Submitted:
10 March 2023
Posted:
13 March 2023
You are already at the latest version
Abstract
Heart failure (HF) diagnosis, phenotyping, prognosis, and treatment decisions are all based on the left ventricular ejection fraction (EF). Heart failure with mid-range EF (HFmrEF) is a third EF category for heart failure with an EF between 40 and 49 percent. Comparatively, heart failure with preserved EF or reduced EF has been largely unexplored. 10–25% of patients with HF have HFmrEF. Although HFmrEF has an intermediate clinical profile, it is more similar to HF with reduced EF, particularly because these patients have a high incidence of ischaemic heart disease. Heart failure with preserved EF has a lower risk of cardiovascular events than heart failure with reduced EF, which is milder. HFmrEF and HF with preserved EF patients have a similar or higher risk of non-cardiovascular adverse events than patients with HF with reduced EF. There is still a great deal of mystery surrounding HFmrEF. The purpose of this review is to describe the major pathophysiology of HFmrEF and its similarities and differences with the other two types of EF. It is the purpose of this paper to present a comprehensive overview of the currently available evidence in support of the pathophysiology of patients with HFmrEF. Further investigation of the pathophysiology, treatment, and prognosis of this condition will be needed in the future in order to better understand it.
Keywords:
heart failure
; ejection fraction
; left ventricle
; systolic dysfunction
; diastolic dysfunction
Background
Heart failure (HF) is becoming a global pandemic, and its prevalence is increasing rapidly. An ageing population and improved survival rates after myocardial infarctions are a few of the factors contributing to the growing prevalence of HF [1,2,3,4], as well as improved treatments for patients suffering from the condition. Due to this, there has been an increase in the number of hospitalizations and costs associated with heart failure [5,6], with HF costs reaching US$30.7 billion in 2012, of which more than two-thirds are directly related to medical costs, and projections suggest that by 2030, these costs will have increased by 127% [7]. While effective therapies are available for patients suffering from heart failure, the prognosis of such patients remains poor [8]. According to various population-wide registries, the average 1-year mortality rate in patients with heart failure is 10 to 35%, and it is significantly higher in the case of individuals who have advanced HF [9,10,11,12].
In HF diagnosis, characterization, prognosis, patient triage, and treatment selection, the left ventricular ejection fraction (EF) is generally measured by echocardiography. Using advanced multivariable analytics (such as machine learning and phenotyping methods) and other parameters for survival calibration and discrimination has shown better accuracy than EF alone [13]. However, without a doubt, EF remains one of the most important parameters for defining HF disease and for determining eligibility to participate in clinical trials for HF. There might be some relevance in the data described in this Review for clinicians and for clinical trial lists until better measurements than the EF are available that meet all of the needs for HF characterization [6,14,15,16].
A condition known as Heart Failure with Reduced EF (HFrEF) is characterized by a reduced EF under 40% and there are effective therapies available for the treatment of patients with this condition. It has long been understood that the term HF with preserved EF (HFpEF) is used to describe patients who present with HF symptoms as well as a preserved EF, a value which is typically defined as >50% or ≥50%. Currently, there have been no clinical trials that have demonstrated a clear benefit from therapy for patients with these conditions [17]. In the 2016 European Society of Cardiology guidelines, there was an introduction of a new HF type called heart failure with mid-range ejection fraction (HFmrEF), defined as an HF with an EF between 40 and 49% (Figure 1) and designed to facilitate research in this EF range that is less well investigated than HFrEF and HFpEF [6].
Epidemiology
There is a wide range of estimates regarding the proportion of HFmrEF in the overall HF population, ranging from 10 to 25% [18,19,20,21,22,23,24]. It was found that the incidence rate of HFmrEF in a large community-based longitudinal cohort free of HF and followed for more than 10 years was 6.7 cases per 10,000 person-years, which compares to 26.9 and 34.9 cases per 10,000 person-years in HFpEF and HFrEF, respectively [22]. Across a range of EFs, there was no real difference in the predictors of incident HF other than a few exceptions [22]. As shown in the European HF LT Registry (ESC-HF-LT) in which 24% of the cohort had prevalent HFmrEF, and in the Swedish HF Registry (SwedeHF) where 21% of the cohort had prevalent HFmrEF [20,21]; both of these registries had rates of prevalent HFmrEF ranging from 33% to 49%. Asian, Australian, and American registries reported slightly lower rates in their respective registries [18,19,23]. Last but not least, in the world of RCTs, specifically within the CHARM population, 17% of individuals were found to have HFmrEF [25].
Clinical Characteristics of HFmrEF
There was a debate about which was the most appropriate matching for the newborn category as a consequence of the introduction of HFmrEF into the spectrum of HF phenotypes, and it became an essential question. Although it might seem obvious to define HFmrEF as being the intermediate phenotype, this approach has not been supported by the available evidence, which in fact highlights the difficulties in setting HFmrEF in a precise scenario [26]. In terms of clinical characteristics, it has been suggested that HFmrEF is closer to HFpEF than they are to HFPEF in previous studies [27,28].
According to the Organized Program for Initiating Lifesaving Treatment in Hospitalized Patients with Heart Failure (OPTIMIZE-HF) study, patients who are borderline with EF have features that are similar to those found in the HFpEF population, in particular when it comes to their age, the presence of systemic hypertension, and the presence of atrial arrhythmias. However, they have intermediate characteristics regarding gender and ischemic causes [27].
It was also found that age, arterial blood pressure, atrial fibrillation, diabetes, chronic obstructive pulmonary disease (COPD), and chronic obstructive pulmonary disease (ADHERE), in the Acute Decompensated Heart Failure Registry (ADHERE), which extended the borderline EF limit to 55%, were comparable to HFpEF, while again gender and ischemic etiology were intermediate [28].
A study published by Get With The GuidelinesHeart Failure (GWTG-HF) Registry recently reported that borderline EF had characteristics which were more similar to those of high-risk EF [29], however, this trend changed in studies published later, showing that HFmrEF had more characteristics similar to those of high-risk EF [20,21].
This study provided a comprehensive assessment of the characteristics of the HF population in Europe based on the ESC-HF-LT study. Many of the characteristics of HFmrEF are similar to those of HFrEF in that the patient is younger, male, ischemic in origin, and has a lower prevalence of atrial fibrillation. In comparison to the other phenotypes, patients with HFmrEF had a lower degree of comorbidity, were less likely to receive diuretics, and were less likely to be symptomatic than those with HFmrEF. A possible explanation for HFmrEF is that it is associated with a milder stage of HFrEF, or rather that it is an early stage of HFrEF that has recovered [20,30].
One thousand and three hundred and twenty-two patients with HFmrEF were recruited through the CHARM program, and the most common characteristics of these patients with HFmrEF were, in general, similar to those of patients with HFrEF, including their age, systolic blood pressure, prevalence of females, history of myocardial infarction and atrial fibrillation [25].
There were more than 9,000 patients in the SwedeHF Registry with HFmrEF whose systemic blood pressure and the prevalence of atrial fibrillation were more similar to that of patients with HFpEF, but many other factors such as age, chronic kidney disease, diabetes mellitus, and ischemic etiology were more similar to those found in HFrEF [21].
HFmrEF showed a higher proportion of females than HFpEF, but was somewhat similar to HFrEF when it came to gender distribution between males and females [31].
Ischemia and Heart Failure
When HFmrEF is seen as a mild manifestation of HFrEF, the underlying ischemic etiology plays an important role in how it is interpreted. Ischemic heart disease has been shown to be a common occurrence in people with HFrEF, and HFmrEF has also been found to have a similar prevalence [19,24,32].
The crude prevalence of ischemic heart disease, as well as the adjusted prevalence, appears to be comparable between the two phenotypes, and HFmrEF patients were exposed to a risk of new ischemic cardiac events similar to that of HFrEF, but significantly higher than that of HFpEF [33].
Pathophysiology of HFmrEF
In accordance with the findings of recent studies, the pathophysiology of HFrEF and HFpEF is distinct from one another [34]. In general, patients with HFrEF are characterized by severe systolic dysfunction, and those with HFpEF by severe diastolic dysfunction. However, there may be some degree of overlap between the two conditions. There was a modest bimodal distribution of LVEF among patients hospitalized for HF in the OPTIMIZE-HF study [27] as well as in other studies [35], which suggests that there are two distinct disease processes associated with HF. However, there is no definitive understanding of HFmrEF's underlying pathophysiology, just as there is for HFpEF. The guidelines of the European Society of Cardiology (ESC) suggest that patients with HFmrEF probably have mild systolic as well as diastolic dysfunction [6]. One of the most important questions that must be asked is whether HFmrEF is itself a clinical syndrome or if patients with HFmrEF are in some way in transition between HFrEF and HFpEF when they have HFmrEF.
In contrast to those with HFrEF and HFpEF, those with HFmrEF seem to be experiencing HF etiology less frequently than those with HFrEF and HFpEF. There is evidence to show that CAD contributes to HF in a smaller percentage of HFrEF patients than in HFpEF patients, but they are closer to HFpEF patients in terms of the rate at which CAD contributes to HF. It is noteworthy, however, that CAD was the primary cause of heart failure in 56.5% of patients in the HFmrEF study, and 27.8%, 8.3%, and 7.4% of the HF etiologies in this group were caused by hypertensive heart disease (HHD), dilated cardiomyopathy (DCM), and valvular heart disease, respectively [24]. There was a similar distribution of HHD between patients with HFrEF and those with HFpEF; however, patients with HFrEF had a higher percentage of HHD contributing to their condition. This study evaluated longitudinal transitions between the HF groups in an ambulatory Japanese population as part of the CHART-2 study [19], which also evaluated the prevalence of HF among different groups of patients. As a result of three years of follow-up, it was found that 45% of patients with HFmrEF underwent a dynamic transition to HFpEF as well as 21% who underwent HFrEF, while only 34% remained as HFmrEF [19]. In contrast, for the HFpEF and HFrEF groups, clinical classifications in their original HF groups retained 88% and 53%, respectively, indicating that these two clinical syndromes are distinct from each other and should be considered separately. Moreover, the term HFmrEF may also be used to encompass patients who are in the process of transitioning from one to the other. This transition or lack thereof may be influenced by CAD, and cardiac comorbidity. Compared to those with HFrEF, patients with HFpEF decline their LVEF more rapidly when CAD is present than those with HFrEF, while CAD does not significantly decrease their LVEF when CAD is present in those with HFrEF [36].
Systolic dysfunction and diastolic dysfunction have traditionally been attributed to HFrEF and HFpEF, respectively. The overlap between the two conditions is becoming increasingly apparent as research progresses. We have a limited understanding of HFpEF, despite the existence of numerous pharmacologic interventions that have shown effectiveness in patients with HFrEF [37,38,39,40,41,42,43,44].
In similar fashion, HFmrEF's pathophysiology is poorly understood. The results of this study were further investigated using echocardiographic data obtained from the TIME-CHF project [24]. As HFpEF progressed to HFmrEF, this cohort's left ventricular cavity dimension progressively increased, while HFrEF exhibited gradual decreases in systolic function parameters. Every group had elevated filling pressures at the left ventricle in all of these studies. A significant amount of hypertrophy of the left ventricle was also observed in all three groups. Compared to the HFrEF group, there was a greater degree of eccentric hypertrophy in the HFpEF group, and a lesser degree of focal remodeling in the HFmrEF group. There were no significant differences between the two groups when it came to diastolic dysfunction [24].
Based on NT-proBNP as a biomarker, the levels of this enzyme are elevated in patients with HFpEF to a similar extent, and the levels in these patients are much higher than those with HFpEF, from a biomarker perspective [24]. The serum creatinine and troponin T levels for patients with HFmrEF and HFrEF are similar when compared to those with HFpEF, with HFmrEF and HFrEF both showing higher levels when compared to HFpEF [24]. On the other hand, patients with HFmrEF tend to show higher levels of cystatin C and lower levels of hemoglobin than do patients with HFpEF [24].
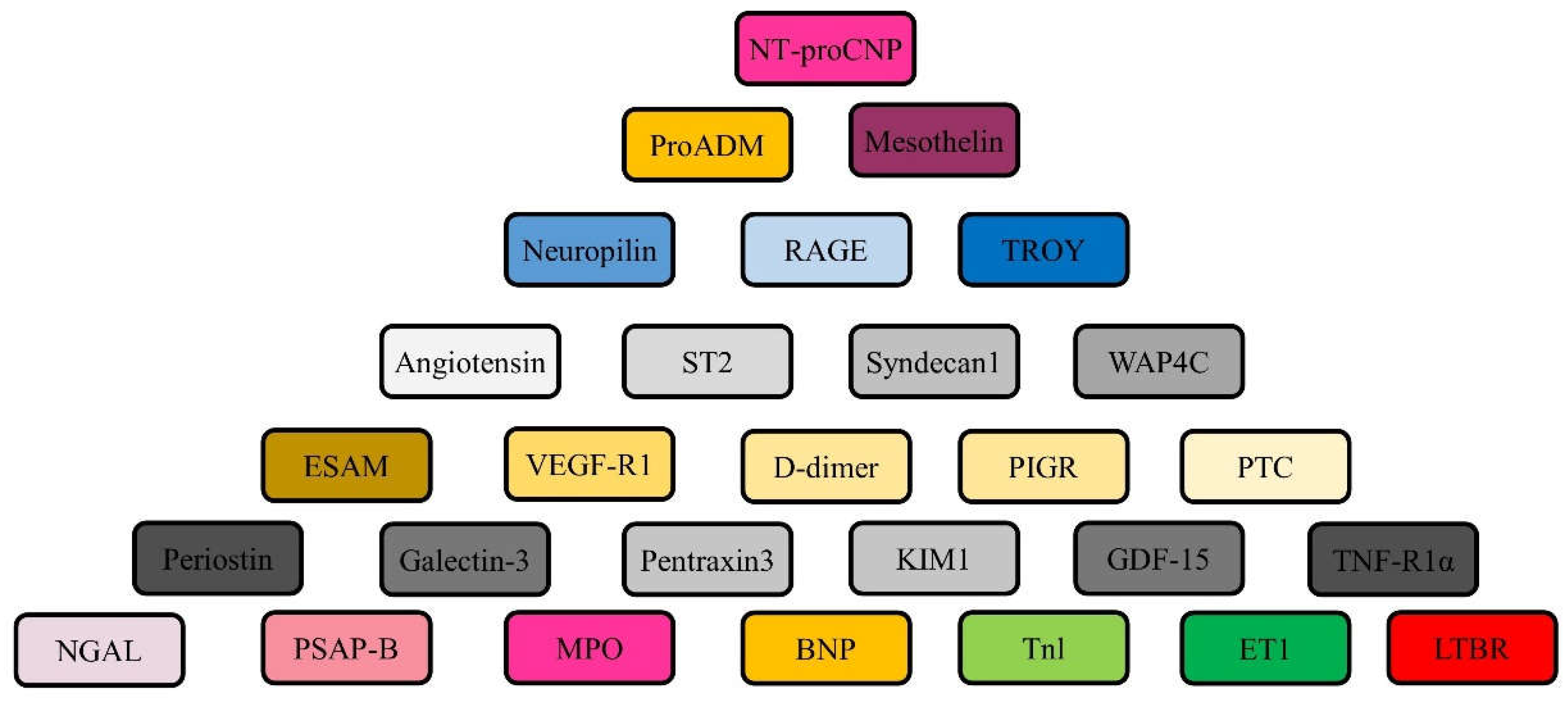
In a study conducted by Tromp et al [45], many biomarkers were evaluated across a wide range of ejection fractions, all of which were associated with pathophysiological domains (Figure 2). HFrEF patients were found to have a profile that appears predominantly to be related to cardiac stretch, while HFpEF patients were found to have cardiac inflammation, while HFmrEF patients were found to have both cardiac stretch and inflammation [45].
A cohort of patients with HFmrEF was found to have cardiac troponin values that were in the middle of the range of cardiac troponin values for patients with HFrEF and HFpEF in the SHOP (Singapore Heart Failure Outcomes and Phenotypes) cohort [46].
HFpEF and HFmrEF patients showed similar neuroendocrine profiles in terms of signaling, with higher neurohormone levels in the HFrEF group, including NTproBNP, renin to aldosterone ratio, aldosterone, and norepinephrine than in the HFpEF group [47].
According to Pugliese et al., exercise intolerance was predominantly the result of peripheral factors (arterial-venous oxygen content difference) in patients with HFpEF and HFmrEF, whereas intolerance was a result of low stroke volume increases among patients with HFrEF [48].
Conclusive Statement
HFmrEF has now been defined in a more comprehensive and comprehensive manner according to the professional guidelines, which has helped us to fully understand the heterogeneous pathophysiology profile and similarly poor outcomes of these patients. It is a comparison between this group and the other HF groups. It may be beneficial to begin the treatment of neurohormonal blockade early if this is otherwise indicated, in addition to close clinical monitoring and aggressive management of comorbidities, including coronary artery disease.
Author Contributions
All authors participated actively in all parts of this study, including research designing, analyzing data, and manuscript writing. All authors have read and agreed to the published version of the manuscript.
Funding
None.
Consent for publication
Not applicable.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Data Availability Statement
Not applicable.
Ethics approval
Not applicable.
Consent to participate
Not applicable.
Acknowledgments
None.
Conflicts of Interest
None.
References
- Conrad, N. et al. (2018) Temporal trends and patterns in heart failure incidence: a population-based study of 4 million individuals. Lancet 391, 572–580. [CrossRef]
- Jernberg, T. et al. (2011) Association between adoption of evidence-based treatment and survival for patients with ST-elevation myocardial infarction. JAMA 305, 1677–1684. [CrossRef]
- van Riet, E. E. et al. (2016) Epidemiology of heart failure: the prevalence of heart failure and ventricular dysfunction in older adults over time. A systematic review. Eur. J. Heart Fail. 18, 242–252. [CrossRef]
- Taylor, C. J. et al. (2019) Trends in survival after a diagnosis of heart failure in the United Kingdom 2000–2017: population based cohort study. BMJ 364, l223. [CrossRef]
- Yancy, C. W. et al. (2017) 2017 ACC/AHA/HFSA focused update of the 2013 ACCF/AHA Guideline for the Management of Heart Failure: a report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines and the Heart Failure Society of America. Circulation 136, e137–e161. [CrossRef]
- Ponikowski, P. et al. (2016) 2016 ESC Guidelines for the diagnosis and treatment of acute and chronic heart failure: the Task Force for the diagnosis and treatment of acute and chronic heart failure of the European Society of Cardiology (ESC) developed with the special contribution of the Heart Failure Association (HFA) of the ESC. Eur. Heart J. 37, 2129–2200. [CrossRef]
- Virani, S. S. et al. (2021) Heart disease and stroke statistics — 2021 update: a report from the American Heart Association. Circulation 143, e254–e743. [CrossRef]
- Thorvaldsen, T. et al. (2016) Use of evidence-based therapy and survival in heart failure in Sweden 2003–2012. Eur. J. Heart Fail. 18, 503–511. [CrossRef]
- Ambrosy, A. P. et al. (2014) The global health and economic burden of hospitalizations for heart failure: lessons learned from hospitalized heart failure registries. J. Am. Coll. Cardiol. 63, 1123–1133. [CrossRef]
- Lund, L. H., et al. (2012) Association between use of renin–angiotensin system antagonists and mortality in patients with heart failure and preserved ejection fraction. JAMA 308, 2108–2117. [CrossRef]
- Lund, L. H. et al. (2017) Association between enrolment in a heart failure quality registry and subsequent mortality — a nationwide cohort study. Eur. J. Heart Fail. 19,1107–1116. [CrossRef]
- Crespo-Leiro, M. G. et al. (2018) Advanced heart failure: a position statement of the Heart Failure Association of the European Society of Cardiology. Eur. J. Heart Fail. 20, 1505–1535. [CrossRef]
- Ahmad, T. et al. (2018) Machine learning methods improve prognostication, identify clinically distinct phenotypes, and detect heterogeneity in response to therapy in a large cohort of heart failure patients. J. Am. Heart Assoc. 7, e008081. [CrossRef]
- Lund, L. H. (2016) Heart failure with “mid-range” ejection fraction — new opportunities. J. Card. Fail. 22, 769–771. [CrossRef]
- Lund, L. H., et al. (2018) Is ejection fraction in heart failure a limitation or an opportunity? Eur. J. Heart Fail. 20, 431–432. [CrossRef]
- Marwick, T. H. (2018) Ejection fraction pros and cons: JACC state-of-the-art review. J. Am. Coll. Cardiol. 72, 2360–2379. [CrossRef]
- Bhatt, D. L. et al. (2020) Sotagliflozin in patients with diabetes and recent worsening heart Failure. N. Engl. J. Med. 384, 117–128. [CrossRef]
- Kapoor JR, et al. (2016) Precipitating Clinical Factors, Heart Failure Characterization, and Outcomes in Patients Hospitalized With Heart Failure With Reduced, Borderline, and Preserved Ejection Fraction. JACC Heart Fail 4, 464–72. [CrossRef]
- Tsuji K, et al. (2017) Characterization of heart failure patients with mid-range left ventricular ejection fraction-a report from the CHART-2 Study. Eur J Heart Fail 19, 1258–69. [CrossRef]
- Chioncel O, et al. (2017) Epidemiology and one-year outcomes in patients with chronic heart failure and preserved, mid-range and reduced ejection fraction: an analysis of the ESC Heart Failure Long-Term Registry. Eur J Heart Fail 19, 1574–85. [CrossRef]
- Koh AS, et al. (2017) A comprehensive population-based characterization of heart failure with mid-range ejection fraction. Eur J Heart Fail 19, 1624–34. [CrossRef]
- Bhambhani V, et al. (2018) Predictors and outcomes of heart failure with mid-range ejection fraction. Eur J Heart Fail 20, 651–9. [CrossRef]
- Lam CSP, et al. (2018) Mortality associated with heart failure with preserved vs. reduced ejection fraction in a prospective international multi-ethnic cohort study. Eur Heart J 39, 1770–80. [CrossRef]
- Rickenbacher P, et al. (2017) Heart failure with mid-range ejection fraction: a distinct clinical entity? Insights from the Trial of Intensified versus standard Medical therapy in Elderly patients with Congestive Heart Failure (TIME-CHF). Eur J Heart Fail 19, 1586–96. [CrossRef]
- Lund LH, et al. (2018) Heart failure with mid-range ejection fraction in CHARM: characteristics, outcomes and effect of candesartan across the entire ejection fraction spectrum. Eur J Heart Fail 20, 1230–9. [CrossRef]
- Lund LH. (2018) Heart Failure with Mid-range Ejection Fraction: Lessons from CHARM. Card Fail Rev 4, 70–2. [CrossRef]
- Fonarow GC, et al. (2007) Characteristics, treatments, and outcomes of patients with preserved systolic function hospitalized for heart failure: a report from the OPTIMIZE-HF Registry. J Am Coll Cardiol 50, 768–77. [CrossRef]
- Sweitzer NK, et al. (2008) Comparison of clinical features and outcomes of patients hospitalized with heart failure and normal ejection fraction (>or =55%) versus those with mildly reduced (40% to 55%) and moderately to severely reduced (<40%) fractions. Am J Cardiol 101, 1151–6. [CrossRef]
- Shah KS, et al. (2017) Heart Failure With Preserved, Borderline, and Reduced Ejection Fraction: 5-Year Outcomes. J Am Coll Cardiol 70, 2476–86. [CrossRef]
- Kalogeropoulos AP, et al. (2016) Characteristics and Outcomes of Adult Outpatients With Heart Failure and Improved or Recovered Ejection Fraction. JAMA Cardiol 1, 510–8. [CrossRef]
- Stolfo D, et al. (2019) Sex-Based Differences in Heart Failure Across the Ejection Fraction Spectrum: Phenotyping, and Prognostic and Therapeutic Implications. JACC Heart Fail 7, 505–15. [CrossRef]
- Ibrahim NE, et al. (2019) Heart failure with mid-range ejection fraction: characterization of patients from the PINNACLE Registry(R). ESC Heart Fail 6, 784–92. [CrossRef]
- Vedin O, et al. (2017) Significance of Ischemic Heart Disease in Patients With Heart Failure and Preserved, Midrange, and Reduced Ejection Fraction: A Nationwide Cohort Study. Circ Heart Fail 10. [CrossRef]
- Lee DS, et al. (2009) Relation of disease pathogenesis and risk factors to heart failure with preserved or reduced ejection fraction: insights from the Framingham Heart Study of the National Heart, Lung, and Blood Institute. Circulation 119, 3070–7. [CrossRef]
- Borlaug BA,et al. (2011) Diastolic and systolic heart failure are distinct phenotypes within the heart failure spectrum. Circulation 123, 2006–13. [CrossRef]
- Dunlay et al. (2012) Longitudinal changes in ejection fraction in heart failure patients with preserved and reduced ejection fraction. Circ. Heart Fail. 5, 720–726. [CrossRef]
- MERIT-HF Study Group. (1999) Effect of metoprolol CR/XL in chronic heart failure: Metoprolol CR/XL randomised intervention trial in congestive heart failure (MERIT-HF). Lancet. 353, 2001–7.
- Poole-Wilson PA, et al. (2003) Comparison of carvedilol and metoprolol on clinical outcomes in patients with chronic heart failure in the Carvedilol or Metoprolol European trial (COMET): randomized controlled trial. Lancet. 362, 7–13. [CrossRef]
- Investigators S, et al. (1991) Effect of enalapril on survival in patients with reduced left ventricular ejection fractions and congestive heart failure. N Engl J Med. 325, 293–302. [CrossRef]
- Consensus Trial Study Group. (1987) Effects of enalapril on mortality in severe congestive heart failure. Results of the Cooperative North Scandinavian Enalapril Survival Study (CONSENSUS). N Engl J Med. 316, 1429–35. [CrossRef]
- Granger CB, et al. (2003) Effects of candesartan in patients with chronic heart failure and reduced left-ventricular systolic function intolerant to angiotensin-converting-enzyme inhibitors: the CHARMalternative trial. Lancet. 362, 772–6. [CrossRef]
- Zannad F, et al. (2011) Eplerenone in patients with systolic heart failure and mild symptoms. N Engl J Med. 364, 11–21. [CrossRef]
- McMurray JJ, et al. (2014) Angiotensin-neprilysin inhibition versus enalapril in heart failure. N Engl J Med. 371, 993–1004. [CrossRef]
- Swedberg K, et al. (2010) Ivabradine and outcomes in chronic heart failure (SHIFT): a randomised placebo-controlled study. Lancet. 376, 875–85. [CrossRef]
- Tromp J, et al. (2017) Biomarker profiles of acute heart failure patients with a mid-range ejection fraction. JACC Heart Fail. 5, 507–17. [CrossRef]
- Gohar A, et al. (2017) The prognostic value of highly sensitive cardiac troponin assays for adverse events in men and women with stable heart failure and a preserved vs. reduced ejection fraction. Eur J Heart Fail. 19, 1638–47. [CrossRef]
- Vergaro G, et al. (2019) Sympathetic and renin-angiotensin-aldosterone system activation in heart failure with preserved, mid-range and reduced ejection fraction. Int J Cardiol. 296, 91–7. [CrossRef]
- Pugliese NR, et al. (2019) Value of combined cardiopulmonary and echocardiography stress test to characterize the haemodynamic and metabolic responses of patients with heart failure and mid-range ejection fraction. Eur Heart J Cardiovasc Imaging. 20, 828–36. [CrossRef]
Figure 1.
Heart Failure and Ejection fraction.
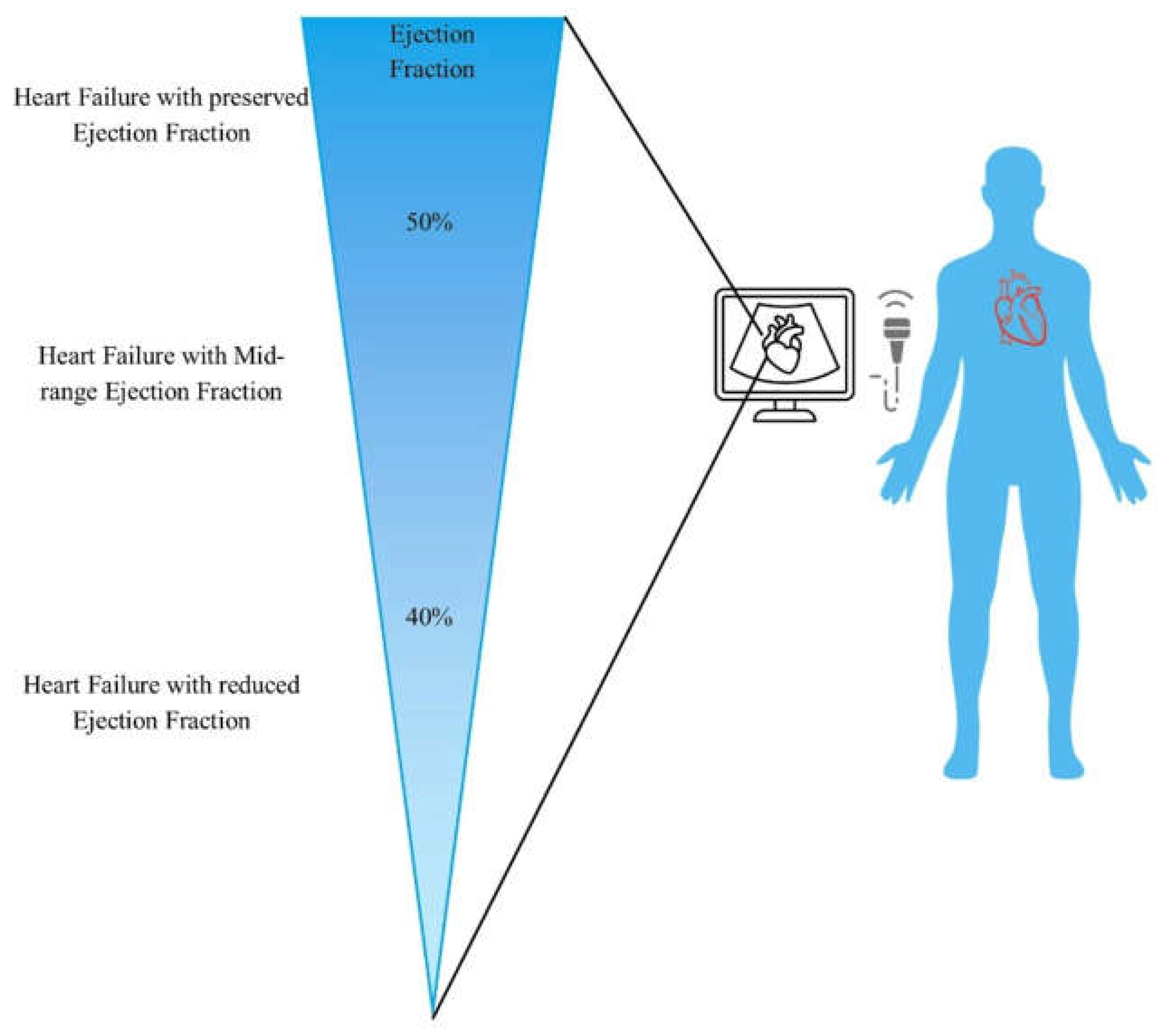
Figure 2.
Biomarkers of HFmrEF. BNP: brain natriuretic peptide; ESAM: endothelial cell-selective adhesion molecule; ET: endothelin; GDF: growth differentiation factor; NGAL: neutrophil gelatinase-associated lipocalin; NT-proCNP: N-terminal pro-C-type natriuretic peptide; PCT: procalcitonin; PIGR: polymeric immunoglobulin receptor; ProADM: pro-adrenomedulin; PSAP-B: prosaposin B; RAGE: receptor for advanced glycation end product; TNF-R1α: tumor necrosis factor-receptor 1 α; VEGF-R1: vascular endothelial growth factor-receptor 1; MPO: myeloperoxidase; LTBR: lymphotoxin beta receptor; TROY: Tumor necrosis factor receptor superfamily member 19; KIM: kidney injury molecule; WAP4C: WAP 4-disulphide core domain protein HE.
Figure 2.
Biomarkers of HFmrEF. BNP: brain natriuretic peptide; ESAM: endothelial cell-selective adhesion molecule; ET: endothelin; GDF: growth differentiation factor; NGAL: neutrophil gelatinase-associated lipocalin; NT-proCNP: N-terminal pro-C-type natriuretic peptide; PCT: procalcitonin; PIGR: polymeric immunoglobulin receptor; ProADM: pro-adrenomedulin; PSAP-B: prosaposin B; RAGE: receptor for advanced glycation end product; TNF-R1α: tumor necrosis factor-receptor 1 α; VEGF-R1: vascular endothelial growth factor-receptor 1; MPO: myeloperoxidase; LTBR: lymphotoxin beta receptor; TROY: Tumor necrosis factor receptor superfamily member 19; KIM: kidney injury molecule; WAP4C: WAP 4-disulphide core domain protein HE.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



