
Submitted:
09 May 2023
Posted:
09 May 2023
You are already at the latest version
Abstract
Bronchial asthma (BA) is considered a chronic inflammatory disorder associated with airway hyperresponsiveness (AHR). Increased oxidative stress (OS) is a clinical feature of BA, which promotes the inflammatory responses in bronchial/airway epithelial cells. Smokers and nonsmokers with asthma have been shown to have increases in several OS and inflammatory biomarkers. A few studies suggest a relationship between antioxidant intake from diet/supplements and BA in smoking and nonsmoking asthmatics. Dietary carotenoids and vitamin C (VC) intake might reduce BA risk in smokers and/or non-smokers. Evidence is lacking on the protective role of antioxidant vitamin and/or mineral consumption against BA in smokers and nonsmokers with respect to inflammation and OS biomarkers. Therefore, the aim of this review is to highlight current knowledge regarding the relations between antioxidant intake, BA and its associated biomarkers in smokers and nonsmokers.
Keywords:
bronchial asthma
; antioxidant
; vitamins
; minerals
; supplements
; biomarkers
; oxidative stress
; inflammation
; smokers
; nonsmokers
1. Introduction
Smoking is regarded as a significant risk factor for asthma progression [1]. The number of asthma deaths due to smoking in 2019 was higher in men than in women [1,2]. Bronchial asthma (BA) is characterized by airway hyperresponsiveness (AHR) and reversible airflow obstruction, which is attributed to increased airway smooth muscle (ASM) contraction [3,4,5]. BA is associated predominantly with mast/CD4+ cells, T lymphocytes and eosinophils. Mucous hypersecretion, luminal obstruction, goblet cell hyperplasia and thickening of bronchial walls are commonly observed features in BA [3].
Tobacco smoke is associated with reduced lung function measured as forced expiratory volume in 1s (FEV1), and increased bronchial hyperresponsiveness in smokers with BA [6]. Smoking ≥10 pack/year at age 46 years was associated with a rapid decline in FEV1 and forced vital capacity (FVC) in asthmatic patients after 12-year follow-up [7]. Secondhand smoke (SHS) exposure has been linked to asthma risk in active and/or former smokers [8]. Exposure to SHS in public places was associated with a marked decrease in peak expiratory flow rate (PEFR) and FVC in asthmatic smokers [9]. The risk of BA among nonsmokers who were exposed to SHS has increased in a large adult-onset asthma population with 16 years of follow-up [10].
Tobacco smoke consists a range of toxic chemicals (e.g., benzopyrene, acrolein, crotonaldehyde, phenols, ammonia, nitrosamines, hydrocarbons, aromatic amines), which are potentially harmful to human bronchial epithelial cells (HBECs), causing airway inflammation by increasing mitochondrial reactive oxygen species (ROS) and pro-inflammatory interleukin (IL)-8 cytokine production [11,12]. Cigarette smoke extract (CSE) exposure in HBECs results in increased oxidative stress (OS) and pro-inflammatory cytokines IL-6, IL-8, and tumor necrosis factor α (TNF-α) by the activation of several inflammatory signaling pathways, including the transcription factor-kappaB (NF-κB), extracellular signal-regulated kinases (ERK 1/2), c-Jun N-terminal kinase (JNK) and mitogen-activated protein kinases (MAPKs) [13]. Tobacco smoke alters immune responses in the lung triggering BA by activating Toll-like receptors (e.g., TLR-2 and TLR-4)-stimulated pro-inflammatory cytokine production and increasing total serum immunoglobulin E (IgE) levels in airway epithelial cells [14]. In asthmatic patients, exposure to environmental tobacco smoke (ETS) results in oxidant/antioxidant imbalance, which leads to increased pro-inflammatory biomarkers, as assessed by increased TNFα, IL-6 and IL-8 [14]. Evidence suggests that nicotine is not carcinogenic, but it may affect the airway epithelial cells of asthmatic smokers by activating nitrosamine 4(methylnitrosamino)-1-(3–pyridyl)-1-butanone (NNK), which binds to the α7 nicotinic acetylcholine receptor (α7nAChR), leading to AHR and inflammation by upregulating the α7nAChR-mediated signaling pathways [15].
The genetic variants-tobacco smoke exposure interaction has been shown to increase BA risk in smokers and nonsmokers. Evidence of the interaction between variants of rs9969775 on chromosome 9, rs5011804 on chromosome 12, and active tobacco smoking was reported in asthmatic adults [16]. Genetic variants of NLR Family CARD Domain Containing 4 (NLRP4) inflammasome are implicated in BA exacerbation in current and former adult smokers as evidenced by high genotype-specific expression of rs16986718G [17]. The presence of mutant AG/GG genotype for CD14 rs2569190 and rs13150331 (TLR) polymorphism in asthmatic adult smokers increases the risk of the disease [18]. Asthmatic non-smokers carrying allele homozygotes of rs1384006 C > T of the OS responsive kinase 1 (OXSR1) gene are at higher asthma exacerbation risk than asthmatics smokers [19].
Few studies have evaluated evidence-based treatment for BA in smokers. Pycnogenol®, a herbal dietary supplement-based extract derived from French Pinus pinaster bark, is regarded as an option for the treatment of asthma when used in combination with the inhalation corticosteroid (ICS) therapy, resulting in improvement of BA symptoms [20]. Asthmatic smokers have ICS insensitivity as compared to asthmatic nonsmokers, and are less responsive to the benefits of ICS treatment alone. Alterations of inflammatory phenotypes, glucocorticoid receptors, and reduction of histone deacetylase (HDAC) activity are considered potential mechanisms of corticosteroid insensitivity in asthmatic smokers [21,22]. The combination of ICS therapy and a long-acting β2 adrenergic (LABA), displays a better clinical improvement for smoking and nonsmoking asthmatics than using ICS alone [23,24]. The use of nicotine replacement therapy, varenicline or bupropion, may significantly improve lung function and AHR in asthmatic smokers [23].
There is still significant amount of uncertainty in the safety and efficacy of dietary supplements for the treatment of lung diseases among smokers and/or nonsmokers due to limited number of randomised controlled trials (RCTs) [25,26]. Thus, there is a need to focus on the role of antioxidant in smoking-related BA risk. A recent review investigating the effects of dietary antioxidant intake on lung cancer (LC) risk among smokers and nonsmokers suggests that dietary vitamins (C, D, E and carotenoids) and minerals (zinc and copper) may exert protective effects against cigarette smoke (CS)-induced OS and/or inflammation. However, dietary retinol and iron intake did not provide any protection, and research suggests caution in recommending these for LC treatment [27]. There is a direct association between LC and BA in smokers [28,29]. Given that smoking is considered a risk factor for BA through increased levels of OS and inflammatory cytokine production [15], targeting dietary/supplement-derived antioxidants might help our understanding of their role in protecting bronchial/airway epithelial cells against CS-induced-OS/inflammatory biomarkers in smokers and nonsmokers. This paper explores this connection to gain insight into the health consequences of antioxidant consumption, and makes recommendations for future studies. To date, there have been no reviews to evaluate antioxidant intake and the biomarkers of OS and inflammation in BA, according to smoking status.
2. Methods
A literature review in the PubMed/MEDLINE database and Google scholar was conducted for English language studies published between 1 January 2000, and 31 April 2023. The following search terms were used: asthma, diet, supplements, antioxidant, vitamins, minerals, OS, lipid peroxidation (LP), inflammation, biomarkers, antioxidant/oxidant enzymes, bronchial/airway epithelial cells, smokers and nonsmokers. Studies focusing on the chronic obstructive pulmonary disease (COPD) were excluded, as the diagnostic biomarkers in BA are different from both COPD and the BA-COPD overlap. All studies relevant to the search terms were included, and the search was not limit to a particular study design.
3. Antioxidant Intake and Its Relationship with BA in Smokers and Nonsmokers
Studies investigating the associations between antioxidant intake and BA in smokers and nonsmokers are limited. Smokers with low dietary vitamin C (VC) intake had chronic bronchitis symptoms associated with BA compared with those who had higher intake [30]. According to quartiles of carotenoid dietary/supplement intake (carotene, lycopene and lutein with zeaxanthin), the risk of BA was reported to be lower in the fourth quartile (≥165.59 μg/kg per day) than the first quartile (<41.43 (μg/kg per day) among current smokers, former smokers and nonsmokers with BA [31]. One trial revealed no effects of 6 weeks of supplemental vitamin E (VE) on AHR in nonsmokers with BA [32]. Supplementation with selenium (Se) had no significant improvement in BA-related quality of life (QoL) and lung function regardless of smoking status [33]. These findings suggest that dietary VC and carotenoids intake may reduce BA in smokers and/or nonsmokers. Supplementation with VE and Se had no effect on BA in smokers and nonsmokers. The associations between antioxidant intake and BA risk are summarized in Table 1.
4. Biomarkers of OS and Inflammation in Smoking and Nonsmoking Asthmatics
OS is regarded as the major contributor to CS-induced airway inflammation [34]. Evidence from many studies, mostly derived from cross-sectional and/or longitudinal case-control design, has shown that CS activates OS by augmenting airway inflammation in smoking and nonsmoking asthmatics.
4.1. Smokers
4.1.1. Biomarkers of OS
Asthmatic current smokers showed increased serum levels of malondialdehyde (MDA), and decreased levels of ferric reducing ability of plasma (FRAP) [35]. Higher MDA levels in expired breath condensate (EBC) have been reported in active smoking asthmatics than former smoking and nonsmoking counterparts [36]. The levels of protein carbonyls and peroxynitrite in plasma were reported to be higher in smoking asthmatics than nonsmoking counterparts [37]. Smoking asthmatics with a lower FEV1 have higher erythrocyte antioxidant enzyme activity, including glutathione peroxidase (GPx), superoxide dismutase (SOD), and reduced OS biomarker glutathione disulfide/oxidized glutathione (GSH) activity than nonsmoking counterparts. Increased antioxidant enzyme activity in smoking asthmatics may protect airway epithelial cells against the harmful effects of free radicals [38]. Active smoking asthmatics exhibit higher pro-oxidant biomarker NADPH oxidase 2 (NOx2) mRNA levels in bronchial epithelial cells, together with increased urinary LP biomarker isoprostane-8-iso prostaglandin F2α (8-iso-PGF2α) as compared to former smoking and non-smoking asthmatics. Smoking asthmatics showed higher levels of hydrogen peroxide (H2O2) and NOx in EBC [39].
4.1.2. Biomarkers of Inflammation
Fractional exhaled nitric oxide (FeNO) was reported in lower levels in smoking asthmatics than nonsmoking counterparts. This reduction could be attributed to higher levels of exhaled carbon monoxide in smokers or suppression of nitric oxide synthase (NOS) levels of exogenous nitrite (NO2) in tobacco smoke [40]. Smoking asthmatics had lower FeNO levels than nonsmoking counterparts, but this decrease does not appear to reflect improvement of BA control [41]. When compared with asthmatic smoking groups, FeNO was associated with NOS2 mRNA levels in active smokers [42]. Current smoking asthmatics exhibit a lower FEV1/FVC ratio, FeNO value, together with higher blood/sputum neutrophil proportions than nonsmoking counterparts [43,44]. Current smokers with severe asthma have lower FeNO value than former smokers and nonsmokers [45]. Increased FeNO levels have been observed in smokers with uncontrolled asthma, which are associated with percentages of sputum eosinophils [46]. Increased levels of FeNO and blood eosinophil count in current/former smokers with asthma gave a poor to fair prediction of type-2 high status in airway epithelial cells [47].
High-sensitivity C-reactive protein (hs-CRP) was reported to be higher in asthmatic smokers than nonsmokers [48]. Matrix metallopeptidase (MMP-1) and (MMP-9) levels, which mediate CS-induced inflammation, have been observed in higher proportions in the nasal tissues of smoking asthmatics compared to nonsmoking counterparts [49]. Sputum MMP12 mRNA levels were found to be higher in smoking asthmatics than in healthy control [50]. Higher levels of MMP-12, C-X-C motif chemokine ligand-8 (CXCL8), neutrophil elastase, azurocidin 1 (AZU-1) and pro-platelet basic protein (PPBP) were observed in the sputum of former smoking asthmatics, which are linked to neutrophilic inflammation [44]. The pro-inflammatory IL-17A mRNA has been detected in higher levels in the nasal tissues of smoking asthmatics than nonsmoking counterparts [51]. Higher sputum eosinophils, eosinophilic cationic protein (ECP), neutrophils and IL-8 levels were observed in asthmatic smokers compared to asthmatic nonsmokers, which were associated with FEV1 and neutrophil count [52]. Comparatively greater levels of sputum IL-1β, IL-5 and Interleukin 18 receptor 1 (IL-18R1) have been reported in current/former smoking severe asthmatics compared to healthy controls [53]. Current and former smokers with BA have higher frequencies of sputum type 3 innate lymphoid cells (ILC3) which has been identified as a biomarker of airway eosinophilic inflammation, and peripheral blood CD45RO-expressing memory-like ILC3s compared with nonsmokers counterparts. ILC3 was associated with M1 alveolar macrophage and circulating neutrophil counts [54]. Eotaxin as an inflammatory biomarker for the prediction of BA, was found at higher levels in the sputum from smokers than nonsmokers. High levels of sputum eotaxin 2 were associated with sputum neutrophil and eosinophil counts and percentages [55].
Overall findings suggest that the oxidant/antioxidant imbalance derived by CS is likely to exist in smoking asthmatics. OS and inflammation biomarkers are increased in current and/or former smokers, but the increase in the enzymatic antioxidants and the reduction in FeNO levels may be insufficient to protect bronchial/airway epithelial cells against oxidative damage. Figure 1 shows the OS and inflammatory biomarkers in smoking asthmatics.
4.2. Nonsmokers
4.2.1. Biomarkers of OS
4.2.2. Biomarkers of Inflammation
Increased levels of FeNO have been observed in the airways of current nonsmoking asthmatics [58,59]. This increase is associated with a decrease in the FEV1 and FEV1/FVC ratio [59]. Compared to active and former smokers with asthma, nonsmokers with asthma had higher FeNO levels [60,61]. FeNO and EBC pH values were higher in nonsmokers with uncontrolled BA than those with partly/well-controlled BA [62]. High FeNO levels and blood eosinophil count provide a moderate prediction of type 2 high status in severe asthmatic nonsmokers [47].
Serum periostin, a biomarker of airway eosinophilia inflammation, has been observed in higher levels in nonsmokers than smokers with BA [63]. In asthmatic patients with persistent obstruction where nonsmokers represented the vast majority, high sputum periostin levels were associated with FEV1 decline and high sputum eosinophil counts, resulting in increased FeNO value, blood eosinophil counts and transforming growth factor beta 1 (TGF-β1) [64]. High serum periostin, TNFα, IL-4, IL-5 and the chitinase-like protein YKL-40 levels, and low serum IL-37 levels were associated with exacerbated BA in nonsmokers [65]. Nonsmokers with BA have significantly elevated sputum and blood eosinophil counts [44]. Compared to healthy nonsmokers, nonsmoking asthmatics demonstrated higher sputum ECP and eosinophil levels [52]. High IL-18 levels in the sputum of nonsmoking asthmatics were associated with FEV1 decline [66]. Bronchoscopy and Bronchoalveolar Lavavge Fluid (BALF) levels of eotaxin-1 and serum/sputum levels of IL-5 were observed to be higher in nonsmoking asthmatics and smoking counterparts. Higher sputum levels of IL-4, IL-5, IL-1β, Interleukin 1 receptor-like 1 (IL-1RL1), Interleukin 1 receptor, type I (IL-1R1), IL-1R2, IL-18R1 and NLRP3 were detected in nonsmoking severe asthmatics compared to mild-moderate asthmatics and healthy controls [53]. High BALF eotaxin-1 was associated with increased BALF eosinophil and neutrophil counts and percentages [55]. Eotaxin-1 in EBC was associated with blood eosinophil count, FeNO value and serum ECP in nonsmoking asthmatics [67].
Levels of serum IgE used as a biomarker of T-helper 2 (Th2)-driven inflammation were associated with reduced risk of small airway obstruction in nonsmoking asthmatics compared to current and former smoking counterparts [68]. A number of inflammation biomarkers (e.g., IL-6, TNF receptor superfamily member 11a; TNFRSF11A, TGF-β1) have been identified in higher proportions in nonsmokers with severe asthma compared to nonsmokers with mild-to-moderate BA [69]. High levels of peripheral blood ILC2, FeNO, and blood eosinophil counts were associated with sputum eosinophil counts in nonsmokers with mild to moderate BA [70]. Higher serum hs-CRP levels were reported in nonsmokers with mild-to-moderate BA than healthy controls, and were associated with sputum eosinophils and impaired FEV1 [71,72]. It can be suggested that nonsmoking asthmatics exhibit higher levels of OS and inflammation biomarkers, which have the potential to increase the risk. Figure 2 shows the OS and inflammatory biomarkers in nonsmoking asthmatics.
5. Potential Effects of Antioxidant on BA-Associated CS-Induced OS and Inflammation Biomarkers
5.1. Antioxidant Vitamins
5.1.1. Vitamin A
Vitamin A (VA) derived from dietary animal-source foods has an active metabolite retinoic acid (RA), which binds retinoic acid receptors (RARs) and retinoid X receptors (RXRs) with high affinity, resulting in a regulation of ASM cell proliferation in BA [73]. Low RA levels in human ASM cells increases the severity of asthma [74]. ASM cells treated with RARγ-specific agonist and all-trans RA (ATRA) lead to inhibition of activator protein-1 (AP-1) and platelet-derived growth factor (PDGF)-stimulated cell proliferation [74]. TGF-β increases the expression of ATRA and 9-cis RA in the ASM cells of patients with severe BA compared with those with mild-to-moderate BA, which results in upregulation of the mRNA of β1-integrin, MMP-9 and hepatocyte growth factor receptor (HGF-R). Treatment with anti-TGF-β reduces the levels of MMP-9 mRNA in ASM cells. This concludes that TGF-β increases ASM cell inflammation in response to exaggerated RA receptor expression, which may lead to airway epithelial repair defects in severe BA [75]. Administration of ATRA suppresses PDGF-induced ASM cell migration via RAR-RXR heterodimer activation and Serine-threonine kinase/Phosphatidylinositol-3 kinase (Akt/PI3K) signaling pathway inhibition [76]. Treatment with RA improves barrier strength of HBECs by reducing TNF-α-induced airway barrier leaks, decreased occludin/claudin-4 and increased ERK1/2 activation [77]. ATRA treatment inhibits airway inflammation in vivo but not in in vitro experimental allergic asthma by suppressing Th2 and Th17-related cytokines IL-4, IL-5, IL-17 [78]. Administration of ATRA and 9-cis RA suppresses IL-4-induced eotaxin mRNA expression in HBECs [79]. 9-cis-RA treatment results in reversing RAR-beta (RAR-β) expression loss in the HBECs of former smokers, suggesting that RA may be considered as a potential agent against BA risk in smokers [80]. Nonsmoker patients with lung emphysema treated with ATRA resulted in improvement in lung function and reduction of airway inflammation through inhibition of TNF-α and IL-3 plasma levels [81]. Overall findings suggest that VA exerts anti-inflammatory effects on ASM/HBECs cells.
5.1.2. Carotenoids
β-carotene, also termed provitamin A/non-polar carotenoid, and other non-provitamin A/polar carotenoids (e.g., lycopene, lutein, zeaxanthin) are natural pigments present primarily in fruits and vegetables, which have been shown to exert anti-inflammatory/OS agents for several diseases [82], including BA [83]. It has been shown that supplementation of HBECs “BEAS-2B” with β-carotene does not promote membrane LP/lactate dehydrogenase (LDH) leakage and α-tocopherol/GSH depletion caused by gas phase smoke [84]. β-carotene exerts a protective effect in HBECs treated with CS-induced lung carcinogen benzo[a]pyrene (BaP) through increasing RAR-β expression [85].
Lycopene exerts a therapeutic effect against BA in vivo by reducing eosinophilic infiltrates and Th2-mediated cytokines IL-4 and IL-5 production in the airways [86]. An in vitro experiment showed that apo-10′-lycopenoic acid treatment, an active metabolite of lycopene, increases accumulation of nuclear factor-E2 related factor 2 (Nrf2)-mediated heme-oxygenase-1 (HO-1) activation, intracellular GSH levels, and decreases intracellular ROS levels and H2O2-induced LDH production in BEAS-2B [87]. Treatment of BEAS-2B with β-cryptoxanthin (BCX) reduces inflammation in vitro, as indicated by increased sirtuin1 (SIRT1) protein levels and inhibited lipopolysaccharide (LPS)-induced TNF-α, MMP2/9, IL-6 and monocyte chemoattractant protein-1 (MCP-1) mRNA levels [88]. BCX supplementation of ferrets led to inhibited CS-induced NF-kB, AP-1 and TNFα expression in HBECs [89]. These findings suggest that β-carotene, lycopene and BCX may protect HBECs against CS-induced inflammation and OS biomarkers.
5.1.3. Vitamin C and E
Epidemiological studies regarding the role of antioxidant VC and VE in the treatment of BA have demonstrated inconsistent findings [90]. The ascorbic acid supplemented diet has been shown to reduce the bronchoconstrictive responses in asthmatic patients, as demonstrated by decreasing post-exercise FeNO, FEV1, and urinary 9α, 11β-PGF2 levels [91]. Administration of VC to ovalbumin (OVA)-sensitized and challenged asthmatic mice attenuates airway inflammation by reducing eosinophilic infiltration into BALF [92].
VE treatment reduces BaP-induced ROS levels by downregulating poly[ADP-ribose] polymerase 1 (PARP-1) and protein 53 (p53) activity in BEAS-2B [93]. Treatment with natural-source d-α-tocopheryl acetate increases plasma levels of α-tocopherol isoform of VE in atopic asthmatics, resulting in reduced BAL levels of IL-3 and IL-4 [94]. In allergic asthmatic adults, γ-tocopherol treatment led to suppression of LPS-induced JNK phosphorylation and Inhibitory kappa B kinase (IkBα) degradation [95]. In human and mice models, supplementation with γ-tocopherol reduced LPS-induced sputum percentages of neutrophils and eosinophils [96]. γ-tocopherol supplementation reduces sputum mucins and eosinophils in mild asthmatics compared to healthy controls [97]. VE-supplemented diet results in decreased IL-4 and IL-5 levels in the bronchial epithelial cells of mice [98]. Treatment with VE attenuates AHR in asthmatic mice through reducing OS and inflammatory biomarkers, as indicated by decreasing LPS-induced IL-5, IL-13 levels, H2O2-mediated ROS production, and increasing Nrf2 levels [99]. Administration of VE reduces exacerbated OVA-induced asthma in mice by decreasing IL-4 levels, ROS producing, serum IgE levels, and increasing GSH levels [100]. VE treatment of OVA-sensitized allergic asthma murine model reduced levels of 8-iso-PGF2α, NO2, IgE, eotaxin, TGF-β1, IL-4, IL-5 and IL-13 [101]. In mice models of asthma, administration of supplemental α-and γ-tocopherol resulted in reduced BAL IL-5, IL-12 and IL-13 levels [102]. This suggests that VC may reduce airway inflammation, while VE may have protective effects against both OS and inflammatory biomarkers.
5.1.4. Vitamin D
Evidence from in vitro and in vivo studies has supported the protective role of VD against BA, by which VD supplementation reduces airway inflammation and improves lung function in asthmatic patients [103]. VD treatment has been shown to decrease IL-6 levels in cultured HBECs from asthmatic donors [104]. In asthmatic patients, supplementation with VD increases serum anti-inflammatory IL-10, and decreases serum levels of IgE, eosinophil, IL-5, IL-9, and IL-13 [105]. Supplementation with VD reduces OS in a murine model of OVA-stimulated asthmatic airway inflammation, as evidenced by decreased levels of IL-4 in BALF and NO2 in serum and BALF [106]. In an asthmatic mouse model, VD treatment decreases the index of airway collagen deposition, mucus reserve, and increases autophagy-related protein expression levels of hypoxia-inducible factor 1 alpha (HIF-1α) and neurogenic locus notch homolog protein 1 (Notch1), resulting in reduced airway inflammation associated with IL-6 and IL-17 cytokines [107]. Supplementation of VD reduces AHR and IgE levels in BALF and serum in asthmatic mice [108]. Administration of VD to VD-deficient mice with asthma reduces BALF levels of neutrophil, eosinophil, IL-5 and IL-13 [109]. In a mouse model of allergic asthma, it has been demonstrated that 1,25(OH)(2)D(3) supplementation reduces serum OVA-specific IgE levels, accompanied with increased serum levels of IL-10 and TGF-β1 via inhibition of NF-kB signaling pathway [110]. It has been shown that VD-supplemented OVA-sensitized and challenged mice with asthma reduce BALF eosinophil numbers, BALF IL-6, IL-17, TNF-α levels, and increase BALF IL-10 levels [111]. In asthmatic mice, VD was found to reduce serum levels of IL-6, IL-1β, TNF-α, and increase serum levels of IL-10 through downregulating high mobility group box 1 proteins (HMGB1)/TLR4/NF-κB signaling pathway [112]. Overall findings suggest that VD may have anti-inflammatory/oxidants effects on HBECs, due to its ability to reduce inflammatory/OS biomarkers, which may therefore be involved in CS-induced BA treatment.
The potential effect of antioxidant vitamins on BA-associated CS-induced biomarkers was shown in Figure 3.
5.2. Antioxidant Minerals
5.2.1. Iron
Iron (Fe) is a critical mineral implicated in free radical production, which has a detrimental effect on BA, as evident by increasing plasma Fe levels in HBECs, which result in a significant increase in OS and LP biomarkers, including NOx, MDA and myeloperoxidase (MPO) [113,114]. IL-6 was shown to enhance ferroptosis in HBECs, identified as regulated cell death, by disrupting iron homeostasis and increasing ROS and MDA-dependent LP [115]. In mice sensitized to OVA, high expression of HO-1, an enzyme responsible for degrading heme into free iron, was found to be associated with asthmatic airway inflammation via increased levels of IL-5, IL-13 and eosinophilia in the lung tissue [116].
High serum levels of saturation of transferrin and ferritin, as indices of Fe homeostasis, were associated with airway obstruction in smokers and nonsmokers with the lowest FEV1/FVC ratio [117]. Exposure to tobacco smoke condensate alters iron homeostasis in human respiratory epithelial cells by increasing serum Fe and ferritin accumulation in the lungs of smokers [118]. This suggests that Fe is associated with increased BA risk, and should not be recommended for smoking asthmatics.
5.2.2. Zinc, Selenium and Copper
Evidence from in vivo and in vitro studies suggests that zinc (Zn), Se and copper (Cu) play a significant role in reducing BA and protecting airway epithelial cells against OS and inflammatory biomarkers [119]. Treatment of airway epithelial (HEp-2) cells with toxic copper oxide nanoparticles (CuONPs) results in induced OS by increasing ROS and 8-isoprostane production [120]. CuONPs increase AHR and the production of ROS and pro-inflammatory cytokines via activating of MAPK signaling in OVA-induced asthmatic mice [121]. Cu and Zn are key components of SOD, which results in a reduction of OS. The plasma levels of Se, Cu, Zn and a cytosolic antioxidant enzyme copper-zinc-superoxide dismutase (CuZnSOD) were reported to be lower in asthmatics than in healthy controls [122,123,124]. Se was found to be associated with decreased levels of OS biomarker plasma thiobarbituric acid reactive substances (TBARS), hs-CRP levels and CD4/CD8 lymphocyte ratios [123]. An in vitro experiment has demonstrated that Zn chelator N,N,N′,N′-tetrakis(2-pyridylmethyl)ethylenediamine inhibits TNFα-induced eotaxin mRNA expression in BEAS-2B cells [125]. In a mouse model of allergic inflammation, Zn supplementation reduced BALF eosinophils and attenuated airway inflammation-induced solute carrier family 39 members 1 and 14 (ZIP1, ZIP14) [126]. Administration of Zn to mice with OVA-induced allergic asthma led to reduced monocytes, neutrophils, eosinophils in BALF, MCP-1 and eotaxin protein production [127]. This suggests that Zn and Cu may have potential antioxidant effects against inflammation biomarkers.
The potential effect of antioxidant minerals on BA-associated CS-induced biomarkers was shown in Figure 4.
6. Concluding Remarks
CS is associated with biomarkers of OS and systemic inflammation in HBECs. Literature from cross-sectional and/or longitudinal case-control design has shown that OS and inflammation have a significant role in the pathogenesis of BA in both smokers and nonsmokers. Smoking and nonsmoking asthmatics showed some similarities in OS and inflammatory biomarkers. However, there were differences in biomarkers of CS-induced OS and/or inflammation between smokers and nonsmokers. OS biomarkers MDA, NOx, 8-iso-PGF2α, H2O2, and inflammation biomarkers MMPs, CXCL8, AZU-1, PPBP and elastase were found to associate with BA in smokers, but not in nonsmokers. Inflammatory biomarkers periostin, IgE, TGF-β1, TNF-α, ILC2 and NLRP3 showed positive association with BA in nonsmokers, but not in smokers. Current and/or former smokers with BA have higher levels of OS biomarkers than nonsmokers, and thus are at a heightened state of OS. The activity of the enzymatic antioxidant defense in smoking asthmatics may not adequately protect the HBECs from CS-induced OS.
Evidence from a few studies suggests that dietary VC and carotenoid intake are associated with reduced BA risk in smokers and/or nonsmokers. Supplementing VE and Se had no effects on improving lung function in smoking asthmatics.
Several in vivo and in vitro studies have demonstrated the protective effects of antioxidant vitamin and mineral against BA-associated biomarkers. Supplementing VA and VC might protect HBECs against inflammatory biomarkers, while supplementing VE, VD, β-carotene, lycopene and BCX might provide protection against both OS and inflammatory biomarkers. Antioxidants Se, Zn and Cu may potentially protect HBECs against BA-associated OS/inflammatory biomarkers. Zn supplementation might be effective in reducing BA-mediated airway inflammation. Fe has adverse effects on HBECs, and should be avoided for smoking and nonsmoking asthmatics.
The potential effects of antioxidant on BA-associated CS-induced biomarkers in both smokers and nonsmokers are difficult to determine, given a limited number of human studies. VA and carotenoids (particularly β-carotene and β-cryptoxanthin) trigger a protective effect against BA in smokers and/or nonsmokers. However, other antioxidants such VC, VE, VD, Zn and Se may have protective potential against BA-associated biomarkers. Such effects lead to the conclusion that these antioxidants might have beneficial effects in reducing BA in smokers and nonsmokers, given that smoking and nonsmoking asthmatics are susceptible to CS-induced OS and inflammatory biomarkers.
The mechanisms by which antioxidant vitamin and mineral might be effective in protecting HBECs against BA-associated biomarkers in smokers and nonsmokers have not been fully elucidated. Human studies on the exact mechanisms (signaling pathways) linking the antioxidant intake to BA in smokers and nonsmokers have not yet confirmed. Few signaling pathways might be involved, as demonstrated by mice models (e.g., TLR4/NF-κB signaling pathway in VD). Further human studies are needed to explore the mechanisms by which antioxidants might be effective in protecting HBECs against BA-associated biomarkers in smokers and nonsmokers.
More studies on smokers and nonsmokers are needed to determine the associations between antioxidant intake from both diet and supplements and BA-associated inflammation and OS biomarkers. Studies included in this review did not determine whether nonsmokers with BA are affected by SHS exposure. Thus, further studies are required to examine whether antioxidant intake in nonsmoking asthmatics exposed to SHS/ETS could protect HBECs against CS-induced BA biomarkers.
Funding
This review received no financial support.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Data Availability Statement
Not applicable.
Conflicts of Interest
The author declares no conflict of interest.
Abbreviations
| AHR | Airway hyperresponsiveness |
| Akt | Serine-threonine kinase |
| AP-1 | Activator protein-1 |
| ASM | Airway smooth muscle |
| ATRA | All-trans RA |
| AZU-1 | Azurocidin 1 |
| BA | Bronchial asthma |
| BALF | Bronchoalveolar Lavavge Fluid |
| BaP | Benzo[a]pyrene |
| BCX | β-cryptoxanthin |
| COPD | Chronic obstructive pulmonary disease |
| CS | Cigarette smoke |
| CSE | Cigarette smoke extract |
| Cu | Copper |
| CuONPs | Copper oxide nanoparticles |
| CuZnSOD | Zinc-superoxide dismutase |
| CXCL | C-X-C motif chemokine ligand |
| EBC | Expired breathe condensate |
| ECP | Eosinophilic cationic protein |
| ERK | Extracellular signal-regulated kinases |
| ETS | Environmental tobacco smoke |
| Fe | Iron |
| FeNO | Fractional exhaled nitric oxide |
| FEV1 | Forced expiratory volume in 1s |
| FRAP | Ferric reducing ability of plasma |
| FVC | Forced vital capacity |
| GPx | Glutathione peroxidase |
| GSH | Reduced glutathione |
| H2O2 | Hydrogen peroxide |
| HBECs | Human bronchial epithelial cells |
| HDAC | Histone deacetylase |
| HGFR | Hepatocyte growth factor receptor |
| HIF-1α | Hypoxia-inducible factor 1 alpha |
| HMGB1 | Mobility group box 1 protein |
| HO-1 | Heme-oxygenase-1 |
| hs-CRP | High-sensitivity C-reactive protein |
| ICS | Inhalation corticosteroid |
| IgE | Immunoglobulin E |
| IkBα | Inhibitory kappa B kinase |
| IL | Interleukin |
| ILC | Innate lymphoid cell |
| IL-18R1 | Interleukin 18 receptor 1 |
| IL-1RL1 | Interleukin 1 receptor-like 1 |
| 8-iso-PGF2α | Isoprostane-8-iso prostaglandin F2α |
| JNK | c-Jun N-terminal kinase |
| LABA | Long-acting β2 adrenergic |
| LC | Lung cancer |
| LDH | Lactate dehydrogenase |
| LP | Lipid peroxidation |
| LPS | Lipopolysaccharide |
| MAPKs | Mitogen-activated protein kinases |
| MCP-1 | Monocyte chemoattractant protein-1 |
| MDA | Malondialdehyde |
| MMP | Matrix metallopeptidases |
| MPO | Myeloperoxidase |
| α7nAChR | α7 nicotinic acetylcholine receptor |
| NF-κB | Nuclear transcription factor-kappaB |
| NLRP | NLR Family CARD Domain Containing |
| NNK | Nitrosamine 4(methylnitrosamino)-1-(3–pyridyl)-1-butanone |
| NO2 | Nitrite |
| NOS | Nitric oxide synthase |
| Notch1 | Neurogenic locus notch homolog protein 1 |
| NOX | Nitric oxidase |
| Nrf2 | Nuclear factor-E2 related factor 2 |
| OS | Oxidative stress |
| OVA | Ovalbumin |
| OXSR1 | Oxidative stress responsive kinase 1 |
| P53 | Protein 53 |
| PARP-1 | Poly[ADP-ribose] polymerase 1 |
| PDGF | Platelet-derived growth factor |
| PEFR | Peak expiratory flow rate |
| PGF2 | Prostaglandin F2 |
| PI3K | Phosphatidylinositol-3 kinase |
| PPBP | Pro-platelet basic protein |
| QoL | Quality of life |
| RA | Retinoic acid |
| RARs | Retinoic acid receptors |
| RXRs | Retinoid X receptors |
| RCTs | Randomised controlled trials |
| ROS | Reactive oxygen species |
| Se | Selenium |
| SHS | Secondhand smoke |
| SIRT1 | Sirtuin1 |
| SLC-39 | Solute carrier family 39 |
| SOD | Superoxide dismutase |
| TBARS | Thiobarbituric acid reactive substances |
| TGF-β1 | Transforming growth factor beta 1 |
| Th | T-helper |
| TLR | Toll-like receptors |
| TNF-α | Tumor necrosis factor α |
| TNFRSF11A | TNF receptor superfamily member 11a |
| VA | Vitamin A |
| VC | Vitamin C |
| VD | Vitamin D |
| VE | Vitamin E |
| Zn | Zinc |
References
- Gan, H.; Hou, X.; Zhu, Z.; Xue, M.; Zhang, T.; Huang, Z.; Cheng, Z.J.; Sun, B. Smoking: a leading factor for the death of chronic respiratory diseases derived from Global Burden of Disease Study 2019. BMC Pulm Med. 2022, 22, 149. [Google Scholar] [CrossRef]
- Institute for Health Metrics and Evaluation. Global Burden of Disease 2017. 2017. Available online: http://vizhub.healthdata.org/gbd-compare/# (accessed on 6 March 2023).
- Aoshiba, K.; Nagai, A. Differences in airway remodeling between asthma and chronic obstructive pulmonary disease. Clin Rev Allergy Immunol. 2004, 27, 35–43. [Google Scholar] [CrossRef]
- Doeing, D.C.; Solway, J. Airway smooth muscle in the pathophysiology and treatment of asthma. J. Appl. Physiol. 2013, 114, 834–843. [Google Scholar] [CrossRef] [PubMed]
- Kume, H. Role of airway smooth muscle in inflammation related to asthma and COPD. Adv Exp Med Biol. 2021, 1303, 139–172. [Google Scholar] [PubMed]
- Shimoda, T.; Obase, Y.; Kishikawa, R.; Iwanaga, T. Influence of cigarette smoking on airway inflammation and inhaled corticosteroid treatment in patients with asthma. Allergy Asthma Proc. 2016, 37, 50–58. [Google Scholar] [CrossRef] [PubMed]
- Tommola, M.; Ilmarinen, P.; Tuomisto, L.E.; Haanpää, J.; Kankaanranta, T.; Niemelä, O.; Kankaanranta, H. The effect of smoking on lung function: A clinical study of adult-onset asthma. Eur Respir J. 2016, 48, 1298–1306. [Google Scholar] [CrossRef] [PubMed]
- Korsbæk, N.; Landt, E.M.; Dahl, M. Second-hand smoke exposure associated with risk of respiratory symptoms, asthma, and COPD in 20,421 adults from the General Population. J Asthma Allergy. 2021, 14, 1277–1284. [Google Scholar] [CrossRef]
- Keogan, S.; Alonso, T.; Sunday, S.; Tigova, O.; Fernández, E.; López, M.J.; Gallus, S.; Semple, S.; Tzortzi, A.; Boffi, R.; et al. Lung function changes in patients with chronic obstructive pulmonary disease (COPD) and asthma exposed to secondhand smoke in outdoor areas. J Asthma. 2021, 58, 1169–1175. [Google Scholar] [CrossRef]
- Coogan, P.F.; Castro-Webb, N.; Yu, J.; O’Connor, G.T.; Palmer, J.R.; Rosenberg, L. Active and passive smoking and the incidence of asthma in the Black Women’s Health Study. Am J Respir Crit Care Med. 2015, 191, 168–176. [Google Scholar] [CrossRef]
- Van der Toorn, M.; Rezayat, D.; Kauffman, H.F.; Bakker, S.J.L.; Gans, R.O.B.; Koëter, G.H.; Choi, A.M.K.; Van Oosterhout, A.J.M.; Slebos, D-J. Lipid-soluble components in cigarette smoke induce mitochondrial production of reactive oxygen species in lung epithelial cells. Am J Physiol Lung Cell Mol Physiol. 2009, 297, L109–L114. [Google Scholar] [CrossRef]
- Zhou, G.; Xiao, W.; Xu, C.; Hu, Y.; Wu, X.; Huang, F.; Lu, X.; Shi, C.; Wu, X. Chemical constituents of tobacco smoke induce the production of interleukin-8 in human bronchial epithelium, 16HBE cells. Tob Induc Dis. 2016, 14, 24. [Google Scholar] [CrossRef] [PubMed]
- Cipollina, C.; Bruno, A.; Fasola, S.; Cristaldi, M.; Patella, B.; Inguanta, R.; Vilasi, A.; Aiello, G.; La Grutta, S.; Torino, C.; et al. Cellular and molecular signatures of oxidative stress in bronchial epithelial cell models injured by cigarette smoke extract. Int J Mol Sci. 2022, 23, 1770. [Google Scholar] [CrossRef]
- Strzelak, A.; Ratajczak, A.; Adamiec, A.; Feleszko, W. Tobacco smoke induces and alters immune responses in the lung triggering inflammation, allergy, asthma and other lung diseases: A mechanistic review. Int J Environ Res Public Health. 2018, 15, 1033. [Google Scholar] [CrossRef] [PubMed]
- Alsharairi, N.A. Scutellaria baicalensis and their natural flavone compounds as potential medicinal drugs for the treatment of nicotine-induced non-small-cell lung cancer and asthma. Int. J. Environ. Res. Public Health 2021, 18, 5243. [Google Scholar] [CrossRef]
- Vonk, J.M.; Scholtens, S.; Postma, D.S.; Moffatt, M.F.; Jarvis, D.; Ramasamy, A.; Wjst, M.; Omenaas, E.R.; Bouzigon, E.; Demenais, F.; et al. Adult onset asthma and interaction between genes and active tobacco smoking: The GABRIEL consortium. PLoS One. 2017, 12, e0172716. [Google Scholar] [CrossRef] [PubMed]
- Uh, S-T. ; Park, J-S.; Koo, S-M.; Kim, Y-K.; Kim, K.U.; Kim, M-A.; Shin, S-W.; Son, J-H.; Park, H-W.; Shin, H.D.; et al. Association of genetic variants of NLRP4 with exacerbation of asthma: The effect of smoking. DNA Cell Biol. 2019, 38, 76–84. [Google Scholar] [CrossRef] [PubMed]
- Losol, P.; Kim, S.H.; Ahn, S.; Lee, S.; Choi, J-P. ; Kim, Y-H.; Hong, S-J.; Kim, B-S.; Chang, Y-S. Genetic variants in the TLR-related pathway and smoking exposure alter the upper airway microbiota in adult asthmatic patients. Allergy. 2021, 76, 3217–3220. [Google Scholar] [CrossRef] [PubMed]
- Kim, M-H. ; Chang, H.S.; Lee, J-U.; Shim, J-S.; Park, J-S.; Cho, Y-J.; Park, C-S. Association of genetic variants of oxidative stress responsive kinase 1 (OXSR1) with asthma exacerbations in non-smoking asthmatics. BMC Pulm Med. 2022, 22, 3. [Google Scholar]
- Belcaro, G.; Luzzi, R.; Cesinaro Di Rocco, P.; Cesarone, M.R.; Dugall, M.; Feragalli, B.; Errichi, B.M.; Ippolito, E.; Grossi, M.G.; Hosoi, M.; et al. Pycnogenol® improvements in asthma management. Panminerva Med. 2011, 53, 57–64. [Google Scholar]
- Thomson, N.C.; Spears, M. The influence of smoking on the treatment response in patients with asthma. Curr OpinAllergy Clin Immunol. 2005, 5, 57–63. [Google Scholar] [CrossRef]
- Thomson, N.C.; Shepherd, M.; Spears, M.; Chaudhuri, R. Corticosteroid insensitivity in smokers with asthma: clinicalevidence, mechanisms, and management. Treat Respir Med. 2006, 5, 467–481. [Google Scholar] [CrossRef] [PubMed]
- Chatkin, J.M.; Dullius, C.R. The management of asthmatic smokers. Asthma Res Pract. 2016, 2, 10. [Google Scholar] [CrossRef] [PubMed]
- Duman, B.; Borekci, S.; Akdeniz, N.; Gazioglu, S.B.; Deniz, G.; Gemicioglu, B. Inhaled corticosteroids’ effects on biomarkers in exhaled breath condensate and blood in patients newly diagnosed with asthma who smoke. J Asthma. 2022, 59, 1613–1620. [Google Scholar] [CrossRef] [PubMed]
- Alsharairi, N.A. The effects of dietary supplements on asthma and lung cancer risk in smokers and non-smokers: A review of the literature. Nutrients 2019, 11, 725. [Google Scholar] [CrossRef]
- Alsharairi, N.A. Supplements for smoking-related lung diseases. Encyclopedia 2021, 1, 76–86. [Google Scholar] [CrossRef]
- Alsharairi, N.A. Dietary antioxidants and lung cancer risk in smokers and non-smokers. Healthcare (Basel). 2022, 10, 2501. [Google Scholar] [CrossRef]
- Santillan, A.A.; Camargo, C.A., Jr.; Colditz, G.A. A meta-analysis of asthma and risk of lung cancer (United States). Cancer Causes Control 2003, 14, 327–334. [Google Scholar] [CrossRef]
- Rosenberger, A.; Bickeböller, H.; McCormack, V.; Brenner, D.R.; Duell, E.J.; Tjønneland, A.; Friis, S.; Muscat, J.E.; Yang, P.; Wichmann, H.E.; et al. Asthma and lung cancer risk: A systematic investigation by the International Lung Cancer Consortium. Carcinogenesis 2012, 33, 587–597. [Google Scholar] [CrossRef]
- Burns, J.S.; Dockery, D.W.; Neas, L.M.; Schwartz, J.; Coull, B.A.; Raizenne, M.; Speizer, F.E. Low dietary nutrient intakes and respiratory health in adolescents. Chest. 2007, 132, 238–245. [Google Scholar] [CrossRef]
- Zhang, W.; Li, W.; Du, J. Association between dietary carotenoid intakes and the risk of asthma in adults: a cross-sectional study of NHANES, 2007-2012. BMJ Open. 2022, 12, e052320. [Google Scholar] [CrossRef]
- Pearson, P.J.K.; Lewis, S.A.; Britton, J.; Fogarty, A. Vitamin E supplements in asthma: a parallel group randomised placebo controlled trial. Thorax. 2004, 59, 652–656. [Google Scholar] [CrossRef] [PubMed]
- Shaheen, S.O.; Newson, R.B.; Rayman, M.P.; Wong, A. P-L.; Tumilty, M.K.; Phillips, J.M.; Potts, J.F.; Kelly, F.J.; White, P.T.; Burney, P.G.J. Randomised, double blind, placebo-controlled trial of selenium supplementation in adult asthma. Thorax. 2007, 62, 483–490. [Google Scholar] [CrossRef] [PubMed]
- Van der Vaart, H.; Postma, D.S.; Timens, W.; Ten Hacken, N.H.T. Acute effects of cigarette smoke on inflammation and oxidative stress: a review. Thorax. 2004, 59, 713–721. [Google Scholar] [CrossRef] [PubMed]
- Yadav, A.S.; Saini, M. Evaluation of systemic antioxidant level and oxidative stress in relation to lifestyle and disease progression in asthmatic patients. J Med Biochem. 2016, 35, 55–62. [Google Scholar] [CrossRef] [PubMed]
- Bartoli, M.L.; Novelli, F.; Costa, F.; Malagrinò, L.; Melosini, L.; Bacci, E.; Cianchetti, S.; Dente, F.L.; Di Franco, A.; Vagaggini, B.; et al. Malondialdehyde in exhaled breath condensate as a marker of oxidative stress in different pulmonary diseases. Mediators Inflamm. 2011, 2011, 891752. [Google Scholar] [CrossRef]
- Anes, A.B.; Nasr, H.B.; Fetoui, H.; Bchir, S.; Chahdoura, H.; Yacoub, S.; Garrouch, A.; Benzarti, M.; Tabka, Z.; Chahed, K. Alteration in systemic markers of oxidative and antioxidative status in Tunisian patients with asthma: relationships with clinical severity and airflow limitation. J Asthma. 2016, 53, 227–237. [Google Scholar] [CrossRef]
- Mak, J.C.W.; Leung, H.C.M.; Ho, S.P.; Law, B.K.W.; Lam, W.K.; Tsang, K.W.T.; Ip, M.C.M.; Chan-Yeung, M. Systemic oxidative and antioxidative status in Chinese patients with asthma. J Allergy Clin Immunol. 2004, 114, 260–264. [Google Scholar] [CrossRef]
- Ueno, T.; Kataoka, M.; Hirano, A.; Iio, K.; Tanimoto, Y.; Kanehiro, A.; Okada, C.; Soda, R.; Takahashi, K.; Tanimoto, M. Inflammatory markers in exhaled breath condensate from patients with asthma. Respirology. 2008, 13, 654–663. [Google Scholar] [CrossRef]
- Hillas, G.; Kostikas, K.; Mantzouranis, K.; Bessa, V.; Kontogianni, K.; Papadaki, G.; Papiris, S.; Alchanatis, M.; Loukides, S.; Bakakos, P. Exhaled nitric oxide and exhaled breath condensate pH as predictors of sputum cell counts in optimally treated asthmatic smokers. Respirology. 2011, 16, 811–818. [Google Scholar] [CrossRef]
- Michils, A.; Louis, R.; Peché, R.; Baldassarre, S.; Van Muylem, A. Exhaled nitric oxide as a marker of asthma control in smoking patients. Eur Respir J. 2009, 33, 1295–1301. [Google Scholar] [CrossRef]
- Emma, R.; Bansal, A.T.; Kolmert, J.; Wheelock, C.E.; Dahlen, S-E. ; Loza, M.J.; De Meulder, B.; Lefaudeux, D.; Auffray, C.; Dahlen, B.; et al. Enhanced oxidative stress in smoking and ex-smoking severe asthma in the U-BIOPRED cohort. PLoS One. 2018, 13, e0203874. [Google Scholar] [CrossRef] [PubMed]
- Telenga, E.D.; Kerstjens, H.A.M.; Ten Hacken, N.H.T.; Postma, D.S.; van den Berge, M. Inflammation and corticosteroid responsiveness in ex-, current- and never-smoking asthmatics. BMC Pulm Med. 2013, 13, 58. [Google Scholar] [CrossRef] [PubMed]
- Takahashi, K.; Pavlidis, S.; Kwong, F.N.K.; Hoda, U.; Rossios, C.; Sun, K.; Loza, M.; Baribaud, F.; Chanez, P.; Fowler, S.J.; et al. Sputum proteomics and airway cell transcripts of current and ex-smokers with severe asthma in U-BIOPRED: an exploratory analysis. Eur Respir J. 2018, 51, 1702173. [Google Scholar] [CrossRef] [PubMed]
- Thomson, N.C.; Chaudhuri, R.; Heaney, L.G.; Bucknall, C.; Niven, R.M.; Brightling, C.E.; Menzies-Gow, A.N.; Mansur, A.H.; McSharry, C. Clinical outcomes and inflammatory biomarkers in current smokers and exsmokers with severe asthma. J Allergy Clin Immunol. 2013, 131, 1008–1016. [Google Scholar] [CrossRef] [PubMed]
- Gao, J.; Wu, F. Association between fractional exhaled nitric oxide, sputum induction and peripheral blood eosinophil in uncontrolled asthma. Allergy Asthma Clin Immunol. 2018, 14, 21. [Google Scholar] [CrossRef] [PubMed]
- Pavlidis, S.; Takahashi, K.; Kwong, F.N.K.; Xie, J.; Hoda, U.; Sun, K.; Elyasigomari, V.; Agapow, P.; Loza, M.; Baribaud, F.; et al. “T2-high” in severe asthma related to blood eosinophil, exhaled nitric oxide and serum periostin. Eur Respir J. 2019, 53, 1800938. [Google Scholar] [CrossRef] [PubMed]
- Sahoo, R.C.; Acharya, P.R.; Noushad, T.H.; Anand, R.; Acharya, V.K.; Sahu, K.R. A study of high-sensitivity C-reactive protein in bronchial asthma. Indian J Chest Dis Allied Sci. 2009, 51, 213–216. [Google Scholar]
- Huang, C-C. ; Wang, C-H.; Wu, P-W.; He, J-R.; Huang, C-C.; Chang, P-H.; Fu, C-H.; Lee, T-J. Increased nasal matrix metalloproteinase-1 and -9 expression in smokers with chronic rhinosinusitis and asthma. Scientific Reports. 2019, 9, 15357.
- Chaudhuri, R.; McSharry, C.; Brady, J.; Donnelly, I.; Grierson, C.; McGuinness, S.; Jolly, L.; Weir, C.J.; Messow, C.M.; Spears, M.; et al. Sputum matrix metalloproteinase-12 in patients with chronic obstructive pulmonary disease and asthma: relationship to disease severity. J Allergy Clin Immunol. 2012, 129, 655–663. [Google Scholar] [CrossRef]
- Huang, C-C. ; Wang, C-H.; Fu, C-H.; Huang, C-C.; Chang, P-H.; Chen, Y-W.; Wu, C-C.; Wu, P-W.; Lee, T-J. Association between cigarette smoking and interleukin-17A expression in nasal tissues of patients with chronic rhinosinusitis and asthma. Medicine (Baltimore). 2016, 95, e5432. [Google Scholar] [CrossRef]
- Chalmers, G.W.; MacLeod, K.J.; Thomson, L.; Little, S.A.; McSharry, C.; Thomson, N.C. Smoking and airway inflammation in patients with mild asthma. Chest. 2001, 120, 1917–1922. [Google Scholar] [CrossRef] [PubMed]
- Rossios, C.; Pavlidis, S.; Hoda, U.; Kuo, C-H. ; Wiegman, C.; Russell, K.; Sun, K.; Loza, M.J.; Baribaud, F.; Durham, A.L.; et al. Sputum transcriptomics reveal upregulation of IL-1 receptor family members in patients with severe asthma. J Allergy Clin Immunol. 2018, 141, 560–570. [Google Scholar] [CrossRef] [PubMed]
- Ham, J.; Kim, J.; Sohn, K-H. ; Park, I-W.; Choi, B-W.; Chung, D.H.; Cho, S-H.; Kang, H.R.; Jung, J-W.; Kim, H.Y. Cigarette smoke aggravates asthma by inducing memory-like type 3 innate lymphoid cells. Nat Commun. 2022, 4, 13–3852. [Google Scholar]
- Krisiukeniene, A.; Babusyte, A.; Stravinskaite, K.; Lotvall, J.; Sakalauskas, R.; Sitkauskiene, B. Smoking affects eotaxin levels in asthma patients. J Asthma. 2009, 46, 470–476. [Google Scholar] [CrossRef]
- Deveci, F.; Ilhan, N.; Turgut, T.; Akpolat, N.; Kirkil, G.; Muz, M.H. Glutathione and nitrite in induced sputum from patients with stable and acute asthma compared with controls. Ann Allergy Asthma Immunol. 2004, 93, 91–97. [Google Scholar] [CrossRef]
- Nadeem, A.; Chhabra, S.K.; Masood, A.; Raj, H.G. Increased oxidative stress and altered levels of antioxidants in asthma. J Allergy Clin Immunol. 2003, 111, 72–78. [Google Scholar] [CrossRef] [PubMed]
- Chamitava, L.; Cazzoletti, L.; Ferrari, M.; Garcia-Larsen, V.; Jalil, A.; Degan, P.; Fois, A.G.; Zinellu, E.; Fois, S.S.; Pasini, A.M.F.; et al. Biomarkers of oxidative stress and inflammation in chronic airway diseases. Int J Mol Sci. 2020, 21, 4339. [Google Scholar] [CrossRef]
- Nerpin, E.; Ferreira, D.S.; Weyler, J.; Schlunnsen, V.; Jogi, R.; Semjen, C.R.; Gislasson, T.; Demoly, P.; Heinrich, J.; Nowak, D.; et al. Bronchodilator response and lung function decline: Associations with exhaled nitric oxide with regard to sex and smoking status. World Allergy Organ J. 2021, 14, 100544. [Google Scholar] [CrossRef]
- Malinovschi, A.; Backer, V.; Harving, H.; Porsbjerg, C. The value of exhaled nitric oxide to identify asthma in smoking patients with asthma-like symptoms. Respir Med. 2012, 106, 794–801. [Google Scholar] [CrossRef]
- Giovannelli, J.; Chérot-Kornobis, N.; Hulo, S.; Ciuchete, A.; Clément, G.; Amouyel, P.; Matran, R.; Dauchet, L. Both exhaled nitric oxide and blood eosinophil count were associated with mild allergic asthma only in non-smokers. Clin Exp Allergy. 2016, 46, 543–554. [Google Scholar] [CrossRef]
- Kostikas, K.; Papaioannou, A.I.; Tanou, K.; Giouleka, P.; Koutsokera, A.; Minas, M.; Papiris, S.; Gourgoulianis, K.I.; Taylor, D.R.; et al. Exhaled NO and exhaled breath condensate pH in the evaluation of asthma control. Respiratory Medicine. 2011, 105, 526e532. [Google Scholar] [CrossRef] [PubMed]
- Thomson, N.C.; Chaudhuri, R.; Spears, M.; Haughney, J.; McSharry, C. Serum periostin in smokers and never smokers with asthma. Respir Med. 2015, 109, 708–7015. [Google Scholar] [CrossRef] [PubMed]
- Cianchetti, S.; Cardini, C.; Puxeddu, I.; Latorre, M.; Bartoli, M.L.; Bradicich, M.; Dente, F.; Bacci, E.; Celi, A.; Paggiaro, P. Distinct profile of inflammatory and remodelling biomarkers in sputum of severe asthmatic patients with or without persistent airway obstruction. World Allergy Organ J. 2019, 12, 100078. [Google Scholar] [CrossRef] [PubMed]
- Yildiz, H.; Alp, H.H.; Sünnetçioğlu, A.; Ekin, S.; Çilingir, B.M. Evaluation serum levels of YKL-40, Periostin, and some inflammatory cytokines together with IL-37, a new anti-inflammatory cytokine, in patients with stable and exacerbated asthma. Heart Lung. 2021, 50, 177–183. [Google Scholar] [CrossRef] [PubMed]
- Rovina, N.; Dima, E.; Gerassimou, C.; Kollintza, A.; Gratziou, C.; Roussos, C. IL-18 in induced sputum and airway hyperresponsiveness in mild asthmatics: effect of smoking. Respir Med. 2009, 103, 1919–1925. [Google Scholar] [CrossRef] [PubMed]
- Zietkowski, Z.; Tomasiak-Lozowska, M.M.; Skiepko, R.; Zietkowska, E.; Bodzenta-Lukaszyk, A. Eotaxin-1 in exhaled breath condensate of stable and unstable asthma patients. Respir Res. 2010, 11, 110. [Google Scholar] [CrossRef]
- Chu, S.; Ma, L.; Wei, J.; Wang, J.; Xu, Q.; Chen, M.; Jiang, M.; Luo, M.; Wu, J.; Mai, L.; et al. Smoking status modifies the relationship between Th2 biomarkers and small airway obstruction in asthma. Can Respir J. 2021, 2021, 1918518. [Google Scholar] [CrossRef]
- Mikus, M.S.; Kolmert, J.; Andersson, L.I.; Östling, J.; Knowles, R.G.; Gómez, C.; Ericsson, M.; Thörngren, J-O. ; Khoonsari, P.E.; Dahlén, B.; et al. Plasma proteins elevated in severe asthma despite oral steroid use and unrelated to Type-2 inflammation. Eur Respir J. 2022, 59, 2100142. [Google Scholar] [CrossRef]
- Liu, T.; Wu, J.; Zhao, J.; Wang, J.; Zhang, Y.; Liu, L.; Cao, L.; Liu, Y.; Dong, L. Type 2 innate lymphoid cells: A novel biomarker of eosinophilic airway inflammation in patients with mild to moderate asthma. Respir Med. 2015, 109, 1391–1396. [Google Scholar] [CrossRef]
- Halvani, A.; Tahghighi, F.; Nadooshan, H.H. Evaluation of correlation between airway and serum inflammatory markers in asthmatic patients. Lung India. 2012, 29, 143–146. [Google Scholar] [CrossRef]
- Shimoda, T.; Obase, Y.; Kishikawa, R.; Iwanaga, T. Serum high-sensitivity C-reactive protein can be an airway inflammation predictor in bronchial asthma. Allergy Asthma Proc. 2015, 36, e23–e28. [Google Scholar] [CrossRef] [PubMed]
- Timoneda, J.; Rodríguez-Fernández, L.; Zaragozá, R.; Marín, M.P.; Cabezuelo, M.T.; Torres, L.; Viña, J.R.; Barber, T. Vitamin A deficiency and the lung. Nutrients. 2018, 10, 1132. [Google Scholar] [CrossRef] [PubMed]
- Defnet, A.E.; Shah, S.D.; Huang, W.; Shapiro, P.; Deshpande, D.A.; Kane, M.A. Dysregulated retinoic acid signaling in airway smooth muscle cells in asthma. FASEB J. 2021, 35, e22016. [Google Scholar] [CrossRef]
- Druilhe, A.; Zahm, J-M. ; Benayoun, L.; El Mehdi, D.; Grandsaigne, M.; Dombret, M-C.; Mosnier, I.; Feger, B.; Depondt, J.; Aubier, M.; et al. Epithelium expression and function of retinoid receptors in asthma. Am J Respir Cell Mol Biol. 2008, 38, 276–282. [Google Scholar] [CrossRef]
- Day, R.M.; Lee, Y.H.; Park, A-M. ; Suzuki, Y.J. Retinoic acid inhibits airway smooth muscle cell migration. Am J Respir Cell Mol Biol. 2006, 34, 695–703. [Google Scholar] [CrossRef] [PubMed]
- Callaghan, P.J.; Rybakovsky, E.; Ferrick, B.; Thomas, S.; Mullin, J.M. Retinoic acid improves baseline barrier function and attenuates TNF-α-induced barrier leak in human bronchial epithelial cell culture model, 16HBE 14o. PLoS One. 2020, 15, e0242536. [Google Scholar] [CrossRef]
- Wu, J.; Zhang, Y.; Liu, Q.; Zhong, W.; Xia, Z. All-trans retinoic acid attenuates airway inflammation by inhibiting Th2 and Th17 response in experimental allergic asthma. BMC Immunol. 2013, 14, 28. [Google Scholar] [CrossRef]
- Takamura, K.; Nasuhara, Y.; Kobayashi, M.; Betsuyaku, T.; Tanino, Y.; Kinoshita, I.; Yamaguchi, E.; Matsukura, S.; Schleimer, R.P.; Nishimura, M. Retinoic acid inhibits interleukin-4-induced eotaxin production in a human bronchial epithelial cell line. Am J Physiol Lung Cell Mol Physiol. 2004, 286, L777–L785. [Google Scholar] [CrossRef]
- Kurie, J.M.; Lotan, R.; Lee, J.J.; Lee, J.S.; Morice, R.C.; Liu, D.D.; Xu, X-C. ; Khuri, F.R.; Ro, J.Y.; Hittelman, W.N.; Walsh, G.L.; et al. Treatment of former smokers with 9-cis-retinoic acid reverses loss of retinoic acid receptorbeta expression in the bronchial epithelium: results from a randomized placebo-controlled trial. J Natl Cancer Inst. 2003, 95, 206–214. [Google Scholar] [CrossRef]
- Frankenberger, M.; Heimbeck, I.; Möller, W.; Mamidi, S.; Kaßner, G.; Pukelsheim, K.; Wjst, M.; Neiswirth, M.; Kroneberg, P.; Lomas, D.; et al. Inhaled all-trans retinoic acid in an individual with severe emphysema. European Respiratory J. 2009, 34, 1487–1489. [Google Scholar] [CrossRef]
- Saini, R.K.; Prasad, P.; Lokesh, V.; Shang, X.; Shin, J.; Keum, Y-S. ; Lee, J-H. Carotenoids: Dietary sources, extraction, encapsulation, bioavailability, and health benefits-A review of recent advancements. Antioxidants (Basel). 2022, 11, 795. [Google Scholar] [CrossRef] [PubMed]
- Park, H.S.; Kim, S.R.; Kim, J.O.; Lee, Y.C. The roles of phytochemicals in bronchial asthma. Molecules. 2010, 15, 6810–6834. [Google Scholar] [CrossRef] [PubMed]
- Arora, A.; Willhite, C.A.; Liebler, D.C. Interactions of beta-carotene and cigarette smoke in human bronchial epithelial cells. Carcinogenesis. 2001, 22, 1173–1178. [Google Scholar] [CrossRef] [PubMed]
- Prakash, P.; Liu, C.; Hu, K-Q. ; Krinsky, N.I.; Russell, R.M.; Wang, X-D. Beta-carotene and beta-apo-14’-carotenoic acid prevent the reduction of retinoic acid receptor beta in benzo[a]pyrene-treated normal human bronchial epithelial cells. J Nutr. 2004, 134, 667–673. [Google Scholar] [CrossRef]
- Hazlewood, L.C.; Wood, L.G.; Hansbro, P.M.; Foster, P.S. Dietary lycopene supplementation suppresses Th2 responses and lung eosinophilia in a mouse model of allergic asthma. J Nutr Biochem. 2011, 22, 95–100. [Google Scholar] [CrossRef]
- Lian, F.; Wang, X-D. Enzymatic metabolites of lycopene induce Nrf2-mediated expression of phase II detoxifying/antioxidant enzymes in human bronchial epithelial cells. Int J Cancer. 2008, 123, 1262–1268. [Google Scholar] [CrossRef]
- Chiaverelli, R.A.; Hu, K.-Q.; Liu, C.; Lim, J.Y.; Daniels, M.S.; Xia, H.; Mein, J.; von Lintig, J.; Wang, X.-D. β-Cryptoxanthin attenuates cigarette-smoke-induced lung lesions in the absence of carotenoid cleavage enzymes (BCO1/BCO2) in mice. Molecules. 2023, 28, 1383. [Google Scholar] [CrossRef]
- Liu, C.; Bronson, R.T.; Russell, R.M.; Wang, X.-D. β-Cryptoxanthin supplementation prevents cigarette smoke-induced lung inflammation, oxidative damage, and squamous metaplasia in ferrets. Cancer Prev. Res. 2011, 4, 1255–1266. [Google Scholar] [CrossRef]
- Allen, S.; Britton, J.R.; Leonardi-Bee, J.A. Association between antioxidant vitamins and asthma outcome measures: systematic review and meta-analysis. Thorax. 2009, 64, 610–619. [Google Scholar] [CrossRef]
- Tecklenburg, S.L.; Mickleborough, T.D.; Fly, A.D.; Bai, Y.; Stager, J.M. Ascorbic acid supplementation attenuates exercise-induced bronchoconstriction in patients with asthma. Respir Med. 2007, 101, 1770–1778. [Google Scholar] [CrossRef]
- Chang, H-H. ; Chen, C-S.; Lin, J-Y. High dose vitamin C supplementation increases the Th1/Th2 cytokine secretion ratio, but decreases eosinophilic infiltration in bronchoalveolar lavage fluid of ovalbumin-sensitized and challenged mice. J Agric Food Chem. 2009, 57, 10471–10476. [Google Scholar] [CrossRef] [PubMed]
- Zhu, W.; Cromie, M.M.; Cai, Q.; Lv, T.; Singh, K.; Gao, W. Curcumin and vitamin E protect against adverse effects of benzo[a]pyrene in lung epithelial cells. PLoS One. 2014, 9, e92992. [Google Scholar] [CrossRef] [PubMed]
- Hoskins, A.; Roberts, J.L.; Milne, G.; Choi, L.; Dworski, R. Natural-source d-α-tocopheryl acetate inhibits oxidant stress and modulates atopic asthma in humans in vivo. Allergy. 2012, 67, 676–682. [Google Scholar] [CrossRef] [PubMed]
- Wiser, J.; Alexis, N.E.; Jiang, Q.; Wu, W.; Robinette, C.; Roubey, R.; Peden, D.B. In vivo gamma-tocopherol supplementation decreases systemic oxidative stress and cytokine responses of human monocytes in normal and asthmatic subjects. Free Radic Biol Med. 2008, 45, 40–49. [Google Scholar] [CrossRef] [PubMed]
- Hernandez, M.L.; Wagner, J.G.; Kala, A.; Mills, K.; Wells, H.B.; Alexis, N.E.; Lay, J.C.; Jiang, Q.; Zhang, H.; Zhou, H.; et al. Vitamin E, γ-tocopherol, reduces airway neutrophil recruitment after inhaled endotoxin challenge in rats and in healthy volunteers. Free Radic Biol Med. 2013, 60, 56–62. [Google Scholar] [CrossRef]
- Burbank, A.J.; Duran, C.G.; Pan, Y.; Burns, P.; Jones, S.; Jiang, Q.; Yang, C.; Jenkins, S.; Wells, H.; Alexis, N.; et al. Gamma tocopherol-enriched supplement reduces sputum eosinophilia and endotoxin-induced sputum neutrophilia in volunteers with asthma. J Allergy Clin Immunol. 2018, 141, 1231–1238. [Google Scholar] [CrossRef]
- Talati, M.; Meyrick, B.; Peebles Jr, R.S.; Davies, S.S.; Dworski, R.; Mernaugh, R.; Mitchell, D.; Boothby, M.; Roberts, L.J.; Sheller, J.R. Oxidant stress modulates murine allergic airway responses. Free Radic Biol Med. 2006, 40, 1210–1219. [Google Scholar] [CrossRef]
- Quoc, Q.L.; Bich, T.C.T.; Kim, S-H. ; Park, H-S.; Shin, Y.S. Administration of vitamin E attenuates airway inflammation through restoration of Nrf2 in a mouse model of asthma. J Cell Mol Med. 2021, 25, 6721–6732. [Google Scholar] [CrossRef]
- Li, J.; Li, L.; Chen, H.; Chang, Q.; Liu, X.; Wu, Y.; Wei, C.; Li, R.; Kwan, J.K.C.; Yeung, K.L.; et al. Application of vitamin E to antagonize SWCNTs-induced exacerbation of allergic asthma. Sci Rep. 2014, 4, 4275. [Google Scholar] [CrossRef]
- Mabalirajan, U.; Aich, J.; Leishangthem, G.D.; Sharma, S.K.; Dinda, A.K.; Ghosh, B. Effects of vitamin E on mitochondrial dysfunction and asthma features in an experimental allergic murine model. J Appl Physiol (1985). 2009, 107, 1285–1292. [Google Scholar] [CrossRef]
- McCary, C.A.; Abdala-Valencia, H.; Berdnikovs, S.; Cook-Mills, J.M. Supplemental and highly elevated tocopherol doses differentially regulate allergic inflammation: reversibility of α-tocopherol and γ-tocopherol’s effects. J Immunol. 2011, 186, 3674–3685. [Google Scholar] [CrossRef] [PubMed]
- Hall, S.C.; Agrawal, D.K. Vitamin D and bronchial asthma: An overview of data from the past 5 years. Clin Ther. 2017, 39, 917–929. [Google Scholar] [CrossRef] [PubMed]
- Pfeffer, P.E.; Lu, H.; Mann, E.H.; Chen, Y-H. ; Ho, T-R.; Cousins, D.J.; Corrigan, C.; Kelly, F.J.; Mudway, I.S.; Hawrylowicz, C.M. Effects of vitamin D on inflammatory and oxidative stress responses of human bronchial epithelial cells exposed to particulate matter. PLoS One. 2018, 13, e0200040. [Google Scholar] [CrossRef] [PubMed]
- Ramos-Martínez, E.; López-Vancell, M.R.; Fernández de Córdova-Aguirre, J.C.; Rojas-Serrano, J.; Chavarría, A.; Velasco-Medina, A.; Velázquez-Sámano, G. Reduction of respiratory infections in asthma patients supplemented with vitamin D is related to increased serum IL-10 and IFNγ levels and cathelicidin expression. Cytokine. 2018, 108, 239–246. [Google Scholar] [CrossRef] [PubMed]
- Adam-Bonci, T-I. ; Bonci, E-A.; Pârvu, A-E.; Herdean, A-I.; Moț, A.; Taulescu, M.; Ungur, A.; Pop, R-M.; Bocșan, C.; Irimie, A. Vitamin D supplementation: Oxidative stress modulation in a mouse model of ovalbumin-induced acute asthmatic airway inflammation. Int J Mol Sci. 2021, 22, 7089. [Google Scholar] [CrossRef] [PubMed]
- Huang, C.; Peng, M.; Tong, J.; Zhong, X.; Xian, J.; Zhong, L.; Deng, J.; Huang, Y. Vitamin D ameliorates asthma-induced lung injury by regulating HIF-1α/Notch1 signaling during autophagy. Food Sci Nutr. 2022, 10, 2773–2785. [Google Scholar] [CrossRef] [PubMed]
- Fischer, K.D.; Hall, S.C.; Agrawal, D.K. Vitamin D supplementation reduces induction of epithelial-mesenchymal transition in allergen sensitized and challenged mice. PLoS One. 2016, 11, e0149180. [Google Scholar] [CrossRef] [PubMed]
- Gorman, S.; Weeden, C.E.; Tan, D.H.W.; Scott, N.M.; Hart, J.; Foong, R.E.; Mok, D.; Stephens, N.; Zosky, G.; Hart, P.H. Reversible control by vitamin D of granulocytes and bacteria in the lungs of mice: an ovalbumin-induced model of allergic airway disease. PLoS One. 2013, 8, e67823. [Google Scholar] [CrossRef]
- Taher, Y.A.; van Esch, B.C.A.M.; Hofman, G.A.; Henricks, P.A.J.; van Oosterhout, A.J.M. 1alpha,25-dihydroxyvitamin D3 potentiates the beneficial effects of allergen immunotherapy in a mouse model of allergic asthma: role for IL-10 and TGF-beta. J Immunol. 2008, 180, 5211–5221. [Google Scholar] [CrossRef]
- Agrawal, T.; Gupta, G.K.; Agrawal, D.K. Vitamin D supplementation reduces airway hyperresponsiveness and allergic airway inflammation in a murine model. Clin Exp Allergy. 2013, 43, 672–683. [Google Scholar] [CrossRef]
- Zhang, H.; Yang, N.; Wang, T.; Dai, B.; Shang, Y. Vitamin D reduces inflammatory response in asthmatic mice through HMGB1/TLR4/NF-κB signaling pathway. Mol Med Rep. 2018, 17, 2915–2920. [Google Scholar] [PubMed]
- Ekmekci, O.P.; Donma, O.; Sardoğan, E.; Yildirim, N.; Uysal, O.; Demirel, H.; Demir, T. Iron, nitric oxide, and myeloperoxidase in asthmatic patients. Biochemistry (Mosc). 2004, 69, 462–467. [Google Scholar] [CrossRef] [PubMed]
- Narula, M.K.; Ahuja, G.K.; Whig, J.; Narang, A.P.S.; Soni, R.K. Status of lipid peroxidation and plasma iron level in bronchial asthmatic patients. Indian J Physiol Pharmacol. 2007, 51, 289–292. [Google Scholar] [PubMed]
- Han, F.; Li, S.; Yang, Y.; Bai, Z. Interleukin-6 promotes ferroptosis in bronchial epithelial cells by inducing reactive oxygen species-dependent lipid peroxidation and disrupting iron homeostasis. Bioengineered. 2021, 12, 5279–5288. [Google Scholar] [CrossRef] [PubMed]
- Kuribayashi, K.; Iida, S-I. ; Nakajima, Y.; Funaguchi, N.; Tabata, C.; Fukuoka, K.; Fujimori, Y.; Ihaku, D.; Nakano, T. Suppression of heme oxygenase-1 activity reduces airway hyperresponsiveness and inflammation in a mouse model of asthma. J Asthma. 2015, 52, 662–668. [Google Scholar] [CrossRef] [PubMed]
- Ghio, A.J.; Hilborn, E.D. Indices of iron homeostasis correlate with airway obstruction in an NHANES III cohort. Int J Chron Obstruct Pulmon Dis. 2017, 12, 2075–2084. [Google Scholar] [CrossRef]
- Ghio, A.J.; Hilborn, E.D.; Stonehuerner, J.G.; Dailey, L.A.; Carter, J.D.; Richards, J.H.; Crissman, K.M.; Foronjy, R.F.; Uyeminami, D.L.; Pinkerton, K.E. Particulate matter in cigarette smoke alters iron homeostasis to produce a biological effect. Am J Respir Crit Care Med. 2008, 178, 1130–1138. [Google Scholar] [CrossRef]
- Zajac, D. Mineral micronutrients in asthma. Nutrients. 2021, 13, 4001. [Google Scholar] [CrossRef]
- Fahmy, B.; Cormier, S.A. Copper oxide nanoparticles induce oxidative stress and cytotoxicity in airway epithelial cells. Toxicol In Vitro. 2009, 23, 1365–1371. [Google Scholar] [CrossRef]
- Park, J-W. ; Lee, I-C.; Shin, N-R.; Jeon, C-M.; Kwon, O-K.; Ko, J-W.; Kim, J-C.; Oh, S-R.; Shin, I-S.; Ahn, K-S. Copper oxide nanoparticles aggravate airway inflammation and mucus production in asthmatic mice via MAPK signaling. Nanotoxicology. 2016, 10, 445–452. [Google Scholar] [CrossRef]
- Sagdic, A.; Sener, O.; Bulucu, F.; Karadurmus, N.; Özel, H.E.; Yamanel, L.; Tasci, C.; Naharci, I.; Ocal, R. ; Aydin Oxidative stress status and plasma trace elements in patients with asthma or allergic rhinitis. Allergol Immunopathol(Madr). 2011, 39, 200–205. [Google Scholar] [CrossRef]
- Guo, C-H. ; Liu, P-J.; Hsia, S.; Chuang, C-J.; Chen, P-C. Role of certain trace minerals in oxidative stress, inflammation, CD4/CD8 lymphocyte ratios and lung function in asthmatic patients. Ann Clin Biochem. 2011, 48, 344–351. [Google Scholar] [CrossRef]
- Mao, S.; Wu, L.; Shi, W. Association between trace elements levels and asthma susceptibility. Respir Med. 2018, 145, 110–119. [Google Scholar] [CrossRef]
- Richter, M.; Cantin, A.M.; Beaulieu, C.; Cloutier, A.; Larivée. P. Zinc chelators inhibit eotaxin, RANTES, and MCP-1 production in stimulated human airway epithelium and fibroblasts. Am J Physiol Lung Cell Mol Physiol. 2003, 285, L719–L729. [Google Scholar] [CrossRef]
- Lang, C.; Murgia, C.; Leong, M.; Tan, L-W. ; Perozzi, G.; Knight, D.; Ruffin, R.; Zalewski, P. Anti-inflammatory effects of zinc and alterations in zinc transporter mRNA in mouse models of allergic inflammation. Am J Physiol Lung Cell Mol Physiol. 2007, 292, L577–L584. [Google Scholar] [CrossRef]
- Lu, H.; Xin, Y.; Tang, Y.; Shao, G. Zinc suppressed the airway inflammation in asthmatic rats: effects of zinc on generation of eotaxin, MCP-1, IL-8, IL-4, and IFN-γ. Biol Trace Elem Res. 2012, 150, 314–321. [Google Scholar] [CrossRef]
Figure 1.
Schematic diagram of the OS and inflammatory biomarkers in smoking asthmatics. Smokers have higher levels of OS and inflammatory biomarkers. High levels of enzymatic antioxidants (GPx,SOD, and GSH) and low levels of FeNO were inadequate to protect smokers from oxidative damage in the airway. (↓) decrease, (↑) increase.
Figure 1.
Schematic diagram of the OS and inflammatory biomarkers in smoking asthmatics. Smokers have higher levels of OS and inflammatory biomarkers. High levels of enzymatic antioxidants (GPx,SOD, and GSH) and low levels of FeNO were inadequate to protect smokers from oxidative damage in the airway. (↓) decrease, (↑) increase.
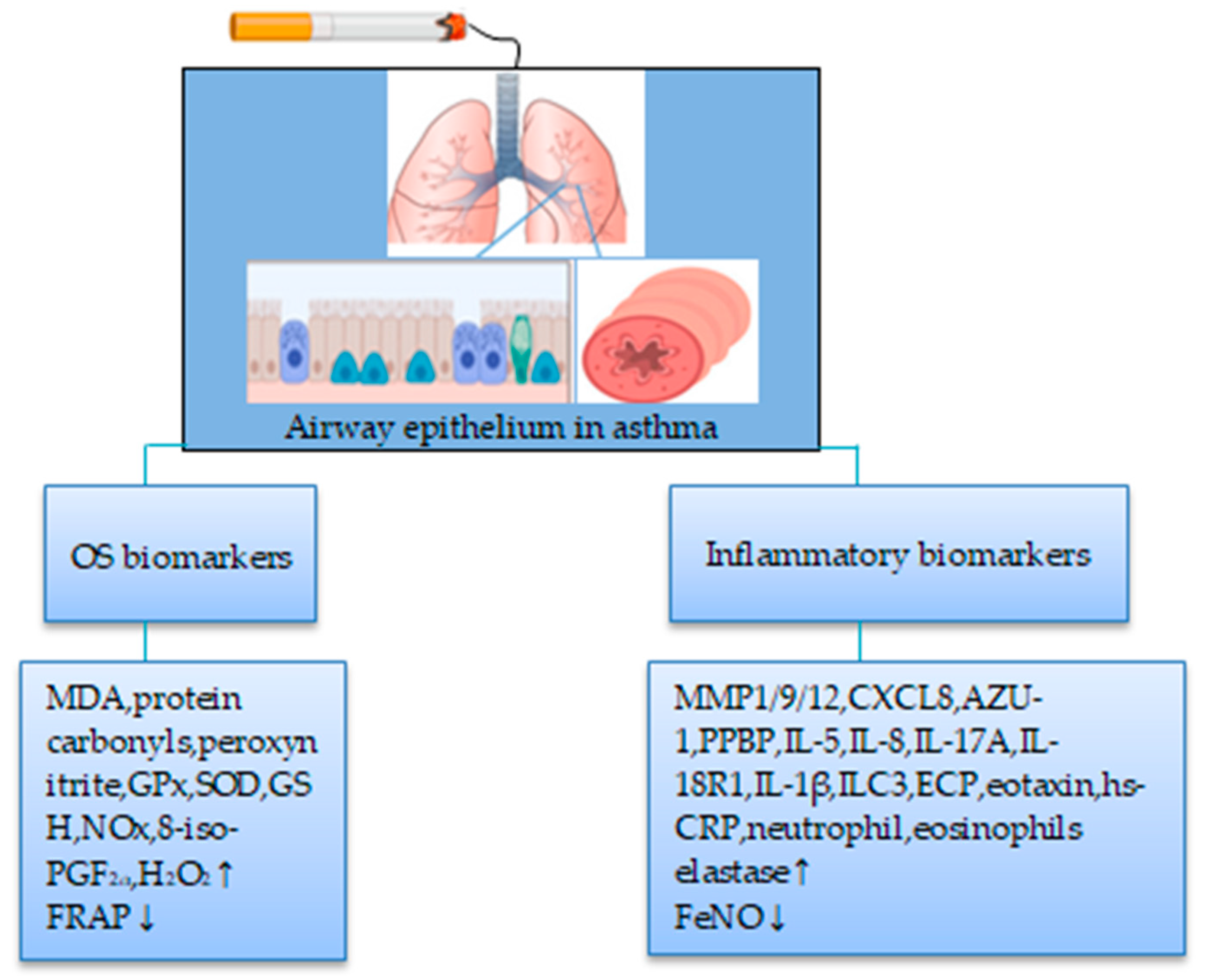
Figure 2.
Schematic diagram of the OS and inflammatory biomarkers in nonsmoking asthmatics. Nonsmokers have higher levels of inflammatory than OS biomarkers. (↓) decrease, (↑) increase.
Figure 2.
Schematic diagram of the OS and inflammatory biomarkers in nonsmoking asthmatics. Nonsmokers have higher levels of inflammatory than OS biomarkers. (↓) decrease, (↑) increase.
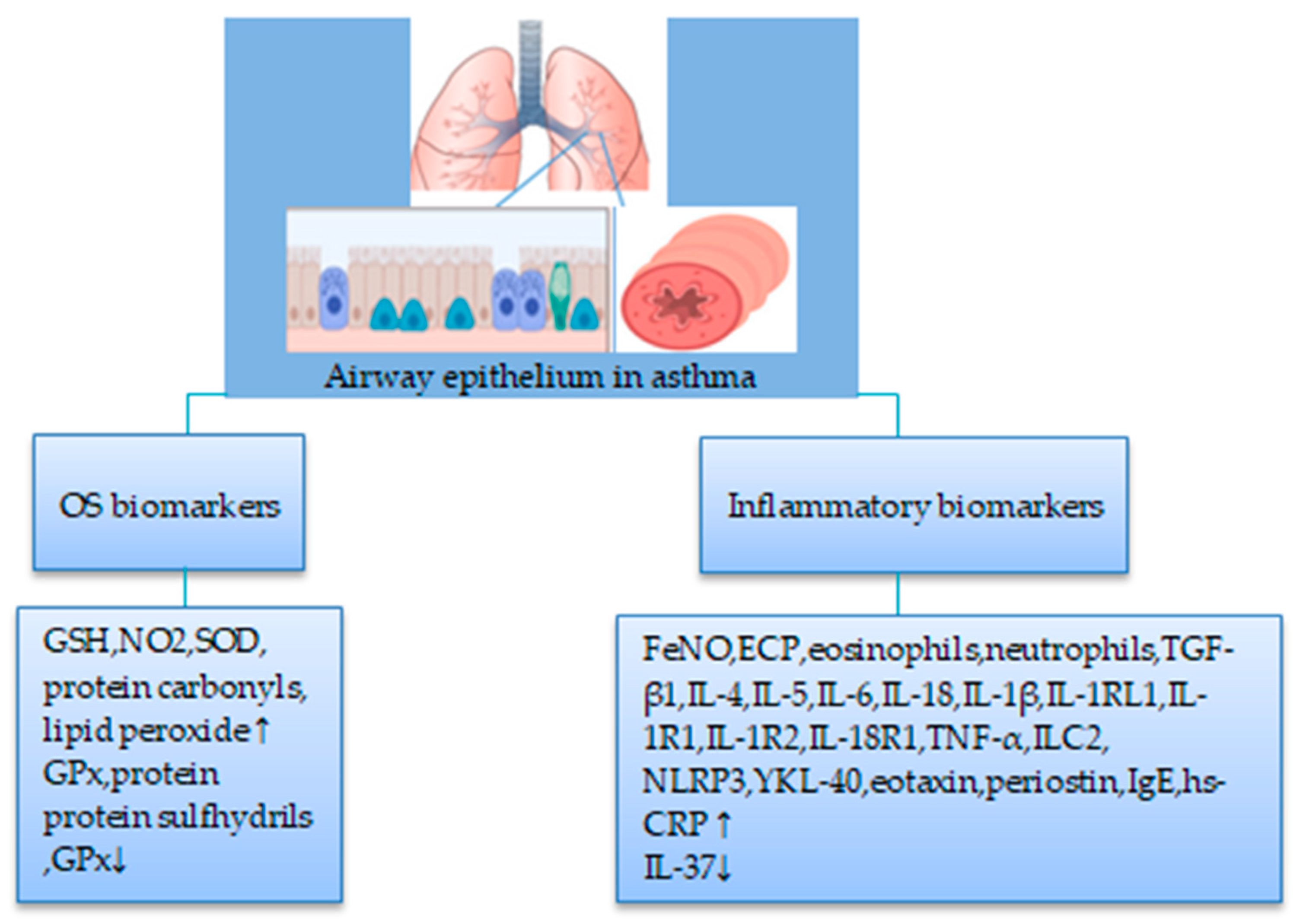
Figure 3.
Potential influence of antioxidant vitamins on CS-induced biomarkers. Antioxidant vitamins may reduce CS-induced OS and inflammatory biomarkers. It may also exert antioxidants and anti-inflammatory effects by increasing GSH and IL-10 levels. Abbreviation: VA, vitamin A; CA, carotenoids, VC, vitamin C; VE, vitamin E; VD, vitamin D; BA, bronchial asthma; CS, cigarette smoke; OS, oxidative stress. (↓) decrease, (↑) increase.
Figure 3.
Potential influence of antioxidant vitamins on CS-induced biomarkers. Antioxidant vitamins may reduce CS-induced OS and inflammatory biomarkers. It may also exert antioxidants and anti-inflammatory effects by increasing GSH and IL-10 levels. Abbreviation: VA, vitamin A; CA, carotenoids, VC, vitamin C; VE, vitamin E; VD, vitamin D; BA, bronchial asthma; CS, cigarette smoke; OS, oxidative stress. (↓) decrease, (↑) increase.
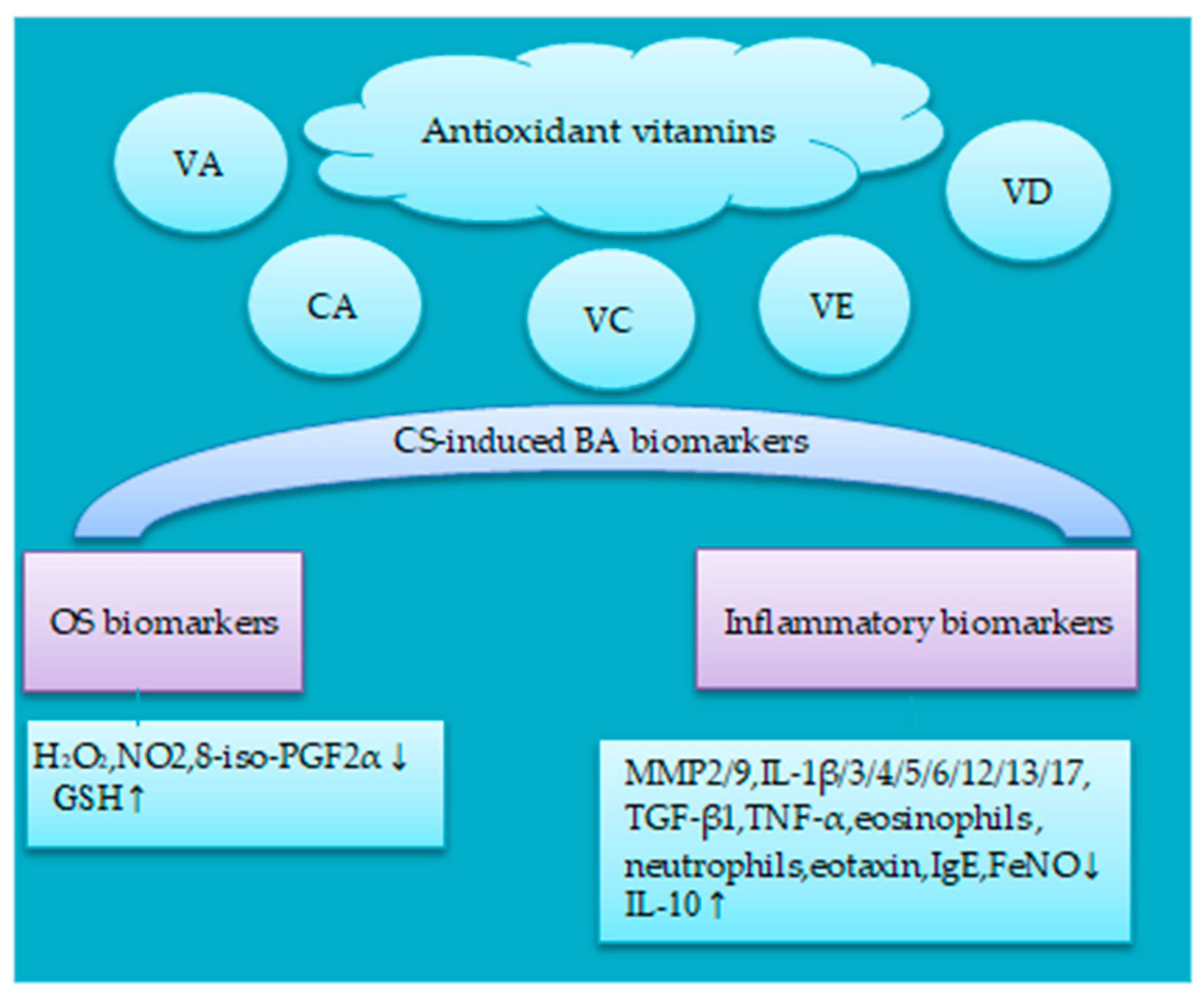
Figure 4.
Potential influence of antioxidant minerals on CS-induced biomarkers. Zn and Se may reduce CS-induced inflammatory biomarkers. Fe has both oxidant and inflammatory effects on BA. Abbreviation: Zn, Zinc; Se, Selenium; Fe, Iron; BA, bronchial asthma; CS, cigarette smoke; OS, oxidative stress. (↓) decrease, (↑) increase.
Figure 4.
Potential influence of antioxidant minerals on CS-induced biomarkers. Zn and Se may reduce CS-induced inflammatory biomarkers. Fe has both oxidant and inflammatory effects on BA. Abbreviation: Zn, Zinc; Se, Selenium; Fe, Iron; BA, bronchial asthma; CS, cigarette smoke; OS, oxidative stress. (↓) decrease, (↑) increase.
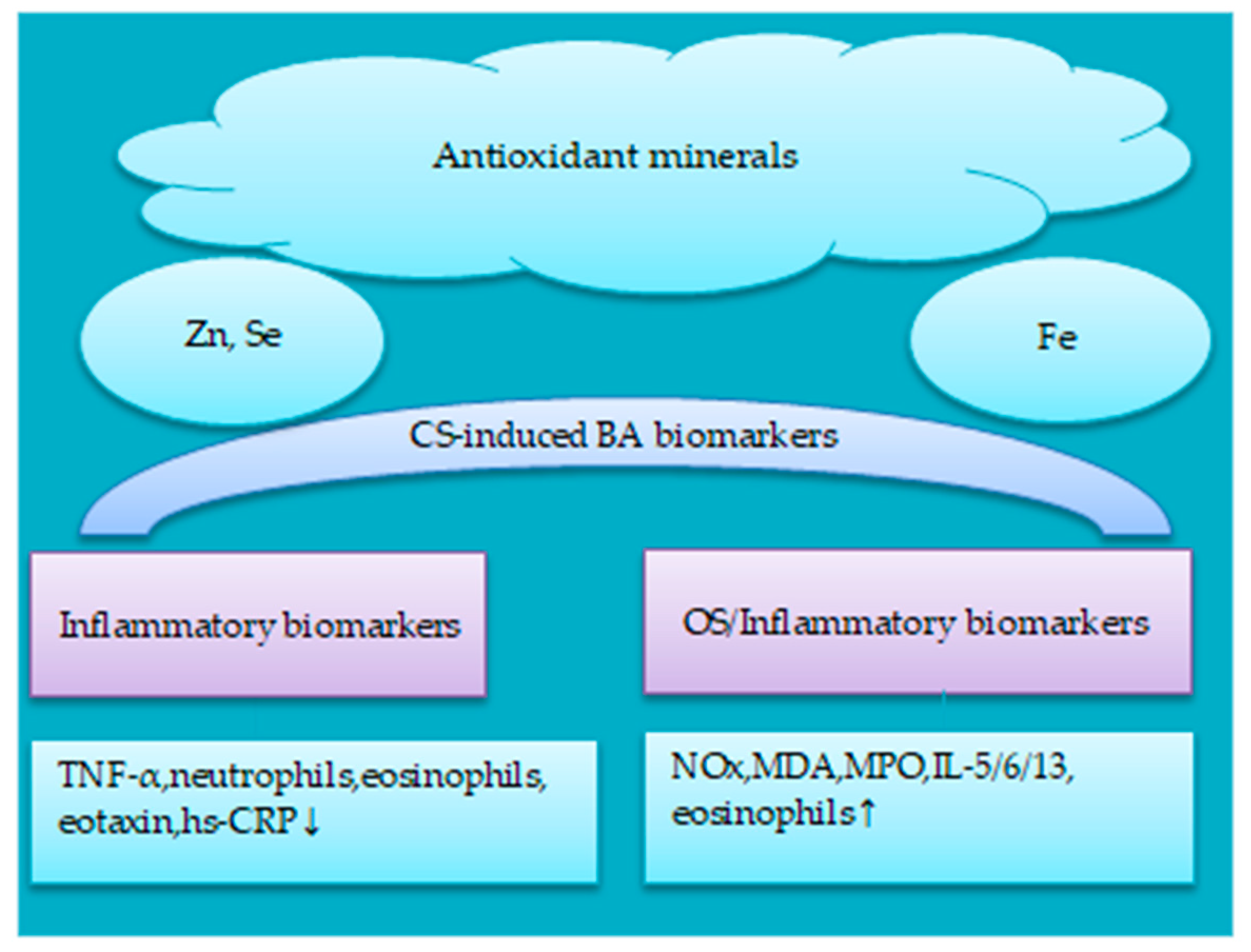

Table 1.
Antioxidants and BA risk in smokers and nonsmokers.
| Design | Study population | Antioxidants | Main findings | Ref. |
| Cross-sectional | Total subjects = 2112 12th grade US students Smokers = 515 |
VC, VE (diet) | Low dietary VC intake (<110 mg/day) was associated with FEV1 decline and respiratory symptoms in smokers with BA VE intake was not associated with BA |
[30] |
| Cross-sectional | Total subjects = 13,039 US adults (20-80 yrs) Current asthma=1784; non-current asthma= 11,255 Nonsmokers= 7106; current smokers= 3304; former smokers= 2624 |
Total carotenoids (diet and supplement) | High intake of carotenoids (≥165.59 μg/kg/day) was associated with reduced BA risk in nonsmokers (OR= 0.63, 95% CI = 0.42 to 0.93), current smokers (OR= 0.54, 95% CI = 0.36 to 0.83) and former smokers (OR= 0.64, 95% CI = 0.42 to 0.97) | [31] |
| RDBPC | Total subjects = 72 UK nonsmoking asthmatic (18-60 yrs) | VE (supplement) 500 mg VE capsules (D-α-tocopherol) in soya bean oil or matched placebo (capsules, gelatine base) for 6 weeks |
VE had no beneficial effects on BA | [32] |
| RDBPC | Total subjects = 197 UK smoking and nonsmoking asthmatic (18-54 yrs) |
Se (supplement) 100 μg/day high-Se yeast preparation or matched placebo (yeast only) for 24 weeks |
Plasma Se was increased by 48% in the Se group. However, no significant improvement in QoL score was observed in the Se group compared with placebo | [33] |
Abbreviation: RDBPC, randomized double blind placebo control; VC, vitamin C; VE, vitamin E; Se, selenium; BA, bronchial asthma; QoL, quality of life; OR, odds ratio.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



