
Submitted:
26 April 2023
Posted:
27 April 2023
You are already at the latest version
Abstract
Abstract: Background: Trauma is the leading cause of morbidity and mortality in young patients, acute surgical conditions cause morbidity and mortality in patients of all ages. Computed tomography scan (CT) assist greatly in the investigation and management of these patients with blunt and penetrating trauma, facilitating early diagnosis and expedites early appropriate treatment of these patients. Acute non-traumatic surgical conditions also mimic non-surgical pathologies and differentiating the two is important because management is different and any delay in surgical intervention results in high morbidity and some may even result in mortality. Method: Literature review of the role of multidetector CT scan (MDCT) in managing acute surgical emergencies and trauma-diagnosis in the trauma patient and patients presenting with acute surgical emergencies. The focus is on the role of the MDCT in the management of these patients. Results highlight that the use of MDCT expedites management of these patients, allowing early surgical intervention and preventing unnecessary surgical interventions where the intervention is not indicated, based on the MDCT results. Conclusion: This paper emphasizes the important role that is played by the MDCT in the management of the above patients.
Keywords:
Multidetector CT
; blunt trauma
; penetrating trauma
; acute surgical emergencies
; imaging
; utility
1. Introduction
Computed tomography (CT) has become the mainstay of evaluating hemodynamically stable patients in trauma since its introduction in 1970’s after development by British engineer Godfrey Hounsfield of EMI Laboratories . He co-invented the CT scanner with Dr Allan Cormack, a South African trained physicist. They were both awarded the Physiology and Medicine Nobel Prize in 1979. The research was funded by the Electric and Music Industries company. [1]. It allows for rapid, dependable imaging in detecting and characterizing various injuries sustained by trauma patients. Additionally, multidetector CT has improved the management of patients presenting with severe acute abdominal pain, by identifying patients that require surgical intervention timeously and allowing those not needing surgery to receive appropriate care.
2. Methods
A focused literature review was undertaken using the PUBMED and Google Scholar systems with the key-words and MeSH terms: trauma, multidetector CT, Pan CT, acute surgical emergency and CT. We focused on review type articles and those published within the most recent 10 years with selected earlier seminal articles.
3. Results
The search returned numerous results and the selected items addressed the current status of the role of CT scans in each of the respective components of penetrating or blunt trauma and in the diagnostic approach to acute surgical emergencies. These are summarized in the discussion with the practical take-home messages for each section.
4. Discussion
The CT scan in trauma can be divided into two categories, namely the whole-body scan commonly known as a Pan CT, or trauma full-body scan, and then selective regional CT Scans, these commonly being the non-contrasted CT Brain; non-contrasted CT Neck; CT angiography with suspected neck vessel or aerodigestive injury; contrasted CT Chest and also contrasted CT Abdomen, with or without renal and cystogram delayed phase images.
- 1. PAN CT (Whole Body CT)
PAN CT is most often used in patients who have sustained multiple injuries after significant trauma and have haemodynamic stability. Recent evidence shows that the patients that have Pan CT have a better survival than patients who have selected imaging with somewhat less risk of missed injury. [2] Advantages of Pan CT in blunt polytrauma patient setting are manifold, including rapid identification of multiple injuries, improved prioritization of management, and the ability to define and guide selective non-operative management of solid organ injuries, in both blunt and penetrating injury [2,3,4] Relying on clinical assessment and mechanism of injury may underestimate the injury severity by up to 30% [5,6]. Pan CT has the benefit that injuries in all cavities will be identified early with one modality and with less contrast exposure [7].
The REACT-2 randomized study found that while pan CT was safe, and shortened the time to imaging completion, there was no survival benefit in their cohort of mainly blunt trauma. Moreover, many patients in the selective group had to return to radiology for further imaging studies with less overall radiation in the pan CT group [8]. Another subset of patients is those with severe traumatic brain injury, especially when polytrauma injuries in other body regions are present. The rapid ability to include or exclude injuries, and determine the severity thereof, found on pan CT scan may help to direct important therapeutic decisions. It should be noted; however, that this is in major trauma patients rather than all patients including those with less severe injury [9,10].
The main concern with the Pan CT is the exposure to radiation which increases the risk of malignancy later in life, however the risk of missed injury outweighs the risk of malignancy later as some injuries results in death if diagnosis is delayed [6,10,11,12]. In a similar vein the risk of contrast induced nephropathy has recently been dispelled in numerous large studies [13,14,15,16].
The pan CT allows for injury severity classification using the American Association for the Surgery of Trauma abbreviated injury scale and assists in non-operative solid organ trauma management as demonstrated in Figure 1. Even with the lack of radiologist resources in many places the pan CT can be safely viewed by the experienced trauma surgeon with highly valid decision-making and low missed injury or error rates [17,18].
The Pan CT is best performed with a standard protocol that consists of the following:
non-contrasted head; non-contrasted cervical spine; an arterial phase from the neck at the skull-base including the chest and abdominal vessels, down to the feet if there are lower limb injuries and the portal venous phase for abdominal organ injury identification. For selected patients the additional steps to the protocol may include a delayed phase of the abdomen/pelvis (also known as the ureteric phase) and CT cystogram [5]. Indications for imaging are listed in Table 1.
Whole body CT in unstable trauma
Carlos Ardonez and colleagues conducted a retrospective study in a level 1 trauma center, in Cali, Colombia, between January 2016 to December 2017. They compared radiation exposure and the time between emergency department and operating room between the patients who had whole body CT versus organ specific CT. One-hundred and twenty-three patients were included, 70 whole body CT and 53 organ specific CT. Forty-seven percent of organ specific CT patients had to have another trip to the scanner to exclude other injuries which was not necessary for the pan CT group. The pan CT group spent less time in the CT scanner than the organ specific group (22 vs. 32 min), in keeping with the REACT-2 findings [8,12].
In light of these findings the authors were convinced that pan CT is an efficient and safe tool for early diagnosis of a severely injured polytrauma patient. This is an area of interest in the trauma community as the pan CT has been advocated for stable patients only but the emerging evidence exists to demonstrate that this tool is useful in unstable patients as it assess all cavities and potential causes of bleeding in less than 30 minutes and the resuscitation continues as the investigation is carried out [12].
- 2.
- CT Neck
Patients presenting with neck pathology whether traumatic or non-traumatic (acute surgical pathology) require an early diagnosis and management plan to prevent high morbidity and mortality associated with delayed management. Multi-detector CT (MDCT) neck is vital in early diagnosis and management of these patients.
CT neck is useful in the diagnosis of the acute trauma to the neck (blunt and penetrating) that are haemodynamicaly stable since most unstable patients require emergency operative or endovascular intervention. It accurately delineates occult injuries and identifies the patient that requires surgical management early. MDCT neck has sensitivity of 94.4% and a specificity of 96.7% in identifying vascular injury of the neck. [19]
Diagnostic evaluation of injuries has evolved over the past few decades from an operative versus non-operative approach, as defined by the neck zones involved, to more selective management based on the combination of the mechanism of injury, signs and symptoms, anatomic location of the wound, and increased use of computed tomography (CT). [20,21] Currently, the no zone approach is used in penetrating cervical trauma, where all the stable patients with an injury that breaches the platysma are investigated with the CT neck which includes the angiogram phase. CT imaging enables visualization of multiple structures across all three zones of the neck [20,21].
Madsen and colleagues conducted a study between January 2011 and May 2018 with penetrating neck injuries (PNI) to identify the correlation between the external wound and the injury sustained internally to assess if a ‘no zone “ approach is feasible. All the patients with confirmed injury were included. PNI was present in 1075 patients, 298 had vascular injury or aerodigestive-tracheal injury. While 176 patients had the internal injury correlating with the external injury, 70 patients had no such correlation. In 52 patients the correlation could not be determined. The ‘no zone’ approach was therefore supported by the study [21].
CT neck will potentially delineate the trajectory of the penetrating injury and that would help to identify patients that will require further imaging to exclude esophageal injury, if one is not immediately visible on the CT images. [22,23] If the trajectory is suggestive of oesophageal injury, water soluble swallow or endoscopy may be performed to exclude the injury. CT also identifies tracheal injury and the injury severity can be assessed and this assists in determining which patients that require surgical intervention from those that can be managed non-operatively. Figure 2 demonstrates a tracheal injury and surgical emphysema.
Parida and colleagues conducted a study looking at laryngotracheal trauma, which is a rare life-threatening emergency that requires early identification and immediate intervention. Twenty-six patients with laryngotracheal trauma from a tertiary hospital in India were included. The retrospective study was conducted between January 2011 and March 2016. Patients with caustic ingestion, superficial injuries and burns injuries were excluded. A total of 253 patients presented with neck injuries only 26 patients had a breach in the laryngotracheal framework (15 blunt & 11 penetrating trauma). All blunt trauma patients had a CT neck and only 4 of penetrating trauma had a CT. All patients with penetrating trauma had surgical exploration. The majority of blunt trauma patients had conservative management with a small number going for surgical exploration. The conclusion was that a CT neck plays a major role in decision making in the management of blunt laryngotracheal injury. [24]
CT neck for acute surgical emergencies will help identify patient with sepsis extending to the retropharynx and mediastinum and deep cervical tissues in order to direct the surgery for these patients. Patients with dental abscess that has pus collection extending to the cervical tissue can also be identified and managed timeously. Pharyngeal abscess can extend to deep cervical tissue and clinical examination may not be able to determine the extent of the disease thus necessitating the use of MDCT neck and chest in order to identify deep seated collection. [25,26]
Eissa and colleagues conducted a study looking at diagnostic accuracy of the CT scan in the diagnosis of the deep-seated neck infection. CT was done do differentiate between the phlegmon and abscess. Among the 66 patients that were included 64 showed abscess and 59 of those patients had abscess on surgical intervention whilst 5 had a phlegmon. The study concluded that CT had a 92% accuracy in diagnosis of neck abscess [25].
Corrosive ingestion is a rare but potentially devastating event and, despite the availability of effective preventive public health strategies, injuries continue to occur. Most clinicians have limited personal experience and rely on guidelines; however, uncertainty persists about best clinical practice. Ingestions range from mild cases with no injury to severe cases with full thickness necrosis involving esophagus and stomach. MDCT scan is superior to endoscopy for stratification of patients to either emergency resection or observation. The study conducted showed that its preferable to evaluate the patient with a CT scan than to perform oesophagoscopy, to avoid risk of perforation. [27]
- 3.
- CT Chest
Chest CT with contrast is mostly used for accurate diagnosis of acute vascular trauma and suspected aerodigestive injury. It identifies the site and type of vascular injury. By defining the trajectory of penetrating trauma helps to identify the patients that require further imaging to exclude esophageal injury.
The MDCT chest does assist with the evaluation of other chest injuries as one can evaluate the severity of pulmonary contusions in the face of parenchymal trauma, thus giving the clinician the indication for level of care for the patient, such as ICU admission if the amount of lung involvement is significant – the clinical picture may lag behind the CT findings. CT also excludes major mediastinal pathology in cases of blunt trauma with pneumomediastinum. [28,29] For blunt thoracic trauma resulting in multiple rib fractures, MDCT delineates the number and site of rib fracture while the 3D reconstruction assists with the planning of the internal rib fixation for the patients that qualify for open reduction and internal fixation (see Figure 3).
Bronchial injuries can also be identified using the MDCT chest and it will help determine the extent of injury thus assisting with decision making regarding surgical intervention. The characteristic expression of tracheal rupture in CT presents as follows: (I) gas dispersion around the broken ends; (II) bronchial lumen stenosis or blockage; (III) bronchial displacement or angular deformity. The injuries that are less than a third of the diameter of the bronchus can be managed nonoperatively if the patient is clinically stable and does not deteriorate clinically [29]. See Figure 4 for an example of such an injury
CT chest has a 100% sensitivity and a negative predictive value for excluding esophageal perforation. In the absence of mediastinal collection, pneumomediastinum and esophageal wall defect the MDCT is adequate to exclude the esophageal injury, but if any of these features are present then fluoroscopy or endoscopy should be performed to rule out an esophageal injury. [30,31]
Strumwasser and colleagues examined the benefit of CT scan in acute penetrating thoracic trauma by means of a retrospective study over a ten-year period. Haemodynamically stable patients with penetrating thoracic trauma were included. A total of 212 patients met the criteria. Thoracic CT scan had a sensitivity of 82%, specificity of 99%, positive predictive value of 90%, a negative predictive value of 99%, and an accuracy of 99% in predicting surgery vs. NOM [31].
CT chest in retained hemothorax identifies the extent and the exact location of the retained hemothorax and also identifies patients that have empyema with an enhancing pseudo-capsule. All this improves patient care by directing the clinician in the management of the retained hemothorax, as to whether the patient requires video-assisted thoracoscopic surgery (VATS) or mini- versus open thoracotomy [32,33]. Velmahos and colleagues compared plain chest x-ray and CT chest in predicting the need for VATS and the study concluded that the x-ray was not adequate for decision-making but the CT had good correlation between the CT findings and amount of blood evacuated concluding that CT chest is the investigation of choice when evaluating the patient with a retained haemothorax [33].
Moving to non-trauma pathology an example is descending necrotizing mediastinitis [DNM], which is a surgical emergency that requires prompt diagnosis so early surgical treatment can be provided to reduce the high mortality that is associated with the condition and a MDCT chest is the best diagnostic tool for diagnosing this condition [34,35,36].
DNM is an inflammation occurring in the oropharynx which descends to deep cervical space and mediastinum. A classification system was thought to be necessary for treatment planning. A new classification system and treatment methods for DNM was required, therefore Kuang and colleagues conducted a study that included 139 patients with DNM. The patients were placed in two groups, old classification and new classification, all based on the MDCT findings. The mortality was significantly lower in the group treated as per the new classification system (25.6 vs 9.4%) [35]
- 4.
- CT Abdomen
Selective contrasted abdominal CT is used for imaging clinically stable patients with blunt abdominal trauma, (including follow-up scans in certain patients), who have no indication for Pan CT, and a select few cases with stable penetrating abdominal trauma (tangential abdominal or right upper quadrant gunshots without peritonitis and patients with posterior abdominal stab wounds [4,37]. Figure 5 shows a bullet tract through the liver and the patient was managed non-operatively.
CT abdomen is the investigation of choice for defining injuries in hemodynamically stable patients. Injuries can be diagnosed and graded according to AAST classification and selective non-operative management can be offered for those patients that qualify for SNOM. It can exclude significant injury despite unusual clinical signs [38].
CT abdomen will timeously diagnose retroperitoneal injuries that require operative management (duodenal and colonic injuries) whether injuries are from blunt or penetrating trauma. These injuries are easily missed on clinical examination and ultrasound studies.
In cases with stab to the back, a study by Meyer and colleagues investigated the role of CT abdomen in the evaluation of these patients. The study had two hundred and five patients with stab backs. One hundred and sixty-nine patients had a negative scan. Seventeen percent (30) of the 169 patients were operated on because of clinical concern and only two had injuries identified at operations, which were diaphragmatic and a combined diaphragmatic and hepatic injury. They observed 139 patients and no sequelae developed in these patients, making this a safe approach and the current standard of care [37].
Thirty-three cases had a positive CT scan, but only twenty patients were taken to operation. Sixteen of the operated patients had significant injuries. Worryingly, seven of the sixteen patients had additional injuries not identified by the scan. There were four false positive scans. Fifteen patients were observed based on clinical judgment, most of these patients had minor injuries on CT and none of the patients developed complications [37].
For right upper quadrant and tangential gunshots, non-operative management is not commonly practiced. Navsaria and colleagues conducted a study of gunshot liver injuries over 52-month period. All stable patients that sustained right upper quadrant or right thoracoabdominal penetrating injury, with or without right sided tenderness had a contrasted CT abdomen to assess the trajectory and the organ injury. Patients without hollow viscus injury were observed with serial abdominal examination.
One hundred and ninety-one patients had a predefined injury but only 54 (28.3%) were selected for NOM. Sixty-one percent of these patients had high grade liver injury and 21 (40%) had Grade I & II injury. Other injuries included renal, diaphragm, pulmonary contusion, haemothorax and rib fractures. The success rate for non-operative management was 94.4%. [39]
A further study by Chmielewski investigated right upper quadrant gunshot patients who are stable, with localized tenderness and GCS 15/15 allowing reliable re-evaluation. Twelve patients fulfilled the criteria and they were successfully observed. One non-therapeutic laparotomy was performed for abdominal tenderness [40]. Selective nonoperative management for right upper quadrant gunshot wound can therefore be used with caution in selected patients [4,34,39]. These were similar to the findings in the scoping review undertaken by Singh and Hardcastle [4]. The take-home message is that carefully selected patients with gunshot liver injury can be managed nonoperatively with minimal morbidity.
The liver is the most frequently damaged organ in abdominal trauma. There is a high risk of hemorrhage and mortality as severity of injury and stage increases. During the last decade, management of liver trauma standards changed when the American Association of the Surgery of Trauma adjusted their guidelines to focus on early computed tomography scanning to determine the severity of liver injury trauma and the need for surgical verses nonsurgical management. Liver injury can be blunt or penetrating. Trauma teams became more multidisciplinary to focus not only on the physical but also on the psychosocial issues with trauma. Algorithms were developed to guide trauma flow and determination of severity of injury by grade. Nursing considerations and management include maintaining hemodynamic stability via accurate fluid resuscitation, monitoring of frequent vitals signs and abdominal assessment. Care must be taken to address pain and the psychosocial and emotional issues of trauma [39,40].
Non-operative management (NOM) is increasingly utilized in blunt abdominal trauma. The 1994 American Association of Surgery of Trauma grading (1994-AAST) is applied for clinical decision-making in many institutions. Recently, classifications incorporating contrast extravasation such as the CT severity index (CTSI) which is useful and 2018 update of the liver and spleen AAST were proposed to predict outcome and guide treatment, but validation is pending. The study demonstrated that the 2018-AAST and CTSI are superior to the old classification system in predicting mortality [41].
A study by Shanmuganathan investigated need for laparotomy post penetrating abdominal trauma and the study results revealed that CT had 100% sensitivity, 96% specificity, 100% negative predictive value, and 97% accuracy in predicting the need for laparotomy [42].
Non-trauma Abdominal CT
The role of abdominal CT scan in non-trauma abdominal surgical emergencies is increasing all the time. Over the past two decades, CT has become the imaging technique of choice in evaluating patients presenting with acute severe abdominal pain. Multidetector CT (MDCT) assists with the management of medical and surgical emergencies. It improves the patient outcome by allowing the clinician to make an appropriate diagnosis early which leads to appropriate management as per imaging. MDCT also reduces the rate of unnecessary surgical procedures that are done because of the clinical suspicion.
A patient presenting with acute severe abdominal pain presents a diagnostic challenge to the treating physician as the differential diagnosis is endless and it remains difficult to differentiate the medical and surgical causes of acute severe abdominal pain on clinical parameters alone with adequate certainty, therefore the use of MDCT abdomen will assist with the diagnosis and prevent unnecessary surgical interventions, that carry both morbidity and mortality when resulting in negative or non-therapeutic laparotomies. Table 2 lists some of the time-critical diagnoses that can present with acute abdominal pain and differentiates the surgical from the non-surgical causes.
Without the list being exhaustive it is obvious that a patient presenting with acute severe abdominal pain requires prompt diagnosis so as to differentiate pathology that requires surgical intervention from those that do not require surgery. Acute intestinal ischemia requires surgical intervention urgently and any delays in diagnosis will definitely result in morbidity and mortality [43].
Acute appendicitis and perforated ulcer or diverticular disease are among the causes of the acute abdominal pain that may require prompt surgical intervention and any delays have resulted in a number of morbidities such as multiple relaparotomies, ileostomies, open abdomen leading to entero-atmospheric fistula, ventral hernia and even death. CT scan in the diagnostic work-up of these conditions is highly supported in the recently published guidelines [44,45].
Acute mesenteric ischaemia is one of the causes of abdominal pain with a high mortality. Ashcof and co-workers did a study looking at the accuracy of the MDCT abdomen at the diagnosis of the acute mesenteric ischaemia. They found that the MDCT had sensitivity of 93%, a specificity of 100%, with positive and negative predictive values of 100% and 94% respectively. This suggested that the MDCT angiography is an accurate tool for expeditious diagnosis of patients suspected to acute mesenteric ischaemia [46].
5. Conclusion
A patient presenting with either acute surgical emergencies or trauma can be evaluated with the MDCT to make an accurate diagnosis which will allow prompt appropriate treatment thereby hopefully reducing the morbidity and mortality associated with a delayed diagnosis. The MDCT therefore forms an integral part of investigation in the management of the trauma patients and patients with acute surgical emergencies, with the benefit of improved outcomes.
Author Contributions
These authors contributed equally to this work. (I) Conception and design: T.N.S and T.C.H.; (II) administrative support: none; (III) provision of study materials or patients: T.N.S. and T.C.H.; (IV) collection and assembly of data: T.N.S and T.C.H.; (V) data analysis and interpretation: T.N.S and T.C.H.; (VI) manuscript writing: T.N.S. and T.C.H.; (VII) final approval of manuscript: T.N.S. and T.C.H. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable. All images used are from the Ethics approved Trauma Unit database and are used with institutional approval.
Data Availability Statement
The study did not report on any new data.
Conflicts of Interest
The authors declare no conflict of interest. The funding sponsors had no role in the design of the study; in the collection, analyses, or interpretation of data; in the writing of the manuscript; or in the decision to publish the results.
References
- Bhattacharyya KB. Godfrey Newbold Hounsfield (1919-2004): The man who revolutionized neuroimaging, Ann Indian Acad Neurol. 2016 Oct-Dec; 19(4):448-450. [CrossRef]
- Harntaweesup S, Krutsri C, Sumritpradit P, Singhatas P, Thampongsa T, Jenjitranant P, Wongwaisayawan S, Saksobhavivat N, Kaewlai R. Usefulness and outcome of whole-body computed tomography (pan-scan) in trauma patients: A prospective study. Ann Med Surg (Lond). 2022 Mar 28;76:103506. [CrossRef]
- Yoong S, Kothari R, Brooks A. Assessment of sensitivity of whole body CT for major trauma. Eur J Trauma Emerg Surg. 2019; 45(3): 489-492. [CrossRef]
- Singh N, Hardcastle TC. Selective non-operative management of gunshot wounds to the abdomen: A Collective Review. Int Emerg Nurs 2015, 23(1): 22-31. [CrossRef]
- Keijzers GB, Giannakopoulos GF, Del Mar C, Bakker FC, Geeraedts LM Jr. The effect of tertiary surveys on missed injuries in trauma: a systematic review. Scand J Trauma Resusc Emerg Med. 2012; 20: 77. 3. Jones J, Murphy A, Kusel K. Whole-body CT (protocol). Radiopeadia.org. 15 May 2010. [CrossRef]
- Hardcastle TC. Missed Injury: Decreasing Morbidity and Mortality. A literature review. S Afr J Surg. 2011; 49: 199 – 201.
- Mayet M, Hardcastle TC, Muckart DJJ. Intra-abdominal injury identified by Computed Tomographic Angiography in haemodynamically stable polytrauma patients with injury both above the thoracic and below the pelvic diaphragm. S Afr J Surg, 2019; 57(1): 49-53. http://doi.org/10.17159/2078-5151/2019/v57n1a2715.
- Sierink JC, Treskes K, Edwards MJ, Beuker BJ, den Hartog D, Hohmann J, Dijkgraaf MG, Luitse JS, Beenen LF, Hollmann MW, Goslings JC; REACT-2 study group. Immediate total-body CT scanning versus conventional imaging and selective CT scanning in patients with severe trauma (REACT-2): a randomised controlled trial. Lancet. 2016; 388(10045): 673-683. [CrossRef]
- Murphy SP, Hawthorne N, Haase D, Chiku C, Wen J, Rodriguez RM. Low Yield of Clinically Significant Injury With Head-To-Pelvis Computed Tomography in Blunt Trauma Evaluation. J Emerg Med. 2017; 53(6): 865-870. [CrossRef]
- Gordic S, Alkadhi H, Hodel S, Whole-body CT-based imaging algorithm for multiple trauma patients: radiation dose and time to diagnosis. Br J Radiol. 2015 Mar;88(1047). [CrossRef]
- Cao, CF., Ma, KL., Shan, H. et al. CT Scans and Cancer Risks: A Systematic Review and Dose-response Meta-analysis. BMC Cancer 22, 1238 (2022). [CrossRef]
- Ordoñez CA, Parra MW, Holguín A, Whole-body computed tomography is safe, effective and efficient in the severely injured hemodynamically unstable trauma patient. Colomb Med (Cali). 2020; 51(4): e4054362. [CrossRef]
- Aycock RD, Westafer LM, Boxen JL, Majlesi N, Schoenfeld EM, Bannuru RR. Acute Kidney Injury After Computed Tomography: A Meta-analysis. Ann Emerg Med. 2018; 71(1): 44-53.e4. [CrossRef]
- Hinson JS, Ehmann MR, Fine DM, Fishman EK, Toerper MF, Rothman RE, Klein EY. Risk of Acute Kidney Injury After Intravenous Contrast Media Administration. Ann Emerg Med. 2017; 69(5): 577-586.e4. [CrossRef]
- Ehmann MR, Mitchell J, Levin S, Smith A, Menez S, Hinson JS, Klein EY. Renal outcomes following intravenous contrast administration in patients with acute kidney injury: a multi-site retrospective propensity-adjusted analysis. Intensive Care Med. 2023 Feb;49(2):205-215. [CrossRef]
- Goto Y, Koyama K, Katayama S, Tonai K, Shima J, Koinuma T, Nunomiya S. Influence of contrast media on renal function and outcomes in patients with sepsis-associated acute kidney injury: a propensity-matched cohort study. Crit Care. 2019; 23(1): 249. [CrossRef]
- Parag P, Hardcastle TC. Interpretation of emergency CT scans in polytrauma: trauma surgeon vs radiologist. Afr J Emerg Med 2020, 10: 90-94. [CrossRef]
- Parag P, Hardcastle TC. Shortage of Radiologists in Low to Middle Income Countries in the Interpretation of CT scans in Trauma. Bangl J Med Sci 2022; 21(03 July): 489-491. [CrossRef]
- Adams A, Shah N, Stephenson R. An approach to accurate computed tomography imaging interpretation in penetrating neck trauma. Acta Radiol Open. 2020 ; 9(6): 2058460120938742. [CrossRef]
- Ryan B. Fransman, Faris K. Azar, William Mallon, The “No zone” Approach to penetrating Neck Trauma. American college of Surgeon, 24 Feb 2021.
- Madsen AS, Bruce JL, Oosthuizen GV. Correlation between the level of the external wound and the internal injury in penetrating neck injury does not favour an initial zonal management approach. BJS Open. 2020 Aug;4(4):704-713. [CrossRef]
- Maritz, JPB; Bagadia, A; Lubbe, JA. Can computed tomographic angiography accurately exclude digestive tract injury after penetrating cervical trauma? S Afr J surg. 2020, 58(4): 92-198. http://doi.org/10.17159/2078-5151/2020/v58n4a3159.
- Conradie WJ, Gebremariam FA. Can computed tomography esophagography reliably diagnose traumatic penetrating upper digestive tract injuries? Clin Imaging 2015; 39(6): 1039-1045. [CrossRef]
- Parida PK, Kalaiarasi R, Alexander A. Management of Laryngotracheal Trauma: A Five-Year Single Institution Experience. Iran J Otorhinolaryngol. 2018; 30(100): 283-290.
- Eissa L., Mehanna AM. Biphasic CT imaging of deep neck infections (DNIs): how does dual injection mode help in differentiation between types of collections? Egypt J Otolaryngol 2020; 36: 40. [CrossRef]
- Yonetsu K, Izumi M, Nakamura T. Deep facial infections of odontogenic origin: CT assessment of pathways of space involvement. AJNR Am J Neuroradiol 1998; 19: 123–128.
- Cutaia, G., Messina, M., Rubino, S. et al. Caustic ingestion: CT findings of esophageal injuries and thoracic complications. Emerg Radiol 2021; 28: 845–856. [CrossRef]
- Muckart DJJ, Hardcastle TC, Skinner DL. Pneumomediastinum and Pneumopericardium Following Blunt Thoracic Trauma: Much Ado About Nothing? Eur J Trauma and Emerg Surg, 2019, 45: 927-931. [CrossRef]
- Mason AC, Mirvis SE, Templeton PA. Imaging of acute tracheobronchial injury: Review of literature. Emergency Radiology, 1994; 1: 250-260. [CrossRef]
- Awais M, Qamar S, Shafqat G. Accuracy of CT chest without oral contrast for ruling out esophageal perforation using fluoroscopic esophagography as reference standard: retrospective study. Eur J Trauma Emerg Surg, 2019; 45: 517-525. [CrossRef]
- Strumwasser A, Chong V, Chu E, Victorino GP. Thoracic computed tomography is an effective screening modality in patients with penetrating injuries to the chest. Injury. 2016; 47(9): 2000-2005. [CrossRef]
- Chou YP, Kuo LC, Soo KM, Tarng YW, Chiang HI, Huang FD, Lin HL. The role of repairing lung lacerations during video-assisted thoracoscopic surgery evacuations for retained haemothorax caused by blunt chest trauma. Eur J Cardiothorac Surg. 2014; 46(1): 107-111. [CrossRef]
- Velmahos GC, Demetriades D, Chan L, Tatevossian R, Cornwell EE, Yassa N, Murray JA, Asensio JA, Berne TV. Predicting the need for thoracoscopic evacuation of residual traumatic hemothorax: chest radiograph is insufficient. J Trauma. 1999; 46(1): 65-70. [CrossRef]
- Scaglione M, Pinto A, Romano L. CT features of descending necrotizing mediastinitis – a pictorial essay. Emerg Radiol, 2007; 14: 77-81. [CrossRef]
- Guan X, Laing X, Wang F, Qian W, Zhang W. A new classification of descending necrotizing mediastinitis and surgical strategies. Ann Transl Med 2021; 9(4): 356. [CrossRef]
- Exarhos DN, Malagari K, Tsatalou EG, Acute mediastinitis: spectrum of computed tomography findings. Eur Radiol. 2005 Aug;15(8): 1569-1574. [CrossRef]
- Meyer DM, Thal ER, Weigelt JA, Redman HC. The role of abdominal CT in the evaluation of stab wounds to the back. J Trauma1989; 29(9): 1226-1228; discussion 1228-1230. [CrossRef]
- Mayet M, Hardcastle TC, Muckart DJ. Benign portal venous gas after blunt abdominal trauma. Injury Extra 2011; 42: 189-191. [CrossRef]
- Navsaria P, Nicol A, Krige J, Edu S, Chowdhury S. Selective nonoperative management of liver gunshot injuries. Eur J Trauma Emerg Surg. 2019; 45(2): 323-328. [CrossRef]
- Chmielewski GW, Nicholas JM, Dulchavsky SA, Diebel LN. Nonoperative management of gunshot wounds of the abdomen. Am. Surg.1995 Aug;61(8). PMID:7618803.
- Morell-Hofert D, Florian Primavesi F, Fodor M. Validation of the revised 2018 AAST-OIS classification and the CT severity index for prediction of operative management and survival in patients with blunt spleen and liver injuries. Eur Radiol. 2020; 30(12) :6570-6581. [CrossRef]
- Shanmuganathan K, Mirvis SE, Chiu WC, Killeen KL, Scalea TM. Triple-contrast helical CT in penetrating torso trauma: a prospective study to determine peritoneal violation and the need for laparotomy. AJR Am J Roentgenol. 2001 Dec;177(6):1247-56. [CrossRef]
- Mahummad Q, Sarah A, Mahmoud HA. Use of Multi-detector computed tomography by the emergency physicians in patients presenting with acute abdomen. A Retrospective Observational study in a large tertiary center. Trauma Emerg Care 6. [CrossRef]
- Sartelli M, Chichom-Mefire A, Labricciosa FM, Hardcastle T, Abu-Zidan FM, Adesunkanmi AK, Ansaloni L, Bala M, Balogh ZJ, Beltrán MA, et al. The management of intra-abdominal infections from a global perspective: 2017 WSES guidelines for management of intra-abdominal infections. World J Emerg Surg. 2017; 12: 29. [CrossRef]
- Sartelli M; Coccolini F; Kluger Y; Agastra E; Abu-Zidan FM; Abbas AES; Ansaloni L; Adesunkanmi AK; Atanasov B; Augustin G; et al. WSES/GAIS/SIS-E/WSIS/AAST Global Clinical Pathways for Patients with Intra-Abdominal Infections. World J Emerg Surg, 2021; 16(1):49. [CrossRef]
- Aschoff AJ, Stuber G, Becker BW, Hoffmann MH, Schmitz BL, Schelzig H, Jaeckle T. Evaluation of acute mesenteric ischemia: accuracy of biphasic mesenteric multi-detector CT angiography. Abdom Imaging. 2009 May-Jun; 34(3): 345-357. [CrossRef]
Figure 1.
CT axial slice showing grade 3-4 AAST liver injury after motor vehicle collision.
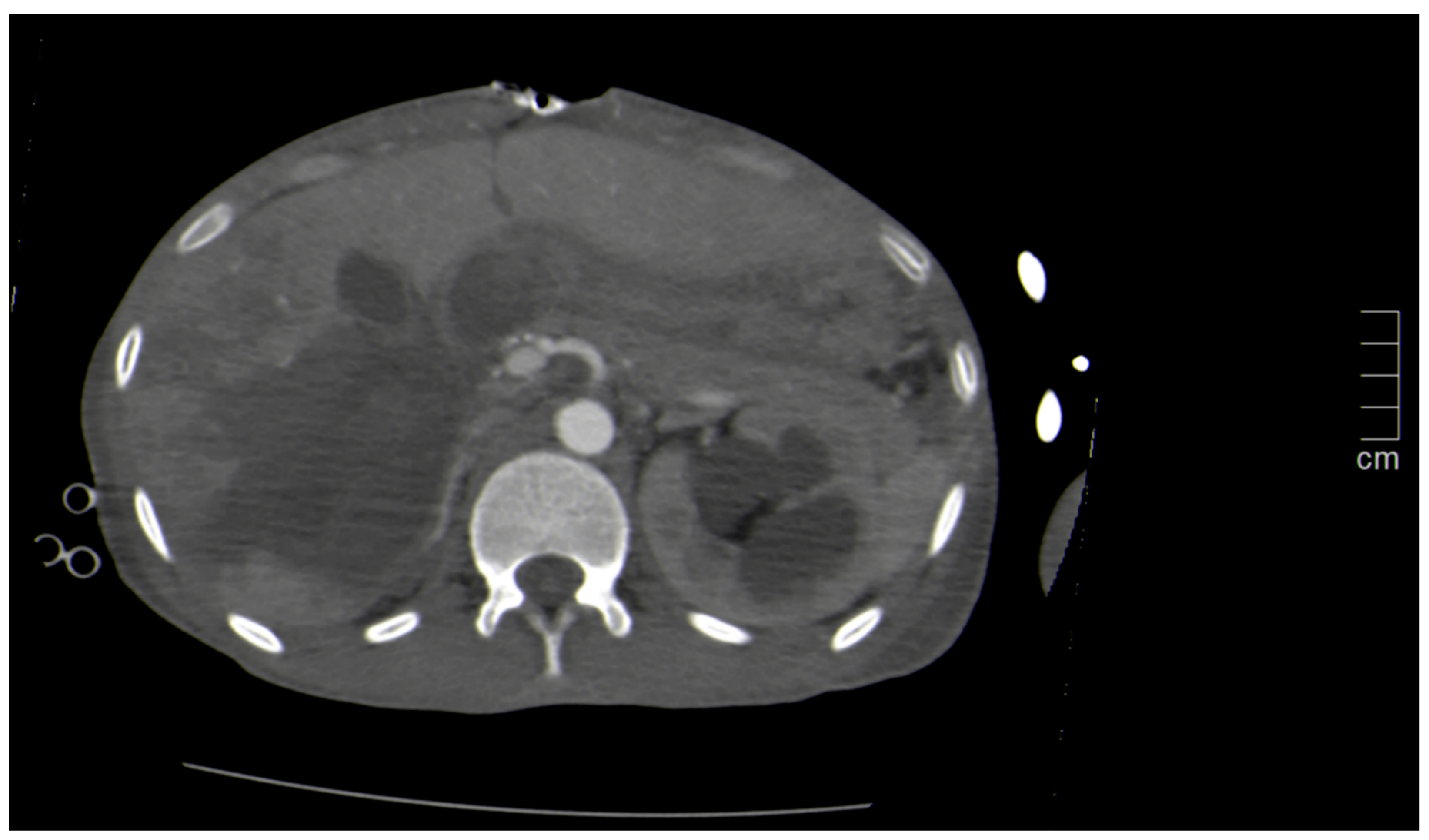
Figure 2.
The red marker shows the tracheal laceration after a stab wound.

Figure 3.
Three-dimensional reconstruction “VRT” images of a chest showing extensive rib fractures in a patient who would benefit from rib-plating.
Figure 3.
Three-dimensional reconstruction “VRT” images of a chest showing extensive rib fractures in a patient who would benefit from rib-plating.
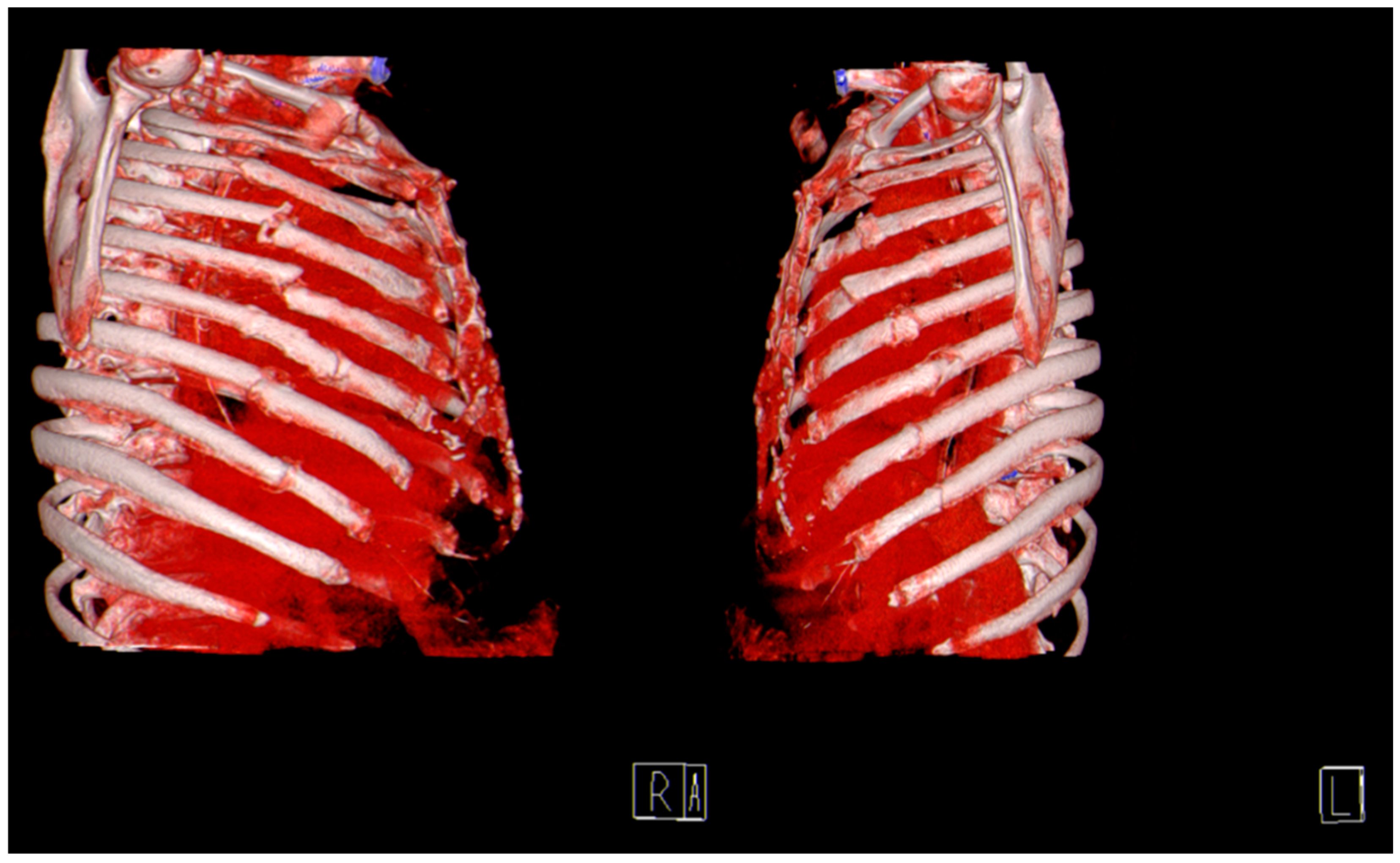
Figure 4.
CT Chest coronal view demonstrating bronchial injury with lung collapse on the right lower lobe.
Figure 4.
CT Chest coronal view demonstrating bronchial injury with lung collapse on the right lower lobe.
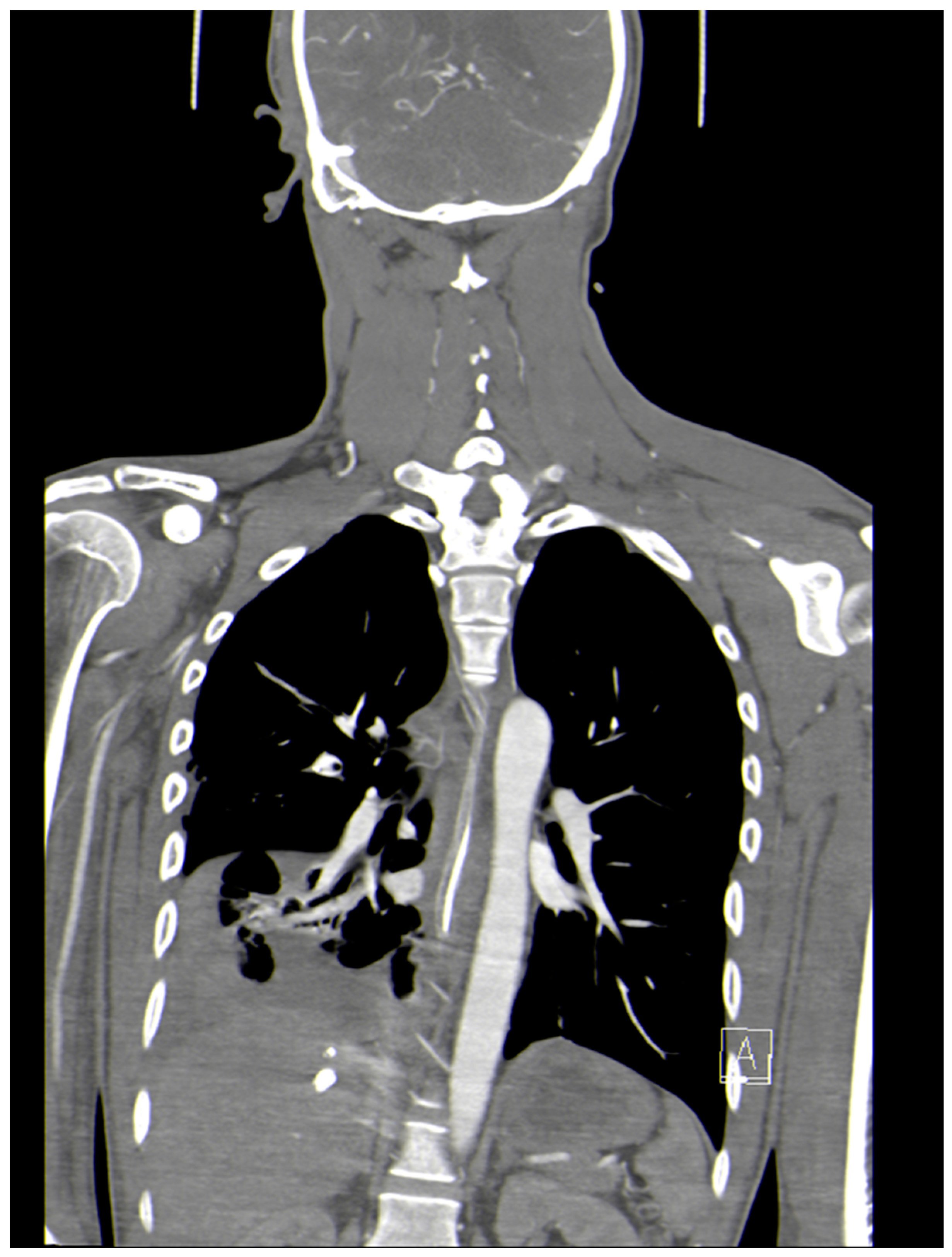
Figure 5.
Bullet tract to the right liver lobe with no other injuries identified on contrasted CT-abdomen. Non-operative management was successful.
Figure 5.
Bullet tract to the right liver lobe with no other injuries identified on contrasted CT-abdomen. Non-operative management was successful.
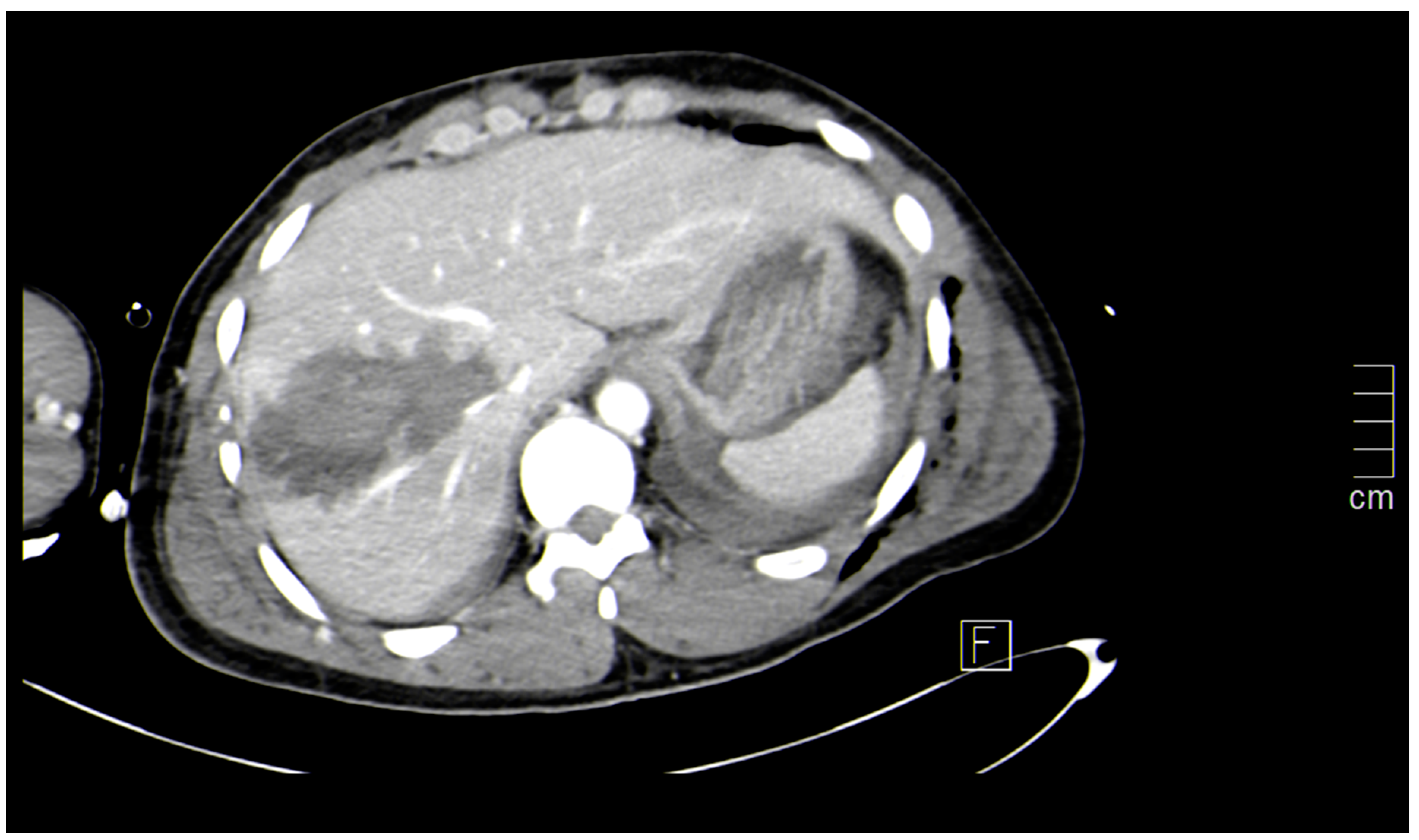

Table 1.
Indications for Pan CT in potential polytrauma.
Indications will vary from institution-to-institution but indications by mechanism include:
|
Table 2.
Surgical and non-surgical causes of acute abdominal pain.
| Surgical causes acute abdomen | Medical causes of Acute Abdomen |
|---|---|
| 1. Acute Gastritis | 1. Acute myocardial infarction |
| 2. Acute Cholecystitis | 2. Diffuse gastritis |
| 3. Acute Appendicitis | 3. Uremic gastritis |
| 4. Acute Pancreatitis | 4. Pneumonia |
| 5. Perforated Peptic ulcer | 5. Pulmonary embolus |
| 6. Pelvic Inflammatory disease | 6. Oesophagitis |
| 7. Urinary tract stones | 7. Pyeloniphritis |
| 8. Testicular torsion | 8. Nephrolithiasis |
| 9. Abdominal aortic aneurysm | 9. Cystitis |
| 10. Acute gynecology pathology such as infections, ovarian torsion, fibroid uterus & ectopic pregnancy. | 10. Acute urinary retention. |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



