Submitted:
12 March 2023
Posted:
13 March 2023
You are already at the latest version
Abstract
Geriatric decisional capacity assessment is a complex medico-legal activity that evaluates normal subjects involved in specific civil matter like wealth transfer, access to treatment or voluntary hospitalization. Our objective was to evaluate how geriatric extrajudicial capacity exams impacted a general psychiatric unit over a decade. We also assessed the value of a surrogate biomarker (neutrophils to lymphocyte ratio) as a screening factor in the capacity assessment process. 72 cases were assessed in one psychiatric unit over a decade (2009-2018). As population was fast ageing, the total number of capacity exams per year doubled in time. None of the subjects had an active diagnostic of severe cognitive impairment or active psychiatric disease. The percentage of subjects receiving an “absence of capacity” conclusion remained constant over time (approx. 20% of all cases). 81% of the subjects within this subgroup had a clinical diagnostic of mild cognitive impairment compared to 46% in the “presence of capacity” subgroup (p<0.001). The surrogate biomarker neutrophils to lymphocyte ratio was significantly higher in the “absence of capacity” subgroup, mainly related to a cognitive impairment diagnostic. The ratio has to be validated by larger studies before to be included in the capacity assessment process as an early screening tool.
Keywords:
Geriatric decisional capacity assessment
; wealth transfer
; mild cognitive impairment
; mild depression
; neutrophils to lymphocytes ratio
; chronic inflammation
1. Introduction
For the first time in history, humans are expected to live significantly more than 60 years [1]. The “senior” age group is the fastest growing segment of the western population [2]. This rapid ageing process [3] is generating new health, economic and legal challenges [4]. As elderlies own more than one-third of existing world wealth [5], seniors are often asked to make complex wealth transactions with results that may generate social, ethical and legal debate [6]. The ageing process alone [7] or in association with various chronic medical conditions may reduce dramatically individual decisional capacity [8,9]. Diminished decisional capacity may increase the risk of financial exploitation, abuse and fraud [10]. Economic loss is notoriously associated with development of depression [11], functional disability and increased dependency in geriatric population [12], aggravating the initial incapacity in an ascending spiral [13]. The every-day reality proved that there is a clear need for increasing seniors’ protection, mainly in relation with transfer of wealth. Because the number of medical experts that are qualified and willing to be involved in medico-legal assessments is low, examining a high number of normal geriatric subjects can be a difficult task [14].
Most of the high-income countries [15] forecasted the need for a consistent assessment of decisional capacity in seniors [16]. Clear medico-legal circumstances that require a capacity assessment in geriatric subjects were identified outside judicial matter (wealth transfer, access to medical research, to treatment, testamentary and advanced life directives) [17]. The expert roles in the capacity assessment process were clearly defined based on ethically accepted boundaries (independent roles for expert, for medical witness and for treating physician) [18]. There is a clear methodology for performing a capacity assessment [19]. There is still place for improvement: scientific precision [20] and portability of results [21] are difficult to obtain as existing psychometric tests are widely influenced by language, culture and judicial systems differences. Heterogenicity of experts’ qualification in various countries [22,23] is another parameter that is under scrutiny.
The situation is far more complex in countries with economy under development [24]. In many East European countries, a sudden but serious geriatrization process was observed recently [25]. This trend was associated with important changes in legal dogma paradigms [26].
In Romania, a country considered to have the second old population in Europe (more than 121 seniors / 100 adults) [27]), seniors’ protection falls under two categories of legal provisions. The first path implies a formal, court-ordered, civil medico-legal assessment. Civil assessments are requested based on articles 998-1003 of the Romanian Civil Code and the 271/2004 medico-legal act, mainly when tort liability is considered (traffic, work, professional liability) or for establishing legal competency. The legal situation of psychiatric patients in relation with different aspects of civil matter is regulated by the mental health act (first emitted in 487/2002, republished in 2004 and refined in 2012 as law 129) which was recently completed by new provisions. Geriatric psychiatric cases are assessed by a formal medico-legal neuropsychiatric committee that will decide about subject’s capacity or discernment [28]. The second path is the extrajudicial assessment. It can be requested by a state notary or directly at the subject’s personal request (or representative as tutor or curator) when the geriatric subject is exposed to well specified financial or medical circumstances. It has to be performed by a psychiatrist, in a psychiatric medical unit. The second path was recently developed (Health Minister ordinance 488/2015 completed with ordinance 3423/2022). The reason for the new legal provisions was a dramatical increase in number of seniors, considered to be mentally “sound” or with mild cognitive impairment, observed in the last two decades [29]. Both categories are exposed to exploitation and fraud when performing complex transfer of wealth transactions or advanced life directives. In essence, the recent ordinances “recommend” that state notaries to ask for a mental health certificate (often named a capacity certificate - CC) for all subjects involved in wealth transactions when there is a doubt concerning their decisional capacity or when the subject is simply “old” [30]. State Notaries, in order to avoid any possible litigation, prefer to ask for a CC in all cases involving subjects older than 65. The new legal provisions increased the burden of complex assessments posed on psychiatry hospitals and specialists’ time and budgets. Beside time and costs, also raised the ethical dilemma of the conflicting role of the physician involved in medico-legal assessments (legal assessor, medical witness or treating physician).
Capacity is a medico-legal concept that is decision-specific, time-specific and situation-specific in every instance. There is a legal presumption of capacity in all adult subjects unless and until the presumption is legally denied [31]. Capacity may fluctuate: a perfectly capable subject may become incapable to make a specific decision under various physio-pathologic conditions or external undue influence [32]. Competency is the juridic reflection of capacity [33]. The exact definition of competency may differ under various juridical dogma, but it is generally accepted that competency cannot fluctuate (it is present or not). Any decision concerning (in)competency will have serious clinical, legal and ethical dimensions involving all aspects of human living (wealth and estate management, financial and testamentary decision access to treatment, medical research, advanced dispositions, sexual consent, voting and driving) [34]. Individuals that do not have capacity will be certainly evaluated for competency and will have to follow a formal medico-legal assessment procedure (court-ordered). As the capacity certificate can be the foundation for any competency decision, the initial psychiatric evaluation has to be as complete as possible. Under these juridic constrains, capacity assessment, a medical task that is ubiquitous in geriatric population [35], is far more complex than it was expected initially [36].
Decisional capacity is an important philosophical and legal principle that governs many aspects of the modern life [37]. There are many published clinical guidelines that may steer the capacity assessment procedure [38] but the overall acceptance of the process is far from being unanimous. The need for better structured capacity assessment instruments is a common observation coming from practice [39]. Most of the existing psychometric tools that are used for capacity testing are based on four-ability model promulgated by Appelbaum and Grisso [40] in the 1980’s and are derivatives of the MacArthur Competence Assessment Tools [41]. Capacity tests do not precisely evaluate cognitive abilities and will provide conclusions that have only limited, medico-legal, value [42,43]. The prevalence of incapacity in healthy older adults is estimated at 3% of population, a percentage that may increase to 26% in inpatient subjects with chronic conditions – a circumstance often seen in aged subjects [44]. Incapacity is rarely discovered outside of the rigid settings of the medico-legal assessment as both clinicians or relatives overestimate patients’ mental abilities [45]. Physicians are reluctant to perform capacity assessments in geriatric patients mentioning the absence of reliable instruments and trained staff for tests administration [46].
Cognitive and mood tests are often needed to support conclusions concerning one’s individual “capacity”. Well-normed psychometric instruments are designed to reveal and quantify early cognitive or mood impairments that may influence the decision-making process. A routine use of these tests in the clinical context is problematic as these have to be administered under controlled conditions and have to be translated and then validated in various populations. Cultural and personal values may influence one’s decisional capacity. Under these values, some perfectly valid decisions can look to others “unwise” or “strange” [47]. Tests often require trained personnel for administration and interpretation [48], staff that is not usually available in a clinical non-academic setting. Unstructured tests exist. These tests are able to avoid the risk of testing depersonalization (“capacitometer” testing trap [49]) but are hard to use and results are not validated, portable and reproducible. The Mini Mental Status Exam (MMSE) [50], the most commonly used cognitive test in daily clinical activity that was translated and validated in many languages and countries, is notoriously not adequate to detect early cognitive changes [51]. Even if a clinical condition like memory loss (that can significantly reduce the decisional capacity) may appear years in advance of the full neurodegenerative disease [52,53], unequivocal detection is difficult even for trained professionals [54] as subjects adopt compensatory behaviors [55]. Simple-to-use instruments (like measuring arithmetic calculation abilities) can detect moderate or advanced Alzheimer Disease [56] but do not correlate well with incipient neurocognitive changes [57]. Financial capacity tests are capable to detect early stages of cognitive impairment but are under the same constrains as the other semi-structured psychometrics [58].
Geriatric CC evaluation is a complex process that may generate serious legal inferences for both the subject and assessor. A well documented conclusion comes with a high investigative cost (four to eight hours of professional service plus the cost of the tests use and supplementary administrative fees). The costs are often not covered by the established exam fee (which is fixed by law). Little is known about the total burden that CC may pose on the activity of a busy psychiatric clinic that works with geriatric cases on a daily basis.
The main objective of our research was to evaluate how routine CC exams may impact a general psychiatric clinic that tested the decisional capacity of nondemented geriatric seniors in relation to non-judicial matter. We were also interested to evaluate how a simple to use, low-cost surrogate biomarker (neutrophils to lymphocyte ratio) may support an early diagnosis of mild cognitive or mood impairment and may assist the capacity assessment, improving precision and reducing costs.
2. Materials and Methods
All CC exams performed in one general psychiatric clinic over a period of 10 years (2009-2018) were audited. Evaluations were done in response to a state notary or a personal request and were made by trained psychiatrists accustomed to work with geriatric population. None of the evaluations was court-ordered. Socio-demographic information (age, sex, marital status, ethnicity) were sampled in all cases. All subjects dwelled in retirement homes or lived independently in an urban area. None of the cases had a clinical diagnostic of dementia (or any form of active psychiatric disorder).
In contrast with the formal medico-legal psychiatric assessment, there is no recommended methodology for evaluating capacity of “normal” geriatric subjects in extra-judicial circumstance [59,60]. We followed Lai and Karlawish guidelines [61] (Figure 1), translating and adapting the every-day decisional capacity questionnaire for the needs of a non-English speaking population with a medium level of education. The semi-structured capacity interview tested the capacity of a subject to understand a specific information, to retain it, to evaluate its pertinence, to reason between existing alternatives and finally to express a decisional choice. The cognitive status was tested using Mini Mental Status Exam – MMSE [62] in all cases. The battery of cognitive tests was completed with Cognitive Dementia Rating-Sum of Boxes - CDR-SB [63], Montreal Cognitive Assessment (MOCA [64]) and the Instrumental Activities of Daily Living (IADL [65]). An additional diagnostic of minor mood disorder was evaluated using geriatric depression scale GDS [66]). Except MMSE, all tests were translated but were not fully validated for Romanian population [67]. A general clinical evaluation and a blood lab work completed each case.
Ethics. Our retrospective, noninterventional research plan was approved by the psychiatry unit ethic committee (5117/2021) (two clinics: “Sfântul Pantelimon” psychiatric hospital Braila and “Elisabeta Doamna” psychiatric hospital Galați). Written informed consent for study participation was waived as the audit was entirely non-interventional, retrospective and subjects were not identifiable (in respect to national legislation and the institutional requirements). Data was audited in accordance with the principles of Declaration of Helsinki.
Statistics. Results were analyzed using PSPP (GNU project, free software, 2015). Only basic descriptive statistic (mean and standard deviation) is presented here. As the number of subjects was low, the only statistic performed was a simple comparison of means (T test) with a p value set at 0.05.
Terminology and definitions. In this paper we used the term “mild cognitive impairment” (MCI) to define the gray zone of cognitive disfunction existing between normality and dementia [68]. Our definition for an “aged” society considers the fraction of the population aged 65+ years exceeding 8–10% [69]. Cut-off scores for normal cognition were: CDR 0.5<, MMSE>27, MOCA>27. IADL score was considered 3 (“independent”) for each activity of daily living that was discussed with each subject. For GDS, the minor depression cut-off score was set between >2 to 6<. In the national Code of Procedure, there is a clear difference between the term “assessment” (judicial, performed based on a court order request) and “evaluation” (extra-judicial, usually performed on a person’s request). For simplification and considering that we audited evaluations done only on extrajudicial requests, in this paper both terms are used equivalently. Terms “civil” and “administrative” matter are also used equally, in relation to transfer of wealth and to access to treatment and hospitalization.
3. Results
In a ten years interval (2009-2018), 72 CC evaluations were performed in our general psychiatry clinic. Socio-demographic data of the whole cohort is presented in Table 1.
The yearly distribution of CCs, main characteristics of the requests and the evaluation conclusions are presented in Table 2. The most important legal context was a contract for sales.
Overall, 62 evaluations were requested by a state notary. Subjects’ mean age was 74.9±6 years. 50% of subjects were females. 80% of them were of Romanian ethnicity and in 54% of cases subjects lived autonomously. The most prominent legal context was CoS (78%). In 14% of cases, another form of wealth transfer was involved (testament or donation). One case was evaluated in response to a health request (one female, 78.4 years old, advanced life directive). Only 54% of subjects received a diagnostic of MCI.
10 evaluations were performed at the subject’s request (or families). The mean age of these subjects was 75.28±6.6 years, 40% of them being females and 90% being of Romanian ethnicity. Wealth transfer was the most notable legal context (70%). In 3 cases the exam was performed in relation with access to treatment. 50% of subjects received a diagnostic of MCI.
A conclusion of “Absence of capacity” was established in 16 cases (Table 3). The mean age of subjects was 77±6.1 years, 56% were females, all subjects were of Romanian ethnicity. The average level of education was 13.5±3.22 years. 55% of them were living independently. 87% of the subjects were married. A contract of sales was mentioned in 57% of cases. In 37% of the cases another form of wealth transfer was mentioned. Only one case was investigated in relation with voluntary hospitalization. 81% of these cases received a clinical diagnostic of MCI. In 3 cases, a diagnostic of depression (GDS score of 5-6) was established. In the subgroup with “preserved” decisional capacity (56 subjects) a MCI diagnostic was established in 47% of cases and mild depression in 62% of cases.
4. Discussion
An accurate estimation of the decisional capacity in “normal” elderly subjects became a subject of salient importance, with multiple legal, financial, and health implications [70]. A clear procedural assessment path must be followed when decisional capacity is tested in response to a court of law request. A low number of psychiatric experts are trained and accept to have medico-legal duties and most of them are involved in the judicial path. Access to this path is a challenge for geriatric subjects without a mental health issue. But these vast majority of “mentally sound” seniors are involved in complex financial transactions and are at risk for financial exploitation and/or abuse. To protect them against financial exploitation and abuse, new law endorsements were added to the mental health act. It is now possible for a geriatric subject to have a capacity evaluation outside of the medico-legal context when 1) the assessment is requested by a state notary or directly by the subject in regard to very precise circumstances and 2) the assessment is performed by a trained psychiatrist, in a designated psychiatric unit. The new “recommendations” generated a sudden increase in the number of requests for extrajudicial capacity assessments but the final burden posed on psychiatric clinics was not clearly recorded by any of the parts.
Assessing capacity is a complex medical task that may induce legal consequences for both the subject and the examiner. The absence of a uniform assessment methodology, the possibility of a brief or fluctuating clouding of capacity by a medical or psychiatric condition, the inability to understand or weight information or a personal understanding of facts based on socio-cultural values, all are circumstances that increase the exam’s complexity. Minimal impairment of cognition or/and minor depression (defined as depression that do not meet the major depressive disorder diagnostic criteria [71]) are clinical conditions often encountered in aged subjects. Both can affect decisional capacity and have to be carefully diagnosed and then weighted in a relation with a specific decision. The exam’s conclusion has to be objective and precise as it may be a foundation for a further, court ordered, medico-legal assessments.
The main objective of our research was to evaluate how routine CC exams impacted a general psychiatric unit that works with a geriatric homogenous population. A secondary objective was to evaluate how minor cognitive impairment and depressive disorder may influence decisional capacity in seniors involved in civil cases (non-court ordered). Finally, we evaluated how a chronic inflammatory biomarker (neutrophiles to lymphocytes ratio), already researched in relation to reduced cognition and geriatric mood disorders, can be used as a low-cost screening tool in the capacity assessment process.
Over a decade (2009-2018), 72 cases of geriatric CC evaluations were performed in one general psychiatry unit (two clinics) that is accustomed to work with geriatric subjects. None of the cases had a major neuro-psychiatric diagnostic at the moment of the exam. None of the team members involved in capacity evaluations were involved in judicial (court-ordered) medico-legal assessments. The number of capacity assessments constantly increased over time interval. The point of change was 2015, when a Health Ministry ordinance completed the existing Mental Health Act. The number of subjects without capacity remained low (approx. 20% each year). A similar percentage was already reported in various geriatric populations of different ethnicities [72,73].
Overall, 62 evaluations (86%) were requested by a state notary. The mean age of subjects was 74.9±6 years. 50% of them were females and 80% of them were of Romanian ethnicity and in 54% of cases subjects lived independently. The most prominent legal context was CoS (78%). In 14% of cases, another form of wealth transfer was involved (testament or donation). One case was evaluated in response to a health request (one female, 78.4 years old, advanced life directive). Only 54% of subjects received a diagnostic of MCI. 10 evaluations were performed at the subject’s request (or families). The mean age of these subjects was 75.28±6.6 years, 40% of them being females and 90% being of Romanian ethnicity. Wealth transfer was the most notable legal context (70%). In 3 cases the exam was performed in relation with access to treatment. 50% of subjects received a diagnostic of MCI.
An assessment conclusion of “Absence of Capacity” was established in 16 cases (Table 3). The mean age of subjects was 77±6.1 years, 56% were females, all subjects were of Romanian ethnicity. The average level of education was 13.5±3.22 years. 55% of them were living independently. 87% of the subjects were married. The most dominant legal context was wealth transfer in 15 cases A contract of sales was mentioned in 57% of cases. In 37% of the cases another form of wealth transfer was mentioned. Only one case was investigated in relation with (in)voluntary hospitalization. 81% of these cases received a clinical diagnostic of MCI. Three cases received a “cognitive normal” diagnostic (18%) but a diagnostic of borderline severe depression was established (GDS score of 6 in two cases - one male, 79.4, and one female 74.4 years old and GDS score of 5 - female, 82 years old). All three cases had important associated organic pathology.
In the subgroup with “preserved” decisional capacity (56 subjects, 74.6±5.8 years old), in 44 cases the assessment was performed in relation with a contract of sales, in four cases with a testament and in other four cases with a donation (in 90% of cases, it was requested by a notary). Four cases were tested in relation to advanced health directives or voluntary hospitalization. MCI diagnostic was established in 47% of cases and mild depression in 62% of cases. Only one case (female, 70.2 years old) had a GDS score of 6.
Our audit confirms that a capacity exam will have to use a large panel of cognitive impairment/mood disorder psychometric investigations and that MMSE is simply not enough to detect early cognitive impairments. Increasing diagnostic precision will come with a serious burden of time and financial costs that are often not covered by the assessment fees. Based on this observation we evaluated how a simple to use surrogate biomarker can be used as a screening tool for an early detection chronic inflammation, often associated with cognitive and mood disorders in geriatric subjects.
The use of biomarkers for increasing diagnostic precision gained a constant research attention in medico-legal biopathology [74]. Between many evaluated biomarkers, the Neutrophil to Lymphocyte Ratio proved to be a handy, reliable, low cost and high reproducible chronic inflammation biomarker [75] with high sensitivity and low specificity. It is already used in the diagnostic of various chronic diseases [76]. In geriatric neuro-psychiatry it was associated mainly with cognitive decline prognosis [77]. A value of NLR between 2.3 to 2.5 was reported in subjects with various degrees of cognitive impairment [78]. Published data also described an association with both minor [79] and major depression in geriatric subjects [80]. As the marker shows the influence of chronic inflammatory stress on both geriatric cognition and mood [81], we postulated that it may be useful as a low-cost, early screening tool in the capacity assessment process. In our study NLR showed a significant difference when the two MCI subgroups were compared (p<0.0001) (Table 4). For mood impairment, comparing ratios was not meaningful as the number of subjects was very small. NLR may help for early identification of subjects with a serious chronic inflammatory condition that may affect decisional capacity. Subjects may benefit from a full cognitive and depression battery of tests. The ratio may lower assessment costs but will maintain exam’s precision. It may also smoothen the serious ethical dilemma that is confronting the evaluator (physician, witness or legal assessor) and will add objectivity in support to the assessment conclusions.
Study limitations. The use of a capacity assessment methodology and cognitive and mood detection tests that were not fully validated for the Romanian population are probably the most important limitations of our study. Their use was justified by the need for a precise evaluation of the subjects in the absence of procedural guidelines. Tests were considered acceptable as the capacity assessment was requested in geriatric subjects outside of the judicial context (transfer of wealth, consent to treatment, voluntary hospitalization). NLR is a surrogate biomarker that showed value in the geriatric clinical settings but is not completely validated as a formal assessment tool (scientific admissibility/reliability rule). The low number of cases that were audited in our research do not allow any causation conclusions. The retrospective, single arm design is another limitation of this study.
5. Conclusions
Rapid geriatrization of population and recently adopted legal provisions designed to protect seniors against financial fraud and exploitation generated an unpredicted increase of extra-judicial capacity certificate assessment requests. Most of the exams are demanded by state notaries in connection with a form of transfer of wealth. As these assessments are done by psychiatry specialists in psychiatry units, the burden posed on the time and budget of the clinics is considerable. We audited all decisional capacity evaluations performed in a clinical psychiatry unit accustomed to work with a homogenous, non-English speaking, geriatric population. Over a decade, 72 cases were evaluated. None of the cases had an active diagnostic of neuro-psychiatric disease. 86% of assessments were requested by a state notary as subjects were involved in a form of transfer of wealth and were over 65 years old. Even if the number of requests increased constantly in time, the percentage of subjects with decisional incapacity remained almost constant (20%). Between the 16 cases of “absence of capacity” that were found over time, 82% of them had a mild form of cognitive impairment. 3 cases were considered cognitive normal but had a high depression score and severe associated pathology. A surrogate biomarker (neutrophils to lymphocytes ratio) that was already evaluated in relation with chronic geriatric inflammation, showed promising value as a possible early screening tool for both cognitive impairment and mild depression. Further studies are needed in order to evaluate the biomarker’s utility in the medico-legal context. Clear procedural provisions and a validated decisional capacity toolkit may increase the objectivity and portability of the extra-judicial assessment and reduce the risk of legal contestation.
Supplementary Materials
All existing data was presented in the article.
Acknowledgement
The study had no funding support to report, and there is no conflict of interests to report, as well. The author thanks to Dr. Marius D Gangal (medacs.ca) for his constant involvement in the research, his scientific support and advice.
Conflicts of Interest
There is no conflict of interest to declare.
References
- World Economic and Social Survey 2007: development in an ageing world. New York: United Nations Department of Social and Economic Affairs Report No. E/2007/50/Rev.1 ST/ESA/314 http://www.un.org/en/development/desa/policy/ wess/wess_archive/2007wess.pdf,.
- Waite LJ. The Demographic Faces of the Elderly. Popul Dev Rev. 2004;30(Supplement):3-16.
- Campisi J, Kapahi P, et al., From discoveries in ageing research to therapeutics for healthy ageing. Nature. 2019 Jul;571(7764):183-192. [CrossRef]
- Christensen K, Doblhammer G, et al Ageing populations: the challenges ahead. Lancet. 2009 Oct 3;374(9696):1196–208. PMID: 19801098. [CrossRef]
- National Financial Partners Corp. Family Wealth Transfers Report [Internet]. New York: WealthX; 2016. Available from: http://www.wealthx.com/wp-content/uploads/2015/01/WealthX_NFP_FamilyWealthTransfersReport-2014.pdf.
- Edersheim J, Murray ED, Padmanabhan JL, Price BH. Protecting the Health and Finances of the Elderly With Early Cognitive Impairment. J Am Acad Psychiatry Law. 2017;45(1):81-91.
- Tannou T, Koeberlé S, Aubry R, Haffen E. How does decisional capacity evolve with normal cognitive aging: systematic review of the literature. Eur Geriatr Med. 2020;11(1):117-129. [CrossRef]
- Tangalos EG, Petersen RC. Mild Cognitive Impairment in Geriatrics. Clin Geriatr Med. 2018 Nov;34(4):563-589. [CrossRef]
- Edersheim J, Murray ED, Padmanabhan JL, Price BH. Protecting the Health and Finances of the Elderly With Early Cognitive Impairment. J Am Acad Psychiatry Law. 2017;45(1):81-91.
- Hudson RB, Goodwin J, Elder Wealth, Cognition and Abuse, 2016, Public Policies & Aging Report26, 1,2-4. [CrossRef]
- Gilhooly MM., Dalley G., et al, Financial elderly abuse through the lens of the bystander intervention model 2016, Public Policies and Aging report.
- Lock SL., Age-Friendly banking How we can help get it right before things go wrong. Public Policy and Aging Report 2016, 26(1), 18-22. [CrossRef]
- Yon Y, Mikton CR, Gassoumis ZD, et al. Elder abuse prevalence in community settings: A systematic review and meta-analysis. Lancet Glob Health, 2017; 5: e147–e156. [CrossRef]
- Walsh K, Scharf T, Keating N. Social exclusion of older persons: a scoping review and conceptual framework, Eur J Ageing. 2016;14(1):81-98. [CrossRef]
- "Doing Business 2019 Fact Sheet: OECD High-Income" (PDF). World Bank. Archived (PDF) from the original on 1 November 2018. Retrieved 31 October 2018.
- Moye J, Marson DC, Edelstein B. Assessment of capacity in an aging society. Am Psychol. 2013;68(3):158-171. [CrossRef]
- Shulman K., Hull IM, et al, Cognitive Fluctuations and the Lucid Interval in Dementia: Implications for Testamentary Capacity2015, J Am Acad Psychiatry Law 43:287–92.
- Owolabi T, Farine D, Bell D, Davis D, Knickle DA, Milne K, et al. Providing Opinion for Medico Legal Cases. SOGC Committee Opinion, 2002, (117), J Obstet Gynecol Can 2002; 24(7):590–2. [CrossRef]
- Health care Consent Act available at https://www.ontario.ca/laws/statute/96h02.
- Lander, T. & Heilbrun, K. (2009). The content and quality of forensic mental health assessment: Validation of a principles-based approach. International Journal of Forensic Mental Health, 8, 115-121. [CrossRef]
- Goldenson, J., Josefowitz, N. Remote Forensic Psychological Assessment in Civil Cases: Considerations for Experts Assessing Harms from Early Life Abuse. Psychol. Inj. and Law 14, 89–103 (2021). [CrossRef]
- Combalbert N., Andronikof A., et all Forensic mental health assessment in France: Recommendations for quality improvement 2014, International Journal of Law and Psychiatry 37 (6) 628-634 . [CrossRef]
- Hermann H, Trachsel M, Mitchell C, Biller-Andorno N., Medical decision-making capacity: knowledge, attitudes, and assessment practices of physicians in Switzerland. Swiss Med Wkly. 2014;144(w14039):1–7. [CrossRef]
- 2015; 24. WHO, World Report on Ageing and Health, 2015.
- Gavrliova N, Gavrilov L., Uhlenberg (ed.), International Handbook of Population Aging. © Springer Science+Business Media B.V. 2009. [CrossRef]
- Jean JP., Gurbanov R., Judicial systems of the Eastern European countries. CEPEJ Studies N21; Council of Europe publishing, 2015.
- Romanian 2021 census @ https://insse.ro/cms/en.
- 1995; 28. Belis Vl et al, Legal Medicine, Medical Publishing House 1995.
- https://www.alzheimer-europe.org/Policy-in-Practice2/Country-comparisons/2013-The-prevalence-of-dementia-in-Europe/Romania.
- Tataru DS, Discernământul în actele juridice, între Codul civil șiLegea nr. 487/2002 privind sănătatea mintală, @ juridice.ro/748871.
- Appelbaum PS (2007). Assessment of patients’ competence to consent to treatment. The New England Journal of Medicine, 357: 1834–40.
- Moye J, Marson DC. Assessment of decision-making capacity in older adults: an emerging area of practice and research. J Gerontol B Psychol Sci Soc Sci. 2007;62(1):P3-P11. [CrossRef]
- Shulman, K. I., Cohen, C. A. and Hull, I. (2005). Psychiatric issues in retrospective challenges of testamentary capacity. International Journal of Geriatric Psychiatry, 20, 63–69. [CrossRef]
- American Bar Association Commission on Law and Aging, & American Psychological Association. Assessment of older adults with diminished capacity: A handbook for psychologists. Washington, DC: Author; 2008.
- Demakis G. Introduction to basic issues in civil capacities. In: Demakis G, editor. Civil capacities in neuropsychology: research findings and practical applications. New York: Oxford University Press; 2012. p. 3–16.
- Marson, D. C., Cody, H. A., Ingram, K. K., Harrell, L. E. (1995). Neuropsychological predictors of competency in Alzheimer's disease using a rational reasons legal standard. Archives of Neurology, 52,955-959;. [CrossRef]
- Tannou T., Koeberle S., et al How does decisional capacity evolve with normal cognitive aging: systematic review of the literature 2019 European Geriatric Medicine (2020) 11:117–129. [CrossRef]
- Drane JF. Competency to give an informed consent. A model for making clinical assessments. JAMA. 1984;252(7):925–927. [CrossRef]
- Barstow C., Shahan B, et al Evaluating Medical Decision-Making Capacity in Practice, Am Fam Physician. 2018 Jul 1;98(1):40-46.
- Appelbaum, P. S., Grisso, T. (1988). Assessing patients' capacities to consent to treatment. New England Journal of Medicine, 319,1635-1638. [CrossRef]
- Grisso T, Appelbaum PS, Hill-Fotouhi C. The MacCAT-T: a clinical tool to assess patients’ capacities to make treatment decisions. Psychiatr Serv. 1997; 48:1415–9. [CrossRef]
- Wood et al. Decision-making capacity evaluations: the role of neuropsychological assessment from a multidisciplinary perspective BMC Geriatrics (2020) 20:535 . [CrossRef]
- Tori K., Kalligeros M., et al The process of obtaining informed consent to research in long term care facilities (LTCFs) An Observational Clinical Study Medicine 2020 99:21. [CrossRef]
- Sessums LL, Zembrzuska H, Jackson JL. Does this patient have medical decision-making capacity? JAMA. 2011; 306(4): 420-427. [CrossRef]
- Mortimer JA: Very early detection of Alzheimer neuropathologyand the role of brain reserve in modifying its clinical expression. J Geriatrc Psychiatry Neurol 18:218 –23, 2005. [CrossRef]
- Tunzi M. Can the patient decide? Evaluating patient capacity in practice. Am Fam Physician. 2001; 64(2): 299-306.
- Hope T, Slowther A, Eccles JBest interests, dementia and the Mental Capacity Act (2005) Journal of Medical Ethics 2009;35:733-738. [CrossRef]
- Gurrera RJ, Karel MJ, Azar AR, Moye J. Agreement between instruments for rating treatment decisional capacity. Am J Geriatr Psychiatry. 2007 Feb;15(2):168-73. [CrossRef]
- Kapp MB, Mossman D. Measuring decisional capacity: cautions on the construction of a “Capacimeter.”. Psychol Public Policy Law. 1996;2:73–95. [CrossRef]
- Folstein MF, Folstein SE, McHugh PR. Mini-mental state: A practical method for grading the cognitive state of patients for the clinician. Journal of Psychiatric Research. 1975; 12(3):189–198. [CrossRef]
- Phillips VL, Diwan S: The incremental effect of dementia-related problem behaviors on the time to nursing home placement in poor, frail, demented older people. 2003 J Am Geriatr Soc 51:188 –9. [CrossRef]
- Okonkwo OC, Griffith HR, Copeland JN, et al: Medical decision-making capacity in mild cognitive impairment: a 3-year longitudinal study. Neurology 71:1474–80, 2008. [CrossRef]
- Ostenmeyer B., Flores A., et al Medical Decision-Making Capacity in depression, 2016, Psychiatric Annals 46:4, . [CrossRef]
- Weiner MF, Hynan LS, Bret ME, et al: Early behavioral symptoms and course of Alzheimer’s disease. Acta Psychiatr Scand 111: 367–71, 2005. [CrossRef]
- Hotopf M. The assessment of mental capacity. Clin Med (Lond). 2005;5(6):580-584. [CrossRef]
- Martin RC, Annis SM, et al. Loss of calculation abilities in patients with mild and moderate Alzheimer disease. Arch Neurol. 2003;60(11):1585-1589. [CrossRef]
- Zamarian, Laura, et al. "Alzheimer's disease and mild cognitive impairment: effects of shifting and interference in simple arithmetic." Journal of the Neurological Sciences 263.1-2 (2007): 79-88. [CrossRef]
- Drima, E.P. Routine Use of Financial Capacity Instruments for Clinical Decisional Capacity Testing: A Scoping Review . Preprints 2022, 2022050413. [CrossRef]
- Krupchanka D, Winkler P. State of mental healthcare systems in Eastern Europe: do we really understand what is going on?. BJPsych Int. 2016;13(4):96-99. [CrossRef]
- Tătaru N, Marinov P, Douzenis A, Novotni A, Kecman B. Forensic psychiatry in some Balkan countries. Curr Opin Psychiatry. 2010 Sep;23(5):472-80. [CrossRef]
- Lai, J. M., & Karlawish, J. (2008). Assessing the Capacity to Make Everyday Decisions: A Guide for Clinicians and an Agenda for Future Research. Retrieved from https://repository.upenn.edu/neuroethics_pubs/34.
- Folstein MF, Folstein SE, McHugh PR. "Mini-mental state”. A practical method for grading the cognitive state of patients for the clinician. J Psychiatr Res. 1975; 12(3):189–98. [CrossRef]
- Morris, J. C. (1997). Clinical dementia rating: a reliable and valid diagnostic and staging measure for dementia of the Alzheimer type. Int. Psychogeriatr. 9, (Suppl. 1), 173–176. [CrossRef]
- Nasreddine ZS, Phillips NA, Bédirian V, et al. The Montreal Cognitive Assessment, MoCA: A Brief Screening Tool for Mild Cognitive Impairment. J Am Geriatr Soc. 2005; 53(4):695–9. [CrossRef]
- Oros, R; Popescu, CA et al The impact of cognitive impairment after stroke on activities of daily living 2016 International Journal of the Bioflux Society, Human and Veterinary Medicine; Cluj-Napoca Vol. 8, Iss. 1, 41-44.
- Montorio, I., & Izal, M. (1996). The Geriatric Depression Scale: A Review of Its Development and Utility. International Psychogeriatrics, 8(1), 103-112. [CrossRef]
- Ciobica, A. Padurariu, M et al General issues encountered while diagnosing mild cognitive impairment in Romanian patients: Mild cognitive impairment in Romanian patients. 2017 International Journal of Geriatric Psychiatry. 32. 116-117. 10.1002/gps.4531.
- Stokin GB, Krell-Roesch J, et al. Mild Neurocognitive Disorder: An Old Wine in a New Bottle. Harv Rev Psychiatry. 2015 Sep-Oct;23(5):368-76. [CrossRef]
- Kinsella, K. and Velkoff, V.A. (2001) An Aging World 2001. Series P95/01-1, US Census Bureau, Washington DC.
- American Bar Association Commission on Law and Aging, & American Psychological Association. Assessment of older adults with diminished capacity: A handbook for psychologists. Washington, DC: Author; 2008.
- Lyness JM, Heo M, et al. Outcomes of minor and subsyndromal depression among elderly patients in primary care settings. Ann Intern Med 2006; 144: 496–504. [CrossRef]
- Chan CY, Yong SW, et al. Audit of Mental Capacity Assessment by Primary Care Physicians Versus Consultation-liaison Psychiatrists. East Asian Arch Psychiatry. 2018 Sep;28(3):95-100.
- Raymont V, Bingley W, Buchanan A, et al. Prevalence of mental incapacity in medical inpatients and associated risk factors: cross-sectional study. Lancet 2004; 364: 1421–1427. [CrossRef]
- Califf RM. Biomarker definitions and their applications. Exp Biol Med (Maywood). 2018 Feb;243(3):213-221. [CrossRef]
- Zahorec R. Neutrophil-to-lymphocyte ratio, past, present and future perspectives. Bratisl Lek Listy. 2021;122(7):474-488. [CrossRef]
- Balta S, Demirkol S, Unlu M, Arslan Z, Celik T (2013) Neutrophil to lymphocyte ratio may be predict of mortality in all conditions Br J Cancer 3125-3126. [CrossRef]
- Schram MT, Euser SM, de Craen AJ (2007) Systemic markers of inflammation and cognitive decline in old age J Am GeriatrSoc708–716. [CrossRef]
- Kalelioglu T., Yuruyen M., The neutrophil and platelet to lymphocyte ratios in people with subjective, mild cognitive impairment and early Alzheimer’s disease, 2017, poster EV0769, 25th European Congress of Psychiatry / European Psychiatry 41S (2017) S645–S709. [CrossRef]
- Drima EP., Gangal MD., Machine Learning Prediction of Minor Depression Diagnostic Based on Specific Serologic Pro-Inflammatory Cytokines Variation in Non-Demented Geriatric Subjects (2023). [CrossRef]
- Bremmer MA, Beekman AT, et al. Inflammatory markers in late-life depression: results from a population-based study. J Affect Disord. 2008 Mar;106(3):249-55. [CrossRef]
- McIntosh RC, Lobo J., Neutrophil to lymphocyte ratio is a transdiagnostic biomarker of depression and structural and functional brain alterations in older adults, J Neuroimmunology, 365 2022. [CrossRef]
Figure 1.
Decisional capacity testing (after Lai and Karlawish) ADL-activities of daily living, IADL– instrumental activities of daily living.
Figure 1.
Decisional capacity testing (after Lai and Karlawish) ADL-activities of daily living, IADL– instrumental activities of daily living.
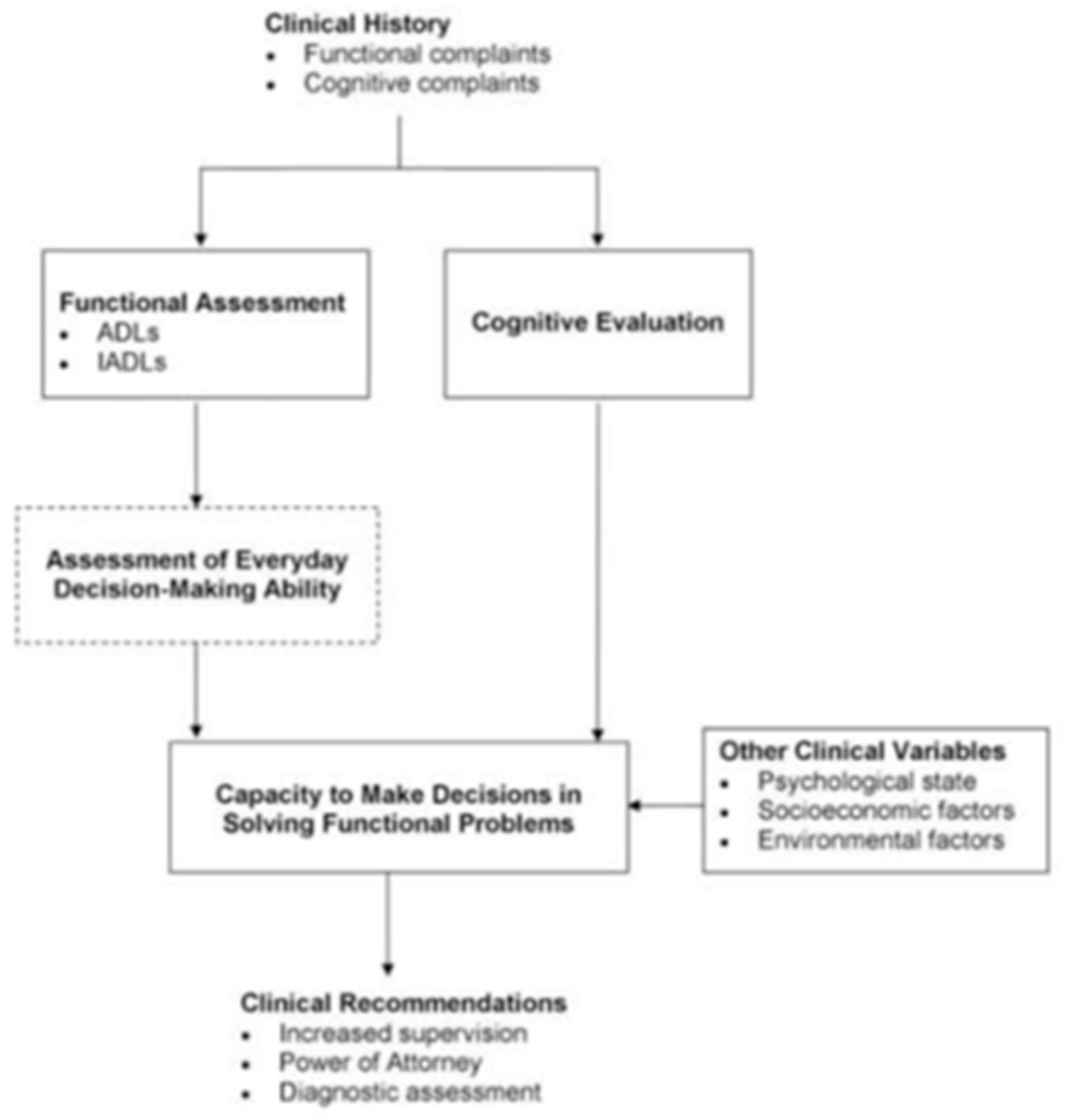

Table 1.
Socio-demographic data of all audited assessments.
| Age (years) | 75.1±6.5 |
| Sex | 51% Males |
| Education | 13±4 |
| Ethnicity | 82% Romanian |
| Marital status | 72% married |
| Dwelling | 54% autonomous living |
| Notary request | 86% |
Table 2.
Yearly distribution of CC exams and the “absence of capacity” conclusion (F=female, CoS=Contract of Sales, TC=Testamentary Capacity, Do=Donation, AT=Access to Treatment, including voluntary hospitalization).
Table 2.
Yearly distribution of CC exams and the “absence of capacity” conclusion (F=female, CoS=Contract of Sales, TC=Testamentary Capacity, Do=Donation, AT=Access to Treatment, including voluntary hospitalization).
| Year | Number of assessments | Age | Sex | Notary | Legal context | Absence of Capacity |
|---|---|---|---|---|---|---|
| 2009 | 1 | 72.1 | 100%F | 100% | 100%CoS | 0 |
| 2010 | 3 | 69.2±6 | 30%F | 100% | 100%CoS | 0 |
| 2011 | 1 | 72.6 | 100%F | 0% | 100%TC | 1 |
| 2012 | 4 | 71.5±6.3 | 50%F | 100% | 100%CoS | 2 |
| 2013 | 4 | 74.4±7.9 | 75%F | 87% | 50%CoS, 50%TC | 2 |
| 2014 | 5 | 75.3±6 | 60%F | 100% | 40%CoS, 20%TC, 20%Do, 20%AT | 2 |
| 2015 | 13 | 74.8±6.9 | 46%F | 75% | 70%CoS, 23%Do, 7%AT | 2 |
| 2016 | 12 | 73.55±4.9 | 55%F | 67% | 75%CoS, 16%TC, 8%Do | 2 |
| 2017 | 14 | 75.7±5.3 | 42%F | 100% | 100%CoS | 2 |
| 2018 | 15 | 75.7±6 | 40%F | 88% | 58%CoS, 12%TC, 12%Do, 12%AT | 3 |
Table 3.
Socio-demographic and clinical data in the subgroup with “absence of capacity” compared with subgroup with “preserved capacity” (#p<0.0001, *p=0.0001, **p<0.0001, $p<0.0001). GDS= geriatric depression score. NLR= neutrophils to lymphocytes ratio. MMSE was used in all evaluations. CDR, MOCA and IADL were gradually added but were used in all evaluations since 2015.
Table 3.
Socio-demographic and clinical data in the subgroup with “absence of capacity” compared with subgroup with “preserved capacity” (#p<0.0001, *p=0.0001, **p<0.0001, $p<0.0001). GDS= geriatric depression score. NLR= neutrophils to lymphocytes ratio. MMSE was used in all evaluations. CDR, MOCA and IADL were gradually added but were used in all evaluations since 2015.
| Absence of Capacity | Presence of capacity | |
|---|---|---|
| Number | 16 | 56 |
| Age | 76±6 | 74.6±5.8 |
| Sex | 50%F | 51%F |
| Education | 13.5±3.2 | 12.9±4.4 |
| Ethnic Romanian | 100% | 76% |
| Marital | 88% | 67% |
| Live Independently | 56% | 54% |
| Notary request | 75% | 90% |
| Legal context | 57% CoS | 78% CoS |
| CDR-SB score | 1.5±0.9(#) | 0.4±0.5(#) |
| MMSE score | 26.2±1.9 | 27.7±2.7 |
| MOCA score | 23.5±1.8 | 24.7±2.7 |
| IADL score | 7.9±2.5($) | 12.9±2($) |
| GDS | 4±1.7(*) | 1.3±1.4(*) |
| NLR | 3.8±1(**) | 2.35±1(**) |
Table 4.
Scores of main psychometric tests used in all assessments and the neutrophils to lymphocytes ratio (AC=absence of capacity, PC=presence of capacity, MCI=mild cognitive impairment, NC=normal cognition, MMSE=mini mental state, GDS=geriatric depression scale, NLR=neutro_to_lympho. ratio) (*) p<0.0001.
Table 4.
Scores of main psychometric tests used in all assessments and the neutrophils to lymphocytes ratio (AC=absence of capacity, PC=presence of capacity, MCI=mild cognitive impairment, NC=normal cognition, MMSE=mini mental state, GDS=geriatric depression scale, NLR=neutro_to_lympho. ratio) (*) p<0.0001.
| AC+NC | AC+MCI | PC+NC | PC+MCI | |
| Nr. Cases | 3 | 12 | 30 | 26 |
| MMSE | 28±1 | 25.7±1.8 | 28.9±1.4 | 25.9±1.7 |
| GDS | 5.66±0.6 | 3.61±1.7 | 1.03±1.3 | 1.5±1.5 |
| NLR | 3.3±0.9 | 3.9±1(*) | 2.4±1.1 | 2.3±0.8(*) |
| Associated Pathology | 100% | 80% | 20% | 45% |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



