Submitted:
28 February 2023
Posted:
06 March 2023
You are already at the latest version
Abstract
Background: Chikungunya virus (CHIKV) diagnosis have become a challenge for primary care physicians in areas where zika virus and/or dengue virus are present. Case definitions for the three arboviral infections are overlapping. Methods: A cross-sectional analysis was carried out. A bivariate analysis was made using confirmed CHIKV infection as the outcome. Variables with significant statistical association were included in an agreement consensus. Agreed variables were analyzed in multiple regression model. The area under the receiver operating characteristic (ROC) curve was calculated to determine a cut-off value and performance. Results: 295 patients with confirmed CHIKV infection were included. A screening tool was made using symmetric arthritis (4 points), fatigue (3 points), rash (2 points) and ankle joint pain (1 point). The ROC curve identified a cut-off value and a score ≥ 5.5 was considered positive to identify CHIKV patients with a sensibility of 64.4% and a specificity of 87.4%, positive predictive value of 85.5%, negative predictive value of 67.7%, area under the curve of 0.72, and an accuracy of 75%. Conclusion: We developed a screening tool for CHIKV diagnosis using only clinical symptoms as well as proposed an algorithm to aid the primary care physician.
Keywords:
Chikungunya virus
; diagnosis
; arbovirus infections
; clinical decision making
; Colombia
1. Introduction
Chikungunya virus (CHIKV) is a member of the Semliki Forest virus antigenic complex and is classified as an alphavirus from the Togaviridae family, which causes acute arthropathy in humans similar to other alphaviruses[1]. After the epidemic in La Reunion in 2006, due to an adaptive mutation of alanine for valine at position 226 (A226V) in the E1 glycoprotein of CHIKV, it gained the ability to be transmitted not only by Aedes (Ae) aegypti but also by Ae. albopictus[2].
The Asian lineage of CHIKV rapidly spread to the Western Hemisphere, affecting 42 countries by 2015 and finally reaching Colombia in August 2014 after arriving at the Island of Saint Martin in 2013[3,4,5,6]. CHIKV infection became a pandemic, affecting countries where other arboviral diseases were present, for example, the infections caused by Zika virus (ZIKAV) or Dengue virus (DENV) (Figure 1).
According to the Centre for Disease Control and Prevention data, half of the countries have reported autochthonous transmission of the three viruses[7,8,9]. In these countries, diagnosis in a primary care setting becomes a challenge since the infections caused by CHIKV, DENV, and ZIKAV share clinical symptoms. Fever, headache, myalgia, and bleeding are frequently reported symptoms in patients suffering from CHIKV, ZIKV, or DENV infection[10,11,12,13,14,15,16,17,18,19,20,21,22,23,24,25,26,27,28,29,30]. However, some symptoms are more specifically associated with each virus, for example, arthralgia and arthritis in CHIKV infection, rashes, and red eyes in ZIKV infection, and fever and gastrointestinal symptoms in DENV infection (Figure 2, Tables S1 and S2).
Therefore, diagnosis of CHIKV infection requires laboratory confirmation by a polymerase chain reaction (PCR), serological test, or viral culture[31]. Directing public health care policies, confirming a clinical diagnosis, and conducting accurate infectious disease surveillance requires proper laboratory testing; however, access is restricted in many middle- or low-income tropical or subtropical countries, especially where primary care physicians face this infection[11,32] . According to reports from the National Health Institute, in Colombia, only 1.08% of CHIKV-infected patients (5231 out of 482326) were clinically confirmed in laboratory during epidemiological week 37 of 2014 to week 44 of 2019[33,34,35,36,37,38]. The lack of confirmation of CHIKV infection increases the need for a reliable clinical diagnostic tool to aid primary care physicians when facing patients where common arboviral diseases caused by CHIKV, ZIKAV, and DENV are endemic or epidemic.
For this reason, we decided to evaluate the performance of the currently used diagnostic criteria for CHIKV infection. We applied the criteria to a population with confirmed CHIKV infection for improvements, and with the help of expert consensus, we created a diagnostic screening tool based on clinical symptoms.
2. Materials and Methods
Study population:
A cross-sectional analysis was conducted in a community cohort from Bogotá, Cali, Medellin, Cúcuta, Bucaramanga, and Barranquilla (Colombia). The included cities were chosen to represent the Colombian population, and the included patients between 2014 and 2015 were aged ≥ 18 years. The Community Oriented Program for Control of Rheumatic Diseases (COPCORD) methodology was used to include patients in the study[39]. COPCORD is an economical program that evaluates and measures disability and pain from rheumatic diseases. It is designed to be implemented in communities of developing countries. In 2014, from August to September, the CHIKV epidemic struck the country while the Colombian COPCORD study was being developed. Since CHIKV infection is mainly associated with musculoskeletal (MSK) symptoms, CHIKV-infected patients had to be identified within the studied population to avoid an increase in cases in the COPCORD study. Information on the socioeconomic and sociodemographic variables was collected using a questionnaire. Individuals were asked about non-traumatic MSK symptoms, such as stiffness, pain, arthralgia, or arthritis. A patient was considered COPCORD-positive if any of these symptoms were present at any moment in their life or 7 days prior to the interview. Every COPCORD-positive patient was questioned regarding CHIKV infection symptoms. If CHIKV infection was considered, a secondary examination was carried out within the following 7 days by a trained rheumatologist or rheumatology fellow. The criteria for suspected cases of CHIKV fever were applied according to the World Health Organization (WHO) guidelines[31]. Blood samples were collected from patients who were asked about their joint, gastrointestinal, and dermatological symptoms using a specifically designed questionnaire. Patients were assessed one time and were factored out when a rheumatic disease was suspected or confirmed by the physician. All samples from the suspected patients, when analyzed for DENV-specific IgM antibody, produced a negative result. At the time of data collection, the ZIKV epidemic was not present in Colombia.
WHO CHIKV infection case definition[31]:
A case was suspected due to epidemiological criteria (living or visiting geographical areas with reports of transmission within 15 days prior to the onset of symptoms) and clinical criteria (acute onset of high temperature >38.5 ºC and “incapacitating joint pain”). A confirmed case was considered when the presence of virus-specific IgM or IgG antibodies were proven irrespective of the clinical presentation or stage of the disease. On the grounds that our sample had no previous reports of CHIKV infection before this epidemic, therefore immunologically naïve, we took into account the presence of virus-specific IgG antibodies in a single serum sample at any point of the disease as positive for confirmed CHIKV infection.
CHIKV serological analysis:
Enzyme-linked immunosorbent assay (ELISA) with chikungunya IgG and IgM antibody was made fitting to the maker's guidelines (ab177848 anti-CHIKV IgM and ab177835 anti-CHIKV IgG, Abcam, Cambridge, UK).
Statistical analysis:
Mean and standard deviation (SD) for continuous variables and counts while percentages for categorical variables were used for descriptive analyses. Two-by-two tables were used to establish the associations between categorical variables. Student’s t-test was used to compare the mean values. Statistical significance was set at p < 5%. For associations, odds ratios (OR) were calculated with 95% confidence intervals (CIs). A positive CHIKV serology result (IgG or IgM) was used to identify subjects with CHIKV infections. Bivariate analysis was performed, including all studied variables, using confirmed CHIKV infection as the outcome. Variables with significant statistical association with the outcome were included in agreement. Agreed variables were analyzed in a multiple regression model using a stepwise forward method. Hosmer and Lemeshow’s goodness-of-fit test was used to assess model performance. The area under the receiver operating characteristic (ROC) curve was calculated to determine the cut-off value and performance. SPSS (Statistical Package for the Social Sciences; version 22.0; IBM, Armonk, NY, USA) was used for data analysis.
Agreement consensus:
Specialists from different regions of Colombia with experience in diagnosing and treating CHIKV infection (five rheumatologists, two epidemiologists, and two tropical medicine specialists) met face-to-face to conduct an agreement study on the clinical characteristics of CHIKV infection and its associations. Sequential questions were prepared and answered in real-time to determine which statistically significant variables obtained from the bivariate analysis should be considered clinical criteria for CHIKV diagnosis. Only the following answers were possible: totally agree, agree, not in agree or disagree, disagree, and totally disagree. Answers were calculated as percentages, and a percentage ≥50% was set as agreement, regardless of the answer. When agreement was not reached, the moderator reformulated the question after discussing the opinions of confronting members. This procedure was repeated until a consensus was reached.
3. Results
3.1. Study participants:
In the COPCORD study, 6528 people were surveyed in their homes. Of these, 548 have been included in the present study due to clinical suggestion of CHIKV infection. All 548 subjects were serologically tested for CHIKV antibody to confirm the diagnosis, and 295 (53.8%) resulted positive for IgG or IgM (Figure 3).
3.2. Demographics:
The mean age was 48.8 years (SD±17.5) for the whole studied population (548 patients). Of the patients, 57.7% (n = 316) were > 45 years old, and most were female (n = 382, 69.7%). According to the WHO criteria for acute clinical CHIKV infection, only 50.5% (n = 149) of the patients were confirmed for the disease by serological analysis (Table 1).
3.3. Clinical characteristics:
In general, all clinical characteristics, including signs and symptoms found by the examiner or described by the patient, were more frequent in patients with serologically confirmed CHIKV infections (Figure 4). Notably, arthritis (regardless of the affected joint) was the most frequent symptom in this group of patients.
3.4. Univariate analysis:
After univariate analysis of signs and symptoms, only shoulder arthralgia was found with no statistical significance between patients with positive and negative CHIKV serology results (Table 2). Feet arthritis showed the highest odds ratio (OR: 45.4); however, it had the widest confidence interval (95% CI: 6.2-332.0). The best variables considering high OR and narrow CI were symmetric arthritis (OR: 18.1; 95% CI: 7.8-42.1), ankle arthritis (OR: 15.8; 95% CI: 4.8-51.4), abdominal rash (OR: 14.0; 95% CI: 6.3-31.0), and fatigue (OR: 10.5; 95% CI: 6.7-16.5).
3.5. Agreement and expert consensus results:
A series of questions were formulated for a group of specialists with statistically significant variables from the univariate analysis to evaluate agreement or disagreement in the diagnosis of CHIKV infection. There was disagreement on the following variables as clinical criteria: mucosal and gastrointestinal symptoms, shoulder and elbow arthralgia, and arthritis (Table 3).
3.6. Multiple logistic regression analysis and ROC curve:
A multiple logistic regression model used on the agreed variables to compare confirmed CHIKV-positive and CHIKV-negative patients. After four steps in the model, CHIKV infection confirmed by positive serology result was independently associated with symmetric arthritis, rash, ankle joint pain, and fatigue. Each sign and symptom were assigned a point based on their coefficients (Table 4).
The ROC curve identified a cut-off value of 5.5, which maximized sensitivity and specificity (Figure 5). A score ≥ 5.5 was considered positive to identify CHIKV-infected patients with a sensitivity of 64.4% (95% CI: 58.7%-69.9%) and a specificity of 87.4% (95% CI: 82.7%-91.2%).
The score performance was compared to other established clinical diagnostic tools for CHIKV, DENV, and ZIKAV infections in our cohort study (Figure 6). Based on this, we proposed a diagnostic screening clinical tool which was compared to other tools and criteria reported for these arboviral diseases (Table 5).
4. Discussion
In the present study, we analyzed the clinical signs and symptoms of 548 patients with suspected CHIKV infection and their association with confirmed CHIKV serology results to formulate a clinical screening tool for use in primary care settings. After univariate analysis, the variables associated with positive CHIKV serology results were discussed with an expert panel. Based on their experience in diagnosis and disease treatment, the most representative variables in CHIKV-infected patients were established.
It is well known that expert consensus defines the most appropriate selection of variables by considering different perspectives and positions of the experts consulted in the process[40]. Therefore, we included more meaningful and valuable variables for clinicians in the final multivariate analysis. The symptoms independently associated with CHIKV infection were observed to be symmetric arthritis, fatigue, rash, and ankle joint pain. A clinical screening tool was developed, which yielded high specificity (87.4%) and positive predictive value (PPV; 85.6%) with moderate sensitivity (64.4%) and negative predictive value (NPV; 67.8%).
When assessing people´s health, two types of tests are used: diagnostic tests that offer final information on the presence or absence of a condition and screening tests that are less demanding on the healthcare system, more accessible, less invasive, time-consuming, and expensive[41]. The screening tests display ideal characteristics for countries where arboviral diseases caused by CHIKV, DENV, and ZIKAV are endemic. These tests are evaluated according to their sensitivity, specificity, PPV, and NPV. In brief, sensitivity and specificity refer to the accuracy of a screening test with a reference or gold standard, whereas PPV and NPV indicate the success of a screening test in classifying people as having or not having a condition[41]. Therefore, in screening situations for individuals in a clinical setting, it is more appropriate to use the PPV and NPV values for evaluating the performance of a screening tool. Our screening tool has a high PPV but a moderate NPV. A high PPV is desirable in situations where the costs of diagnostics, treatment, and services are increased when the studied condition progresses slowly or is not life-threatening[41]. A moderate NPV might be acceptable if later assessments can be programmed and completed or if the condition is possible to sort out with no treatment[41]. Since chikungunya disease displays the above-mentioned characteristics, we believe that our screening tool will be useful in diagnosing CHIKV infection in a primary care setting where only clinical variables are at hand.
Other performance indicators of our screening tool, such as the Youden index (YI; 52) and accuracy (75.0%) when applied to our cohort, were higher than the previously developed diagnostic criteria or screening tools for CHIKV infection. The WHO case definition showed lower performance values in our cohort than our screening tool. Due to the ambiguity of the definition (Supplementary Table S3), only the mandatory symptoms (joint pain and fever) were used to calculate performance in our cohort[31]. Fever and joint pain are commonly included in other arboviral case definitions. For example, the WHO ZIKAV case definition (2016) states that the presence of fever or rash plus at least one more symptom, of which arthralgia is one, constitutes a suspected case[42]. In addition, the WHO DENV case definition includes fever plus two more symptoms, in which pain and aches are also present[43]. In fact, the recurring symptoms in the WHO case definitions of CHIKV, ZIKAV, and DENV are fever, aches, and pain (interpreted as arthralgia or myalgia). Furthermore, in the WHO CHIKV case definition, the use of terms like “usually incapacitating” or “usually accompanied by…” could lead to misinterpretation by physicians resulting in over or underdiagnosis and finally poor performance when used in epidemics. Moreover, using fever as a mandatory or inclusion symptom dismisses asymptomatic patients, which increases the percentage of false negatives and selection bias.
Multiple attempts have been made to develop a better screening tool. Sissoko et al. (2010) found the combination of fever and polyarthralgia as the most relevant clinical pattern of CHIKV infection to identify presumptive cases during epidemics, yielding an accuracy of 87% with high sensitivity (84%) and specificity (89%)[11]. However, when applied to our cohort, the accuracy and sensitivity decreased to 69% and 51%, respectively. A possible explanation could be attributed to the median age of their cohort (24 years) since symptomatic expression of infection is lower in younger age groups[11].
In 2013, Thiberville et al. developed a clinical score with fever and arthralgia as mandatory symptoms. They added the presence of specific joint involvement (wrist or hand arthralgia) and the absence of myalgia to improve performance[26]. Their clinical score had the best performance in our cohort, with similar results as our own (Table 5). We believe that the resemblance lies in the use of specific disease symptoms. Our screening tool requires the inclusion of symmetrical arthritis or ankle joint pain to reach the cut-off point when added to other more generic symptoms such as fatigue and rash. These symptoms are almost unique to CHIKV infection and are rare in other arboviral infections caused by ZIKAV or DENV.
A study by Macpherson et al. (2014) found that a patient with joint pain and any combination of fever, myalgia, or rash was in 85% agreement with a positive CHIKV serological test result[12]. However, when applied to our cohort, the combination of arthralgia and fever yielded the best accuracy but sacrificed YI. Combining arthralgia with myalgia or rash increased specificity at the expense of sensitivity.
Other authors have elaborated on screening tools using simple clinical laboratory parameters. For example, the performance of Thiberville screening tool increases if lymphopenia is present[26]. Godaert et al. (2017) used lymphopenia in the presence of fever and ankle arthralgia and the absence of neutrophil leukocytosis for CHIKV infection screening in elderly people[16] . Laboratory studies improve diagnosis; however, even simple laboratory tests are sometimes unavailable to primary care physicians. Therefore, developing a diagnostic tool based on clinical parameters was our primary goal.
With the appearance of ZIKAV epidemics, the clinical symptoms that help differentiate CHIKV from ZIKAV or DENV have been studied. Cleton et al. (2015) found that arthralgia, arthritis, and rash were associated with CHIKV infection, whereas DENV-positive patients had increased odds ratios for rash, fever, and hemorrhagic symptoms[44]. In our cohort, the syndromic combination of arthritis and rash yielded a high specificity but moderate to low sensitivity, yet a similar PPV and NPV to our screening tool.
Sahadeo et al. (2015) compared patients with confirmed DENV and CHIKV infections to obtain clinical and laboratory features that could help distinguish between the two diseases[27]. The combination with the best performance to differentiate between DENV and CHIKV infection was rash, joint pain, and leukocyte count <7x103/µl. However, the PPV (58%) was less than optimal.
Another study by Lee et al. (2012) designed decision tree models for discriminating between DENV and CHIKV infections using clinical symptoms (presence of fever and its duration, bleeding, and illness) or laboratory tests (presence of thrombocytopenia)[22]. Interestingly, fever was associated with DENV infection and absent in CHIKV infection. A similar feature was found in our screening tool, where fever was not a mandatory symptom for suspected CHIKV diagnosis.
In a noteworthy study by Braga et al. (2017), a case definition was developed from a cohort of patients where CHIKV, DENV, and ZIKA were co-circulating[17]. A score ≥ 7.5 granted the diagnosis of ZIKV from the following symptoms: pruritus, rash, conjunctival hyperemia, and the absence of fever and anorexia. This is consistent with the decision tree of Lee et al. (2012) and our screening tool, where fever as a symptom was not included. Half of the patients in our cohort with confirmed CHIKV would test positive for ZIKAV according to Braga’s ZIKAV case definition using a combination of no fever and rash (true positives: 58.9%), rash and pruritus (true positives: 44.7%), and no fever or pruritus (true positives: 55.9%). This can be explained by the fact that rash, a frequent symptom in our CHIKV-confirmed patients (87.4%), was awarded a high score (7 points from a cut-off of 7.5) in Braga’s case definition. Other studies on CHIKV epidemics have reported similar findings[45,46]. One could argue that if the CHIKV sample in Braga et al. (2017) study was larger, the appointed value for rash would be smaller and would have less preponderance in the score.
The same exercise yielded similar results when the WHO DENV case definitions were applied to our cohort. This exemplifies the need to assign importance to cardinal and specific symptoms of each infection. Although fatigue and rash are present in other definitions of DENV and ZIKAV, the presence of joint involvement (symmetrical arthritis or ankle joint pain) is mandatory in our screening tool to reach the cut-off point of 5.5. With this in mind, we proposed an algorithm for the clinical approach to CHIKV, ZIKAV, and DENV infections (Figure 7).
Our study has some limitations. First, given that our study resulted from the structure of a COPCORD approach, there is a selection bias regarding MSK symptoms. Second, since there was no physical exam when the symptoms started in each patient, these symptoms could not be validated by a physician; therefore, recall bias could be present. Third, PCR was not performed to confirm CHIKV infection because of its high cost. Lastly, our screening tool has not been validated in other cohorts.
Nevertheless, our study has several strengths. The country’s population is well represented in the study, bearing in mind the number of samples and the six geographic regions in which the study was performed. In addition, the accuracy of physical examination, especially of the musculoskeletal system, was warranted because all the patients were evaluated by a trained or in training professional of rheumatology. Finally, since the patients were evaluated in their homes and not in a medical setting, we could find even asymptomatic patients who otherwise would not attend a physician.
5. Conclusion
We developed a screening tool for CHIKV diagnosis using only clinical symptoms and proposed an algorithm to aid primary care physicians in the approach of common arboviral infections when laboratory tests are not available.
Supplementary Materials
The following supporting information can be downloaded at the website of this paper posted on Preprints.org. Table S1: Percentage of most common symptoms in arboviral diseases; Table S2: Statistical differences between symptoms and arboviral diseases; Table S3: Definitions of diagnostic criteria and screening tools.
Author Contributions
Conceptualization: JCR, IPB, JIA, AMS, CP, JL; Methodology: JCR, IPB, JIA, AMS, CP, JL; Formal analysis and investigation: JCR, IPB, JIA, AMS, CP, ELS, JMR, EF, DLS, PXP, MJM, CVE, JCS, IR, GRS, MHC, JL; Writing-original draft preparation: JCR; Writing-review and editing: JCR, IPB, JIA, AMS, CP, ELS, JMR, EF, DLS, PXP, MJM, CVE, JCS, IR, GRS, MHC, JL; Funding acquisition: JCR, AMS, JL; Resources: JL; Supervision: JCR, AMS, JL.
Funding
This work was supported by the Colombian Rheumatology Association [ACTA 169 10th JULY 2015], Universidad de La Sabana [MED-197-2015], and COLCIENCIAS doctoral scholarship [757-2016].
Institutional Review Board Statement
This study was executed in accordance with the Declaration of Helsinki 2013. Informed consent was obtained prior to admission. Our study was ratified by the ethics committee of Hospital Militar Central (study approval number 106-2016) and La Universidad de La Sabana (study approval number MED-197-2015).
Data Availability Statement
The data that support the findings of this study are available from the corresponding author, [JL], upon reasonable request.
Acknowledgments
The authors sincerely thank all participating patients for their support and patience.
Conflicts of Interest
The authors declare no conflict of interest. The funders had no role in the design of the study; in the collection, analyses, or interpretation of data; in the writing of the manuscript; or in the decision to publish the results.
References
- Powers, A.M.; Brault, A.C.; Tesh, R.B.; Weaver, S.C. Re-emergence of chikungunya and o’nyong-nyong viruses: Evidence for distinct geographical lineages and distant evolutionary relationships. J. Gen. Virol. 2000, 81, 471–479. [CrossRef]
- Tsetsarkin, K.A.; Vanlandingham, D.L.; McGee, C.E.; Higgs, S. A single mutation in Chikungunya virus affects vector specificity and epidemic potential. PLoS Pathog. 2007, 3, 1895–1906. [CrossRef]
- The Pan American Health Organization. Number of Reported Cases of Chikungunya Fever in the Americas , by Country or Territory Cumulative cases ( Updated 15 May 2015 ) Data source : Cases reported by IHR NFPs to PAHO / WHO and / or through Member States websites or official news publication. 2015, 2015, 2048.
- Padilla, J.C.; Lizarazo, F.E.; Murillo, O.L.; Mendigaña, F.A.; Pachón, E.; Vera, M.J. Epidemiología de las principales enfermedades transmitidas por vectores en Colombia, 1990-2016. Biomédica 2017, 37, 27.
- Rodas, J.D.; Kautz, T.; Camacho, E.; Paternina, L.; Guzmán, H.; Díaz, F.J.; Blanco, P.; Tesh, R.; Weaver, S.C. Genetic Characterization of Northwestern Colombian Chikungunya Virus Strains from the 2014-2015 Epidemic. Am. J. Trop. Med. Hyg 2016, 95, 639–646. [CrossRef]
- Cassadou, S.; Boucau, S.; Petit-Sinturel, M.; Huc, P.; Leparc-Goffart, I.; Ledrans, M. Emergence of chikungunya fever on the French side of Saint Martin island, October to December 2013. Eurosurveillance 2014, 19. [CrossRef]
- Dengue Around the World | Dengue | CDC Available online: https://www.cdc.gov/dengue/areaswithrisk/around-the-world.html (accessed on Dec 4, 2019).
- Geographic Distribution | Chikungunya virus | CDC Available online: https://www.cdc.gov/chikungunya/geo/index.html (accessed on Dec 4, 2019).
- Zika Travel Information | Travelers’ Health | CDC Available online: https://wwwnc.cdc.gov/travel/page/zika-information (accessed on Dec 4, 2019).
- Kularatne, S.A.M.; Gihan, M.C.; Weerasinghe, S.C.; Gunasena, S. Concurrent outbreaks of Chikungunya and Dengue fever in Kandy, Sri Lanka, 2006-07: A comparative analysis of clinical and laboratory features. Postgrad. Med. J. 2009, 85, 342–346.
- Sissoko, D.; Ezzedine, K.; Moendandzé, A.; Giry, C.; Renault, P.; Malvy, D. Field evaluation of clinical features during chikungunya outbreak in Mayotte, 2005-2006. Trop. Med. Int. Heal. 2010, 15, 600–607. [CrossRef]
- Macpherson, C.; Noël, T.; Fields, P.; Jungkind, D.; Yearwood, K.; Simmons, M.; Widjaja, S.; Mitchell, G.; Noel, D.; Bidaisee, S.; et al. Clinical and serological insights from the asian lineage Chikungunya outbreak in Grenada, 2014: An observational study. Am. J. Trop. Med. Hyg. 2016, 95, 890–893. [CrossRef]
- Bloch, D.; Roth, N.M.; Caraballo, E. V.; Muñoz-Jordan, J.; Hunsperger, E.; Rivera, A.; Pérez-Padilla, J.; Rivera Garcia, B.; Sharp, T.M. Use of Household Cluster Investigations to Identify Factors Associated with Chikungunya Virus Infection and Frequency of Case Reporting in Puerto Rico. PLoS Negl. Trop. Dis. 2016, 10, e0005075. [CrossRef]
- van Genderen, F.T.; Krishnadath, I.; Sno, R.; Grunberg, M.G.; Zijlmans, W.; Adhin, M.R. First Chikungunya Outbreak in Suriname; Clinical and Epidemiological Features. PLoS Negl. Trop. Dis. 2016, 10, 1–18.
- Anaya, J.-M.; Rodríguez, Y.; Monsalve, D.M.; Vega, D.; Ojeda, E.; González-Bravo, D.; Rodríguez-Jiménez, M.; Pinto-Díaz, C.A.; Chaparro, P.; Gunturiz, M.L.; et al. A comprehensive analysis and immunobiology of autoimmune neurological syndromes during the Zika virus outbreak in Cúcuta, Colombia. J. Autoimmun. 2017, 77, 123–138. [CrossRef]
- Godaert, L.; Bartholet, S.; Najioullah, F.; Hentzien, M.; Fanon, J.L.; Césaire, R.; Dramé, M. Screening for Chikungunya virus infection in aged people: Development and internal validation of a new score. PLoS One 2017, 12, 1–9. [CrossRef]
- Braga, J.U.; Bressan, C.; Dalvi, A.P.R.; Calvet, G.A.; Daumas, R.P.; Rodrigues, N.; Wakimoto, M.; Nogueira, R.M.R.; Nielsen-Saines, K.; Brito, C.; et al. Accuracy of Zika virus disease case definition during simultaneous Dengue and Chikungunya epidemics. PLoS One 2017, 12, e0179725. [CrossRef]
- Silva, M.M.; Tauro, L.B.; Kikuti, M.; Anjos, R.O.; Santos, V.C.; Gonçalves, T.S.F.; Paploski, I.A.D.; Moreira, P.S.S.; Nascimento, L.C.J.; Campos, G.S.; et al. Concomitant transmission of dengue, chikungunya and Zika viruses in Brazil: Clinical and epidemiological findings from surveillance for acute febrile illness. Clin. Infect. Dis. 2018, 8.
- Carabali, M.; Lim, J.K.; Palencia, D.C.; Lozano-Parra, A.; Gelvez, R.M.; Lee, K.S.; Florez, J.P.; Herrera, V.M.; Kaufman, J.S.; Rojas, E.M.; et al. Burden of dengue among febrile patients at the time of chikungunya introduction in Piedecuesta, Colombia. Trop. Med. Int. Heal. 2018, 23, 1231–1241. [CrossRef]
- Sánchez-Carbonel, J.; Tantaléan-Yépez, D.; Aguilar-Luis, M.A.; Silva-Caso, W.; Weilg, P.; Vásquez-Achaya, F.; Costa, L.; Martins-Luna, J.; Sandoval, I.; del Valle-Mendoza, J. Identification of infection by Chikungunya, Zika, and Dengue in an area of the Peruvian coast. Molecular diagnosis and clinical characteristics. BMC Res. Notes 2018, 11, 175.
- Azeredo, E.L.; Hoscher Romanholi, I.; Badolato-Corrêa, J.; Cunha, R.; Barbosa, L.S.; de-Oliveira-Pinto, L.M.; Dal Fabbro, M.; dos Santos, F.B.; Sánchez-Arcila, J.C.; Nunes, P.C.G.; et al. Clinical and Laboratory Profile of Zika and Dengue Infected Patients: Lessons Learned From the Co-circulation of Dengue, Zika and Chikungunya in Brazil. PLoS Curr. 2018. [CrossRef]
- Lee, V.J.; Chow, A.; Zheng, X.; Carrasco, L.R.; Cook, A.R.; Lye, D.C.; Ng, L.C.; Leo, Y.S. Simple Clinical and Laboratory Predictors of Chikungunya versus Dengue Infections in Adults. PLoS Negl. Trop. Dis. 2012, 6.
- Vega, F.L.R.; Bezerra, J.M.T.; Said, R.F. de C.; Gama Neto, A.N. da; Cotrim, E.C.; Mendez, D.; Amâncio, F.F.; Carneiro, M. Emergence of chikungunya and Zika in a municipality endemic to dengue, Santa Luzia, MG, Brazil, 2015-2017. Rev. Soc. Bras. Med. Trop. 2019, 52, 1–9. [CrossRef]
- Taraphdar, D.; Sarkar, A.; Mukhopadhyay, B.B.; Chatterjee, S. A Comparative Study of Clinical Features between Monotypic and Dual Infection Cases with Chikungunya Virus and Dengue Virus in West Bengal, India. Am. J. Trop. Med. Hyg. 2012, 86, 720–723. [CrossRef]
- Mohd Zim, M.A.; Sam, I.-C.; Omar, S.F.S.; Chan, Y.F.; AbuBakar, S.; Kamarulzaman, A. Chikungunya infection in Malaysia: Comparison with dengue infection in adults and predictors of persistent arthralgia. J. Clin. Virol. 2013, 56, 141–145. [CrossRef]
- Thiberville, S.D.; Boisson, V.; Gaudart, J.; Simon, F.; Flahault, A.; de Lamballerie, X. Chikungunya Fever: A Clinical and Virological Investigation of Outpatients on Reunion Island, South-West Indian Ocean. PLoS Negl. Trop. Dis. 2013, 7. [CrossRef]
- Sahadeo, N.; Mohammed, H.; Allicock, O.M.; Auguste, A.J.; Widen, S.G.; Badal, K.; Pulchan, K.; Foster, J.E.; Weaver, S.C.; Carrington, C.V.F. Molecular Characterisation of Chikungunya Virus Infections in Trinidad and Comparison of Clinical and Laboratory Features with Dengue and Other Acute Febrile Cases. PLoS Negl. Trop. Dis. 2015, 9, 1–18.
- Waggoner, J.J.; Gresh, L.; Vargas, M.J.; Ballesteros, G.; Tellez, Y.; Soda, K.J.; Sahoo, M.K.; Nuñez, A.; Balmaseda, A.; Harris, E.; et al. Viremia and Clinical Presentation in Nicaraguan Patients Infected With Zika Virus, Chikungunya Virus, and Dengue Virus. Clin. Infect. Dis. 2016, 63, 1584–1590. [CrossRef]
- Romero, C.; Zogbi, H.; Carvalho, M.S.; de Souza, R.V.; Calvet, G.A.; Brasil, P.; de Filippis, A.M.B.; Bressan, C. da S.; Mendonça, M.C.L. de; Alves, S.S.; et al. Zika Virus Outbreak in Rio de Janeiro, Brazil: Clinical Characterization, Epidemiological and Virological Aspects. PLoS Negl. Trop. Dis. 2016, 10, e0004636. [CrossRef]
- Danis-Lozano, R.; Díaz-González, E.E.; Trujillo-Murillo, K. del C.; Caballero-Sosa, S.; Sepúlveda-Delgado, J.; Malo-García, I.R.; Canseco-Ávila, L.M.; Salgado-Corsantes, L.M.; Domínguez-Arrevillaga, S.; Torres-Zapata, R.; et al. Clinical characterization of acute and convalescent illness of confirmed chikungunya cases from Chiapas, S. Mexico: A cross sectional study. PLoS One 2017, 12, 1–15. [CrossRef]
- World Health Organization (WHO) Chikungunya: case definitions for acute, atypical and chronic cases. Conclusions of an expert consultation, Managua, Nicaragua, 20-21 May 2015. Relev. Epidemiol. Hebd. 2015, 90, 410–4.
- Petti, C.A.; Polage, C.R.; Quinn, T.C.; Ronald, A.R.; Sande, M.A. Laboratory Medicine in Africa: A Barrier to Effective Health Care. Clin. Infect. Dis. 2006, 42, 377–382. [CrossRef]
- Salas Botero, D. Informe Final del Evento Chikungunya, Colombia 2014 Available online: http://www.ins.gov.co/buscador-eventos/Informesdeevento/Chikunguña 2014.pdf.
- Salas Botero, D. Informe Final del Evento Chikungunya, Colombia 2015 Available online: http://www.ins.gov.co/buscador-eventos/Informesdeevento/Chikunguña 2015.pdf.
- Pinilla Farias, A. Informe del Evento Chikungunya Periodo Epidemiológico XIII, Colombia 2016 Available online: http://www.ins.gov.co/buscador-eventos/Informesdeevento/Chikunguña 2016.pdf#search=chikungunya.
- Rodriguez Reyes, A.J. Informe del Evento Chikungunya, Colombia 2017 Available online: http://www.ins.gov.co/buscador-eventos/Informesdeevento/CHIKUNGUNYA 2017.pdf#search=chikungunya.
- 2018; 37. Instituto Nacional de Salud Boletín Epidemiológico Semanal Semana epidemiológica 52 23 al 29 de Diciembre de 2018; 2018.
- 2019; 38. Instituto Nacional de Salud Semana epidemiológica 44; 2019.
- Rueda, J.C.; Santos, A.M.; Angarita, J.I.; Giraldo, R.B.; Saldarriaga, E.L.; Ballesteros Muñoz, J.G.; Forero, E.; Valencia, H.; Somoza, F.; Martin-Arsanios, D.; et al. Demographic and clinical characteristics of chikungunya patients from six Colombian cities, 2014-2015. Emerg. Microbes Infect. 2019, 8, 1490–1500. [CrossRef]
- Fernández-Ávila, D.G.; Rojas, M.X.; Rosselli, D. Delphi method in rheumatology research: Are we doing well? Rev. Colomb. Reumatol. 2019.
- Trevethan, R. Sensitivity, Specificity, and Predictive Values: Foundations, Pliabilities, and Pitfalls in Research and Practice. Front. Public Heal. 2017, 5, 307.
- OMS Zika virus disease: Interim case definitions. Who/Zikv/Sur/16.1 2016, 2016.
- Organization, W.H. Dengue : Guidelines for Diagnosis Treatment Prevention and Control (New Edition 2009).; World Health Organization, 2009; ISBN 978 92 4 154787 1.
- Cleton, N.B.; Reusken, C.B.E.M.; Wagenaar, J.F.P.; van der Vaart, E.E.; Reimerink, J.; van der Eijk, A.A.; Koopmans, M.P.G. Syndromic Approach to Arboviral Diagnostics for Global Travelers as a Basis for Infectious Disease Surveillance. PLoS Negl. Trop. Dis. 2015, 9, 1–15. [CrossRef]
- Borgherini, G.; Poubeau, P.; Staikowsky, F.; Lory, M.; Moullec, N.L.; Becquart, J.P.; Wengling, C.; Michault, A.; Paganin, F. Outbreak of Chikungunya on Reunion Island: Early Clinical and Laboratory Features in 157 Adult Patients. Clin. Infect. Dis. 2007, 44, 1401–1407. [CrossRef]
- Kumar, R.; Sharma, M.; Jain, S.; Yadav, S.; Singhal, A. Cutaneous manifestations of chikungunya fever: Observations from an outbreak at a Tertiary Care Hospital in Southeast Rajasthan, India. Indian Dermatol. Online J. 2017, 8, 336. [CrossRef]
Figure 1.
World distribution of DENV, CHIKV, and ZIKAV. DENV: Dengue virus; CHIKV: Chikungunya virus; ZIKAV: Zika virus.
Figure 1.
World distribution of DENV, CHIKV, and ZIKAV. DENV: Dengue virus; CHIKV: Chikungunya virus; ZIKAV: Zika virus.
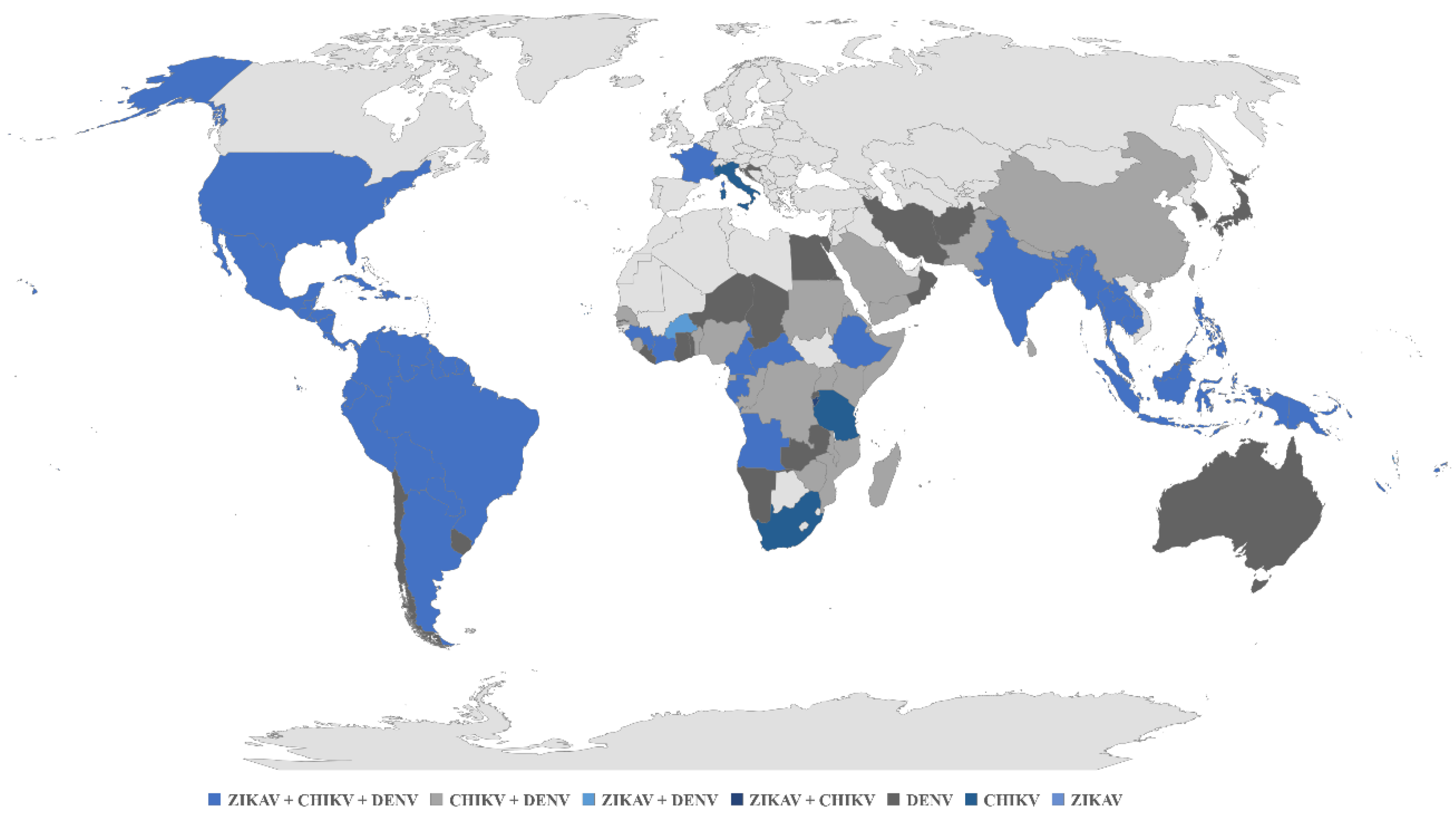
Figure 2.
Common symptoms in arboviral infection (DENV, CHIKV and ZIKAV). DENV: Dengue virus; CHIKV: Chikungunya virus; ZIKAV: Zika virus; p <0.05: *DENV-CHIKV; †DENV-ZIKAV; ‡CHIKV-ZIKAV.
Figure 2.
Common symptoms in arboviral infection (DENV, CHIKV and ZIKAV). DENV: Dengue virus; CHIKV: Chikungunya virus; ZIKAV: Zika virus; p <0.05: *DENV-CHIKV; †DENV-ZIKAV; ‡CHIKV-ZIKAV.
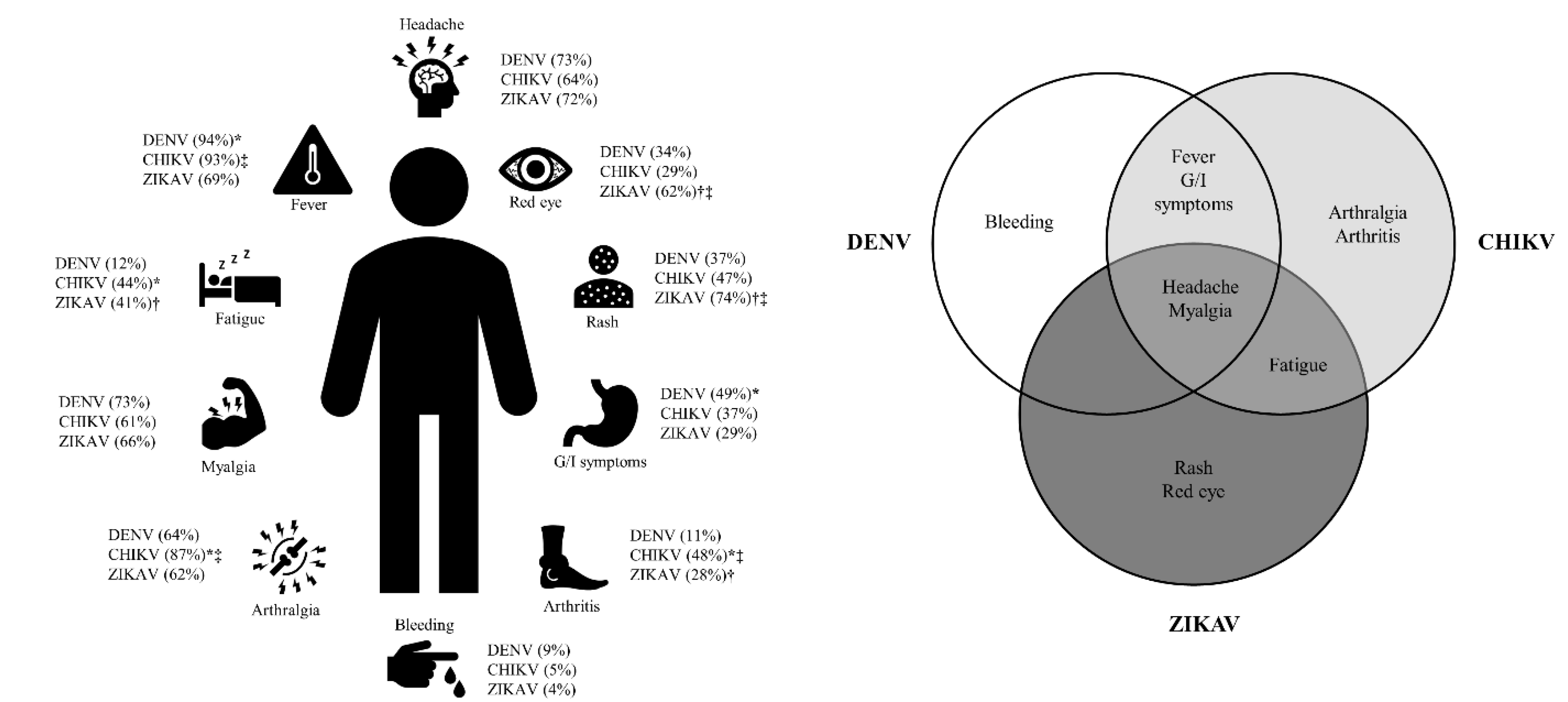
Figure 3.
Profile of the study population. COPCORD: Community Oriented Program for Control of Rheumatic Diseases; CHIKV: Chikungunya virus.
Figure 3.
Profile of the study population. COPCORD: Community Oriented Program for Control of Rheumatic Diseases; CHIKV: Chikungunya virus.
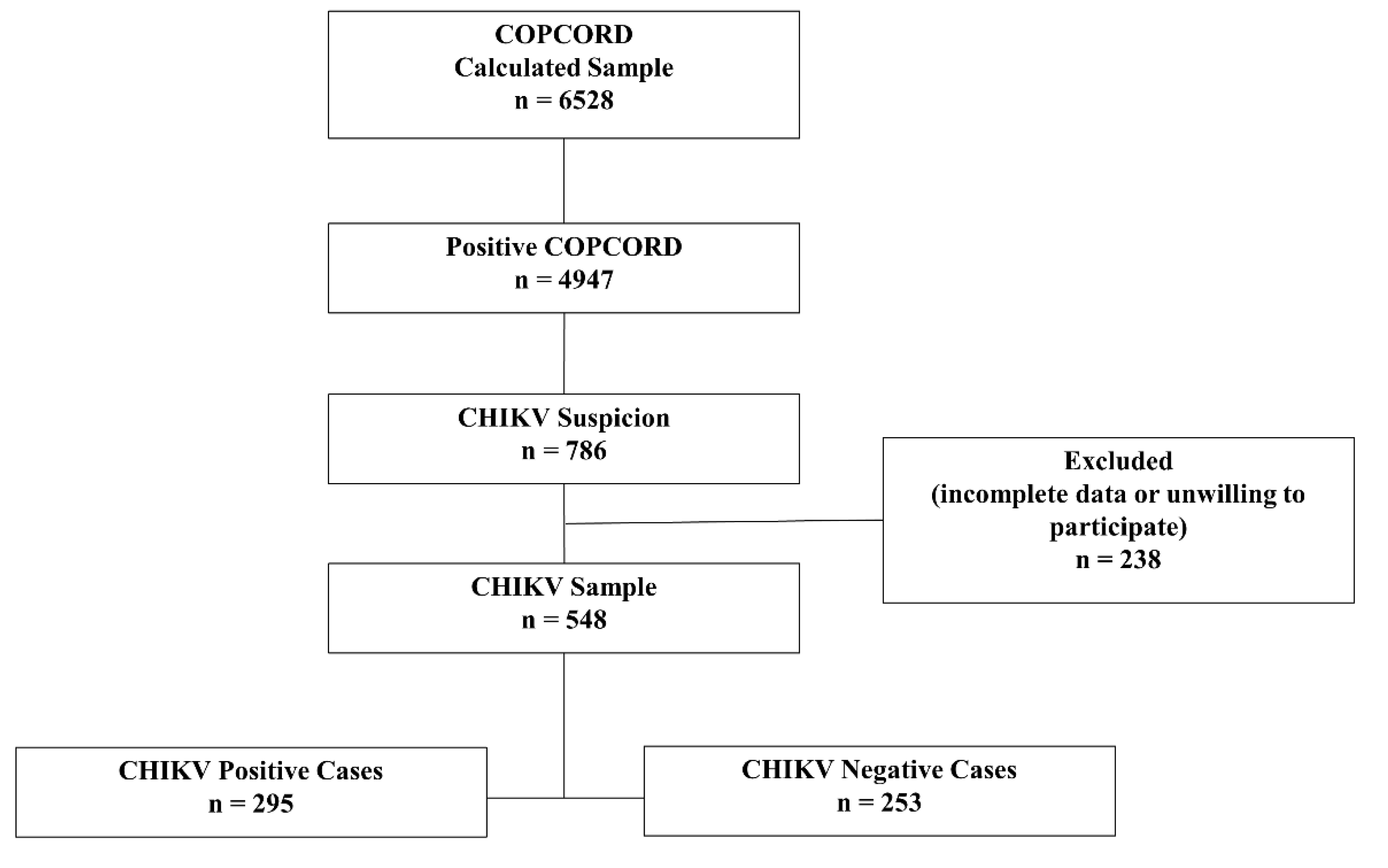
Figure 4.
Clinical characteristics of the study population. CHIKV: Chikungunya virus.
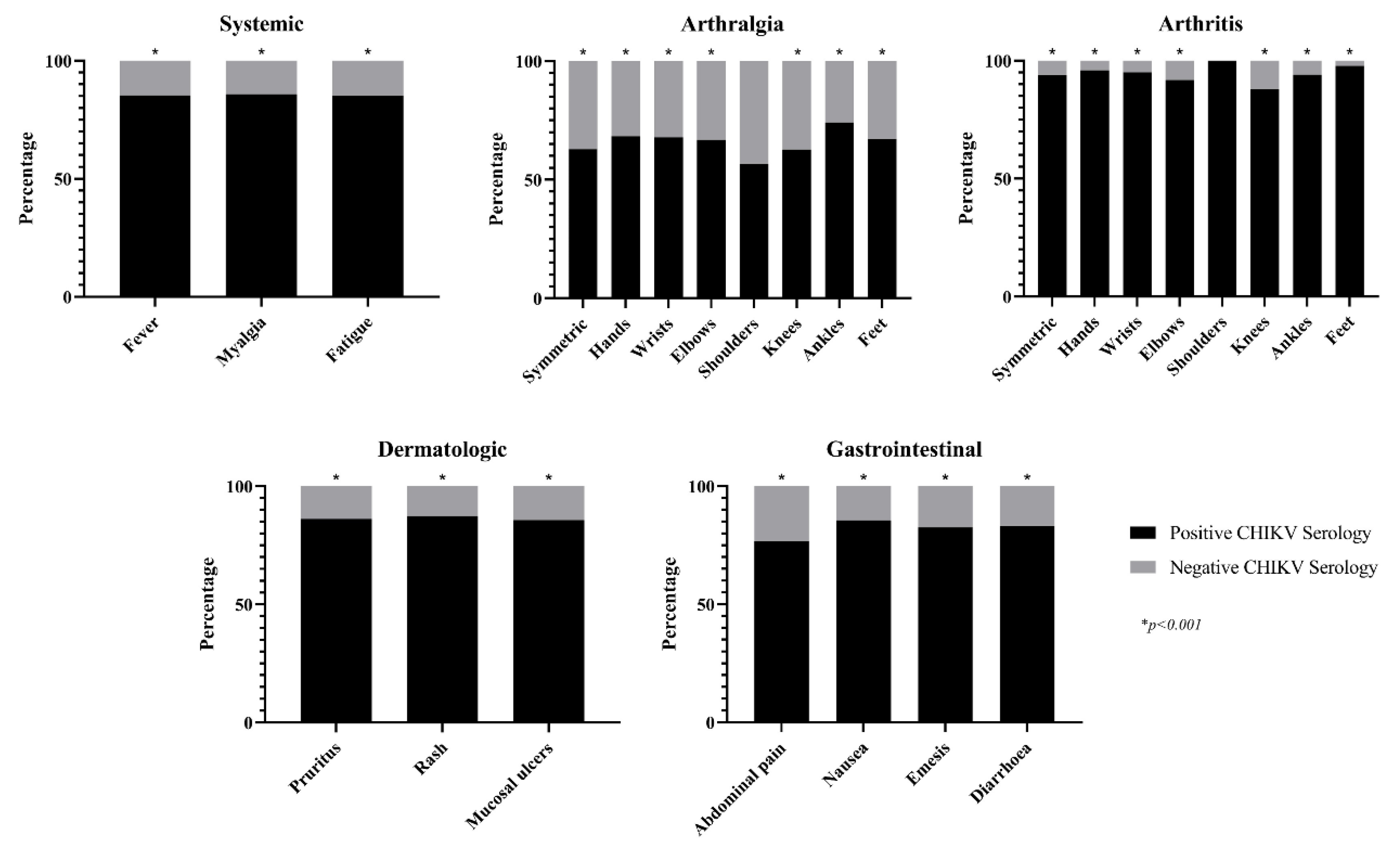
Figure 5.
ROC curve of the screening score for CHIKV infection. ROC: Receiver operating characteristic; CHIKV: Chikungunya virus.
Figure 5.
ROC curve of the screening score for CHIKV infection. ROC: Receiver operating characteristic; CHIKV: Chikungunya virus.
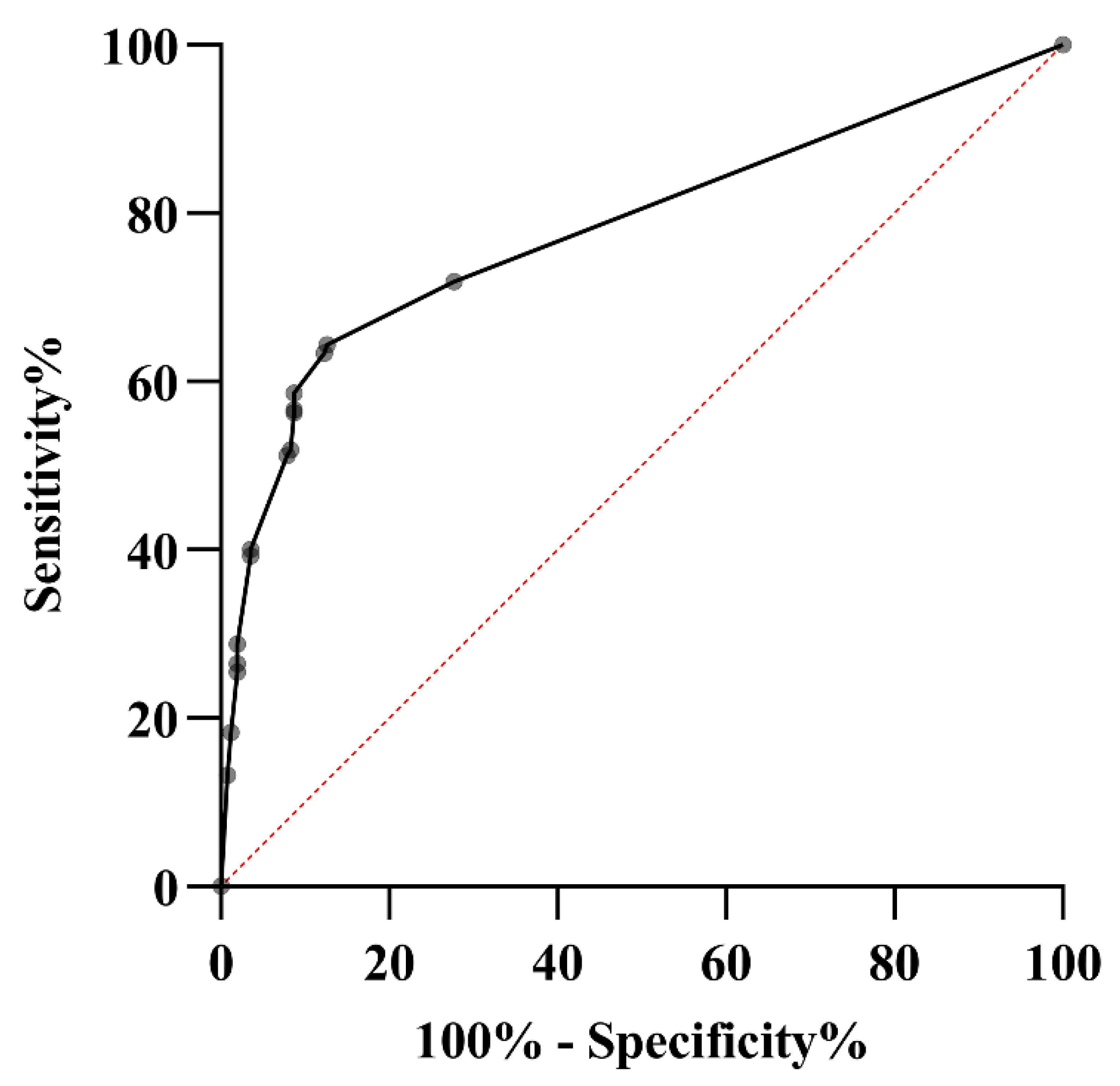
Figure 6.
ROC curves of multiple diagnostic and screening tools in CHIKV, DENV and ZIKAV. ROC: Receiver operating characteristic; CHIKV: Chikungunya virus, DENV: Dengue virus; ZIKAV: Zika virus.
Figure 6.
ROC curves of multiple diagnostic and screening tools in CHIKV, DENV and ZIKAV. ROC: Receiver operating characteristic; CHIKV: Chikungunya virus, DENV: Dengue virus; ZIKAV: Zika virus.
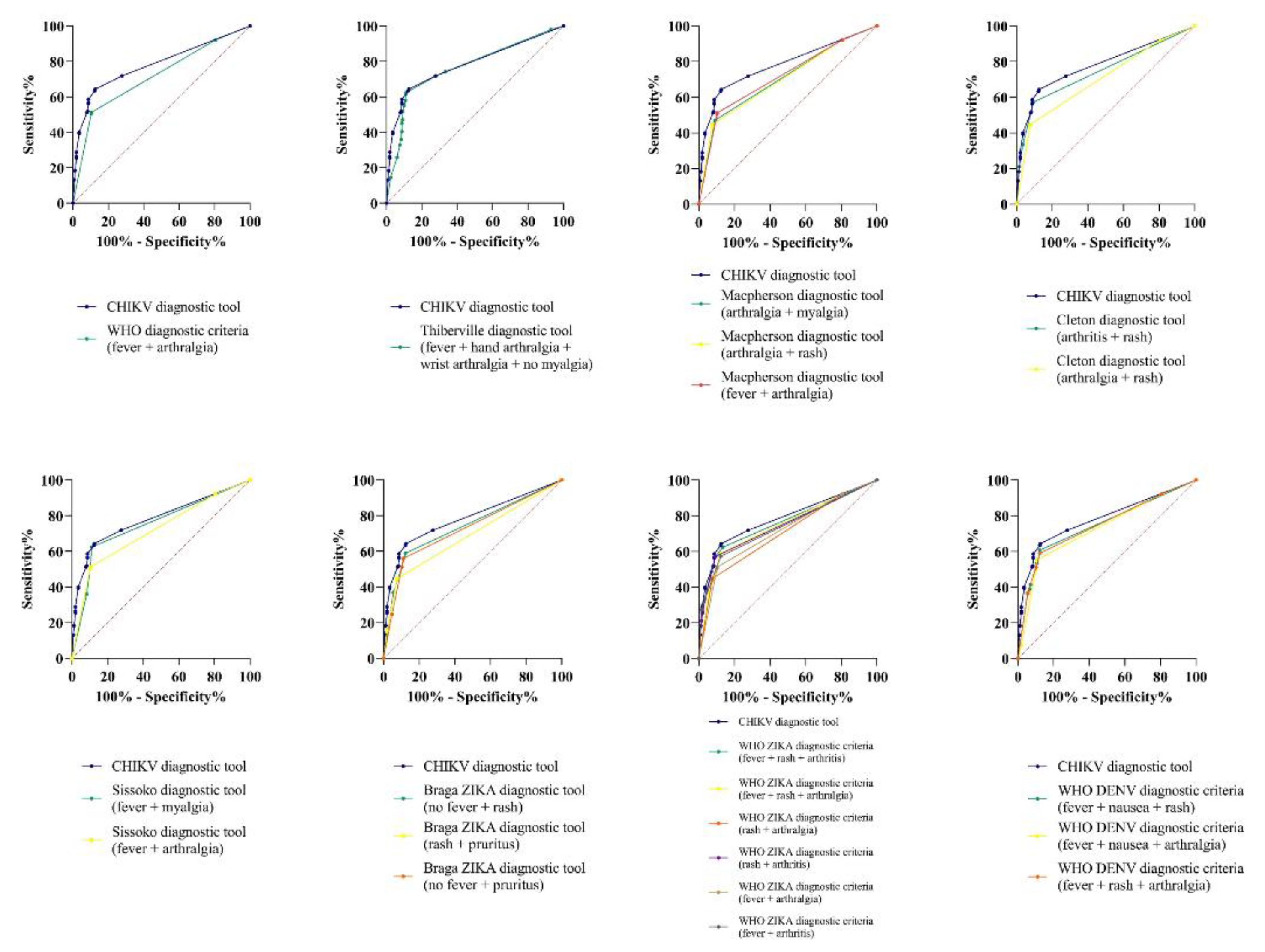
Figure 7.
Proposed algorithm for clinical approach of CHIKV, ZIKAV and DENV. CHIKV: Chikungunya virus; ZIKAV: Zika virus; DENV: Dengue virus.
Figure 7.
Proposed algorithm for clinical approach of CHIKV, ZIKAV and DENV. CHIKV: Chikungunya virus; ZIKAV: Zika virus; DENV: Dengue virus.
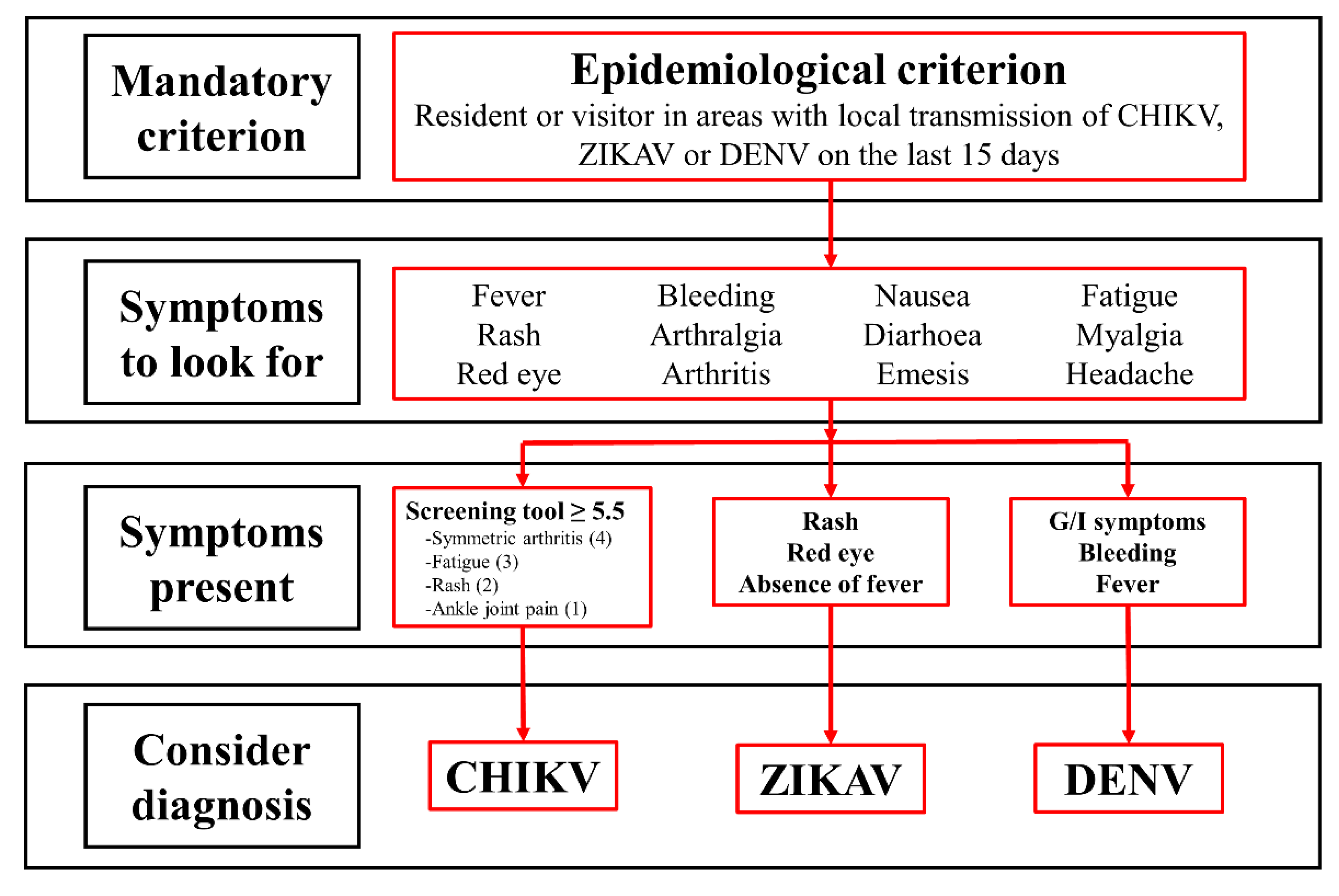

Table 1.
Demographics in patients with suspected CHIKV infection.
|
Positive CHIKV Serology†(n=295) |
Negative CHIKV Serology‡(n=253) |
Total (n=548) |
p value | |
| Age in years (mean ± SD) | 48.3 ± 17.4 | 49.6 ± 17.6 | 48.8 ± 17.5 | |
|
Gender Female Male |
208 (70.5%) 87 (29.5%) |
174 (68.8%) 79 (31.2%) |
382 (69.7%) 166 (30.3%) |
|
|
Age-group in years 18-29 30-39 40-49 50-59 60-69 70-79 ≥80 |
60 (20.3%) 43 (14.6%) 42 (14.2%) 60 (20.3%) 56 (19.0%) 26 (8.8%) 8 (2.7%) |
37 (14.6%) 47 (18.6%) 45 (17.8%) 44 (17.4%) 44 (17.4%) 25 (9.9%) 11 (4.3%) |
97 (17.7%) 90 (16.4%) 87 (15.9%) 104 (19.0%) 100 (18.2%) 51 (9.3%) 19 (3.5%) |
|
|
WHO acute clinical case[31] Fulfil criteria Do not fulfil criteria |
149 (50.5%) 146 (49.5%) |
26 (10.3%) 227 (89.7%) |
175 (31.9%) 373 (68.1%) |
<0.001 <0.001 |
CHIKV: chikungunya virus; †IgM or IgG positive CHIKV serology; ‡IgM or IgG negative CHIKV serology; World Health Organization Criteria for confirmed case of CHIKV; SD: standard deviation
Table 2.
Univariate analysis of clinical features of patients with suspected CHIKV infection.
|
Positive CHIKV Serology† (n=295) |
Negative CHIKV Serology‡ (n=253) |
Total (n=548) |
OR (CI) | p value | |
|
Systemic Fever Myalgia Whole body Extremities Back Fatigue |
151 (85.3%) 139 (85.8%) 40 (95.2%) 96 (82.1%) 22 (84.6%) 173 (85.2%) |
26 (14.7%) 23 (14.2%) 2 (4.8%) 21 (17.9%) 4 (15.4%) 30 (14.8%) |
177 (32.3%) 162 (29.6%) 42 (7.7%) 117 (21.4%) 26 (4.7%) 203 (37.0%) |
9.1 (5.7-14.6) 8.9 (5.5-14.5) 19.7 (4.7-82.3) 5.3 (3.2-8.9) 5.0 (1.7-14.7) 10.5 (6.7-16.5) |
< 0.001 < 0.001 < 0.001 < 0.001 0.001 < 0.001 |
|
Joint Arthralgia Symmetric Hands Wrists Elbows Shoulders Knees Ankles Feet Arthritis Symmetric Hands Wrists Elbows Shoulders Knees Ankles Feet |
270 (57.0%) 240 (62.8%) 158 (68.4%) 93 (67.9%) 74 (66.7%) 81 (56.6%) 184 (62.6%) 137 (74.1%) 104 (67.1%) 99 (91.7%) 90 (93.8%) 47 (95.9%) 19 (95.0%) 11 (91.7%) 9 (100.0%) 22 (88.0%) 47 (94.0%) 45 (97.8%) |
204 (43.0%) 142 (37.2%) 73 (31.6%) 44 (32.1%) 37 (33.3%) 62 (43.4%) 110 (37.4%) 48 (25.9%) 51 (32.9%) 9 (8.3%) 6 (6.3%) 2 (4.1%) 1 (5.0%) 1 (8.3%) 0 (0.0%) 3 (12.0%) 3 (6.0%) 1 (2.2%) |
474 (86.5%) 382 (69.7%) 231 (42.2%) 137 (25.0%) 111 (20.3%) 143 (26.1%) 294 (53.6%) 185 (33.8%) 155 (28.3%) 108 (19.7%) 96 (17.5%) 49 (8.9%) 20 (3.6%) 12 (2.2%) 9 (1.6%) 25 (4.6%) 50 (9.1%) 46 (8.4%) |
2.6 (1.5-4.3) 3.4 (2.3-5.0) 2.8 (1.9-4.0) 2.1 (1.4-3.3) 1.9 (1.3-3.0) 1.2 (0.8-1.7) 2.1 (1.5-3.0) 3.7 (2.5-5.4) 2.2 (1.5-3.2) 13.7 (6.7-27.8) 18.1 (7.8-42.1) 23.8 (5.7-99.0) 17.3 (2.3-130.5) 9.7 (1.2-76.1) 6.7 (2.0-22.7) 15.8 (4.8-51.4) 45.4 (6.2-332.0) |
< 0.001 < 0.001 < 0.001 < 0.001 0.002 0.433 < 0.001 < 0.001 < 0.001 < 0.001 < 0.001 < 0.001 < 0.001 0.008 < 0.001 < 0.001 < 0.001 |
|
Dermatologic Rash Face Thorax Abdomen Back Extremities Pruritus Mucosa Oral Genital |
132 (87.4%) 94 (88.7%) 84 (91.3%) 84 (92.3%) 73 (91.3%) 91 (86.7%) 87 (86.1%) 12 (85.7%) 9 (90.0%) 11 (84.6%) |
19 (12.6%) 12 (11.3%) 8 (8.7%) 7 (7.7%) 7 (8.7%) 14 (13.3%) 14 (13.9%) 2 (14.3%) 1 (10.0%) 2 (15.4%) |
151 (27.6%) 106 (19.3%) 92 (16.8%) 91 (16.6%) 80 (14.6%) 105 (19.2%) 101 (18.4%) 14 (2.6%) 10 (1.8%) 13 (2.4%) |
9.9 (6.0-16.8) 9.4 (5.0-17.6) 12.2 (5.8-25.6) 14.0 (6.3-31.0) 11.5 (5.2-25.6) 7.6 (4.2-13.7) 7.1 (3.9-13.0) 5.3 (1.2-24.0) 7.9 (1.0-63.0) 4.9 (1.1-22.1) |
< 0.001 < 0.001 < 0.001 < 0.001 < 0.001 < 0.001 < 0.001 0.015 0.021 0.024 |
|
Gastrointestinal Diarrhoea Emesis Nausea Abdominal pain |
75 (83.3%) 33 (82.5%) 34 (85.0%) 23 (76.7%) |
15 (16.7%) 7 (17.5%) 6 (15.0%) 7 (23.3%) |
90 (16.4%) 40 (7.3%) 40 (7.3%) 30 (5.5%) |
5.4 (3.0-9.6) 4.4 (1.9-10.1) 5.6 (2.2-13.0) 3.0 (1.2-7.0) |
< 0.001 < 0.001 < 0.001 0.010 |
CHIKV: chikungunya virus; †IgM or IgG positive CHIKV serology; ‡IgM or IgG negative CHIKV serology; OR: odds ratio; CI: 95% confidence interval
Table 3.
Agreement percentage to formulated questions on CHIKV clinical characteristics.
| Do you consider as clinical criteria? | Totally Agree | Agree | Not Agree or Disagree | Disagree | Totally Disagree | Type of Agreement (Total) |
|---|---|---|---|---|---|---|
| Symmetrical joint involvement | 100 | 0 | 0 | 0 | 0 | Agree (100) |
| Abrupt onset of symptoms | 100 | 0 | 0 | 0 | 0 | Agree (100) |
| Fever | 38 | 50 | 12 | 0 | 0 | Agree (78) |
| Rash | 13 | 75 | 0 | 12 | 0 | Agree (88) |
| Mucosal involvement | 0 | 0 | 0 | 63 | 37 | Disagree (100) |
| Myalgia | 25 | 75 | 0 | 0 | 0 | Agree (100) |
| Fatigue | 63 | 25 | 12 | 0 | 0 | Agree (88) |
| Gastrointestinal involvement | 0 | 12 | 0 | 25 | 63 | Disagree (88) |
| Shoulder arthralgia | 0 | 25 | 12 | 38 | 25 | Disagree (63) |
| Shoulder arthritis | 0 | 0 | 0 | 38 | 62 | Disagree (100) |
| Elbow arthralgia | 0 | 0 | 0 | 88 | 12 | Disagree (100) |
| Elbow arthritis | 0 | 0 | 0 | 25 | 75 | Disagree (100) |
| Wrist arthralgia | 50 | 25 | 13 | 0 | 12 | Agree (75) |
| Wrist arthritis | 75 | 13 | 0 | 12 | 0 | Agree (88) |
| Hand arthralgia | 88 | 12 | 0 | 0 | 0 | Agree (100) |
| Hand arthritis | 88 | 12 | 0 | 0 | 0 | Agree (100) |
| Knee arthralgia | 13 | 63 | 0 | 12 | 12 | Agree (76) |
| Knee arthritis | 13 | 63 | 12 | 0 | 12 | Agree (76) |
| Ankle arthralgia | 100 | 0 | 0 | 0 | 0 | Agree (100) |
| Ankle arthritis | 100 | 0 | 0 | 0 | 0 | Agree (100) |
| Foot arthralgia | 50 | 38 | 0 | 12 | 0 | Agree (88) |
| Foot arthritis | 75 | 13 | 0 | 12 | 0 | Agree (88) |
CHIKV: chikungunya virus.
Table 4.
Multivariate analysis of predictors of CHIKV infection.
| Odds ratio | 95% Confidence interval | p value | Point value | |
| Symmetric arthritis | 4.75 | 1.88-11.98 | 0.001 | 4 |
| Fatigue | 3.47 | 1.91-6.32 | < 0.001 | 3 |
| Rash | 2.70 | 1.37-5.31 | 0.004 | 2 |
| Ankle joint pain | 1.69 | 1.06-2.68 | 0.026 | 1 |
CHIKV: chikungunya virus.
Table 5.
Performance of different diagnostic tools in our confirmed CHIKV infected patients.
| Sensitivity % (CI) |
Specificity % (CI) |
PPV % (CI) |
NPV % (CI) |
AUC (CI) |
Accuracy % (CI) |
YI % |
|
|---|---|---|---|---|---|---|---|
| Proposed screening tool (Score ≥ 5.5) | 64.4 (58.5-69.8) |
87.3 (82.6-91.1) |
85.5 (80.9-89.2) |
67.7 (64.1-71.1) |
0.72 (0.67-0.76) |
75.0 (71.1-78.5) |
52 |
|
CHIKV WHO case definition (2015) Fever + arthralgia |
51.2 (45.3-57.0) |
85.3 (85.3-93.1) |
85.3 (79.9-89.5) |
61.2 (58.2-64.1) |
0.71 (0.67-0.75) |
68.9 (64.9-72.8) |
36 |
|
Sissoko (2010) Fever + arthralgia Fever + myalgia |
51.2 (45.3-57.0) 62.3 (56.5-67.9) |
85.3 (85.3-93.1) 88.9 (84.4-92.5) |
85.3 (79.9-89.5) 86.7 (82.1-90.4) |
61.2 (58.2-64.1) 66.9 (63.4-70.2) |
0.71 (0.67-0.75) 0.75 (0.71-0.79) |
68.9 (64.9-72.8) 74.6 (70.7-78.2) |
36 51 |
|
Thiberville (2013) Fever + arthralgia hands + arthralgia wrists + no myalgia |
62.3 (56.5-67.9) |
88.9 (84.4-92.5) |
86.7 (82.1-90.4) |
66.9 (63.4-70.2) |
0.76 (0.72-0.81) |
74.6 (70.7-78.2) |
51 |
|
Cleton syndromic approach (2015) Arthritis + rash |
57.2 (51.4-63.0) |
90.5 (86.2-93.8) |
87.5 (82.6-91.2) |
64.5 (61.2-67.6) |
0.74 (0.70-0.78) |
72.6 (68.6-76.3) |
48 |
|
Macpherson (2016) Arthralgia + myalgia Arthralgia + rash Arthralgia + fever |
47.1 (41.3-52.9) 44.7 (38.9-50.6) 51.2 (45.3-57.0 |
90.9 (86.6-94.1) 92.4 (88.5-95.4) 85.3 (85.3-93.1) |
85.8 (80.1-90.1) 87.4 (81.5-91.6) 85.3 (79.9-89.5) |
59.6 (56.8-62.3) 58.9 (56.2-61.5) 61.2 (58.2-64.1) |
0.71 (0.66-0.74) 0.70 (0.66-0.74) 0.71 (0.67-0.75) |
67.3 (63.2-71.2) 66.7 (62.6-70.7) 68.9 (64.9-72.8) |
38 38 36 |
|
ZIKAV WHO case definition (2016) Rash + fever + arthralgia Rash + fever + arthritis Rash + arthralgia Rash + arthritis Fever + arthralgia Fever + arthritis |
58.8 (53.1-64.6) 62.3 (56.5-67.9) 44.7 (38.9-50.6) 57.2 (51.4-63.0) 51.2 (45.3-57.0 57.2 (51.4-63.0) |
87.7 (83.1-91.5 86.5 (81.7-90.5) 92.4 (88.5-95.4) 90.5 (86.2-93.8) 85.3 (85.3-93.1) 87.7 (83.1-91.5) |
84.8 (79.9-88.7) 84.4 (79.6-88.2) 87.4 (81.5-91.6) 87.5 (82.6-91.2) 85.3 (79.9-89.5) 84.5 (79.4-88.4) |
64.7 (61.3-67.9) 66.3 (62.8-69.7) 58.9 (56.2-61.5) 64.5 (61.2-67.6) 61.2 (58.2-64.1) 63.7 (60.5-66.9) |
0.74 (0.70-0.78) 0.76 (0.72-0.80) 0.70 (0.66-0.74) 0.74 (0.70-0.78) 0.71 (0.67-0.75) 0.73 (0.69-0.77) |
72.2 (68.3-75.9) 73.5 (69.6-77.1) 66.7 (62.6-70.7) 72.6 (68.6-76.3) 68.9 (64.9-72.8) 71.3 (67.3-75.1) |
46 49 38 48 36 45 |
|
Braga ZIKAV (2017) No fever + rash Rash + pruritus No fever + pruritus |
58.9 (53.1-64.6) 44.7 (38.9-50.6) 55.9 (50.0-61.6) |
87.7 (83.1-91.5) 92.4 (88.5-95.4) 88.9 (84.4-92.5) |
84.8 (79.9-88.7) 87.4 (81.5-91.6) 85.4 (80.3-89.4) |
64.7 (61.3-67.9) 58.9 (56.2-61.5) 63.3 (60.1-66.4) |
0.74 (0.69-0.78) 0.68 (0.64-0.73) 0.72 (0.68-0.76) |
72.2 (68.3-75.9) 66.7 (62.6-70.7) 71.1 (67.1-74.9) |
47 37 45 |
|
DENV WHO case definition (2009) Fever + nausea + rash Fever + nausea + arthralgia Fever + rash + arthralgia |
60.7 (54.8-66.2) 55.2 (49.3-61.0) 58.8 (53.1-64.6) |
87.7 (83.1-91.5) 89.3 (84.8-92.8) 87.7 (83.1-91.5) |
85.2 (80.3-89.0) 85.7 (80.6-89.7) 84.8 (79.9-88.7) |
65.6 (62.2-68.9) 63.1 (59.9-66.1) 64.7 (61.3-67.9) |
0.74 (0.70-0.78) 0.72 (0.68-0.77) 0.74 (0.70-0.78) |
73.1 (69.2-76.8) 70.9 (66.9-74.7) 72.2 (68.3-75.9) |
48 45 46 |
CHIKV: chikungunya virus; CI: 95% confidence interval; PPV: positive predictive value; NPV: negative predictive value; LRP: positive test likelihood ratio; LRN: negative test likelihood ratio; AUC: area under the curve; YI: Youden´s index (Sensitivity + sensibility – 100); WHO: World Health Organization; ZIKV: zika virus; DENV: dengue virus.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



