
Submitted:
27 April 2023
Posted:
27 April 2023
You are already at the latest version
Abstract
Ischemia-reperfusion injury (IRI) is a complex pathophysiological process that can lead to severe and irreversible consequences, including the complete loss of renal function. While standardized strategies for preventing IRI during "back-table" and cold preservation are available, various intraoperative prevention methods have been proposed to mitigate the harmful effects of warm ischemia and reperfusion of the kidney. These methods include pharmacological agents, mechanical interventions, and surgical techniques such as renal capsulotomy, ischemic preconditioning, venous blood reperfusion, renal perfusion, and the use of tissue engineering techniques like mesenchymal stromal/stem cells and/or decellularization. In this comprehensive analysis, we provide a detailed overview of pharmacological agents and intraoperative methods and approaches for the prevention and treatment of renal IRI. We begin by discussing the mechanisms of IRI and the challenges of preventing it during surgery. Then using a bibliometric analysis and molecular docking of brand-new legends we showed eplerenone have the most binding affinity to Aldehyde dehydrogenase (AD), Estrogen receptor (ER), Klotho protein, Mineralocorticoid receptor (MR), and Toll-like receptor 4 (TLR4) for preventing IRI comparing with other available therapeutics, Benzodioxole, Hydrocortisone, Indoles, Nicotinamide adenine dinucleotide, and Niacinamide. Next, we provide a comprehensive analysis of the potential benefits and limitations of various prevention strategies, including an in-depth discussion of the mechanisms of action of pharmacological agents, mechanical interventions, and surgical techniques. Furthermore, we introduce a novel scoring system for the prevention methods of kidney IRI, which takes into account the effectiveness, feasibility, and safety of each method. We then analyze the current state of clinical research in this area and discuss the implications of these methods for future clinical practice. Overall, this article provides a valuable resource for clinicians and researchers seeking to prevent and treat renal IRI in surgical settings, and introduces a new scoring system that can be used to guide the selection of the most effective and safe prevention methods.
Keywords:
Ischemia/reperfusion injury
; Molecular docking
; Bibliometric analysis
; Kidney reperfusion
; Kidney transplantation
; Renal resection
1. Introduction
Kidney transplantation is currently considered the optimal method of renal replacement therapy, as it is clinically and economically superior to hemodialysis [1,2,3]. Immunosuppressive therapy has been successful in reducing the possibility of organ rejection. However, during kidney transplantation, the organ undergoes ischemia, which occurs before it becomes functional in the recipient's body [4]. These changes in the organ begin with brain death in cadaveric donors and, in living donors, from the moment of compression of the renal artery. The hypothermic or normothermic preservation of the kidneys before transplantation and the warm ischemic time (WIT) of varying duration during vascular anastomosis can lead to ischemic tissue damage [4]. The final and main stage of graft tissue damage occurs during organ reperfusion, which leads to the production of reactive oxygen species, activation of lipid peroxidation, and ferroptotic cell death due to the reoxygenation of the organ by arterial blood [5,6]. This complex process is known as ischemic reperfusion injury (IRI). As a result, ischemia and reperfusion initiate a cascade of immunological and inflammatory reactions in the organ, which can lead to severe consequences, including the complete loss of the organ [5,7,8]. The mechanism of transplant IRI is reflected in Figure 1 [9].
IRI may develop several hours or days after the initial start of blood flow in the kidney, and the morphological substrate is tubular necrosis. Clinically, this manifests as delayed graft function (DGF) followed by a long kidney recovery period [10]. A direct and significant relationship has been established between IRI and DGF and between the severity of IRI and the frequency of acute rejection episodes [11]. Therefore, DGF occurs in about 20% of cases of all kidney transplants [12]. Data from one meta-analysis showed that even after the first year of transplantation, with adequate restoration of graft function, DGF continues to have an adverse effect, while the risk of kidney transplant loss during the first 3.2 years is 41% higher than in patients without DGF [13]. Barba et al. indicated that after 18 hours, every hour of cold kidney ischemia increases the likelihood of DGF by 10% [14]. During reperfusion, a cooled graft undergoes a rapid change in temperature from hypothermia to normothermia, which leads to mitochondrial respiratory dysfunction and the induction of the mitochondrial pathway of apoptosis [15].
The warm ischemic time (WIT) can have a negative impact on kidney transplantation outcomes, particularly when it is prolonged [16,17]. Experimental studies have shown that each minute of warm ischemia is associated with a 6% increased risk of subsequent acute renal failure and a 7% increased risk of acute onset of end-stage renal failure [18]. Additionally, every 10 minutes of WIT (vascular anastomosis time or renal resection time) has a greater negative effect on the subsequent function of the kidney transplant than every hour of cold ischemia [19,20]. Methods for reducing kidney IRI, as outlined by Tasoulis et al. [21], can be conditionally divided into the following groups:
- The use of antioxidants to minimize oxidative stress
- Active agents for the removal of harmful metabolic products
- Preconditioning methods (ischemic, hypoxic, pharmacological, and remote ischemic preconditioning) to prepare cells for a better response to the upcoming IRI.
Prevention and treatment of IRI can be carried out at all stages of transplantation, including before, during, and after the procedure [22]. This includes preoperative diet therapy, adequate preservation and conditioning of potential donors, the use of mesenchymal stromal/stem cells (MSCs), and early reperfusion of the ischemic organ. The purposes of this article were: 1) using a bibliometric analysis and molecular docking of brand-new legends compare available therapeutic molecules for preventing IRI and 2) to study the existing intraoperative strategies and approaches for the prevention of kidney IRI during warm ischemia and reperfusion in light of the latest scientific data and their evaluation.
2. Materials and Methods
2.1. Data Collection and Extraction for Pharmacologic Methods for the Prevention of Kidney IRI
On February 1, 2023, we performed an accurate assessment on PubMed online database to identify the most frequent anticancer components in the extract of differ-ent sorts of sea cucumber, using the following search strategy: Search: ((kidney ischemia-reperfusion injury[Title/Abstract]) OR (kidney ischemia-reperfusion injury [MeSH Terms])) AND ((operative method*[MeSH Terms]) OR (operative method*[Title/Abstract])).
Next, we analyzed the resulting publications using VOSviewer software (v.1.6.8, 2018) [23], which can analyze the semantic contents of publication titles, keywords, abstracts, and relate them to citation count data. The software produced a bubble map that revealed the most frequent compounds that have been studied for their anticancer properties in sea cucumber extracts.
2.2. Bibliometric Search Strategy
2.2.1. Analysis of the Most Frequent MeSH Keywords
First, in order to achieve a general review of all MeSH keywords and the newest keywords that have been used in related field, we included all 752 keywords into our analysis except human, male, female, animal, mice, rat, dog, rabbit, perfusion injury, random allocation, kidney, apoptosis, and any age related keyword. Finally, Network and Overlay Visualization were conducted by VOSviewer software.
Second, among all keywords that are mentioned in related studies, we chose MeSH keywords that have at least 5 times occurrence. Then, we exclude some keywords from our analysis including human, male, female, animal, mice, rat, dog, rabbit, perfusion injury, random allocation, kidney, apoptosis, and any age-related keyword. Besides, we performed both Network Visualization and Overlay Visualization and after that, we considered total link strength and occurrence of each keyword as a criterion of attention of scientists to that keyword in related studies through recent years.
2.2.2. Analysis of the Most Involved Authors in the Field of Examining the Studies in Which Various Operative Methods for Preventing Kidney Ischemia-Reperfusion Injury Are Studied
We include all authors that have one published manuscript in related field. After that, we analyzed them by Network Visualization of VOSviewer software.
2.2.3. Analysis of the Average Publication Year of Authors
In our analysis, we examined the time range of activity of authors with the most number of surveys in related field by overlay visualization of VOSviewer software. We also examine the time range activity of the authors that have published their first manuscript in mentioned field and among them, we considered the authors with the average publication year of 2020 and more as new interested authors in related scientific area by mentioned analysis.
2.2.4. Analysis of Authors That Have the Most Tendency to Collaborate with Other Researcher and Have the Widest Range of Activity in Related Field
In our bibliometric analysis, the number of link for each author displays the amount of cooperation of that author with other researcher and total link strength demonstrated the range of activity (participating in publishing manuscript) in related field. Thus, we chose authors with the most total link strength as author with the widest range of activity in related field.
2.3. Molecular Interaction
After analysis the most used MeSH keywords in related field by VOSviewer software, we performed a manual search in our Overlay visualization of mentioned keywords in order to find latest compounds, protein and receptors that have been undergone studies in which their role in ischemic renal reperfusion injury (IRI) has been studied.
After finding remarked compounds, protein and receptors, we went through different studies in Google scholar database to realize their role in IRI.
In the next step, molecular docking of mentioned compounds, protein and receptors was conducted by Autodock Vina [24] with the purpose of discovering the most valuable compound that have undergone various studies in which IRI has been studied. We obtained the 3D structures of the six ligands and nine receptors (Aldehyde dehydrogenase (AD), Estrogen receptor (ER), Glucuronidase, Kloth protein, Mineralocorticoid receptor (MR), myeloid differentiation factor (MDF), Sitruin1, Toll-like receptor 4 (TLR4), and tumor necrosis factor receptor (TNFR)) from the PUBCHEM [25] and Protein Data Bank (PDB) databases. The PDB codes for these receptors were 1cw3, 1a52, 1bhg, 5vak, 1y9r, 2js7, 5btr, 5nam and 7kpa, respectively.
In the next step, remodeling of receptors with SWISS-MODEL Server [26] was performed. After that, we merged nonpolar hydrogens and ione pairs and assigned Gasteiger partial charges to each ligand atom. Grid boxes were generated using the Computed Atlas of Surface Topography of proteins (CASTp 3.0). Finally, we conducted docking and achieved nine conformations for each receptor and dye. All docking conformations were ranked according to the binding affinity, and the conformation with the lowest negative energy and RMSD ≤ 2 Å was selected as the best one.
2.4. Visualization of Inter-Molecular Interaction
The visualization of the 3D structure of the best conformations was performed using PyMOL software (The PyMOL Molecular Graphics System, Version 1.2r3pre, Schrödinger, LLC.). In addition, the detailed data about intermolecular interactions between the ligand and receptor were visualized in 2D using Discovery studio visualizer [27].
2.5. Data Collection and Extraction for Intraoperative Methods for the Prevention of Kidney IRI
The PubMed database was searched for articles using the following keywords: renal trans-plantation, ischemic-reperfusion injury of the kidney, and methods of prevention of is-chemic-reperfusion injury. Due to the limited number of available reports, publications from the last 12 years were selected. The titles and abstracts were independently screened by three authors to identify relevant articles. The search process included original articles, experimental studies, meta-analyses, and literature reviews that described intraoperative methods (during the surgery process) for the prevention of kidney IRI.
3. Results
3.1. Pharmacologic Methods for the Prevention of Kidney IRI: Bibliometric Search Strategy
3.1.1. The Most Frequent MeSH Keywords in Studies in Which Various Operative Methods for Preventing Kidney Ischemia-Reperfusion Injury Are Studied
Our analysis demonstrated that 752 MeSH keywords have been used in relevant field. Besides, all of these keywords that are used in relative surveys are shown in Figure 2.
On the other side, Network Visualization of our bibliometric analysis demonstrates that there are 86 items, 5 clusters, 1421 links and 2910 total link strength are existing in order to find most frequent MeSH keywords in studies in which various operative methods for preventing IRI are studied. Among all included MeSH keywords, treatment outcome, creatinine, ischemia and time factors are the most searched MeSH keywords (Figure 2 and Table 1).
Moreover, overlay visualization of our bibliometric analysis displayed the average publication year of various MeSH keywords in relevant field (Figure 3).
3.1.2. Brito, Marcus Vinicius Henriques Is the Most Involved Authors in the Field of Examining the Studies in Which Various Operative Methods for Preventing Kidney Ischemia-Reperfusion Injury Are Studied
According to our bibliometric co-authorship analysis, Brito, Marcus Vinicius Henriques was the most active researcher in related field with 5 documents (Figure 4 and Table 2). After him, Barakat, Nashwa and Corso, Carlos Otávio were in the second and third place. Detailed information about the top 10 authors with the greatest number of published manuscripts are listed in Table 2.
3.1.3. Authors That Are Interested in the Field of Examining the Studies in Which Various Operative Methods for Preventing Kidney Ischemia-Reperfusion Injury Are Studied
Figure 5 shows the condition of average publication of each author that is involved in related field. Moreover, Table 2 and Figure S1 demonstrate the average publication year of authors with the greatest number of published manuscripts in related field. As it is revealed in mentioned Table 2 and Figure S1, the average publication years of these authors are before 2018. On the other hand, authors with one published article in related field that have published their work since 2020 are demonstrated in Figure S2 this group of authors are known as newly interested authors in related fields that begin their research in mentioned scientific area.
3.1.4. Brito, Marcus Vinicius Henriques Has the Most Tendency to Collaborate with Other Researcher and Has the Widest Range of Activity in Related Field
Our bibliometric Network Analysis displayed that Brito, Marcus Vinicius Henriques with the link of 22 and total link strength of 35 has the greatest number of collaborations with other researchers in related field (Figure 6 and Table 3). After him, Hausenloy, Derek J and Ariti, Cono are in second and third place, respectively (Table 3). Detailed data about top 10 authors with the most tendency to collaborate with other researcher and has the widest range of activity in related field are listed in Table 3.
3.1.5. Brand New Compounds, Protein and Receptors That Have Been Undergone Studies in Which Their Role in IRI Has Been Studied
3.2. Molecular Docking Analysis of Brand-New Ligands and Receptors That Have Been Undergone Studies in Which Their Role I IRI Has Been Studied
Table 5 shows the binding affinity of brand-new ligands and receptors that have been undergone studies in which their role in IRI has been studied. Eplerenone demonstrated the most binding affinity to following receptors: Aldehyde dehydrogenase (AD), Estrogen receptor (ER), Klotho protein, Mineralocorticoid receptor (MR), and Toll-like receptor 4 (TLR4). On the other hand, nicotinamide adenine dinucleotide (NAD) displayed the most binding affinity to Glucuronidase, myeloid differentiation factor (MDF) and, tumor necrosis factor (TNFR).
Detailed data about features of interactions between mentioned ligands and receptors is presented in Figure 7.
3.3. Intraoperative Methods for the Prevention of Kidney IRI
The review analyzed the outcomes of various intraoperative methods for the prevention of kidney IRI (Table 6). A total of 24 publications were identified, which described intraoperative methods for the prevention of kidney IRI. Most of the data were presented in the form of experimental studies (n = 15) or clinical studies (n = 8), and one review (n = 1). Out of the 23 articles, 18 were published after 2015.
The following methods were described: local cooling of the kidney using devices and/or irrigation systems (10 articles), local cooling of the kidney with a cold solution through the renal artery (1), retrograde cooling of the kidney with a cold solution through the ureter (2), intraoperative administration of MSCs (2), surgical technique of vascular anastomosis to shorten the time of vascular thrombosis (VTI) (1), intraoperative hydrodynamic effect on the kidney (2), renal capsulotomy (3), intraoperative preconditioning (2), and kidney perfusion with venous blood (1). The results of these studies suggest the effectiveness of these methods in preventing kidney IRI during surgery.
Experimental and clinical studies have shown that WIT has a greater negative impact on the subsequent function of the kidney than cold ischemia [22]. The shorter the period of WIT, the less the degree of ischemic damage to the renal tissue. Therefore, cooling the kidney and maintaining an optimal temperature during this phase is one of the main conditions for preventing the consequences of kidney IRI.
4. Discussion
4.1. Treatment Outcome, Creatinine and Ischemia Were the Most Frequent MeSH Keywords in Related Studies
The Network Visualization of our bibliometric analysis showed that the most attractive Mesh keyword in related surveys was treatment outcome. On the other side, previous studies have mentioned that the treatment outcome of IRI therapy in still insufficient [64]. Thus, this fact validates our remarked bibliometric finding that the treatment outcome of IRI is still a challenge for researcher and they have focused a major part of their attention and effort on facing it.
Creatinine was the second most frequent Mesh keyword in related surveys. Prior surveys have mentioned that researchers consider creatinine as an important criteria in order to measure kidney injury in IRI situations [65]. Therefore, this finding confirms the result coming from the Network Visualization of our bibliometric analysis.
Ischemia is an important process that plays a crucial role in the pathogenesis of various organs including kidney. Thus, scientists have tried to discover a reliable solution for it [66]. Our Network Visualization analysis confirms this fact.
The Network Visualization demonstrates that Marcus Vinicius Henriques, Barakat, Nashwa and Corso, Carlos Otávio have been involved in the greatest number of manuscripts in relevant fields. This finding will help interested authors in related field for choosing the most experienced person for cooperation. In spite of this fact, Overlay Visualization of these mentioned authors demonstrated that the main time range activity of them is before 2018 and they had tendency to work with authors that have not worked in related field since 2018 (Table 2 and Figure S1). Therefore, authors that are interested in related field and want to make any scientific collaboration in mentioned field should consider this finding.
According to analysis of Overlay Visualization, authors that are mentioned in Figure S2 has begun their scientific activity since 2018. They are known as new interested authors in mentioned field and they are also known as a proper researcher to collaborate with. Thus, interested researchers can consider these mentioned authors as a proper choice in order to cooperate with in related scientific area.
According to Network Analysis (Table 2 and Figure 5) Brito, Marcus Vinicius Henriques with the link and total link strength of 22 and 35, respectively has the most tendency for cooperating with other researcher but he has not worked with new interested authors that have published manuscript since 2018. Interestingly, other researchers that are listed in Table 3 have had strong collaboration with each other (Figure S4). This fact demonstrates that their published manuscript may have a high value in related scientific field.
4.2. Brand New Compounds, Protein and Receptors in Recent Studies in Related Field
Table 4 contains the list of recent compounds, protein and receptors that have gained the attention of researchers who are studying about relevant field. According to Network and Overlay Visualization analysis, most of these compounds and molecules have the occurrence number of one- and the-time range of 2018 to 2021 (Table 4 and Figure S3). This result can guide other authors in order to gain a paradigm for performing their future researches in related field.
4.2.1. Eplerenone Affinities
Previous researches have demonstrated that Aldehyde dehydrogenase 2 can suppress the effect of 4-hydroxy-2-nonenal. In ischemic situations, 4-hydroxy-2-nonenal can lead renal cells to apoptosis [34]. On the other side, eplerenon demonstrated the most affinity to Aldehyde dehydrogenase 2. Thus, this compound demonstrated a coordination between its previous ameliorating IRI effects and mentioned in-silico affinity. On the other side Eplerenone had the most tendency to estrogen receptor. This receptor ameliorates IRI [37]. Moreover, prior researches have mentioned that eplerenone can suppress the process of IRI through Klotho, NF-κB and SIRT1/SIRT3/PGC-1α signalling pathways [29]. Our in-silico analysis displayed that this compound has the most tendency to Klotho protein (Table 5). This protein has a remarkable potential for attenuating the IRI process [41]. Therefore, our in-silico analysis of eplerenon is confirmed by previous surveys. Besides, this agent showed the highest affinity to Sirtuin1 which its ameliorative effects on IRI process has been proved by previous surveys[42]. Our in-silico based result for tendency of eplerenon to Sirtuin1 is validated by prior researches.
On the other side, eplerenon demonstrated a high affinity to Mineralocorticoid receptor and Toll-like receptor 4 (Table 5). This in-silico based result is in appose with the results of previous surveys about the role of eplerenon in the process of IRI [29]. Besides, early srudies have demonstrated that both mentioned receptors have the capability of amplification of IRI process and inhibiting them has been studied as a method for suppressing IRI (Table 6) [35,38]. Thus, our results about the tendency of this agent to both remarked receptors are not validated by previous surveys.
4.2.2. Nicotinamide Adenine Dinucleotide
Nicotinamide adenine dinucleotide has the highest binding affinity to Glucuronidase, MDF and TNFR. on the other hand, previous studies have demonstrated the ameliorative effects of NAD on the process of IRI (Table 5) [32]. This fact confirms the in-silico affinity of mentioned component to Glucuronidase because inhibiting effects of mentioned receptor has been proved by prior researches (Table 5) [40]. But the affinity of NAD to TNFR1 and MDF is not confirmed by previous surveys because these receptors have the capability to amplify IRI condition (Table 5) [36,39].
4.3. Local Cooling of the Kidney
A widespread method of reducing the effect of WIT is local cooling of the kidney by placing ice around it [67,68]. It is often used for both resection of the kidney and for its transplantation during secondary WIT in the recipient. In these cases, ice is applied directly to the kidney surface or the kidney is placed in an elastic container with ice slush [22,43]. Various methods of irrigation of the kidney with a cold solution with simultaneous aspiration or ice coating during laparoscopic resection are also used [69,70].
The next stage in the development of methods of local cooling of the kidney can be considered the use of various types of devices with a closed circulating cooling system [44,45,46,47,48]. Cold saline solution, ethanol solution with methylene blue or simple sterile water with different feed rates are used as perfusate in the system. These methods make it possible to maintain the optimal temperature in the contour around the renal graft within the range of 4-15°C.
Khan et al. developed and experimentally tested a thermally insulating jacket made of synthetic material for the kidney [49]. This device, based on the thermos principle, allows the kidney temperature to be maintained for a long time (up to 60 minutes), which was reached during the "back-table" procedure or cold preservation.
According to the authors, the described methods of local cooling of the kidney decrease the negative effect of WIT, reduce the frequency of DGF and, thereby, allow obtaining better functional indicators in comparison with kidney surgery without cooling. However, Karipineni et al. reported that during a one-year follow-up period for 66 kidney recipients who were operated with an ice bag during WIT, they did not find a significant decrease in the frequency or duration of DGF compared to the group without an ice bag [50].
In 37 patients, Liu et al. demonstrated the possibility of cooling the kidney by perfusion with a cold Ringer's solution through a cannulated (and clamped) renal artery with evacuation of fluid through an incision in the renal vein [51]. This cooling technique allowed the authors to perform resection of a kidney, which was disconnected from the bloodstream for 60 minutes, without negative consequences, even in the absence or functional insufficiency of the contralateral kidney. However, additional cannulation of the renal artery and then suturing of the artery and vein wounds lengthen the duration of the surgery.
The method of local cooling of the kidney by continuous retrograde perfusion of a cold solution through a cannulated ureter is a novel approach [52,53]. This cooling technique allows the operating field to remain "dry", which is not observed with renal surface irrigation with a cold solution or covering the kidney with an icy slush.
4.4. Renal Perfusion
In an experimental study on pigs, Schopp et al. demonstrated a twofold decrease in mitochondrial dysfunction and apoptosis after organ reperfusion by gradually increasing the temperature of the kidney graft from 4°C to 20°C before reperfusion [16]. This technique can be translated to clinical practice with some modifications. In another experimental study, Collett et al. restored the capillary microcirculation of the parenchyma, reduced inflammatory cell infiltration, and significantly decreased blood creatinine levels by retrograde hydrodynamic perfusion through the renal vein of the graft before reperfusion, which led to rapid recovery of kidney function [54]. However, this method requires catheterization of the renal vein for a prolonged time, although with some modifications, it can be adapted for use in recipients in clinical transplantation.
4.5. Renal Capsulotomy
Some animal studies have demonstrated the advantages of intraoperative capsulotomy of the kidney, such as the elimination of compartment syndrome [55,56,57]. However, in clinical practice, capsulotomy is not applicable or can be used in extremely rare cases. The technique proposed by Japanese researchers to maintain intraoperative systolic blood pressure in the renal artery ≥150 mmHg is simple to execute [58]. In a comparative study of 106 recipients, they revealed that the use of this method may be associated with early stabilization of renal graft function. Maintenance of systolic blood pressure ≥150 mmHg was achieved by increasing the volume of infusion and administering vasopressors if necessary.
4.6. Ischemic Preconditioning
Ischemic pre- and postconditioning are commonly used methods for preventing ischemic injury [60,71,72]. In an experimental study, a group of researchers used preconditioning by performing splenectomy and intraoperative compression of the lower extremities [59,60]. Although these methods are easy to execute, their effectiveness in reducing IRI is questioned [73].
4.7. Tissue Engineering
Tissue engineering involves the use of a combination of cells, biomaterials, and growth factors to create functional tissue constructs that can be used to replace damaged or diseased tissues. In the context of kidney IRI, tissue engineering approaches have focused on creating functional kidney tissue constructs that can be transplanted into the damaged kidney to help repair or replace damaged tissue [74,75].
One approach to tissue engineering for kidney IRI involves the use of mesenchymal stromal/stem cells (MSCs), which have been shown to have anti-inflammatory and regenerative properties. These cells can be incorporated into a scaffold made of biomaterials, such as hyaluronic acid or collagen, and then transplanted into the damaged kidney. The MSCs can then release growth factors and cytokines that promote tissue repair and regeneration, reduce inflammation, and enhance blood vessel formation. The use of MSCs in kidney recipients shows promise [76]. Preliminary experimental studies have shown the effectiveness of MSCs in reducing the effects of IRI when administered via intraoperative injection into the abdominal cavity, renal artery, or vein [61,62]. The use of MSCs in organ recipients is currently in the stage of experimental and clinical studies and has not yet become routine [76].
Another approach to tissue engineering for kidney IRI involves the use of decellularized kidney scaffolds, which are created by removing all cellular components from a donor kidney, leaving behind a structural framework of extracellular matrix (ECM) proteins [77]. This decellularized scaffold can then be reseeded with kidney cells, such as renal tubular epithelial cells, and cultured in vitro to create a functional kidney tissue construct [78]. This tissue construct can then be transplanted into the damaged kidney, where it can integrate with the host tissue and promote tissue repair and regeneration.
In summary, tissue engineering approaches hold great promise for the treatment of kidney IRI by providing functional kidney tissue constructs that can help repair and replace damaged tissue. These approaches have the potential to improve the outcomes for patients with kidney IRI, reducing the risk of acute and chronic kidney disease and improving overall quality of life.
4.8. Venous Blood Reperfusion
Researchers Cetin et al. experimentally demonstrated the advantages of preliminary perfusion of an ischemic kidney with venous blood before conventional arterial reperfusion [63]. By using low-oxygenated venous blood, they were able to reduce the production of reactive oxygen species and achieve an antioxidant effect. Preliminary results of another similar study also showed encouraging results [79].
The inevitability of kidney IRI during transplantation has necessitated the development of various prevention methods, particularly during warm ischemia and reperfusion, which are the most aggressive periods for the transplant. While prevention strategies for "back-table" and cold preservation are relatively standardized, various intraoperative prevention methods have been proposed to counteract the negative effects of warm ischemia and reperfusion on the kidney. Many of these methods are still in the experimental and clinical trial phases. Of course, there is no single ideal method for eliminating the consequences of IRI, although the use of MSCs shows promise.
4.9. Pros and Cons of Innovative Approaches to Prevent Kidney IRI
To better understand the mechanisms behind kidney IRI and to develop new treatments, researchers have employed various models to study the effects of ischemia and reperfusion on the kidney. In this table, we compare some of the most commonly used models for studying the impact of kidney IRI. We outline the pros and cons of each model, highlighting their advantages and limitations, to provide a comprehensive overview of the different approaches used to study kidney IRI (Table 7).
4.10. Scoring of Prevention Methods of Kidney IRI
The scoring system for the intraoperative methods of preventing ischemia-reperfusion injury of the kidney is based on three categories of research: clinical, in vivo, and in vitro (Table 8).
The clinical category refers to research conducted on human patients, and examines the effectiveness of the therapeutic approach in preventing ischemia-reperfusion injury during kidney surgery. The maximum score for this category is 3 points, with a score of 3 indicating strong evidence of clinical effectiveness, a score of 2 indicating moderate evidence, and a score of 1 indicating weak evidence. If there is no clinical evidence, the score is 0.
The in vivo category refers to research conducted on animal models, such as rats or mice, and examines the effectiveness of the therapeutic approach in preventing ischemia-reperfusion injury in these models. The maximum score for this category is 3 points, with a score of 3 indicating strong evidence of in vivo effectiveness, a score of 2 indicating moderate evidence, and a score of 1 indicating weak evidence. If there is no in vivo evidence, the score is 0.
The in vitro category refers to research conducted on isolated cells or tissues, such as kidney cells or kidney tissue, and examines the effectiveness of the therapeutic approach in preventing ischemia-reperfusion injury in these cells or tissues. The maximum score for this category is 3 points, with a score of 3 indicating strong evidence of in vitro effectiveness, a score of 2 indicating moderate evidence, and a score of 1 indicating weak evidence. If there is no in vitro evidence, the score is 0.
Once the scores for each category are determined, the total score for each therapeutic approach is calculated by summing the scores for the three categories. The maximum total score is 9 points, which indicates strong evidence of effectiveness in all three categories.
It's important to note that this scoring system is subjective and depends on the available research articles that have been reviewed. Different researchers or reviewers may assign different scores to the same therapeutic approach based on their interpretation of the available evidence.
In the second scoring table, I used a different set of criteria to score each therapeutic approach (Table 9). Here's an explanation of each criteria and how I scored each approach:
Clinical Approval: This criterion takes into account the degree to which the therapeutic approach has been clinically approved and is currently used in medical practice. I assigned scores from 1 to 3 based on the following criteria:
1: Little or no clinical approval, and not currently used in medical practice.
2: Some clinical approval, but not widely used in medical practice.
3: Widely accepted in medical practice and highly clinically approved.
Difficulty of Test: This criterion takes into account the difficulty and complexity of the tests or procedures required to administer the therapeutic approach. I assigned scores from 1 to 5 based on the following criteria:
1: Simple and easy to administer, with minimal training required.
2: Requires moderate training and technical skill to administer.
3: Moderately difficult to administer, with specialized training or equipment required.
4: Highly specialized and complex tests or procedures required.
5: Extremely difficult and complex tests or procedures required.
Cost of Operation: This criterion takes into account the cost of administering the therapeutic approach. I assigned scores from 1 to 5 based on the following criteria:
1: Very low cost, with minimal equipment or resources required.
2: Low cost, but some specialized equipment or resources required.
3: Moderate cost, with significant equipment or resources required.
4: High cost, with specialized equipment or resources required.
5: Extremely high cost, with very specialized equipment or resources required.
Equipment Needed: This criterion takes into account the type and amount of equipment or resources needed to administer the therapeutic approach. I assigned scores from 1 to 5 based on the following criteria:
1: Minimal equipment or resources needed.
2: Some specialized equipment or resources needed.
3: Moderate amount of specialized equipment or resources needed.
4: High amount of specialized equipment or resources needed.
5: Very high amount of specialized equipment or resources needed.
Availability: This criterion takes into account the availability of the therapeutic approach, including the availability of trained medical personnel and equipment or resources needed. I assigned scores from 1 to 4 based on the following criteria:
1: Widely available, with little or no barriers to access.
2: Somewhat available, with some barriers to access.
3: Moderately available, with significant barriers to access.
4: Limited availability, with significant barriers to access.
For each criterion, we assigned a score to each therapeutic approach based on my subjective interpretation of the available research in the field. Then, we added up the scores for each therapeutic approach to get a total score, with higher scores indicating more effective therapeutic approaches based on the specific criteria used.
In this table, each therapeutic approach is scored based on the available clinical, in vivo, and in vitro research, with a maximum score of 3 points for each category. The total score is the sum of the three categories, with a maximum score of 9 points. The scoring system is subjective and may vary depending on the research articles you review.
Tissue Engineering has the highest total score of 17, indicating that it is the most effective therapeutic approach when taking into account clinical approval, difficulty of test, cost of operation, equipment needed, and availability. Renal Capsulotomy has the lowest total score of 13, indicating that it may be less effective than the other approaches based on these criteria.
Based on the results of the two scoring tables, it is clear that there are several promising therapeutic approaches for preventing and treating kidney ischemia-reperfusion injury (IRI). The first scoring table suggests that the most effective intraoperative methods for preventing IRI include ischemic preconditioning, renal perfusion, and tissue engineering. These approaches scored the highest based on their effectiveness in clinical, in vivo, and in vitro studies.
However, the second scoring table highlights other important factors to consider when evaluating the effectiveness of therapeutic approaches, including clinical approval, difficulty of test, cost of operation, equipment needed, and availability. When taking these factors into account, renal perfusion scored highest, followed by ischemic preconditioning and tissue engineering.
5. Conclusions
In conclusion, the molecular interaction of brand-new compounds, proteins, and receptors has been extensively studied in recent years to identify potential therapeutic agents for the treatment of ischemia-reperfusion injury (IRI). Our in-silico analysis of eplerenone showed a high affinity to Aldehyde dehydrogenase 2, Klotho protein, and Sirtuin1, which have all been previously reported to have ameliorative effects on the IRI process. However, eplerenone's affinity to Mineralocorticoid receptor and Toll-like receptor 4, which have the potential to amplify IRI, is not confirmed by prior research. In the case of Nicotinamide Adenine Dinucleotide, our analysis showed the highest binding affinity to Glucuronidase, which is consistent with the inhibiting effects of this receptor on IRI. However, the affinity to TNFR1 and MDF is not confirmed by previous surveys as these receptors have the capability to amplify IRI. Overall, the findings of this study provide valuable insights into the molecular interactions of new compounds and their potential therapeutic applications in treating IRI. Further experimental studies are warranted to validate these findings and explore the clinical utility of these compounds in the management of IRI.
The prevention and treatment of kidney IRI require a comprehensive strategy that takes into account all stages of its development. The investigation of the multifaceted pathogenesis of IRI and the development of effective methods for its prevention and treatment, particularly during periods of secondary warm ischemia and reperfusion, can enhance the survival rates of both transplant and organ recipients. In addition to the intraoperative methods discussed in this article, promising therapeutic methods, such as renal perfusion, may also serve as potential strategies for preventing and treating kidney IRI. Continued research and clinical trials are necessary to determine the optimal prevention and treatment strategies for kidney IRI. Furthermore, the results of these scoring tables suggest that renal perfusion may be a particularly promising therapeutic approach for preventing and treating kidney IRI, as it scored high on both tables. Continued research and clinical trials are necessary to determine the optimal prevention and treatment strategies for kidney IRI, and to further evaluate the effectiveness of promising approaches such as renal perfusion.
Supplementary Materials
The following supporting information can be downloaded at the website of this paper posted on Preprints.org. Figure S1: the average publication year of authors with the greatest number of published manuscripts and the condition of their connections with other authors. The average publication year of Brito, Marcus Vinicius Henriques (A), Barakat, Nashwa (B), Corso, Carlos Otávio (C), Costa, Felipe Lobato Da Silva (D), Gomes, Regina De Paula Xavier (E), Guven, Ahmet (F), Hausenloy, Derek J (G), Hussein, Abdel-Aziz M (H), Korkmaz, Ahmet (I), Santos, Emanuel Burck Dos (J) are displayed.; Figure S2: (A-G): newly interested authors in related fields that begin their research in mentioned scientific area.; Figure S3: The result of manual search through Overlay Visualization resulted from our bibliometric analysis for finding the latest compounds, protein and receptors that are underwent studies in which their role I ischemic reperfusion injury has been studied.; Figure S4: Network Visualization of authors with the most tendency to collaborate with other researchers in mentioned field. The size of each square of each author represents the number of link of that author.
Author Contributions
Conceptualization, Myltykbay S. Rysmakhanov, Afshin Zare, Mehmet Haberal and Amin Tamadon; Data curation, Amin Tamadon; Investigation, Myltykbay S. Rysmakhanov, Aibolat S. Smagulov, Nurgul A. Abenova, Nadiar M. Mussin, Yerlan B. Sultangereyev, Bazylbek S. Zhakiyev, Gani K. Kuttymuratov, Mehmet Haberal, Nazanin Jafari, Hanieh Baneshi, Shabnam Bakhshalizadeh and Farhad Rahmanifar; Methodology, Myltykbay S. Rysmakhanov, Afshin Zare, Aibolat S. Smagulov, Nurgul A. Abenova, Yerlan B. Sultangereyev, Bazylbek S. Zhakiyev, Gani K. Kuttymuratov, Mehmet Haberal, Nazanin Jafari and Hanieh Baneshi; Project administration, Nadiar M. Mussin and Amin Tamadon; Resources, Nadiar M. Mussin, Mahdi Mahdipour and Farhad Rahmanifar; Software, Afshin Zare; Supervision, Amin Tamadon; Writing – original draft, Myltykbay S. Rysmakhanov and Afshin Zare; Writing – review & editing, Nadiar M. Mussin, Yerlan B. Sultangereyev, Shabnam Bakhshalizadeh, Mahdi Mahdipour and Amin Tamadon.
Funding
This study received no funding.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Data Availability Statement
Data are contained within the article. Datasets related to this project can be obtained from corresponding author based on a reasonable request.
Acknowledgments
Not applicable.
Conflicts of Interest
The authors Afshin Zare, Nazanin Jafari, Hanieh Baneshi and Amin Tamadon were employed by PerciaVista R&D Co. The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
References
- Labus, A.; Niemczyk, M.; Czyzewski, L.; Fliszkiewicz, M.; Kulesza, A.; Mucha, K.; Paczek, L. Costs of Long-Term Post-Transplantation Care in Kidney Transplant Recipients. Ann Transplant 2019, 24, 252–259. [Google Scholar] [CrossRef]
- Axelrod, D.A.; Schnitzler, M.A.; Xiao, H.; Irish, W.; Tuttle-Newhall, E.; Chang, S.H.; Kasiske, B.L.; Alhamad, T.; Lentine, K.L. An economic assessment of contemporary kidney transplant practice. Am J Transplant 2018, 18, 1168–1176. [Google Scholar] [CrossRef] [PubMed]
- Jensen, C.E.; Sorensen, P.; Petersen, K.D. In Denmark kidney transplantation is more cost-effective than dialysis. Danish Medical Journal 2014, 61, A4796. [Google Scholar] [PubMed]
- Qiu, L.; Zhang, Z.J. Therapeutic Strategies of Kidney Transplant Ischemia Reperfusion Injury: Insight From Mouse Models. Biomed J Sci Tech Res 2019, 14. [Google Scholar]
- Eleftheriadis, T.; Pissas, G.; Filippidis, G.; Liakopoulos, V.; Stefanidis, I. Reoxygenation induces reactive oxygen species production and ferroptosis in renal tubular epithelial cells by activating aryl hydrocarbon receptor. Mol Med Rep 2021, 23, 1–1. [Google Scholar] [CrossRef]
- Vatazin, A.; Nesterenko, I.; Zulkarnaev, A.; Shakhov, N. Pathogenetic mechanisms of the development of ischemic and reperfusion damage the kidneys as a promising target specific therapy. Russian Journal of Transplantology and Artificial Organs 2015, 17, 147–156. [Google Scholar] [CrossRef]
- Menke, J.; Sollinger, D.; Schamberger, B.; Heemann, U.; Lutz, J. The effect of ischemia/reperfusion on the kidney graft. Curr Opin Organ Transplant 2014, 19, 395–400. [Google Scholar] [CrossRef]
- Garg, J.P.; Vucic, D. Targeting cell death pathways for therapeutic intervention in kidney diseases. In Proceedings of the Seminars in Nephrology; 2016; pp. 153–161. [Google Scholar]
- Salvadori, M.; Rosso, G.; Bertoni, E. Update on ischemia-reperfusion injury in kidney transplantation: Pathogenesis and treatment. World J Transplant 2015, 5, 52–67. [Google Scholar] [CrossRef]
- Summers, D.M.; Watson, C.J.; Pettigrew, G.J.; Johnson, R.J.; Collett, D.; Neuberger, J.M.; Bradley, J.A. Kidney donation after circulatory death (DCD): state of the art. Kidney Int 2015, 88, 241–249. [Google Scholar] [CrossRef]
- Cardinal, H.; Dieude, M.; Hebert, M.J. Endothelial Dysfunction in Kidney Transplantation. Front Immunol 2018, 9, 1130. [Google Scholar] [CrossRef]
- Zhao, H.; Alam, A.; Soo, A.P.; George, A.J.T.; Ma, D. Ischemia-Reperfusion Injury Reduces Long Term Renal Graft Survival: Mechanism and Beyond. EBioMedicine 2018, 28, 31–42. [Google Scholar] [CrossRef] [PubMed]
- Han, F.; Lin, M.Z.; Zhou, H.L.; Li, H.; Sun, Q.P.; Huang, Z.Y.; Hong, L.Q.; Wang, G.; Cai, R.M.; Sun, Q.Q. Delayed graft function is correlated with graft loss in recipients of expanded-criteria rather than standard-criteria donor kidneys: a retrospective, multicenter, observation cohort study. Chin Med J (Engl) 2020, 133, 561–570. [Google Scholar] [CrossRef] [PubMed]
- Yarlagadda, S.G.; Coca, S.G.; Formica, R.N., Jr.; Poggio, E.D.; Parikh, C.R. Association between delayed graft function and allograft and patient survival: a systematic review and meta-analysis. Nephrol Dial Transplant 2009, 24, 1039–1047. [Google Scholar] [CrossRef] [PubMed]
- Barba, J.; Zudaire, J.J.; Robles, J.; Tienza, A.; Rosell, D.; Berián, J.; Pascual, I. Existe un intervalo de tiempo de isquemia fría seguro para el injerto renal? Actas Urológicas Españolas 2011, 35, 475–480. [Google Scholar] [CrossRef] [PubMed]
- Schopp, I.; Reissberg, E.; Luer, B.; Efferz, P.; Minor, T. Controlled Rewarming after Hypothermia: Adding a New Principle to Renal Preservation. Clin Transl Sci 2015, 8, 475–478. [Google Scholar] [CrossRef] [PubMed]
- Hameed, A.; Yuen, L.; Pang, T.; Rogers, N.; Hawthorne, W.; Pleass, H. Techniques to ameliorate the impact of second warm ischemic time on kidney transplantation outcomes. In Proceedings of the Transplantation Proceedings; 2018; pp. 3144–3151. [Google Scholar]
- Tennankore, K.K.; Kim, S.J.; Alwayn, I.P.; Kiberd, B.A. Prolonged warm ischemia time is associated with graft failure and mortality after kidney transplantation. Kidney Int 2016, 89, 648–658. [Google Scholar] [CrossRef]
- Heylen, L.; Pirenne, J.; Samuel, U.; Tieken, I.; Naesens, M.; Sprangers, B.; Jochmans, I. The Impact of Anastomosis Time During Kidney Transplantation on Graft Loss: A Eurotransplant Cohort Study. Am J Transplant 2017, 17, 724–732. [Google Scholar] [CrossRef]
- Patel, A.R.; Eggener, S.E. Warm ischemia less than 30 minutes is not necessarily safe during partial nephrectomy: every minute matters. In Proceedings of the Urologic Oncology: Seminars and Original Investigations; 2011; pp. 826–828. [Google Scholar]
- Tasoulis, M.K.; Douzinas, E.E. Hypoxemic reperfusion of ischemic states: an alternative approach for the attenuation of oxidative stress mediated reperfusion injury. J Biomed Sci 2016, 23, 7. [Google Scholar] [CrossRef]
- Kaminska, D.; Koscielska-Kasprzak, K.; Chudoba, P.; Halon, A.; Mazanowska, O.; Gomolkiewicz, A.; Dziegiel, P.; Drulis-Fajdasz, D.; Myszka, M.; Lepiesza, A.; et al. The influence of warm ischemia elimination on kidney injury during transplantation - clinical and molecular study. Sci Rep 2016, 6, 36118. [Google Scholar] [CrossRef]
- Van Eck, N.J.; Waltman, L. VOSviewer: Visualizing scientific landscapes. Leiden University in the Netherlands 2010. [Google Scholar]
- Trott, O.; Olson, A.J. AutoDock Vina: improving the speed and accuracy of docking with a new scoring function, efficient optimization, and multithreading. J Comput Chem 2010, 31, 455–461. [Google Scholar] [CrossRef]
- Kim, S.; Chen, J.; Cheng, T.; Gindulyte, A.; He, J.; He, S.; Li, Q.; Shoemaker, B.A.; Thiessen, P.A.; Yu, B.; et al. PubChem 2023 update. Nucleic Acids Res 2023, 51, D1373–D1380. [Google Scholar] [CrossRef] [PubMed]
- Waterhouse, A.; Bertoni, M.; Bienert, S.; Studer, G.; Tauriello, G.; Gumienny, R.; Heer, F.T.; de Beer, T.A.P.; Rempfer, C.; Bordoli, L.; et al. SWISS-MODEL: homology modelling of protein structures and complexes. Nucleic Acids Res 2018, 46, W296–W303. [Google Scholar] [CrossRef] [PubMed]
- BIOVIA, D.S. Software product name. Software version], San Diego: Dassault Systèmes,[Year]. Please note that all current BIOVIA software products start with the company name, and should be referenced as such. All products can be found at https://3ds. com/products-services/biovia/products 2019.
- Wang, Y.; Wen, J.; Almoiliqy, M.; Wang, Y.; Liu, Z.; Yang, X.; Lu, X.; Meng, Q.; Peng, J.; Lin, Y.; et al. Sesamin Protects against and Ameliorates Rat Intestinal Ischemia/Reperfusion Injury with Involvement of Activating Nrf2/HO-1/NQO1 Signaling Pathway. Oxid Med Cell Longev 2021, 2021, 5147069. [Google Scholar] [CrossRef] [PubMed]
- Barati, A.; Rahbar Saadat, Y.; Meybodi, S.M.; Nouraei, S.; Moradi, K.; Kamrani Moghaddam, F.; Malekinejad, Z.; Hosseiniyan Khatibi, S.M.; Zununi Vahed, S.; Bagheri, Y. Eplerenone reduces renal ischaemia/reperfusion injury by modulating Klotho, NF-kappaB and SIRT1/SIRT3/PGC-1alpha signalling pathways. J Pharm Pharmacol 2022. [Google Scholar] [CrossRef]
- Azari, O.; Kheirandish, R.; Azizi, S.; Farajli Abbasi, M.; Ghahramani Gareh Chaman, S.; Bidi, M. Protective Effects of Hydrocortisone, Vitamin C and E Alone or in Combination against Renal Ischemia-Reperfusion Injury in Rat. Iran J Pathol 2015, 10, 272–280. [Google Scholar]
- Papi, S.; Ahmadvand, H.; Sotoodehnejadnematalahi, F.; Yaghmaei, P. The Protective Effects of Indole-Acetic Acid on the Renal Ischemia-Reperfusion Injury via Antioxidant and Antiapoptotic Properties in A Rat Model. Iran J Kidney Dis 2022, 16, 125–134. [Google Scholar]
- Hosseini, L.; Vafaee, M.S.; Mahmoudi, J.; Badalzadeh, R. Nicotinamide adenine dinucleotide emerges as a therapeutic target in aging and ischemic conditions. Biogerontology 2019, 20, 381–395. [Google Scholar] [CrossRef]
- Fontecha-Barriuso, M.; Lopez-Diaz, A.M.; Carriazo, S.; Ortiz, A.; Sanz, A.B. Nicotinamide and acute kidney injury. 2021, 14, 2453–2462. [Google Scholar] [CrossRef]
- Panisello-Rosello, A.; Lopez, A.; Folch-Puy, E.; Carbonell, T.; Rolo, A.; Palmeira, C.; Adam, R.; Net, M.; Rosello-Catafau, J. Role of aldehyde dehydrogenase 2 in ischemia reperfusion injury: An update. World J Gastroenterol 2018, 24, 2984–2994. [Google Scholar] [CrossRef]
- Mejía-Vilet, J.M.; Ramírez, V.; Cruz, C.; Uribe, N.; Gamba, G.; Bobadilla, N.A. Renal ischemia-reperfusion injury is prevented by the mineralocorticoid receptor blocker spironolactone. American Journal of Physiology-Renal Physiology 2007, 293, F78–F86. [Google Scholar] [CrossRef] [PubMed]
- Donnahoo, K.K.; Shames, B.D.; Harken, A.H.; Meldrum, D.R. Review article: the role of tumor necrosis factor in renal ischemia-reperfusion injury. J Urol 1999, 162, 196–203. [Google Scholar] [CrossRef]
- Ma, H.Y.; Chen, S.; Du, Y. Estrogen and estrogen receptors in kidney diseases. Ren Fail 2021, 43, 619–642. [Google Scholar] [CrossRef]
- Wu, H.; Chen, G.; Wyburn, K.R.; Yin, J.; Bertolino, P.; Eris, J.M.; Alexander, S.I.; Sharland, A.F.; Chadban, S.J. TLR4 activation mediates kidney ischemia/reperfusion injury. J Clin Invest 2007, 117, 2847–2859. [Google Scholar] [CrossRef] [PubMed]
- Hu, X.; Ding, C.; Ding, X.; Fan, P.; Zheng, J.; Xiang, H.; Li, X.; Qiao, Y.; Xue, W.; Li, Y. Inhibition of myeloid differentiation protein 2 attenuates renal ischemia/reperfusion-induced oxidative stress and inflammation via suppressing TLR4/TRAF6/NF-kB pathway. Life Sci 2020, 256, 117864. [Google Scholar] [CrossRef]
- Panesso, M.C.; Shi, M.J.; Cho, H.J.; Paek, J.; Ye, J.F.; Moe, O.W.; Hu, M.C. Klotho has dual protective effects on cisplatin-induced acute kidney injury. Kidney International 2014, 85, 855–870. [Google Scholar] [CrossRef] [PubMed]
- Hu, M.C.; Moe, O.W. Klotho as a potential biomarker and therapy for acute kidney injury. Nature Reviews Nephrology 2012, 8, 423–429. [Google Scholar] [CrossRef]
- Khader, A.; Yang, W.L.; Kuncewitch, M.; Jacob, A.; Prince, J.M.; Asirvatham, J.R.; Nicastro, J.; Coppa, G.F.; Wang, P. Sirtuin 1 activation stimulates mitochondrial biogenesis and attenuates renal injury after ischemia-reperfusion. Transplantation 2014, 98, 148–156. [Google Scholar] [CrossRef]
- Menon, M.; Abaza, R.; Sood, A.; Ahlawat, R.; Ghani, K.R.; Jeong, W.; Kher, V.; Kumar, R.K.; Bhandari, M. Robotic kidney transplantation with regional hypothermia: evolution of a novel procedure utilizing the IDEAL guidelines (IDEAL phase 0 and 1). Eur Urol 2014, 65, 1001–1009. [Google Scholar] [CrossRef]
- Zhang, P.; Han, X.; Zhang, X.; Zhu, X.; Li, T.; Li, Y.; Chen, Y.; Li, G.; Han, L.; Zhang, R. A controllable double-cycle cryogenic device inducing hypothermia for laparoscopic orthotopic kidney transplantation in swine. Transl Androl Urol 2021, 10, 3046–3055. [Google Scholar] [CrossRef]
- Li, Y.; Han, X.; Dagvadorj, B.U.; Zhao, Y.; Zhang, X.; Zhu, X.; Li, T.; Zhang, P.; Chen, Y.; Li, G.; et al. An Effective Cooling Device for Minimal-Incision Kidney Transplantation. Ann Transplant 2020, 25, e928773. [Google Scholar] [CrossRef] [PubMed]
- Longchamp, A.; Meier, R.P.H.; Colucci, N.; Balaphas, A.; Orci, L.A.; Nastasi, A.; Longchamp, G.; Moll, S.; Klauser, A.; Pascual, M.; et al. Impact of an intra-abdominal cooling device during open kidney transplantation in pigs. Swiss Med Wkly 2019, 149, w20143. [Google Scholar] [CrossRef] [PubMed]
- Meier, R.P.H.; Piller, V.; Hagen, M.E.; Joliat, C.; Buchs, J.B.; Nastasi, A.; Ruttimann, R.; Buchs, N.C.; Moll, S.; Vallee, J.P.; et al. Intra-Abdominal Cooling System Limits Ischemia-Reperfusion Injury During Robot-Assisted Renal Transplantation. Am J Transplant 2018, 18, 53–62. [Google Scholar] [CrossRef] [PubMed]
- Territo, A.; Piana, A.; Fontana, M.; Diana, P.; Gallioli, A.; Gaya, J.M.; Huguet, J.; Gavrilov, P.; Rodriguez-Faba, O.; Facundo, C.; et al. Step-by-step Development of a Cold Ischemia Device for Open and Robotic-assisted Renal Transplantation. Eur Urol 2021, 80, 738–745. [Google Scholar] [CrossRef] [PubMed]
- Khan, T.; Kwarcinski, J.; Pang, T.; Hameed, A.; Boughton, P.; O’Grady, G.; Hawthorne, W.J.; Rogers, N.M.; Wong, G.; Pleass, H.C. Protection from the second warm ischemic injury in kidney transplantation using an ex vivo porcine model and thermally insulating jackets. In Proceedings of the Transplantation Proceedings; 2021; pp. 750–754. [Google Scholar]
- Karipineni, F.; Campos, S.; Parsikia, A.; Durinka, J.B.; Chang, P.-N.; Khanmoradi, K.; Zaki, R.; Ortiz, J. Elimination of warm ischemia using the Ice Bag Technique does not decrease delayed graft function. International journal of surgery 2014, 12, 551–556. [Google Scholar] [CrossRef] [PubMed]
- Liu, F.; Yuan, H.; Li, X.; Ma, X.; Wang, M. Application of Hypothermic Perfusion via a Renal Artery Balloon Catheter During Robot-assisted Partial Nephrectomy and Effect on Renal Function. Acad Radiol 2019, 26, e196–e201. [Google Scholar] [CrossRef] [PubMed]
- Colli, J.L.; Dorsey, P.; Grossman, L.; Lee, B.R. Retrograde renal cooling to minimize ischemia. Int Braz J Urol 2013, 39, 37–45. [Google Scholar] [CrossRef] [PubMed]
- Saitz, T.R.; Dorsey, P.J.; Colli, J.; Lee, B.R. Induction of cold ischemia in patients with solitary kidney using retrograde intrarenal cooling: 2-year functional outcomes. Int Urol Nephrol 2013, 45, 313–320. [Google Scholar] [CrossRef]
- Collett, J.A.; Corridon, P.R.; Mehrotra, P.; Kolb, A.L.; Rhodes, G.J.; Miller, C.A.; Molitoris, B.A.; Pennington, J.G.; Sandoval, R.M.; Atkinson, S.J.; et al. Hydrodynamic Isotonic Fluid Delivery Ameliorates Moderate-to-Severe Ischemia-Reperfusion Injury in Rat Kidneys. J Am Soc Nephrol 2017, 28, 2081–2092. [Google Scholar] [CrossRef]
- van Smaalen, T.C.; Mestrom, M.G.; Kox, J.J.; Winkens, B.; van Heurn, L.W. Capsulotomy of Ischemically Damaged Donor Kidneys: A Pig Study. Eur Surg Res 2016, 57, 89–99. [Google Scholar] [CrossRef]
- Herrler, T.; Tischer, A.; Meyer, A.; Feiler, S.; Guba, M.; Nowak, S.; Rentsch, M.; Bartenstein, P.; Hacker, M.; Jauch, K.W. The intrinsic renal compartment syndrome: new perspectives in kidney transplantation. Transplantation 2010, 89, 40–46. [Google Scholar] [CrossRef]
- Herrler, T.; Wang, H.; Tischer, A.; Schupp, N.; Lehner, S.; Meyer, A.; Wallmichrath, J.; Habicht, A.; Mfarrej, B.; Anders, H.J.; et al. Decompression of inflammatory edema along with endothelial cell therapy expedites regeneration after renal ischemia-reperfusion injury. Cell Transplant 2013, 22, 2091–2103. [Google Scholar] [CrossRef] [PubMed]
- Kinoshita, K.; Yamanaga, S.; Kaba, A.; Tanaka, K.; Ogata, M.; Fujii, M.; Hidaka, Y.; Kawabata, C.; Toyoda, M.; Uekihara, S. Optimizing Intraoperative Blood Pressure to Improve Outcomes in Living Donor Renal Transplantation. In Proceedings of the Transplantation Proceedings; 2020; pp. 1687–1694. [Google Scholar]
- Shen, Y.; Qiu, T.; Liu, X.H.; Zhang, L.; Wang, Z.S.; Zhou, J.Q. Renal ischemia-reperfusion injury attenuated by splenic ischemic preconditioning. Eur Rev Med Pharmacol Sci 2018, 22, 2134–2142. [Google Scholar] [CrossRef] [PubMed]
- Costa, F.L.; Teixeira, R.K.; Yamaki, V.N.; Valente, A.L.; Silva, A.M.; Brito, M.V.; Percario, S. Remote ischemic conditioning temporarily improves antioxidant defense. J Surg Res 2016, 200, 105–109. [Google Scholar] [CrossRef] [PubMed]
- Rodrigues, C.E.; Capcha, J.M.; de Braganca, A.C.; Sanches, T.R.; Gouveia, P.Q.; de Oliveira, P.A.; Malheiros, D.M.; Volpini, R.A.; Santinho, M.A.; Santana, B.A.; et al. Human umbilical cord-derived mesenchymal stromal cells protect against premature renal senescence resulting from oxidative stress in rats with acute kidney injury. Stem Cell Res Ther 2017, 8, 19. [Google Scholar] [CrossRef] [PubMed]
- Yamada, Y.; Nakashima, A.; Doi, S.; Ishiuchi, N.; Kanai, R.; Miyasako, K.; Masaki, T. Localization and Maintenance of Engrafted Mesenchymal Stem Cells Administered via Renal Artery in Kidneys with Ischemia-Reperfusion Injury. Int J Mol Sci 2021, 22, 4178. [Google Scholar] [CrossRef] [PubMed]
- Cetin, N.; Suleyman, H.; Sener, E.; Demirci, E.; Gundogdu, C.; Akcay, F. The prevention of ischemia/reperfusion induced oxidative damage by venous blood in rabbit kidneys monitored with biochemical, histopatological and immunohistochemical analysis. J Physiol Pharmacol 2014, 65, 383–392. [Google Scholar] [PubMed]
- Zheng, H.; Lan, J.; Li, J.; Lv, L. Therapeutic effect of berberine on renal ischemia-reperfusion injury in rats and its effect on Bax and Bcl-2. Exp Ther Med 2018, 16, 2008–2012. [Google Scholar] [CrossRef] [PubMed]
- Shiva, N.; Sharma, N.; Kulkarni, Y.A.; Mulay, S.R.; Gaikwad, A.B. Renal ischemia/reperfusion injury: An insight on in vitro and in vivo models. Life Sci 2020, 256, 117860. [Google Scholar] [CrossRef]
- Li, X.; Ma, N.; Xu, J.; Zhang, Y.; Yang, P.; Su, X.; Xing, Y.; An, N.; Yang, F.; Zhang, G.; et al. Targeting Ferroptosis: Pathological Mechanism and Treatment of Ischemia-Reperfusion Injury. Oxid Med Cell Longev 2021, 2021, 1587922. [Google Scholar] [CrossRef]
- Abe, T.; Sazawa, A.; Harabayashi, T.; Shinohara, N.; Maruyama, S.; Morita, K.; Matsumoto, R.; Aoyagi, T.; Nonomura, K. Renal hypothermia with ice slush in laparoscopic partial nephrectomy: the outcome of renal function. J Endourol 2012, 26, 1483–1488. [Google Scholar] [CrossRef]
- Ramirez, D.; Caputo, P.A.; Krishnan, J.; Zargar, H.; Kaouk, J.H. Robot-assisted partial nephrectomy with intracorporeal renal hypothermia using ice slush: step-by-step technique and matched comparison with warm ischaemia. BJU Int 2016, 117, 531–536. [Google Scholar] [CrossRef] [PubMed]
- Hruby, S.; Lusuardi, L.; Jeschke, S.; Janetschek, G. Cooling mechanisms in laparoscopic partial nephrectomy: are really necessary? Arch Esp Urol 2013, 66, 139–145. [Google Scholar] [PubMed]
- Arai, Y.; Kaiho, Y.; Saito, H.; Yamada, S.; Mitsuzuka, K.; Miyazato, M.; Nakagawa, H.; Ishidoya, S.; Ito, A. Renal hypothermia using ice-cold saline for retroperitoneal laparoscopic partial nephrectomy: evaluation of split renal function with technetium-99m-dimercaptosuccinic acid renal scintigraphy. Urology 2011, 77, 814–818. [Google Scholar] [CrossRef] [PubMed]
- Plotnikov, E.Y. Ischemic Preconditioning of the Kidney. Bull Exp Biol Med 2021, 171, 567–571. [Google Scholar] [CrossRef]
- Veighey, K.V.; Nicholas, J.M.; Clayton, T.; Knight, R.; Robertson, S.; Dalton, N.; Harber, M.; Watson, C.J.E.; De Fijter, J.W.; Loukogeorgakis, S.; et al. Early remote ischaemic preconditioning leads to sustained improvement in allograft function after live donor kidney transplantation: long-term outcomes in the REnal Protection Against Ischaemia-Reperfusion in transplantation (REPAIR) randomised trial. Br J Anaesth 2019, 123, 584–591. [Google Scholar] [CrossRef]
- Menting, T.P.; Wever, K.E.; Ozdemir-van Brunschot, D.M.; Van der Vliet, D.J.; Rovers, M.M.; Warle, M.C. Ischaemic preconditioning for the reduction of renal ischaemia reperfusion injury. Cochrane Database Syst Rev 2017, 3, CD010777. [Google Scholar] [CrossRef]
- Mirmoghtadaei, M.; Khaboushan, A.S.; Mohammadi, B.; Sadr, M.; Farmand, H.; Hassannejad, Z.; Kajbafzadeh, A.M. Kidney tissue engineering in preclinical models of renal failure: a systematic review and meta-analysis. Regen Med 2022, 17, 941–955. [Google Scholar] [CrossRef]
- Zamorano, M.; Castillo, R.L.; Beltran, J.F.; Herrera, L.; Farias, J.A.; Antileo, C.; Aguilar-Gallardo, C.; Pessoa, A.; Calle, Y.; Farias, J.G. Tackling Ischemic Reperfusion Injury With the Aid of Stem Cells and Tissue Engineering. Front Physiol 2021, 12, 705256. [Google Scholar] [CrossRef]
- Kouchakian, M.R.; Baghban, N.; Moniri, S.F.; Baghban, M.; Bakhshalizadeh, S.; Najafzadeh, V.; Safaei, Z.; Izanlou, S.; Khoradmehr, A.; Nabipour, I.; et al. The Clinical Trials of Mesenchymal Stromal Cells Therapy. Stem Cells Int 2021, 2021, 1634782. [Google Scholar] [CrossRef]
- Keshvari, M.A.; Afshar, A.; Daneshi, S.; Khoradmehr, A.; Baghban, M.; Muhaddesi, M.; Behrouzi, P.; Miri, M.R.; Azari, H.; Nabipour, I.; et al. Decellularization of kidney tissue: comparison of sodium lauryl ether sulfate and sodium dodecyl sulfate for allotransplantation in rat. Cell Tissue Res 2021, 386, 365–378. [Google Scholar] [CrossRef] [PubMed]
- Bombelli, S.; Meregalli, C.; Scalia, C.; Bovo, G.; Torsello, B.; De Marco, S.; Cadamuro, M.; Vigano, P.; Strada, G.; Cattoretti, G.; et al. Nephrosphere-Derived Cells Are Induced to Multilineage Differentiation when Cultured on Human Decellularized Kidney Scaffolds. Am J Pathol 2018, 188, 184–195. [Google Scholar] [CrossRef] [PubMed]
- Rysmakhanov, M.; Smagulov, A.; Mussin, N.; Kaliyev, A.; Zhakiyev, B.; Sultangereyev, Y.; Kuttymuratov, G. Retrograde reperfusion of renal grafts to reduce ischemic-reperfusion injury. Korean J Transplant 2022, 36, 253–258. [Google Scholar] [CrossRef] [PubMed]
Figure 1.
Biological pathways of ischemic-reperfusion injury.
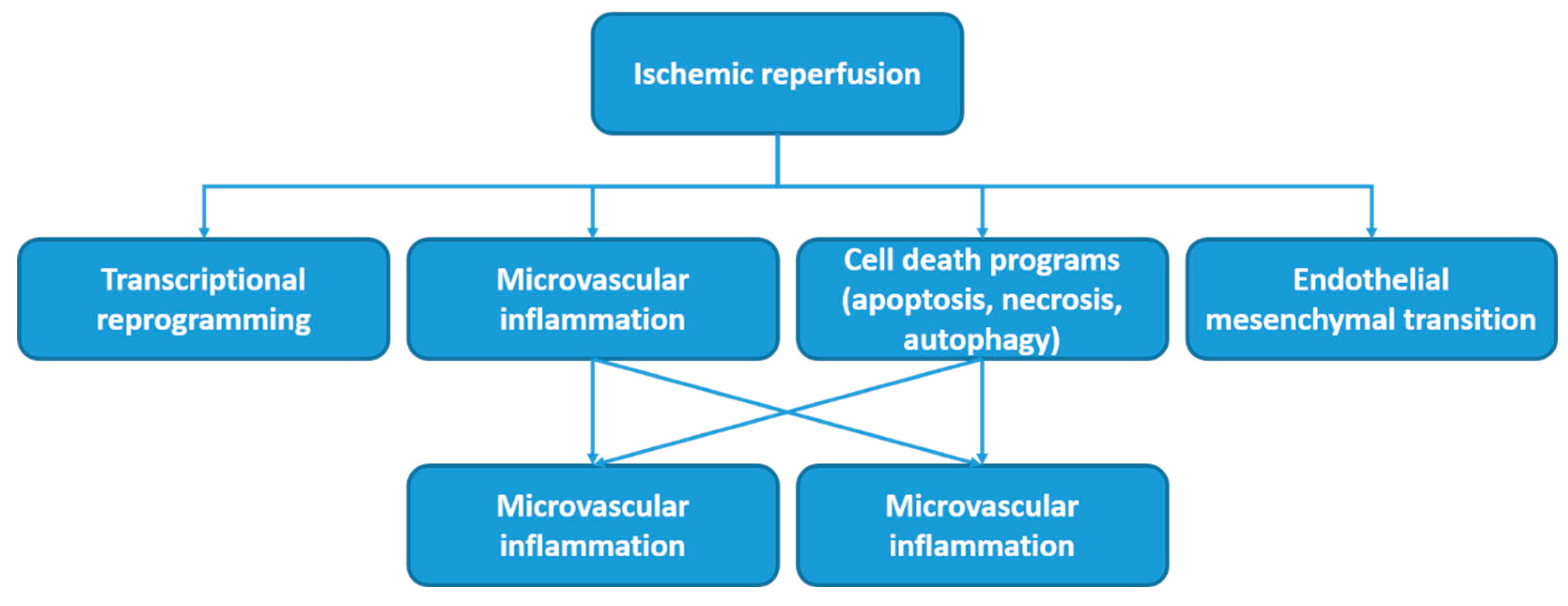
Figure 2.
The network visualization of the most used MeSH keywords in studies in which various operative methods for preventing kidney ischemia-reperfusion injury are studied.
Figure 2.
The network visualization of the most used MeSH keywords in studies in which various operative methods for preventing kidney ischemia-reperfusion injury are studied.
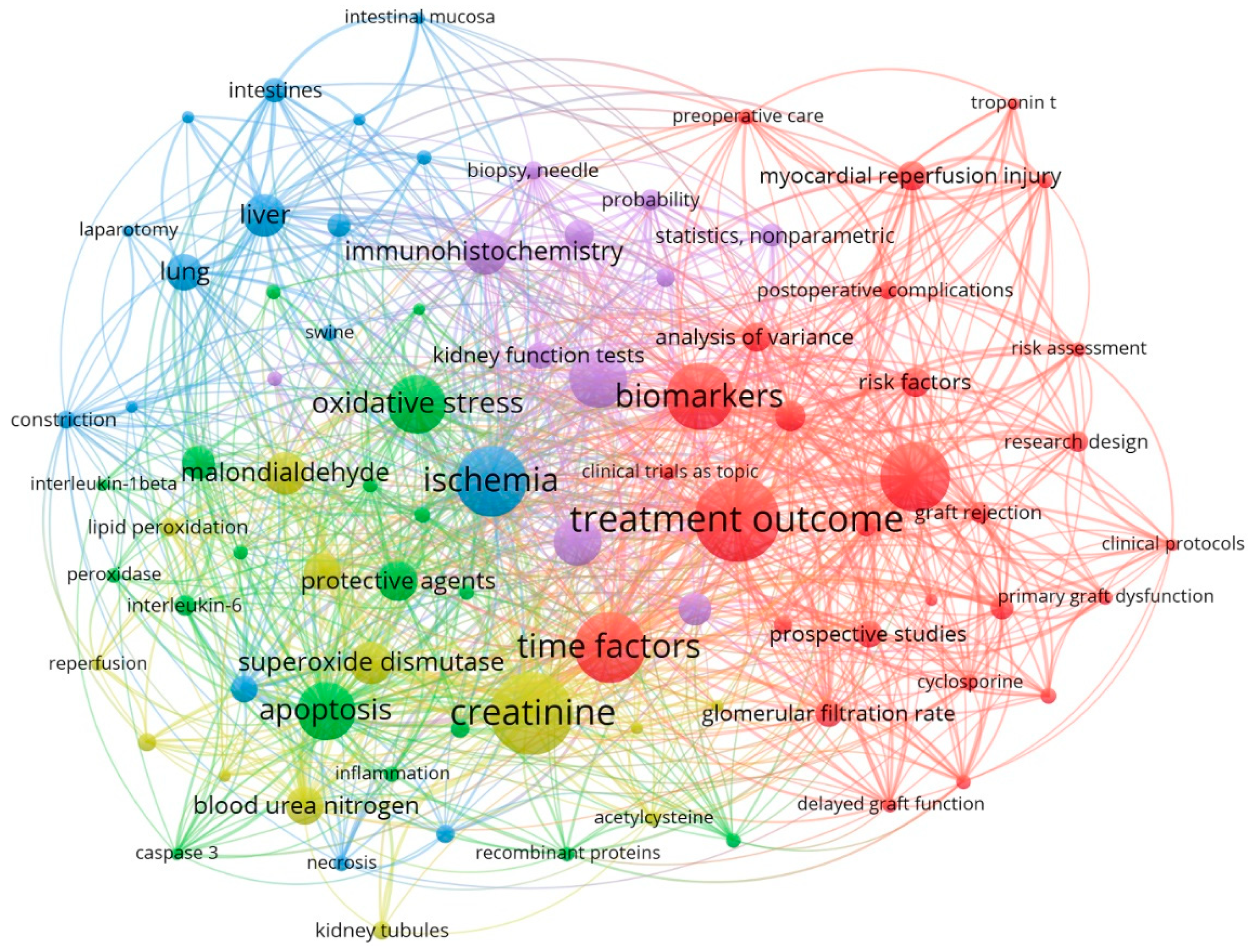
Figure 3.
The overlay visualization of all MeSH keywords that are used in relevant researches.
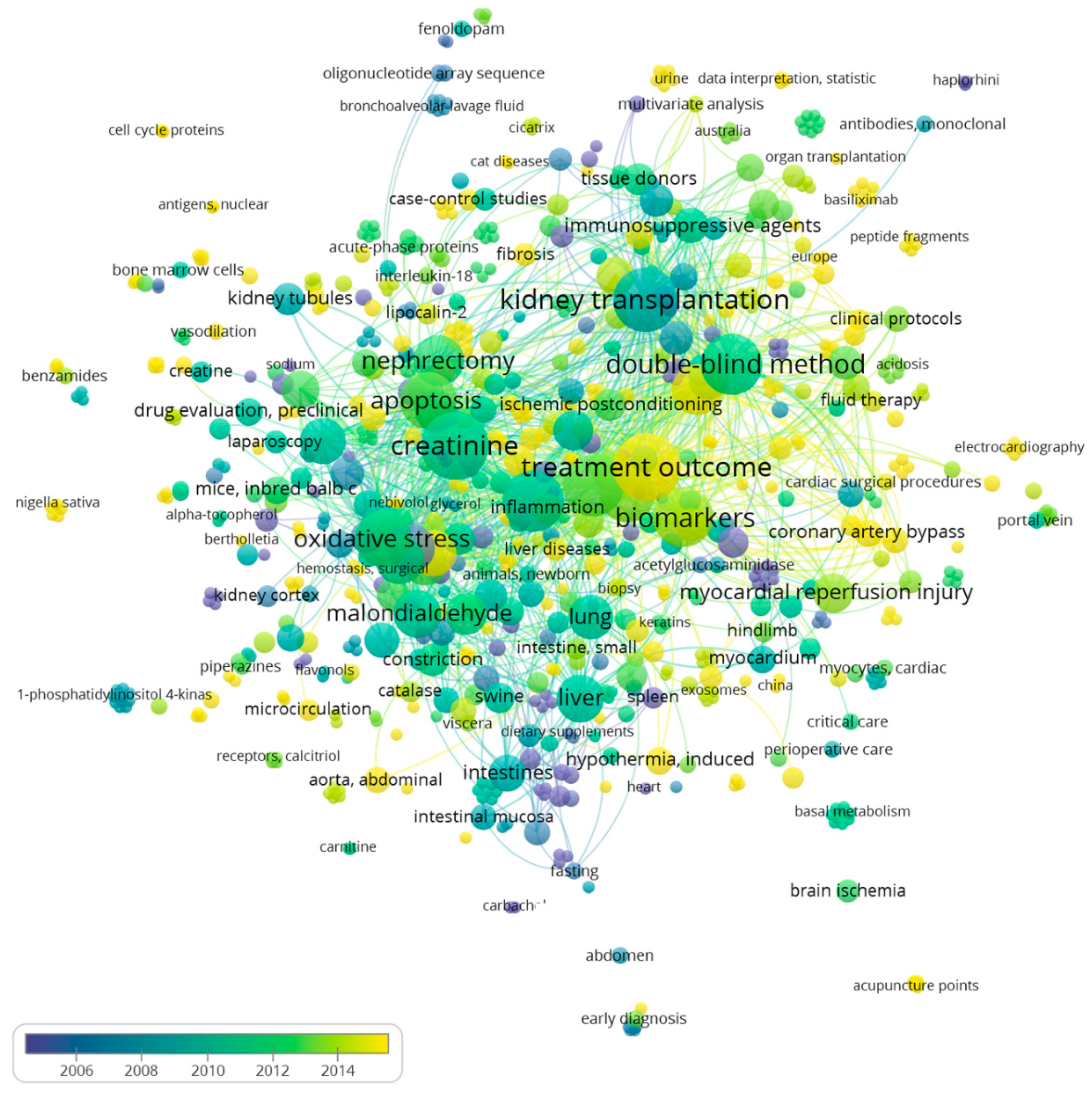
Figure 4.
Network visualization of the most involved authors in related field. The size of each square of each author demonstrates the number of published manuscripts of that author.
Figure 4.
Network visualization of the most involved authors in related field. The size of each square of each author demonstrates the number of published manuscripts of that author.
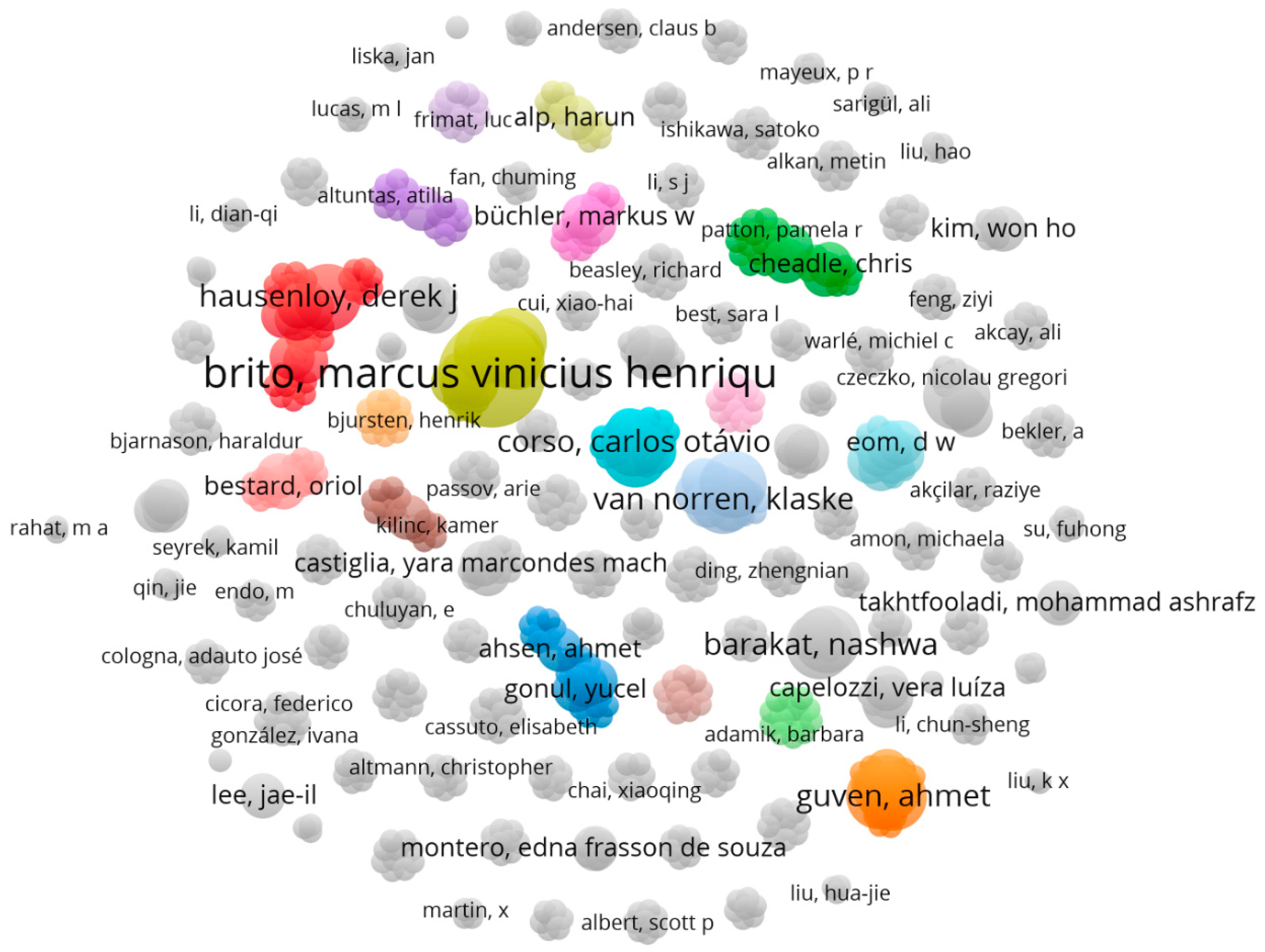
Figure 5.
The average publication year of authors that are involved in the field of examining the studies in which various operative methods for preventing kidney ischemia-reperfusion injury are studied.
Figure 5.
The average publication year of authors that are involved in the field of examining the studies in which various operative methods for preventing kidney ischemia-reperfusion injury are studied.
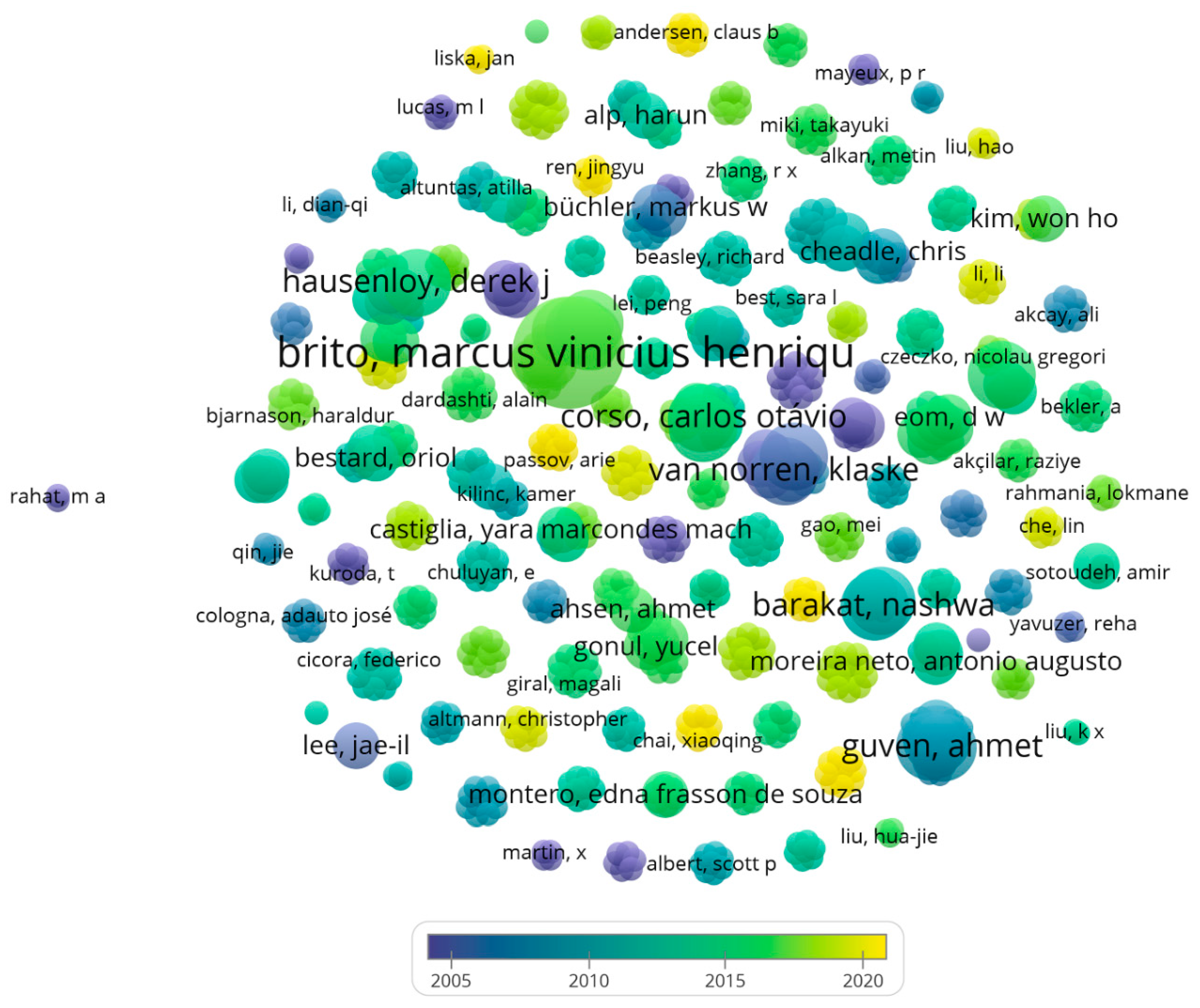
Figure 6.
Network Visualization of authors with the most tendency to cooperate with other researchers in related field. The size of each square of each author demonstrates the number of link (which represents the tendency of each author for cooperation with other scientists) of that author.
Figure 6.
Network Visualization of authors with the most tendency to cooperate with other researchers in related field. The size of each square of each author demonstrates the number of link (which represents the tendency of each author for cooperation with other scientists) of that author.
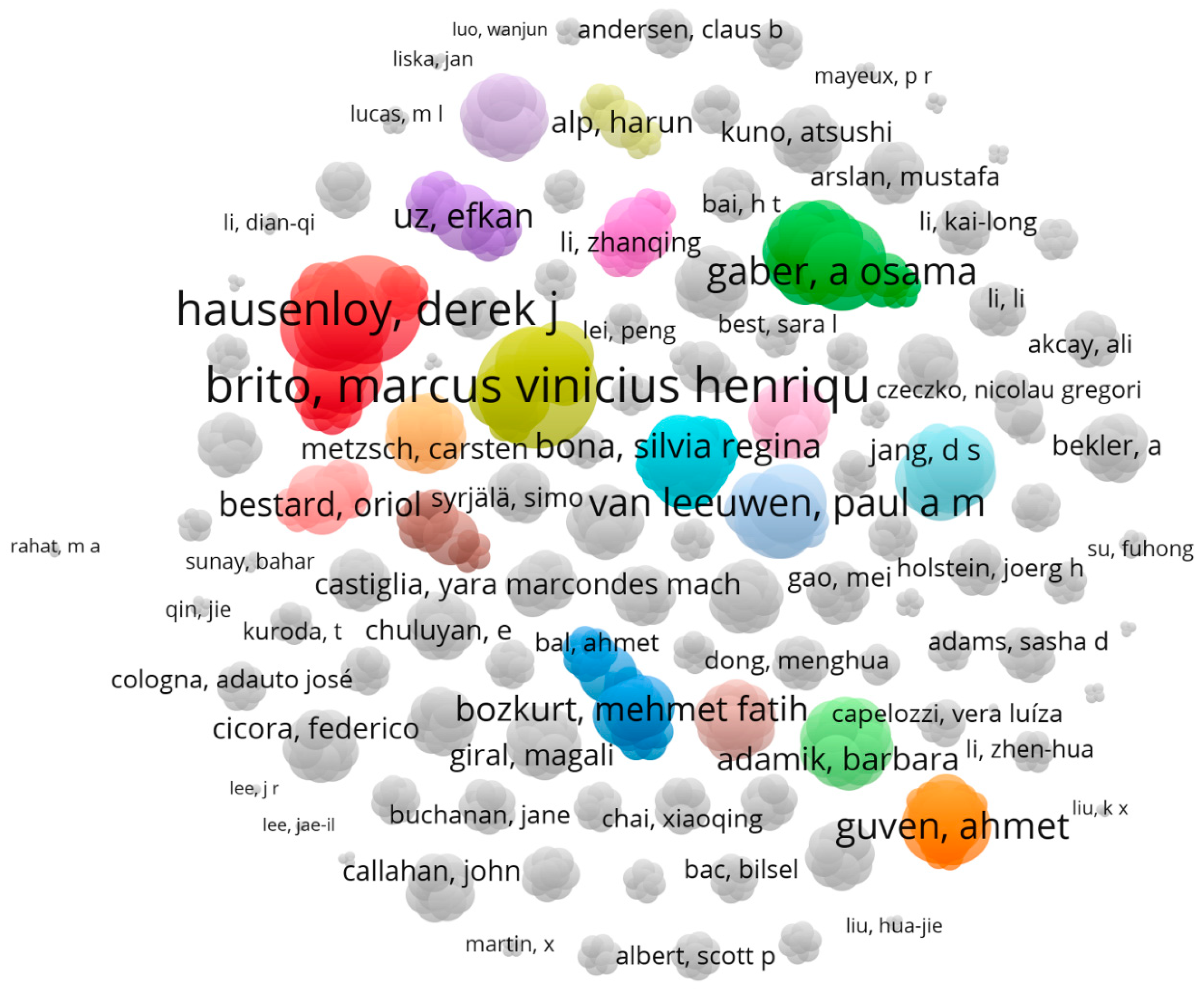
Figure 7.
The molecules and interactions that are involved in the binding site of best binding conformation Eplerenone and nicotinamide adenine dinucleotide (NAD) with the latest receptors that have been undergone studies in which their role in ischemic renal reperfusion injury (IRI) has been studied. The interactions between Eplerenone and following receptors: Aldehyde dehydrogenase (AD) (A), Estrogen receptor (ER) (B), Kloth protein (D), Mineralocorticoid receptor (MR) (E), Sitruin1 (F), Toll-like receptor 4 (TLR4) (G) and the interaction between NAD with Glucuronidase (C), myeloid differentiation factor (MDF) (F), and tumor necrosis factor receptor (TNFR) (I) are demonstrated in details.
Figure 7.
The molecules and interactions that are involved in the binding site of best binding conformation Eplerenone and nicotinamide adenine dinucleotide (NAD) with the latest receptors that have been undergone studies in which their role in ischemic renal reperfusion injury (IRI) has been studied. The interactions between Eplerenone and following receptors: Aldehyde dehydrogenase (AD) (A), Estrogen receptor (ER) (B), Kloth protein (D), Mineralocorticoid receptor (MR) (E), Sitruin1 (F), Toll-like receptor 4 (TLR4) (G) and the interaction between NAD with Glucuronidase (C), myeloid differentiation factor (MDF) (F), and tumor necrosis factor receptor (TNFR) (I) are demonstrated in details.
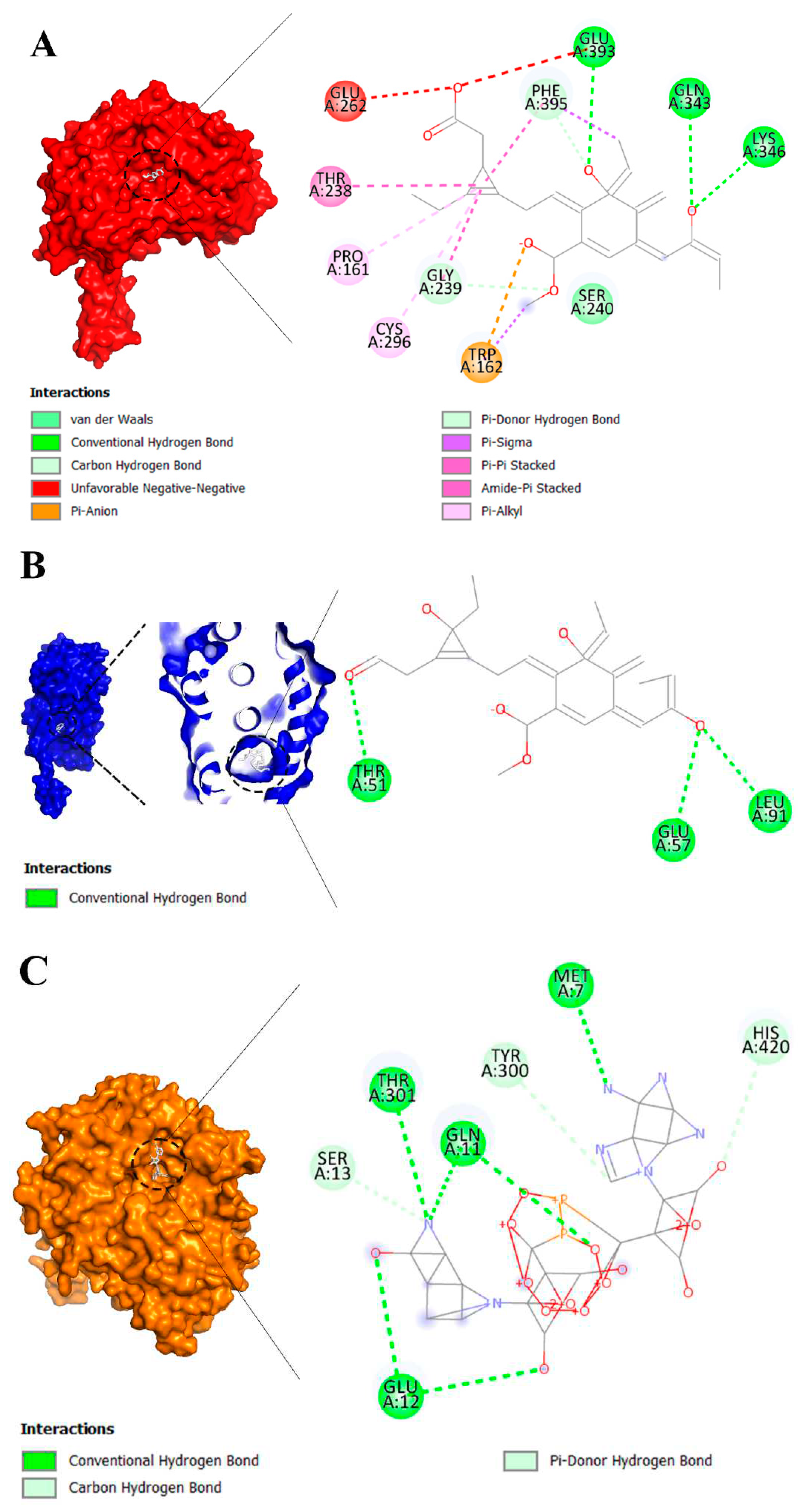
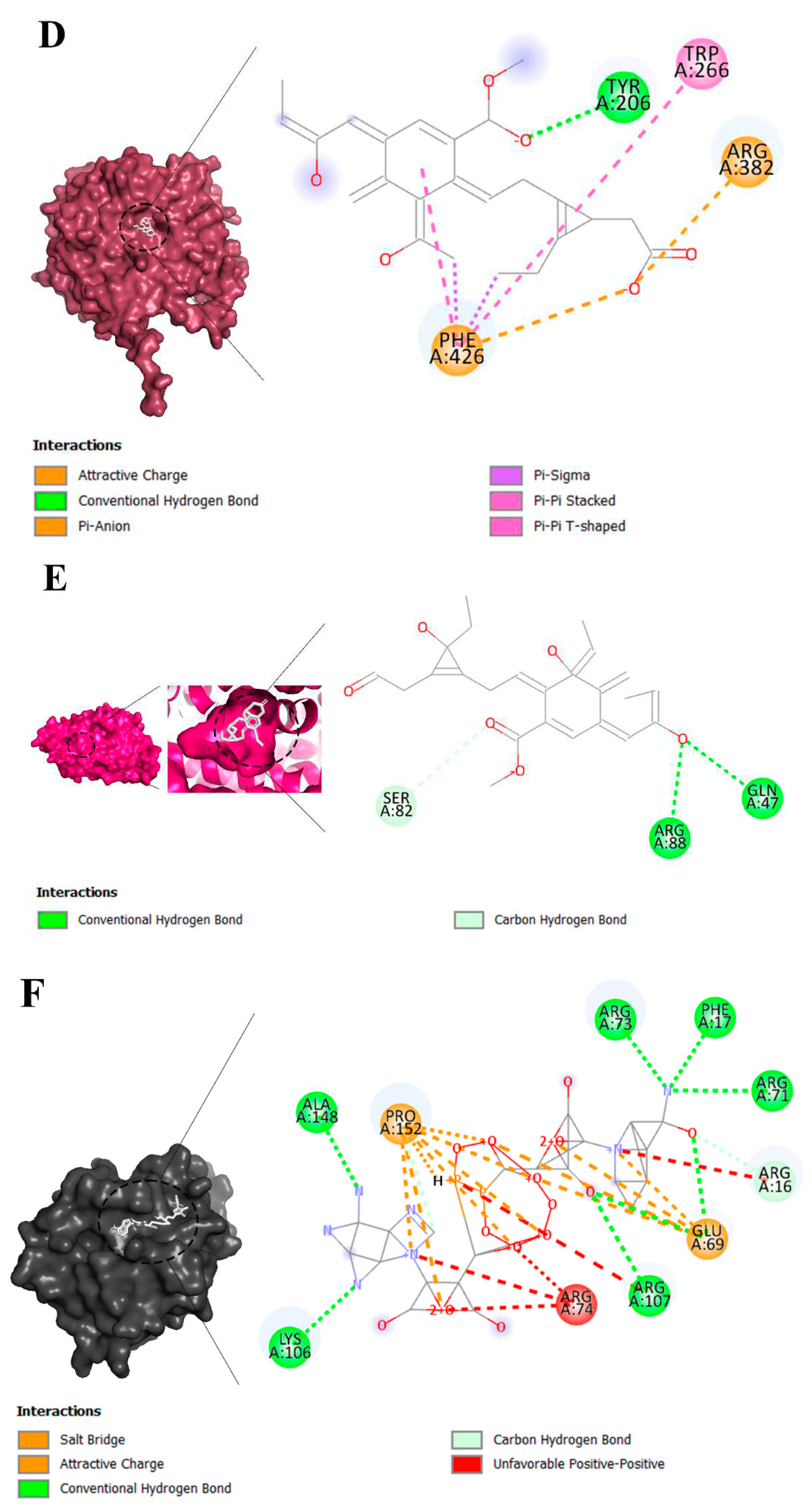
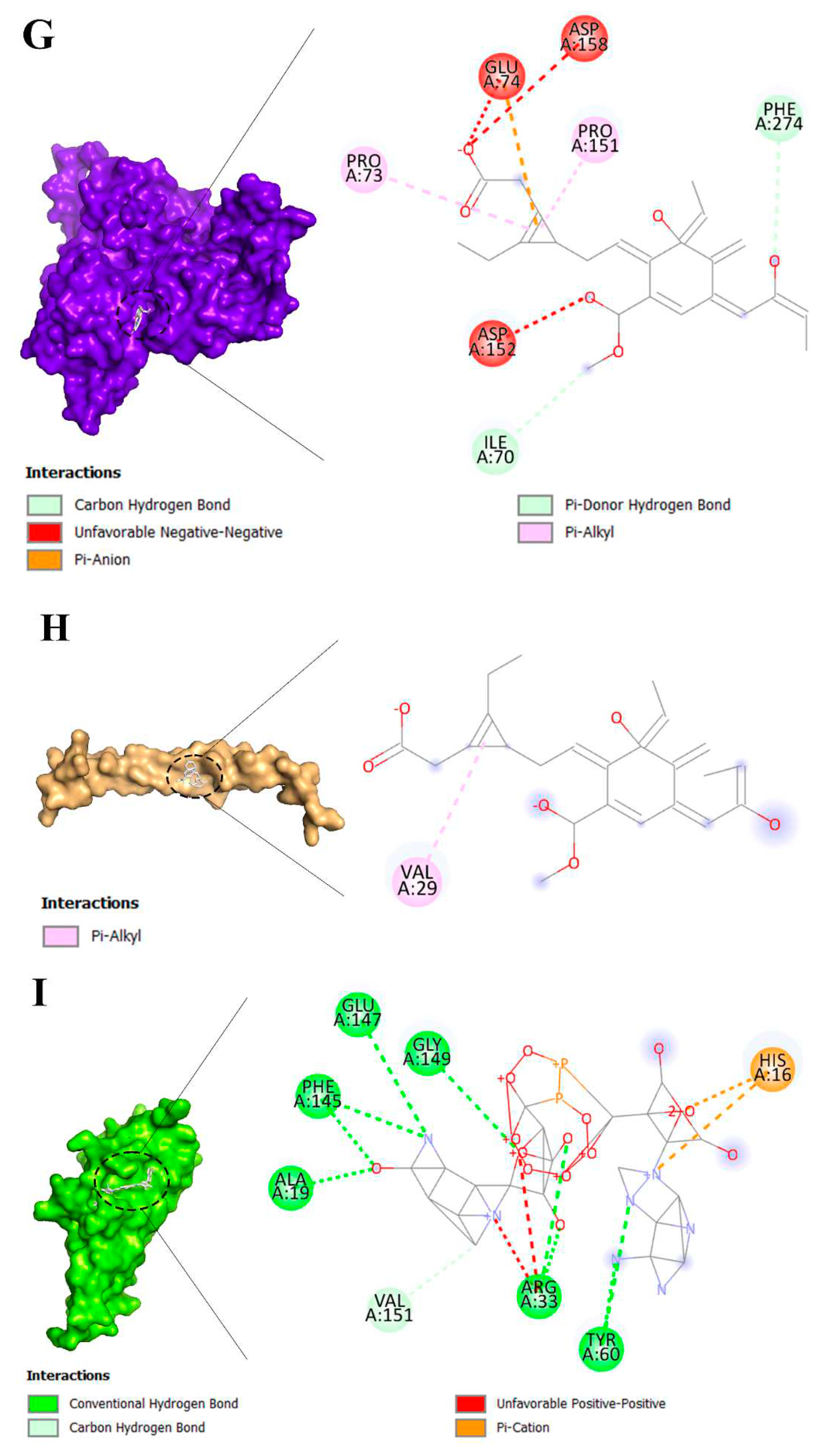

Table 1.
The most used MeSH keywords in studies in which various operative methods for preventing kidney ischemia-reperfusion injury are studied.
Table 1.
The most used MeSH keywords in studies in which various operative methods for preventing kidney ischemia-reperfusion injury are studied.
| NO | Keyword | Occurrences | Total link strength | NO | Keyword | Occurrences | Total link strength |
|---|---|---|---|---|---|---|---|
| 1 | Treatment outcome | 44 | 255 | 11 | Immunohistochemistry | 21 | 120 |
| 2 | Creatinine | 43 | 247 | 12 | Liver | 20 | 105 |
| 3 | Ischemia | 36 | 194 | 13 | Malondialdehyde | 20 | 109 |
| 4 | Time factors | 36 | 206 | 14 | Superoxide dismutase | 20 | 105 |
| 5 | Double-blind method | 35 | 204 | 15 | Protective agents | 19 | 100 |
| 6 | Biomarkers | 34 | 209 | 16 | Blood urea nitrogen | 18 | 89 |
| 7 | Apoptosis | 29 | 157 | 17 | Antioxidants | 17 | 84 |
| 8 | Oxidative stress | 29 | 187 | 18 | Lung | 17 | 80 |
| 9 | Ischemic preconditioning | 28 | 150 | 19 | Kidney diseases | 15 | 57 |
| 10 | Nephrectomy | 23 | 119 | 20 | Tumor necrosis factor-alpha | 15 | 84 |
Table 2.
The list of top 10 authors with the greatest number of published manuscripts in the field of examining the studies in which various operative methods for preventing kidney ischemia-reperfusion injury are studied and their average publication year.
Table 2.
The list of top 10 authors with the greatest number of published manuscripts in the field of examining the studies in which various operative methods for preventing kidney ischemia-reperfusion injury are studied and their average publication year.
| NO | Author | Documents | Total link strength | Average publication year |
|---|---|---|---|---|
| 1 | Brito, Marcus Vinicius Henriques | 5 | 35 | 2016 |
| 2 | Barakat, Nashwa | 3 | 8 | 2011 |
| 3 | Corso, Carlos Otávio | 3 | 21 | 2015 |
| 4 | Costa, Felipe Lobato Da Silva | 3 | 19 | 2016 |
| 5 | Gomes, Regina De Paula Xavier | 3 | 13 | 2015 |
| 6 | Guven, Ahmet | 3 | 21 | 2008 |
| 7 | Hausenloy, Derek J | 3 | 31 | 2014 |
| 8 | Hussein, Abdel-Aziz M | 3 | 8 | 2011 |
| 9 | Korkmaz, Ahmet | 3 | 21 | 2008 |
| 10 | Santos, Emanuel Burck Dos | 3 | 21 | 2015 |
Table 3.
The list of top 10 authors with the most tendency to collaborate with other researcher in related field.
Table 3.
The list of top 10 authors with the most tendency to collaborate with other researcher in related field.
| NO | Author | Link | Total Link Strength |
|---|---|---|---|
| 1 | Brito, Marcus Vinicius Henriques | 22 | 35 |
| 2 | Hausenloy, Derek J | 27 | 31 |
| 3 | Ariti, Cono | 19 | 23 |
| 4 | Candilio, Luciano | 19 | 23 |
| 5 | Kolvekar, Shyam | 19 | 23 |
| 6 | Yellon, Derek M | 19 | 23 |
| 7 | Van Leeuwen, Paul A M | 14 | 22 |
| 8 | Van Norren, Klaske | 14 | 22 |
| 9 | Gaber, A Osama | 21 | 22 |
| 10 | Hemmerich, Stefan | 21 | 22 |
Table 4.
Latest compounds, protein and receptors that have been undergone studies in which their role in ischemic renal reperfusion injury (IRI) has been studied.
Table 4.
Latest compounds, protein and receptors that have been undergone studies in which their role in ischemic renal reperfusion injury (IRI) has been studied.
| Keyword | Occurrences | Total link strength | Average publication year | Their role in IRI | References |
|---|---|---|---|---|---|
| Ligands | |||||
| Benzodioxole | 1 | 4 | 2018 | Amelioration | [28] |
| Eplerenone | 1 | 8 | 2018 | Amelioration | [29] |
| Hydrocortisone | 1 | 9 | 2018 | Amelioration | [30] |
| Indoles | 1 | 5 | 2019 | Amelioration | [31] |
| Nicotinamide adenine dinucleotide | 1 | 13 | 2021 | Amelioration | [32] |
| Niacinamide | 1 | 13 | 2021 | Amelioration | [33] |
| Receptors | |||||
| Aldehyde dehydrogenase, mitochondrial | 1 | 4 | 2018 | Amelioration | [34] |
| Mineralocorticoid receptor antagonists | 1 | 8 | 2018 | Amplification | [35] |
| TNF receptor-associated factor 6 | 1 | 5 | 2018 | Amplification | [36] |
| Estrogen receptor alpha | 1 | 5 | 2018 | Amelioration | [37] |
| Toll-like receptor 4 | 1 | 5 | 2018 | Amplification | [38] |
| Myeloid differentiation factor 88 | 1 | 5 | 2018 | Amplification | [39] |
| Glucuronidase | 2 | 26 | 2020 | Amelioration | [40] |
| Klotho proteins | 2 | 26 | 2020 | Amelioration | [41] |
| Sirtuin 1 | 1 | 13 | 2021 | Amelioration | [42] |
Table 5.
The binding affinity of brand-new ligands and receptors that have been undergone studies in which their role in ischemic reperfusion injury has been studied (Kcal/mole).
Table 5.
The binding affinity of brand-new ligands and receptors that have been undergone studies in which their role in ischemic reperfusion injury has been studied (Kcal/mole).
| Ligands | Receptors | ||||||||
|---|---|---|---|---|---|---|---|---|---|
| AD* | ER | Glucuronidase | Klotho protein | MR | MDF | Sirtuin 1 | TLR4 | TNFR | |
| Benzodioxole | -5.5 | -5.7 | -6.2 | -6.2 | -6.2 | -5.4 | -6.2 | -3.9 | -5.4 |
| Eplerenone | -13.4 | -12.9 | -11.3 | -11.7 | -12.6 | -9.2 | -11.7 | -8.8 | -9.0 |
| Hydrocortisone | -12.3 | -11.6 | -11.5 | -10.5 | -11.5 | -8.6 | -11.6 | -8.4 | -8.6 |
| Indole-3-acetic acid | -6.6 | -7.0 | -8.1 | -7.8 | -7.3 | -6.1 | -7.1 | -5.4 | -5.3 |
| Nicotinamide | -5.9 | -5.6 | -6.3 | -5.8 | -5.7 | -4.8 | -5.7 | -4.0 | -5.3 |
| NAD | -12.5 | -11.6 | -12.1 | -11.5 | -10.4 | -10.6 | -10.8 | -7.3 | -11.0 |
*AD, Aldehyde dehydrogenase; ER, Estrogen receptor; MR, Mineralocorticoid receptor; MDF, myeloid differentiation factor; TLR4, Toll-like receptor 4; TNFR, tumor necrosis factor receptor; NAD, nicotinamide adenine dinucleotide
Table 6.
Methods of prevention of ischemia-reperfusion injury of the kidney and their effects
| Method | Patients/Model | Effects | References |
|---|---|---|---|
| Local cooling of the kidney graft using a plastic bag filled with ice. | 23 patients | Long-term maintenance of optimally low temperature during kidney vascular anastomoses to reduce the negative effects of WIT, such as a low frequency of DGF and acute rejection, and optimal GFR after surgery. | [22] |
| Local cooling of the pelvis using ice slush during robotic kidney transplantation. | 7 patients | Local cooling during vascular anastomoses to reduce the negative effects of WIT. | [43] |
| A controllable double-cycle cryogenic device with a circulating cooling system (cold saline solution: 0-4°C) and warming system (warm sterile water: 30-35°C). | 20 pigs | Local cooling of the renal graft during vascular anastomoses to reduce the negative effects of WIT with simultaneous warming of the peritoneum and lumbar muscles. | [44] |
| Net-restrictive plastic jacket with a circulating cooling system that uses saline solution at a temperature of 0-4°C. | 9 patients | Local cooling of the renal graft during vascular anastomoses to reduce the negative effects of WIT. | [45] |
| Intra-abdominal cooling device with double silicone sheaths for continuous circulation of 4°C ethanol and methylene blue during open kidney transplantation. | 13 pigs | Local cooling of the renal graft during vascular anastomoses by continuously circulating 4°C ethanol and methylene blue to reduce the negative effects of WIT. | [46] |
| Intra-abdominal cooling device with double silicone sheaths for continuous circulation of 4°C ethanol and methylene blue during robotic kidney transplantation. | 23 pigs | Local cooling of the renal graft during vascular anastomoses by continuously circulating 4°C ethanol and methylene blue to reduce the negative effects of WIT. | [47] |
| A cooling device for the kidney graft made of thermal insulation materials with a cold saline circulation system. | 6 pigs 5 patients |
Long-term maintenance of optimal temperature (10-15°C) during vascular anastomoses to reduce the negative effects of WIT. | [48] |
| A thermally insulating jacket for the kidney. | 5 pigs | Long-term maintenance of optimal temperature (0-15°C) during vascular anastomoses to reduce the negative effects of WIT. | [49] |
| An ice bag for placing the kidney transplant during implantation. | 66 patients | Local cooling of the renal graft during vascular anastomoses to reduce the negative effects of WIT. | [50] |
| Kidney cooling with Ringer's solution through the renal artery with drainage through an incision in the renal vein during robotic laparoscopic resection. | 37 patients | Local intraparenchymal cooling of the kidney during its resection to reduce the negative effects of WIT. | [51] |
| Continuous retrograde cooling of the kidney with irrigated cold saline solution (1.0-1.3°C) through the ureter during ischemia. | 6 pigs | Renal pelvis continuous local cooling during clamping of the renal artery to reduce the negative effects of WIT. | [52] |
| Continuous retrograde cooling of the kidney during resection with irrigated cold saline solution through a catheterized ureter. | 10 patients | Renal pelvis local cooling of the kidney during ischemia to reduce the negative effects of WIT. | [53] |
| Gradual controlled increase in kidney temperature by machine perfusion (from 4°C to 20°C) after cold ischemia and before reperfusion. | 12 pigs | A gradual increase of the renal temperature before reperfusion reduces mitochondrial dysfunction and apoptosis after kidney reperfusion by half. | [16] |
| Hydrodynamic fluid injection into the renal vein (retrograde) after ischemia and reperfusion. | 5 rats | Retrograde fluid injection improves microcirculation after ischemia and reperfusion, reduces inflammatory cell infiltration of parenchyma, and leads to a rapid recovery of renal function. | [54] |
| Capsulotomy of the kidney after cold and warm ischemia. | 8 pigs | Reduction of intraparenchymal pressure and elimination of compartment syndrome after reperfusion to improve the structural and functional condition of the transplanted kidney. | [55] |
| Microcapsulotomy after ischemia and reperfusion. | 13 mice | Reducing the severity of compartment syndrome of the transplanted kidney to improve its structural and functional condition. | [56] |
| Microcapsulotomy in combination with the introduction of endothelial stem cells. | 29 mice | Combination therapy reduces morphological damage to the kidneys (tubules), infiltration of macrophages, and increases the index of proliferation and regeneration. | [57] |
| Intraoperative increase of blood pressure in the kidney. | 106 patients | Maintenance of arterial blood pressure ≥150 mmHg before and during reperfusion improves microcirculation of the kidney and is associated with early stabilization of its function. | [58] |
| Intraoperative splenic ischemic preconditioning before kidney implantation. | 18 rats | Reduction of the release of inflammatory mediators and effective reduction of serum creatinine levels. | [59] |
| Remote ischemic preconditioning of the lower limb before organ ischemia. | 18 rats | Activation of antioxidant protection of liver and kidney cells during ischemia. | [60] |
| Intraabdominal administration of MSCs after ischemia and reperfusion of both kidneys. | 18 rats | Improvement of kidney function after ischemia-reperfusion injury by reducing inflammatory and oxidative reactions. | [61] |
| Introduction of MSCs into the renal artery and renal vein after ischemia and reperfusion of the kidney. | 10 rats | Improvement of kidney function in ischemia-reperfusion injury, reduction of renal tissue fibrosis, and induced IRI. | [62] |
| Introduction of own venous blood (1 ml) into the renal artery before kidney reperfusion. | 30 rabbits | Venous blood reduces the production of reactive oxygen species and has an antioxidant effect on renal tissue after ischemia and reperfusion. | [63] |
DGF, delayed graft function; GFR, glomerular filtration ratio; IRI, ischemic-reperfusion injury; MSC, mesenchymal stromal/stem cells; WIT, warm ischemic time.
Table 7.
Comparison of models on the impact on kidney IRI.
| Type | Method | Pros | Cons | Author |
|---|---|---|---|---|
| Local kidney cooling by a closed system | Local cooling of the kidney graft with a plastic bag with ice (23 patients) |
|
|
[22] |
| Local cooling of the pelvis with ice slush during robotic kidney transplantation (7 patients) |
|
|
[43] | |
| A controllable double-cycle cryogenic device with circulating cooling (cold saline solution: 0-4°C) and warming (warm sterile water: 30-35°C) system (20 pigs) |
|
|
[44] | |
| Net-restrictive plastic jacket with circulating cooling system by saline solution at a temperature of 0-4°C (9 patients) |
|
|
[45] | |
| Intra-abdominal cooling device with double silicone sheaths for continuously circulating of 4°C ethanol and methylene blue in open kidney transplantation (13 pigs) |
|
|
[46] | |
| Intra-abdominal cooling device with double silicone sheaths for continuously circulating of 4°C ethanol and methylene blue in robotic kidney transplantation (23 pigs) |
|
|
[47] | |
| Cooling device for kidney graft made of thermal insulation materials with cold saline circulation system (6 pigs – phase #0; 5 patients – phase #1) |
|
|
[48] | |
| Thermally insulating jacket for kidney (5 pigs) |
|
|
[49] | |
| An ice bag for placing a kidney transplant during implantation (66 patients) |
|
|
[50] | |
| Local cooling of the kidney with cold solution irrigation or ice slush during its laparoscopic resection (Review) |
|
|
[69] | |
| Continuous retrograde cooling of the kidney with irrigated cold saline solution (1.0-1.3°C) through the ureter during ischemia (Pig model) |
|
|
[52] | |
| Continuous retrograde cooling of the kidney during its resection with irrigated cold saline solution through a catheterized ureter (10 patients) |
|
|
[53] | |
| Renal perfusion | Cooling of the kidney with Ringer's solution through the renal artery with evacuation through an incision in the renal vein during its robotic laparoscopic resection (37 patients) |
|
|
[51] |
| Gradual controlled increase of kidney temperature by machine perfusion (from 4°C to 20°C) after cold ischemia and before reperfusion (12 pigs) |
|
|
[16] | |
| Intraoperative increase of blood pressure in the kidney (106 patients) |
|
|
[58] | |
| Hydrodynamic fluid injection into the renal vein (retrograde) after ischemia and reperfusion (5 rats) |
|
|
[54] | |
| Renal capsulotomy | Capsulotomy of the kidney after cold and warm ischemia (8 pigs) |
|
|
[55] |
| Microcapsulotomy after ischemia and reperfusion (13 mice) |
|
|
[57] | |
| Microcapsulotomy in combination with the introduction of endothelial stem cells (29 mice) |
|
|
Herrler T et al.40 | |
| Ischemic preconditioning | Intraoperative splenic ischemic preconditioning before kidney implantation (18 rats) |
|
|
[59] |
| Remote ischemic preconditioning of the lower limb before organs ischemia (18 rats) |
|
|
[60] | |
| Using the MSC | Intraabdominal administration of MSC after ischemia and reperfusion of both kidneys (18 rats) |
|
|
[61] |
| Introduction of MSC into the renal artery and renal vein after ischemia and reperfusion of the kidney (10 rats) |
|
|
[62] | |
| Venous blood reperfusion | Introduction of own venous blood (1 ml) into the renal artery before kidney reperfusion (30 rabbits) |
|
|
[63] |
| Retrograde venous kidney reperfusion before conventional arterial reperfusion (15 patients) |
|
|
[79] |
IRI = ischemic-reperfusion injury, WIT = warm ischemic time, DGF = delayed graft function, GFR = glomerular filtration ratio, CIT = cold ischemic time, MSC = mesenchymal stem cells.
Table 8.
Scoring system for intraoperative methods of preventing ischemia-reperfusion injury of the kidney: a comprehensive overview of pharmacological, surgical, and cellular approaches based on clinical, in vivo, and in vitro research.
Table 8.
Scoring system for intraoperative methods of preventing ischemia-reperfusion injury of the kidney: a comprehensive overview of pharmacological, surgical, and cellular approaches based on clinical, in vivo, and in vitro research.
| Therapeutic approach | Clinical research (0-3) | In vivo research (0-3) | In vitro research (0-3) | Total score (0-9) |
|---|---|---|---|---|
| Ischemic preconditioning | 3 | 3 | 3 | 9 |
| Renal perfusion | 3 | 3 | 2 | 8 |
| Tissue engineering | 2 | 2 | 3 | 7 |
| Local cooling of the kidney | 2 | 2 | 1 | 5 |
| Renal capsulotomy | 1 | 2 | 1 | 4 |
| Venous blood reperfusion | 2 | 1 | 1 | 4 |
Table 9.
Scoring System for Intraoperative Methods of Preventing Ischemia-Reperfusion Injury of the Kidney.
Table 9.
Scoring System for Intraoperative Methods of Preventing Ischemia-Reperfusion Injury of the Kidney.
| Therapeutic Approach | Clinical Approval | Difficulty of Test | Cost of Operation | Equipment Needed | Availability | Total Score |
|---|---|---|---|---|---|---|
| Tissue Engineering | 1 | 5 | 5 | 5 | 1 | 17 |
| Local Cooling | 3 | 2 | 4 | 2 | 4 | 15 |
| Renal Perfusion | 2 | 3 | 3 | 3 | 3 | 14 |
| Ischemic Preconditioning | 2 | 3 | 3 | 2 | 4 | 14 |
| Venous Blood Reperfusion | 2 | 2 | 4 | 3 | 3 | 14 |
| Renal Capsulotomy | 1 | 4 | 2 | 4 | 2 | 13 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



