
Submitted:
21 May 2023
Posted:
22 May 2023
You are already at the latest version
Abstract
Targeted radionuclide therapy is become increasingly prominent as a nuclear medicine subspe-cialty. For many decades, treatment with radionuclides has been mainly restricted to the use of iodine-131 in thyroid disorders. Currently, radiopharmaceuticals, consisting of a radionuclide coupled to a vector that binds to a desired biological target with high specificity, are being de-veloped. The objective is to be as selective as possible at the tumor level, while limiting the dose received at the healthy tissue level. In recent years, a better understanding of molecular mecha-nisms of cancer, as well as the appearance of innovative targeting agents (antibodies, peptides, small molecules) and the availability of new radioisotopes, have enabled considerable advances in the field of vectorized internal radiotherapy with a better therapeutic efficacy, radiation safety and personalized treatments. For instance, targeting the tumor microenvironment, instead of the cancer cells, now appears as particularly attractive. Several radiopharmaceuticals for therapeutic targeting have shown clinical value in severals types of tumors and have been or will soon be approved and authorized for clinical use.
Keywords:
Radionuclide therapy
; nuclear medicine
; radiopharmaceutical
; antibody
; peptide
; small molecule inhibitor
; tumor
; microenvironment
1. Introduction
In the 1940’s, the use of iodine-131 in the treatment of benign and malignant thyroid disorders turned nuclear medicine into a therapeutic reality. Since that time, millions of patients, particularly with differentiated thyroid carcinoma, have been effectively treated with radioiodine, due to high affinity of the iodide ion (I-) for a transmembrane glycoprotein expressed at the surface of thyroid cells, the sodium/iodide symporter (NIS) [1].
Subsequently, relying on a number of different mechanisms to achieve selective uptake in tissues, other radiopharmaceuticals have appeared for the treatment of various malignant tumors [2,3]. To name a few, small synthetic molecules targeting metabolic processes, such as radiophosphorus and metaiodobenzylguanidine, or targeting extracellular mechanisms, like bone seeking agents, biological compounds targeting specific cell surface receptors or antigens, or particulates delivered in situ or in the vicinity of the tumor, such as radioiodized oil or radiolabeled microspheres for the radioembolization of liver tumors, or radiocolloids for radiosynovectomy of painful joints in rheumatoid arthritis. Though the concept of using radionuclides as a treatment modality is not new, the latest advances in understanding of the complex molecular mechanisms underlying cancer biology and with the knowledge of radiobiology, nuclear medicine has moved towards the use of more and more specific radiotracers, for research and clinical use [4].
Ionising radiation causes irreversible damage to the DNA of targeted cancer cells, directly related to the nature and energy of the radiation emitted, which may lead to apoptosis (Figure 1). Unlike external-beam radiotherapy (EBRT), with radionuclide therapy (RNT), the decay of the radionuclide near the target cells delivers a constant radiation dose at a low dose rate (6 versus about 0.01-1.00 Gy/min respectively). The foremost advantage of RNT over EBRT is the fact that it has proven to be useful for the treatment of both localized tumors and small metastatic tumors spread throughout the body [5].
Radionuclides, radiolabeled molecules, or radiolabeled supramolecular objects (nano- or microparticles) are systemically or loco-regionally injected to target and kill selected cells or tissues while sparing healthy ones. Contrary to molecular imaging, which uses radionuclides which are very penetrating but not very ionizing (γ or β+-emitting radionuclides), RNT makes use of radionuclides with lower penetrating but more energetic, hence more ionizing, emissions (β-, α or Auger e- emitters) (Table 1). As illustrated on Figure 1, β- particles are able to irradiate large volumes of multicellular dimensions. Because of their long range in tissue, they are considered ideal to treat large tumors, but it also implies that untargeted neighboring cells may be exposed to irradiation too (cross-fire effect). α particles can irradiate tumors of cell dimensions. Targeted α-therapy (TAT) is therefore generally used for the treatment of small hematological tumors or micrometastases. Auger electrons irradiate volumes with subcellular dimensions. They are especially appropriate for delivering high levels of radiation directly to the nucleus of cancer cells, avoiding off-site damages [6,7]. Main challenge will therefore be the careful targeting to the selected site [8].
There have been impressive results with some therapeutic radiopharmaceuticals or radioactive constructs not actively targeted at a specific site, such as the aforementioned radioiodine, [223Ra]radium dichloride for the management of painful bone metastases in mCRPC patients or radioembolization of liver cancers [1,9,10]. But, the use of a specific vector molecule of a tumor target can allow selective and specific accumulation of radioactivity on its target with a favorable tumor-to-healthy tissue ratio. The ideal target is a receptor overexpressed in a malignant cell, while having no or very little expression in physiological tissues. It should be easily accessible, and thus preferentially expressed on the cell membrane or possess an extracellular moiety [11]. Such targets include cell-surface and transmembrane glycoproteins (such as cluster of differentiation (CD) antigens, folate receptors…), glyco- or phospholipids (e.g. disialoganglioside GD2, phosphatidylserine…), carbohydrates (e.g. lectins), cell-surface receptors (e.g. G protein-coupled receptors), integrins (e.g. αVβ3 …), growth factor receptors (e.g. EGFR and VEGFR), transporters (e.g. LAT1, norepinephrine transporter …), or enzymes (e.g. matrix metalloproteinase …) [12,13]. To address those targets, receptor-specific ligands range from small biomolecules and synthetic inhibitors, peptides and peptidomimetics, mono- and polysaccharides to large proteins and oligonucleotides (antibodies and fragments, aptamers …), peptides and peptidomimetics, mono- and polysaccharides (e.g., mannose, N-acetylgalactosamine, hyaluronic acid…), to small bio- and synthetic molecules (e.g., nucleosides, vitamins, sulfonamides, rucaparib…) [14]. Unlike for targeted therapies and immunotherapy, heterogeneous target expression within the tumor mass is less of a problem for RNT, because it only necessitates a few bound molecules to destroy the target cell. Consequently, it is possible to destroy cells that have low expression levels.
Generally, with β- emitters, it necessitates the specific attachment of several hundreds radiotracers to the targeted cell in order to be able to destroy it, whereas α-emitters, due to their high radiotoxicity, only need a few of them. Since several different receptors are likely to be conjointly overexpressed on cancer cells, multitargeting might be an elegant method for enhanced targeting [15].
Over the past two decades, our understanding of cancer biology has improved significantly. Cancer now appears to be a profoundly heterogeneous pathology, with substantial intra- and inter tumoral variability. Thus, the characteristics of cancer have changed from a cell-centred view, with tumors consisting in malignant cells only, to a more comprehensive tissue-oriented one, including also stromal cells and extracellular matrix components, which account for over 90 % of the tumor mass and form the tumor microenvironment (TME) [16]. Though varying between patients, there are strong similarities among individuals’ TME phenotypes [17]. The TME is a dynamic ecosystem in which complex interactions occur between malignant cells and the extracellular matrix (ECM), as well as with resident and recruited cells. It stimulates tumor growth, immune evasion, and metastasis by creating a tumor-permissive microenvironment, characterized by high interstitial pressure, hypoxia, acidosis, angiogenesis and a deregulated metabolism. [18]. It thus plays an essential role in therapeutic resistance [19,20]. In view of these characteristics and their universal expression in a large subset of cancers, TME biomarkers represent attractive targets for RNT [21].
In particular, cancer-associated fibroblasts (CAFs), have been shown to participate in tumor progression by secreting cytokines, growth factors and exosomes and to inhibit therapeutic response by promoting fibrosis and solid stress [22]. Due to their direct participation to the invasion of neighboring tissues and the resistance to treatment, it has been postulated that selectively irradiating CAFs could lower the risk of recurrence due to residual disease. The immune response has also recently attracted attention as a target of choice [23]. While tumor-associated macrophages (TAMs) have only been targeted with diagnostic radiopharmaceuticals, tumor-infiltrating lymphocytes (TILs) represent one of the currently most promising targets both for imaging and therapy [24,25]. Another strategy could be to target the tumor’s abnormal vasculature, neoangiogenesis, to starve the tumor and eventually kill it [26]. Targeting extracellular matrix and altered TME processes might be another alternative [27]. In solid tumors, microvasculature is often anomalous, resulting in an imbalance between oxygen supply and consumption. As a result, hypoxia is a key feature in most solid tumors and is often associated with poor outcome. In fact, it is closely associated with tumor growth, malignant progression and resistance to chemotherapy and radiotherapy. This could make hypoxia an attractive therapeutic target [28]. All these advances stimulated the exploration of new potential specific targets for RNT [29] (Figure 2).
Until recently, RNT was generally considered only as a therapy of last resort and was not part of the clinical referral process. In most cases, it has only been available in a few number of centres in the context of small clinical trials or for compassionate use [4,30]. The vast majority of investigated therapeutic radiotracers are in a preclinical stage. Yet, because of impressive outcomes against primary cancers as well as distant metastases, it is now accepted as a safe, effective and economically viable therapeutic modality. Targeted RNT is therefore receiving renewed attention from the oncology community as well as from pharmaceutical firms [31]. An overview of the important considerations involved in developing targeted radionuclide therapies is given in Figure 3.
2. Radioimmunotherapy (RIT)
2.1. Antibodies and derivatives
Although monoclonal antibodies have widely demonstrated their therapeutic potential in oncology and beyond, it is nevertheless possible to increase their effectiveness by coupling them to radioelements. The first historical use of radiolabeled antibodies in human was performed by William H. Beierwaltes in 1950’s and shown promising results [32]. Despite these encouraging results, it was not before the end of the 1970’s that this new therapeutic modality started to rise, with the discovery, by Kohler and Milstein, of the hybridoma technology to produce monoclonal antibodies (mAb) specifically directed at tumor antigens [33]. The first clinical use of a radioimmunoconjugate was achieved for localised irradiation of B-cell lymphoma [34]. The rationale of this therapeutic approach combining the specificity of mAbs associated to the cytotoxic effects of radionuclides is important and paved the way of the RIT in cancer management.
Despite the success of this first RIT clinical trial, health regulators, concerned about potential dosimetric side-effects on healthy tissue, have slowed the development of this promising strategy. This initial indication (B-cell lymphoma) was the result of a judicious choice, considering both the high antigen overexpression and the radiosensibility of the tumor. In the 2000s, non-Hodgkin's lymphoma (NHL) was the first major application of radiolabeled monoclonal antibodies. In this indication, two radioimmunoconjugates able to target the CD20 antigen have been approved by a number of national regulatory authorities: [131I]I-tositumomab (Bexxar®) and [90Y]Y-ibritumomab tiuxetan (Zevalin®). Clinical results obtained with Bexxar® or Zevalin® showed a significant efficacy and a long-term response [35]. Knowledge increase in hematologic malignancies has allowed the development of new mAbs targeting other antigens, such anti-CD22 (epratuzumab), anti-CD37 (lilotomab) or anti-tenascin. These mAbs were radiolabeled with 90Y, 131I or 177Lu for clinical use in non-Hodgkin’s lymphoma trials [36,37,38,39].
Subsequently, chimeric and humanized antibodies were developed as a result of biotechnological advances in mAb production. As was anticipated, these compounds have proven to be less immunogenic and have a better pharmacological tolerability profile for patients. The new properties of humanized mAbs allowed multiple injections and dose fractionation to increase overall tumor irradiation and improve survival of healthy cells. However, mAbs have the pharmacokinetic disadvantages of being large molecules that diffuse relatively slowly and poorly within solid tumor. In order to overcome these disadvantages, bioengineers and immunochemists have developed antibody fragments such as F(ab) and F(ab’)2. Those smaller protein fragments, which conserve the specificity/affinity of entire mAbs, are produced by the reduction/digestion of initial mAb. In a recent clinical trial, an F(ab')2 fragment targeting the sodium-dependent phosphate transport protein 2b (NaPi2b) was used in radioimmunotherapy for ovarian cancer. High efficacy in small solid tumors was demonstrated in this trial. Although F(ab')2 is cleared by kidneys, side effects have been reported to be acceptable [40]. Based on this successful proof-of-concept for mAb fragments, bioengineering has led to the development of other small synthetic proteins (Figure 4), like minibodies or fusion protein-like single-chain variable fragments (scFvs), which contain only a few parts of the entire mAb. Minibodies comprise CH3 (constant heavy 3) and VL / VH (variable light and variable heavy) moieties, where as single chain variable fragments (scFv) are composed of VL / VH moieties only. Minibodies and scFv are currently used for clinical imaging applications in nuclear medicine. Such engineered minibodies and scFv have been radiolabeled essentially with β+ radiotracers for PET imaging, but also with β- or α- radiotracers for radionuclide therapy [41]. To date, therapeutic studies are still in the preclinical phase, but studies in human start to come out [42].
Single domain antibodies (also known as sdAb or nanobodies) have lately been developed from heavy chains antibodies found in camelids (dromedaries, camels, llama, etc.). They are composed of a monomeric part of the mAb VH fragment. It has now been possible to generate them from microbial hosts, and it appears that they will be used in future RIT clinical trials [43]. On the other hand, preclinical studies are underway on synthetic compounds consisting of three alpha-helix scaffold proteins (called affibodies) selected from a phage display library for their affinity to a specific antigenic structure [44].
2.2. Pretargeting approach
The risk-to-benefit ratio of RIT is mainly driven by the ability to irradiate the tumor with a reduced dose to healthy tissues. To optimize the tumor cell delivery dose, pretargeting approach was developped in order to reconcile the relatively long pharmacokinetic half-lives of mAbs and the need for fast tumor biodistribution of the radionuclides. Pretargeting involves pre-injection a non-radioactive bispecific antibody followed by injection a radiolabeled bivalent hapten peptide [45]. This protocol known as “Affinity Enhancement System – AES” allows to circumvent the slow clearance of the mAb. After a determination of the best time interval between the two injections (i.e. bispecific mAb and radiolabeled hapten) the hapten, designed to bind rapidly and specifically to the bispecific antibody pre-localized on the tumor, can be injected. The unbound haptens are rapidly excreted from the circulation via the kidneys, resulting in minimal exposure of healthy tissue.
In different clinical trials, encouraging therapeutic outcomes have been obtained using an anti-CEA pretargeted approach, in metastatic medullary thyroid carcinoma [46,47]. The conclusion of these studies is a favourable balance between efficacy and toxicity, with a long-term stabilisation of the disease.
2.3. Dose fractionation approach
One of the most frequent side effects with RIT concerns haematological toxicity. The recent arrival of humanized mAbs made it possible to consider the possibility of dose-fractionation with repeatable injections of the radiolabeled antibody. This dose-fractionation approach is well known in conventional external radiotherapy and allows a bone marrow regeneration between two injections. The dose-fractionation approach allows an increase in total injected dose compared to the classical single dose protocol, with an improvement of the clinical efficacy (in term of progression free survival) without increment of the toxicity [48,49].
3. Oligonucleotides
Oligonucleotides appear to be relevant in RNT, and are thus currently studied at the preclinical level. Oligonucleotides consist in short single-stranded oligomers of purine and pyrimidine bases. They exhibit the interesting capacity to bind with high specificity to biological structures, with the same order of magnitude than antibody-antigen binding (KD is in nanomolar or sub-nanomolar range) [50]. These oligonucleotides are synthetic compounds and could be constituted by ribonucleotides (RNA aptamers) or deoxyribonucleotides (DNA aptamers). Aptamer compounds were developed in the beginning of the 1990s from a large library of randomly selected oligonucleotide sequences. The oligonucleotide sequence with the best affinity for a given biological target was selected in vitro by the SELEX method (Systematic Evolution of Ligands by Exponential Enrichment). The stability of these bioconjugates under several chemical conditions for radiolabeling, their ease of functionalization with various chemical moieties for the labeling with different radionuclides, coupled to their comparatively low production cost have been their major advantages over monoclonal antibodies. Initial investigations in nuclear medicine, in preclinical studies, made use of aptamers for diagnostic applications, which confirmed these could be used as radionuclide vectors [51]. However, their use was rather limited due to the rapid renal clearance in vivo and the substantial instability towards nucleases. Several approaches have been developed to optimize these pharmacokinetic profile, like the introduction of non-oligonucleotide patterns in the aptamer sequence, for instance sugar rings, phosphodiester bonds or unnatural nucleotides in the single strand [52]. A recent promising improvement is based on the modification of the sugar chain with phosphorodiamidate morpholino oligomers (PMO), to give compounds called morpholinos (Figure 5) with better pharmacodynamic and pharmacokinetic profiles [53]. The use of this class of conjugates for RNT has not yet reached the clinical stage but may represent an elegant solution, holding great promises in the near future, and their development thus deserves to be followed [54].
4. Peptide Receptor Radionuclide Therapy (PRRT)
Peptides, usually classified as containing less than 50 amino acids, are much smaller biomolecules. Peptides offer numerous advantages, including non-immunogenicity, favorable pharmacokinetics and simple production. On the other hand, major limitations are possible nephrotoxicity due to high renal absorption and rapid in vivo degradation. Most natural peptides have a high affinity for their receptors, but, due to their rapid degradation, cannot be used for targeting for imaging or therapy. Peptides are nevertheless straightforwardly modified to improve stability, receptor affinity and permit the convenient grafting of various radiolabels [55,56,57]. However, the modifications of these small molecules to allow their labeling and improve their stability can strongly disturb their binding to the receptor if the amino acids essential for the binding have been modified or if the coupling of the chelating agent induces a phenomenon of steric hindrance. In the case of peptides, the difficulty therefore lies in obtaining molecules exhibiting a certain stability in vivo, while retaining sufficient affinity for cancer cells [58,59].
Many human tumors overexpress regulatory peptide receptors (Table 2), most of which belong to the G protein-coupled receptors (GPCRs) superfamily, a class of transmembrane receptors that are responsible for the transport of a variety of molecules across membranes. Peptides represent a particularly relevant class of molecules for medical use, particularly, but not exclusively, in nuclear oncology [60,61,62]. Many radiolabeled peptide derivatives are currently undergoing clinical trials around the world, one (a 177Lu-labeled somatostatin analog, Lutathera®) has even recently been approved for use.
4.1. The G protein-coupled receptors family
4.1.1. Somatostatin analogs
Somatostatin (SST) is a hormone peptide naturally present in the human body. It exists in two active forms of 14 and 28 amino acids, and is secreted by cells of the hypothalamus but also of the stomach, intestine and pancreas. Somatostatin has a regulatory function of the endocrine system, and plays a role in the neurotransmission and cell proliferation. To play its role, somatostatin binds to 5 membrane receptors subtypes named SSTR1 to SSTR5. Those receptors are widely expressed in healthy tissues, with distinct level. In several tumor contexts such as gastroentero-pancreatic neuroendocrine tumors (GEP-NET), as well as pituitary adenomas and some other malignancies (e.g., hepatocellular carcinomas, lymphomas, small cell lung cancers, etc.) SSTRs are overexpressed [63]. Therefore, many somatostatin analogues have been developed to target these membrane receptors for therapeutic purposes, with mixed results, except for neuroendocrine tumors, for which those analogs have been approved (Table 3). Many somatostatin analogs have already been labeled with various radioelements, whether for imaging or for therapy, with probes used today in routine clinical applications, and more compounds that are in clinical stage [64]. Four somatostatin analogs are currently approved for neuroendocrine tumor imaging, [111In]In-Pentetreotide ([111In-DTPA0]-octreotide, Octreoscan®), now increasingly replaced by [68Ga]Ga-DOTATATE (NETSPOT™), [64Cu]Cu-DOTATATE (Detectnet™), both approved in the US, and [68Ga]Ga-DOTATOC (Somakit TOC®) in both Europe and the US [65]. On the therapeutic side, [177Lu]Lu-DOTATATE (Lutathera®) has been approved in well-differentiated, unresectable or metastatic, progressive midgut neuroendocrine tumors, both in Europe and in the US [66].
PRRT with somatostatin analogs has been widely reviewed [64,67,68,69,70]. Eventually, two beta emitters derivatives, [90Y]Y-DOTATOC (Octreother®) and [177Lu]Lu-DOTATATE (Lutathera®), have demonstrated their clinical utility. The successful NETTER-1 Phase 3 trial, with [177Lu]Lu-DOTATATE, can be considered as the cornerstone of PRRT, which it established as a treatment modality to be considered, opening the way for a truly vibrant research area [71]. Current and extensive research with [177Lu]Lu-DOTATATE aims to improve the safety and efficacy of this PRRT and allows the identification of prognostic and predictive factors to optimize the patient care management, to enlarge possible indications [72]. In parallel, α-labeled somatostatin analogs (either DOTATOC or DOTATATE) were shown to outperform 177Lu [73,74,75].
Unexpectedly, but with increasing evidence, antagonist analogs have been proven to outperform agonist ones (higher tumor uptake, better dosimetry profile, and faster clearance), despite the absence of internalization of the ligand-receptor complex [76]. This higher tumor uptake is a direct consequence of the presence of more target binding sites for antagonists associated to a more slowly dissociation than for agonists. This may notably widen applications to targeting to tumors with lower receptors expression [77]. Preclinical and clinical studies have confirmed the potential superiority for antagonist-based tracers [78]. However, the firstly SSTR antagonist developed ([111In]In-DOTA-BASS) has shown only a very modest affinity for the principal expressed SSTR subtype (SSTR2) in neuroendocrine tumor. To go around this issue, a second generation of this class of biomolecules was designed (LM3, JR10, and JR11), with improved pharmacological characteristics (cf. Table 4) [79]. A pilot study first compared [177Lu]Lu-DOTA-JR11 ([177Lu]Lu-satoreotide tetraxetan) with [177Lu]Lu-DOTATATE. The results showed a higher tumor dose up to 10 times greater for the antagonist compound [80]. As a consequence, a phase I study was performed. This clinical trial includied 20 refractory and well-differentiated NET patients who have been treated with an activity of 7.4 GBq per 3 months, 6 patients receiving 1 cycle and 14 receiving 2 cycles. Preliminary results were encouraging, with a response rate of 45 %, a disease control in 85 % of patients and a median progression-free survival of 21 months. There were, however, some safety concerns, since grade 4 myelosuppression was observed in 57.1% (4/7) of cases after the second cycle, requiring a protocol amendment to reduce the activity of the second cycle by 50 %, in order to limit the bone marrow dose to 1 Gy. [81]. [177Lu]Lu-DOTA-LM3, on its side, has been studied in 51 NET patients using the same dosimetry protocol as for [177Lu]Lu-DOTATATE. Once again, antagonist compound showed a higher tumor dose and disease control was observed in 85% of patients, without severe adverse effects except for thrombocytopenia in a few patients [82]. Current developments thus logically focus on the use of α-emitting nuclides and a switch from agonist to antagonist somatostatin analogs [83,84].
4.1.2. Bombesin analogs
Gastrin-releasing peptide receptors (GRPr) are a subtype of the bombesin receptor family, overexpressed in several malignancies, among which lung, prostate, breast, gastric and colorectal carcinomas [85]. Their activation stimulates both cell growth and proliferation. Bombesin is a natural 14-amino acid peptide isolated from the frog Bombina bombina with a strong-affinity for GRPr. Its 27-amino acid mammalian version, named GRP, shares the same final 7 amino acids sequence (Trp-Ala-Val-Gly-His-Leu-Met-NH2), used in the receptor recognition. Several radiolabeled bombesin derivatives have thus been developed and investigated, as a useful tool for the detection and/or treatment of cancers [86]. To date, bombesin derivatives have been mainly investigated in clinical studies for imaging approaches. Recently, bombesin derivatives have been the subject of therapeutic clinical studies after radiolabeling with 177Lu, but several preclinical studies with other β- and α-emitters have been reported [87].
The first, and still the most widely tested, therapeutic analog, is [177Lu]Lu-AMBA ([177Lu]Lu-DOTA-Gly-4-aminobenzyl-BBN(7–14)). [177Lu]Lu-AMBA has initially been investigated in a phase I study, with 7 patients who suffered from hormone-refractory metastatic prostate cancer, with disappointing results, because of a low plasma stability and strong pancreas uptake [88]. As with somatostatin analogs, bombesin antagonists have been reported to outclass agonists [89,90]. GRPr antagonists RM2 and NeoBOMB1 (now rechristened NeoB) (Table 4), were labeled with 68Ga for imaging breast and prostate cancer patients. Results displayed high contrast for the tumor lesions, despite lower internalization. Therapeutic applications, with 4.5 ± 0.9 GBq of [177Lu]Lu-RM2, have been considered in a first-in-human dosimetry study [91]. Some preliminary results in 4 patients suffering from mCRPC showed mean absorbed dose of 6.20 ± 3.00 Gy/GBq in the tumor lesions without side effects. Major risk organ appears to be the pancreas. A derivative with improved stability and affinity, [177Lu]Lu-AMTG ([177Lu]Lu-α-Me-l-Trp8-RM2), has recently been reported [92]. [177Lu]Lu-NeoB is currently investigated in a Phase I/II study in patients with advanced solid tumors (NCT03872778). The patients were selected after preclinical evaluation for GRPr expression [93,94]. The preliminary results with these antagonists showed a need for further optimization, in particular regarding safety [87]. Lately, an original 67Cu-labeled antagonist derivative has been reported, [67Cu]Cu-SAR-BBN, demonstrating encouraging tumor inhibition in mice bearing prostate carcinoma model [95]. Of note that a clinical trial is currently underway in Australia with the homologous diagnostic [64Cu]Cu-SAR-BBN, in metastatic ER+/PR+/HER2- breast cancer (ACTRN12619001383156).
4.1.3. Substance P
Neurokinin (or tachykinin) receptors are located in the central and peripheral nervous system and possess three subtypes, NK1, NK2 and NK3. Among them, NK1 has been proven to be overexpressed in primary malignant gliomas [96]. Physiologically, substance P (SP), an 11-amino acid neuropeptide, is an endogenous ligand for NK1 receptor. As a consequence, this neuropeptide appears as an interesting targeting agent for brain tumors imaging and therapy [97].
Initial results in some pilot studies with 90Y or 177Lu-labeled SP indicated potential clinical therapeutic indications. The growing interest towards α-particle-emitting radionuclides, particularly the short-lived 213Bi, brings encouraging preliminary results in term of feasibility, efficacy and safety [98]. The use of 1.4 to 9.7 GBq of [213Bi]Bi-DOTA-SP has demonstrated a median 5.8 months progression free-survival and 16.4 months overall survival time [99]. The radiotracer has been administered via a surgically implanted catheter inside the tumor or, after its resection, in the resultant cavity, to enable to pass the blood-brain barrier and improve tumor uptake. Currently, preclinical and early clinical studies are ongoing with other alpha-emitters such as 211At- or 225Ac. These innovative alpha-emitters radionuclides present the advantage of longer half-lives than 213Bi, respectively 9.9 days for 225Ac, 7.2 hours for 211At and 46 minutes for 213Bi.
4.1.4. Other analogs
G protein-coupled receptors form a large superfamily of cell-surface receptor. They represent a common large group of protein expressed in eukaryotes cells. Some of these receptors appears to be a credible alternative – or supplementary - target for nuclear medicine purposes [103]. Several promising results from preclinical and early clinical studies involving the utilization of radiolabeled peptides, targeting receptors such as glucagon-like peptide-1 (GLP-1), melanocortin type 1, neuropeptide Y, neurotensin, or vasoactive intestinal peptide, have been documented. [104,105,106]. Cholecystokinin-2 receptor is for instance of particular interest, especially in medullary thyroid carcinoma, and can be specifically targeted with gastrin-derived peptides [107]. Initial findings were reported regarding the use of [177Lu]Lu-PP-F11N ([177Lu]Lu-DOTA-(D-Glu)6-Ala-Tyr-Gly-Trp-Nle-Asp-PheNH2), a mini-gastrin analog labeled with 177Lu, for treating advanced medullary thyroid carcinoma in patients. According to the dosimetry results, it has been found to be a viable tool for therapy. However, stomach was the organ-at-risk, while absorbed doses in the kidney and bone marrow were low. [108]. There is therefore a wide field of possible investigations in this area of research.
4.2. C-X-C chemokine receptor type 4 (CXCR-4)
Chemokines are involved in many physiological and pathological processes linked to cell homing and migration. In this large chemokine family, the CXCR4 protein (also called fusin or CD184) is widely studied in nuclear medicine for RNT of cancers. CXCR4 is an alpha chemokine receptor for the stromal-derived factor-1 (SDF-1, also called CXCL12) initially discovered for its involvement in HIV infection. CXCR4 is naturally present in the blood cell lineage from hematopoietic stem cells (HSCs) and hematopoietic progenitor cells (HPCs), while stromal cells secrete CXCL12. The interplay between CXCL12 and CXCR4 plays a crucial role in regulating several hematological processes such as homing, quiescence, and retention of HSCs and HPCs in the bone marrow microenvironment [109]. More recently, studies have shown that the CXCR4 protein is expressed in over 20 types of human hematological and solid cancers. [110,111]. Tumor growth, metastasis, angiogenesis, relapse and therapeutic resistance have been correlated to an overexpression of CXCR4. Accordingly, CXCR4 could be a target of great interest for imaging (diagnosis and following) as well as in a therapeutic perspective [112]. Over the past two decades, several CXCR4 binding peptides have been developed, like the T140 series (linear 14 amino acid CXCR4 antagonist peptides), AMD3100 derivatives (bicyclam organic compounds acting as an inhibitor of CXCR4 function), and FC131 compounds (cyclopentapeptides also presenting a CXCR4 antagonistic activity). More recently, attention has shifted towards the development of another peptide, FC231, a small cyclic pentapeptide derivative presenting great promises for targeting CXCR4 for radiotherapeutic applications [113]. At preclinical time of FC231 derivatives, correlation between CXCR4 affinity and modifications in chemical structure were found. Through an extensive screening, the optimal peptide/chelator/radiometal combination in order to proceed to a radiopharmaceutical was established. To preserve the best affinity despite the radiolabeling, the chemical scaffold was adapted for imaging ([68Ga]Ga-Boclatixafortide; Pentixafor®) or therapy ([177Lu]Lu-Anditixafortide; Pentixather®) [114] (Figure 6).
Radiolabeled with β- emitting nuclides, as 90Y or 177Lu, Pentixather® has shown very promising results for poor prognosis patients with advanced multiple myeloma [115]. This success, coupled with the ubiquitous CXCR4/CXCL12 axis in the development of various hematologic and solid tumors, indicates a potential wideaspread use of CXCR4 targeting in RNT. Ongoing clinical investigations are being carried out to determine the safety and efficacy profile of CXCR4-targeted RNT. Typical side effects observed so far were blood dysplasia and kidney failure due to tumor lysis syndrome, while hepato- and overall nephrotoxicities remained limited [116]. Despite these side effects, CXCR4 has proven to be a safe and well-tolerated for therapeutic approaches in various clinical situations [117,118,119].
4.3. Other peptide derivatives
Several other peptide-based targeting agents have shown promising results for therapeutic purposes, such as integrins, especially the cell adhesion receptors αVβ3 and αVβ5. These integrins are notably engaged in various tumor processes, such as angiogenesis, proliferation, survival and metastasis [120]. The tri amino-acids sequence Arg-Gly-Asp (RGD), being specifically recognized by αVβ3 receptors, has led to the development of numerous radiolabeled RGD peptides, including dimeric compounds, with improved affinity [121]. These have been labeled with 90Y, 177Lu, and 188Re for therapeutic purposes, but none of these compounds have been used in clinic yet. A recent paper by Notni aims at explaining the reasons for the lack of clinical success for radiolabeled RGD peptides [122]. It has been postulated of other integrins might be more suitable for tumor targeting [123]. Another receptor, vascular endothelial growth factor receptor (VEGFR), which is particularly involved in the tumor neo-angiogenensis, could be targeted with radiolabeled peptides to affect the angiogenesis process [124]. Another membrane receptor related to vascular endothelial growth factor receptor which may be targeted with radiolabeled peptide is neuropilin-1, expressed by several tumors, like for instance glioma. A 177Lu-labeled peptide targeting NRP-1 has recently been reported, but need some more optimization before being considered further [125].
The expertise field concerning radiolabeling peptidic analog development is higly active, with an important increase in the number of reports [126,127]. A new method being explored is the development of peptides that target highly specific proteins in tumors, such as glypican 3 for hepatocellular carcinoma. [128]. Another strategy is to target different tumor compartments, such as ECM and TAMs. Innovative tools, such as cell-penetrating and tumor-homing peptides, also clearly deserve attention as putative radiopharmaceutical candidates. All of these potential avenues are currently being studied. [129].
5. Radioligand Therapy (RLT)
Compared to antibody- or peptide-based radiopharmaceuticals, small molecules present several pharmacological and pharmacokinetic benefits. They are typically less expensive to produce and have faster pharmacokinetics due to their lower molecular weights and higher lipophilicity. Furthermore, they can be radiolabeled in more stringent conditions (higher temperatures or broader pH range). Recent developments in non-peptidic antagonists have shown promising biological and physicochemical properties. These compounds, such as [177Lu]Lu-3BP-227, a potent neurotensin receptor 1 antagonist, has shown encouraging clinical results in a proof-of-concept clinical trial in pancreas cancer (Table 4)[130]. In a similar manner, though it has yet only been demonstrated in vitro or in mice models, 177Lu-labeled non-peptidic NK1R and CCK2R antagonists exhibited better binding characteristics than their respective agonists counterparts [102,131]. In addition, many indications take advantage of radioligand therapy with small organic molecules or metallic radiocomplexes.
5.1. Bone-seeking agents
Bone metastases are a very common complication in several cancer types. They notably occur in approximately half the cases of breast carcinoma, the primary cancer in females, and in 80% of men with prostate adenocarcinoma, the second most common one in males [132]. The term skeletal metastasis covers two entities; on the one hand, the infiltration of the bone marrow, which represents probably the first structure invaded, and, on the other hand, the involvement of the bone matrix, most often secondary to the first. Tumor infiltration is directly responsible for the pain phenomenon. Targeted radionuclide therapy can offer a significant therapeutic alternative to relieve pain for the patients [133]. Increased osteoblastic activity under the effect of metastatic tumor cells is responsible for the hyperfixation of the radiotracer. Consequently, all localizations are treated immediately by means of a single intravenous injection, even in the case of plurifocal lesions. However, there is no specificity of the fixation; any hypervascularization induces an hyperfixation. Initial use of therapeutic radionuclides to treat the pain of bone metastases relied on [32P]-orthophosphate or [32P]-biphosphonate, which are molecules having a very strong affinity toward calcium present in the actively growing bone [134,135]. Unfortunately, 32P has a high hematological toxicity, because of its significant dose delivered to bone marrow.
Subsequently, a large variety of radiopharmaceuticals able to deliver radiation to metastatic bone sites have been developed [136,137,138,139,140,141,142,143] (Table 5). Among all those developed compounds, four are currently commercially available: [89Sr]SrCl2 (Metastron®) and [223Ra]RaCl2 (Xofigo®), taking advantage of the Sr2+ and Ra2+ ions’ mimicking the Ca2+ cation, and thus having a natural tropism for the inorganic bone matrix, and [153Sm]Sm-EDTMP (Quadramet®), and [186Re]Re-HEDP ([186Re]Re-etidronate®), where the radionuclides are used as phosphonates (EDTMP = ethylenediaminetetramethylene phosphonate and HEDP = hydroxyethylidene diphosphonate), binding to the hydroxyapatite of bone surface, then penetrating deeper through remodeling of the matrix. To date, [223Ra]RaCl2 is the only one with a proven benefit on overall survival [141]. However, [188Re]Re-HEDP, replacing rhenium-186 with its rhenium-188 congener, might prove itself as clinically useful. Indeed, there has been some evidence that the latter could also lead to an improvement in overall survival. In a retrospective analysis, based on a former Phase 2 trial, repeated injections (from 1 to 3) were correlated with a gain in survival from 4.50 to 15.66 months [144,145]. A Phase 3 trial, aiming at comparing the respective efficacies of [188Re]Re-HEDP with [223Ra]RaCl2, , in patients with castration-resistant prostate cancer metastatic to bone is currently ongoing (RaRe trial, NCT03458559).
Beside rhenium-188, lutetium-177 is another potentially interesting radionuclide for bone-pain palliation [146]. Several clinical studies, investigating [177Lu]Lu-EDTMP and [177Lu]Lu-DOTAZOL (177Lu-zoledronic acid) have been published, warranting further investigation [147,148]. Nevertheless, with the advent of the radiotherapeutic PSMA derivatives, the question of the future clinical utility of these bone-seeking agents for the management of metastatic prostate cancers arises.
5.2. [131I]mIBG
Firstly designed to allow imaging adrenal medulla, meta-iodobenzylguanidine (mIBG), or iobenguane, is an aralkylguanidine radioiodinated in meta-position of its benzene moiety [149]. This physiological analogue of the noradrenaline (or norepinephrine) neurotransmitter is not metabolized and could be excreted without any modification unlike adrenaline. It could also be gathered by cell through either non-specific and non-saturable passive diffusion in all cells, or an active, specific, and saturable uptake in cells expressing the norepinephrine transporter, with high-affinity. This active absorption is reported in many tumors, especially those of neural crest and neuroendocrine origin (neuroblastoma, carcinoid tumors, paraganglioma, and pheochromocytoma) and is about 30 times more efficient than passive transport. [150].
MIBG can be commercially labeled with iodine-123 (123I), for the purpose of imaging, or iodine-131 (131I), for the purpose of therapy or, rarely, for imaging as well. [131I]mIBG is synthesized by isotopic exchange with radioiodine, resulting in a consequent amount of unlabeled mIBG (low specific activity, LSA) in the radiopharmaceutical product. This cold product can enter in competition with radiolabeled [131I]mIBG, restraining tumor cell uptake. However, another kind of process enables to yield no-carrier-added (n.c.a.) [131I]mIBG, with a very high specific activity (1600 mCi/mol, HSA) allowing a more potent therapeutic dose that is less likely to saturate receptors on tumor cells, thereby resulting in an increased cytotoxic activity. It has been reported, that repeated low-specific activity [131I]mIBG injections might be as effective in controlling tumor expansion [151]. EANM have established procedure guidelines to select best responding patients [152]. [131I]mIBG treatment is generally well tolerated, although high-dose treatment regimens are susceptible to conduce to a myelotoxicity.
There have been clinical studies demonstrating the effectiveness of both HSA and LSA [131I]mIBG as a therapeutic agent, and it has received approval in both the US and Europe [153]. However, there have been only limited randomized controlled trials and its availability has often been problematic, which has hindered its clinical use for the benefice of [177Lu]Lu-DOTATATE, that have replaced it in some indications [151,154]. Nevertheless, [131I]mIBG is still under clinical investigations. Recently, the potential use of Auger-emitting 125I or α-emitting 211At to replace 131I for the treatment of residual or metastatic pheochromocytomas and paragangliomas has been explored [155,156] and a first-in-human trial of [211At]mABG was recently introduced [157].
5.3. Prostate-specific membrane antigen (PSMA) inhibitors
Originally discovered in the 1990s, PSMA is an antigenic transmembrane glycoprotein presenting two enzymatic activities, acting as glutamate carboxypeptidase and folate hydrolase. Firstly, it has been described as a prostate specific enzyme, located in the cytosol of the physiologic prostate cells. In prostate cancer context, PSMA becomes an overexpressed transmembrane bound protein [158]. PSMA is not a secreted protein and it appears to have an upregulation in patients treated by an androgen deprivation therapy; metastatic lesions of prostate cancer also appear to be PSMA positive. In recent works, PSMA have been identified to be expressed in other malignancies as well, particularly in the neovasculature of tumors such as glioblastoma, renal cell carcinoma, hepatocellular carcinoma, lung cancer or breast cancer [159,160,161]. Initially, biologists created monoclonal antibodies like 7E11-C5.3 and HuJ591 directed towards PSMA. Currently, the clinical use of PSMA in nuclear medicine is based on small molecules that target PSMA enzyme activity, with better pharmacokinetic profile than antibodies, i.e. faster tumor uptake coupled with faster kidney elimination. Consequently, they present better dosimetric and efficacy profiles. [162]. The small molecules which target PSMA are urea-based enzyme inhibitors, and can be used for diagnosis and radionuclide therapy. The current development of PSMA inhibitors allows a theragnostic approach with PET imaging and therapeutic using respectively gallium-68 and lutetium-177. To achieve this radiolabeling, DOTAGA-chelator moiety was added to PSMA molecules in order to functionalize it; this new compound is dubbed PSMA-I&T (for Imaging and Therapy). To improve the pharmacokinetic profile (decreasing kidney and salivary gland absorption), some modifications were made to the PSMA-targeting molecules, leading to the creation of PSMA-617. (Figure 7). While preclinical studies in mice demonstrated that PSMA-617 had better renal dosimetry than PSMA-I&T, this advantage was not observed in humans and the two molecules appear to be quite similar. [163]. Despite this renal uptake, the Phase III global VISION clinical trial (NCT 03511664) showed promising results for [177Lu]Lu-PSMA-617 in RNT of metastatic castration-resistant prostate cancer (mCRPC) [164]. In terms of toxicity, the most exposed organs are kidneys, but they could be protected effectively by co-injecting an amino-acid solution, salivary glands leading to dry mouth syndrome, lacrimal glands and bone marrow. All of these adverse effects are transient and do not present a severe degree. The principal serious side effect is hematological symptoms of grade ≥ 3 which was reported in 12 % of treated patients [165]. Phase III global VISION clinical trial displayed major prolongations of imaging-based progression free and overall survivals, respectively 5.3 months (median 8.7 vs. 3.4 months) and 4.0 months (median 15.3 vs. 11.3 months).
Consequently, PSMA-targeting is rising in RNT and appears to be a real increment in the care management of metastatic castration resistant prostate cancer. Nevertheless, approximatively 30% of patients do not respond to the [177Lu]Lu-PSMA-617 RNT. α-particle emitting radionuclides, such as 225Ac or 213Bi, have been used to radiolabel PSMA-617, in order to increase the anti-tumor activity, and to treat relapsed patients with no major risk of side effects. First clinical use of [225Ac]Ac-PSMA-617 or [213Bi]Bi-PSMA-617 displayed images of complete response with no major hematologic toxicity. Only observed side effect was xerostomia due to the salivary gland uptake [166,167]. These preliminary results of α-RNT are promising and could be an alternative for advanced staged patients escaping [177Lu]Lu-PSMA-617. However, a large clinical trial have to be conducted to confirm these results.
5.4. Fibroblast-activation protein (FAP) inhibitors
Cancer-associated fibroblasts (CAFs) are the most abundant cell type inside the tumor microenvironment. They are characterized by the expression of fibroblast activation protein-α (FAP), a type II membrane-bound glycoprotein serine protease [168]. The latter is highly expressed on the cell surface of activated fibroblasts but not on quiescent ones. Of note, more than 90 % of epithelial cancers’ stroma are expressing FAP. In addition, FAP has notably been linked with a poor prognosis by enhancing tumor growth, matrix remodeling and angiogenesis. More than 28 tumor types have been proven to strongly fix a FAP-targeted 68Ga-radiopharmaceutical [169]. Consequently, this new targed has driven a high interest for therapy as well as for imaging [170].
Quinoline-based small molecules that function as FAP inhibitors (FAPis) have demonstrated highly promising outcomes in both preclinical and clinical investigations [171,172]. These molecules may also be the first pan-cancer theranostic agent. Multiple clinical studies have been conducted using [68Ga]Ga-FAPI-04, and it exhibited outstanding uptake in tumors, displaying high sensitivity and image quality across various tumors, though the evidence of some potential false-positive results may raise concerns [169,173]. Use of the ubiquitous DOTA chelator allows to substitute the diagnostic-aimed 68Ga with therapeutic nuclides, i.e. 90Y or 177Lu. Radiolabeled FAPi derivatives have thus been investigated in proof-of concept studies for potential therapeutic application, though, to date, no large clinical trial has been initiated. FAPI-04 appears to be limited by rapid clearance from tumor, resulting in a limited radiation dose [171,174]. Further derivatives were developed, such as FAPI-46 (Figure 8). Initial investigations in small cohorts with 90Y- and 177Lu-labeled FAPI-46 displayed encouraging results, since treatment was well tolerated, while it was observed some clinical response [175,176,177,178,179,180]. On the opposite, labeling with the β— emitter of medium-energy samarium-153, conducted to poor results due to low-specific activity in one case-report with sarcoma [181]. Yet, further clinical application may be challenging because of a too fast clearance and an insufficient tumor retention.
To improve pharmacokinetic profile, and subsequently therapeutic effectiveness, of these radiotracers, some ligand optimization has been performed. One strategy has been to attach an albumin-binder to extend circulation and increase tumor accumulation, with apparently encouraging results [182,183,184]. Another proposed strategy has been the use of dimeric agents [185,186]. A first-in-human study with a 177Lu-labeled squaric acid-derivatized dimeric FAPi derivative showed it was well tolerated and displayed a high tumor uptake [187]. This was further confirmed in a subsequent pilot study in 15 patients with iodine-refractory differentiated thyroid carcinoma [188].
The evaluation of novel labeled FAP-targeting agents in first-in-human studies has been initiated, with such compounds as FAP-2286, a DOTA-modified FAP-binding peptide chelator, and PNT6555, also a DOTA-based radiotracer, with a boronated FAP-targeting moiety, all radiolabeled with 177Lu (Figure 8). Only results regarding FAP2286 have been currently reported [189]. 11 patients with various primary tumors were treated with 5.8 ± 2.0 GBq of [177Lu]Lu-FAP-2286. It demonstrated long retention in the tumors, with acceptable side effects. Another FAP ligand, with ultra-high affinity, in the subnanomolar range (680 pM, vs. 6.5 nM for FAPI-04), has newly been reported, and labeled with 177Lu [190]. This radiotracer (OncoFAP) demonstrated a favorable in vivo biodistribution in tumor-bearing mice [191]. Its dimer derivative was demonstrated to display an even more stable and prolonged tumor uptake, with respectively 20 % ID/g vs. 4 % ID/g 24 h post-injection [192]. More studies need to be conducted to confirm their clinical usefulness.
Stromal and malignant cells in the primary tumor could be targeted using the cross-fire effect, radiolabeling FAPi with β--emitting radionuclides. Otherwise, α-particle or Auger electron emitting radionuclides’ short range could be exploited to target pro-tumorigenic CAFs while avoiding tumor-suppressive CAFs. For this purpose, [225Ac]Ac-FAPI was developed and evaluated in a pancreatic carcinoma model, displaying a rapidly emerging therapeutic effect but lasting less than its 177Lu-labeled counterpart [193]. However, the therapeutic effect was limited, leading to the suggestion that FAPI labeled with 188Re or 211At might be more appropriate. Yet, no 211At-labeled FAPi compound has been described so far. FAPI-34, on its side, has been reported as a FAPi ligand amenable for radiolabeling with 188Re, though its radiolabeling has only been reported for the homologous 99mTc right now [194].
There have been relatively few clinical studies conducted on FAP-targeted radionuclide therapy, and the results have been varied, which may be due to the multiple tumor types and patient conditions evaluated. Further research on ligand design is necessary. Additional research is necessary to establish the efficacy of this therapy, and it has been recommended that its use in combination with other treatment modalities, for instance immunotherapy, should be explored as it may provide a better efficacy [195,196].
5.5. Poly(ADP-Ribose)Polymerase (PARP) inhibitors
Poly(ADP-Ribose)polymerase (PARP), which are vital DNA repair enzymes associated with chromatin, are prominently expressed in the nucleus of mammalian cells. Due to the high rate of proliferation and replicative stress, tumor cells are susceptible to genomic instability, resulting in the overexpression of PARP, unlike normal ones [197]. Targeting of PARP enzymes has therefore recently emerged as potentially attractive to selectively target tumor tissues [198]. Blocking the expression of PARP, particularly PARP1, disrupts replication and leads to cell death, with a greater effect on faster-growing malignant cells. Additionally, PARP inhibition has been used as a chemo- or radiosensitizer in combination therapies [199]. In recent years, various PARP1-targeted inhibitors (PARPIs) like olaparib, talazoparib, and rucaparib have been approved for use. They have shown promises in preventing DNA repair after exposure to external-beam radiotherapy or radioimmunotherapy. To optimize the benefits of this treatment modality, it is crucial to non-invasively determine the level of PARP1 expression, as it could help predict the response to PARP inhibitor therapies [200]. Several radiolabeled PARPIs have thus logically been reported, mostly olaparib or rucaparib derivatives, both for imaging and therapy [201]. Alpha particles and Auger electron emitters are considered more appropriate, although there have been some descriptions of radiotracers labeled with beta particle emitters [202]. Latest efforts in the domain have been recently reviewed [203].
PARPis are a type of small organic molecules that are often preferred to be labeled with radiohalogens as they don’t require any chelator on the contrary of radiometals [204,205]. In a preclinical study, using a neuroblastoma model, [211At]At-MM4, a rucaparib derivative labeled with an alpha emitter, demonstrated favorable uptake and a significant increase in median survival especially with multiple fractionated doses, while toxicity remained limited [206]. On the other hand, an analog of [211At]At-MM4 labeled with an Auger emitter, [125I]I-KX1, was found to be less effective but could potentially be useful in treating micrometastatic neuroblastoma [207]. Another Auger-emitting PARPi, [123I]I-MAPI, also demonstrated an increase in survival with limited toxicity in mice with glioblastoma multiforme, a type of brain cancer with a very poor prognosis [208]. Its main limitation is its inability to cross the blood-brain barrier, that could be overcome with the use of nanoparticles. These findings suggest that PARPis labeled with alpha or Auger emitters have potential as a targeted therapy for various cancers. Pharmacokinetic profiles seem to be the major limitation of these compounds, since [125I]PARPi-01, a radiolabeled olaparib derivative investigated in a triple-negative breast cancer model, showed rapid clearance, counterbalancing its effective radiotoxicity [209]. Improvements in that domain are therefore necessary before translation to the clinic.
5.6. Carbonic Anhydrase IX (CA IX) inhibitors
Characterisation of solid tumors is mostly done with hypoxia, eventually inducing genetic instability, subsequently leading to an aggressive tumor phenotype and treatment resistance [210]. Hypoxic cells use various mechanisms to adapt and survive in their environment. One of these mechanisms involves the expression of the carbonic anhydrase protein, which is part of a group of zinc metalloenzymes playing a vital role in several physiological processes [211]. In particular, two isoforms of this protein, CA IX and CA XII, are associated with tumors. While the first is found in most solid tumors and gastrointestinal mucosa, the latter is present in not only tumors but also several other organs. Therefore, CA IX is a more suitable biomarker from a clinical perspective [212]. Additionally, the expression of CA IX is correlated with treatment resistance and with metastases, and is globally a marker of cancer’s poor prognosis.
CA IX is a protein with a molecular weight of 50 kDa and it consists of several domains including proteoglycan-like, catalytic, transmembrane, and intracellular domains. The catalytic domain of CA IX is located on the outer membrane of the cell and contains a zinc atom in its active center. Most CA inhibitors aim at targeting this extracellular catalytic domain. These entities contain a segment that can bind to zinc, either by attaching directly to the Zn2+ cation or indirectly by forming adducts with zinc-bound water or hydroxyl outside of the active site. The first group of entities consists of sulfonamide scaffold derivatives potent inhibitors. The second group is composed of synthetic molecules, peptidomimetics, and antibodies [213]. Several radiolabeled inhibitors have been described, mostly for imaging [214]. Apart from radiolabeled antibodies, there has only been one small molecule reported so far for radionuclide therapy. This molecule is a radiocomplex called [90Y]Y-US2, which is labeled with yttrium-90 and contains a ureidosulfonamide group. Its efficacy has been tested in mice with CA IX tumors expressing high levels of the protein. [215]. In this study, mice that were administered [90Y]Y-US2 experienced a significant delay in tumor growth compared to non-treated mice. Furthermore, there was limited hematological toxicity observed. Although not as extensively studied as antibodies, small synthetic molecules have potential as radiotherapeutic drugs due to their superior pharmacokinetic properties and potentially lower toxicity. Further research is needed to explore their potential [216].
5.7. Vitamins
Vitamins are essential nutrients for the organism. In particular, they are critical for rapidly dividing cells such as, for instance, malignant cancer cells. B vitamins, including riboflavin (B2), biotin (B7), folic acid (B9), and cobalamins (B12), play a crucial role in tumor growth, with many solid tumor cells overexpressing receptors that facilitate their uptake (Figure 9). As a result, targeting these receptors has become an appealing approach. Numerous studies have shown that vitamin-based bioconjugates, particularly folate, have significant potential for imaging and therapy [217].
Biotin, a water-soluble vitamin also referred as vitamin B7 or H, weighs 244 Daltons and plays a significant role in various metabolic processes, including gluconeogenesis and cell growth stimulation. The vitamin is internalized by binding to the sodium-dependent multivitamin transporter (SMVT) located on the surface of the cells. This transporter is present in high amounts in certain cancer types such as colon, breast, lung, renal, and ovarian cancers. In such cancers, targeting with biotinylated agents might be an interesting strategy [218]. However, to date, apart from some imaging applications, radiolabeled biotin derivatives have only been applied as a tool for pretargeting, using the streptavidin/biotin approach [219].
Folic acid, also known as vitamin B9 or folacin, is a crucial nutrient that the body needs to make DNA and RNA and to metabolize amino acids required for cell division. Folate receptors (FRs) can internalize it, making it possible to selectively deliver a drug and facilitate its complete and rapid internalization by receptor endocytosis. Among all vitamins, folic acid is the most extensively investigated for tumor targeting [220]. FRs are 38-44 kDa glycoproteins that anchor in the cell membrane using a glycosylphosphatidylinositol domain, with limited expression in healthy tissues, except for the kidneys. In contrast, several solid epithelial tumors, including breast, cervical, colorectal, endometrial renal, nasopharyngeal, and ovarian carcinomas, as well as tumor-associated macrophages overexpress FRs. Targeting FRs has thus gained significant interest for developing imaging and therapeutic agents for these cancers [221,222]. Folate derivatives bind to FRs with high affinity and clear rapidly from FR-negative tissues. Hydrophilic folate conjugates present a better biodistribution profile than lipophilic ones, but kidney uptake is dose-limiting. This can be mitigated by using diuretics or pretreating with antifolate drugs [223,224]. Albumin-binding moieties can prolong blood circulation, heightening the tumor-to-kidney ratio and potentially making folate-based radiopharmaceuticals safe for clinical use [225]. Currently, one single radiolabeled FR-targeting agent has been investigated in clinic, for PET imaging. A 177Lu-radiolabeled one has been investigated in preclinical models and has been shown to significantly inhibit tumor growth without radiotoxicity. Substituting 177Lu with 161Tb increased the therapeutic efficacy [226,227].
Vitamin B12, also known as cobalamin, is crucial for the function of methionine synthase, an enzyme that controls one of the primary pathways for the production of folates. Its uptake into cells is made possible by the plasma carrier protein transcobalamin II (TCII), which is often highly expressed in many types of tumors. In cancer cells, TCII facilitates cell uptake by binding to upregulated specific receptors (i.e. CD320). Investigations have been done on various radiolabeled cobalamin derivatives, mostly with γ-emitters, both in preclinical models and in patients with different tumor types that express TCII [217]. One example of a positron-emitting cobalamin derivative (with 89Zr) has also been reported [228]. So far, the only known use of cobalamin in a therapeutic setting involves its application as a receptor-specific radiosensitizer in combination with external-beam radiotherapy. In a pancreatic adenocarcinoma preclinical model, cobalamin was used as a vector for a fluorophore (Bodipy650) [229].
5.8. Phospholipid ether analogues
Several years ago, phospholipid ether (PLE) analogues of the naturally-occurring alkyl lysophospholipid and alkylphosphocholines have been demonstrated to be taken up preferentially by cancer cells and, moreover, to display antitumor and antimetastatic activities [230]. Combination with radiotherapy has shown interesting results [231]. However, the metabolic difference between neoplastic and normal cells could be exploited as a mean to selectively target tumors and deliver a radioactive payload into the cancer cell. Indeed, PLE analogues accumulate in cancer cells, exploiting the altered lipid composition of tumor cell membranes. PLEs are taken up into cells via lipid rafts, cholesterol-rich regions of the plasma membrane, which have highly increased amounts in malignant cells as opposed to normal cells [232]. When the lipid rafts undergo transmembrane flipping, PLEs are internalized, delivering the radioactive payload intracellularly and, in the case of a therapeutic radionuclide, causing double-strand DNA breaks, eventually leading to apoptosis. Major advantage of this system is based on the fact it is broadly applicable to a wide variety of cancer types, indiscriminately targeting all cells within a tumor, independently of the expression of a specific antigen [233].
Radioiodinated PLE analogues were therefore developed, both for imaging and for therapy of a variety of hematologic and solid tumor types [234,235,236,237]. Structure-activity studies demonstrated localization and clearance properties of these radiotracers depend on the length of the alkyl chain [238]. This eventually led to the development of 131I-radiolabeled iopofosine (18-(p-[131I] iodophenyl)octadecylphosphocholine), currently evaluated in several in the Phase I and Phase II trials [239,240,241,242,243,244,245]. A radiometallated analog (NM600) has been reported, labeled with 86/90Y and 177Lu, that preclinically demonstrated its ability to immunomodulate the TME in several tumor models, facilitating combined immunotherapy treatment [246,247].
5.9. Melanin targeting agents
Melanoma is a malignant disease originating from melanocytes. It is the deadliest and the most common skin cancer. A late diagnosis can drastically reduce survival rate, because of the ability of melanoma metastases to quickly disseminate. The search for a radiopharmaceutical with high affinity for melanoma, for early detection, and subsequent therapy, has therefore been an active field of investigations [248]. RIT, targeting surface antigens, and PRRT, targeting melanocortin receptors, hardly reached the clinic. In that context, targeting melanin appeared as particularly attractive [249]. The melanin pigment is an antigen present in >92% of melanomas [250]. Its primary function is to protect the skin against UV-induced damage, but, because of increased tyrosinase activity, it is overexpressed in melanoma cells [8,9]. It is expressed intracellularly, but, thanks to the high cellular turnover of tumor cells, some melanin can be found at the extracellular level, and thus be easily accessible for targeting. Some therapeutic melanin-binding antibodies have been successfully developed, notably labeled with rhenium-188 [251]. However, most promising results have been obtained with small molecules, which are able to bind to intracellular melanin with high specificity.
Organic compounds having aromatic rings and a tertiary amino group have been demonstrated to exhibit high affinity for melanin. These include dyes, such as methylene blue or acridine orange, and benzamide or heteroarylcarboxamide derivatives or related compounds [252]. It is hypothesized these compounds strongly bind to melanin fragments, both through π-interaction between aromatic rings of the radiotracer and indole moieties of melanin and ionic interaction between the protonated cation of the tertiary amine and melanin’s carboxylates (Figure 10). Several benzamide derivatives have been synthesized and evaluated, to find the compound with the best characteristics for melanoma uptake [253,254,255]. Even though some derivatives have been labeled with metals, radioiodinated compounds appeared as the most attractive ones [255,256].
Several of these compounds, radiolabeled with iodine-123, have been investigated in small clinical trials. [123I]BZA (N-(2-diethylaminoethyl)-4-iodobenzamide) has even been evaluated in a Phase 2, including 110 patients. It demonstrated an 81% sensitivity and a 100% specificity [257]. On the contrary, most of the therapeutic derivatives, labeled with iodine-131 or astatine-211, are still in a preclinical stage, with promising outcomes [258,259,260,261]. Some of these radiotracers have nonetheless been evaluated in patients. In a pilot study including 26 patients with histologically proven metastasized malignant melanoma, [131I]I-BA52 (N-(4-((2-diethylaminoethylcarbamoyl)-2-iodo-5-methoxyphenyl)benzo[1,3]dioxole-5-carboxamide) was effective in three of the five patients who were treated with a single dose over 4.3 GBq [262]. More recently, [131I]ICF01012 (N-(2-diethylaminoethyl)-6-iodoquinoxaline-2-carb oxamide) is currently being evaluated in a dose-escalation phase 1 trial [263]. Though [211At]-methylene blue was alleged to have been granted approval for a phase 1 clinical trial, no subsequent clinical trial seems to have been initiated [258].
6. Conclusions
Targeted radionuclide therapy has evolved towards precision medicine, especially when used with a companion diagnostic agent, to enhance patient selection. The understanding of the inter- and intra-individual heterogeneity of tumors and advances in radiobiology have led to the improvement of that theranostic strategy. The ALSYMPCA, NETTER-1, and VISION phase III trials have demonstrated the effectiveness of targeted radionuclide therapy in treating respectively bone metastases of mCRPC patients, neuroendocrine tumors, and prostate cancer respectively, inspiring further research. The latest research has shown a shift towards antagonists and α-emitters, as well as a pan-cancer approach that targets more widely expressed components of the tumor microenvironment, such as CXCR4 and FAPI radioconjugates. However, the challenge is now to select the most suitable agent for each patient. Carefully designed clinical trials are now compulsory to explore the dosimetry, new indications, and combination therapies of promising agents. The focus is also shifting from treating bulky tumors to treating minimal residual malignancies, where targeted radionuclide therapy is most appropriate. As pharmaceutical companies show increasing interest, targeted radionuclide therapy is set to become an essential component of nuclear medicine and, to a greater extent, oncology.
Author Contributions
Authors contributed equally to this review. All authors have read and agreed to the published version of the manuscript.
Funding
This work was partly supported by Labex IRON (grant no. ANR-11-LABX-0018) and Cancéropôle Grand Ouest.
Data Availability Statement
Not applicable.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Hertz, B.; Watabe, T.; Baum, R.P. Celebrating 80 years anniversary of radioiodine for use in thyroid cancer and perspectives for theranostics. Ann. Nucl. Med. 2022, 36, 1007–1009. [Google Scholar] [CrossRef] [PubMed]
- Volkert, W.A.; Hoffman, T.J. Therapeutic Radiopharmaceuticals. Chem. Rev. 1999, 99, 2269–2292. [Google Scholar] [CrossRef] [PubMed]
- Gabriel, M. Radionuclide therapy beyond radioiodine. Wien. Med. Wochenschr. 2012, 162, 430–439. [Google Scholar] [CrossRef] [PubMed]
- Sgouros, G.; Bodei, L.; McDevitt, M.R.; Nedrow, J.R. Radiopharmaceutical therapy in cancer: clinical advances and challenges. Nat. Rev. Drug Discov. 2020, 19, 589–608. [Google Scholar] [CrossRef] [PubMed]
- James, S.S.; Bednarz, B.; Benedict, S.; Buchsbaum, J.C.; Dewaraja, Y.; Frey, E.; Hobbs, R.; Grudzinski, J.; Roncali, E.; Sgouros, G.; et al. Current Status of Radiopharmaceutical Therapy. Int. J. Radiat. Oncol. 2021, 109, 891–901. [Google Scholar] [CrossRef] [PubMed]
- Pouget, J.-P.; Santoro, L.; Raymond, L.; Chouin, N.; Bardiès, M.; Bascoul-Mollevi, C.; Huguet, H.; Azria, D.; Kotzki, P.-O.; Pèlegrin, M.; et al. Cell Membrane is a More Sensitive Target than Cytoplasm to Dense Ionization Produced by Auger Electrons. Radiat. Res. 2008, 170, 192–200. [Google Scholar] [CrossRef] [PubMed]
- Fernandes, C.; Palma, E.; Silva, F.; Belchior, A.; Pinto, C.I.G.; Guerreiro, J.F.; Botelho, H.M.; Mendes, F.; Raposinho, P.; Paulo, A. Searching for a Paradigm Shift in Auger-Electron Cancer Therapy with Tumor-Specific Radiopeptides Targeting the Mitochondria and/or the Cell Nucleus. Int. J. Mol. Sci. 2022, 23, 7238. [Google Scholar] [CrossRef] [PubMed]
- Pirovano, G.; Wilson, T.C.; Reiner, T. Auger: The future of precision medicine. Nucl. Med. Biol. 2021, 96-97, 50–53. [Google Scholar] [CrossRef]
- Parker, C.; Nilsson, S.; Heinrich, D.; Helle, S.I.; O'Sullivan, J.M.; Fosså, S.D.; Chodacki, A.; Wiechno, P.; Logue, J.; Seke, M.; et al. Alpha Emitter Radium-223 and Survival in Metastatic Prostate Cancer. N. Engl. J. Med. 2013, 369, 213–223. [Google Scholar] [CrossRef]
- Garin, E.; Tselikas, L.; Guiu, B.; Chalaye, J.; Edeline, J.; Assenat, E.; Tacher, V.; Terroir-Cassou-Mounat, M.; Mariano-Goulart, D.; Amaddeo, G.; et al. Personalised versus standard dosimetry approach of selective internal radiation therapy in patients with locally advanced hepatocellular carcinoma (DOSISPHERE-01): a randomised, multicentre, open-label phase 2 trial. Lancet Gastroenterol. Hepatol. 2021, 6, 17–29. [Google Scholar] [CrossRef]
- Cheever, M.A.; Allison, J.P.; Ferris, A.S.; Finn, O.J.; Hastings, B.M.; Hecht, T.T.; Mellman, I.; Prindiville, S.A.; Viner, J.L.; Weiner, L.M.; et al. The Prioritization of Cancer Antigens: A National Cancer Institute Pilot Project for the Acceleration of Translational Research. Clin. Cancer Res. 2009, 15, 5323–5337. [Google Scholar] [CrossRef] [PubMed]
- Boonstra, M.C.; De Geus, S.W.; Prevoo, H.A.; Hawinkels, L.J.; Van De Velde, C.J.; Kuppen, P.J.; Vahrmeijer, A.L.; Sier, C.F. Selecting Targets for Tumor Imaging: An Overview of Cancer-Associated Membrane Proteins. Biomarkers Cancer 2016, 8, 119–133. [Google Scholar] [CrossRef] [PubMed]
- Aloj, L.; Attili, B.; Lau, D.; Caraco, C.; Lechermann, L.M.; Mendichovszky, I.A.; Harper, I.; Cheow, H.; Casey, R.T.; Sala, E.; et al. The emerging role of cell surface receptor and protein binding radiopharmaceuticals in cancer diagnostics and therapy. Nucl Med Biol. 2021, 92, 53–64. [Google Scholar] [CrossRef] [PubMed]
- Chakraborty, D.; Das, A.; Bal, C.S. Tumor-targeting agents. In: S. Harsini et al. (eds), Nuclear Medicine and Immunology. Springer Nature. 2022; 217-236.
- Liolios, C.; Sachpekidis, C.; Schäfer, M.; Kopka, K. Bispecific radioligands targeting prostate-specific membrane antigen and gastrin-releasing peptide receptors on the surface of prostate cancer cells. J. Label. Compd. Radiopharm. 2019, 62, 510–522. [Google Scholar] [CrossRef] [PubMed]
- Hanahan, D.; Weinberg, R.A. Hallmarks of cancer: The next generation. Cell 2011, 144, 646–674. [Google Scholar] [CrossRef]
- Qian, J.; Olbrecht, S.; Boeckx, B.; Vos, H.; Laoui, D.; Etlioglu, E.; Wauters, E.; Pomella, V.; Verbandt, S.; Busschaert, P.; et al. A pan-cancer blueprint of the heterogeneous tumor microenvironment revealed by single-cell profiling. Cell Res. 2020, 30, 745–762. [Google Scholar] [CrossRef]
- Poltavets, V.; Kochetkova, M.; Pitson, S.M.; Samuel, M.S. The Role of the Extracellular Matrix and Its Molecular and Cellular Regulators in Cancer Cell Plasticity. Front. Oncol. 2018, 8, 431. [Google Scholar] [CrossRef]
- Khalaf, K.; Hana, D.; Chou, J.T.-T.; Singh, C.; Mackiewicz, A.; Kaczmarek, M. Aspects of the Tumor Microenvironment Involved in Immune Resistance and Drug Resistance. Front. Immunol. 2021, 12. [Google Scholar] [CrossRef]
- Ni, Y.; Zhou, X.; Yang, J.; Shi, H.; Li, H.; Zhao, X.; Ma, X. The Role of Tumor-Stroma Interactions in Drug Resistance Within Tumor Microenvironment. Front. Cell Dev. Biol. 2021, 9. [Google Scholar] [CrossRef]
- van der Heide, C.D.; Dalm, S.U. Radionuclide imaging and therapy directed towards the tumor microenvironment: a multi-cancer approach for personalized medicine. Eur J Nucl Med Mol Imaging. 2022, 49, 4616–4641. [Google Scholar] [CrossRef]
- Kharaishvili, G.; Simkova, D.; Bouchalova, K.; Gachechiladze, M.; Narsia, N.; Bouchal, J. The role of cancer-associated fibroblasts, solid stress and other microenvironmental factors in tumor progression and therapy resistance. Cancer Cell Int. 2014, 14. [Google Scholar] [CrossRef] [PubMed]
- Corroyer-Dulmont, A.; Jaudet, C.; Frelin, A.-M.; Fantin, J.; Weyts, K.; Vallis, K.A.; Falzone, N.; Sibson, N.R.; Chérel, M.; Kraeber-Bodéré, F.; et al. Radioimmunotherapy for Brain Metastases: The Potential for Inflammation as a Target of Choice. Front. Oncol. 2021, 11. [Google Scholar] [CrossRef] [PubMed]
- Mukherjee, S.; Sonanini, D.; Maurer, A.; Daldrup-Link, H.E. The yin and yang of imaging tumor associated macrophages with PET and MRI. Theranostics 2019, 9, 7730–7748. [Google Scholar] [CrossRef] [PubMed]
- Kircher, M.; Herhaus, P.; Schottelius, M.; Buck, A.K.; Werner, R.A.; Wester, H.-J.; Keller, U.; Lapa, C. CXCR4-directed theranostics in oncology and inflammation. Ann. Nucl. Med. 2018, 32, 503–511. [Google Scholar] [CrossRef] [PubMed]
- Masłowska, K.; Halik, P.K.; Tymecka, D.; Misicka, A.; Gniazdowska, E. The Role of VEGF Receptors as Molecular Target in Nuclear Medicine for Cancer Diagnosis and Combination Therapy. Cancers 2021, 13, 1072. [Google Scholar] [CrossRef] [PubMed]
- Henke, E.; Nandigama, R.; Ergün, S. Extracellular Matrix in the Tumor Microenvironment and Its Impact on Cancer Therapy. Front. Mol. Biosci. 2020, 6, 160. [Google Scholar] [CrossRef] [PubMed]
- Wilson, W.R.; Hay, M.P. Targeting hypoxia in cancer therapy. Nat. Rev. Cancer 2011, 11, 393–410. [Google Scholar] [CrossRef] [PubMed]
- Lee, S.T.; Burvenich, I.; Scott, A. Novel Target Selection for Nuclear Medicine Studies. Semin. Nucl. Med. 2019, 49, 357–368. [Google Scholar] [CrossRef]
- Turck, R. Radio-pharmaceuticals for cancer treatment: are they ready for prime time yet? Ann Oncol. 2018, 29, 1594–1597. [Google Scholar] [CrossRef]
- Herrmann, K.; Schwaiger, M.; Lewis, J.S.; Solomon, S.B.; McNeil, B.J.; Baumann, M.; Gambhir, S.S.; Hricak, H.; Weissleder, R. Radiotheranostics: a roadmap for future development. Lancet Oncol. 2020, 21, e146–e156. [Google Scholar] [CrossRef]
- Srivastava, S.C.; Buraggi, G.L. NATO Advanced Study Institute on "radiolabeled monoclonal antibodies for imaging and therapy--potential, problems, and prospects". Int J Biol Markers. 1987, 2, 43–48. [Google Scholar] [CrossRef] [PubMed]
- Köhler, G.; Milstein, C. Continuous cultures of fused cells secreting antibody of predefined specificity. Nature 1975, 256, 495–497. [Google Scholar] [CrossRef] [PubMed]
- DeNardo, S.J.; DeNardo, G.L.; O'Grady, L.F.; Macey, D.J.; Mills, S.L.; Epstein, A.L.; Peng, J.-S.; McGahan, J.P. Treatment of a Patient with b Cell Lymphoma by 1-131 Lym-1 Monoclonal Antibodies. Int. J. Biol. Markers 1987, 2, 49–53. [Google Scholar] [CrossRef] [PubMed]
- Morschhauser, F.; Radford, J.; Van Hoof, A.; Botto, B.; Rohatiner, A.Z.; Salles, G.; Soubeyran, P.; Tilly, H.; Bischof-Delaloye, A.; van Putten, W.L.; et al. 90Yttrium-ibritumomab tiuxetan consolidation of first remission in advanced-stage follicular non-Hodgkin lymphoma: updated results after a median follow-up of 7.3 years from the International, Randomized, Phase III First-Line Indolent trial. J Clin Oncol. 2013, 31, 1977–1983. [Google Scholar] [CrossRef] [PubMed]
- Morschhauser, F.; Kraeber-Bodéré, F.; Wegener, W.A.; Harousseau, J.-L.; Petillon, M.-O.; Huglo, D.; Trümper, L.H.; Meller, J.; Pfreundschuh, M.; Kirsch, C.-M.; et al. High Rates of Durable Responses With Anti-CD22 Fractionated Radioimmunotherapy: Results of a Multicenter, Phase I/II Study in Non-Hodgkin's Lymphoma. J. Clin. Oncol. 2010, 28, 3709–3716. [Google Scholar] [CrossRef] [PubMed]
- Blakkisrud, J.; Løndalen, A.; Martinsen, A.C.T.; Dahle, J.; Holtedahl, J.E.; Bach-Gansmo, T.; Holte, H.; Kolstad, A.; Stokke, C. Tumor-Absorbed Dose for Non-Hodgkin Lymphoma Patients Treated with the Anti-CD37 Antibody Radionuclide Conjugate 177Lu-Lilotomab Satetraxetan. J. Nucl. Med. 2017, 58, 48–54. [Google Scholar] [CrossRef] [PubMed]
- Stokke, C.; Blakkisrud, J.; Løndalen, A.; Dahle, J.; Martinsen, A.C.T.; Holte, H.; Kolstad, A. Pre-dosing with lilotomab prior to therapy with 177Lu-lilotomab satetraxetan significantly increases the ratio of tumor to red marrow absorbed dose in non-Hodgkin lymphoma patients. Eur. J. Nucl. Med. 2018, 45, 1233–1241. [Google Scholar] [CrossRef]
- Gritti, G.; Gianatti, A.; Petronzelli, F.; De Santis, R.; Pavoni, C.; Rossi, R.L.; Cattaneo, L.; Spagnoli, L.G.; Ferrari, S.; Rossi, A.; et al. Evaluation of tenascin-C by tenatumomab in T-cell non-Hodgkin lymphomas identifies a new target for radioimmunotherapy. Oncotarget 2018, 9, 9766–9775. [Google Scholar] [CrossRef]
- Bäck, T.; Haraldsson, B.; Hultborn, R.; Jensen, H.; Johansson, M.E.; Lindegren, S.; Jacobsson, L. Glomerular filtration rate after alpha-radioimmunotherapy with 211At-MX35-F(ab')2: a long-term study of renal function in nude mice. Cancer Biother Radiopharm. 2009, 24, 649–658. [Google Scholar]
- Adams, G.; Shaller, C.; Chappell, L.; Wu, C.; Horak, E.; Simmons, H.; Litwin, S.; Marks, J.; Weiner, L.; Brechbiel, M. Delivery of the α-emitting radioisotope bismuth-213 to solid tumors via single-chain Fv and diabody molecules. Nucl. Med. Biol. 2000, 27, 339–346. [Google Scholar] [CrossRef]
- Diebolder, P.; Mpoy, C.; Scott, J.; Huynh, T.T.; Fields, R.; Spitzer, D.; Bandara, N.; Rogers, B.E. Preclinical Evaluation of an Engineered Single-Chain Fragment Variable-Fragment Crystallizable Targeting Human CDJ. Nucl. Med. 2021, 62, 137–143. [Google Scholar] [CrossRef] [PubMed]
- Altunay, B.; Morgenroth, A.; Beheshti, M.; Vogg, A.; Wong, N.C.L.; Ting, H.H.; Biersack, H.-J.; Stickeler, E.; Mottaghy, F.M. HER2-directed antibodies, affibodies and nanobodies as drug-delivery vehicles in breast cancer with a specific focus on radioimmunotherapy and radioimmunoimaging. Eur. J. Nucl. Med. 2021, 48, 1371–1389. [Google Scholar] [CrossRef] [PubMed]
- Tolmachev, V.; Orlova, A.; Pehrson, R.; Galli, J.; Baastrup, B.; Andersson, K.; Sandström, M.; Rosik, D.; Carlsson, J.; Lundqvist, H.; et al. Radionuclide therapy of HER2-positive microxenografts using a 177Lu-labeled HER2-specific Affibody molecule. Cancer Res. 2007, 67, 2773–2782. [Google Scholar] [CrossRef] [PubMed]
- Barbet, J.; Kraeber-Bodéré, F.; Vuillez, J.-P.; Gautherot, E.; Rouvier. ; Chatal, J.-F.; Bodet-Milin, C.; Ferrer, L.; Rauscher, A.; Masson, D.; et al. Pretargeting with the Affinity Enhancement System for Radioimmunotherapy. Cancer Biotherapy Radiopharm. 1999, 14, 153–166. [Google Scholar] [CrossRef] [PubMed]
- Kraeber-Bodéré, F.; Rousseau, C.; Bodet-Milin, C.; Ferrer, L.; Faivre-Chauvet, A.; Campion, L.; Vuillez, J.-P.; Devillers, A.; Chang, C.-H.; Goldenberg, D.M.; et al. Targeting, toxicity, and efficacy of 2-step, pretargeted radioimmunotherapy using a chimeric bispecific antibody and 131I-labeled bivalent hapten in a phase I optimization clinical trial. J. Nucl. Med. 2006, 47, 247–55. [Google Scholar] [PubMed]
- Salaun, P.Y.; Campion, L.; Bournaud, C.; Faivre-Chauvet, A.; Vuillez, J.P.; Taieb, D.; Ansquer, C.; Rousseau, C.; Borson-Chazot, F.; Bardet, S.; et al. Phase II trial of anticarcinoembryonic antigen pretargeted radioimmunotherapy in progressive metastatic medullary thyroid carcinoma: biomarker response and survival improvement. J Nucl Med. 2012, 53, 1185–1192. [Google Scholar] [CrossRef]
- Batra, J.S.; Karir, B.; Pinto-Chengot, K.; Jhanwar, Y.S.; Vallabhajosula, S.; Christos, P.J.; Hodes, G.; Lam, L.; Molina, A.; Beltran, H.; et al. MP50-19 DOSE-FRACTIONATED ANTI-PSMA RADIOIMMUNOTHERAPY ( 177 LU-J591) FOR MCRPC. J. Urol. 2016, 195. [Google Scholar] [CrossRef]
- Kraeber-Bodere, F.; Pallardy, A.; Maisonneuve, H.; Campion, L.; Moreau, A.; Soubeyran, I.; Le Gouill, S.; Tournilhac, O.; Daguindau, E.; Jardel, H.; et al. Consolidation anti-CD22 fractionated radioimmunotherapy with 90 Y-epratuzumab tetraxetan following R-CHOP in elderly patients with diffuse large B-cell lymphoma: a prospective, single group, phase 2 trial. Lancet Haematol. 2017, 4, e35–e45. [Google Scholar] [CrossRef]
- Filippi, L.; Bagni, O.; Nervi, C. Aptamer-based technology for radionuclide targeted imaging and therapy: a promising weapon against cancer. Expert Rev. Med Devices 2020, 17, 751–758. [Google Scholar] [CrossRef]
- Gijs, M.; Aerts, A.; Impens, N.; Baatout, S.; Luxen, A. Aptamers as radiopharmaceuticals for nuclear imaging and therapy. Nucl. Med. Biol. 2016, 43, 253–271. [Google Scholar] [CrossRef]
- Varmira, K.; Hosseinimehr, S.J.; Noaparast, Z.; Abedi, S.M. An improved radiolabelled RNA aptamer molecule for HER2 imaging in cancers. J. Drug Target. 2014, 22, 116–122. [Google Scholar] [CrossRef] [PubMed]
- Summerton, J.; Weller, D.D.; Tunç, C.U.; Öztaş, D.Y.; Uzunoğlu, D.; Bayrak. F.; Çulha, M.; Cleaves, H.J.; Meringer, M.; Goodwin, J.; et al. Morpholino Antisense Oligomers: Design, Preparation, and Properties. Antisense Nucleic Acid Drug Dev. 1997, 7, 187–195. [Google Scholar] [CrossRef] [PubMed]
- Zhong, Y.; Wu, P.; He, J.; Zhong, L.; Zhao, Y. Advances of Aptamer-based Clinical Applications for the Diagnosis and Therapy of Cancer. Discov Med. 2020, 29, 169–180. [Google Scholar] [PubMed]
- de Visser, M.; Verwijnen, S.M.; de Jong, M. Update:Improvement Strategies for Peptide Receptor Scintigraphy and Radionuclide Therapy. Cancer Biotherapy Radiopharm. 2008, 23, 137–157. [Google Scholar] [CrossRef] [PubMed]
- Tornesello, A.L.; Buonaguro, L.; Tornesello, M.L.; Buonaguro, F.M. New Insights in the Design of Bioactive Peptides and Chelating Agents for Imaging and Therapy in Oncology. Molecules 2017, 22, 1282. [Google Scholar] [CrossRef]
- Gharibkandi, N.A.; Conlon, J.M.; Hosseinimehr, S.J. Strategies for improving stability and pharmacokinetic characteristics of radiolabeled peptides for imaging and therapy. Peptides 2020, 133, 170385. [Google Scholar] [CrossRef]
- Qu, T.; Wang, Y.; Zhu, Z.; Rusckowski, M.; Hnatowich, D.J. Different chelators and different peptides together influence the in vitro and mouse in vivo properties of 99Tcm. Nucl. Med. Commun. 2001, 22, 203–215. [Google Scholar] [CrossRef]
- Fani, M.; Del Pozzo, L.; Abiraj, K.; Mansi, R.; Tamma, M.L.; Cescato, R.; Waser, B.; Weber, W.A.; Reubi, J.C.; Maecke, H.R. PET of somatostatin receptor-positive tumors using 64Cu- and 68Ga-somatostatin antagonists: the chelate makes the difference. J Nucl Med. 2011, 52, 1110–1118. [Google Scholar] [CrossRef]
- E Weiner, R.; Thakur, M.L. Radiolabeled peptides in the diagnosis and therapy of oncological diseases. Appl. Radiat. Isot. 2002, 57, 749–763. [Google Scholar] [CrossRef]
- Morgat, C.; Mishra, A.K.; Varshney, R.; Allard, M.; Fernandez, P.; Hindié, E. Targeting Neuropeptide Receptors for Cancer Imaging and Therapy: Perspectives with Bombesin, Neurotensin, and Neuropeptide-Y Receptors. 2014, 55, 1650–1657. [CrossRef]
- Tornesello, A.L.; Tornesello, M.L.; Buonaguro, F.M. An Overview of Bioactive Peptides for in vivo Imaging and Therapy in Human Diseases. Mini-Reviews Med. Chem. 2017, 17, 758–770. [Google Scholar] [CrossRef]
- Reubi, J.; Waser, B.; Schaer, J.-C.; Laissue, J.A. Somatostatin receptor sst1–sst5 expression in normal and neoplastic human tissues using receptor autoradiography with subtype-selective ligands. Eur. J. Nucl. Med. 2001, 28, 836–846. [Google Scholar] [CrossRef] [PubMed]
- Eychenne, R.; Bouvry, C.; Bourgeois, M.; Loyer, P.; Benoist, E.; Lepareur, N. Overview of Radiolabeled Somatostatin Analogs for Cancer Imaging and Therapy. Molecules 2020, 25, 4012. [Google Scholar] [CrossRef] [PubMed]
- Hennrich, U.; Benešová, M. [68Ga]Ga-DOTA-TOC: The First FDA-Approved 68Ga-Radiopharmaceutical for PET Imaging. Pharmaceuticals (Basel) 2020, 13, 38. [Google Scholar] [CrossRef] [PubMed]
- Hennrich, U.; Kopka, K. Lutathera®: The First FDA- and EMA-Approved Radiopharmaceutical for Peptide Receptor Radionuclide Therapy. Pharmaceuticals 2019, 12, 114. [Google Scholar] [CrossRef] [PubMed]
- A Kaltsas, G.; Papadogias, D.; Makras, P.; Grossman, A.B. Treatment of advanced neuroendocrine tumours with radiolabelled somatostatin analogues. Endocrine-Related Cancer 2005, 12, 683–699. [Google Scholar] [CrossRef] [PubMed]
- Haider, M.; Das, S.; Al-Toubah, T.; Pelle, E.; El-Haddad, G.; Strosberg, J. Somatostatin receptor radionuclide therapy in neuroendocrine tumors. Endocrine-Related Cancer 2021, 28, R81–R93. [Google Scholar] [CrossRef] [PubMed]
- Uccelli, L.; Boschi, A.; Cittanti, C.; Martini, P.; Panareo, S.; Tonini, E.; Nieri, A.; Urso, L.; Caracciolo, M.; Lodi, L.; et al. 90Y/177Lu-DOTATOC: From Preclinical Studies to Application in Humans. Pharmaceutics 2021, 13, 1463. [Google Scholar] [CrossRef] [PubMed]
- Puliani, G.; Chiefari, A.; Mormando, M.; Bianchini, M.; Lauretta, R.; Appetecchia, M. New Insights in PRRT: Lessons From 2021. Front. Endocrinol. 2022, 13, 861434. [Google Scholar] [CrossRef]
- Strosberg, J.; El-Haddad, G.; Wolin, E.; Hendifar, A.; Yao, J.; Chasen, B.; Mittra, E.; Kunz, P.L.; Kulke, M.H.; Jacene, H.; et al. Phase 3 Trial of 177Lu-Dotatate for Midgut Neuroendocrine Tumors. N. Engl. J. Med. 2017, 376, 125–135. [Google Scholar] [CrossRef]
- Bidakhvidi, N.A.; Goffin, K.; Dekervel, J.; Baete, K.; Nackaerts, K.; Clement, P.; Van Cutsem, E.; Verslype, C.; Deroose, C.M. Peptide Receptor Radionuclide Therapy Targeting the Somatostatin Receptor: Basic Principles, Clinical Applications and Optimization Strategies. Cancers 2021, 14, 129. [Google Scholar] [CrossRef]
- Kratochwil, C.; Giesel, F.L.; Bruchertseifer, F.; Mier, W.; Apostolidis, C.; Boll, R.; Murphy, K.; Haberkorn, U.; Morgenstern, A. 213Bi-DOTATOC receptor-targeted alpha-radionuclide therapy induces remission in neuroendocrine tumours refractory to beta radiation: a first-in-human experience. Eur. J. Nucl. Med. 2014, 41, 2106–2119. [Google Scholar] [CrossRef] [PubMed]
- Ballal, S.; Yadav, M.P.; Bal, C.; Sahoo, R.K.; Tripathi, M. Broadening horizons with 225Ac-DOTATATE targeted alpha therapy for gastroenteropancreatic neuroendocrine tumour patients stable or refractory to 177Lu-DOTATATE PRRT: first clinical experience on the efficacy and safety. Eur. J. Nucl. Med. 2020, 47, 934–946. [Google Scholar] [CrossRef] [PubMed]
- Koh, T.; Bezak, E.; Chan, D.; Cehic, G. Targeted alpha-particle therapy in neuroendocrine neoplasms: A systematic review. World J. Nucl. Med. 2021, 20, 329–335. [Google Scholar] [CrossRef] [PubMed]
- Ginj, M.; Zhang, H.; Waser, B.; Cescato, R.; Wild, D.; Wang, X.; Erchegyi, J.; Rivier, J.; Mäcke, H.R.; Reubi, J.C. Radiolabeled somatostatin receptor antagonists are preferable to agonists for in vivo peptide receptor targeting of tumors. Proc Natl Acad Sci USA 2006, 103, 16436–16441. [Google Scholar] [CrossRef] [PubMed]
- Fani, M.; Peitl, P.K.; Velikyan, I. Current Status of Radiopharmaceuticals for the Theranostics of Neuroendocrine Neoplasms. Pharmaceuticals 2017, 10, 30. [Google Scholar] [CrossRef] [PubMed]
- Wild, D.; Fani, M.; Behe, M.; Brink, I.; Rivier, J.E.; Reubi, J.C.; Maecke, H.R.; Weber, W.A. First Clinical Evidence That Imaging with Somatostatin Receptor Antagonists Is Feasible. J. Nucl. Med. 2011, 52, 1412–1417. [Google Scholar] [CrossRef] [PubMed]
- Fani, M.; Nicolas, G.P.; Wild, D. Somatostatin Receptor Antagonists for Imaging and Therapy. J. Nucl. Med. 2017, 58, 61S–66S. [Google Scholar] [CrossRef]
- Wild, D.; Fani, M.; Fischer, R.; Del Pozzo, L.; Kaul, F.; Krebs, S.; Rivier, J.E.; Reubi, J.C.; Maecke, H.R.; Weber, W.A. Comparison of Somatostatin Receptor Agonist and Antagonist for Peptide Receptor Radionuclide Therapy: A Pilot Study. J. Nucl. Med. 2014, 55, 1248–1252. [Google Scholar] [CrossRef]
- Reidy-Lagunes, D.; Pandit-Taskar, N.; O'Donoghue, J.A.; Krebs, S.; Staton, K.D.; Lyashchenko, S.K.; Lewis, J.S.; Raj, N.; Gönen, M.; Lohrmann, C.; et al. Phase I Trial of Well-Differentiated Neuroendocrine Tumors (NETs) with Radiolabeled Somatostatin Antagonist 177Lu-Satoreotide Tetraxetan. Clin. Cancer Res. 2019, 25, 6939–6947. [Google Scholar] [CrossRef]
- Baum, R.P.; Zhang, J.; Schuchardt, C.; Mueller, D.; Maecke, H. First-in-Humans Study of the SSTR Antagonist 177Lu-DOTA-LM3 for Peptide Receptor Radionuclide Therapy in Patients with Metastatic Neuroendocrine Neoplasms: Dosimetry, Safety, and Efficacy. J. Nucl. Med. 2021, 62, 1571–1581. [Google Scholar] [CrossRef]
- Fani, M.; Mansi, R.; Nicolas, G.P.; Wild, D. Radiolabeled Somatostatin Analogs—A Continuously Evolving Class of Radiopharmaceuticals. Cancers 2022, 14, 1172. [Google Scholar] [CrossRef] [PubMed]
- Harris, P.E.; Zhernosekov, K. The evolution of PRRT for the treatment of neuroendocrine tumors; What comes next? Front Endocrinol 2022, 13, 941832. [Google Scholar] [CrossRef]
- Van de Wiele C, Dumont F, van Belle S, Slegers G, Peers SH, Dierckx RA. Is there a role for agonist gastrin-releasing peptide receptor radioligands in tumour imaging? Nucl Med Commun. 2001, 22, 5–15. [Google Scholar] [CrossRef] [PubMed]
- Smith, C.J.; Volkert, W.A.; Hoffman, T.J. Radiolabeled peptide conjugates for targeting of the bombesin receptor superfamily subtypes. Nucl. Med. Biol. 2005, 32, 733–740. [Google Scholar] [CrossRef] [PubMed]
- Mansi, R.; Nock, B.A.; Dalm, S.U.; Busstra, M.B.; van Weerden, W.M.; Maina, T. Radiolabeled Bombesin Analogs. Cancers 2021, 13, 5766. [Google Scholar] [CrossRef] [PubMed]
- Bodei L, Ferrari M, Nunn A, Llull J, Cremonesi M, Martano L, Laurora G, Scardino E, Tiberini S, Bufi G, Eaton S, de Cobelli O, Paganelli G. . 177Lu-AMBA bombesin analogue in hormone refractory prostate cancer patients: A phase I escalation study with single-cycle administrations. Eur. J. Nucl. Med. Mol. Imaging. 2007, 34, S221. [Google Scholar]
- Cescato, R.; Maina, T.; Nock, B.; Nikolopoulou, A.; Charalambidis, D.; Piccand, V.; Reubi, J.C. Bombesin Receptor Antagonists May Be Preferable to Agonists for Tumor Targeting. J. Nucl. Med. 2008, 49, 318–326. [Google Scholar] [CrossRef] [PubMed]
- Maina, T.; Nock, B.A.; Kulkarni, H.; Singh, A.; Baum, R.P. Theranostic Prospects of Gastrin-Releasing Peptide Receptor–Radioantagonists in Oncology. PET Clin. 2017, 12, 297–309. [Google Scholar] [CrossRef]
- Kurth, J.; Krause, B.J.; Schwarzenböck, S.M.; Bergner, C.; Hakenberg, O.W.; Heuschkel, M. First-in-human dosimetry of gastrin-releasing peptide receptor antagonist [177Lu]Lu-RM2: a radiopharmaceutical for the treatment of metastatic castration-resistant prostate cancer. Eur. J. Nucl. Med. 2020, 47, 123–135. [Google Scholar] [CrossRef]
- Guenther, T.; Deiser, S.; Felber, V.; Beck, R.; Wester, H.-J. Substitution of l-Tryptophan by α-Methyl-l-Tryptophan in 177Lu-RM2 Results in 177Lu-AMTG, a High-Affinity Gastrin-Releasing Peptide Receptor Ligand with Improved In Vivo Stability. J. Nucl. Med. 2022, 63, 1364–1370. [Google Scholar] [CrossRef]
- Montemagno, C.; Raes, F.; Ahmadi, M.; Bacot, S.; Debiossat, M.; Leenhardt, J.; Boutonnat, J.; Orlandi, F.; Barbato, D.; Tedesco, M.; et al. In Vivo Biodistribution and Efficacy Evaluation of NeoB, a Radiotracer Targeted to GRPR, in Mice Bearing Gastrointestinal Stromal Tumor. Cancers 2021, 13, 1051. [Google Scholar] [CrossRef] [PubMed]
- Ruigrok EAM, Verhoeven M, Konijnenberg MW, de Blois E, de Ridder CMA, Stuurman DC, Bertarione L, Rolfo K, de Jong M, Dalm SU. Safety of [177Lu]Lu-NeoB treatment: a preclinical study characterizing absorbed dose and acute, early, and late organ toxicity. Eur J Nucl Med Mol Imaging. 2022, 49, 4440–4451. [Google Scholar] [CrossRef] [PubMed]
- Huynh, T.T.; van Dam, E.M.; Sreekumar, S.; Mpoy, C.; Blyth, B.J.; Muntz, F.; Harris, M.J.; Rogers, B.E. Copper-67-Labeled Bombesin Peptide for Targeted Radionuclide Therapy of Prostate Cancer. Pharmaceuticals 2022, 15, 728. [Google Scholar] [CrossRef] [PubMed]
- Majkowska-Pilip, A.; Halik, P.K.; Gniazdowska, E. The Significance of NK1 Receptor Ligands and Their Application in Targeted Radionuclide Tumour Therapy. Pharmaceutics 2019, 11, 443. [Google Scholar] [CrossRef] [PubMed]
- Kneifel, S.; Cordier, D.; Good, S.; Ionescu, M.C.; Ghaffari, A.; Hofer, S.; Kretzschmar, M.; Tolnay, M.; Apostolidis, C.; Waser, B.; et al. Local Targeting of Malignant Gliomas by the Diffusible Peptidic Vector 1,4,7,10-Tetraazacyclododecane-1-Glutaric Acid-4,7,10-Triacetic Acid-Substance P. Clin. Cancer Res. 2006, 12, 3843–3850. [Google Scholar] [CrossRef] [PubMed]
- Cordier, D.; Krolicki, L.; Morgenstern, A.; Merlo, A. Targeted Radiolabeled Compounds in Glioma Therapy. Semin. Nucl. Med. 2016, 46, 243–249. [Google Scholar] [CrossRef] [PubMed]
- Krolicki, L.; Bruchertseifer, F.; Kunikowska, J.; Koziara, H.; Królicki, B.; Jakuciński, M.; Pawlak, D.; Apostolidis, C.; Mirzadeh, S.; Rola, R.; et al. Prolonged survival in secondary glioblastoma following local injection of targeted alpha therapy with 213Bi-substance P analogue. Eur. J. Nucl. Med. 2018, 45, 1636–1644. [Google Scholar] [CrossRef]
- Królicki, L.; Kunikowska, J.; Bruchertseifer, F.; Koziara, H.; Królicki, B.; Jakuciński, M.; Pawlak, D.; Rola, R.; Morgenstern, A.; Rosiak, E.; et al. 225Ac- and 213Bi-Substance P Analogues for Glioma Therapy. Semin. Nucl. Med. 2020, 50, 141–151. [Google Scholar] [CrossRef]
- Halik, P.K.; Lipiński, P.F.J.; Matalińska, J.; Koźmiński, P.; Misicka, A.; Gniazdowska, E. Radiochemical Synthesis and Evaluation of Novel Radioconjugates of Neurokinin 1 Receptor Antagonist Aprepitant Dedicated for NK1R-Positive Tumors. Molecules 2020, 25, 3756. [Google Scholar] [CrossRef]
- Matalińska J, Kosińska K, Halik PK, Koźmiński P, Lipiński PFJ, Gniazdowska E, Misicka A. Novel NK1R-Targeted 68Ga-/177Lu-Radioconjugates with Potential Application against Glioblastoma Multiforme: Preliminary Exploration of Structure-Activity Relationships. Int J Mol Sci. 2022, 23, 1214. [Google Scholar] [CrossRef]
- Davenport AP, Scully CCG, de Graaf C, Brown AJH, Maguire JJ. Advances in therapeutic peptides targeting G protein-coupled receptors. Nat Rev Drug Discov. 2020, 19, 389–413. [Google Scholar] [CrossRef] [PubMed]
- Ansquer, C.; Kraeber-Bodere, F.; Chatal, J.F. Current Status and Perspectives in Peptide Receptor Radiation Therapy. Curr. Pharm. Des. 2009, 15, 2453–2462. [Google Scholar] [CrossRef] [PubMed]
- Franco Machado J, Silva RD, Melo R, G Correia JD. Less Exploited GPCRs in Precision Medicine: Targets for Molecular Imaging and Theranostics. Molecules 2018, 24, 49. [Google Scholar] [CrossRef]
- Thakur, M.L.; Tripathi, S.K.; Gomella, L.G.; Salmanoglu, E.; Kim, S.; Kelly, W.K.; Keith, S.W.; Intenzo, C.; McCue, P.; Hoffman-Censits, J.; et al. Imaging urothelial bladder cancer: A VPAC PET targeted approach. Can J Urol. 2021, 28, 10596–10602. [Google Scholar] [PubMed]
- von Guggenberg, E.; Kolenc, P.; Rottenburger, C.; Mikołajczak, R.; Hubalewska-Dydejczyk, A. Update on Preclinical Development and Clinical Translation of Cholecystokinin-2 Receptor Targeting Radiopharmaceuticals. Cancers 2021, 13, 5776. [Google Scholar] [CrossRef]
- Rottenburger, C.; Nicolas, G.P.; McDougall, L.; Kaul, F.; Cachovan, M.; Vija, A.H.; Schibli, R.; Geistlich, S.; Schumann, A.; Rau, T.; et al. Cholecystokinin 2 Receptor Agonist 177Lu-PP-F11N for Radionuclide Therapy of Medullary Thyroid Carcinoma: Results of the Lumed Phase 0a Study. J. Nucl. Med. 2020, 61, 520–526. [Google Scholar] [CrossRef]
- Kawaguchi, N.; Zhang, T.-T.; Nakanishi, T. Involvement of CXCR4 in Normal and Abnormal Development. Cells 2019, 8, 185. [Google Scholar] [CrossRef]
- Chatterjee, S.; Azad, B.B.; Nimmagadda, S. The Intricate Role of CXCR4 in Cancer. Adv. Cancer Res. 2014, 124, 31–82. [Google Scholar] [CrossRef]
- Werner, R.A.; Kircher, S.; Higuchi, T.; Kircher, M.; Schirbel, A.; Wester, H.-J.; Buck, A.K.; Pomper, M.G.; Rowe, S.P.; Lapa, C. CXCR4-Directed Imaging in Solid Tumors. Front. Oncol. 2019, 9, 770. [Google Scholar] [CrossRef]
- Kircher, M.; Herhaus, P.; Schottelius, M.; Buck, A.K.; Werner, R.A.; Wester, H.-J.; Keller, U.; Lapa, C. CXCR4-directed theranostics in oncology and inflammation. Ann. Nucl. Med. 2018, 32, 503–511. [Google Scholar] [CrossRef]
- Schottelius, M.; Osl, T.; Poschenrieder, A.; Hoffmann, F.; Beykan, S.; Hänscheid, H.; Schirbel, A.; Buck, A.K.; Kropf, S.; Schwaiger, M.; et al. [177Lu]pentixather: Comprehensive Preclinical Characterization of a First CXCR4-directed Endoradiotherapeutic Agent. Theranostics 2017, 7, 2350–2362. [Google Scholar] [CrossRef] [PubMed]
- Osl T, Schmidt A, Schwaiger M, Schottelius M, Wester HJ. A new class of PentixaFor- and PentixaTher-based theranostic agents with enhanced CXCR4-targeting efficiency. Theranostics. 2020, 10, 8264–8280. [Google Scholar] [CrossRef] [PubMed]
- Herrmann, K.; Schottelius, M.; Lapa, C.; Osl, T.; Poschenrieder, A.; Hänscheid, H.; Lückerath, K.; Schreder, M.; Bluemel, C.; Knott, M.; et al. First-in-Human Experience of CXCR4-Directed Endoradiotherapy with 177Lu- and 90Y-Labeled Pentixather in Advanced-Stage Multiple Myeloma with Extensive Intra- and Extramedullary Disease. J. Nucl. Med. 2016, 57, 248–251. [Google Scholar] [CrossRef] [PubMed]
- Maurer, S.; Herhaus, P.; Lippenmeyer, R.; Hänscheid, H.; Kircher, M.; Schirbel, A.; Maurer, H.C.; Buck, A.K.; Wester, H.-J.; Einsele, H.; et al. Side Effects of CXC-Chemokine Receptor 4–Directed Endoradiotherapy with Pentixather Before Hematopoietic Stem Cell Transplantation. J. Nucl. Med. 2019, 60, 1399–1405. [Google Scholar] [CrossRef] [PubMed]
- Schottelius, M.; Herrmann, K.; Lapa, C. In Vivo Targeting of CXCR4—New Horizons. Cancers 2021, 13, 5920. [Google Scholar] [CrossRef] [PubMed]
- Buck, A.K.; Serfling, S.E.; Lindner, T.; Hänscheid, H.; Schirbel, A.; Hahner, S.; Fassnacht, M.; Einsele, H.; Werner, R.A. CXCR4-targeted theranostics in oncology. Eur. J. Nucl. Med. 2022, 49, 4133–4144. [Google Scholar] [CrossRef] [PubMed]
- Chen, Z.; Xue, Q.; Yao, S. Nuclear Medicine Application of Pentixafor/Pentixather Targeting CXCR4 for Imaging and Therapy in Related Disease. Mini-Reviews Med. Chem. 2023, 23, 787–803. [Google Scholar] [CrossRef]
- Desgrosellier, J.S.; Cheresh, D.A. Integrins in cancer: biological implications and therapeutic opportunities. Nat. Rev. Cancer 2010, 10, 9–22. [Google Scholar] [CrossRef]
- Haubner, R.; Decristoforo, C. Radiolabelled RGD peptides and peptidomimetics for tumour targeting. Front. Biosci. 2009, 14, 872–886. [Google Scholar] [CrossRef]
- Notni, J. RGD Forever! — Past, Present, and Future of a 3-Letter-Code in Radiopharmacy and Life Sciences. Pharmaceuticals 2023, 16, 56. [Google Scholar] [CrossRef]
- Kossatz, S.; Beer, A.J.; Notni, J. It’s Time to Shift the Paradigm: Translation and Clinical Application of Non-αvβ3 Integrin Targeting Radiopharmaceuticals. Cancers 2021, 13, 5958. [Google Scholar] [CrossRef] [PubMed]
- Masłowska, K.; Halik, P.K.; Tymecka, D.; Misicka, A.; Gniazdowska, E. The Role of VEGF Receptors as Molecular Target in Nuclear Medicine for Cancer Diagnosis and Combination Therapy. Cancers 2021, 13, 1072. [Google Scholar] [CrossRef] [PubMed]
- Masłowska K, Witkowska E, Tymecka D, Halik PK, Misicka A, Gniazdowska E. Synthesis, Physicochemical and Biological Study of Gallium-68- and Lutetium-177-Labeled VEGF-A165/NRP-1 Complex Inhibitors Based on Peptide A7R and Branched Peptidomimetic. Pharmaceutics. 2022, 14, 100. [Google Scholar] [CrossRef] [PubMed]
- Ayo, A.; Laakkonen, P. Peptide-Based Strategies for Targeted Tumor Treatment and Imaging. Pharmaceutics 2021, 13, 481. [Google Scholar] [CrossRef]
- Khalily MP, Soydan M. Peptide-based diagnostic and therapeutic agents: Where we are and where we are heading? Chem Biol Drug Des. 2022, 1–22. [Google Scholar]
- Cao, R.; Liu, H.; Cheng, Z. Radiolabeled Peptide Probes for Liver Cancer Imaging. Curr. Med. Chem. 2020, 27, 6968–6986. [Google Scholar] [CrossRef]
- Ciobanasu, C. Peptides-based therapy and diagnosis. Strategies for non-invasive therapies in cancer. J. Drug Target. 2021, 29, 1063–1079. [Google Scholar] [CrossRef]
- Baum, R.P.; Singh, A.; Schuchardt, C.; Kulkarni, H.R.; Klette, I.; Wiessalla, S.; Osterkamp, F.; Reineke, U.; Smerling, C. 177Lu-3BP-227 for Neurotensin Receptor 1–Targeted Therapy of Metastatic Pancreatic Adenocarcinoma: First Clinical Results. J. Nucl. Med. 2018, 59, 809–814. [Google Scholar] [CrossRef]
- Nock, B.A.; Kanellopoulos, P.; Chepurny, O.G.; Rouchota, M.; Loudos, G.; Holz, G.G.; Krenning, E.P.; Maina, T. Nonpeptidic Z360-Analogs Tagged with Trivalent Radiometals as Anti-CCK2R Cancer Theranostic Agents: A Preclinical Study. Pharmaceutics 2022, 14, 666. [Google Scholar] [CrossRef]
- Gdowski, A.S.; Ranjan, A.; Vishwanatha, J.K. Current concepts in bone metastasis, contemporary therapeutic strategies and ongoing clinical trials. J. Exp. Clin. Cancer Res. 2017, 36. [Google Scholar] [CrossRef]
- Liepe, K.; Kotzerke, J. Internal radiotherapy of painful bone metastases. Methods 2011, 55, 258–270. [Google Scholar] [CrossRef] [PubMed]
- Potsaid, M.S.; Irwin, R.J.; Castronovo, F.P.; Prout, G.R.; Harvey, W.J.; Francis, M.D.; Tofe, A.J.; Zamenhof, R.G. [32P] diphosphonate dose determination in patients with bone metastases from prostatic carcinoma. J Nucl Med. 1978, 19, 98–104. [Google Scholar] [PubMed]
- Roberts, D.J. 32P-Sodium Phosphate Treatment of Metastatic Malignant Disease. Clin. Nucl. Med. 1979, 4, 92–93. [Google Scholar] [CrossRef]
- Mathieu, L.; Chevalier, P.; Galy, G.; Berger, M. Preparation of rhenium-186 labelled EHDP and its possible use in the treatment of osseous neoplasms. Int. J. Appl. Radiat. Isot. 1979, 30, 725–727. [Google Scholar] [CrossRef] [PubMed]
- Hosain, F.; Spencer, R.P. Radiopharmaceuticals for palliation of metastatic osseous lesions: Biologic and physical background. Semin. Nucl. Med. 1992, 22, 11–16. [Google Scholar] [CrossRef] [PubMed]
- Bouchet, L.G.; E Bolch, W.; Goddu, S.M.; Howell, R.W.; Rao, D.V. Considerations in the selection of radiopharmaceuticals for palliation of bone pain from metastatic osseous lesions. J Nucl Med. 2000, 41, 682–7. [Google Scholar]
- Pauwels, E.K.; Stokkel, M.P. Radiopharmaceuticals for bone lesions. Imaging and therapy in clinical practice. Q J Nucl Med. 2001, 45, 18–26. [Google Scholar]
- Lange, R.; ter Heine, R.; Knapp, R. (.; de Klerk, J.M.; Bloemendal, H.J.; Hendrikse, N.H. Pharmaceutical and clinical development of phosphonate-based radiopharmaceuticals for the targeted treatment of bone metastases. Bone 2016, 91, 159–179. [Google Scholar] [CrossRef]
- Liepe K, Shinto A. From palliative therapy to prolongation of survival: 223RaCl2 in the treatment of bone metastases. Ther Adv Med Oncol. 2016, 8, 294–304. [Google Scholar] [CrossRef]
- Das, T.; Banerjee, S. Radiopharmaceuticals for metastatic bone pain palliation: available options in the clinical domain and their comparisons. Clin. Exp. Metastasis 2017, 34, 1–10. [Google Scholar] [CrossRef]
- Fernández, R.; Eppard, E.; Lehnert, W.; Jiménez-Franco, L.D.; Soza-Ried, C.; Ceballos, M.; Ribbeck, J.; Kluge, A.; Roesch, F.; Meckel, M.; et al. Evaluation of Safety and Dosimetry of 177Lu-DOTA-ZOL for Therapy of Bone Metastases. J. Nucl. Med. 2021, 62, 1126–1132. [Google Scholar] [CrossRef] [PubMed]
- Palmedo H, Manka-Waluch A, Albers P, Schmidt-Wolf IG, Reinhardt M, Ezziddin S, Joe A, Roedel R, Fimmers R, Knapp FF Jr, Guhlke S, Biersack HJ. Repeated bone-targeted therapy for hormone-refractory prostate carcinoma: tandomized phase II trial with the new, high-energy radiopharmaceutical rhenium-188 hydroxyethylidenediphosphonate. J Clin Oncol. 2003, 21, 2869–2875. [Google Scholar] [CrossRef] [PubMed]
- Biersack, H.-J.; Palmedo, H.; Andris, A.; Rogenhofer, S.; Knapp, F.F.; Guhlke, S.; Ezziddin, S.; Bucerius, J.; von Mallek, D. Palliation and Survival After Repeated 188Re-HEDP Therapy of Hormone-Refractory Bone Metastases of Prostate Cancer: A Retrospective Analysis. J. Nucl. Med. 2011, 52, 1721–1726. [Google Scholar] [CrossRef] [PubMed]
- Liberal, F.D.G.; Tavares, A.A.S.; Tavares, J.M.R. Palliative treatment of metastatic bone pain with radiopharmaceuticals: A perspective beyond Strontium-89 and Samarium-153. Appl. Radiat. Isot. 2016, 110, 87–99. [Google Scholar] [CrossRef] [PubMed]
- Liepe, K.; Murray, I.; Flux, G. Dosimetry of Bone Seeking Beta Emitters for Bone Pain Palliation Metastases. Semin. Nucl. Med. 2022, 52, 178–190. [Google Scholar] [CrossRef] [PubMed]
- Askari, E.; Harsini, S.; Vahidfar, N.; Divband, G.; Sadeghi, R. 177Lu-EDTMP for Metastatic Bone Pain Palliation: A Systematic Review and Meta-Analysis. Cancer Biotherapy Radiopharm. 2021, 36, 383–390. [Google Scholar] [CrossRef] [PubMed]
- Wieland, D.M.; Swanson, D.P.; E Brown, L.; Beierwaltes, W.H. Imaging the adrenal medulla with an I-131-labeled antiadrenergic agent. J Nucl Med. 1979, 20, 155–8. [Google Scholar]
- Vallabhajosula, S.; Nikolopoulou, A. Radioiodinated Metaiodobenzylguanidine (MIBG): Radiochemistry, Biology, and Pharmacology. Semin. Nucl. Med. 2011, 41, 324–333. [Google Scholar] [CrossRef]
- Jungels, C.; Karfis, I. 131I-metaiodobenzylguanidine and peptide receptor radionuclide therapy in pheochromocytoma and paraganglioma. Curr. Opin. Oncol. 2021, 33, 33–39. [Google Scholar] [CrossRef]
- Giammarile F, Chiti A, Lassmann M, Brans B, Flux G; EANM. EANM procedure guidelines for 131I-meta-iodobenzylguanidine (131I-mIBG) therapy. Eur J Nucl Med Mol Imaging. 2008, 35, 1039–1047. [Google Scholar] [CrossRef]
- Jimenez, C.; Erwin, W.; Chasen, B. Targeted Radionuclide Therapy for Patients with Metastatic Pheochromocytoma and Paraganglioma: From Low-Specific-Activity to High-Specific-Activity Iodine-131 Metaiodobenzylguanidine. Cancers 2019, 11, 1018. [Google Scholar] [CrossRef] [PubMed]
- Prado-Wohlwend, S.; del Olmo-García, M.I.; Bello-Arques, P.; Merino-Torres, J.F. Response to targeted radionuclide therapy with [131I]MIBG AND [177Lu]Lu-DOTA-TATE according to adrenal vs. extra-adrenal primary location in metastatic paragangliomas and pheochromocytomas: A systematic review. Front. Endocrinol. 2022, 13, 957172. [Google Scholar] [CrossRef] [PubMed]
- Sisson, J.C.; Shapiro, B.; Hutchinson, R.J.; Shulkin, B.L.; Zempel, S. Survival of Patients with Neuroblastoma Treated with 125-I MIBG. Am. J. Clin. Oncol. 1996, 19, 144–148. [Google Scholar] [CrossRef] [PubMed]
- Ohshima, Y.; Sudo, H.; Watanabe, S.; Nagatsu, K.; Tsuji, A.B.; Sakashita, T.; Ito, Y.M.; Yoshinaga, K.; Higashi, T.; Ishioka, N.S. Antitumor effects of radionuclide treatment using α-emitting meta-211At-astato-benzylguanidine in a PC12 pheochromocytoma model. Eur. J. Nucl. Med. 2018, 45, 999–1010. [Google Scholar] [CrossRef] [PubMed]
- Ukon, N.; Higashi, T.; Hosono, M.; Kinuya, S.; Yamada, T.; Yanagida, S.; Namba, M.; Nakamura, Y. Manual on the proper use of meta-[211At] astato-benzylguanidine ([211At] MABG) injections in clinical trials for targeted alpha therapy (1st edition). Ann. Nucl. Med. 2022, 36, 695–709. [Google Scholar] [CrossRef] [PubMed]
- Silver, D.A.; Pellicer, I.; Fair, W.R.; Heston, W.D.; Cordon-Cardo, C. Prostate-specific membrane antigen expression in normal and malignant human tissues. Clin. Cancer Res. 1997, 3, 81–85. [Google Scholar] [PubMed]
- Backhaus, P.; Noto, B.; Avramovic, N.; Grubert, L.S.; Huss, S.; Bögemann, M.; Stegger, L.; Weckesser, M.; Schäfers, M.; Rahbar, K. Targeting PSMA by radioligands in non-prostate disease—current status and future perspectives. Eur. J. Nucl. Med. 2018, 45, 860–877. [Google Scholar] [CrossRef]
- Uijen, M.J.M.; Derks, Y.H.W.; Merkx, R.I.J.; Schilham, M.G.M.; Roosen, J.; Privé, B.M.; van Lith, S.A.M.; van Herpen, C.M.L.; Gotthardt, M.; Heskamp, S.; et al. PSMA radioligand therapy for solid tumors other than prostate cancer: background, opportunities, challenges, and first clinical reports. Eur. J. Nucl. Med. 2021, 48, 4350–4368. [Google Scholar] [CrossRef]
- An, S.; Huang, G.; Liu, J.; Wei, W. PSMA-targeted theranostics of solid tumors: applications beyond prostate cancers. Eur. J. Nucl. Med. 2022, 49, 3973–3976. [Google Scholar] [CrossRef]
- Kratochwil, C.; Haberkorn, U.; Giesel, F.L. Radionuclide Therapy of Metastatic Prostate Cancer. Semin. Nucl. Med. 2019, 49, 313–325. [Google Scholar] [CrossRef]
- Kulkarni, H.R.; Singh, A.; Schuchardt, C.; Niepsch, K.; Sayeg, M.; Leshch, Y.; Wester, H.-J.; Baum, R.P. PSMA-Based Radioligand Therapy for Metastatic Castration-Resistant Prostate Cancer: The Bad Berka Experience Since 2013. J. Nucl. Med. 2016, 57, 97S–104S. [Google Scholar] [CrossRef] [PubMed]
- Sanli, Y.; Simsek, D.H.; Sanli, O.; Subramaniam, R.M.; Kendi, A.T. 177Lu-PSMA Therapy in Metastatic Castration-Resistant Prostate Cancer. Biomedicines 2021, 9, 430. [Google Scholar] [CrossRef] [PubMed]
- Rahbar, K.; Ahmadzadehfar, H.; Kratochwil, C.; Haberkorn, U.; Schäfers, M.; Essler, M.; Baum, R.P.; Kulkarni, H.R.; Schmidt, M.; Drzezga, A.; et al. German Multicenter Study Investigating 177Lu-PSMA-617 Radioligand Therapy in Advanced Prostate Cancer Patients. J. Nucl. Med. 2017, 58, 85–90. [Google Scholar] [CrossRef] [PubMed]
- Kratochwil, C.; Bruchertseifer, F.; Rathke, H.; Bronzel, M.; Apostolidis, C.; Weichert, W.; Haberkorn, U.; Giesel, F.L.; Morgenstern, A. Targeted α-Therapy of Metastatic Castration-Resistant Prostate Cancer with 225Ac-PSMA-617: Dosimetry Estimate and Empiric Dose Finding. J. Nucl. Med. 2017, 58, 1624–1631. [Google Scholar] [CrossRef]
- Wang, F.; Li, Z.; Feng, X.; Yang, D.; Lin, M. Advances in PSMA-targeted therapy for prostate cancer. Prostate Cancer Prostatic Dis. 2021, 25, 11–26. [Google Scholar] [CrossRef] [PubMed]
- Tao, L.; Huang, G.; Song, H.; Chen, Y.; Chen, L. Cancer associated fibroblasts: An essential role in the tumor microenvironment. Oncol. Lett. 2017, 14, 2611–2620. [Google Scholar] [CrossRef] [PubMed]
- Kratochwil, C.; Flechsig, P.; Lindner, T.; Abderrahim, L.; Altmann, A.; Mier, W.; Adeberg, S.; Rathke, H.; Röhrich, M.; Winter, H.; et al. 68Ga-FAPI PET/CT: Tracer Uptake in 28 Different Kinds of Cancer. J. Nucl. Med. 2019, 60, 801–805. [Google Scholar] [CrossRef] [PubMed]
- Calais, J. FAP: The Next Billion Dollar Nuclear Theranostics Target? J Nucl Med. 2020, 61, 163–165. [Google Scholar] [CrossRef]
- Lindner, T.; Loktev, A.; Altmann, A.; Giesel, F.; Kratochwil, C.; Debus, J.; Jäger, D.; Mier, W.; Haberkorn, U. Development of Quinoline-Based Theranostic Ligands for the Targeting of Fibroblast Activation Protein. J. Nucl. Med. 2018, 59, 1415–1422. [Google Scholar] [CrossRef]
- Zhao, L.; Chen, J.; Pang, Y.; Fu, K.; Shang, Q.; Wu, H.; Sun, L.; Lin, Q.; Chen, H. Fibroblast activation protein-based theranostics in cancer research: A state-of-the-art review. Theranostics 2022, 12, 1557–1569. [Google Scholar] [CrossRef]
- Roustaei H, Kiamanesh Z, Askari E, Sadeghi R, Aryana K, Treglia G. Could Fibroblast Activation Protein (FAP)-Specific Radioligands Be Considered as Pan-Tumor Agents? Contrast Media Mol Imaging. 2022, 2022, 3948873. [Google Scholar]
- Kuyumcu, S.; Kovan, B.M.; Sanli, Y.; Buyukkaya, F.; Simsek, D.H.; Özkan, Z.G.; Isik, E.G.; Ekenel, M.; Turkmen, C. Safety of Fibroblast Activation Protein–Targeted Radionuclide Therapy by a Low-Dose Dosimetric Approach Using 177Lu-FAPI04. Clin. Nucl. Med. 2021, 46, 641–646. [Google Scholar] [CrossRef] [PubMed]
- Rathke H, Fuxius S, Giesel FL, Lindner T, Debus J, Haberkorn U, Kratochwil C. Two Tumors, One Target: Preliminary Experience With 90Y-FAPI Therapy in a Patient With Metastasized Breast and Colorectal Cancer. Clin Nucl Med. 2021, 46, 842–844. [Google Scholar] [CrossRef] [PubMed]
- Assadi M, Rekabpour SJ, Jafari E, Divband G, Nikkholgh B, Amini H, Kamali H, Ebrahimi S, Shakibazad N, Jokar N, Nabipour I, Ahmadzadehfar H. Feasibility and Therapeutic Potential of 177Lu-Fibroblast Activation Protein Inhibitor-46 for Patients With Relapsed or Refractory Cancers: A Preliminary Study. Clin Nucl Med. 2021, 46, e523–e530. [Google Scholar] [CrossRef] [PubMed]
- Fu, K.; Pang, Y.; Zhao, L.; Lin, L.; Wu, H.; Sun, L.; Lin, Q.; Chen, H. FAP-targeted radionuclide therapy with [177Lu]Lu-FAPI-46 in metastatic nasopharyngeal carcinoma. Eur. J. Nucl. Med. 2021, 49, 1767–1769. [Google Scholar] [CrossRef] [PubMed]
- Ferdinandus, J.; Costa, P.F.; Kessler, L.; Weber, M.; Hirmas, N.; Kostbade, K.; Bauer, S.; Schuler, M.; Ahrens, M.; Schildhaus, H.-U.; et al. Initial clinical experience with 90Y-FAPI-46 radioligand therapy for advanced stage solid tumors: a case series of nine patients. J. Nucl. Med. 2022, 63, 727–734. [Google Scholar] [CrossRef] [PubMed]
- Fu, H.; Huang, J.; Sun, L.; Wu, H.; Chen, H. FAP-Targeted Radionuclide Therapy of Advanced Radioiodine-Refractory Differentiated Thyroid Cancer With Multiple Cycles of 177Lu-FAPI-46. Clin. Nucl. Med. 2022, 47, 906–907. [Google Scholar] [CrossRef]
- Fendler, W.P.; Pabst, K.M.; Kessler, L.; Costa, P.F.; Ferdinandus, J.; Weber, M.; Lippert, M.; Lueckerath, K.; Umutlu, L.; Kostbade, K.; et al. Safety and Efficacy of 90Y-FAPI-46 Radioligand Therapy in Patients with Advanced Sarcoma and Other Cancer Entities. Clin. Cancer Res. 2022, 28, 4346–4353. [Google Scholar] [CrossRef]
- Kratochwil, C.; Giesel, F.L.; Rathke, H.; Fink, R.; Dendl, K.; Debus, J.; Mier, W.; Jäger, D.; Lindner, T.; Haberkorn, U. [153Sm]Samarium-labeled FAPI-46 radioligand therapy in a patient with lung metastases of a sarcoma. Eur. J. Nucl. Med. 2021, 48, 3011–3013. [Google Scholar] [CrossRef]
- Zhang, P.; Xu, M.; Ding, J.; Chen, J.; Zhang, T.; Huo, L.; Liu, Z. Fatty acid-conjugated radiopharmaceuticals for fibroblast activation protein-targeted radiotherapy. Eur. J. Nucl. Med. 2022, 49, 1985–1996. [Google Scholar] [CrossRef]
- Xu, M.; Zhang, P.; Ding, J.; Chen, J.; Huo, L.; Liu, Z. Albumin Binder–Conjugated Fibroblast Activation Protein Inhibitor Radiopharmaceuticals for Cancer Therapy. J. Nucl. Med. 2022, 63, 952–958. [Google Scholar] [CrossRef] [PubMed]
- Wen, X.; Xu, P.; Shi, M.; Liu, J.; Zeng, X.; Zhang, Y.; Shi, C.; Li, J.; Guo, Z.; Zhang, X.; et al. Evans blue-modified radiolabeled fibroblast activation protein inhibitor as long-acting cancer therapeutics. Theranostics 2022, 12, 422–433. [Google Scholar] [CrossRef] [PubMed]
- Moon, E.S.; Ballal, S.; Yadav, M.P.; Bal, C.; Van Rymenant, Y.; Stephan, S.; Bracke, A.; Van der Veken, P.; De Meester, I.; Roesch, F. Fibroblast Activation Protein (FAP) targeting homodimeric FAP inhibitor radiotheranostics: a step to improve tumor uptake and retention time. Am J Nucl Med Mol Imaging. 2021, 11, 476–491. [Google Scholar] [PubMed]
- Zhao, L.; Chen, J.; Pang, Y.; Fang, J.; Fu, K.; Meng, L.; Zhang, X.; Guo, Z.; Wu, H.; Sun, L.; et al. Development of Fibroblast Activation Protein Inhibitor-Based Dimeric Radiotracers with Improved Tumor Retention and Antitumor Efficacy. Mol. Pharm. 2022, 19, 3640–3651. [Google Scholar] [CrossRef] [PubMed]
- Ballal, S.; Yadav, M.P.; Moon, E.S.; Kramer, V.S.; Roesch, F.; Kumari, S.; Bal, C. First-In-Human Results on the Biodistribution, Pharmacokinetics, and Dosimetry of [177Lu]Lu-DOTA.SA.FAPi and [177Lu]Lu-DOTAGA.(SA.FAPi)2. Pharmaceuticals 2021, 14, 1212. [Google Scholar] [CrossRef]
- Ballal, S.; Yadav, M.P.; Moon, E.S.; Roesch, F.; Kumari, S.; Agarwal, S.; Tripathi, M.; Sahoo, R.K.; Mangu, B.S.; Tupalli, A.; et al. Novel Fibroblast Activation Protein Inhibitor-Based Targeted Theranostics for Radioiodine-Refractory Differentiated Thyroid Cancer Patients: A Pilot Study. Thyroid® 2022, 32, 65–77. [Google Scholar] [CrossRef]
- Baum RP, Schuchardt C, Singh A, Chantadisai M, Robiller FC, Zhang J, Mueller D, Eismant A, Almaguel F, Zboralski D, Osterkamp F, Hoehne A, Reineke U, Smerling C, Kulkarni HR. Feasibility, Biodistribution and Preliminary Dosimetry in Peptide-Targeted Radionuclide Therapy (PTRT) of Diverse Adenocarcinomas using 177Lu-FAP-2286: First-in-Human Results. J Nucl Med. 2022, 63, 415–423. [Google Scholar] [CrossRef]
- Millul, J.; Bassi, G.; Mock, J.; Elsayed, A.; Pellegrino, C.; Zana, A.; Plaza, S.D.; Nadal, L.; Gloger, A.; Schmidt, E.; et al. An ultra-high-affinity small organic ligand of fibroblast activation protein for tumor-targeting applications. Proc. Natl. Acad. Sci. 2021, 118. [Google Scholar] [CrossRef]
- Bartoli F, Elsinga P, Nazario LR, Zana A, Galbiati A, Millul J, Migliorini F, Cazzamalli S, Neri D, Slart RHJA, Erba PA. Automated Radiosynthesis, Preliminary In Vitro/In Vivo Characterization of OncoFAP-Based Radiopharmaceuticals for Cancer Imaging and Therapy. Pharmaceuticals (Basel). 2022, 15, 958. [Google Scholar] [CrossRef]
- Galbiati, A.; Zana, A.; Bocci, M.; Millul, J.; Elsayed, A.; Mock, J.; Neri, D.; Cazzamalli, S. A Dimeric FAP-Targeting Small-Molecule Radioconjugate with High and Prolonged Tumor Uptake. J. Nucl. Med. 2022, 63, 1852–1858. [Google Scholar] [CrossRef]
- Liu, Y.; Watabe, T.; Kaneda-Nakashima, K.; Shirakami, Y.; Naka, S.; Ooe, K.; Toyoshima, A.; Nagata, K.; Haberkorn, U.; Kratochwil, C.; et al. Fibroblast activation protein targeted therapy using [177Lu]FAPI-46 compared with [225Ac]FAPI-46 in a pancreatic cancer model. Eur. J. Nucl. Med. 2022, 49, 871–880. [Google Scholar] [CrossRef] [PubMed]
- Lindner T, Altmann A, Krämer S, Kleist C, Loktev A, Kratochwil C, Giesel F, Mier W, Marme F, Debus J, Haberkorn U. Design and Development of 99mTc-Labeled FAPI Tracers for SPECT Imaging and 188Re Therapy. J Nucl Med. 2020, 61, 1507–1513. [Google Scholar] [CrossRef] [PubMed]
- Lindner, T.; Giesel, F.L.; Kratochwil, C.; Serfling, S.E. Radioligands Targeting Fibroblast Activation Protein (FAP). Cancers 2021, 13, 5744. [Google Scholar] [CrossRef] [PubMed]
- Imlimthan, S.; Moon, E.S.; Rathke, H.; Afshar-Oromieh, A.; Rösch, F.; Rominger, A.; Gourni, E. New Frontiers in Cancer Imaging and Therapy Based on Radiolabeled Fibroblast Activation Protein Inhibitors: A Rational Review and Current Progress. Pharmaceuticals 2021, 14, 1023. [Google Scholar] [CrossRef]
- Pazzaglia, S.; Pioli, C. Multifaceted Role of PARP-1 in DNA Repair and Inflammation: Pathological and Therapeutic Implications in Cancer and Non-Cancer Diseases. Cells 2019, 9, 41. [Google Scholar] [CrossRef] [PubMed]
- Chan, C.Y.; Tan, K.V.; Cornelissen, B. PARP Inhibitors in Cancer Diagnosis and Therapy. Clin. Cancer Res. 2021, 27, 1585–1594. [Google Scholar] [CrossRef]
- Jannetti, S.A.; Zeglis, B.M.; Zalutsky, M.R.; Reiner, T. Poly(ADP-Ribose)Polymerase (PARP) Inhibitors and Radiation Therapy. Front. Pharmacol. 2020, 11, 170. [Google Scholar] [CrossRef]
- Carney, B.; Kossatz, S.; Reiner, T. Molecular Imaging of PARP. J. Nucl. Med. 2017, 58, 1025–1030. [Google Scholar] [CrossRef]
- Sankaranarayanan, R.A.; Kossatz, S.; Weber, W.; Beheshti, M.; Morgenroth, A.; Mottaghy, F.M. Advancements in PARP1 Targeted Nuclear Imaging and Theranostic Probes. J. Clin. Med. 2020, 9, 2130. [Google Scholar] [CrossRef]
- Jannetti, S.A.; Carlucci, G.; Carney, B.; Kossatz, S.; Shenker, L.; Carter, L.M.; Salinas, B.; Brand, C.; Sadique, A.; Donabedian, P.L.; et al. PARP-1–Targeted Radiotherapy in Mouse Models of Glioblastoma. J. Nucl. Med. 2018, 59, 1225–1233. [Google Scholar] [CrossRef]
- Nguyen NT, Pacelli A, Nader M, Kossatz S. DNA Repair Enzyme Poly(ADP-Ribose) Polymerase 1/2 (PARP1/2)-Targeted Nuclear Imaging and Radiotherapy. Cancers (Basel). 2022, 14, 1129. [Google Scholar] [CrossRef] [PubMed]
- Zhou, D.; Chen, H.; Mpoy, C.; Afrin, S.; Rogers, B.E.; Garbow, J.R.; Katzenellenbogen, J.A.; Xu, J. Radiosynthesis and Evaluation of Talazoparib and Its Derivatives as PARP-1-Targeting Agents. Biomedicines 2021, 9, 565. [Google Scholar] [CrossRef] [PubMed]
- Destro G, Chen Z, Chan CY, Fraser C, Dias G, Mosley M, Guibbal F, Gouverneur V, Cornelissen B. A radioiodinated rucaparib analogue as an Auger electron emitter for cancer therapy. Nucl Med Biol. 2022, 116‒117, 108312. [Google Scholar]
- Makvandi, M.; Lee, H.; Puentes, L.N.; Reilly, S.W.; Rathi, K.S.; Weng, C.-C.; Chan, H.S.; Hou, C.; Raman, P.; Martinez, D.; et al. Targeting PARP-1 with Alpha-Particles Is Potently Cytotoxic to Human Neuroblastoma in Preclinical Models. Mol. Cancer Ther. 2019, 18, 1195–1204. [Google Scholar] [CrossRef] [PubMed]
- Lee, H.; Riad, A.; Martorano, P.; Mansfield, A.; Samanta, M.; Batra, V.; Mach, R.H.; Maris, J.M.; Pryma, D.A.; Makvandi, M. PARP-1–Targeted Auger Emitters Display High-LET Cytotoxic Properties In Vitro but Show Limited Therapeutic Utility in Solid Tumor Models of Human Neuroblastoma. J. Nucl. Med. 2020, 61, 850–856. [Google Scholar] [CrossRef] [PubMed]
- Pirovano, G.; Jannetti, S.A.; Carter, L.M.; Sadique, A.; Kossatz, S.; Guru, N.; De Souza França, P.D.; Maeda, M.; Zeglis, B.M.; Lewis, J.S.; et al. Targeted Brain Tumor Radiotherapy Using an Auger Emitter. Clin. Cancer Res. 2020, 26, 2871–2881. [Google Scholar] [CrossRef] [PubMed]
- Sankaranarayanan, R.A.; Florea, A.; Allekotte, S.; Vogg, A.T.J.; Maurer, J.; Schäfer, L.; Bolm, C.; Terhorst, S.; Classen, A.; Bauwens, M.; et al. PARP targeted Auger emitter therapy with [125I]PARPi-01 for triple-negative breast cancer. EJNMMI Res. 2022, 12, 1–12. [Google Scholar] [CrossRef] [PubMed]
- Brown, J.M. Tumor Hypoxia in Cancer Therapy. Methods Enzymol. 2007, 435, 295–321. [Google Scholar] [CrossRef]
- Supuran, C.T. Structure and function of carbonic anhydrases. Biochem. J. 2016, 473, 2023–2032. [Google Scholar] [CrossRef]
- Benej M, Pastorekova S, Pastorek J. Carbonic Anhydrase IX: Regulation and role in cancer. In Carbonic Anhydrase: Mechanism, Regulation, Links to Disease, and Industrial Applications; Subcellular Biochemistry; Springer: Dordrecht, The Netherlands, 2014. [Google Scholar]
- Singh, S.; Lomelino, C.L.; Mboge, M.Y.; Frost, S.C.; McKenna, R. Cancer Drug Development of Carbonic Anhydrase Inhibitors beyond the Active Site. Molecules 2018, 23, 1045. [Google Scholar] [CrossRef]
- Lau, J.; Lin, K.-S.; Bénard, F. Past, Present, and Future: Development of Theranostic Agents Targeting Carbonic Anhydrase IX. Theranostics 2017, 7, 4322–4339. [Google Scholar] [CrossRef] [PubMed]
- Iikuni, S.; Ono, M.; Watanabe, H.; Shimizu, Y.; Sano, K.; Saji, H. Cancer radiotheranostics targeting carbonic anhydrase-IX with 111In- and 90Y-labeled ureidosulfonamide scaffold for SPECT imaging and radionuclide-based therapy. Theranostics 2018, 8, 2992–3006. [Google Scholar] [CrossRef] [PubMed]
- Janoniene, A.; Petrikaite, V. In Search of Advanced Tumor Diagnostics and Treatment: Achievements and Perspectives of Carbonic Anhydrase IX Targeted Delivery. Mol. Pharm. 2020, 17, 1800–1815. [Google Scholar] [CrossRef] [PubMed]
- Shahrokhi, P.; Farahani, A.M.; Tamaddondar, M. Radiolabeled vitamins as the potential diagnostic probes for targeted tumor imaging. Bioorganic Chem. 2022, 122, 105717. [Google Scholar] [CrossRef] [PubMed]
- Jurczyk, M.; Jelonek, K.; Musiał-Kulik, M.; Beberok, A.; Wrześniok, D.; Kasperczyk, J. Single- versus Dual-Targeted Nanoparticles with Folic Acid and Biotin for Anticancer Drug Delivery. Pharmaceutics 2021, 13, 326. [Google Scholar] [CrossRef] [PubMed]
- Jallinoja, V.I.; Houghton, J.L. Current Landscape in Clinical Pretargeted Radioimmunoimaging and Therapy. J. Nucl. Med. 2021, 62, 1200–1206. [Google Scholar] [CrossRef]
- Russell-Jones, G.; McTavish, K.; McEwan, J.; Rice, J.; Nowotnik, D. Vitamin-mediated targeting as a potential mechanism to increase drug uptake by tumours. J. Inorg. Biochem. 2004, 98, 1625–1633. [Google Scholar] [CrossRef] [PubMed]
- Low, P.S.; Kularatne, S.A. Folate-targeted therapeutic and imaging agents for cancer. Curr. Opin. Chem. Biol. 2009, 13, 256–262. [Google Scholar] [CrossRef]
- Xia, W.; Low, P.S. Folate-Targeted Therapies for Cancer. J. Med. Chem. 2010, 53, 6811–6824. [Google Scholar] [CrossRef]
- Muller, C. Folate Based Radiopharmaceuticals for Imaging and Therapy of Cancer and Inflammation. Curr. Pharm. Des. 2012, 18, 1058–1083. [Google Scholar] [CrossRef]
- Müller, C.; Guzik, P.; Siwowska, K.; Cohrs, S.; Schmid, R.M.; Schibli, R. Combining Albumin-Binding Properties and Interaction with Pemetrexed to Improve the Tissue Distribution of Radiofolates. Molecules 2018, 23, 1465. [Google Scholar] [CrossRef] [PubMed]
- Benešová, M.; Guzik, P.; Deberle, L.M.; Busslinger, S.D.; Landolt, T.; Schibli, R.; Müller, C. Design and Evaluation of Novel Albumin-Binding Folate Radioconjugates: Systematic Approach of Varying the Linker Entities. Mol. Pharm. 2022, 19, 963–973. [Google Scholar] [CrossRef] [PubMed]
- Boss, S.D.; Ametamey, S.M. Development of Folate Receptor−Targeted PET Radiopharmaceuticals for Tumor Imaging—A Bench-to-Bedside Journey. Cancers 2020, 12, 1508. [Google Scholar] [CrossRef] [PubMed]
- Müller C, Schibli R. Prospects in folate receptor-targeted radionuclide therapy. Front Oncol. 2013, 3, 249. [Google Scholar]
- Kuda-Wedagedara ANW, Workinger JL, Nexo E, Doyle RP, Viola-Villegas N. 89Zr-Cobalamin PET Tracer: Synthesis, Cellular Uptake, and Use for Tumor Imaging. ACS Omega. 2017, 2, 6314–6320. [Google Scholar] [CrossRef] [PubMed]
- Gendron LN, Zites DC, LaRochelle EPM, Gunn JR, Pogue BW, Shell TA, Shell JR. Tumor targeting vitamin B12 derivatives for X-ray induced treatment of pancreatic adenocarcinoma. Photodiagnosis Photodyn Ther. 2020, 30, 101637. [Google Scholar] [CrossRef]
- Snyder, F.; Wood, R. Alkyl and alk-1-enyl ethers of glycerol in lipids from normal and neoplastic human tissues. Cancer Res. 1969, 29, 251–7. [Google Scholar] [PubMed]
- Vink SR, van Blitterswijk WJ, Schellens JH, Verheij M. Rationale and clinical application of alkylphospholipid analogues in combination with radiotherapy. Cancer Treat Rev. 2007, 33, 191–202. [Google Scholar] [CrossRef]
- Mollinedo, F.; Gajate, C. Lipid rafts and clusters of apoptotic signaling molecule-enriched rafts in cancer therapy. Futur. Oncol. 2010, 6, 811–821. [Google Scholar] [CrossRef]
- Weichert, J.P.; Clark, P.A.; Kandela, I.K.; Vaccaro, A.M.; Clarke, W.; Longino, M.A.; Pinchuk, A.N.; Farhoud, M.; Swanson, K.I.; Floberg, J.M.; et al. Alkylphosphocholine Analogs for Broad-Spectrum Cancer Imaging and Therapy. Sci. Transl. Med. 2014, 6, 240ra75–240ra75. [Google Scholar] [CrossRef]
- Meyer, K.L.; Schwendner, S.W.; Counsell, R.E. Potential tumor or organ-imaging agents. Radioiodinated phospholipid ethers. J. Med. Chem. 1989, 32, 2142–2147. [Google Scholar] [CrossRef] [PubMed]
- Plotzke, K.P.; Haradahira, T.; Stancato, L.; Olken, N.M.; Skinner, S.; Gross, M.D.; Wahl, R.L.; Counsell, R.E. Selective localization of radioiodinated alkylphosphocholine derivatives in tumors. Int. J. Radiat. Appl. Instrumentation. Part B. Nucl. Med. Biol. 1992, 19, 765–773. [Google Scholar] [CrossRef] [PubMed]
- Rampy, M.; Chou, T.; Pinchuk, A.; Skinner, R.; Gross; Fisher, S. ; Wahl, R.; Counsell, R. Synthesis and biological evaluation of radioiodinated phospholipid ether analogs. Nucl. Med. Biol. 1995, 22, 505–512. [Google Scholar] [CrossRef] [PubMed]
- Grudzinski, J.J.; Hall, L.T.; Cho, S.; Liu, G.; Traynor, A.; Lee, M.H.; Longino, M.; Pinchuk, A.; Jaskowiak, C.; Bednarz, B.; et al. Clinical Imaging and Dosimetry of a Pan-Cancer Targeting Alkylphosphocholine Analog, [124I]I-NM404. Radiation 2022, 2, 215–227. [Google Scholar] [CrossRef]
- Pinchuk, A.N.; Rampy, M.A.; Longino, M.A.; Skinner, R.W.S.; Gross, M.D.; Weichert, J.P.; Counsell, R.E. Synthesis and Structure−Activity Relationship Effects on the Tumor Avidity of Radioiodinated Phospholipid Ether Analogues. J. Med. Chem. 2006, 49, 2155–2165. [Google Scholar] [CrossRef] [PubMed]
- Morris, Z.S.; Weichert, J.P.; Saker, J.; Armstrong, E.A.; Besemer, A.; Bednarz, B.; Kimple, R.J.; Harari, P.M. Therapeutic combination of radiolabeled CLR1404 with external beam radiation in head and neck cancer model systems. Radiother. Oncol. 2015, 116, 504–509. [Google Scholar] [CrossRef] [PubMed]
- Lubner SJ, Mullvain J, Perlman S, Pishvaian M, Mortimer J, Oliver K, Heideman J, Hall L, Weichert J, Liu G. A Phase 1, Multi-Center, Open-Label, Dose-Escalation Study of 131I-CLR1404 in Subjects with Relapsed or Refractory Advanced Solid Malignancies. Cancer Invest. 2015, 33, 483–489. [Google Scholar] [CrossRef] [PubMed]
- Hall, L.T.; Titz, B.; Robins, H.I.; Bednarz, B.P.; Perlman, S.B.; Weichert, J.P.; Kuo, J.S. PET/CT imaging of the diapeutic alkylphosphocholine analog 124I-CLR1404 in high and low-grade brain tumors. Am J Nucl Med Mol Imaging. 2017, 7, 157–166. [Google Scholar]
- Baiu, D.C.; Marsh, I.R.; Boruch, A.E.; Shahi, A.; Bhattacharya, S.; Jeffery, J.J.; Zhao, Q.; Hall, L.T.; Weichert, J.P.; Bednarz, B.P.; et al. Targeted Molecular Radiotherapy of Pediatric Solid Tumors Using a Radioiodinated Alkyl-Phospholipid Ether Analog. J. Nucl. Med. 2018, 59, 244–250. [Google Scholar] [CrossRef]
- Hall, L.T.; Titz, B.; Baidya, N.; van der Kolk, A.G.; Robins, H.I.; Otto, M.; Perlman, S.B.; Weichert, J.P.; Kuo, J.S. [124I]CLR1404 PET/CT in High-Grade Primary and Metastatic Brain Tumors. Mol. Imaging Biol. 2020, 22, 434–443. [Google Scholar] [CrossRef]
- Shahi, A.; Weiss, G.E.; Bhattacharya, S.; Baiu, D.C.; Marino, R.; Pula, T.; Callander, N.S.; Asimakopoulos, F.; Otto, M. Targeted treatment of multiple myeloma with a radioiodinated small molecule radiopharmaceutical. Leuk. Lymphoma 2021, 62, 1518–1521. [Google Scholar] [CrossRef] [PubMed]
- Longcor, J.; Callander, N.; Oliver, K.; Chanan-Khan, A.; Ailawadhi, S. Iopofosine I-131 treatment in late-line patients with relapsed/refractory multiple myeloma post anti-BCMA immunotherapy. Blood Cancer J. 2022, 12, 130. [Google Scholar] [CrossRef]
- Grudzinski JJ, Hernandez R, Marsh I, Patel RB, Aluicio-Sarduy E, Engle J, Morris Z, Bednarz B, Weichert J. Preclinical Characterization of 86/90Y-NM600 in a Variety of Murine and Human Cancer Tumor Models. J Nucl Med. 2019, 60, 1622–1628. [Google Scholar] [CrossRef] [PubMed]
- Hernandez, R.; Grudzinski, J.J.; Aluicio-Sarduy, E.; Massey, C.F.; Pinchuk, A.N.; Bitton, A.N.; Patel, R.; Zhang, R.; Rao, A.V.; Iyer, G.; et al. 177Lu-NM600 Targeted Radionuclide Therapy Extends Survival in Syngeneic Murine Models of Triple-Negative Breast Cancer. J. Nucl. Med. 2020, 61, 1187–1194. [Google Scholar] [CrossRef] [PubMed]
- Norain, A.; Dadachova, E. Targeted Radionuclide Therapy of Melanoma. Semin. Nucl. Med. 2016, 46, 250–259. [Google Scholar] [CrossRef] [PubMed]
- Allen, K.J.H.; Malo, M.E.; Jiao, R.; Dadachova, E. Targeting Melanin in Melanoma with Radionuclide Therapy. Int. J. Mol. Sci. 2022, 23, 9520. [Google Scholar] [CrossRef] [PubMed]
- Thomas NE, Kricker A, Waxweiler WT, Dillon PM, Busman KJ, From L, Groben PA, Armstrong BK, Anton-Culver H, Gruber SB, Marrett LD, Gallagher RP, Zanetti R, Rosso S, Dwyer T, Venn A, Kanetsky PA, Orlow I, Paine S, Ollila DW, Reiner AS, Luo L, Hao H, Frank JS, Begg CB, Berwick M; Genes, Environment, and Melanoma (GEM) Study Group. Comparison of clinicopathologic features and survival of histopathologically amelanotic and pigmented melanomas: a population-based study. JAMA Dermatol. 2014, 150, 1306–1314. [Google Scholar] [CrossRef]
- Klein, M.; Lotem, M.; Peretz, T.; Zwas, S.T.; Mizrachi, S.; Liberman, Y.; Chisin, R.; Schachter, J.; Ron, I.G.; Iosilevsky, G.; et al. Safety and Efficacy of 188-Rhenium-Labeled Antibody to Melanin in Patients with Metastatic Melanoma. J. Ski. Cancer 2013, 2013, 1–8. [Google Scholar] [CrossRef]
- Rouanet, J.; Quintana, M.; Auzeloux, P.; Cachin, F.; Degoul, F. Benzamide derivative radiotracers targeting melanin for melanoma imaging and therapy: Preclinical/clinical development and combination with other treatments. Pharmacol. Ther. 2021, 224, 107829. [Google Scholar] [CrossRef]
- Mohammed, A.; Nicholl, C.; Titsch, U.; Eisenhut, M. Radioiodinated N-(alkylaminoalkyl)-substituted 4-methoxy-, 4-hydroxy-, and 4-aminobenzamides: Biological investigations for the improvement of melanoma-imaging agents. Nucl. Med. Biol. 1997, 24, 373–380. [Google Scholar] [CrossRef]
- Eisenhut M, Hull WE, Mohammed A, Mier W, Lay D, Just W, Gorgas K, Lehmann WD, Haberkorn U. Radioiodinated N-(2-diethylaminoethyl)benzamide derivatives with high melanoma uptake: structure-affinity relationships, metabolic fate, and intracellular localization. J Med Chem. 2000, 43, 3913–3922. [Google Scholar] [CrossRef] [PubMed]
- Auzeloux, P.; Papon, J.; Pasqualini, R.; Madelmont, J.-C. Synthesis and Biodistribution of a New Oxo-technetium-99m Bis(aminothiol) Complex as a Potential Melanoma Tracer. J. Med. Chem. 2001, 44, 1116–1121. [Google Scholar] [CrossRef] [PubMed]
- Oltmanns, D.; Eisenhut, M.; Mier, W.; Haberkorn, U. Benzamides as Melanotropic Carriers for Radioisotopes, Metals, Cytotoxic Agents and as Enzyme Inhibitors. Curr. Med. Chem. 2009, 16, 2086–2094. [Google Scholar] [CrossRef] [PubMed]
- Michelot, J.M.; Moreau, M.F.; Veyre, A.J.; Bonafous, J.F.; Bacin, F.J.; Madelmont, J.C.; Bussiere, F.; A Souteyrand, P.; Mauclaire, L.P.; Chossat, F.M. Phase II scintigraphic clinical trial of malignant melanoma and metastases with iodine-123-N-(2-diethylaminoethyl 4-iodobenzamide). J Nucl Med. 1993, 34, 1260–6. [Google Scholar] [PubMed]
- Link, EM. Targeting melanoma with 211At/131I-methylene blue: preclinical and clinical experience. Hybridoma. 1999, 18, 77–82. [Google Scholar] [CrossRef] [PubMed]
- Joyal, J.L.; Barrett, J.A.; Marquis, J.C.; Chen, J.; Hillier, S.M.; Maresca, K.P.; Boyd, M.; Gage, K.; Nimmagadda, S.; Kronauge, J.F.; et al. Preclinical Evaluation of an 131I-Labeled Benzamide for Targeted Radiotherapy of Metastatic Melanoma. Cancer Res 2010, 70, 4045–4053. [Google Scholar] [CrossRef]
- Degoul F, Borel M, Jacquemot N, Besse S, Communal Y, Mishellany F, Papon J, Penault-Llorca F, Donnarieix D, Doly M, Maigne L, Miot-Noirault E, Cayre A, Cluzel J, Moins N, Chezal JM, Bonnet M. In vivo efficacy of melanoma internal radionuclide therapy with a 131I-labelled melanin-targeting heteroarylcarboxamide molecule. Int J Cancer. 2013, 133, 1042–1053. [Google Scholar] [CrossRef]
- Xu, X.; Yuan, L.; Gai, Y.; Liu, Q.; Yin, L.; Jiang, Y.; Wang, Y.; Zhang, Y.; Lan, X. Targeted radiotherapy of pigmented melanoma with 131I-5-IPN. J. Exp. Clin. Cancer Res. 2018, 37, 1–13. [Google Scholar] [CrossRef]
- Mier, W.; Kratochwil, C.; Hassel, J.C.; Giesel, F.L.; Beijer, B.; Babich, J.W.; Friebe, M.; Eisenhut, M.; Enk, A.; Haberkorn, U. Radiopharmaceutical Therapy of Patients with Metastasized Melanoma with the Melanin-Binding Benzamide 131I-BA52. 2013, 55, 9–14. 14. [CrossRef]
- Thivat, E.; Rouanet, J.; Auzeloux, P.; Sas, N.; Jouberton, E.; Levesque, S.; Billoux, T.; Mansard, S.; Molnar, I.; Chanchou, M.; et al. Phase I study of [131I] ICF01012, a targeted radionuclide therapy, in metastatic melanoma: MELRIV-1 protocol. BMC Cancer 2022, 22, 1–10. [Google Scholar] [CrossRef]
Figure 1.
Linear Energy Transfert (LET) for different particle types (β-, α and Auger electron).
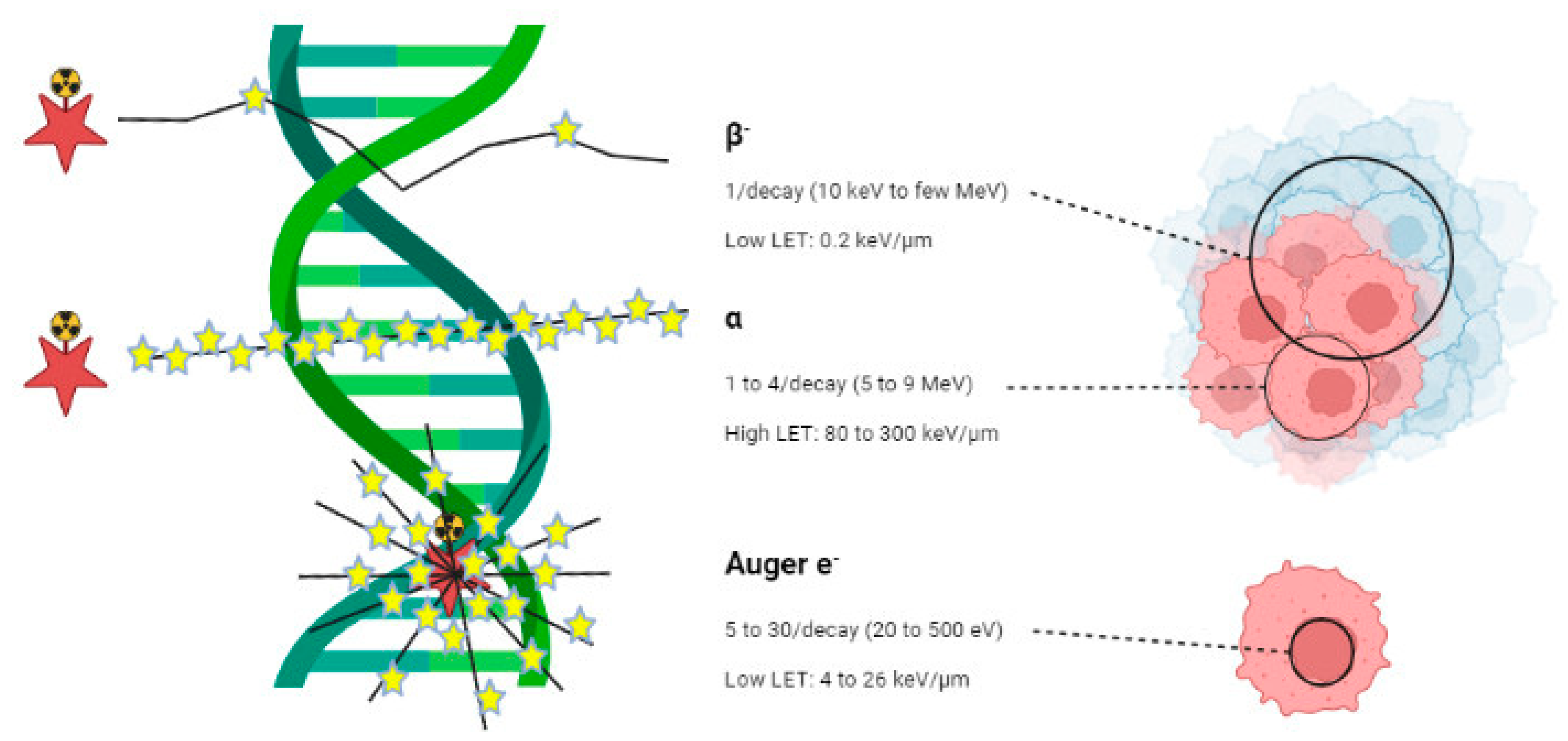
Figure 2.
Possible targets for targeted radionuclide therapy.
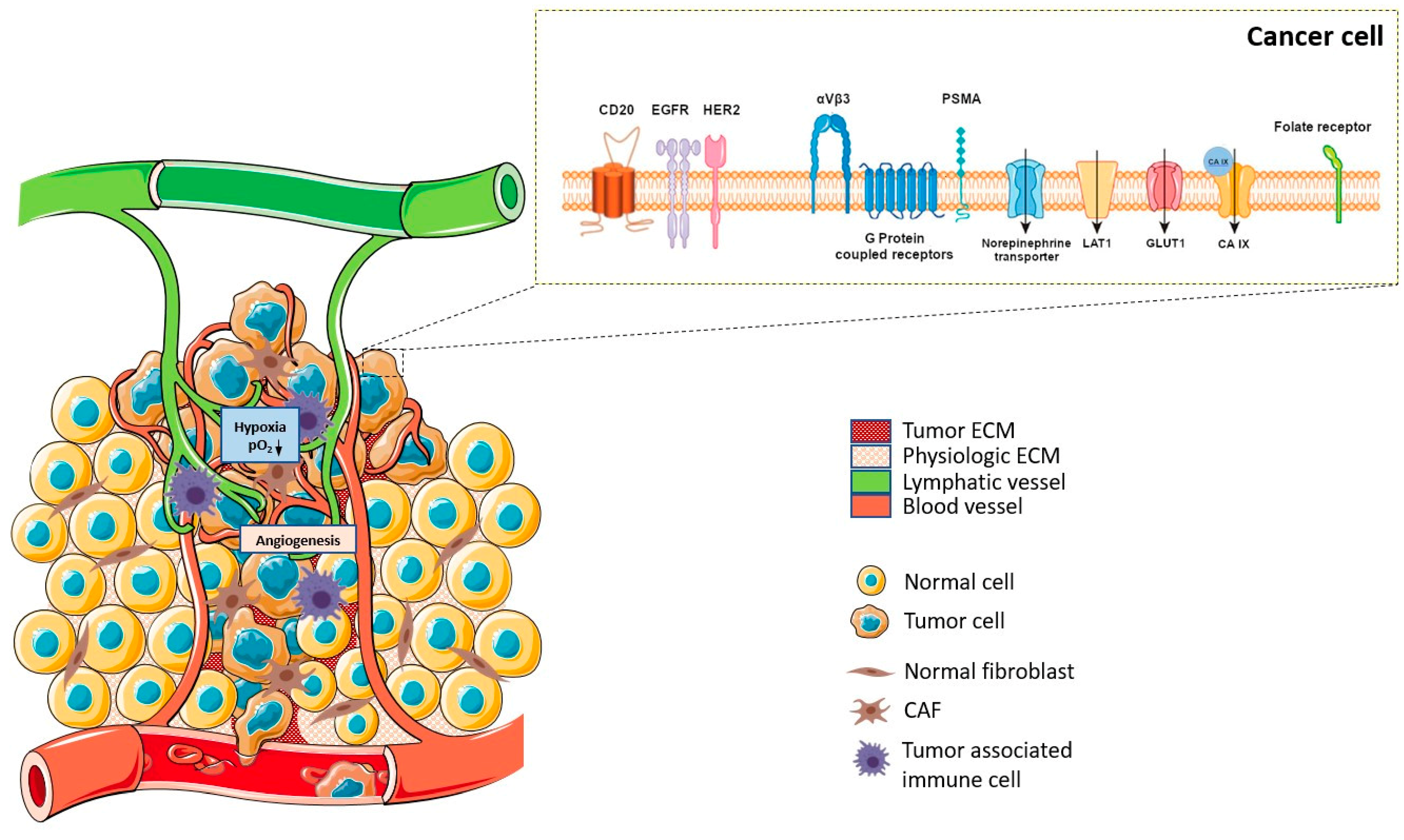
Figure 3.
Overview of targeted radionuclide therapy considerations.
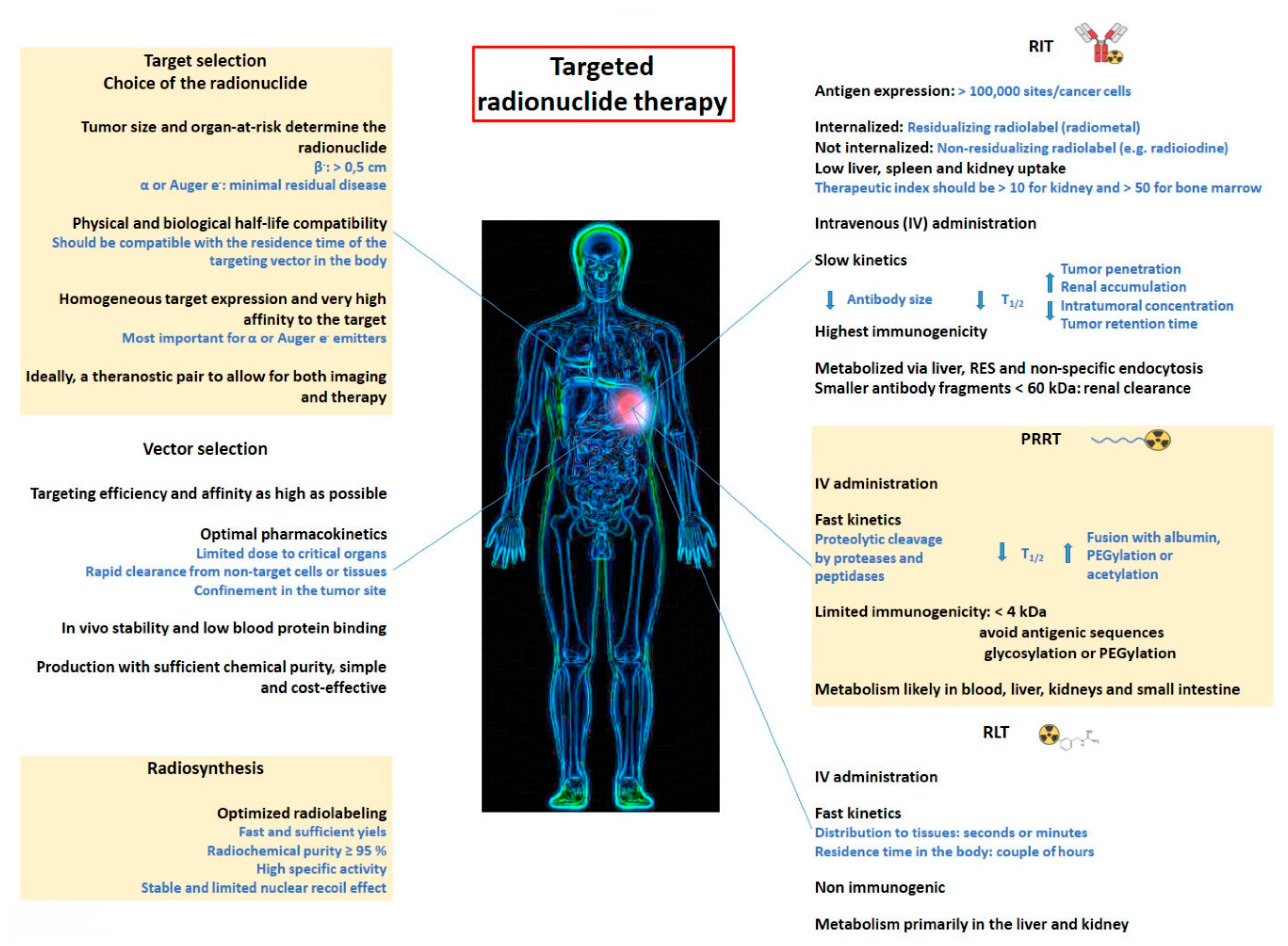
Figure 4.
mAbs and derivates used in RIT procedures.
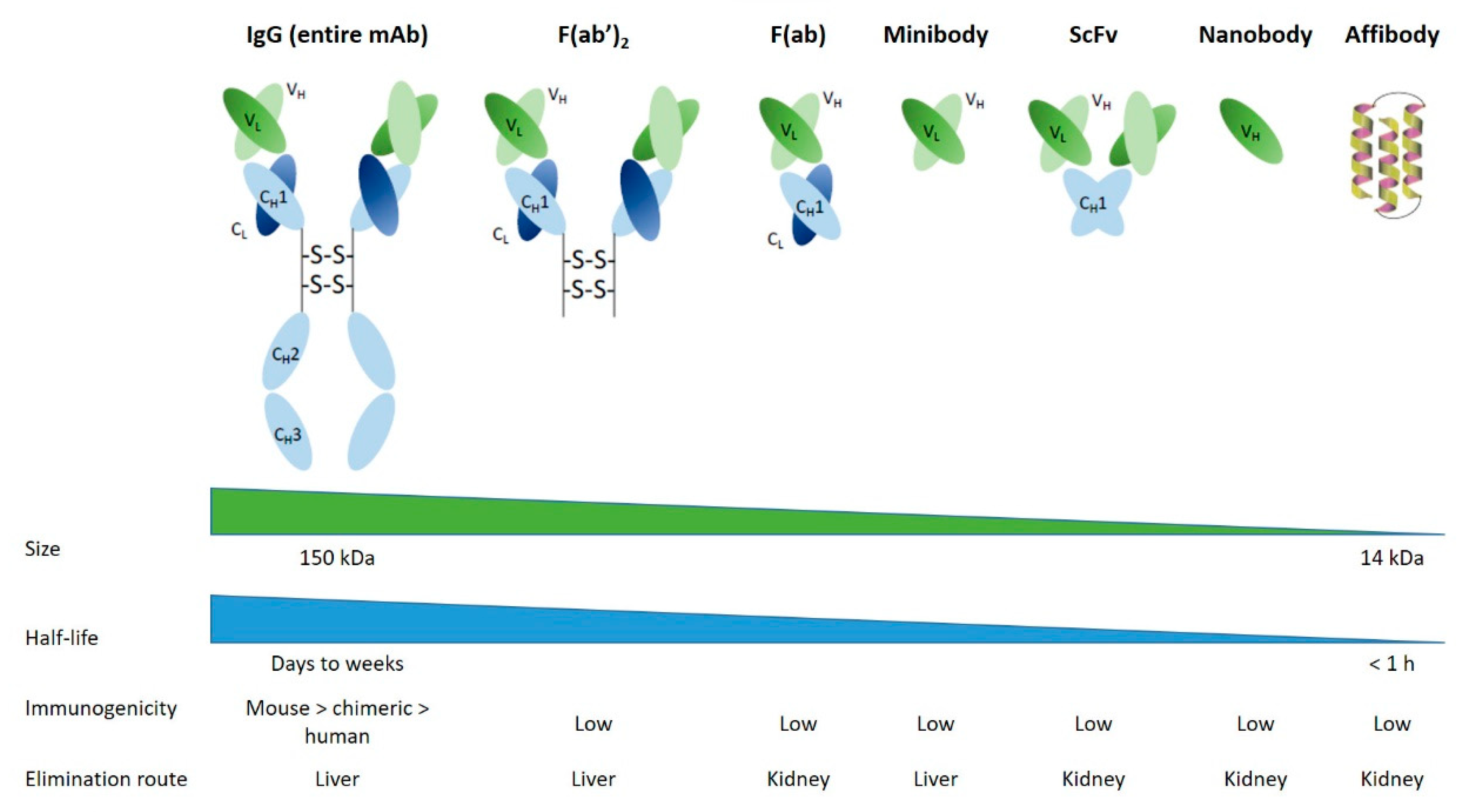
Figure 5.
The different types of aptamers.
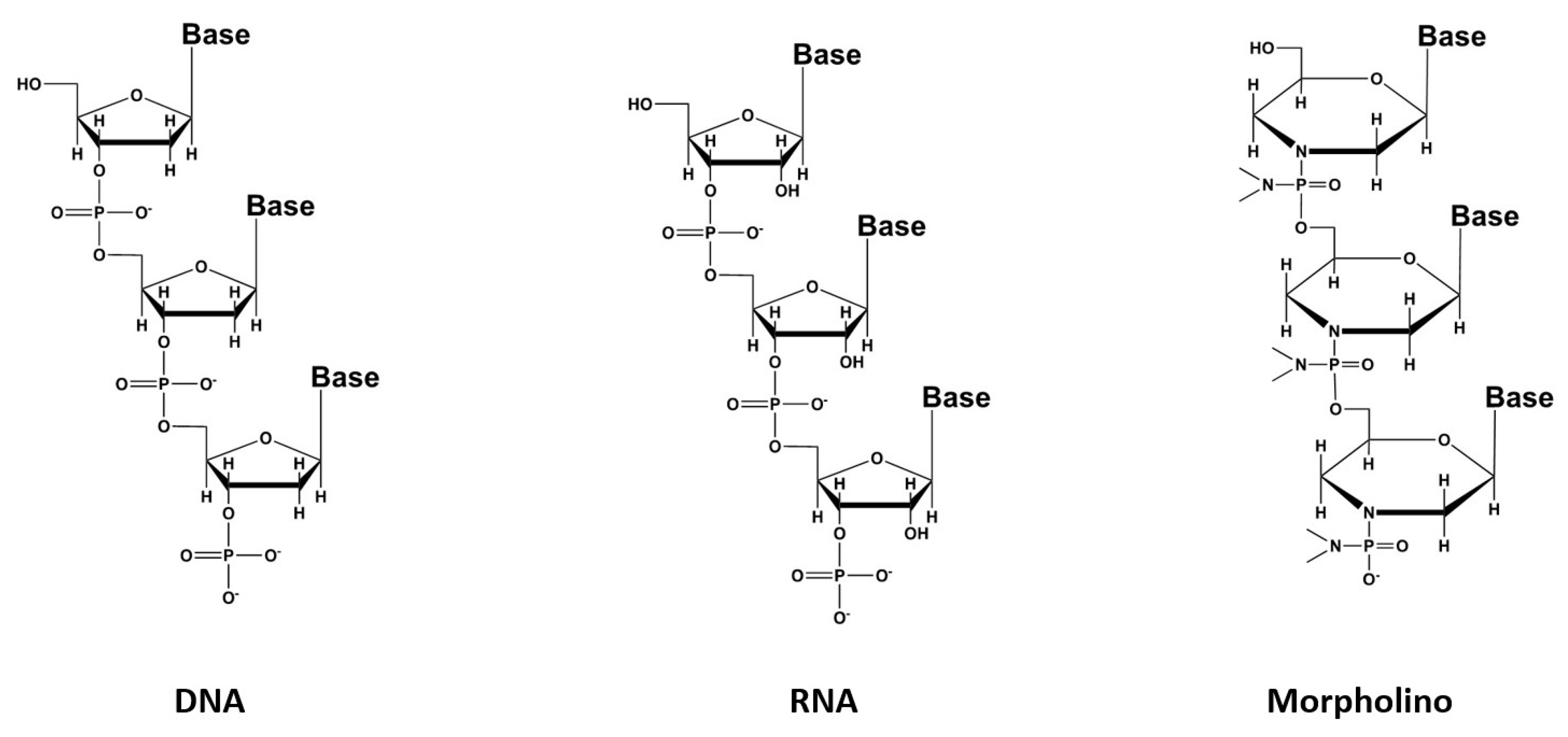
Figure 6.
CXCR4-targeting peptide derivatives. R = H: Pentixafor®, R = I: Pentixather®.
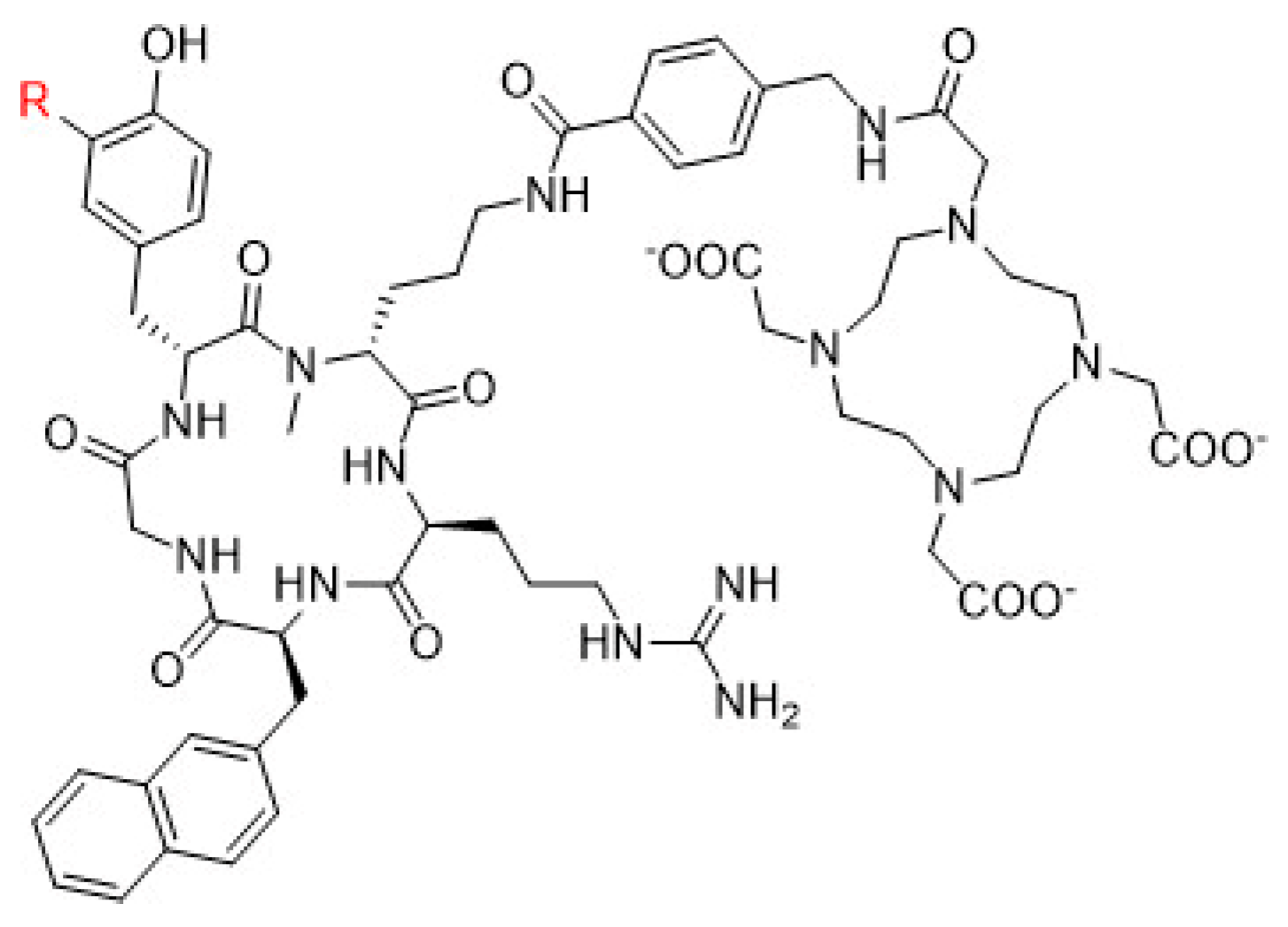
Figure 7.
PSMA-I&T (left)and PSMA-617 (right) structures.
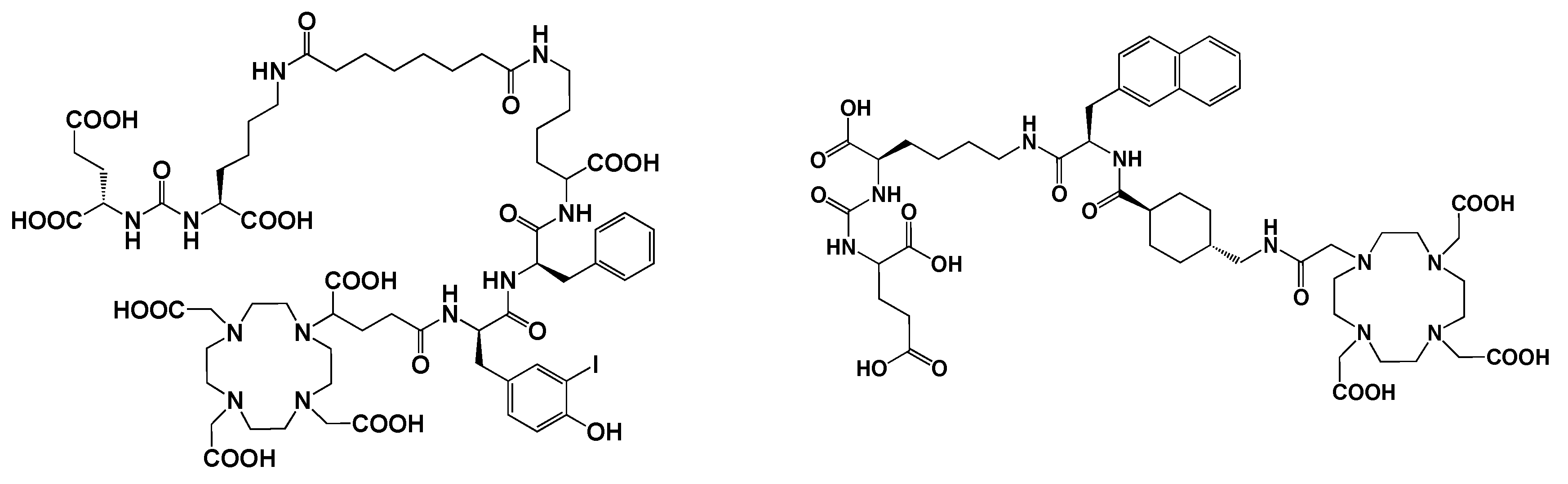
Figure 8.
FAP inhibitors of interest for targeted radionuclide therapy.
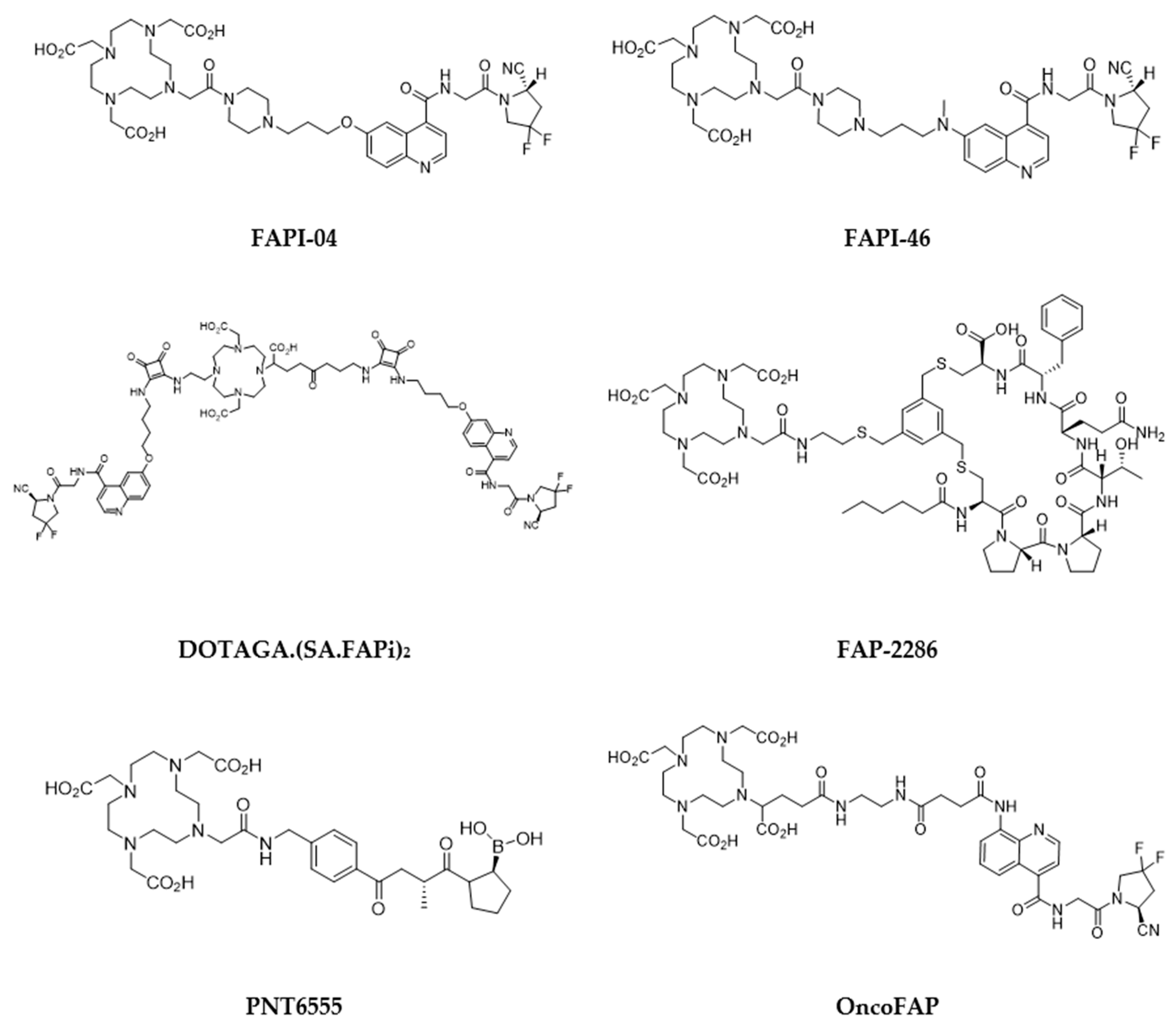
Figure 9.
Vitamins of interest as receptor-specific targeting agents.
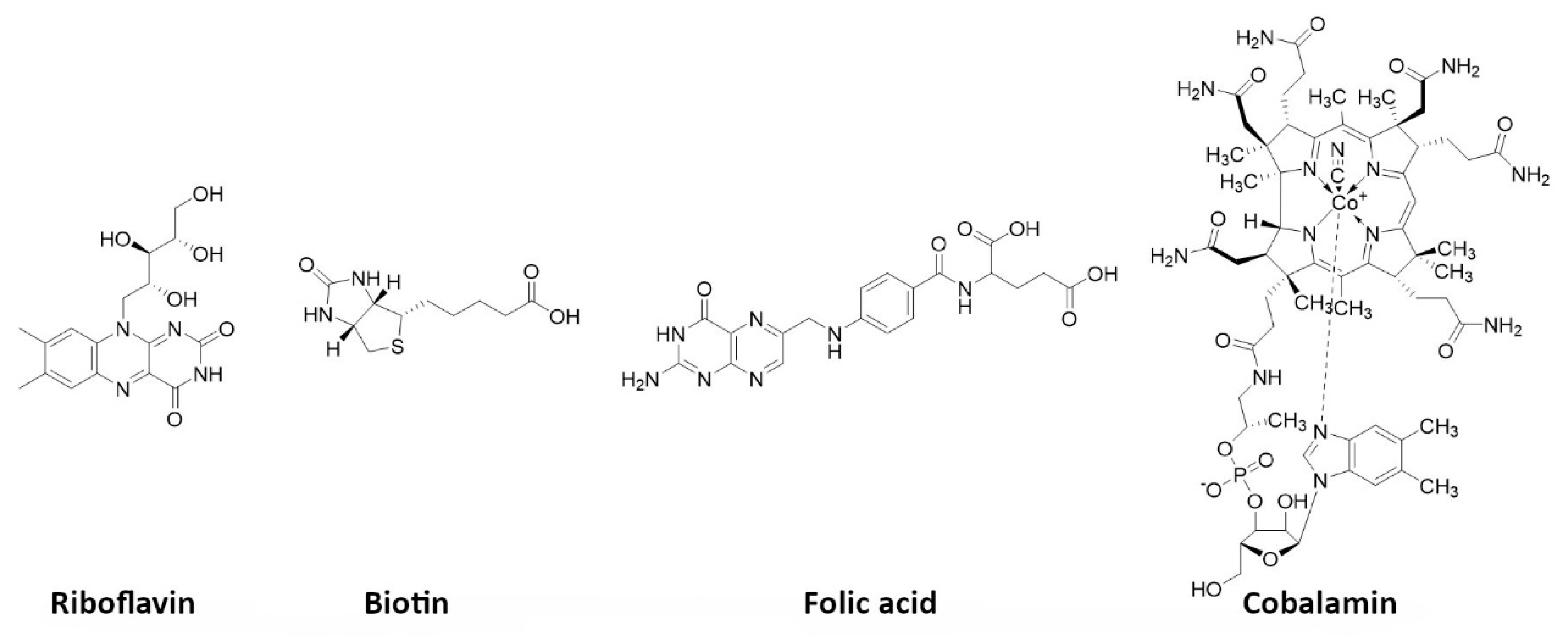
Figure 10.
Proposed binding mechanism of a benzamide derivative ([131I]ICF01012) with melanin fragment (adapted from [252]).
Figure 10.
Proposed binding mechanism of a benzamide derivative ([131I]ICF01012) with melanin fragment (adapted from [252]).
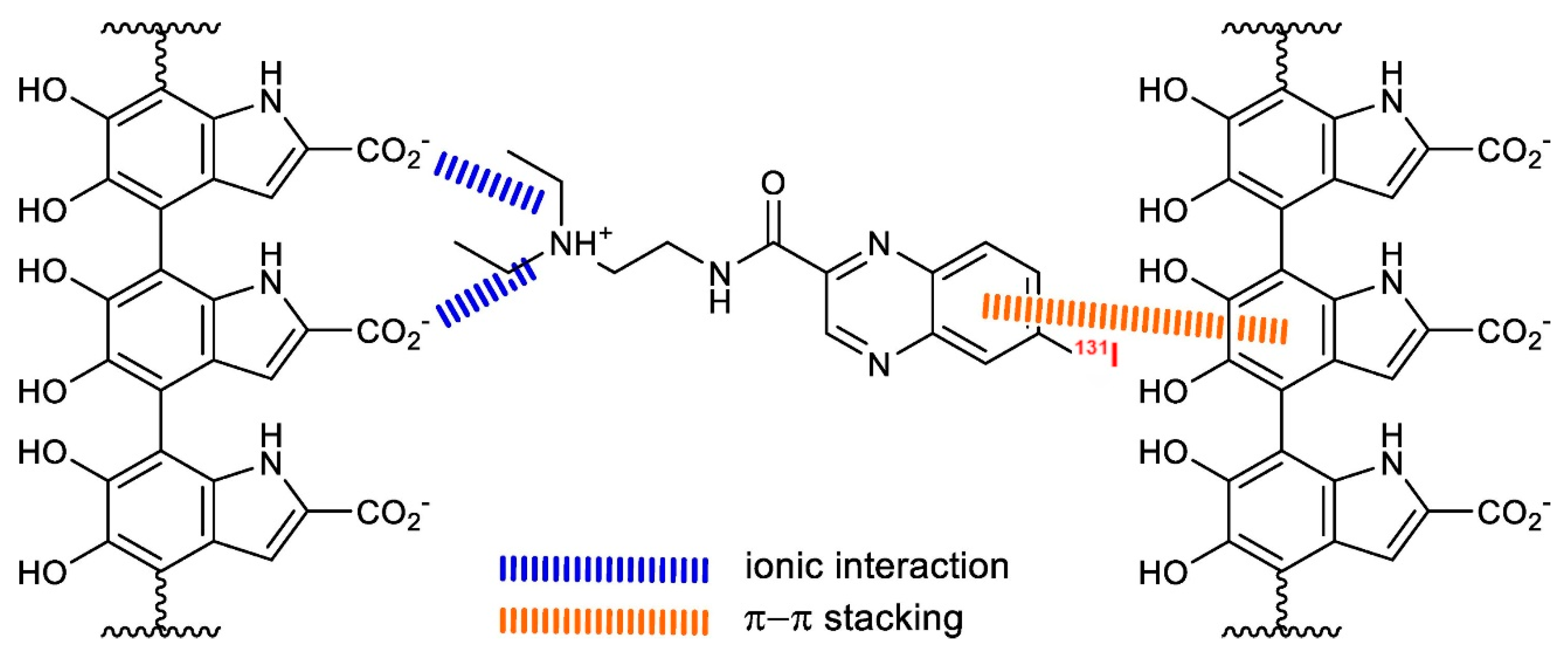

Table 1.
Main radionuclides used in therapy.
| Radionuclide | Half-life | Energy (MeV) | Eγ (keV) | Tissue penetration range (mm) |
| β-emitter | ||||
| 90Y | 2.7 days | 2.284 | / | 12 |
| 131I | 8 days | 0.81 | 0.364 | 2.4 |
| 161Tb | 6.9 days | 0.593 | 74.6 | 3 |
| 177Lu | 6.7 days | 0.497 | 208113 | 2.2 |
| 188Re | 17 hours | 2.118 | 155 | 11 |
| α-emitter | ||||
| 149Tb | 4.1 hours | 3.97 | Multiple emissions (165-800) | < 100 µm |
| 211At | 7.2 hours | 7.45 | 85 (X-Ray) | |
| 212Pb | 10.6 hours | 8.78 | 238, 300 | |
| 213Bi | 0.8 hours | 8.38 | 440 | |
| 223Ra | 11.4 days | 5.71, 6.82, 7.39, 6.62 | 270 | |
| 225Ac | 10 days | 5.8, 6.3, 7.1, 8.38 | 218, 440 (from daughters) | |
| 227Th | 18.7 days | 6.14, 5.71, 6.82, 7.39, 6.62 | 236 | |
| Auger e- emitter | ||||
| 111In | 2.8 days | 0.007 | 405 | < 1 µm |
| 125I | 60 days | 0.019 | 42 |
Table 2.
Peptides suitable for tumor targeting: their receptors (in bold, receptor types overexpressed in human) and tumor expression.
Table 2.
Peptides suitable for tumor targeting: their receptors (in bold, receptor types overexpressed in human) and tumor expression.
| Peptide | Receptor | Tumor expression |
| α-Melanocyte-stimulating hormone | MCR1, MCR3, MCR5 | Melanomas |
| Bombesin/Gastrin-releasing peptide | BB1, BB2 (GRPR), BB3, BB4 | Glioblastomas, prostate, breast, pancreatic, gastric, colorectal cancers, small cell lung |
| Cholecystokinin/gastrin | CCK1, CCK2 | Adenomas, astrocytomas, gastrointestinal and ovarian stromal tumors, medullary thyroid, pancreatic and small cell lung cancers |
| Epidermal Growth Factor | EGFR | Breast cancer |
| Exendin | GLP-1 | Gastrinomas, insulinomas,medullary thyroid carcinomas, paragangliomas and pheochromocytomas |
| Gonadotropin-releasing hormone | GnRH-R | Breast and prostate cancers |
| Neuropeptide Y | Y1, Y2, Y4, Y5 | Breast, ovary, adrenal, brain, kidney, GI-tract, bone (Ewing’s sarcoma) |
| Neurotensin | NTR1, NTR2, NTR3 | Breast, colon, pancreatic, prostate, small cell lung cancers, meningiomas |
| RGD | αVβ3 integrin | Tumor-induced angiogenesis |
| SDF-1α/CXCL12 | CXCR4, CXCR7 | Leukemias, lymphomas, melanomas, brain, breast, kidney, lung, ovarian, pancreas, prostate tumors |
| Somatostatin | Sstr1, sstr2, sstr3, sstr4, sstr5 | Neuroendocrine tumors, lymphomas, paragangliomas, brain, breast, renal, small cell lung cancers |
| Substance P | NK1, NK2, NK3 | Glial tumors, breast, medullary thyroid, pancreas, small cell lung cancers |
| Vasoactive intestinal peptide | VPAC1, VPAC2 | Bladder, breast, gastrointestinal, non-small cell lung, ovarian, pancreatic, prostate cancers |
Table 3.
Peptidic sequences of mainly clinical used somatostatin agonist analogs.
| Peptide | Peptidic Sequence |
| OC Octreotide |
d-Phe-cyclo(Cys-Phe-d-Trp-Lys-Thr-Cys)Thr(ol) |
| LAN Lanreotide |
β-d-Nal-cyclo(Cys-Tyr-d-Trp-Lys-Val-Cys)Thr-NH2 |
| VAP Vapreotide |
d-Phe-cyclo(Cys-Phe-d-Trp-Lys-Val-Cys)Trp-NH2 |
| TOC [Tyr3]-Octreotide |
d-Phe-cyclo(Cys-Tyr-d-Trp-Lys-Thr-Cys)Thr(ol) |
| TATE [Tyr3]-Octreotate |
d-Phe-cyclo(Cys-Tyr-d-Trp-Lys-Thr-Cys)Thr |
| NOC [1-Nal3]-Octreotide |
d-Phe-cyclo(Cys-1-Nal-d-Trp-Lys-Thr-Cys)Thr(ol) |
| SOM230 Pasireotide |
Cyclo(Hyp(Unk)-Phg- d-Trp-Lys-Tyr(Bn)-Phe) |
| P2045 Tozaride |
Ser-Thr-Cys(Trt)-Phe(4-NH2)-(β-DAP)-CH2CO-S-cyclo((N-Me)HCy-Phe-Tyr-d-Trp-Lys-Thr) |
Table 4.
Main antagonists currently investigated.
| Target | Name | Structure |
|---|---|---|
| SSTR | DOTA-BASS |  |
| DOTA-LM3 |  |
|
| DOTA-JR11 (Satoreotide) | 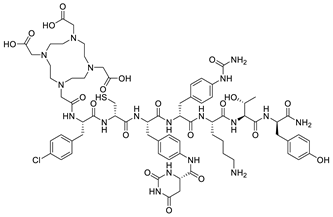 |
|
| GRPR | DOTA-RM2 | 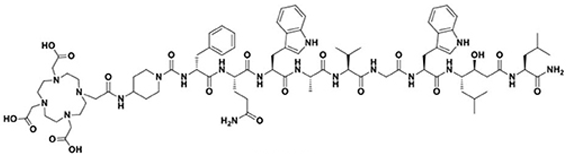 |
| NeoB | 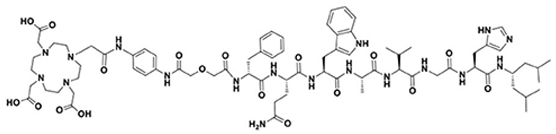 |
|
| NTR | 3BP-227 | 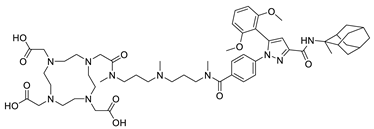 |
Table 5.
Radiotherapeutic bone-seeking agents.
| Radionuclide | Agent |
|---|---|
| Approved Agents for Clinical Use | |
| Strontium-89 (β-) (50.5 d) | [89Sr]SrCl2 – Metastron® |
| Samarium-153 (β-) (1.9 d) | EDTMP – Quadramet® |
| Rhenium-186 (β-) (3.7 d) | HEDP |
| Radium-223 (α) (11.4 d) | [223Ra]RaCl2 – Xofigo® |
| Agents in Clinical Trials | |
| Rhenium-188 (β-) (17 h) | HEDP Zoledronic acid |
| Lutetium-177 (β-) (6.8 d) | EDTMP DOTMP* Zoledronic acid (Dotazol) |
| Holmium-166 (β-) (1.1 d) | DOTMP* |
| Tin-117m (CE) (13.6 d) | DTPA** |
* DOTMP = 1,4,7,10tetraazacyclododecanetetramethylenephosponic acid. **DTPA = diethylenetriaminepentaacetic acid.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



