
Submitted:
09 May 2023
Posted:
10 May 2023
You are already at the latest version
Abstract
The aim of the research presented here is to assess the magnitude of the burden of health limitations resulting from air pollution on the world's economies. This burden was determined by the estimated number of premature years of life lost (YLLs) or health lost (YLDs) due to air pollution-related diseases in the working-age population. Attention was drawn to the problem of existing inequalities in the global burden of national economies with different income levels. The hypothesis of a persistently high level of inequality was verified on the basis of an analysis of the convergence process in a group of 204 countries over the period 1990-2019. The results obtained indicate a strong variation in the level of health constraints caused by air pollution. The analysis of the catch-up process of the least advantaged countries (highest level of health constraints due to air pollution) did not show a positive convergence effect in the study group.
Keywords:
air pollution
; disease burden
; YLLs
; YLDs
; health inequalities
; productivity loss
1. Introduction
Air pollution issues must now be seen not only as an environmental problem. By generating a large global burden of disease, it must also be considered in economic terms. Although the consequences of poor air quality are particularly evident among the elderly (as a result of long-term exposure), the measurable effects of the burden of this risk factor can also be estimated for the working-age population. In terms of economic (social) costs, years of health and life lost prematurely due to illness or death significantly reduce the human resource potential of an economy [1,2,3], representing a source of its lost productivity [4,5,6,7]. There is epidemiological evidence that pollution particles with a diameter of less than 2.5 (PM2.5) represent an extremely hazardous factor for human health [8], indicating the need to study the impact of air pollution on morbidity and mortality, also in terms of the so-called indirect costs of disease. Reduced physical and mental fitness is now identified as one of the main causes of inactivity among people of working age [9,10], and the mechanisms by which health affects economic productivity are the subject of numerous studies [11,12,13,14]. Although air pollution is commonly associated with areas of high production intensity, data on morbidity and mortality due to this risk factor indicate that the burden of disease due to air pollution is greatest in low- and middle-income countries [15]. It is in the lowest-producing countries that air pollution is now one of the major (or main) risk factors for the burden of disability or premature death.
The aim of the research presented here is to assess the magnitude of the burden of health limitations resulting from air pollution on the world's economies. This burden was determined by the estimated number of years of life lost prematurely (YLLs) or health lost (YLDs) due to air pollution-related diseases in the working-age population. The analysis used Institute for Health Metrics and Evaluation (IHME) data from the Global Burden of Disease Study 2019 (GBD 2019) [16]. Attention was drawn to the problem of existing inequalities in the level of global burden on national economies determined by their income levels. The hypothesis of persistently high levels of inequality was verified on the basis of an analysis of the convergence process in a group of 204 countries over the period 1990-2019.
Observations on the global burden of disease due to environmental risk factors indicate that mortality rates due to air pollution tend to increase as countries, through increased industrialisation, move from low to middle income levels [17]. Once a country reaches a higher level of development, these rates again reach lower levels as both air quality and access to health care improve. In contrast, the phenomenon of exponential increases in air pollution with increasing industrialisation in middle-income countries results in the highest mortality from this risk factor in this group of countries in many studies. The concept of unequal burden of the effects of air pollution is based on the relationship between income inequality and economic development, put forward by Simon Kuznets in 1955 [18]. This is the so-called Environmental Kuznets Curve (EKC), which is often used to describe the relationship between economic growth and environmental quality. It refers to the hypothesis that there is an inverted U-shaped relationship between the value of output per capita and certain measures of environmental quality. The EKC thus describes a hypothetical relationship between various indicators of environmental degradation and the level of per capita income. During the initial phase of a country's economic growth, emissions increase and environmental quality deteriorates, but above a certain level of income per capita (different for different environmental indicators) this trend reverses, resulting in an improvement in the environment at high income levels [19]. It should therefore be assumed that the level of environmental burden can be expressed as an inverted U-shaped function of per capita income. According to the EKC concept, the condition for environmental improvement is therefore an increase in income, which can then be translated into effective environmental policies. In the literature, the model has seen numerous proposals for modifications regarding the relationship between environmental parameters and economic growth, revealing potential mechanisms for adaptation of emission reduction practices that may deviate significantly from the theoretical assumptions of the EKC model [20,21,22].
Ambient and domestic air pollution is currently a key global health problem, contributing to approximately 7 million (potentially preventable) deaths per year, reduced life expectancy and significant direct and indirect social costs [23,24]. Currently, air pollution is a major environmental risk factor for premature deaths and is responsible for significant morbidity with short- and long-term health consequences [25]. Analyses of the association between ambient air pollution and cerebrovascular [25,26,27,28], neurological [29,30,31] and psychiatric [32,33,34] disorders are widely presented in the literature. Exposure to various forms of air pollutants, especially fine particulate matter that easily enters the body, can potentially contribute to stroke, dementia, Parkinson's disease, cognitive impairment and neurodevelopmental disorders [35,36]. Evidence of a positive correlation between high ambient PM 2.5 levels and the occurrence of depression has also been revealed [37]. Inflammation and oxidative stress are considered to be central pathophysiological mechanisms through which air pollution causes brain damage [38]. Due to an increase in clotting factors and platelet activation, it also creates conditions for thrombus formation [39]. At the same time, studies confirm a strong association between air pollution and cardiovascular morbidity and mortality [40,41].
As a result of the indicated multifaceted impact on the human body, air pollution is now a major contributor to the burden of disease worldwide. In 2019, 6.67 million deaths were attributed to this risk factor, accounting for 11.8% of all deaths. Of this number, 4.1 million deaths (more than 61%) were specifically attributed to outdoor air pollution. According to data from the Institute for Health Metrics and Evaluation (IHME) published in the Global Burden of Disease Study 2019 [16], air pollution (outdoor and indoor) is the fourth most common risk factor in terms of intensity of exposure ending in death, after hypertension, smoking and poor diet. It is also one of the main causes of the burden of non-communicable diseases (NCDs), primarily ischaemic heart disease, stroke, lower respiratory tract infections and chronic obstructive pulmonary disease. Air pollution is the fourth most important risk factor (after malnutrition, high blood pressure and smoking) contributing to the global burden of disease as measured by the number of healthy life years lost due to death or disability. According to IMHE estimates, air pollution contributed to 213.3 million healthy life years lost due to premature death or disability in 2019. This represents 17.5% of the global burden of disease generated by all risk factors combined.
Over the period 1990-2019, the global average total air pollution mortality rate fell from 121.5 to 86.2 deaths per 100,000 people, with the decline mainly due to improvements in indoor air quality (the indoor air pollution mortality rate fell from 81.5 to 29.9 deaths per 100,000 people). During this period, the mortality rate due to ambient (outdoor) air pollution increased from 38.3 to 53.5 deaths per 100 000 people, now accounting for more than 62% of the total burden of premature death due to air pollution [16]. The same data show a persistent burden attributed to ozone air pollution over the study period. The estimated burden of premature mortality due to exposure to this risk factor increased from 3.4 in 1990 to 4.7 deaths per 100 000 people in 2019. Consistent with the reduction in mortality, the contribution of airborne ozone to the global air pollution burden increased from 2.8 to 5.5 per cent over this period.
2. Materials and Methods
Institute for Health Metrics and Evaluation (IHME) data from the Global Burden of Disease Study 2019 were used to assess the magnitude of the burden of disease caused by air pollution on working-age populations in 204 countries worldwide [16]. The spatial distribution of the burden was assessed by taking as a measure indicators representing the number of life years lost (YLLs) and the number of potential years of life with disability (YLDs) following diseases associated with exposure to air pollution. The level of burden measures was adopted based on methodologies proposed in the literature to assess the phenomenon under study [42,43,44]. The approach adopted makes it possible to estimate the potentially lost effective working time of people of working age, while also indicating the degree of burden of disease caused by a given risk factor on national economies. In the GBD 2019 study, three groups of pollutants were considered in estimating the level of air pollution, i.e. (1) ambient particulate pollution taken as the annual average daily exposure to outdoor concentrations of particulate matter with aerodynamic diameter ≤2. 5 μm (PM2.5), (2) household air pollution (NDS) from solid fuels taken as the individual exposure to indoor PM2.5 concentrations due to the use of solid fuels for cooking and heating, and (3) ozone air pollution. Due to the objective of the study, the variables analysed were aggregated for the population aged 20-54 years, taking this age range as the one characterised by maximum productivity. Comparability of data between countries was achieved through intensity ratios relating to the number of observed cases per population size (rate). Statistical measures were used to determine the level of variation in the parameters analysed across the study group of 204 countries.
Estimating the level of disease burden resulting from air pollution required simultaneous consideration of both the area-specific intensity of the risk factor (mainly PM2.5 in µg/m³, indoors and outdoors) and the sensitivity of individual diseases to long-term exposure to these factors. A set of risk curves created from GBD data [45] (Figure 1) indicates that chronic obstructive pulmonary disease is particularly sensitive to increases in PM2.5 intensity. In this case, the level of relative risk (RR) burden increases practically linearly reaching RR=5.6 at a potential PM2.5 concentration of 600 µg/m³. This means that the probability of adverse effects of chronic obstructive pulmonary disease (loss of life or health) in a person with long-term exposure to this level of PM2.5 is more than 5.5 times higher than in a person not exposed to this risk factor. A significant increase in the relative risk level with increasing PM2.5 concentrations in m3 is also evident for ischaemic heart disease - in this case, with long-term exposure to PM2.5 at 600 µg/m³, the RR increases to 3.2. For the burden of diseases such as strokes, type 2 diabetes, tracheal, bronchial and lung cancers and lower respiratory tract infections, an intense increase in relative risk is seen at initial exceedances of the safe exposure standards, while exceedances of 100 µg/m³ no longer have a significant effect on the increase in risk. In the case of stroke, long-term exposure to PM2.5 concentrations on the order of 90 µg/m³ creates more than 3.5 times the likelihood of a person exposed to such exposure becoming ill or dying compared to those without exposure (RR=3.6).
GBD 2019 summary exposure value (SEV) data [45] simultaneously indicate a decreasing global exposure to total air pollutants over the last 30 years (Table 1), with the decrease determined by a significant reduction in exposure to household air pollution from solid fuels. For risk factors such as ambient particulate matter pollution and ambient ozone pollution, total exposure has increased.
Currently, air pollution levels are characterised by large differences in severity across regions and countries. A greater burden of air pollution is observed in low- and middle-income countries, and the reasons for this are both the high indoor pollution rates characteristic of low-income countries (due to reliance on solid fuels for cooking and heating) on the one hand, and the increasing levels of outdoor air pollution as developing countries become more industrialised on the other [46]. Global data on air pollution levels confirm the inequalities that still exist in this area. Indeed, high average PM2.5 concentrations mainly affect African and Asian countries (Figure 2). Countries with the highest average PM2.5 concentrations include India (83 µg/m³), Niger (80 µg/m³), Nigeria (70 µg/m³) and Egypt (68 µg/m³). The values recorded there are almost twice as high as the global average and more than 500% above the average value for the European region. Between 1990 and 2019, while the European area saw a decrease of almost 30% in PM2.5 pollution levels, the intensity of this risk factor increased by 9% in the Asian area. In the case of the Indian area, this was an increase of 16%. However, the largest increase in PM2.5 intensity (43% increase) was recorded in Mongolia.
An analysis of the relationship between a country's level of income (GDP per capita) and the average level of PM2.5 intensity (µg/m³) in its area shows that there is a persistent unfavourable relationship worldwide between air pollution levels and national product levels. This means that a large proportion of countries with low production values (low GDP per capita) experience high levels of PM2.5 intensity (Figure 3). Over the period 1990-2019, the level of the correlation coefficient between the value of gross domestic output per capita and the intensity of PM2.5 in the air increased from -0.34 (1990) to -0.37 (2019), indicating a continuing stable trend in this regard.
According to IHME [16] data on the global burden of disease worldwide, in 2019, in the population aged 20-54 years, the average burden of disease resulting from long-term exposure to air pollution, as measured by the number of years of life and health lost due to these diseases (DALYs), was 1145.2 per 100,000 people in this age group. Taking into account the 204 global economies included in the study , this rate, depending on the country, ranged between 8672.6 (Solomon Islands) and 33.1 (Sweden). The key sources of air pollution burden in this age group were cardiovascular diseases (DALYrate=786.5), chronic respiratory diseases (DALYrate=108.7), diabetes and kidney disesse (DALYrate=102.4), respiratory infections and tuberculososos (DALYrate=84.1), and neoplasms (DALYrate=54.7).
A characteristic feature of the health burden caused by exposure to air pollution is the relatively high burden of premature mortality among those affected. The proportion of years of life lived with disability (YLDs) in relation to the total number of years of healthy life lost (DALYs) following exposure to air pollution in the population aged 20-54 years averaged 10.0%. In the study group, it ranged between 4.3% (Solomon Islands) and 39.3% (Norway). A key problem of the burden on the potential of people of working age is therefore the high mortality rate of those affected by air quality-determined diseases.
Over the period 1990-2019, the burden of premature mortality caused by air pollution managed to decrease significantly in the studied group of 204 countries - the average YLL(AP)rate decreased 1349.0 from 879.8 life years lost per 100,000 people aged 20-54 (the study also confirmed the statistical significance of these differences assuming α=0.05, Wilcoxon test results p=0.000). However, the values remained highly dispersed, which indicates persistent inequalities within the group (Figure 4). During the study period, the coefficient of variation of the YLL(AP)rate parameter increased from 81.0 to 100.4%. In contrast, the level of disability burden due to air pollution did not change significantly. The average YLD(AP)rate decreased from 144.6 to 143.0 life years lost per 100,000 people aged 20-54. The level of the coefficient of variation fell from 54.7 to 52.7 per cent over the period under review, indicating no apparent trend towards levelling out existing inequalities in this area (Table 2).
Given the demonstrated heterogeneity of the burden of air pollution and its variability over time, the assumed global convergence in the burden of lost productivity on national economies was measured separately for parameters based on estimates of the burden of premature death (YLL(AP)rate) and long-term disability (YLD(AP)rate) in the working-age population defined for the whole study. The expected effect of decreasing global inequalities in the level of the burden of the consequences of air pollution on the world's economies will be an apparent process of positive convergence consisting of a decrease over time in the average level of the indicators studied as their level of dispersion decreases. In assessing the system under study's progress towards equilibrium, the concept of beta (β) unconditional convergence, which takes into account different initial conditions and predicts that outliers catch up faster with respect to the target, and the concept of sigma (σ) convergence, defined as a decrease in dispersion in performance, was used. To verify the beta-convergence hypothesis using cross-sectional data, a model was used to explain the growth of the trait under study in each country (i=1....N) between period t0 and t0 +T using the initial value of the trait in each member country according to the formula:
where: yit - value of trait y in area i in period t; uit - random disturbance. The occurrence of beta-convergence is confirmed by the negative and statistically significant value of the estimator b:
A negative sign of the parameter b indicates the presence of beta convergence (convergence) between member countries.
The analysis assumes that beta convergence occurs in the study area if countries with an initially worse value of a given variable (the highest level of the YLL(AP)rate or YLD (AP)rate) catch up by showing a faster rate of transition to the expected state, i.e. the relation of the parameters y /yit0+Tit0 tends towards zero. The inclusion of absolute (unconditional) convergence in the study implies the assumption that all countries move towards the same long-run equilibrium state and reach this state at the same time. Countries with a worse initial position, however, have a longer way to go. The occurrence of sigma convergence implies the achievement of the expected reduction in the level of dispersion (dispersion) of the trait under study over time. In order to verify the hypothesis of the occurrence of sigma-convergence in the studied system, as a measure of the dispersion of the trait in question, the amount of variance from the population in period t (σt2) was taken according to the formula:
where: yit - value of trait y in area i, in period t, ȳt - arithmetic mean of trait yi (for i=1,...N countries) in period t.
It was assumed that sigma convergence would occur if the value of the adopted dispersion index at the end of the analysed period (t0+T ) was significantly lower than at the beginning (t0 ). Taking into account the specificity of the studied process (burden of the studied world economies with the consequences of diseases caused by air pollution), the expected positive effect of the convergence process is a decrease in the average level of the studied parameters over time ( along with a simultaneous decrease in the level of their dispersion (). The results obtained will allow the evaluation of the convergence pattern in the studied system.
3. Results
Preliminary analysis of the IHME data confirms the assumption of inequalities in the level of the global health burden of the consequences of air pollution observed also for the working-age population. This means that these people experience different levels of risk of morbidity and mortality due to air pollution depending on the level of economic development of the area. Consequently, most countries in Africa and Asia experience high levels of morbidity and mortality caused by exposure to air pollution, with a high contribution of this risk factor to the burden as measured by the number of healthy life years lost through death (YLLs) or disability (YLDs). The regional divide that exists in this respect is apparent, i.e. most countries in Europe, North America and Latin America represent areas with low levels of air pollution's contribution to total morbidity and mortality (Figure 5). In the study group of 204 countries, for the age group 20-54 years, the highest share of air pollution-related deaths in total deaths occurred in Solomon Islands (20.0%), Vanuatu (17.7%), Kuwait (17.6%) and Egypt (16.9%). In contrast, the smallest contribution of air pollution diseases to premature deaths was recorded in Finland (0.5%), Sweden (0.5%) Iceland (0.7%) and Estonia (0.7%). The highest contribution of air pollution to the burden measured by the number of years of disability for people in the 20-54 year old population was in Papua New Guinea (3.4%), Solomon Islands (3.4%) and Vanuatu (3.2%), while the lowest was in Iceland (0.09%), New Zealand (0.10%) and Sweden (0.11%).
According to IHME data on the global burden of disease in 2019 [16], depending on a country's level of economic development (as measured by the World Bank), the YLL(AP)rate (i.e. YLLs per 100,000 people) in the population aged 20-54 years varied between 219.4 (High Income group countries) and 1428.5 (Low Income group countries). The level of the YLD(AP)rate (i.e. YLDs per 100,000 people) in the population aged 20-54 years, during the study period, varied between 68.7 (High Income group countries) and 223.3 (Lower Middle Income group countries) (Table 3). The contribution of diseases caused by air pollution to the total number of years of life lost prematurely (YLLs) in the 20-54 age group varied between 3.1% (High Income group countries) and 9.5% (Lower Middle Income group countries). It should be noted that in the High and Upper Middle Income group of countries, this share has decreased significantly over the period 1990-2019 (Table 3). In the low-income countries (Lower Middle and Low Income group), the share of air pollution as a risk factor for premature death increased by more than 12% on average. For healthy life years lost (YLDs), the share of air pollution-related diseases in the total number of years lived with disability from all causes varied between 0.5% (High Income countries) and 2.0% (Lower Middle Income groups). Over the period 1990-2019, this share increased for the High Income countries (an increase of 3.4%) and decreased for the Middle and Low Income groups (a decrease between 3 and 5% depending on the income group).
The assessment of the correlation between the level of economic development and the level of the burden of consequences of diseases caused by air pollution confirms the existence of a relatively strong relationship between the indicated parameters in the studied group of 204 countries (Figure 6). The results show a clear correlation between the level of economic development of a country, measured by the value of GDP per capita, and the number of years of life (YLL(AP)rate) and health (YLD(AP)rate) lost due to air pollution. The relationships presented here confirm the unfavourable patterns observed globally - residents of countries with lower national product can statistically expect a higher burden of premature deaths and diseases caused by air pollution.
Relatively strong (r≥0.5) and statistically significant (p<0.05, for α=0.05) levels of negative correlation were obtained for both variable analyses (Table 4). The results obtained explain to some extent the reasons for the phenomenon of high air pollution burden in low-income economies . The statistically significant correlation (r = -0.37) shown between the level of national product (GDP per cap.) and the level of PM2.5 pollution in its area indicates that a large part of low-productivity economies are affected by higher levels of air pollution. At the same time, these results do not confirm the expected high level of positive correlation between PM2.5 intensity and the burden of disease consequences of this risk factor on national economies. This indicates that there are other determinants of this process, such as access to healthcare. In the case of the burden of premature mortality caused by air pollution on the economy (YLLrate) in the 20-54 age group, the correlation coefficient was only 0.28. There was a greater correlation between the intensity of exposure to PM2.5 and the burden of years of life with disability (YLDrate). In this case, the correlation coefficient was 0.56 (with static significance) (Table 4).
In order to assess the persistence of globally existing inequalities in the level of the burden of the consequences of air pollution on the world's economies, the correlation of the observed 1990-2019 rate of change in the parameters under study (%ΔY, 1990-2019) with their level in 2019 was additionally assessed. The correlation level obtained for the YLLrate parameter, r=0.46 (at p<0.05, for α=0.05), indicates the existence of a statistically significant, but not very strong, relationship between the current level of the burden of premature death due to air pollution and its rate of change over the study period. The results indicate that for a significant proportion of the countries studied, a high level of the burden indicator was matched by a higher rate of increase. This indicates that inequalities in the study group are perpetuated over time. In the case of the burden of the effects of air pollution as measured by the number of years of disability (YLDrate), the level of correlation between the relative increase over time and the current level of burden was 0.16, which does not confirm the existing relationships in this area.
In order to verify the hypothesis assuming the existence of beta-convergence in the studied process, an explanatory model of the growth of the studied characteristic in individual countries was used according to formula (1). Assuming different initial conditions for individual world economies determined by the level of the variables YLL(AP)rate and YLD(AP)rate in 1990, the rate of change of the analysed parameters in individual countries in the studied period (relation 2019/1990) was determined. It was assumed that in the case of countries with difficult initial conditions (high initial levels of variables), this relation should be as low as possible, indicating a rapid rate of decline of the parameter under study giving the effect of catching up with the group (beta convergence).
Estimated from formula (1), the regression models explaining the growth of the studied indicators determining the burden of premature death (YLLrate) or disability (YLDrate) due to air pollution-related diseases in the study group of 204 countries took the form:
- a)
- YLL (AP)rate variable:
- b)
- YLD variable (AP)rate:
The resulting linear regression results of the parameters studied are shown in Figure 7.
In the case of the YLL(AP)rate parameter, the regression results obtained show that the value of the b estimator is positive, indicating the absence of positive convergence effects within the group, despite a slight decrease in the degree of dispersion (variance) of the indicator under study between 1990 and 2019 (data in Table 2). This implies that disparities between the countries under study have decreased, but the observed lack of beta-convergence does not warrant further inference in this respect. The expected effects of convergence bringing the outlier economies (with the highest mortality burden) closer to the average values observed globally are not visible.
In the case of the YLD(AP)rate parameter, the regression results obtained indicate that the value of the b estimator is negative at -0.061 (at p=0.044, for α=0.05), which could indicate a slow convergence effect in the group (the so-called half-life index determined from it, however, indicates that at the rate of convergence determined, the current disparities would only be halved in the next 330 years). The level of variance of this variable has also decreased slightly over time (data in Table 2), confirming the slow levelling of disparities associated with the congregation process. However, the lack of a measurable decline in YLD(AP)rata over time in the studied group of world economies (the level of the variable declined by only 7% over the studied period 1990-2019), as well as the previously indicated small share of this burden in the total air pollution burden, does not provide a viable basis for inferring a reduction in global inequalities in the health burden of air pollution.
The estimated regression model explaining the incremental total burden of premature death and disability (DALYrate) due to air pollution-related diseases in the study group of 204 countries (Figure 8) took the form:
The results confirm that there is therefore no basis for inferring an ongoing process of convergence in the total health burden of air pollution worldwide. The parameter b (regression coefficient) is in this case positive b=0.1184 and statistically significant (p=0.0012, with an assumed α=0.05).
4. Discussion
Research findings presented in the literature indicate that adverse health effects of PM are strongly related to pollutant particle size, composition and concentration and may occur even if relative risk estimates indicate that pollutant parameters are within the designated range of values. The combination of species and diurnal variations in particulate mass and composition is also a key contributor to the toxicity of particulate air pollution [48]. In practice, measuring the relevant parameters and quantifying their health effects is a difficult task, as numerous additional external factors strongly influence human morbidity and mortality [49]. Identifying and correcting the influence of confounding factors remains a difficult task, even though scientific advances are providing new information on the toxicity of trace elements in ambient PM all the time [50,51]. It is to be expected that in the future, multi-element analysis will be necessary for PM determination, allowing the use of models to identify and partition pollutant sources [52,53]. On the other hand, a growing number of studies indicate that air pollution is more hazardous to human health than previously thought [54]. The currently established limit values for total mass concentrations of PM10 and PM2.5 are assumed to be indicators of potential risk to the environment and human health. The PM10 fraction is light enough to float in the air for long periods of time, so it can be transported over long distances; while PM2.5 is of particular health concern, as it is small enough to even enter the bloodstream through the lungs and cause severe disease [55]. In September 2021, the WHO published updated global air quality guidelines, with the new reference values being significantly lower for most air pollutants than in the previous guidelines. Annual average values for PM2.5 have been reduced from 10 to 5 μg/m3 , for PM10 from 20 to 15 μg/m3 , and for nitrogen dioxide from 40 to 10 μg/m3 [56].
Air pollution is a key determinant of human wellbeing worldwide, and the impact of air pollution and socioeconomic position (SEP) on health is well documented in the literature. Research findings show that many socially disadvantaged communities, including in particular low-income and ethnic minority communities, are exposed to disproportionately high levels of air pollution and, due to the additional effects of material deprivation and psychosocial stress, are likely to be more susceptible to the health effects of these pollutants It should be emphasised, however, that the issue of assessing the socio-economic consequences of air pollution is particularly complicated because of the mechanisms that determine both the level of an area's exposure to environmental risk factors and its ability to protect society from their negative effects. Recent studies increasingly indicate that the level of air pollution burden is significantly determined by the socioeconomic position of those exposed and may play a key role in the epidemiology of disease and death [57]. As a consequence of the determinants indicated, it must be taken into account that a single variable, or a single index of several variables, cannot fully capture the mechanisms responsible for the cumulative health effects observed in specific communities following exposure to adverse environmental factors. However, many studies, for lack of other options, rely only on single measures of SES, e.g. income or educational attainment, without being able to consider the broader mechanisms through which SES may influence the relationship between air pollution and health.
The findings presented in this study are part of a trend in the literature concerning the unequal exposure of certain populations to environmental hazards and the disproportionate distribution of the effects of these hazards among populations [58,59,60,61,62]. At the same time, they relate to theories of environmental inequalities, allowing deeper insights into the pathways of SES effects on levels of health inequalities [63,64], as well as providing an analytical framework to develop studies of interactions between air pollution and social inequalities undertaken in the literature [65,66]. Indeed, it appears that groups with high SES, even when exposed to higher concentrations of air pollution, do not necessarily have a higher risk of illness or death. The findings presented in this paper confirm that, globally, a greater correlation can be observed between the level of gross domestic product than between the level of average exposure of an area and PM2.5. Socio-economic differences determining limited access to resources thus appear to be the common denominator underlying environmental inequalities.
The study of environmental inequalities, through its interdisciplinary nature, allows the use of a range of perspectives and tools appropriate to both the social and natural sciences and the health sciences. Economic inequalities and their consequences for health have long been the focus of research conducted by both economists and researchers from other disciplines concerned with population health. These researchers seek to understand the pathways by which socio-economic status is inversely correlated with indicators of health and illness. In their proposed models, people's characteristics are linked to various environmental exposures, access to and quality of healthcare [67,68,69,70]. These studies clearly confirm the influence of socioeconomic factors and air pollution on life expectancy [71,72].
Despite the remarkable popularity of the issues of social and environmental inequalities taken up in terms of health burdens, there is still a need to both seek answers and formulate proposals for solutions to this issue. Few studies in the area of environmental risks have even addressed changes in inequalities over time, which this study tries to fill to some extent. Essentially, its aim was to answer the question: if we assume that a global air protection policy has been pursued over the past few decades, has it succeeded in reducing the existing differences between countries in this area? The results of the present study do not provide a positive answer to this question, because, despite a decrease in the average air pollution burden measured in terms of years of life and health lost, there has been no convergence in this area, resulting in a decrease in the average differences between countries as the worse-off countries catch up with the better-off ones.
It should be emphasised that considerable progress has been made over the past decade in assessing the economic burden of air pollution [73,74], however, estimates based on indirect costs of disease are still subject to a high level of uncertainty. Indeed, there is still no consensus on appropriate methods for valuing both the value of life and the cost of air pollution mortality [75]. The economic effect of premature deaths is attempted to be assessed on the basis of, for example, the value of statistical life expectancy (VSL) [76], or the effect of pollution, mortality and disease on GDP growth rates [77]. This makes it difficult to objectively value the persistent inequalities in the health burden of air pollution between countries, as well as making it difficult to set public and environmental health priorities.
5. Conclusions
The economic cost of the health burden of air pollution varies significantly depending on the valuation methods adopted. In this study, the health burden was shown to be unevenly distributed globally, and correlated to a greater extent with the level of national product than with the actual level of an area's exposure to PM2.5 concentrations. This indicates that reducing the health burden of air pollution requires addressing two issues simultaneously, i.e.: reducing exposure to pollutants and improving overall health conditions and healthcare in low-income countries. The results did not positively verify the assumption of an ongoing process of positive convergence in the global burden of health consequences of air pollution. Despite the observed decline in the average values of the air pollution burden measured by the number of years of life and health lost over the period 1990-2019, a reduction in the average differences between countries was not achieved as countries with a worse situation (higher burden) caught up with countries with better performance.
By focusing the analysis on the working-age population, it was possible to simultaneously gain perspective on the so-called indirect costs of air pollution-related disease resulting from lost economic productivity. In the case of low-income economies, this reveals an existing mechanism for amplifying negative environmental effects, as even relatively minor increases in risk factors have serious health effects. At the same time, the results obtained go beyond the environmental aspect by presenting quantifiable possibilities for estimating the economic costs of air pollution in individual countries, taking into account the costs of lost economic productivity. The development of a counterfactual scenario involving the reduction or elimination of a risk factor in a given area is important in this case.
Data Availability Statement
Global Burden of Disease Collaborative Network. Global Burden of Disease Study 2019 (GBD 2019) Results. Seattle, United States: Institute for Health Metrics and Evaluation (IHME), 2020. Available from https://vizhub.healthdata.org/gbd-results/; Global Burden of Disease Collaborative Network. Global Burden of Disease Study 2019 (GBD 2019) Air Pollution Exposure Estimates 1990-2019. Seattle, United States of America: Institute for Health Metrics and Evaluation (IHME), 2021; Global Burden of Disease Health Financing Collaborator Network produced estimates for Gross Domestic Product (GDP) from 1960-2050. Estimates are reported as GDP per person in constant 2021 purchasing-power parity-adjusted (PPP) dollars. https://ghdx.healthdata.org/record/ihme-data/global-gdp-per-capita-1960-2050-fgh-2021.
Acknowledgments
In this section, one may acknowledge any support given which is not covered by the author contribution or funding sections. This may include administrative and technical support, or donations in kind (e.g., materials used for experiments).
Conflicts of Interest
The authors declare no conflict of interest.
References
- Cole, M.A.; Neumayer, E. The impact of poor health on total factor productivity. The Journal of Development Studies 2006, 42(6), 918-938. [CrossRef]
- William J.; Lewis, M. Health investments and economic growth: Macroeconomic evidence and microeconomic foundations; World Bank Policy Research Working Paper Series, 2009.
- Jakubowska, A.; Bilan, S.; Werbiński, J. Chronic diseases and labour resources: “Old and new” European Union member states. Journal of International Studies 2021, 14(1). [CrossRef]
- Bialowolski, P.; McNeely, E.; VanderWeele, T.J.; Weziak-Bialowolska, D. Ill health and distraction at work: Costs and drivers for productivity loss. Plos one 2020, 15(3), e0230562. [CrossRef]
- Zhang, W.; Sun, H. How to analyze work productivity loss due to health problems in randomized controlled trials? A simulation study. BMC Med Res Methodol 2021, 130. [CrossRef]
- Krol, M.; Brouwer, W. How to estimate productivity costs in economic evaluations. Pharmacoeconomics 2014, 32, 335-344. [CrossRef]
- Yoshimoto, T.; Oka, H.; Fujii, T.; Nagata, T.; Matsudaira, K. The Economic Burden of Lost Productivity due to Presenteeism Caused by Health Conditions Among Workers in Japan. J Occup Environ Med. 2020, Oct;62(10):883-888. PMID: 32826548; PMCID: PMC7537733. [CrossRef]
- Miller, M.R.; Shaw, C.A.; Langrish, J.P. From particles to patients: oxidative stress and the cardiovascular effects of air pollution. Future Cardiol 2012, Jul;8(4):577-602PMID: 22871197. [CrossRef]
- Van Rijn, R.M.; Robroek, S.J.; Brouwer, S.; Burdorf, A. Influence of poor health on exit from paid employment: a systematic review. Occupational and environmental medicine 2014, 71(4), 295-301. [CrossRef]
- Rice, N.E.; Lang, I.A.; Henley, W.; Melzer, D. Common health predictors of early retirement: findings from the English Longitudinal Study of Ageing. Age Ageing 2011, 40(1), 54-61. [CrossRef]
- Brouwer, W.; Verbooy, K.; Hoefman, R. et al. Production Losses due to Absenteeism and Presenteeism: The Influence of Compensation Mechanisms and Multiplier Effects. PharmacoEconomics 2023. [CrossRef]
- Bloom, D.E.; Canning, D.; Fink, G. Disease and development revisited. Journal of Political Economy 2014, 122(6), 1355-1366. [CrossRef]
- Abegunde, D.; Stanciole, A. An estimation of the economic impact of chronic noncommunicable diseases in selected countries, Working paper; WHO Department of Chronic Diseases and Health Promotion, CHP, 2006.
- Brown, S.; Sessions, J.G. The economics of absence: theory and evidence. Journal of economic surveys 1996, 10(1), 23-53.
- GBD 2019 Risk Factors Collaborators. Global burden of 87 risk factors in 204 countries and territories, 1990-2019: a systematic analysis for the Global Burden of Disease Study 2019. Lancet 2020, Oct 17;396(10258):1223-1249. PMID: 33069327; PMCID: PMC7566194. [CrossRef]
- Global Burden of Disease Collaborative Network. Global Burden of Disease Study 2019 (GBD 2019) Results. Seattle, United States: Institute for Health Metrics and Evaluation (IHME), 2020. Available from https://vizhub.healthdata.org/gbd-results/.
- Stern, D.I. The environmental Kuznets curve. Companion to Environmental Studies 2018, 49(54), 49-54.
- Kuznets, S. Economic growth and income inequality. The American economic review 1955, 45(1), 1-28.
- Dinda, S. Environmental Kuznets curve hypothesis: a survey. Ecological economics 2004, 49(4), 431-455.
- Chen, J.; Hu, T.E.; Van Tulder, R. Is the environmental Kuznets curve still valid: a perspective of wicked problems. Sustainability 2019, 11(17), 4747. [CrossRef]
- Leal P.H.; Marques A.C. The evolution of the environmental Kuznets curve hypothesis assessment: A literature review under a critical analysis perspective. Heliyon. 2022 Nov 11;8(11):e11521. PMID: 36406679; PMCID: PMC9668524. [CrossRef]
- Ojaghlou, M.; Ugurlu, E.; Kadłubek, M.; Thalassinos, E. Economic Activities and Management Issues for the Environment: An Environmental Kuznets Curve (EKC) and STIRPAT Analysis in Turkey. Resources 2023, 12, 57. [CrossRef]
- Mannucci, P.M.; Franchini, M. Health Effects of Ambient Air Pollution in Developing Countries. Int. J. Environ. Res. Public Health 2017, 14, 1048. [CrossRef]
- Mannucci, P.M.; Harari, S.; Franchini, M. Novel evidence for a greater burden of ambient air pollution on cardiovascular disease. Haematologica 2019, Dec;104(12):2349-2357. [CrossRef]
- Roth, G.A.; Mensah, G.A.; Fuster, V. The Global Burden of Cardiovascular Diseases and Risks: A Compass for Global Action. J Am Coll Cardiol 2020, Dec 22;76(25):2980-2981. PMID: 33309174. [CrossRef]
- Rajagopalan, S.; Al-Kindi, S.; Brook R, et al. Air Pollution and Cardiovascular Disease. J Am Coll Cardiol. 2018 Oct, 72(17) 2054–2070. [CrossRef]
- Cai, J.; Yu, S.; Pei, Y.; Peng, C.; Liao, Y.; Liu, N.; Ji, J.; Cheng, J. Association between Airborne Fine Particulate Matter and Residents’ Cardiovascular Diseases, Ischemic Heart Disease and Cerebral Vascular Disease Mortality in Areas with Lighter Air Pollution in China. Int. J. Environ. Res. Public Health 2018, 15, 1918. [CrossRef]
- Sørensen, M.; Poulsen, A. H.; Hvidtfeldt, U. A.; Christensen, J. H.; Brandt, J.; Frohn, L. M.; ... & Raaschou-Nielsen, O. Effects of Sociodemographic Characteristics, Comorbidity, and Coexposures on the Association between Air Pollution and Type 2 Diabetes: A Nationwide Cohort Study. Environmental health perspectives 2023, 131(2), 027008. [CrossRef]
- Bandyopadhyay, A. Neurological Disorders from Ambient (Urban) Air Pollution Emphasizing UFPM and PM2.5 . Curr Pollution Rep 2016, 2, 203–211. [CrossRef]
- Kim, H.; Kim, W.H.; Kim, Y.Y.; Park, H.Y. Air pollution and central nervous system disease: a review of the impact of fine particulate matter on neurological disorders. Frontiers in Public Health 2020, 8, 575330. [CrossRef]
- Aldraihem, M.O.; Al-Ghamdi, F.; Murtaza, G. et al. Air pollution and performance of the brain. Arab J Geosci 2020, 13, 1158. [CrossRef]
- Buoli, M.; Grassi, S.; Caldiroli, A.; Carnevali, G.S.; Mucci, F.; Iodice, S.; ... & Bollati, V. Is there a link between air pollution and mental disorders?. Environment international 2018, 118, 154-168. [CrossRef]
- Khan, A.; Plana-Ripoll, O.; Antonsen, S.; Brandt, J.; Geels, C.; Landecker, H.; ... & Rzhetsky, A. Environmental pollution is associated with increased risk of psychiatric disorders in the US and Denmark. PLoS biology 2019, 17(8), e3000353. [CrossRef]
- Attademo, L.; Bernardini, F.; Garinella, R.; Compton, M.T. Environmental pollution and risk of psychotic disorders: A review of the science to date. Schizophrenia research 2017, 181, 55-59. [CrossRef]
- Hahad, O.; Lelieveld, J.; Birklein, F.; Lieb, K.; Daiber, A.; Münzel, T. Ambient Air Pollution Increases the Risk of Cerebrovascular and Neuropsychiatric Disorders through Induction of Inflammation and Oxidative Stress. Int. J. Mol. Sci. 2020, 21, 4306. [CrossRef]
- Wang, Y.; Duong, M.; Brauer, M.; Rangarajan, S.; Dans, A.; Lanas, F., ... & Hystad, P. Household Air Pollution and Adult Lung Function Change, Respiratory Disease, and Mortality across Eleven Low-and Middle-Income Countries from the PURE Study. Environmental Health Perspectives 2023, 131(4), 047015. [CrossRef]
- Rajkumar, R.P. The Relationship between Ambient Fine Particulate Matter (PM2.5) Pollution and Depression: An Analysis of Data from 185 Countries. Atmosphere 2023, 14, 597. [CrossRef]
- Migliore, L.; Coppedè, F. Environmental-induced oxidative stress in neurodegenerative disorders and aging. Mutation Research/Genetic Toxicology and Environmental Mutagenesis 2009, 674(1-2), 73-84. [CrossRef]
- Argacha, J.F.; Bourdrel, T.; van de Borne, P. Ecology of the cardiovascular system: A focus on air-related environmental factors. Trends Cardiovasc Med 2018, Feb;28(2):112-126. [CrossRef]
- Franchini, M.; Mannucci, P.M. Thrombogenicity and cardiovascular effects of ambient air pollution. Blood 2011, Sep 1;118(9):2405-12. Epub 2011 Jun 10. PMID: 21666054. [CrossRef]
- Laden, F.; Schwartz, J.; Speizer, F.E.; Dockery D.W. Reduction in fine particulate air pollution and mortality: Extended follow-up of the Harvard Six Cities study. Am J Respir Crit Care Med 2006, Mar 15;173(6):667-72. Epub 2006 Jan 19. PMID: 16424447; PMCID: PMC2662950. [CrossRef]
- Williams, A., Calculating the global burden of disease: time for a strategic reappraisal?, Health economics 1999, 8(1), 1-8.
- Łyszczarz, B.; Sowa, K. Production losses due to mortality associated with modifiable health risk factors in Poland. The European Journal of Health Economics 2022, 23(1), 33-45. [CrossRef]
- Mahrouseh, N.; Chen-Xu, J.; Charalampous, P.; Eikemo, T.; Varga, O.; Grad, D.; ... & Baravelli, C. Premature mortality and levels of inequality in years of life lost across 296 regions of 31 european countries in 2019: A burden of disease study. Population Medicine 2023, 5. [CrossRef]
- Global Burden of Disease Collaborative Network. Global Burden of Disease Study 2019 (GBD 2019) Air Pollution Exposure Estimates 1990-2019. Seattle, United States of America: Institute for Health Metrics and Evaluation (IHME), 2021.
- Global Burden of Disease Health Financing Collaborator Network produced estimates for Gross Domestic Product (GDP) from 1960-2050. Estimates are reported as GDP per person in constant 2021 purchasing-power parity-adjusted (PPP) dollars. https://ghdx.healthdata.org/record/ihme-data/global-gdp-per-capita-1960-2050-fgh-2021.
- Ritchie, H.; Roser, M. Air Pollution. Published online at OurWorldInData.org. Retrieved from: https://ourworldindata.org/air-pollution [Online Resource], https://ourworldindata.org/air-pollution#citation.
- Davidson, C.I.; Phalen, R.F.; Solomon, P.A. Airborne particulate matter and human health: a review. Aerosol Science and Technology 2005, 39(8), 737-749. [CrossRef]
- Al-Kindi, S.G.; Brook, R.D.; Biswal, S. et al. Environmental determinants of cardiovascular disease: lessons learned from air pollution. Nat Rev Cardiol 2020, 17, 656–672. [CrossRef]
- Agibayeva, A.; Guney, M.; Karaca, F.; Kumisbek, A.; Kim, J.R.; Avcu, E. Analytical Methods for Physicochemical Characterization and Toxicity Assessment of Atmospheric Particulate Matter: A Review. Sustainability 2022, 14, 13481. [CrossRef]
- Hassan Bhat, T.; Jiawen, G.; Farzaneh, H. Air Pollution Health Risk Assessment (AP-HRA), Principles and Applications. Int. J. Environ. Res. Public Health 2021, 18, 1935. [CrossRef]
- Ogrizek, M.; Kroflič, A.; Šala, M. Critical review on the development of analytical techniques for the elemental analysis of airborne particulate matter. Trends in Environmental Analytical Chemistry 2022, e00155. [CrossRef]
- Lavigne, E.; Burnett, R.T.; Weichenthal, S. Association of short-term exposure to fine particulate air pollution and mortality: effect modification by oxidant gases. Sci Rep 2018, 8, 16097. [CrossRef]
- Carvalho, H.; New WHO global air quality guidelines: more pressure on nations to reduce air pollution levels. The Lancet Planetary Health 2021, 5(11), e760-e761. [CrossRef]
- Lelieveld, J.; Evans, J.; Fnais, M. et al. The contribution of outdoor air pollution sources to premature mortality on a global scale. Nature 2015, 525(7569), 367–371. [CrossRef]
- WHO global air quality guidelines. Particulate matter (PM2.5 and PM10), ozone, nitrogen dioxide, sulfur dioxide and carbon monoxide. Geneva: World Health Organization; 2021.
- O'Neill, M.S.; Jerrett, M.; Kawachi, I.; Levy, J.I.; Cohen, A.J.; Gouveia, N.; ... & Workshop on Air Pollution and Socioeconomic Conditions. Health, wealth, and air pollution: advancing theory and methods. Environmental health perspectives 2003, 111(16), 1861-1870. [CrossRef]
- Hajat, A.; Hsia, C.; O’Neill, M.S. Socioeconomic disparities and air pollution exposure: a global review. Current environmental health reports 2015, 2(4), 440-450. [CrossRef]
- Gouveia N. Addressing Environmental Health Inequalities. International journal of environmental research and public health 2016, 13(9), 858. Doi: 10.3390/ijerph13090858.
- Goodman, A.; Wilkinson, P.; Stafford, M. et al. Characterising socio-economic inequalities in exposure to air pollution: a comparison of socio-economic markers and scales of measurement. Health Place 2011, 17(3), 767–774. [CrossRef]
- Molitor, J.; Su, J.; Molitor, NT.; et al. Identifying vulnerable populations through an examination of the association between multi-pollutant profiles and poverty. Environ Sci Technol. 2011, 45(18), 7754–7760. [CrossRef]
- Jakubowska, A.; Rabe, M. Air Pollution and Limitations in Health: Identification of Inequalities in the Burdens of the Economies of the “Old” and “New” EU. Energies 2022, 15, 6225. [CrossRef]
- Grandjean, P.; Bellanger, M. Calculation of the disease burden associated with environmental chemical exposures: application of toxicological information in health economic estimation. Environ Health 16, 123 (2017). [CrossRef]
- Miranda, M.L.; Edwards, S.E.; Keating, M.H.; Paul, C.J. Making the Environmental Justice Grade: The Relative Burden of Air Pollution Exposure in the United States. Int. J. Environ. Res. Public Health 2011, 8, 1755-1771. [CrossRef]
- Fairburn, J.; Schüle, S.A.; Dreger, S.; Karla Hilz, L.; Bolte, G. Social Inequalities in Exposure to Ambient Air Pollution: A Systematic Review in the WHO European Region. Int. J. Environ. Res. Public Health 2019, 16, 3127. [CrossRef]
- Shen, W.; Srivastava, S.; Yang, L.; Jain, K.; Schröder, P. Understanding the impacts of outdoor air pollution on social inequality: Advancing a just transition framework. Local Environment 2020, 25(1), 1-17. [CrossRef]
- Santana, P.; Almendra, R.; Pilot, E.; Doreleijers, S.; Krafft, T. Environmental inequalities in global health. In: Handbook of Global Health; Kickbusch, I., Ganten, D., Moeti, M., Eds.; Springer, Cham,2021. [CrossRef]
- Spalt, E.W.; Curl, C.L.; Allen R.W. et al. Factors influencing time-location patterns and their impact on estimates of exposure: the Multi-Ethnic Study of Atherosclerosis and Air Pollution (MESA Air). J Expo Sci Environ Epidemiol 2016, Jun;26(4), 341-8. [CrossRef]
- Samet, J.M.. The environment and health inequalities: problems and solutions. Journal of Health Inequalities 2019, 5(1), 21-27. [CrossRef]
- Martinez, G.S.; Spadaro, J.V.; Chapizanis, D.; Kendrovski, V.; Kochubovski, M.; Mudu, P. Health Impacts and Economic Costs of Air Pollution in the Metropolitan Area of Skopje. Int. J. Environ. Res. Public Health 2018, 15, 626. [CrossRef]
- Yang, H.; Wang, S.; Ren, Z.; Liu, H.; Tong, Y.; & Wang, N. Life expectancy, air pollution, and socioeconomic factors: a multivariate time-series analysis of Beijing City, China. Social Indicators Research 2022, 162(3). 979-994. [CrossRef]
- Pu, H.; Wang, S.; Wang, Z. et al. Non-linear relations between life expectancy, socio-economic, and air pollution factors: a global assessment with spatial disparities. Environ Sci Pollut Res 2022, 29, 53306–53318. [CrossRef]
- Yin, H.; Brauer, M.; Zhang, J.; Cai, W.; Navrud, S.; Burnett, R.; ... & Liu, Z. Global economic cost of deaths attributable to ambient air pollution: Disproportionate burden on the ageing population. medRxiv 2020, 2020.04.28.20083576. [CrossRef]
- Conti, S.; Ferrara, P.; D'Angiolella, L. S.; Lorelli, S. C.; Agazzi, G.; Fornari, C.; ... & Mantovani, L. G. The economic impact of air pollution: a European assessment. European Journal of Public Health 2020, 30(Supplement_5), ckaa165-084. [CrossRef]
- Nair, M.; Bherwani, H.; Mirza, S.; Anjum, S.; Kumar, R. Valuing burden of premature mortality attributable to air pollution in major million-plus non-attainment cities of India. Sci Rep. 2021, Dec 2;11(1):22771. [CrossRef]
- Safari, Z.; Fouladi-Fard, R.; Vahedian, M. et al. Health impact assessment and evaluation of economic costs attributed to PM2.5 air pollution using BenMAP-CE. Int J Biometeorol 2022, 66, 1891–1902. [CrossRef]
- Maiti, M.; Jadhav, P. Impact of pollution level, death rate and illness on economic growth: evidence from the global economy. SN Bus Econ 1, 109 (2021). [CrossRef]
Figure 1.
Integrated exposure response curve for long-term exposure to PM2.5 - relative risk (RR) values as a function of total PM2.5 intensity. Source: own elaboration based on: [45].
Figure 1.
Integrated exposure response curve for long-term exposure to PM2.5 - relative risk (RR) values as a function of total PM2.5 intensity. Source: own elaboration based on: [45].
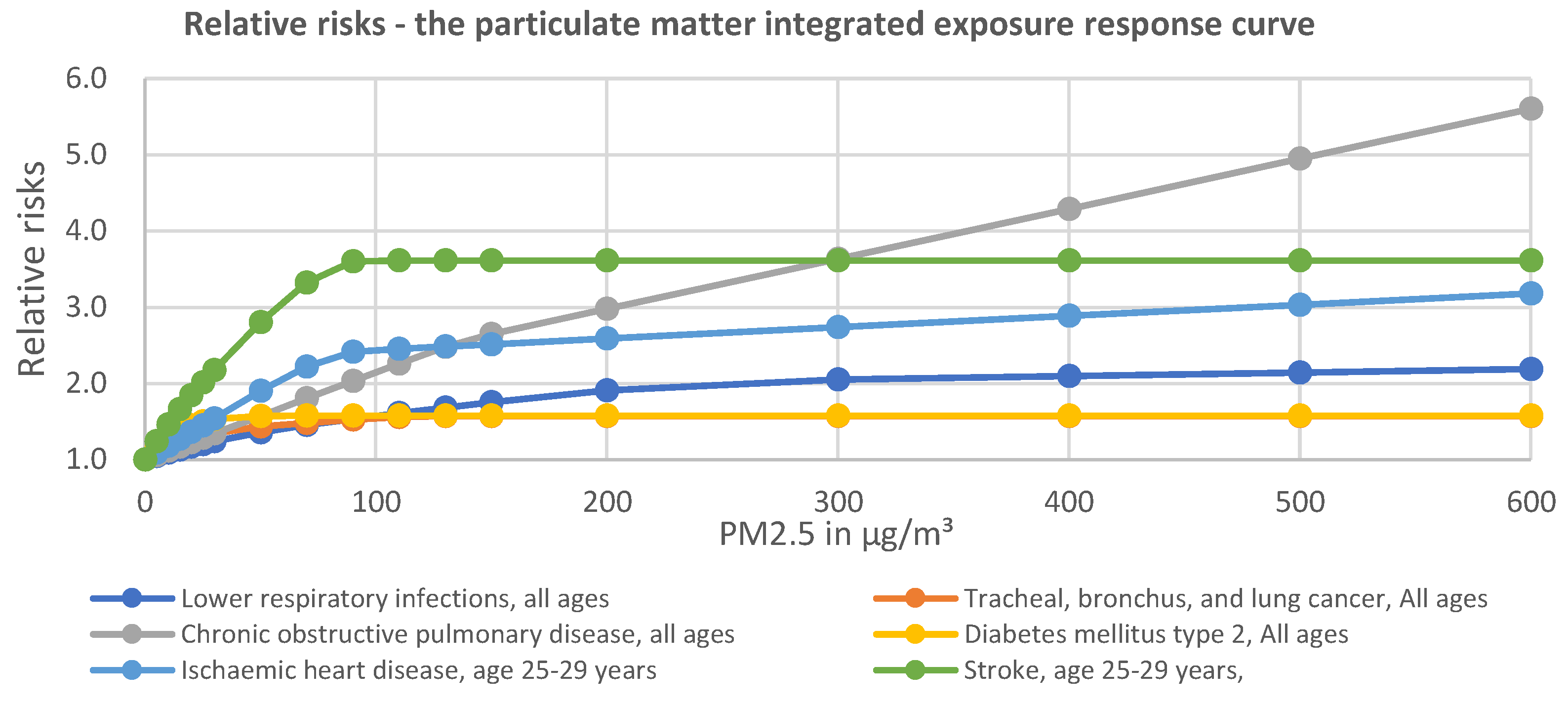
Figure 2.
Spatial distribution of PM2.5 levels in 2019 and change from 1990 to 2019, N=204. Source: own elaboration based on: [45].
Figure 2.
Spatial distribution of PM2.5 levels in 2019 and change from 1990 to 2019, N=204. Source: own elaboration based on: [45].
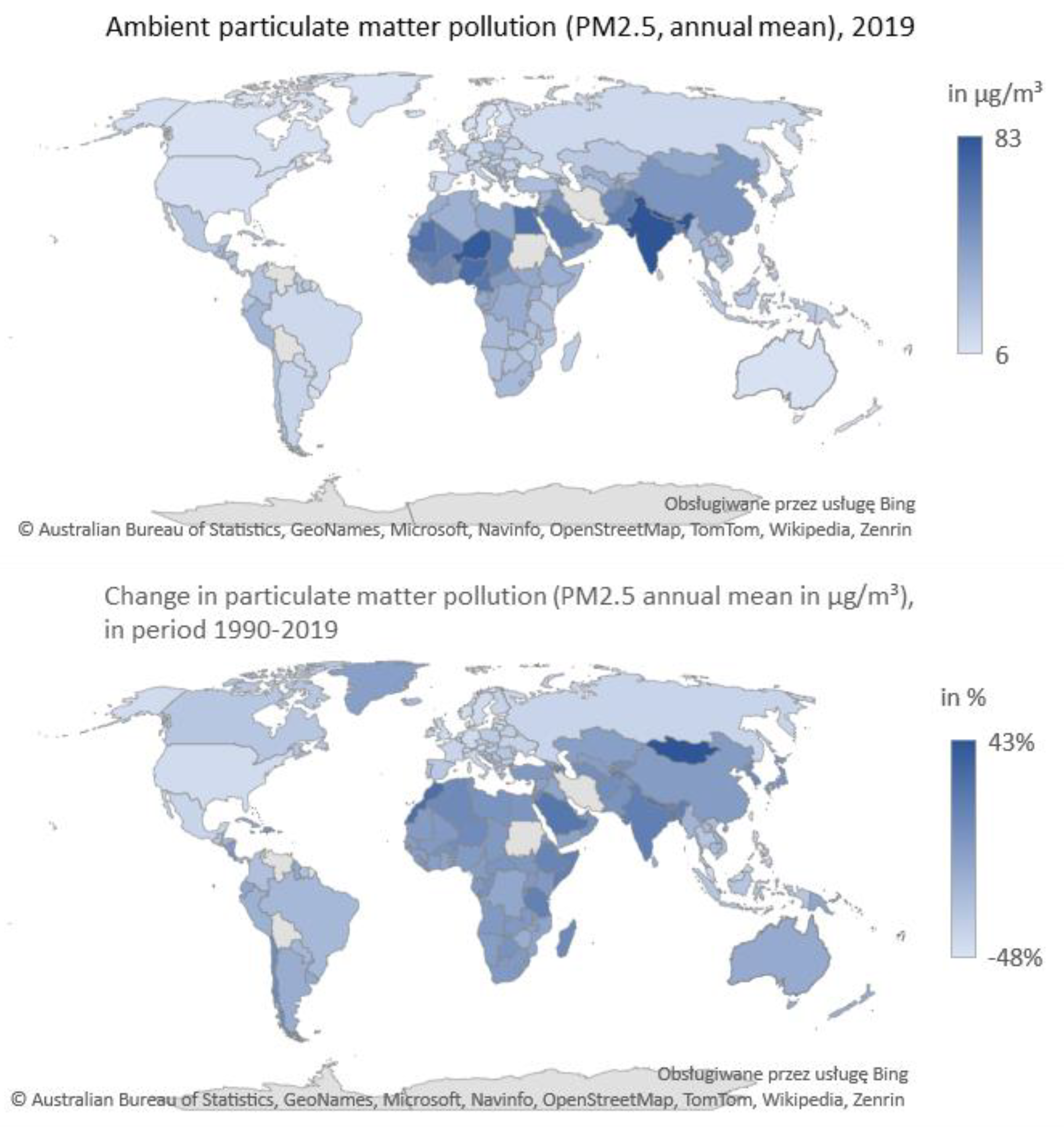
Figure 3.
Relationship between GDP per capita income level and PM2.5 air pollution levels. Source: GDP per capita [46] and PM2.5 in µg/m³ [45].
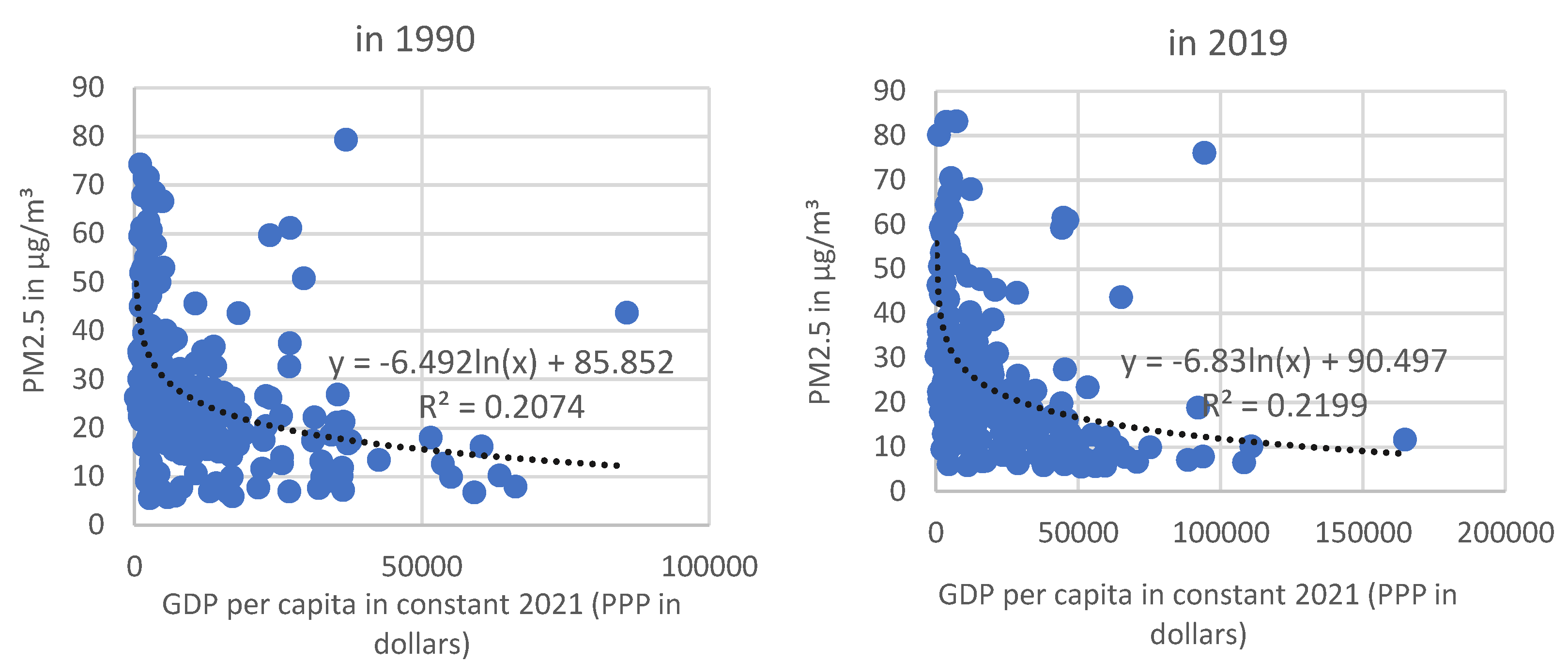
Figure 4.
Distribution of YLL(AP)rate and YLD(AP)rate, population aged 20-54, 1990 and 2019, N=204. Source: own study based on the data: [16].
Figure 4.
Distribution of YLL(AP)rate and YLD(AP)rate, population aged 20-54, 1990 and 2019, N=204. Source: own study based on the data: [16].
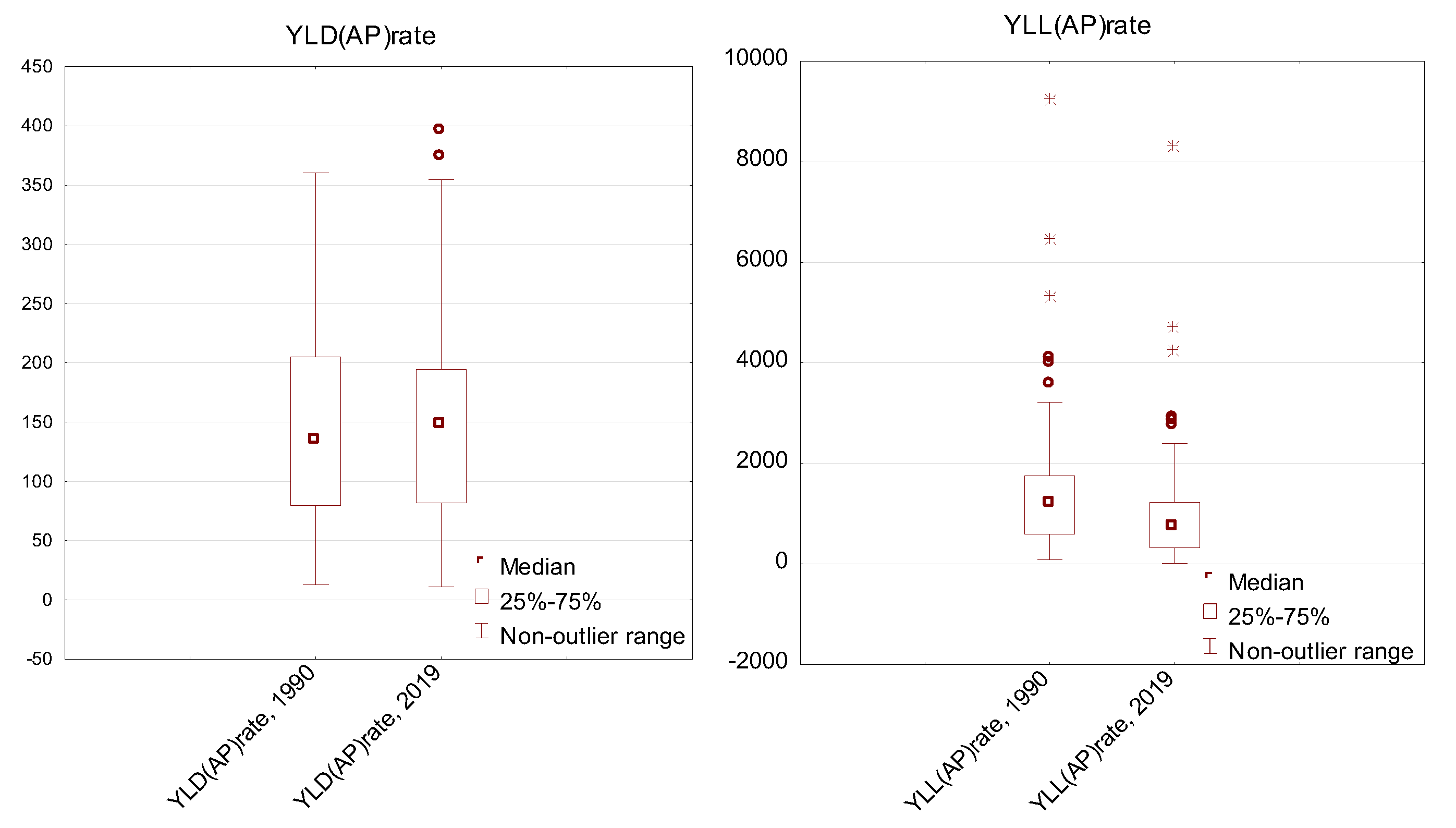
Figure 5.
Contribution of air pollution (AP) to premature deaths and years of life with a disability, population aged 20-54, in 2019, N=204.
Figure 5.
Contribution of air pollution (AP) to premature deaths and years of life with a disability, population aged 20-54, in 2019, N=204.

Figure 6.
Correlation matrix.
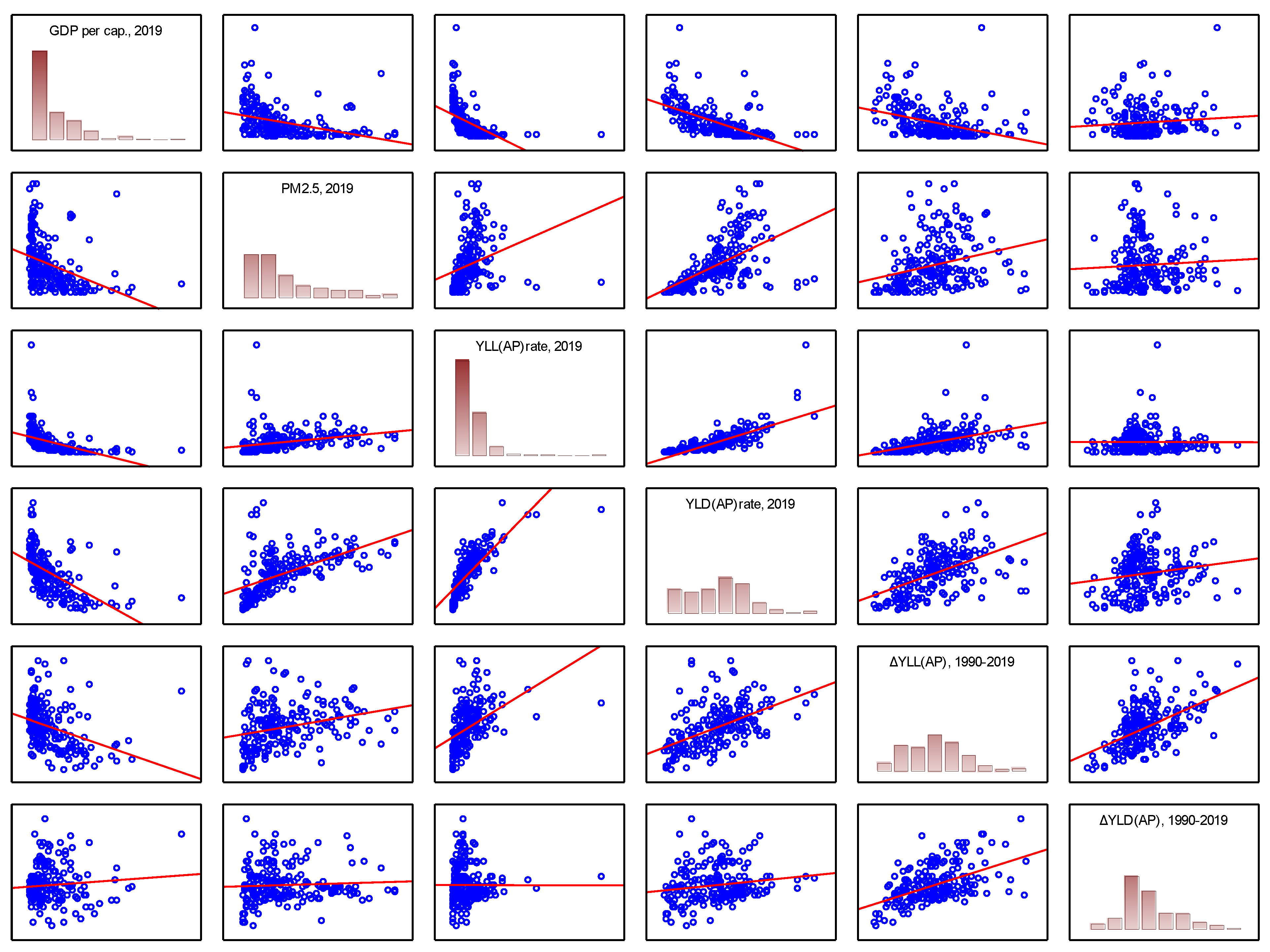
Figure 7.
YLLrate and YLDrate convergence patterns due to air pollution - beta convergence, over the period 1990-2019, N=204.
Figure 7.
YLLrate and YLDrate convergence patterns due to air pollution - beta convergence, over the period 1990-2019, N=204.
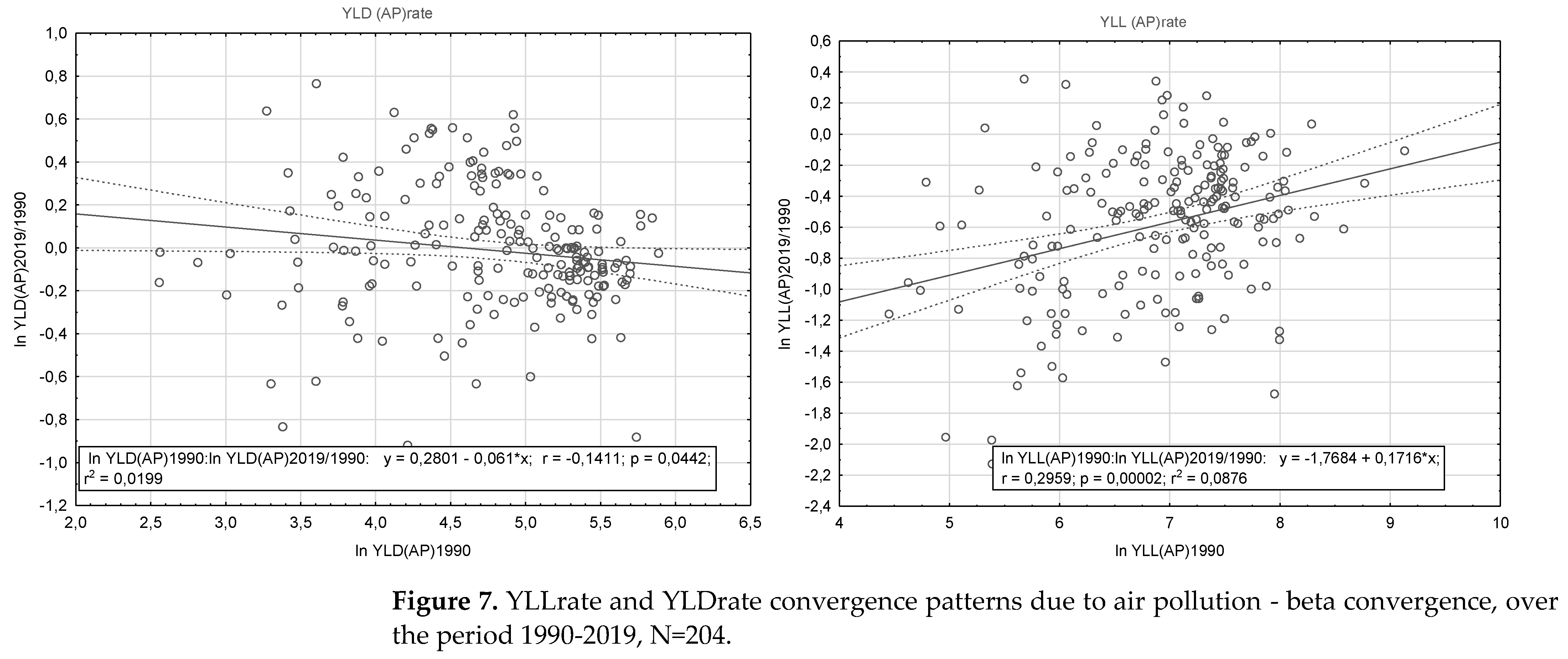
Figure 8.
DALYrate convergence patterns due to air pollution - beta convergence, over the period 1990-2019, N=204.
Figure 8.
DALYrate convergence patterns due to air pollution - beta convergence, over the period 1990-2019, N=204.
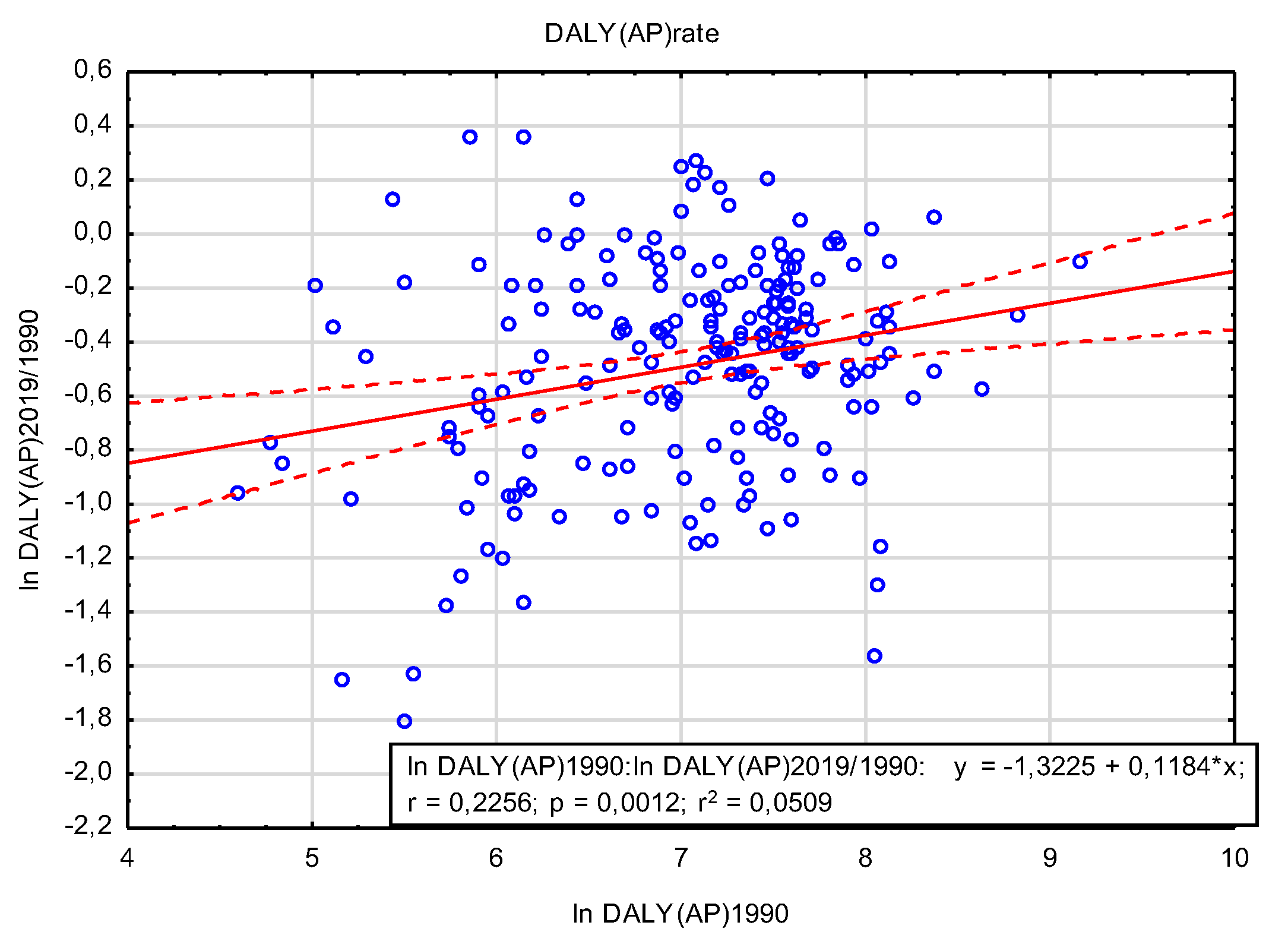

Table 1.
Summary exposure value (SEV) rate for 1990, 2019 and annualized rate of change (ARC) for 1990-2019.
Table 1.
Summary exposure value (SEV) rate for 1990, 2019 and annualized rate of change (ARC) for 1990-2019.
| Risks | SEV 1990* | SEV 2019 | ARC 1990-2019 |
| I. Environmental/occupational risks | 52.55 (48.66-55.92)** |
45.36 (41.16-49.19) |
-0.51 (-0.62- -0.40)* |
| A. Air pollution | 45.37 (32.89-56.28) |
34.72 (25.86-44.40) |
-0.92 (-1.25- -0.61)* |
| A1. Particulate matter pollution | 44.26 (31.87-55.07) |
33.84 (25.08-43.43) |
-0.93 (-1.26- -0.61)* |
| A1a. Ambient particulate matter pollution | 15.65 (10.61-21.58) |
26.19 (21.55-30.48) |
1.78 (0.95-2.71)* |
| A1b. Household air pollution from solid fuels | 27.33 (16.18-38.86) |
12.04 (6.72-18.82) |
-2.83 (-3.53- -2.20)* |
| A2. Ambient ozone pollution | 50.67 (22.95-73.01) |
61.19 (32.26-80.39) |
0.65 (0.33-1.25)* |
* Summary exposure value (SEV) is the RR-weighted prevalence of exposure, a univariate measure of risk weighted exposure, taking the value zero when no excess risk for a population exists and the value one when the population is at the highest level of risk. SEVs has been reported on a scale from 0% to 100% on which a decline in SEV indicates reduced exposure to a given risk factor and an increase in SEV indicates increased exposure. **95% uncertainty interval (UI) Source: [45].
Table 2.
descriptive statistics - YLL(AP)rate and YLD(AP)rate, population aged 20-54, 1990 and 2019, N=204.
Table 2.
descriptive statistics - YLL(AP)rate and YLD(AP)rate, population aged 20-54, 1990 and 2019, N=204.
| Variable | Descriptive statistics | ||||||
| N valid | Mean | Min. | Max. | Variance | SD | CV | |
| YLL(AP)rate, 1990 | 204 | 1349,0 | 86,0 | 9249,9 | 1193365,6 | 1092,4 | 81,0 |
| YLL(AP)rate, 2019 | 204 | 879,8 | 20,4 | 8299,1 | 780868,3 | 883,7 | 100,4 |
| YLD(AP)rate, 1990 | 204 | 144,6 | 12,9 | 360,3 | 6259,0 | 79,1 | 54,7 |
| YLD(AP)rate, 2019 | 204 | 143,0 | 11,0 | 396,3 | 5674,7 | 75,3 | 52,7 |
Source: own study based on the data: [16].
Table 3.
Air pollution (AP) burden of disease - YLLrate/YLD rate, population aged 20-54, by country group (breakdown by World Bank Income Levels), in 2019 and change from 1990 to 2019.
Table 3.
Air pollution (AP) burden of disease - YLLrate/YLD rate, population aged 20-54, by country group (breakdown by World Bank Income Levels), in 2019 and change from 1990 to 2019.
| World Bank Income Group | YLLs (AP) 2019 | YLDs (AP) 2019 | ||||
|---|---|---|---|---|---|---|
| Rate* | % in | Rate* | % in | |||
| all causes | NCD | all causes | NCD | |||
| 2019 | ||||||
| High Income | 219,4 | 3,1% | 4,2% | 68,7 | 0,5% | 0,6% |
| Upper Middle Income | 771,5 | 7,6% | 12,4% | 163,6 | 1,6% | 1,9% |
| Lower Middle Income | 1343,0 | 9,5% | 16,3% | 223,3 | 2,0% | 2,5% |
| Low Income | 1428,5 | 7,3% | 15,5% | 209,8 | 1,9% | 2,5% |
| Change over the period 1990-2019 (in %) | ||||||
| High Income | -50,0% | -31,5% | -40,3% | 7,9% | 3,4% | 1,4% |
| Upper Middle Income | -40,4% | -17,6% | -19,9% | -2,4% | -4,7% | -6,8% |
| Lower Middle Income | -22,6% | 12,6% | -7,5% | -7,6% | -4,1% | -7,2% |
| Low Income | -35,2% | 12,6% | -11,0% | -10,8% | -3,5% | -11,9% |
* YLLs/YLDs per 100,000 people.
Table 4.
Correlation results.
| Average | SD | GDP per cap., 20191 | PM2.5 (annual mean, µg/m3), 20192 | YLL(AP)rate, 20193 | YLD(AP)rate, 20193 | %ΔYLL(AP)rate, 1990-2019 | %ΔYLD(AP)rate, 1990-2019 | |
| GDP per cap., 2019 | 22658 | 24332 | 1,000 | -0,368* | -0,489* | -0,595* | -0,362* | 0,092 |
| PM2.5 (annual mean, µg/m3), 2019 | 26,1 | 17,7 | -0,368* | 1,000 | 0,283* | 0,560* | 0,274* | 0,056 |
| YLL(AP)rate, 2019 | 879,8 | 883,7 | -0,489* | 0,283* | 1,000 | 0,785* | 0,458* | -0,002 |
| YLD(AP)rate, 2019 | 143,0 | 75,3 | -0,595* | 0,560* | 0,785* | 1,000 | 0,516* | 0,163* |
| ΔYLL(AP)rate, 1990-2019 | -38% | 26% | -0,362* | 0,274* | 0,458* | 0,516* | 1,000 | 0,522* |
| ΔYLD(AP)rate, 1990-2019 | 3% | 31% | 0,092 | 0,056 | -0,002 | 0,163* | 0,522* | 1,000 |
*Correlation coefficients determined are significant with p < .05000, N=204.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the author. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



