Submitted:
05 March 2023
Posted:
06 March 2023
You are already at the latest version
Abstract
This study was to determine the prevalence of hepatitis C virus (HCV) among febrile patients attending a General Hospital in Emohua LGA, Rivers State, Nigeria. Eighty-nine patients, including 31 males and 58 females, aged 2 to 60 years, were recruited for this study. Blood samples were screened for antibodies to hepatitis C virus (HCV) using a commercially available anti-HCV-Ab enzyme-linked immunosorbent assay (ELISA) based kits following the manufacturer's description. The results showed an overall prevalence of 5.6%. Higher prevalence of HCV was observed among females (6.9%), age groups >41 years (11.1%), singles (7.9%) and patients with primary education (33.3%). Among all the variables evaluated, only education (p = 0.007) was significantly associated with the prevalence of HCV. Age (p = 0.21), sex (p = 0.47) and marital status (p = 0.42) were not associated with the prevalence of HCV among the studied population. This study showed a prevalence rate (5.6%) that is slightly alarmingly well above several other studies done in the past in Nigeria. The seropositivity of HCV among febrile patients remains a great danger to public health. Therefore, HCV screening by ELISA methods in all patients is recommended. Planned prevention, screening and treatment are needed to reduce further transmission.
Keywords:
Antibodies
; HCV
; Prevalence
; Febrile Patients
; Nigeria
1. Introduction
Viruses are the most common cause of hepatitis, which is an inflammation of the liver (CDC, 2019, 2020, 2022). Hepatitis A, B, and C are the three most prevalent viral hepatitis. While certain hepatitis viruses can cause similar symptoms, each one affects the liver differently, infects people differently, and affects typically distinct populations (CDC, 2019, 2020, 2022).
The RNA virus known as the hepatitis C virus (HCV) is a member of the Flavivirus family. It primarily spreads through parental contact, though it can also be acquired vertically or through sexual contact (CDC, 1998; Abeni et al., 2020). Compared to the human immunodeficiency virus, HCV is more contagious and requires less contact to infect a person (Te & Jensen, 2001). Because it persists in about 85% of infected people, HCV infection is clinically significant because it presents a serious risk of chronic liver damage (Omolade & Adeyemi, 2018). The Hepatitis C virus, unlike the hepatitis B virus, cannot be prevented by vaccination, although it is treatable (Kesson, 2002; Ernest Nwagwu, 2021).
Injection drug use (IDU) is the leading risk factor for infection and the most effective method of hepatitis C virus (HCV) transmission (CDC, 2019; Abeni et al., 2020). Rates of HCV infection nearly doubled among women who gave birth to live children between 2009 and 2014 as the number of new HCV infections among individuals of reproductive age (Patrick et al., 2017). Mothers with hepatitis C delivered 0.38% of live babies in 2015 (Schillie et al., 2018, 2020). This report updates and augments earlier CDC recommendations for adult hepatitis C testing in the United States, released in 1998 and 2012 (CDC, 1998; Smith et al., 2012).
Hepatitis C infection is estimated to affect between 2.6% and 3.1% of the world's population. However, a precise global estimate is impossible due to the high number of undiagnosed patients and improper data collection (Syed-Mohammed & Stuart, 2018). Hepatitis C infection rates differ from area to region and even across communities within a nation. Local differences in each area, such as the culture and habits of the local population and the predominance of hazardous behaviours, may cause a disparity in HCV prevalence. The World Health Organization reported hepatitis C virus prevalence as follows: Africa 5.3%, America 1.7%, and South-East Asia. 2.15%, Western Pacific 3.9%, Europe 1.03%, and the Eastern Mediterranean 4.6% (Karoney & Siika, 2013; Ernest Nwagwu, 2021).
HCV endemicity in Nigeria has long been established, although epidemiological data are scarce (Riou et al., 2016). Nigeria has a sizable population with a wide range of seroprevalence for HCV infection. Nigeria's prevalence rate ranges from 0.4% to 18.3%, or 1 to 30 million people, and the Federal Ministry of Health claims a prevalence of 2.2%, or 4 million Nigerians, who have the hepatitis C virus (Riou et al., 2016; Ernest Nwagwu, 2021).
Thankfully, hepatitis A and B may both be prevented with reliable immunizations. Hepatitis C has no vaccine but can be cured with life-saving medicine (CDC, 2019, 2020, 2022). It poses a substantial risk to public health, claims thousands of lives each year, and is a significant factor in liver cancer (CDC, 2019, 2020, 2022). Unfortunately, there is a lack of data regarding the incidence of the hepatitis C virus in Nigerian patients who visit public healthcare facilities. Hepatitis C prevalence in Nigeria has not been surveyed; however, studies indicate that it fluctuates between 0.4% and 14.7%, depending on the population segment being considered (Adesina et al., 2016). The study aims to determine the prevalence of HCV antibodies among patients attending a General Hospital in Emohua LGA, Rivers State, Nigeria.
2. Materials and Methods
2.1. Study Area
The study area was the General Hospital, Ogbakiri, in Emohua LGA, Rivers State, Nigeria. A small communal settlement of the Ikwere-speaking tribe of Rivers State with vast land covering almost the area, the people are known to be hunters, traders and other business activities done in its peaceful environment.
2.2. Study Design
This hospital-based cross-sectional study involves patients at the General Hospital, Ogbakiri, in Emohua Local Government Area, Rivers State, Nigeria.
2.3. Study Population
The targeted population constituted all patients who were at the hospital to receive medical care. A total of 89 blood samples were collected from patients who were included in the study.
2.4. Inclusion and Exclusion Criteria
The patients included in this study comprised patients who were at the General Hospital, Ogbakiri, in Emohua LGA, Rivers State, Nigeria and in which they gave their consent to participate in the study. Patients who gave no consent were excluded from this study.
2.5. Sample Collection, Transport, Preparation & Storage
From the study population, 89 blood samples were collected from the patients. Four millilitres (4 ml) of blood samples were aseptically collected from each patient into sterile EDTA tubes. The collected blood sample was carefully transported with an ice pack to the Virus & Genomics Research Unit of the Department of Microbiology, University of Port Harcourt. In the laboratory, the blood samples were centrifuged, after which serum samples were collected using a micropipette. After collection, the plasma was stored at -200C till it was ready for use.
2.6. Serological Analysis
Plasma samples were analyzed for HCV antibodies using the ELISA kit manufactured by Dia. Pro. Diagnostic Bioprobes, Milano, Italy. The analysis was performed according to the manufacturer’s instructions. Results were interpreted according to the manufacturer’s guide. The values obtained were used to interpret the results as the ratio of the sample OD450nm and the cut-off value according to the following: S/CO<0.9 as negative, 0.9-1.1 as equivocal and >1.1 as positive.
2.7. Data analysis
Data were analyzed using Microsoft Excel version 16.0 (Microsoft, USA). Statistical significance for all analyses was determined at a 5% significance level.
3. Results And discussion
3.1. Patients Characteristics
In this study, 89 (100%) patients were tested for HCV antibodies; their age range was between 2 years and above. The samples were that of patients in the hospital for a routine check. A total of 89 patients were sampled in this study, with their socio-demographic data stratified in Table 1.
3.2. Overall Prevalence of HCV Antibody
Of 89 patients who participated in the study, 5(5.6%) tested positive, while 84(94.4) were negative. This result, however, indicates the seroprevalence of HCV Ab, as in Figure 1.
3.3. Prevalence of HCV with Age
This study indicates that the prevalence of HCV is higher within the age range of >41(11.1%) than in other age groups, 21-40 (5.7%) and 2-20 years (0.0%). Nevertheless, there was no significant relationship between age (p = 0.21) and HCV antibody, as shown in Figure 2.
3.4. Prevalence of HCV with Sex
Figure 3 shows the prevalence of HCV Ab with sex. A higher prevalence occurred in females (6.9%) than in males (3.2%). There was no relationship between sex (p = 0.47) and the prevalence of HCV Ab.
3.5. Prevalence of HCV with Marital Status
From the result obtained, the percentage of positive individuals concerning their marital status shows 7.9% for married and 3.9% for singles (Figure 4). However, there was no relationship between marital status (p = 0.42) and the prevalence of HCV.
3.6. Prevalence of HCV with Educational Status
The study indicates a higher prevalence of HCV among primary school education (33.3%) than secondary education (11.8%) and those without formal education (1.8%).
Those with university education had zero prevalence (0.0%), as shown in (Figure 5). There was a significant relationship between educational status (p = 0.007) and the prevalence of HCV.
4. Discussion
The prevalence rate of 5.6% obtained from this study is comparable to the prevalence rate of 5.20% that was reported in Ghana (Acquaye & Tettey-Donkor, 2000). It is also comparable to the 5.70% reported in Jos, Nigeria (Inyama et al., 2005), the 5.0% reported in Port Harcourt, Nigeria (Abeni et al., 2020) and the 6.1% and 6.0% reported by Dammulak et al. (2013) in Jos and Buseri et al. (2009) in Osogbo, respectively.
The 5.6% revealed in this study is also more significant than the results of other earlier investigations conducted in Nigeria and elsewhere outside Nigeria. It exceeds the global prevalence of 3.0% (WHO, 1999), the 2.3% and 3.86% found in Abuja (Tremeau-Bravard et al., 2012; Anyanwu et al., 2020), the 3.3% in Lagos State (Akinbami et al., 2010), the 4.50% in Benin (Nwannadi et al., 2012), and the 1.6% in North-Western Nigeria (Hamza et al., 2013). The 2.9% previously reported in Rivers State (Koate et al., 2005), the 3.0%, 3.4%, and 4.1% reported by Ejele et al. (2006) in the Niger Delta region, Kano State (Bala et al., 2012), and Benin City, Edo State are all greater than the 4.1% described in this paper (Nwannadi et al., 2014) and the 4.8% obtained by Halim and Ajayi (2000). When compared to other African nations, it was also greater than the 3.2% and 4.4% results found in Kenya and Ghana by Kamande et al. (2016) and Walana et al. (2014), respectively; the 4.7% in Southern Taiwan (Tsai et al., 2015); and the 1.6% in Senegal, West Africa (Diop-Ndiaye et al., 2008).
This value is in contrast to studies by Okonko et al. (2014), Cookey et al. (2021), Opaleye et al. (2016), who reported a 0.0% prevalence rate of HCV antibodies in southwestern Nigeria, and Alli et al. (2010), who similarly reported a 0.0% HCV seroprevalence rate in Ibadan, Oyo State, Nigeria. There have also been reports of other exceedingly low incidence rates in Nigeria. 1.0% was recorded by Aaron et al. in Port Harcourt, Nigeria, in 2021. Ikeako et al. (2014) observed 0.16% prevalence in the south-east of Nigeria, 0.5% in Anyigba, 0.7% in the south-east (Diwe et al., 2013), 0.8% in Abuja (Agboghoroma & Ukaire, 2020), and 0.8% and 0.9% reported by Oluremi et al. (2021) and Onyekwere and Hameed (2015), respectively.
This number is less than the 22.5% found in a recent study conducted in Port Harcourt, Nigeria (Okonko et al., 2022), the 15.0% found in Ughelli, Delta State, Nigeria (Ogbodo et al., 2015), and the 8.0% and 12.30% found in Port-Harcourt and Benin, respectively (Nwannadi et al., 2012). The figures reported by Ayolabi et al. (2006) in Lagos, Ebie and Pela (2006) in Enugu, Nigeria, and Strickland (2002) in Kaduna, Nigeria, respectively, were 8.4%, 14.9%, and 11.9% lower. Also, it is lower than the 14.7% obtained in other parts of South Western Nigeria (Balogun et al., 2012), the 23.5% reported in Abeokuta, Ogun State, Nigeria (Ogwu-Richard et al., 2015), the 7.0% reported in Benin City (Ojide et al., 2015), and the 10.0% in Kenya, East Africa (Muriuki et al., 2013), the 13.4% in South Africa (Parboosing et al., 2008) and the 18.1% in another Eastern Africa state, Tanzania (Nagu et al., 2008).
Past research has found variable prevalence rates of HCV in various population segments in Nigeria and certain African and Middle Eastern nations (Jeremiah et al., 2008). Low HCV prevalence rates were noted in various studies conducted in Kano, Nigeria (0.40%), Namibia (0.90%), Sudan (1.90%), Senegal (0.80%), and Ghana (0.90%), which are comparable to the prevalence of 0.40% observed in the study by Jeremiah et al. (2008). (Jeremiah et al., 2008; Imoru et al., 2003). Natalie et al. (2011) in Burkina Faso and Frank et al. (2013) in Egypt reported prevalence rates of 8.6% and 20.0%, respectively. The discrepancy in prevalence can be caused by variations in the social behaviours of the study participants and the populations of the separate studies (Ayele et al., 2002).
Age-specific prevalence was found to be higher in those above the age of 41 (11.1%) than in those between the ages of 21 and 40 (5.7%) and 20 years (0.0%), but there was no correlation between age and HCV antibodies (p > 0.05). Comparing this to the findings of our previous study in Port Harcourt, Nigeria (Okonko et al., 2022) shows that the prevalence was greater in the age group of 31 to 40 years. That contradicts the findings of Jeremiah et al. (2008), who found that anti-HCV prevalence was highest in age groups between 21 and 30. According to Tessema et al. (2010), in a study that included patients aged 41 to 50, the condition was more prevalent; this conclusion is consistent with ours. These most recent findings were consistent with our earlier research in Ibadan, Nigeria (Okonko et al., 2012), which found a higher frequency in people over 40. This observation, however, differs from studies we conducted in Port Harcourt (Abeni et al., 2020) and Ugheli, Delta State, Nigeria (Ogbodo et al., 2015), which found greater prevalences in the age group >26 years.
As individuals get older, their seroprevalence of HCV rises, and it is significantly greater in the age group over 41. This observation matches Klevens et al. (2009)'s findings, which agree with the findings of this study. The outcome is also consistent with other data points from throughout the globe, demonstrating that ageing increases a person's risk of contracting HCV (Nagu et al., 2008; Spradling et al., 2010; Ogbodo et al., 2015). The increased seropositivity shown in the elderly age group may be due to social behaviours that are different, parenteral exposures, a loss in physical mobility, and a lower incidence of medical examinations when compared to younger people, which increases the likelihood of infection transmission (Lee et al., 2011).
Females (6.9%) had a higher prevalence than males (3.2%). No association between sex and the prevalence of HCV Ab was found (p > 0.05). This finding is consistent with research from Jemilohun et al. (2014) and our recent study in Port Harcourt, Nigeria, which found a somewhat greater frequency among females than males. Our findings concur with those of a prior investigation conducted in the Nigerian regions of Ilorin, Kwara State, and the Niger Delta, all showing a greater prevalence of HCV among the female participants (Udeze et al., 2011; Ogbodo et al., 2015). This observation is also consistent with earlier research in Nigeria (Lesi et al., 2007; Balogun et al., 2012). This finding may be explained by the fact that absent additional means of HCV transmission, females are more likely to become infected through unprotected sex than males are (Tohme, 2010; Ogbodo et al., 2015).
The greater frequency was observed among males in Jos, Plateau State, Nigeria (Egah et al., 2004), in Osogbo, Osun State, Nigeria (Buseri et al., 2009), Ibadan, Oyo State, Nigeria (Udeze et al., 2009; Okonko et al., 2012), and Port Harcourt, Rivers State, Nigeria (Udeze et al., 2009; Okonk (Abeni et al., 2020). Due to the generally low disease frequency in the research population, and the difference is not statistically significant, it is challenging to identify a specific cause for the somewhat higher female preponderance. Other research from other parts of Nigeria has verified this demographic tendency (Kassim et al., 2012; Okocha et al., 2015; Okoroiwu et al., 2018; Abeni et al., 2020).
According to our study, unmarried people (7.9%) had a greater prevalence of HCV than married people (3.9%). The prevalence of HCV Ab and marital status were not related (p > 0.05). This outcome supports our earlier investigation in Port Harcourt, Nigeria (Okonko et al., 2022). When compared to the study of Ejele et al. (2006), where they discovered a higher incidence among single respondents (4.1%) than married ones (2.2%), this observation was marginally higher. Compared to Obienu et al. (2011), this study indicated a substantially lower prevalence in connection to marital status; the prevalence of the viral infection in married people was 27.2%, and it was 21.3% in singles. Our results were in line with those of Abeni et al. (2020), who found that unmarried participants had a considerably greater prevalence (6.0%) than married participants (3.0%). This finding is consistent with a 2013 study by Afolabi et al. in Ibadan, which likewise found a greater prevalence of HCV in the unmarried population. The fact that there was a significant frequency in the general population despite the absence of any apparent risk factors may not be unrelated. Another factor might be that single people are more likely to engage in illegal activities, which increases their chance of getting HCV and other diseases (Abeni et al., 2020). As the unmarried participants could not have been more sexually active than the married participants, sexual transmission as a risk factor was not raised in this area. Furthermore, repeated or extensive direct percutaneous exposure to blood is the most effective way for the virus to spread.
The prevalence of HCV Ab was significantly correlated with education (p <0.05). According to the study, elementary school students (33.3%) have a higher prevalence of HCV than students in secondary education (11.8%) or those with no formal education (1.8%). The incidence among university students was zero (0.0%). This observation runs counter to a recent study by Okonko et al. (2022) that found a higher frequency among patients with tertiary education and a study by Onyekwere et al. (2016) that found a higher prevalence among people with no formal education. The numbers here also differ from what they found in their survey, where the prevalence of those without formal education was 4.0%, and those with elementary education was 1.8%. Those with secondary education were 0%.
5. Conclusion
The study shows a low prevalence of HCV (5.6%) among febrile patients presenting at a General Hospital in Emohua LGA, Rivers State, Nigeria. In general, the study found low prevalence in the socio-demographic data collected; therefore, this could be due to some variables, including a lack of awareness and low or absent medical checkups. A larger-scale study that includes rural residents and urban distribution is required to assess the disease burden.
Compliance with ethical standards
Acknowledgements
The authors would like to acknowledge the support obtained from Mrs Mercy Elenwo, the management and staff of General Hospital, Ogbakiri, Emohua LGA, Rivers State, Nigeria during the enrollment and collection of samples used in this study. The authors are grateful to the participants for their willingness to be part of the study.
Disclosure of conflict of interest
The authors have declared that no competing interests exist.
Statement of ethical approval
All authors declare that all experiments have been examined and approved by the University of Port Harcourt Research Ethics committee. Therefore, the study is performed following the ethical standards laid down in the 1964 Declaration of Helsinki.
Statement of informed consent
“All authors declare that informed consent was obtained from all individual participants included in the study.”
References
- Aaron, U. U., Okonko, I. O. & Frank-Peterside, N. (2021). The Prevalence of Hepatitis E, Hepatitis C and Hepatitis B Surface Antigenemia in HAART Experienced People Living with Human Immunodeficiency Virus (HIV) in Rivers State, Nigeria. Journal of Biomedical Sciences 10(S4):001.
- Abeni, B.A., Frank-Peterside, N., Agbagwa, O.E., Adewuyi, S.A., Cookey, T.I. & Okonko, I.O. (2020). Seropositivity of Hepatitis C Virus Among Intending Blood Donors in Rivers State, Nigeria. Asian Journal of Research and Reports in Gastroenterology 3(3): 24-31.
- Acquaye, J. K. & Tettey-Donkor, D. (2000). frequency of hepatitis C virus antibodies and elevated serum alanine transaminase levels in Ghanaian blood donors. West Africa Journal Medical, 19 (4), 239–241.
- Adesina OA, Akinyemi JO, Ogunbosi BO, Michael OS, Awolude OA, & Adewole IF (2016). Seroprevalence and factors associated with hepatitis C coinfection among HIV-positive pregnant women at the University College Hospital, Ibadan, Nigeria. Tropical Journal of Obstetrics & Gynaecology, 33, 153-158. [CrossRef]
- Afolabi AY, Abraham A, Oladipo EK, Adefolarin AO, Fagbami AH. Transfusion transmissible viral infections among potential blood donors in Ibadan, Nigeria. African Journal of Clinical and Experimental Microbiology. 2013;14(2):84-87. [CrossRef]
- Agboghoroma CO, Ukaire BC. Prevalence and Risk Factors of Human Immunodeficiency Virus and Hepatitis C Virus Infection among Pregnant Women Attending Antenatal Care at a Tertiary Hospital in Abuja, Nigeria. Nigerian Medical Journal. 2020;61(5):245-251. [CrossRef]
- Akinbami AA, Oshinaike OO, Adeyemo TA, Adediran A, Oshikomaiya BI, Ismail KA. Seroprevalence of hepatitis C infection in HIV patients using a rapid one-step test strip kit. Nigerian Quarterly Journal of Hospital Medicine. 2010;20(3):144-146.
- Alli JA, Okonko IO, Abraham OA, Kolade AF, Ogunjobi PI, Tonade OO, et al. A serosurvey of blood parasites (Plasmodium, Microfilaria, HIV, HBsAg, HCV antibodies) in prospective Nigerian blood donors. Research Journal in Medical Sciences. 2010;4(4):255-275. [CrossRef]
- Anyanwu CJN, Sunmonu PT, Mathew MH. Viral hepatitis B and C coinfection with Human Immunodeficiency Virus among adult patients attending selected highly active anti-retroviral therapy clinics in Nigeria's capital. Journal of Immunoassay and Immunochemistry. 2020;41(2):171-183. [CrossRef]
- Ayele, W., D. J. Nokes, A. Abebe, T. Messele, A. Dejene, F. Enquselassie, T. F. Rinke de Wit, and A. L. Fontanet. Higher prevalence of anti-HCV antibodies among HIV-positive compared to HIV-negative inhabitants of Addis Ababa, Ethiopia. J. Med. Virol., 2002; 68: 12-17. [CrossRef]
- Ayolabi CL, Taiwo MA, Omilabu SA, Abebisi AO, Fatoba OM. Sero-prevalence of hepatitis C virus among donors in Lagos, Nigeria. African Journal of Biotechnology. 2006;5:1944-6.
- Bala JA, Kawo AH, Muktar MD, Sarki A, Magaji N, Aliyu IA. Prevalence of hepatitis C infection among blood donors in some selected hospitals in Kano, Nigeria. International Resource Journal of Microbiology. 2012;3:21722.
- Balogun, T. M., S. Emmanuel, and E. F. Ojerinde. HIV, Hepatitis B and C viruses’ coinfection among patients in a Nigerian tertiary hospital. Pan Afr. Med. J., 2012; 12.
- Buseri FI, Muhibi MA, Jeremiah JA. Seroepidemiology of transfusion-transmissible infectious diseases among blood donors in Osogbo, South-West Nigeria. Blood Transfusion. 2009;7(4):293-299. [CrossRef]
- Center for Disease Control & Prevention. (CDC, 2019). Viral hepatitis surveillance report—United States, 2017. Atlanta, GA: US Department of Health and Human Service. https://www.cdc.gov/hepatitis/statistics/2017surveillance/index.htm. Published November 2019. Accessed 03 March 2023.
- Centers for Disease Control and Prevention. 2019 Viral Hepatitis Surveillance Report.
- https://www.cdc.gov/hepatitis/statistics/SurveillanceRpts.htm. Published July 2021. Accessed 03 March 2023.
- Centers for Disease Control and Prevention. Viral Hepatitis Surveillance Report – United States, 2020. https://www.cdc.gov/hepatitis/statistics/2020surveillance/index.htm. Published September 2022. Accessed 03 March 2023.
- Center for Disease Control & Prevention. (CDC, 1998). Recommendations for Prevention and Control of Hepatitis C Virus (HCV) Infection and HCV-Related Chronic Disease. Mortality and Morbidity Weekly Reports, Recommendations and Reports, 47(RR19): 1-39.
- Cookey, T. I., Okonko, I. O. & Frank-Peterside, N. (2021). Zero Prevalence of HIV and HCV Coinfection in the Highly HIV-infected Population of Rivers State, Nigeria. Asian Journal of Research in Medical and Pharmaceutical Sciences, 10(3): 9-16. [CrossRef]
- Dammulak OD, Pina TO, Joseph DE, Ogbenna AA, Kut SD, Godit P. Hepatitis C virus antibody among blood donors: the experience in a Nigerian blood transfusion centre. Global Advance Resource Journal of Medical Science. 2013;2:108–13.
- Diop-Ndiaye, H., C. Toure-Kane, J. F. Etard, G. Lo, P. Diaw, N. F. Ngom-Gueye, P. M. Gueye, K. Ba-Fall, I. Ndiaye, P. S. Sow, E. Delaporte, and S. Mboup. Hepatitis B, C seroprevalence and delta viruses in HIV-1 Senegalese patients at HAART initiation (retrospective study). J. Med. Virol., 2008; 80: 1332-1336. [CrossRef]
- Diwe CK, Okwara EC, Enwere OO, Azike JE, Nwaimo NC. Sero-prevalence of hepatitis B virus and hepatitis C virus among HIV patients in a suburban University Teaching Hospital in South-East Nigeria. Pan African Medical Journal. 2013;16:7. [CrossRef]
- Ebie JC, Pela OA. Some sociocultural aspects of the problem of drug abuse in Nigeria. Drug and Alc. Dep. 2006;8:301-306. [CrossRef]
- Egah DZ, Mandong BM, Iya D, Gomwalk NE, Audu ES, Banwat EB, Onile BA. Hepatitis C virus antibodies among blood donors in Jos, Nigeria. Annals of African Medicine. 2004;3(1):35-37.
- Ejele OA, Erhabor O, Nwanche CA. The risk of acquired hepatitis C virus infection among blood donors in Port Harcourt: The question of blood safety in Nigeria. Nigeria Journal of Clinical Practices. 2006;9:18–21.
- Ejele, O. A., Nwauche, C. A., & Erhabor, O. (2006). Seroprevalence of hepatitis C virus in the Niger Delta of Nigeria. The Nigerian postgraduate medical journal, 13(2), 103-106. [CrossRef]
- Ernest Nwagwu, H. C. (2021). Prevalence of Hepatitis C Virus among Febrile Patients Attending a General Hospital in Emohua LGA, Rivers State, Nigeria. A Postgraduate Diploma Project in the Department of Microbiology, University of Port Harcourt, Port Harcourt, Nigeria.
- Frank J, Hassan Y, Grassucci RA. Hepatitis C virus-like internal ribosome entry site displaces elf 3 to gain access to the 40S subunit. Nature. 2013;503(7477): 539-543. [CrossRef]
- Halim NKD, Ajayi OI. Risk factors and seroprevalence of Hepatitis C antibody in blood donors in Nigeria. East Africa Medical Journal. 2000;77(8):410-412.
- Hamza M, Samaila AA, Yakasai AM, Babashani M, Borodo MM, Habib AG. Prevalence of hepatitis B and C virus infections among HIV-infected patients in a tertiary hospital in North-Western Nigeria. Nigerian Journal of Basic and Clinical Sciences. 2013;10:76-81. [CrossRef]
- Ikeako LC, Ezegwui HU, Ajah LO, Dim CC, Okeke TC. Seroprevalence of Human Immunodeficiency Virus, Hepatitis B, Hepatitis C, syphilis, and coinfections among antenatal women in a tertiary institution in the south-east, Nigeria. Annals of Medical and Health Sciences Research. 2014;4(6). [CrossRef]
- Imoru, M., Eke, C., & Adegoke, A. (2003). Prevalence of Hepatitis-B Surface Antigen (HbsAg), Hepatitis C Virus (HCV) and Human Immunodeficiency Virus (HIV) among Blood Donors in Kano State, Nigeria. Journal of Medical Laboratory Science, 12(1), 59-63. [CrossRef]
- Inyama P U, Uneke C J, Anyanwu G I, Njoku O M, Idoko J H, Idoko J A. Prevalence of antibodies to Hepatitis C virus among Nigerian patients with HIV infection. Online J Hlth Allied Scs. 2005;2:2. [CrossRef]
- Jemilohun, A. C., Oyelade, B. O., & Oiwoh, S. O. (2014). Prevalence of Hepatitis C virus antibody among undergraduates in Ogbomoso, Southwestern Nigeria. African Journal of infectious Diseases, 8(2), 40-43. [CrossRef]
- Jeremiah, Z. A., Koate, B., Buseri, F., & Emelike, F. (2008). Prevalence of antibodies to hepatitis C virus in apparently healthy Port Harcourt blood donors and association with blood groups and other risk indicators. Blood Transfusion, 6(3), 150. [CrossRef]
- Kamande MW, Kibebe H, Mokua J. Prevalence of transfusion transmissible infections among blood donated at Nyeri satellite transfusion Centre in Kenya. IOSR Journal of Pharmacists. 2016;6:20–30.
- Karoney, M. J., & Siika, A. M. (2013). Hepatitis C virus (HCV) infection in Africa: a review. Pan African medical journal, 14(1). [CrossRef]
- Kassim OD, Oyekale TO, Aneke JC, Durosinmi MA. Prevalence of seropositive blood donors for hepatitis B, C and HIV viruses at the Federal Medical Centre, Ado-Ekiti Nigeria. Ann Trop Pathol. 2012; 3:47–55.
- Kesson AM (2002).Diagnosis and Management of paediatric hepatitis C infection. Journal Paediatr child health; 38: 213–218. [CrossRef]
- Klevens, R. M., Miller, J., Vonderwahl, C., Speers, S., Alelis, K., Sweet, K., & Gallagher, K. (2009). Population-based surveillance for hepatitis C virus, United States, 2006–2007. Emerging infectious diseases, 15(9), 1499. [CrossRef]
- Koate BBD, Buseri FI, Jeremiah ZA. Seroprevalence of hepatitis C virus among blood donors in Rivers State, Nigeria. Transfusion Medicine. 2005;15:449-451. [CrossRef]
- Lee, S. R., Kardos, K. W., Schiff, E., Berne, C. A., Mounzer, K., Banks, A. T., ... & Roehler, M. (2011). Evaluation of a new, rapid test for detecting HCV infection, suitable for use with blood or oral fluid. Journal of virological methods, 172(1-2), 27-31. [CrossRef]
- Lesi, O. A., M. O. Kehinde, D. N. Oguh, and C. O. Amira. Hepatitis B and C virus infection in Nigerian patients with HIV/AIDS. Niger. Postgrad. Med. J., 2007; 14: 129–133. [CrossRef]
- Muriuki, B. M., M. M. Gicheru, D. Wachira, A. K. Nyamache, and S. A. Khamadi. Prevalence of hepatitis B and C viral coinfections among HIV-1 infected individuals in Nairobi, Kenya. BMC Research Notes, 2013; 6: 363. [CrossRef]
- Nagu, T. J., M. Bakari, and M. Matee. Hepatitis A, B and C viral coinfections among HIV-infected adults presenting for care and treatment at Muhimbili National Hospital in Dar es Salaam, Tanzania. BMC Public Health, 2008; 8: 416. [CrossRef]
- Nwannadi IA, Alao O, Shoaga L. Hepatitis C among blood donors in teaching hospital in North Central Nigeria. IOSR Journal of Dental Medical Science. 2014;13:20–3.
- Nwannadi, I. A., Alao, O. O., Bazuaye, G. N., Omoti, C. E., & Halim, N. K. (2012). Seroprevalence of hepatitis C virus antibodies in sickle cell anaemia patients in Benin City, Nigeria. Gomal Journal of Medical Sciences, 10(1).
- Obienu, O., Nwokediuko, S., Malu, A., & Lesi, O. A. (2011). Risk factors for Hepatitis C virus transmission obscure in Nigerian patients. Gastroenterology research and practice, 2011. [CrossRef]
- Ogbodo, E. N., Otue A. & Okonko, I. O. (2015). Anti-HCV antibody among newly diagnosed HIV patients in Ughelli, a suburban area of Delta State Nigeria. African Health Sciences 15(3):728-736. [CrossRef]
- Ogwu-Richard SO, Ojo DA, Akingbade OA, Okonko IO. Triple positivity of HBsAg, anti-HCV antibody, and HIV and their influence on CD4+ lymphocyte levels in the highly HIV infected population of Abeokuta, Nigeria. African Health Sciences. 2015;15(3):719-727. [CrossRef]
- Ojide CK, Kalu EI, Ogbaini-Emevon E, Nwadike VU. Coinfections of hepatitis B and C with human immunodeficiency virus among adult patients attending human immunodeficiency virus outpatients clinic in Benin City, Nigeria. Nigerian Journal of Clinical Practice. 2015;18(4):516-521. [CrossRef]
- Okocha EC, Aneke JC, Ezeh TU, Ibeh NC, Nwosu GA, Okorie IO. The epidemiology of transfusion-transmissible infections among blood donors in Nnewi, South-East Nigeria. African Journal of Medical Health Science. 2015;14:125–9. [CrossRef]
- Okonko, I. O., Ikunga, C. V., Anugweje, K. C. & Okerentugba, P. O. (2014). Anti-hepatitis C virus (HCV) antibody detection among fresh undergraduate students in Port Harcourt, Nigeria. Basic Sciences of Medicine, 3(2): 26–29.
- Okonko IO, Cookey TI & Innocent-Adiele HC. (2022). Dual positivity of HIV and anti-HCV in the highly infected population of Rivers State, Nigeria. International Journal of Scientific Research Updates, 04(02), 039–048. [CrossRef]
- Okonko IO, Oyediji TO, Anugweje KC, Adeniji FO, Alli JA, Abraham OA. Detection of HCV antibody among intending blood donors. Nature and Science. 2012;10(1): 53-58.
- Okoroiwu HU, Okafor IM, Asemota EA, Okpokam DC. Seroprevalence of transfusion-transmissible infections (HBV, HCV, syphilis and HIV) among prospective blood donors in a tertiary health care facility in Calabar, Nigeria; An eleven years evaluation. BMC Public Health. 2018;18: 645. [CrossRef]
- Oluremi AS, Opaleye OO, Ogbolu DO, Alli OAT, Ashiru FT, Alaka OO, et al. Serological evidence of HIV, Hepatitis B, C, and E viruses among liver disease patients attending tertiary hospitals in Osun State, Nigeria. Journal of Immunoassay and Immunochemistry. 2021;42(1): 69-81. [CrossRef]
- Omatola CA, Lawal C, Omosayin DO, Okolo MO, Adaji DM, Mofolorunsho CK, Bello KE. Seroprevalence of HBV, HCV, and HIV and Associated Risk Factors Among Apparently Healthy Pregnant Women in Anyigba, Nigeria. Viral immunology. 2019;32(4):186-191. [CrossRef]
- Omolade O, Adeyemi A. Prevalence of hepatitis C virus antibody among university students in Nigeria. Journal of Virus Eradication. 2018;4(4):228–229. [CrossRef]
- Onyekwere CA, Hameed L. Hepatitis B and C virus prevalence and association with demographics: report of population screening in Nigeria. Tropical Doctor. 2015;45(4):231-235. [CrossRef]
- Onyekwere, C. A., Ogbera, A. O., Dada, A. O., Adeleye, O. O., Dosunmu, A. O., Akinbami, A. A., ... & Hameed, O. (2016). Hepatitis C virus (HCV) prevalence in special populations and associated risk factors: A report from a tertiary hospital. Hepatitis monthly, 16(5). [CrossRef]
- Opaleye OO, Igboama MC, Ojo JA, Odewale G. Seroprevalence of HIV, HBV, HCV, and HTLV among Pregnant Women in Southwestern Nigeria. Journal of Immunoassay and Immunochemistry. 2016;37(1):29-42. [CrossRef]
- Parboosing, R., I. Paruk, and U. G. Lalloo. Hepatitis C virus seropositivity in a South African Cohort of HIV co-infected, ARV naive patients is associated with renal insufficiency and increased mortality. J. Med. Virol., 2008; 80: 1530-1536. [CrossRef]
- Patrick, S. W., Bauer, A. M., Warren, M. D., Jones, T. F., & Wester, C. (2017). Hepatitis C virus infection among women giving birth—Tennessee and United States, 2009–2014. MMWR. Morbidity and mortality weekly report, 66(18), 470. [CrossRef]
- Riou J, Aït Ahmed M., Blake A, Vozlinsky S, Brichler S, Eholié S, Boëlle PY, Fontanet A. HCV epidemiology in Africa group hepatitis C virus seroprevalence in adults in Africa: A systematic review and meta-analysis. Journal of Viral Hepatitis. 2016;23:244–255. [CrossRef]
- Schillie SF, Canary L, Koneru A, et al. Hepatitis C virus in women of childbearing age, pregnant women, and children. Am J Prev Med 2018;55:633–41. [CrossRef]
- Schillie, S., Wester, C., Osborne, M., Wesolowski, L., & Ryerson, A. B. (2020). CDC recommendations for hepatitis C screening among adults—United States, 2020. MMWR Recommendations and Reports, 69(2), 1. [CrossRef]
- Smith BD, Morgan RL, Beckett GA, et al. Recommendations for the identification of chronic hepatitis C virus infection among persons born during 1945-1965. MMWR Recomm Rep 2012;61(RR-4):1–32.
- Spradling, P. R., J. T. Richardson, K. Buchacz, A. C. Moorman, L. Finelli, B. P. Bell, and J. T. Brooks. Trends in hepatitis C virus infection among patients in the HIV Outpatient Study, 1996-2007. J. Acquir. Immune Defic. Syndr., 2010; 53: 388-396. [CrossRef]
- Strickland GT. HCV in developing Countries. Postgrad. Doc. (Africa). 2002; 24:18-20.
- Syed-Mohammed J, Stuart CG (2018). Epidemiology of Hepatitis C. Clinical Liver Disease; 12(5):140–142.
- Te HS, Jensen DM (2001). Epidemiology of hepatitis B and C viruses: A global overview. Clin Liver Dis; 14(1):1-21. [CrossRef]
- Tessema, B., Yismaw, G., Kassu, A., Amsalu, A., Mulu, A., Emmrich, F., & Sack, U. (2010). Seroprevalence of HIV, HBV, HCV and syphilis infections among blood donors at Gondar University Teaching Hospital, Northwest Ethiopia: declining trends over a period of five years. BMC Infectious diseases, 10(1), 1-7. [CrossRef]
- Tohme, R. A. A. H., S. D. Is sexual contact a major mode of hepatitis C virus transmission? Hepatology, 2010; 1497–1505. [CrossRef]
- Tremeau-Bravard A, Ogbukagu IC, Ticao CJ, Abubakar JJ. Seroprevalence of hepatitis B and C infection among the HIV-positive population in Abuja, Nigeria. African Health Sciences. 2012;12(3):312-317. [CrossRef]
- Tsai HC, Chou PY, Wann SR, Lee SSJ, Chen YS. (2015). Chemokine co-receptor usage in HIV-1-infected treatment-naïve voluntary counselling and testing clients in Southern Taiwan. BMJ Open. 2015;5(4):e007334. [CrossRef]
- Udeze, A. O., Bamidele, R. A., Okonko, I. O., and Sule, W. F. (2011). Hepatitis C Virus (HCV) Antibody Detection Among First Year Students of University of Ilorin, Ilorin, Nigeria. World J of Med Sci. 6.162-167.
- Udeze, A. O., Okonko, I. O., Donbraye, E., Sule, W. F., Fadeyi, A. and Uche, L. N. (2009). Seroprevalence of Hepatitis C Virus Antibodies Amongst Blood Donors in Ibadan, Southwestern Nigeria. World ApplSci J., 7: 1023-1028.
- Walana W, Ahiaba S, Hokey P, Vicar EK, Acquah SEK, Der EM. Seroprevalence of HIV, HBV and HCV among blood donors in Kintampo municipal hospitals, Ghana. Br Microbiology Resource Journal. 2014;12: 1491–9.
- World Health Organization (WHO, 1999). Global surveillance and control of hepatitis C. Report of a WHO Consultation organized in collaboration with the Viral Hepatitis Prevention Board, Antwerp, Belgium. J Viral Hepatitis, 6.35-47.
Figure 1.
Overall Prevalence of Hepatitis C Virus
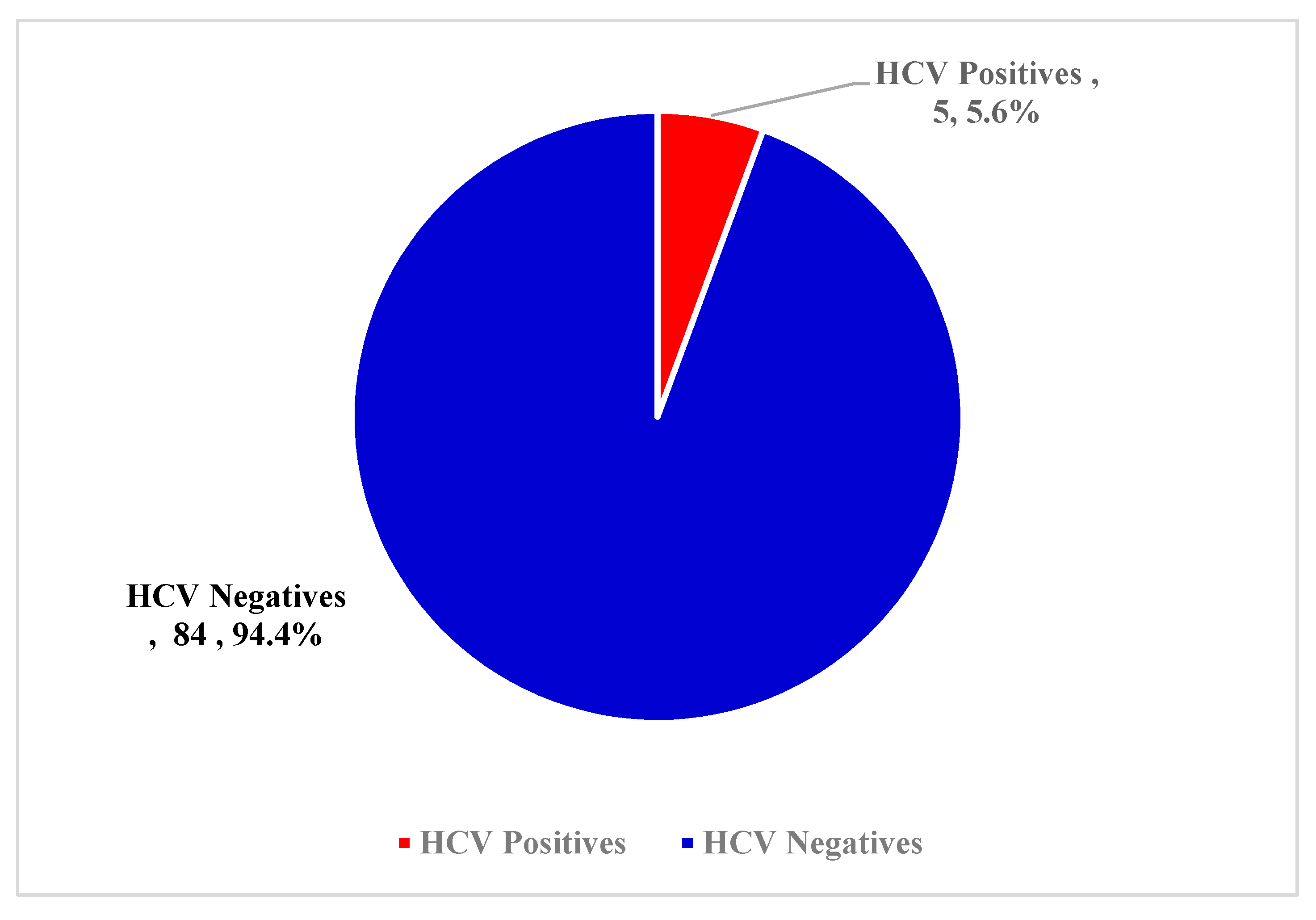
Figure 2.
Prevalence of Hepatitis C Virus with age.
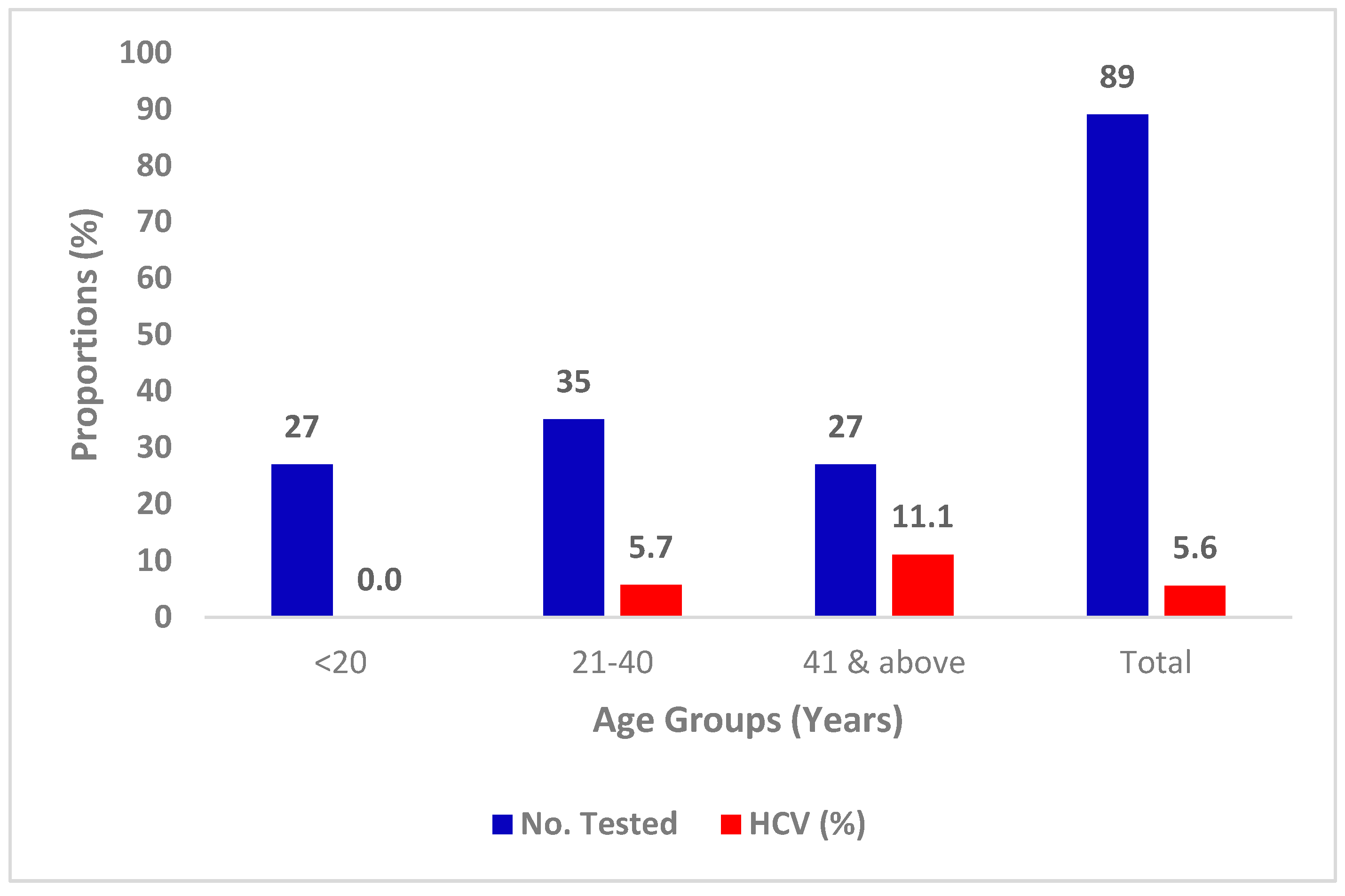
Figure 3.
Prevalence of Hepatitis C Virus with sex
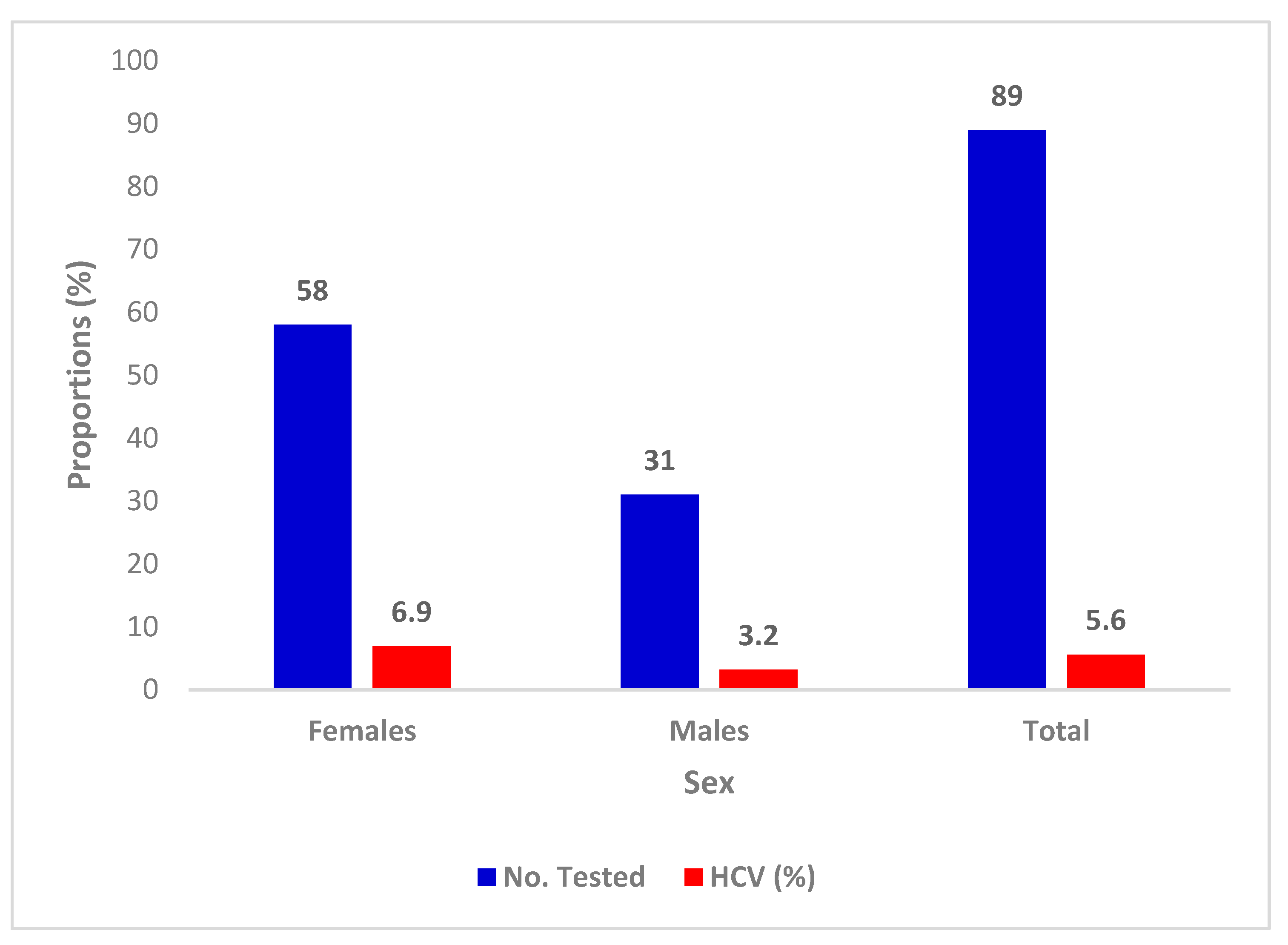
Figure 4.
Prevalence of Hepatitis C Virus with Marital Status
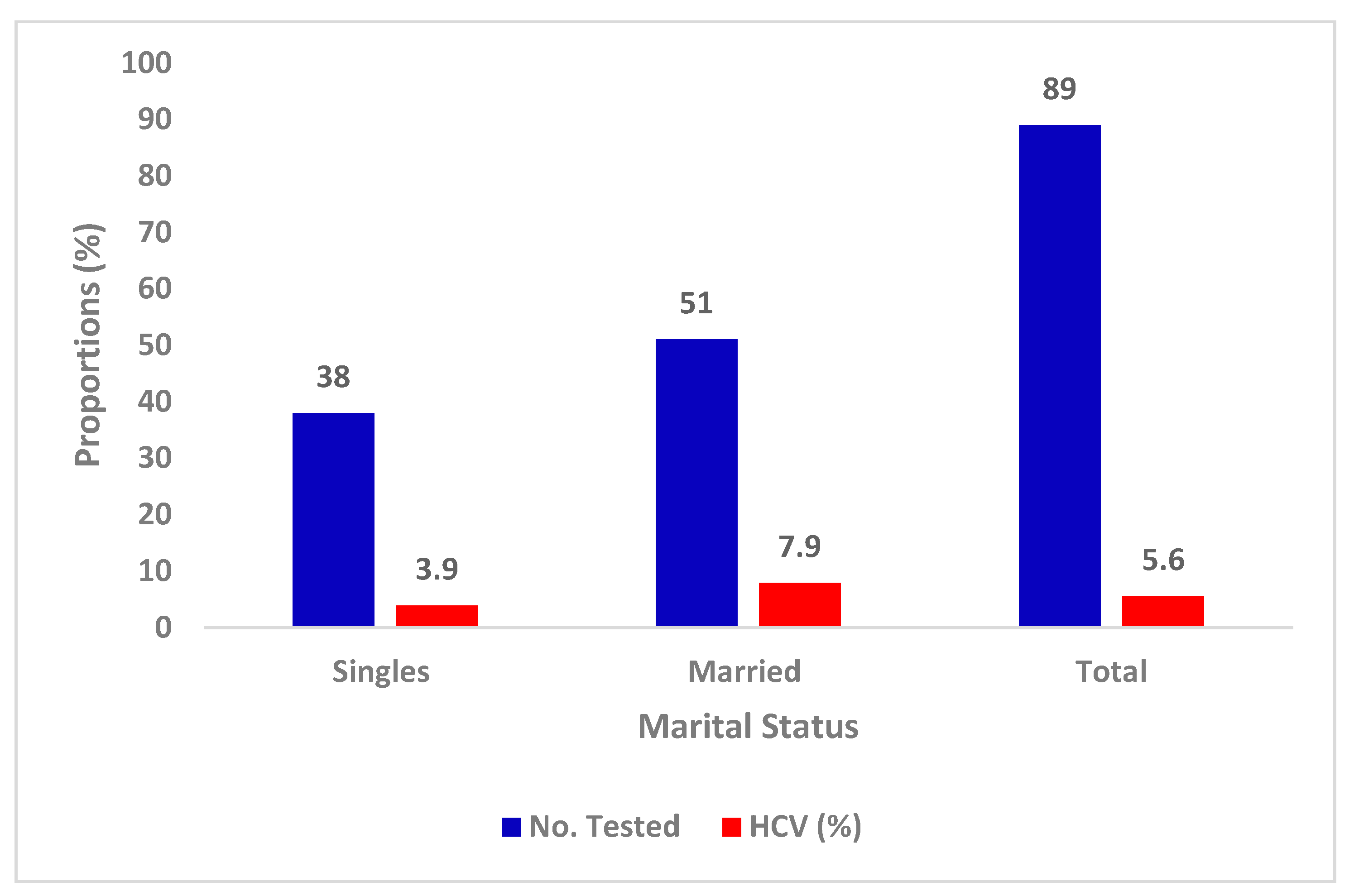
Figure 5.
Prevalence of Hepatitis C Virus with Educational Status.
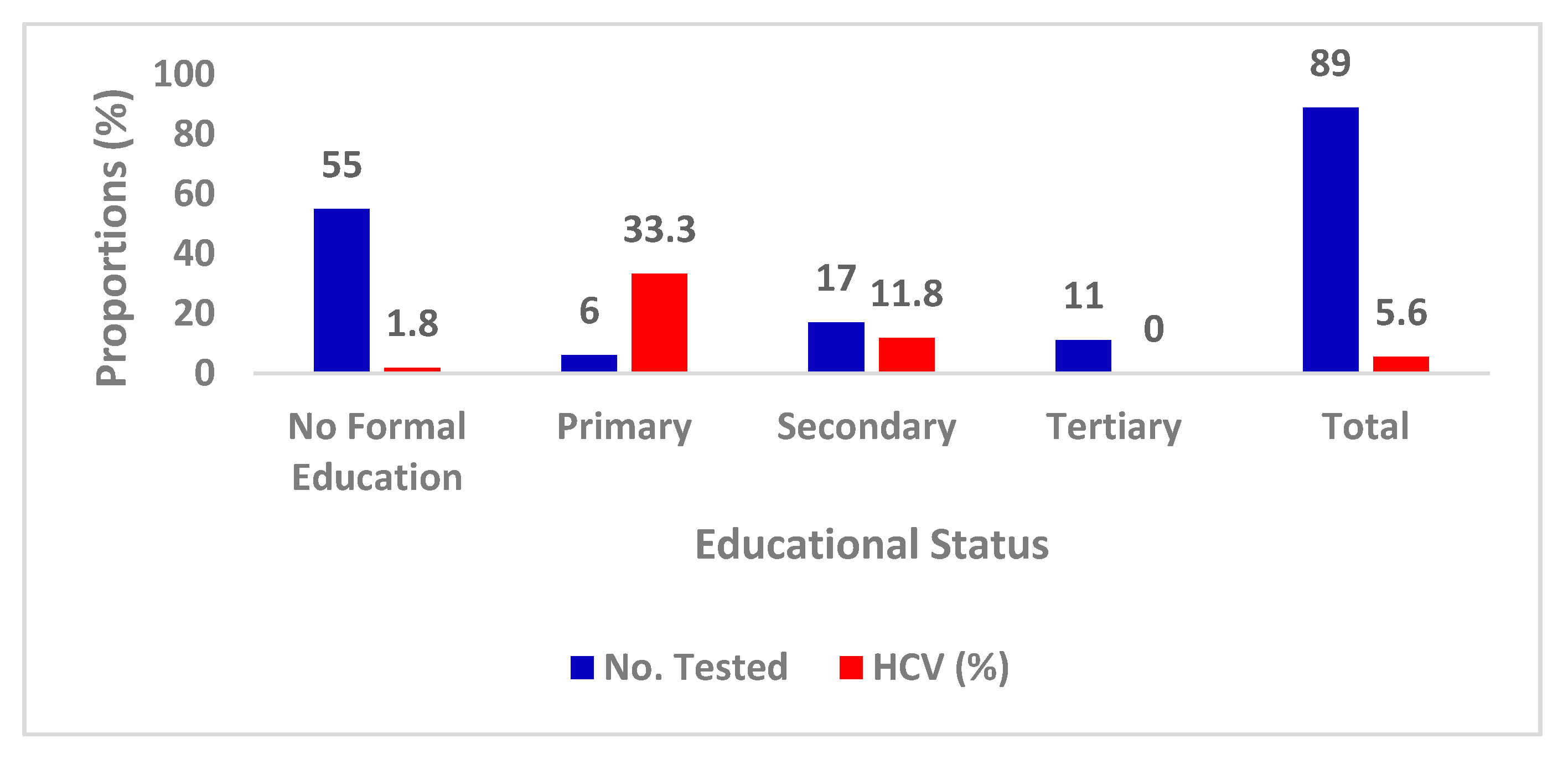

Table 1.
Socio-demographic of the studied Febrile Patient’s population
| Characteristics | Categories | No. Tested | Percentage |
|---|---|---|---|
| Age group (years) | 2-20 | 27 | 30.3 |
| 21-40 | 35 | 39.3 | |
| 41 & above | 27 | 30.3 | |
| Gender | Females | 58 | 65.1 |
| Males | 31 | 34.8 | |
| Marital status | Married | 51 | 57.3 |
| Single | 38 | 42.7 | |
| Educational | No formal | 55 | 61.7 |
| Primary | 6 | 6.7 | |
| Secondary | 17 | 19.2 | |
| University | 11 | 12.4 | |
| Total | 89 | 100.0 | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



