in UC [20]. The number of eosinophils can vary, but they are usually intermingled with plasma cells. Interestingly, an increased number of eosinophils (>60 / 10 HPF) in treatment-naïve UC patients has been found to correlate with poor treatment response [21,22].
The presence of neutrophils in the lamina propria marks the active phase of disease and can lead to glandular and surface epithelial injuries, such as cryptitis, cryptic abscesses, mucosal erosions and ulcers.
Another histological hallmark is represented by architectural abnormalities , including crypt distortion, namely convoluted, dilated and non- parallel crypts, crypt branching, characterized by a dicotomic sprouting at the lower third of the crypt and crypt atrophy, qualified by crypts shorter than normal. Architectural abnormalities in the lamina propria have been found in 57-100% of UC cases, and directly correlate with a long-standing disease. Conversely, the crypt architecture can be almost normal at onset [23].
Reactive epithelial changes such as mucin depletion and left-sided Paneth cell metaplasia can be frequently seen in active and long-standing diseases respectively. The so-called back-wash ileitis is characterized by the reactive villous atrophy and inflammation of the more distal part of the ileum . It has been found to characterize the 20% of patients suffering from active ulcerative pancolitis. A mild degree of neutrophilic infiltration can also be seen in the lamina propria at histology, including cryptitis and crypt abscesses [24]. Moreover, the segmental (incomplete) response to previous treatments has been found to lead to a discontinuous distribution of the mucosal inflammation (e.g. the so called cecal patch) in long-standing disease [25].
The architectural abnormalities are usually mild and discontinuous in CD, and the mucosal inflammation is patchy as compared to UC. Neutrophil infiltration and epithelial injuries marks the active phase of disease, as seen in UC. A peculiar feature in CD onset is the infiltration of the superficial epithelium by neutrophils and eosinophils [26,27]. The active inflammation could also manifest as aphtoid ulcers, occurring as mucosal ulceration onto the top of a mucosa-associated lymphoid aggregate , mostly in ileal CD. The two histological features can also be associated in the same mucosal samples . The epithelioid cell granulomas, with or without multinucleated giant cells, are more frequently observed in children than in adults. Caution should be paid in excluding the occurrence of cryptolitic granulomas. Reactive epithelial changes could also be detected in ileal mucosa, including irregular villous architecture . Pyloric gland metaplasia has been found in 2-27% of ileal biopsies in CD patients. The detection of the histological features suggesting the intestinal inflammation to be chronic represents a crucial tool in distinguishing IBD from acute self-limiting colitis at the onset [19].
3. Histological Mucosal Healing
The endoscopic remission has been historically considered the unique parameter in describing MH , but growing evidences suggest that the endoscopic features should not be considered as an exhaustive descriptor of MH in IBD. Particularly, a residual amount of neutrophil infiltration in the lamina propria was found in more than 40% of patients displaying endoscopic features that would have pointed toward clinical remission [10,11,12]. This finding has impactful implications in clinical practice, since histological inflammation was proven to be associated with worse clinical outcomes [1]. Hence, the histological evaluation was recommended to be included in the definition of MH [28]. The histological remission and MH have not been completely defined so far, neither in UC nor in CD, and disagreement still remains on the topic. First, terminology should be properly re-assessed, as histological healing and remission are not synonyms, thus they should not be used as interchangeable terms. The histological remission is defined by a spectrum of features in UC, ranging from the evidence of residual foci of chronic inflammation and architectural distortion to the almost normal mucosa [10]. The International Organization of Inflammatory Bowel Disease (IO-IBD) [17] has recently recommended histological parameters to be included as diagnostic treatment-aiding tools in both UC and CD. They included:
- disappearance of neutrophil infiltration in the lamina propria;
- reduction of plasma cell infiltration (to normal values) and disappearance of basal plasmacytosis;
- reduction of eosinophil infiltration (to normal values).
The presence of basal plasma cells still remains a matter of concern in the histological definition of MH in IBD. Basal plasma cells represent an important diagnostic clues in IBD with a high predictive value at the onset of disease. It is commonly used in discriminating IBD from non-IBD colitis [20,23,29,30,31] and it represents an independent predictor of relapse in clinical remitting UC patients [32]. Accordingly, it has been proposed that basal plasmacytosis should be absent in healed mucosa [33].
Thus, the reappearance of basal plasmacytosis in treated patients could be interpreted as a predictor of forthcoming relapse, even though they are clinically remitting [14].
Furthermore, some studies did not confirm the predictive role of basal plasmacytosis in clinical relapse in UC patients with endoscopic remission [34]. Overall, plasma cells mark the presence of IBD, but they do not provide any definition on its activity. Their predicting role of forthcoming relapse in treated patients has been also postulated.
Eosinophils represent a common finding in mucosal samples from IBD patients. The significance of eosinophils as a histological marker of activity is unclear [35]. They have been found to be more numerous than normal in active as well as in quiescent disease, being usually intermingled with plasma cells both in UC and CD [20,31]. Eosinophil density has been found to correlate with both disease extent and a lesser responsiveness to glucocorticoid therapy, but not with the activity of disease [22,36].
Consistently, the European Crohn’ s and Colitis Organization (ECCO) stated that “eosinophils alone should not be used as a marker of histological activity “ in UC [37].
According to our experience, neutrophil infiltration in the lamina propria and neutrophil-related injuries in crypts and surface epithelium represent the histological hallmark of disease activity in IBD. Hence, the finding of neutrophil infiltration should be used in distinguishing the active vs quiescent phase of disease and it should be considered in the histological MH definition [38,39]. Accordingly, the absence of both neutrophils and neutrophil-mediated mucosal injuries in the lamina propria was claimed to represent a mandatory requirement to histologically define remission in IBD [37,40]. A worth-noting issue to be addressed is how to properly approach to the histopathological assessment of disease activity in IBD. First, mucosal samples should be evaluated in order to differentiate IBD from non-IBD-colitis, and then the disease activity should be considered. Moreover, thorough clinical- endoscopic data should be available. A proper methodological approach also includes technical requirements, encompassing both the completeness of the mucosal sampling at endoscopy and a proper handling after samples were collected. Particularly, at least two pinch biopsies from both the terminal ileum and the five colorectal segments (cecum- ascending, transverse, descending, sigmoid and rectum) should be collected. Mucosal ulcers detected at endoscopy should be accurately sampled, including the edges of the lesion [37,40]. The orientation of the mucosal samples is another mandatory requirement to achieve the histological diagnosis [19,37]. Each sample should be sequentially placed by the endoscopist in a straight line onto a cellulose acetate substrate, with the luminal surface upwards [19]. A “clarinet beak-shaped cut” marks the proximal end of the strip in order to provide clues on the segmental location of each samples. Once fixed (37% formaldehyde solution), specimens are processed and then paraffin-embedded. A 90 degrees rotation of the filter-specimens complex must be performed by the technicians in order to warrant the optimal trans-sectional orientation to the biopsies. A sequential sectioning is advisable, mostly when the presence of the histological hallmarks is focal or not straight-forward[19]. Alternatively, mucosal sampling should be send a vial per segment [37].
4. Histological scores in IBD
Several histological scoring systems, approximately 30 for UC and 13 for CD, have been proposed to date, both to differentiate the active vs quiescent disease and to evaluate the therapeutic efficacy. However, they were exceedingly heterogeneous on terminology, histological features and classification criteria. Moreover, they resulted tricky, time-consuming and subjective, not suitable for the routine diagnostic practice [41,42]. A few of them are currently used with research purposes, but not in clinical practice, since they were burdened by a low inter-observer reproducibility both among general and GI pathologists [37,43]. After the first attempt from Truelove et al. [13], the Simplified Geboes Score (SGS), the Robarts Histological Index (RHI) and the Nancy Histological Index (NHI) are the most commonly used for scoring the disease activity in UC. Among them, only the RHI and NHI scores are fully validated and recommended from the European Crohn’s and Colitis Organization (ECCO) for randomized case-control studies, observational studies and clinical trials. [37]. In fact, NHI is simple and suitable for the clinical practice [44]. Currently, there are no validated scoring systems to be applied to CD. Limitations were represented by the patchy distribution of disease and the trans-mural extension of the inflammation. The ECCO recommendations stated that GS, RHI and NHI can be used for intestinal biopsies from CD patients [40], even though they were shown to be insufficient in predicting the clinical outcomes in CD [45]. A simplified score was recently proposed for the routine diagnostic practice. It was suitable for the assessment of the histological features, mostly about the disease activity and the MH, in both UC and CD [46].
4.1. Geboes Score
It has been developed by Geboes et al. in 2000 [47]. It has been the most used score in clinical trials, but it was limited by complexity. It evaluated six histological features (Grade), including architectural changes (Grade 0), chronic inflammatory infiltrate (Grade 1), lamina propria neutrophils and eosinophils (Grade 2A, Grade 2B), neutrophils in epithelium (Grade 3), crypt destruction (Grade 4) and erosions or ulcerations (Grade 5). Each grade of the score was further divided in 4 subgrades, ranging from 0 to 3, with the exception of the surface epithelial injury, which ranges from 0 to 4. The sub-grades were evaluated onto the most inflamed area in the biopsy, without average evaluations. GS can be variably used, either applying a single score, ranging from 0 to 6, focusing onto the most inflamed area in the biopsy by summing the sub-grades recorded from all the grades, obtaining a total score ranging from 0 to 22 (known as continuous GS). To reduce its complexity, a simplified GS (SGS) was proposed in 2016 [48] (Table 1).
4.2. Nancy Histological Index
NHI was developed in 2015 [49]. It comprises three histological items that define five parameters of the histological activity, including the absence of significant histological disease (grade 0), chronic inflammation (grade 1), mildly active disease (grade 2), moderately active disease (grade 3) and severely active disease (grade 4). The NHI is characterized by a stepwise evaluation, based on the worst feature observed in the biopsy to determine the final score. Erosions and ulcerations were categorized as NHI is 4. The active inflammation without erosions nor ulceration were graded as grade 2 or 3, according to the severity of inflammation. The chronic inflammation is defined as grade 1, whereas the grade 0 described the absence of chronic inflammation or, if any, it was mild (Table 1). The histological remission was defined as NHI=0 and histological response as NHI≤1. According to the authors of NHI, the index system is simple and easy to use with a good intraobserver and interobserver reproducibility. Furthermore, the orientation of the biopsy specimen is not essential for the assessment of the histological features [49]. Magro et al [44] demonstrated that NHI and continuous GS strongly correlate for both histological remission and treatment response in UC.
4.3. Robarts Histological Index
RHI was developed in 2017 through a multiple linear regression model [50]. It is based on the GS and includes the four original items that showed the highest inter-rater and intra-rater reliability. The items evaluated by RHI included chronic inflammation, neutrophil infiltration, intra-epithelial neutrophils, surface injury, namely erosion and ulcerations (Table 1). The final score is obtained by combining the sub-scores from the four items, ranked from 0 to 3 and yielding a total score ranging from 0 (absence of disease activity) to 33 (high disease activity). In UC, the histological remission is defined as RHI ≤3 (with sub-scores equal to 0 for both lamina propria and intra-epithelial neutrophils, and without erosions nor ulceration), while the histological response is defined as RHI≤ 9 (with sub-scores equal to 0 for intra-epithelial neutrophils and without erosions nor ulceration) [37]. RHI was recently shown to be strongly correlated with continuous GS in UC [51].
5. Simplified Histological Mucosal Healing Scheme (SHMHS)
A simplified scheme was proposed in 2017 [46]. It focuses on neutrophil infiltration as the hallmark of active inflammation and it can be applied for assessing the grade of the activity and MH in both UC and CD. It is composed by eight questions about histological parameters, including the number of pinch biopsies and the sites of active and quiescent inflammation. The scheme also encompasses three histologic variables, including neutrophil infiltration, cryptitis or crypt abscesses and epithelial neutrophil-mediated injuries, encompassing erosions and ulcerations (Figure 1). The SHMHS is subdivided in two parts, both of each including eight questions (Table 1). The first part inquires the histological features. The score 1 means present and it is assigned when at least one mucosal fragment shows that feature at histology; the score 0 means absent. The second part addresses how the mucosal inflammation is distributed in the gut. A question per intestinal segment is proposed, referring to the right colon, the transverse and descending colon, the sigmoid colon and rectum. The mucosal sampling from terminal ileum is only considered in CD patients. The score is assigned as 1 for active inflammation, while score 0 is assigned to quiescent disease or normal (non-IBD) mucosa. The disease is considered as active when at least one mucosal fragment per segment harbors neutrophil infiltration or neutrophil-mediated epithelial injuries. The disease is considered as quiescent when at least one mucosal fragment per segment shows the histological features of chronic inflammation, including crypt distortion, basal plasmacytosis but, importantly, the active inflammation is lacking. The scoring system lead toward a total score ranging from 0 to 8. A total score ≥2 stands for active disease. The SHMHS has been developed considering easy-to-find histological features, resulting in a simple and time-sparing tool for assessing disease activity and mucosal healing in IBD. Such a scheme resulted to be suitable to be employed in the routine clinical practice both by general and GI pathologists, because it is simple to be applied and less subjective than other schemes. It was shown to be a reliable grading system, achieving similar results as compared to the previously validated schemes, such as GS, NHI and RHI [46]. The score has shown a very good inter-rater agreement (k=0.94). Moreover, a strong correlation with Mayo Clinic Endoscopic Score and Simple Endoscopic Score was highlighted in a nation-wide multicentre study on both UC and CD [52]. On a similar note, another attempt to simplify UC scoring worth mentioning is the PI-CaSSO Histological Remission Index (PHRI) [53]. The score was designed to reduce all the assessments to the sole detection of neutrophils. The mucosa is divided in four functional areas, superficial epithelium, cryptal epithelium, lamina propria and cryptal lumen. PHRI ranges from 0 to 4, with 0 considered as remission and any score above that as active disease. Scores are counted summing the numer of areas with at least one neutrophil at 40x magnification. In addition, evidence of erosions or ulcers are considered pathognomonic of inflammation regardless of neutrophils. This approach, demonstrated a very good interobserved variability, and correlation with endoscopy at no expense of outcome stratification.
6. Future directions
The MH is an evolving concept and the tools to assess it keep evolving likewise. Automatic processes and specific algorithms employed in grading active inflammation in IBD represent a promising support to the diagnostic practice, as shown by pioneering Authors [53,54,55]. Such technical innovation could lead to improve the diagnostic standardization, also limiting the inter-observer variability, but further validations are needed. Another intriguing topic is represented by novel putative markers of inflammation in IBD. The treatment options are currently based on immunosuppression leading to disease transient symptomatic relief. A better understanding of the underlying mechanisms involved in the gut-immune homeostasis could help identify new molecular targets to be employed as therapeutic targets. The glucocorticoid-induced leucine zipper (GILZ) has been found to be involved in mediating some of the glucocorticoid effects, mostly in immune cells. However GILZ was recently established to exert a secretory role in the gut, being delivered by goblet cells into the lumen. Both in UC and CD it resulted to be impaired in active disease, while it was restored in quiescent disease, thus correlating with neutrophil infiltration and epithelial injury [56]. Moreover, it was also found to be directly related to MUC2, one of the major components of the mucus barrier, as well as to TLR2 and TLR4, which are involved in several gut mucosal functions including permeability [57]. Recently, GILZ has gained attention in IBD as it negatively modulates neutrophil activation, thus promoting a negative control on the main cellular effector of disease activity in IBD [58,59]. It is worth-nothing that the exogenous administration of GILZ (TAT-GILZ) was shown to ameliorate the colitis symptoms in mice model of IBD, thus providing a pre-clinical assessment of its efficacy in treating colitis [60]. Taken together, these findings suggest GILZ to be a molecule of interest in IBD treatment.
7. Conclusions
The assessment of the histological MH has now become a tool of critical importance in evaluating the treatment efficacy in IBD. A reliable histological score to be used in assessing the treatment response is still lacking. The available scores are complex and subjective, mostly limited to research purposes, as they are based on different histological parameters and not standardized mucosal sampling at endoscopy. Conversely, the SHMHS could help assess the histological remission in the routine diagnostic practice.
Author Contributions
All Authors contributed to conceptualization; methodology; investigation; data curation; writing—original draft preparation; writing—review and editing. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Data Availability Statement
No new data were created or analyzed in this study.
Acknowledgments
This study did not include any administrative and technical support, or donations.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Bryant, R.V.; Burger, D.C.; Delo, J.; Walsh, A.J.; Thomas, S.; von Herbay, A.; Buchel, O.C.; White, L.; Brain, O.; Keshav, S.; Warren, B.F.; Travis, S.P. Beyond endoscopic mucosal healing in UC: histological remission better predicts corticosteroid use and hospitalisation over 6 years of follow-up. Gut 2016, 65, 408–414. [Google Scholar] [CrossRef] [PubMed]
- Neurath, Markus, F.; Travis, Simon P. L. Mucosal healing in inflammatory bowel diseases: a systematic review. Gut 2012, 61, 1619–1935. [CrossRef] [PubMed]
- Samaan, M.A.; Mosli, M.H.; Sandborn, W.J.; Feagan, B.G.; DʼHaens, G.R.; Dubcenco, E., Baker, K.A.; Levesque, B.G. A systematic review of the measurement of endoscopic healing in ulcerative colitis clinical trials: recommendations and implications for future research. Inflamm Bowel Dis. 2014, 20, 1465–1471. [CrossRef]
- Schroeder, K.W.; Tremaine, W.J.; Ilstrup, D.M. Coated oral 5-aminosalicylic acid therapy for mildly to moderately active ulcerative colitis. A randomized study. N Engl J Med. 1987, 317, 1625–1629. [Google Scholar] [CrossRef] [PubMed]
- Travis, S.P.; Higgins, P.D.; Orchard, T.; Van Der Woude, C.J.; , Panaccione; Bitton, A., O'Morain, C.; Panés, J.; Sturm,A.; Reinisch, W.; Kamm, M.A.; D'Haens, G. Review article: defining remission in ulcerative colitis. Aliment Pharmacol Ther. 2011, 34, 113–124. [CrossRef]
- Colombel, J.F.; Rutgeerts, P.; Reinisch, W.; Esser, D;, Wang, Y.; Lang, Y.; Marano, C.W.; Strauss, R.; Oddens, B.J.; Feagan, B.G.; Hanauer, S.B.; Lichtenstein, G.R.; Present, D.; Sands, B.E.; Sandborn, W.J. Early mucosal healing with infliximab is associated with improved long-term clinical outcomes in ulcerative colitis. Gastroenterology 2011, 141, 1194–1201. [CrossRef]
- Shah, S.C; Colombel, J.F; Sands, B.E.; Narula, N. Mucosal Healing Is Associated With Improved Long-term Outcomes of Patients With Ulcerative Colitis: A Systematic Review and Meta-analysis. Clin Gastroenterol Hepatol. 2016, 14, 1245–1255. [Google Scholar] [CrossRef] [PubMed]
- Ardizzone, S.; Cassinotti, A.; Duca, P.; Mazzali, C.; Penati, C.; Manes, G.; Marmo, R.; Massari, A.; Molteni, P.; Maconi, G.; Porro, G.B. Mucosal healing predicts late outcomes after the first course of corticosteroids for newly diagnosed ulcerative colitis. Clin Gastroenterol Hepatol. 2011, 9, 483–489. [Google Scholar] [CrossRef]
- Frøslie, K.F; Jahnsen, J.; Moum, B.A; Vatn, M.H.; IBSEN Group. Mucosal healing in inflammatory bowel disease: results from a Norwegian population-based cohort. Gastroenterology 2007, 133, 412–422. [Google Scholar] [CrossRef]
- Riley, S.A.; Mani, V.; Goodman, M.J.; Dutt, S.; Herd, M.E. Microscopic activity in ulcerative colitis: what does it mean? Gut 1991, 32, 174–178. [Google Scholar] [CrossRef]
- Mosli, M.H.; Feagan, B.G.; Sandborn, W.J.; Dʼhaens, G.; Behling, C.; Kaplan, K.; Driman, D.K.; Shackelton, L.M.; Baker, K.A.; Macdonald, J.K.; Vandervoort, M.K.; Geboes, K.; Levesque, B-G. Histologic evaluation of ulcerative colitis: a systematic review of disease activity indices. Inflamm Bowel Dis. 2014, 20, 564–575. [CrossRef]
- Pai, R.K.; Jairath, V.; Vande Casteele, N.; Rieder, F.; Parker, C.E.; Lauwers, G.Y. The emerging role of histologic disease activity assessment in ulcerative colitis. Gastrointest Endosc. 2018, 88, 887–898. [Google Scholar] [CrossRef] [PubMed]
- Truelove, S.C.; Richards, W.C. Biopsy studies in ulcerative colitis. Br Med J. 1956, 1(4979), 1315–1358. [Google Scholar] [CrossRef]
- Gupta, A.; Yu, A.; Peyrin-Biroulet, L.; Ananthakrishnan, A.N. Treat to Target: The Role of Histologic Healing in Inflammatory Bowel Diseases: A Systematic Review and Meta-analysis. Clin Gastroenterol Hepatol. 2021, 19, 1800–1813. [Google Scholar] [CrossRef] [PubMed]
- Gupta, R.B.; Harpaz, N.; Itzkowitz, S.; Hossain, S.; Matula, S.; Kornbluth, A.; Bodian, C.; Ullman, T. Histologic inflammation is a risk factor for progression to colorectal neoplasia in ulcerative colitis: a cohort study. Gastroenterology 2007, 133, 1099–1105. [Google Scholar] [CrossRef] [PubMed]
- Food and Drug Admistration. Ulcerative colitis: Clinical Trial Endpoints Guidance for Industry. Draft guidance. Silver Spring, MD: FDA, 2016; 19.
- Bryant, R.V.; Winer, S.; Travis, S.P.; Riddell, R.H. Systematic review: histological remission in inflammatory bowel disease. Is 'complete' remission the new treatment paradigm? An IOIBD initiative. J Crohns Colitis 2014, 8, 1582–1597. [Google Scholar] [CrossRef]
- Christensen, B.; Erlich, J.; Gibson, P.R.; Turner, J.R.; Hart, J.; Rubin, D.T. Histologic Healing Is More Strongly Associated with Clinical Outcomes in Ileal Crohn's Disease than Endoscopic Healing. Clin Gastroenterol Hepatol. 2020, 18, 2518–2525. [Google Scholar] [CrossRef] [PubMed]
- Villanacci, V.; Reggiani-Bonetti, L.; Salviato, T.; Leoncini, G.; Cadei, M.; Albarello, L.; Caputo, A.; Aquilano, M.C.; Battista, S.; Parente, P. Histopathology of IBD Colitis. A practical approach from the pathologists of the Italian Group for the study of the gastrointestinal tract (GIPAD). Pathologica 2021, 113, 39–53. [Google Scholar] [CrossRef]
- Canavese, G.; Villanacci, V.; Antonelli, E,.; Cadei, M.; Sapino, A.; Rocca, R.; Daperno, M.; Suriani, R.; Di Santo, M.G.; Cassoni, P.; Bernardini, N.; Bassotti, G. Eosinophilia - associated basal plasmacytosis: an early and sensitive histologic feature of inflammatory bowel disease. APMIS 2017, 125, 179–183. [CrossRef]
- Zezos, P.; Patsiaoura, K.; Nakos, A.; Mpoumponaris, A.; Vassiliadis, T.; Giouleme, O.; Pitiakoudis, M.; Kouklakis, G.; Evgenidis, N. Severe eosinophilic infiltration in colonic biopsies predicts patients with ulcerative colitis not responding to medical therapy. Colorectal Dis. 2014, 16, O420–O430. [Google Scholar] [CrossRef]
- Leoncini, G.; Villanacci, V.; Marin, M.G.; Crisafulli, V.; Cadei, M.; Antonelli, E.; Leoci, C.; Bassotti, G. Colonic hypereosinophilia in ulcerative colitis may help to predict the failure of steroid therapy. Tech Coloproctol. 2018, 22, 941–946. [Google Scholar] [CrossRef] [PubMed]
- Langner, C.; Magro, F.; Driessen, A.; Ensari, A.; Mantzaris, G.J.; Villanacci, V.; Becheanu, G.; Borralho Nunes, P.; Cathomas, G.; Fries, W.; Jouret-Mourin, A.; Mescoli, C.; de Petris, G.; Rubio, C.A.; Shepherd, N.A.; Vieth, M,.;Eliakim, R.; Geboes, K.; European Society of Pathology; European Crohn's and Colitis Foundation. The histopathological approach to inflammatory bowel disease: a practice guide. Virchows Arch. 2014, 464, 511–527. [CrossRef]
- Yantiss, R.K.; Odze, R.D. Diagnostic difficulties in inflammatory bowel disease pathology. Histopathology 2006, 48, 116–132. [Google Scholar] [CrossRef] [PubMed]
- Bernstein, C.N.; Shanahan, F.; Anton, P.A.; Weinstein, W.M. Patchiness of mucosal inflammation in treated ulcerative colitis: a prospective study. Gastrointest Endosc. 1995, 42, 232–237. [Google Scholar] [CrossRef] [PubMed]
- Sankey, E.A.; Dhillon, A.P,.; Anthony, A.; Wakefield ,A.J.; Sim, R.; More, L.; Hudson, M.; Sawyerr, A.M., Pounder, R.E. Early mucosal changes in Crohn's disease. Gut 1993, 34, 375–381. [CrossRef]
- Villanacci, V.; Bassotti, G. Histopathological findings of extra-ileal manifestations at initial diagnosis of Crohn's disease-related ileitis. Virchows Arch. 2017, 470, 595–596. [Google Scholar] [CrossRef]
- Turner, D.; Ricciuto, A.; Lewis, A.; D'Amico, F.; Dhaliwal, J.; Griffiths, A.M.; Bettenworth, D.; Sandborn, W.J.; Sands, B.E.; Reinisch, W.; Schölmerich, J.; Bemelman, W.; Danese, S.; Mary, J.Y.; Rubin, D.; Colombel, J.F.; Peyrin-Biroulet, L.; Dotan, I.; Abreu, M.T.; Dignass, A. International Organization for the Study of IBD.STRIDE-II: An Update on the Selecting Therapeutic Targets in Inflammatory Bowel Disease (STRIDE) Initiative of the International Organization for the Study of IBD (IOIBD): Determining Therapeutic Goals for Treat-to-Target strategies in IBD. Gastroenterology 2021, 160, 1570–1583. [Google Scholar] [CrossRef]
- Magro, F.; Langner, C.; Driessen, A.; Ensari, A:, Geboes, K.; Mantzaris, G.J.; Villanacci, V.; Becheanu, G.; Borralho Nunes, P.; Cathomas, G.; Fries, W.; Jouret-Mourin, A.; Mescoli, C.; de Petris, G.; Rubio, C.A.; Shepherd, N.A.; Vieth, M.; Eliakim, R.; European Society of Pathology (ESP); European Crohn's and Colitis Organisation (ECCO). European consensus on the histopathology of inflammatory bowel disease. J Crohn’s Colitis 2013, 7, 827–851. [CrossRef]
- Stange, E.F.,Travis, S.P.; Vermeire, S.; Reinisch, W.; Geboes, K.; Barakauskiene, A.; Feakins, R.; Fléjou, J.F.; Herfarth, H.; Hommes, D.W.;Kupcinskas, L.; Lakatos, P.L.; Mantzaris, G.J.; Schreiber, S.; Villanacci, V.; Warren, B.F.; European Crohn's and Colitis Organisation (ECCO). European evidence-based Consensus on the diagnosis and management of ulcerative colitis: Definitions and diagnosis. J Crohns Colitis 2008, 2, 1–23. [CrossRef]
- Villanacci, V.; Antonelli, E.; Reboldi, G.; Salemme, M.; Casella, G.; Bassotti, G. Endoscopic biopsy samples of naïve "colitides" patients: role of basal plasmacytosis. J Crohns Colitis 2014, 8, 1438–1443. [Google Scholar] [CrossRef]
- Bessissow, T.; Lemmens, B.; Ferrante, M.; Bisschops, R.; Van Steen, K.; Geboes, K.; Van Assche, G.; Vermeire, S.; Rutgeerts, P.; De Hertogh, G. Prognostic value of serologic and histologic markers on clinical relapse in ulcerative colitis patients with mucosal healing. Am J Gastroenterol. 2012, 107, 684–692. [Google Scholar] [CrossRef] [PubMed]
- Pai, R.K.; Geboes, K. Disease activity and mucosal healing in inflammatory bowel disease: a new role for histopathology? Virchows Arch. 2018, 472, 99–110. [Google Scholar] [CrossRef] [PubMed]
- Farkas, K.; Reisz, Z.; Sejben, A.; Tiszlavicz, L.; Szűcs, M.; Nyári, T.; Szepes, Z.; Nagy, F.; Rutka, M.; Balint, A.; Bor, R.; Milassin, Á.; Molnàr, T. Histological activity and basal plasmacytosis are nonpredictive markers for subsequent relapse in ulcerative colitis patients with mucosal healing. J Gastroenterol Pancreatol Liver Disord 2016, 3, 01–04. [Google Scholar] [CrossRef]
- Al-Haddad, S.; Riddell, R.H. The role of eosinophils in inflammatory bowel disease. Gut 2005, 54, 54,1674–1675. [Google Scholar] [CrossRef] [PubMed]
- Vande Casteele, N.; Leighton, J.A.; Pasha, S.F.; Cusimano, F.; Mookhoek, A.; Hagen, C.E.; Rosty, C.; Pai, R.K.; Pai, R.K. Utilizing Deep Learning to Analyze Whole Slide Images of Colonic Biopsies for Associations Between Eosinophil Density and Clinicopathologic Features in Active Ulcerative Colitis. Inflamm Bowel Dis. 2022, 28, 539–546. [Google Scholar] [CrossRef] [PubMed]
- Magro, F.; Doherty, G.; Peyrin-Biroulet, L.; Svrcek, M.; Borralho, P.; Walsh, A.; Carneiro, F.; Rosini, F.; de Hertogh, G.; Biedermann, L.; Pouillon, L.; Scharl, M.; Tripathi, M.; Danese, S.; Villanacci, V.; Feakins, R. ECCO Position Paper: Harmonization of the Approach to Ulcerative Colitis Histopathology. J Crohns Colitis 2020, 14, 1503–1511. [Google Scholar] [CrossRef]
- Dixon, M.F.; Genta, R.M.; Yardley, J.H.; Correa, P. Classification and grading of gastritis. The updated Sydney System. International Workshop on the Histopathology of Gastritis, Houston 1994. Am J Surg Pathol 1996, 20, 1161–1181. [Google Scholar] [CrossRef]
- Villanacci, V.; Bassotti, G.; Langner, C. Histological remission in inflammatory bowel disease: where are we, and where are we going? J Crohns Colitis 2015, 9, 428. [Google Scholar] [CrossRef]
- Magro, F.; Sabino, J.; Rosini, F.; Tripathi, M.; Borralho, P.; Baldin, P.; Danese, S.; Driessen, A; Gordon, I.O.; Iacucci, M.; Noor, N.; Svrcek, M.; Peyrin-Biroulet, L.; Feakins, R. ECCO Position on Harmonisation of Crohn's Disease Mucosal Histopathology. J Crohns Colitis 2022, 16, 876–883. [CrossRef]
- Mosli, M.H.; Parker, C.E.; Nelson, S.A.; Baker, K.A.; MacDonald, J.K.; Zou, G.Y.; Feagan, B.G.; Khanna, R.; Levesque, B.G.; Jairath, V. Histologic scoring indices for evaluation of disease activity in ulcerative colitis. Cochrane Database Syst Rev. 2017, 5, CD011256. [Google Scholar] [CrossRef]
- Novak, G.; Parker, C.E.; Pai, R.K.; MacDonald, J.K.; Feagan, B.G.; Sandborn, W.J.; D'Haens, G.; Jairath, V.; Khanna, R. Histologic scoring indices for evaluation of disease activity in Crohn's disease. Cochrane Database Syst Rev. 2017, 7, CD012351. [Google Scholar] [CrossRef] [PubMed]
- Römkens, T.E.H.; Kranenburg, P.; Tilburg, A.V.; Bronkhorst, C.; Nagtegaal, I.D.; Drenth, J.P.H.; Hoentjen, F. Assessment of Histological Remission in Ulcerative Colitis: Discrepancies Between Daily Practice and Expert Opinion. J Crohns Colitis 2018, 12, 425–431. [Google Scholar] [CrossRef] [PubMed]
- Magro, F.; Lopes, J.; Borralho, P.; Dias, C.C.; Afonso, J.; Ministro, P.; Santiago, M.; Geboes, K.; Carneiro, F.; Portuguese IBD Study Group [GEDII]. Comparison of the Nancy Index With Continuous Geboes Score: Histological Remission and Response in Ulcerative Colitis. J Crohns Colitis 2020, 14, 1021–1025. [Google Scholar] [CrossRef] [PubMed]
- Marion, L.; Amélie, B.; Zoubir, D.; Guillaume, C.; Elise, M.S.; Hedia, B.; Margaux, L.S.; Aude, M.; Camille, B.R. Histological Indices and Risk of Recurrence in Crohn's Disease: A Retrospective Study of a Cohort of Patients in Endoscopic Remission. Inflamm Bowel Dis. 2022, 28, 1395–1404. [Google Scholar] [CrossRef] [PubMed]
- Villanacci, V.; Antonelli, E.; Lanzarotto, F.; Bozzola, A.; Cadei, M.; Bassotti, G. Usefulness of Different Pathological Scores to Assess Healing of the Mucosa in Inflammatory Bowel Diseases: A Real Life Study. Sci Rep. 2017, 7, 6839. [Google Scholar] [CrossRef] [PubMed]
- Geboes, K.; Riddell, R.; Ost, A.; Jensfelt, B.; Persson, T.; Löfberg, R. A reproducible grading scale for histological assessment of inflammation in ulcerative colitis. Gut 2000, 47, 404–409. [Google Scholar] [CrossRef] [PubMed]
- Jauregui-Amezaga, A.; Geerits, A.; Das, Y.; Lemmens, B.; Sagaert, X.; Bessissow, T.; Lobatón, T.; Ferrante, M.; Van Assche, G.; Bisschops, R.; Geboes, K.; De Hertogh, G.; Vermeire, S. A Simplified Geboes Score for Ulcerative Colitis. J Crohns Colitis 2017, 11, 305–313. [Google Scholar] [CrossRef] [PubMed]
- Marchal-Bressenot, A.; Salleron, J.; Boulagnon-Rombi, C.; Bastien, C.; Cahn, V.; Cadiot, G.; Diebold, M.D.; Danese, S.; Reinisch, W.; Schreiber, S.; Travis, S.; Peyrin-Biroulet, L. Development and validation of the Nancy histological index for UC. Gut 2017, 66, 43–49. [Google Scholar] [CrossRef]
- Mosli, M.H.; Feagan, B.G.; Zou, G., Sandborn, W.J.; D'Haens, G.; Khanna, R.; Shackelton, L.M.; Walker, C.W.; Nelson, S.; Vandervoort, M.K.; Frisbie, V.; Samaan, M.A.; Jairath, V.; Driman, D.K.; Geboes, K.; Valasek, M.A.; Pai, R.K.; Lauwers, G.Y.; Riddell, R.; Stitt, L.W.; Levesque, B.G. Development and validation of a histological index for UC. Gut 2017, 66, 50–58. [CrossRef]
- Magro, F.; Lopes, J.; Borralho, P.; Lopes, S.; Coelho, R.; Cotter, J.; Dias de Castro, F.; Tavares de Sousa, H.; Salgado, M.; Andrade, P.; Vieira, A.I.; Figueiredo, P.; Caldeira, P.; Sousa, A.; Duarte, M.A.; Ávila, F.; Silva, J.; Moleiro, J., Mendes, S.; Giestas, S.; Ministro, P.; Sousa, P.; Gonçalves, R.; Gonçalves, B.; Oliveira, A.; Chagas, C.; Cravo, M:, Dias, C.C.; Afonso, J.; Portela, F.; Santiago, M.; Geboes, K.; Carneiro, F. Comparing the Continuous Geboes Score With the Robarts Histopathology Index: Definitions of Histological Remission and Response and their Relation to Faecal Calprotectin Levels. J Crohns Colitis 2020, 14, 169–175. [CrossRef]
- Caputo, A.; Parente, P.; Cadei, M.; Fassan, M.; Rispo, A.; Leoncini, G.; Bassotti, G.; Del Sordo, R.; Metelli, C.; Daperno, M.; Armuzzi, A.; Villanacci, V.; SHMHS Study Group. Correction to: Simplified Histologic Mucosal Healing Scheme (SHMHS) for inflammatory bowel disease: a nationwide multicenter study of performance and applicability. Tech Coloproctol. 2023, 27, 167–168. [Google Scholar] [CrossRef] [PubMed]
- Gui, X.; Bazarova, A.; Del Amor, R.; Vieth, M.; de Hertogh, G.; Villanacci, V.; Zardo, D.; Parigi, T.L.; Røyset, E.S.; Shivaji, U.N.; Monica, M.A.T.; Mandelli, G.; Bhandari, P.; Danese, S.; Ferraz, J.G.; Hayee, B.; Lazarev, M.; Parra-Blanco, A.; Pastorelli, L.; Panaccione, R.; Rath, T.; Tontini, G.E., Kiesslich, R.; Bisschops, R.; Grisan, E.; Naranjo, V.; Ghosh, S.; Iacucci, M. PICaSSO Histologic Remission Index (PHRI) in ulcerative colitis: development of a novel simplified histological score for monitoring mucosal healing and predicting clinical outcomes and its applicability in an artificial intelligence system. Gut 2022, 71, 889–898. [CrossRef]
- Iacucci, M.; Parigi, T.L.; Del Amor, R.; Meseguer, P.; Mandelli, G.; Bozzola, A.; Bazarova, A.; Bhandari, P.; Bisschops, R.; Danese, S., De Hertogh, G:, Ferraz, J.G.; Goetz, M.; Grisan, E.; Gui, X.; Hayee, B.; Kiesslich, R.; Lazarev, M.; Panaccione, R.; Parra-Blanco, A.; Pastorelli, L.; Rath, T.; Røyset, E.S.; Tontini, G.E.; Vieth, M.; Zardo, D.; Ghosh, S.; Naranjo, V.; Villanacci, V. Artificial Intelligence Enabled Histological Prediction of Remission or Activity and Clinical Outcomes in Ulcerative Colitis. Gastroenterology 2023, S0016-5085(23)00216-0. [CrossRef]
- Kuntz, S.; Krieghoff-Henning, E.; Kather, J.N.; Jutzi, T.; Höhn, J.; Kiehl, L.; Hekler, A.; Alwers, E.; von Kalle, C.; Fröhling, S.; Utikal, J.S.; Brenner, H.; Hoffmeister, M.; Brinker, T.J. Gastrointestinal cancer classification and prognostication from histology using deep learning: Systematic review. Eur J Cancer 2021, 155, 200–215. [Google Scholar] [CrossRef] [PubMed]
- Leoncini, G.;Gentili, M.; Lusenti, E.; Caruso, L.; Calafà, C.; Migliorati, G ; Riccardi, C. ;Villanacci, V.; Ronchetti, S. The novel role of glucocorticoid-induced leucine zipper as a marker of mucosal healing in inflammatory bowel diseases. Pharmacol Res 2022, 182, 106353. [CrossRef] [PubMed]
- Cari, L.; Rosati, L.; Leoncini, G.; Lusenti, E.; Gentili, M.; Nocentini, G.; Riccardi, C.; Migliorati, G.; Ronchetti, S. Association of GILZ with MUC2, TLR2, and TLR4 in Inflammatory Bowel Disease. Int J Mol Sci 2023, 24, 2235. [Google Scholar] [CrossRef] [PubMed]
- Ronchetti, S.; Ricci, E.; Migliorati, G.; Gentili, M.; Riccardi, C. How Glucocorticoids Affect the Neutrophil Life. Int J Mol Sci. 2018, 19, 4090. [Google Scholar] [CrossRef]
- Ricci, E.; Ronchetti, S.; Gabrielli, E.; Pericolini, E.; Gentili, M.; Roselletti, E.; Vecchiarelli, A.; Riccardi, C. GILZ restrains neutrophil activation by inhibiting the MAPK pathway. J Leukoc Biol. 2019, 105, 187–194. [Google Scholar] [CrossRef]
- Gentili, M.; Hidalgo-Garcia, L.; Vezza, T.; Ricci, E.; Migliorati, G.; Rodriguez-Nogales, A., Riccardi, C.; Galvez, J.; Ronchetti, S. A recombinant glucocorticoid-induced leucine zipper protein ameliorates symptoms of dextran sulfate sodium-induced colitis by improving intestinal permeability. FASEB J. 2021, 35, e21950. [CrossRef]
Figure 1.
(A) Crypt abscess (Hematoxylin-Eosin dye). Magnification x 40; (B) Cryptitis (Hematoxylin-Eosin dye). Magnification x 40; (C) Neutrophil infiltration in the lamina propria, intermingled with eosinophils (Hematoxylin-Eosin dye). Magnification x 40; (D) Neutrophil infiltration in the surface epithelium (Hematoxylin-Eosin dye). Magnification x 40.
Figure 1.
(A) Crypt abscess (Hematoxylin-Eosin dye). Magnification x 40; (B) Cryptitis (Hematoxylin-Eosin dye). Magnification x 40; (C) Neutrophil infiltration in the lamina propria, intermingled with eosinophils (Hematoxylin-Eosin dye). Magnification x 40; (D) Neutrophil infiltration in the surface epithelium (Hematoxylin-Eosin dye). Magnification x 40.
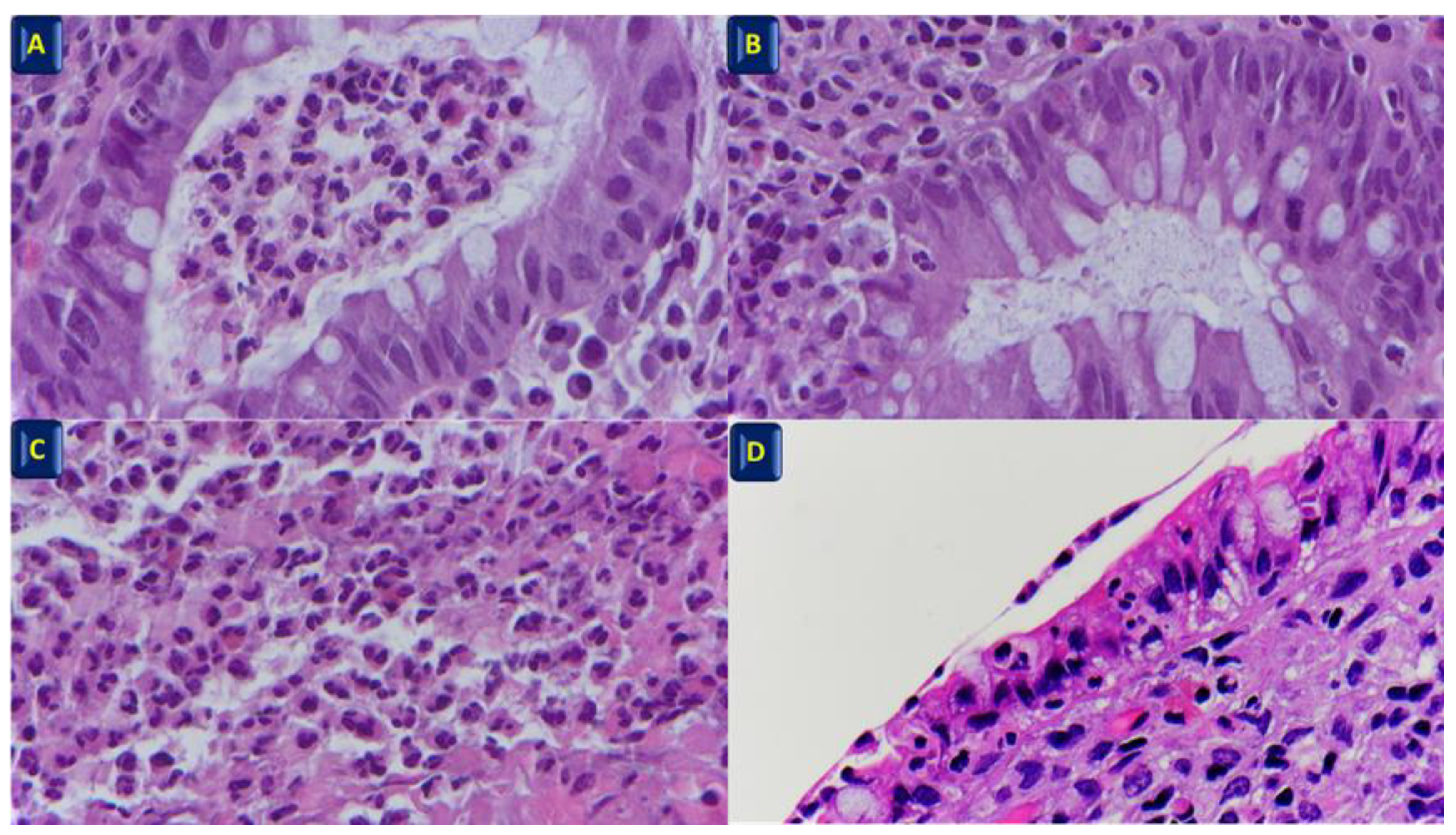

Table 1.
Main scores.
| Simplified Geboes Score | Nancy Score | Robarts Score | SHMHS | |||||
|---|---|---|---|---|---|---|---|---|
| Grade 0: No inflammatory activity |
0.0 No abnormalities 0.1 Presence of architectural changes 0.2 Presence of architectural changes and chronic mononuclear infiltrate |
Chronic inflammatory infiltrate (quantity of lymphocytes and plasmacytes in the biopsy) | 0 No increase 1 Mild but unequivocal increase 2 Moderate increase 3 Marked increase |
Chronic inflammatory infiltrate | 0 No increase 1 Mild but unequivocal increase 2 Moderate increase 3 Marked increase |
Part I. Features | ||
| Neutrophils in lamina propria | 1 Present 0 Absent |
|||||||
| Cryptitis or crypt abscesses (presence of neutrophils) | 1 Present 0 Absent |
|||||||
| Grade 1: Basal plasma cells |
1.0 No increase 1.1.Mild increase 1.2 Marked increase |
Neutrophils in the epithelium | 0 None 1<50% crypt involved 2>50% crypt involved |
Lamina propria neutrophils | 0 None 1 Mild but unequivocal increase 2 Moderate increase 3 Marked increase |
Erosions or ulcerations (presence of granulation tissue) | 1 Present 0 Absent |
|
| Grade 2A: Eosinophils in lamina propria | 2A.0 No increase 2A.1 Mild increase 2A.2 Marked increase |
Ulceration (visible epithelial injury, regeneration, fibrin,tissue granulation) | 0 Absent 1 Present |
Part II. Site of involvement | ||||
| Neutrophils in the epithelium | 0 None 1<5% crypts involved 2<50% crypts involved 3>50% crypts involved |
Ileum (CD patient only) | 1 Active 0 Quiescent 0 Not involved |
|||||
| Grade 2B: Neutrophils in lamina propria | 2B.0 No increase 2B.1 Mild increase 2B.2 Marked increase |
Acute inflammatory cell infiltrate | 0 None 1 Mild 2 Moderate 3 Severe |
Right colon | 1 Active 0 Quiescent 0 Not involved |
|||
| Erosion or ulceration | 0 No erosion, ulceration or granulation tissue 1 Recovering epithelium+ adjacent inflammation 1 Probable erosion-focally stripped 2 Unequivocal erosion 3 Ulcer or granulation tissue |
|||||||
| Grade 3: Neutrophils in epithelium | 3.0 None 3.1<50% crypts involved 3.2>50% crypts involved |
Mucin depletion | 0 None 1 Mild 2 Moderate 3 Severe |
Trasverse colon | 1 Active 0 Quiescent 0 Not involved |
|||
| Grade 4: Epithelial injury (in crypt and surface epithelium) | 4.0 None 4.1 Marked attenuation 4.2 Probable crypt destruction: probable erosions 4.3 Unequivocal crypt destruction: unequivocal erosions 4.4 Ulcer or granulation tissue |
Neutrophils in lamina propria | 0 None 1 Mild 2 Moderate 3 Severe |
Descending Colon | 1 Active 0 Quiescent 0 Not involved |
|||
| Sigmoid colon and rectum | 1 Active 0 Quiescent 0 Not involved |
|||||||
| Basal plasmacytosis | 0 None 1 Mild 2 Moderate 3 Severe |
|||||||
| Serrated architectural (defined as the presence of dilated crypts showing a scalloped lumen) | 0 None 1<5% crypt involved 2<50% crypt involved 3 >50% crypt involved |
|||||||
SHMHS: Simplified Histologic Mucosal Healing Scheme.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



