Submitted:
11 February 2023
Posted:
14 February 2023
You are already at the latest version
Abstract
Mesenchymal Stromal Cells (MSCs) are multipotent, non-hematopoietic progenitor cells with a wide range of immune conditioning and regenerative potential which qualify them as potential component of cell based therapy for various autoimmune / chronic inflammatory ailments. Their immunomodulatory properties include the secretion of immunosuppressive cytokines, the ability to suppress T-cell activation and differentiation, and the induction of regulatory T-cells. In view of this and our interest, we here discuss the significance of MSC for the management of Graft-versus-Host Disease (aGVHD), one of the autoimmune manifestation in human.. In pre-clinical models, MSCs have been shown to reduce the severity of aGVHD symptoms, including skin and gut damage, which are the most common and debilitating manifestations of this disease. While initial clinical studies of MSCs in aGVHD cases were promising, the results were variable in randomized studies. So, further studies are warranted to fully understand their potential benefits, safety profile, and optimal dosing regimens. In view of these inevitable issues, here we discuss various mechanisms, how MSCs can be employed in managing aGVHD, as a therapeutic option for this disease.
Keywords:
Mesenchymal Stromal Cells
; Graft-versus-Host-Disease
; Immunomodulation
; Apoptosis
; Efferocytosis
; Secretome
Introduction
Mesenchymal stromal cells are well known for their potential to improve the outcomes of allogeneic hematopoietic stem cell transplantation (HSCT). Allogeneic HSCT is a life-saving procedure in which a healthy donor’s stem cells are transplanted into a recipient with an abnormal or malignant hematopoietic system to restore normal functioning. The primary goal of allogeneic HSCT is to successfully engraft donor stem cells into the recipient, allowing for the production of healthy and functional blood cells. However, allogeneic HSCT is associated with a high risk of graft-versus-host-disease (GVHD), which can be fatal and is caused by the donor’s immune cells attacking the recipient’s healthy cells. MSCs have been studied for their ability to reduce GVHD, improve donor stem cell engraftment, and modulate the recipient’s immune system in a beneficial way. This review will provide an overview of the role of MSCs on GVHD. Alexander Friedenstein and his colleagues studied the bone marrow microenvironment and first isolated MSCs from the bone marrow in the late 1960s and early 1970s [1–5]. Mesenchymal stromal cells are multipotent heterogeneous populations of adult non-hematopoietic stem cells that can self-renew, have fibroblast-like-morphology and can be isolated from various sources such as bone marrow, umbilical cord, umbilical cord blood, Wharton jelly, amniotic fluid, amniotic membrane, dermal, skeletal muscle, adipose tissue, the dental pulp, synovial fluid, menstrual blood, peripheral blood, and many more. The persistence of MSCs in various organs leads to the notion that MSCs reside in the perivascular niche and show that the perivascular progenitor cells are precursors of MSCs as these shared similar immune-phenotypic expression of stemness-associated surface markers with a few different markers such as CD146. Additionally, available evidence shows that naïve MSCs share little functionality with pericytes and adventitial cells, leading to the concept that MSCs might derive from blood vessel-associated cells mainly, pericytes. Thus, all MSCs are pericytes but all pericytes are not MSCs as the pericytes do not demonstrate multipotency. In 2006, the International Society for Cellular Therapy (ISCT) defines three minimum criteria for the identification and characterization of MSCs- 1) Adherence to plastic; 2) Exhibiting ≥95% expression of CD105, CD73, CD90, CD29, lower expression of HLA-I, and absence or ≤ 2% of lineage-specific markers (CD34, CD45, CD14, CD16, CD11b), HLA-II molecule; 3) ability to differentiate into mesodermal (osteogenic, chondrogenic and adipogenic) lineages under in vitro conditions [6,7].
However, surface markers may not be the ideal parameters to characterize MSCs due to the plasticity in the expression of CD34 surface markers under in vitro and in vivo conditions. Mesenchymal stromal cells stably express CD34 in vivo, however this often remain unstable in vitro which depends on culture conditions (cell-culture media, plastic adherence), donor, and passage [8]. Additionally, the expression of HLA-DR was also upregulated due to the addition of IFN-γ in the culture media [8–10]. Thus, in 2019, ISCT committee members recommends using the acronym “MSC” with tissue-source and functional assays to demonstrate tissue-specific and therapeutic properties of MSCs respectively [8,11]. Additionally, the stemness of the MSC population should be confirmed in vitro and in vivo [12,13].
In 2019, the ISCT proposed the following criteria to define MSCs: 1) Adherence to plastic, 2) Marked by ≥95% expression of CD105, CD73, CD90, CD29, lower expression of HLA-I, and absence or ≤ 2% of lineage-specific markers (CD34, CD45, CD14, CD16, CD11b), HLA-II molecule, 3) Trilineage differentiation to mesodermal lineage. 4) Specify the tissue origin with the acronym MSC. 5) Stemness of MSCs must be established by in vitro and in vivo data. 6) Assay matrix should provide either qualitative or quantitative data with precision or a detailed mechanism of action of MSCs.
Arnold I Caplan argued that ‘stem cell’ is not an appropriate term for MSCs due to their variability in the functional properties in vitro and in vivo. Another aspect is related to the variability in their in vivo behavior. MSCs home to sites of inflammation or tissue injury and secrete massive levels of bioactive agents that have both immunomodulatory and trophic properties. Thus, Arnold I Caplan suggests the term “Medicinal Signaling Cells” due to its in vivo behavior [14].
Therapeutic Mechanism of MSCs
Owing to their potential of migrating to injury sites, secreting bioactive factors with pleiotropic effects such as anti-apoptotic, angiogenic, anti-inflammatory, anti-fibrotic, immunomodulatory, and antioxidant, and eventually lead to the repair of injured tissue [13,15–17], MSC are now competent tool of regenerative medicine and/or immune conditioning approaches. In [18] such as GVHD [17,19], Crohn’s disease [17,20], Liver diseases [17,21,22], Aplastic anemia [23], Rheumatoid arthritis [17,24], Multiple sclerosis [25], neurodegenerative diseases [17,26,27], spinal cord injuries [17,28], COVID-19 [29], and others. Together, MSCs bear the capacity of overcoming the barrier of immune rejection due to their ability to lower down expression of MHC class-I molecules and the absence of MHC-II molecules, facilitating their administration without donor-recipient HLA matching [30] and exerting their immunoregulatory effects through cell-cell contact [31], transfer of mitochondria through tunnelling nanotubes and microvesicles to target cells [30,32] and paracrine secretion of soluble factors and microvesicles containing RNA and other molecules [13,30,33]. The utilization of MSCs in inflammatory diseases might reflect two different functions of MSCs: 1) Engraftment and 2) Tissue homeostasis. Depending on the extent of inflammation and stimulation of MSCs through Toll-like receptors, these can switch between pro-inflammatory (M1) and anti-inflammatory (M2) phenotypes [34]. Nevertheless, MSCs are not inherently immunosuppressive while these are conditioned by in vivo milieu to modulate the immune system [35].
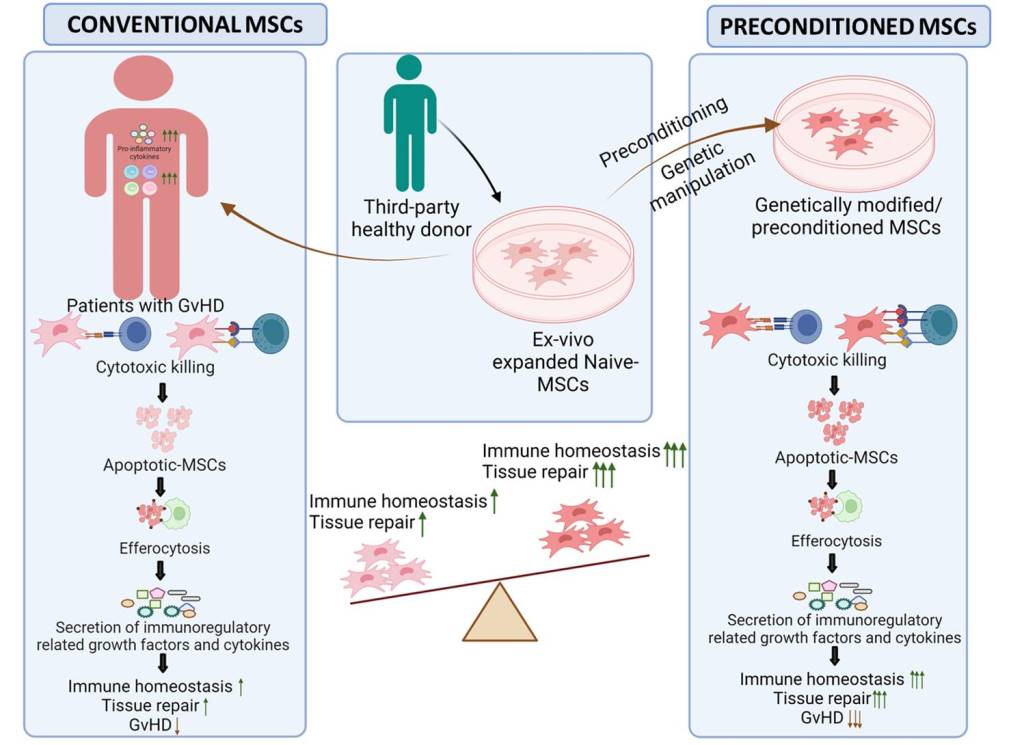
The immunosuppression caused by MSCs in GVHD dependents on the type of death (largely apoptosis) of MSCs by activated cytotoxic T lymphocytes and to some extent by natural killer cells [36,37] followed by the clearance of dead MSCs by monocytes / DC, termed efferocytosis [37,38]. This in turn, release an array of immunosuppressive mediators (HLA-G, PGE-2, IDO, TGF-β, COX-2, PD-L1, IL-1RA, IL-10, IL-6, CCL2) [39–42] which promote differentiation of effector/regulatory phenotype of immune cells like NK / T cells and Macrophages for attaining immune homeostasis [39]. Therefore, apoptosis and efferocytosis are two prime requirements for MSCs-mediated immune conditioning in GVHD, depicted in Figure 1. Furthermore, majority of the infused MSCs are undetectable within a few hours in vivo, thus, MSCs can act as “a drug instead of a cell”. Intriguingly, the efficacy of apoptotic-MSCs is still controversial in various immune-mediated disorders. In preclinical mice model of GVHD, the potency of apoptotic-MSCs is ineffective or comparably low as compared to their live counterparts [43] suggesting that viability of MSCs is pre requisite for their therapeutic potential. Apart from the immune condioning in GVHD, MSCs potentially contribute to the repair of injured tissues also by their differentiation to damaged tissues and paracrine secretion of trophic factors [18,44]. The exact chemokines, cytokines, and growth factors released by MSCs that mediate tissue repair in GVHD are still unclear.
There is increasing evidence that transplant-associated thrombotic microangiopathy (TA-TMA), and endothelial dysfunction contributes to the pathogenesis of steroid-refractory GVHD [45,46] and is linked to high mortality and morbidity rates after HSCT [45,47,48]. The pathogenesis of TA-TMA has 3 major contributors: endothelial cell activation, complement dysfunction, and microvascular haemolytic anemia that leads to the dysfunctioning of multiple organs and ultimately to the death of transplant recipients due to delay in diagnosis [49].
Previous pre-clinical / clinical studies reported that MSCs have a shorter life span in vivo due to their sensitivity for perforin-dependent apoptosis causing by activated cytotoxic T cells and subsequent Efferocytosis [36,43,50–52]. Moreover, MSCs activate the complement system that not only caused the death of MSCs by forming a ‘membrane attack complex’ [50,53] but also causes the release of anaphylatoxins C3a, and C5a, that in turn bind to their receptors on neutrophils followed by the activation of neutrophils that cause apoptosis of MSCs through the oxidative burst [50,54–56]. Additionally, MSCs express complement regulatory proteins such as CD46, CD55, CD59, and soluble factor H that confer protection from complement-mediated lysis of MSCs [53,55–58]. Nonetheless, these mechanisms are not sufficient to protect MSCs from cell death. Thus, additional unknown factors are likely attenuating complement activation and contributing to immunosuppressive potential of MSCs thus advocating the clinical application of MSCs in complement-mediated disorders such as TA-TMA. Previous pre-clinical studies also demonstrated that the persistence of MSCs can be enhanced by depleting neutrophils and inhibiting the production of anaphylatoxins using monoclonal antibodies and surface modification of MSCs by complement inhibitors [50,59].
Clinical Scenario of MSCs In GVHD
There is no gold standard treatment for steroid-refractory GVHD (SR-GVHD) despite the availability of second-line treatments such as Ruxolitinib (JAK inhibitors) [60], and TNF-α inhibitors [61,62]. Owing to the immune condioning potential of MSCs, these have become ideal tools for cell-based therapeutic approach for (SR-GVHD). The first clinical application of MSCs for managing SR-GVHD was reported in 2004. In this case, allogeneic BM-MSCs were administered intravenously to the patient twice (a first dose on D+73 and another dose on D+150) to treat SR-GVHD. MSCs were well tolerated by the patient as he showed a little improvement at the first infusion while the second infusion remarkably enhanced the recovery of the patient [30,63]. This study showed promising results for GVHD and augmented the clinical use of MSCs which was approved by the FDA as the name of Prochymal for the treatment of SR-GVHD in paediatric patients. In 2012, Prochymal was the first MSCs-based drug that was approved in a few countries such as Canada, New Zealand, and Japan but not in USA and China [64]. Later on, the therapeutic efficacy of Remestemcel-L, a commercial off-the-shelf MSCs product was assessed in a phase-III randomized trial [65,66] but the study failed to demonstrate their promising results over the placebo with second-line therapy in terms of complete response (CR) and overall response (OR) [66,67]. However, the post-hoc analysis demonstrated that Remestemcel-L had a higher OR rate than the placebo arm [65,66]. Moreover, another commercial BM-MSC product, TEMCELL, was approved in Japan for the treatment of SR-GVHD patients in 2016, and interestingly, the therapeutic efficacy of TEMCELL was found to be equivalent to a prospective study of Remestemcel-L and identified elements that could predict OR and non-relapse mortality (NRM) in SR-GVHD patients [66,68]. Moreover, in 2020 phase-III trials were conducted by Osiris Therapeutics Ltd. using Remestemcel-L for paediatric SR-aGVHD patients in the absence of immunosuppressive agents. Infection-related adverse events were recorded, and the OR and CR rate was 70% and 44.6% on D+28 and D+100 respectively [69].
Induced MSCs (iMSCs) are more homogeneous than primary MSCs since iMSCs originated from a single induced pluripotent stem cell (iPSC) clone. This concept led to the development of therapeutic intervention based on iPSCs-derived MSCs for GVHD by Cynata’s Therapeutics in 2016. Further, Cynata’s Therapeutics got approval for the clinical phase I study involving iPSC-derived MSCs for SR-aGVHD and the results demonstrate the clinical efficacy of iPSC-derived MSCs [70]. A brief overview of clinical trials involving MSCs-based therapy for GVHD, registered in ClinicalTrials.gov is summarized in Table 1.
However, phase I/II clinical trials involving MSCs for the treatment of immune-related disorders yielded unpredicted outcomes in terms of the complete response (CR) over the placebo. Thus, the efficacy of MSCs in clinical trials is variable and unpredictable and the underlying mechanism of its efficacy/inefficacy has not been explored fully. The heterogeneous response of MSCs in immune-mediated disorders is attributed to the heterogeneity/viability of MSCs and pathological scores of the patients. Other factors like tissue source, age, sex, genetic makeup, the health status of the donor, culture conditions, long term-preservation, passage number, and other parameters including the severity of GVHD, heterogeneity of the disease, organ involvement, diverse patient characteristics, dose, mode and frequency of administration of MSCs [71] also potentially contribute to the efficacy of MSC. Additionally, there is no available biomarker that could predict the response of GVHD/SR-GVHD patients to MSCs.
Preconditioning of MSCs to Improve Clinical Efficacy
In view of heterogencity of MSC in various diseases discussed above, There is a need to augment the therapeutic immunomodulatory potential of MSCs in GVHD. Various strategies have been suggested to enhance the immunoregulatory potency of MSCs while maintaining their stemness and therapeutic efficacy. It is well known that an in vivo milieu could dictate the fate of MSCs and several approaches have been designed to enhance their therapeutic efficacy in immune-mediated disorders, discussed in followed section.
- 1)
- Preconditioning with cytokines:
Several reports suggested that preconditioning of MSCs using Th17 effectors (IFN-γ +TNF-α+IL-1β+IL-17) enhances their immunosuppressive potency through increasing homing of MSCs to injured tissues and production of immunosuppressive soluble factors. This promotes the differentiation of effector immune cells to their respective regulatory phenotype (Tregs, Th2, M2 macrophage). Preclinical studies with IFN-γ pre-conditioned MSCs in NOD/SCID mice model imposed a positive impact on their survival while reducing GVHD by activation of JAK/STAT and nd IDO [92,93]. These promising results led to Phase I clinical trial (NCT04328714) that involves the use of IFN-γ primed BM-MSCs as prophylactic conditioning of GVHD [94]. Nonetheless, inflammatory cytokines activated a specific signaling pathway that exerted an immune regulatory effect employing immunomodulatory trophic factors which are summarized in Figure 2 and Table 2. Additionally, they enhanced the homing of MSCs by increasing the expression of chemokines (CXCL9, CXCL10, and CXCL11) and adhesion molecules (VCAM-1, ICAM-1) [94].
- 2)
- Hypoxia preconditioning:
Hypoxia is one of the intrinsic factor which is known to promote angiogenic switch and augment immunosuppressive / Th2 microenvironment. Hypoxia enhances glycolysis of MSCs that leads to an increase in lactate level while the combination of IFN-γ and hypoxia enhanced the expression of IDO, PGE2, HLA-G, HLA-E, leading to inhibition of T cells activation [94]. Hypoxia with calcium ions causes a significant reduction in GVHD due to an increase in the polo-like kinase-1 (PLK1), zinc-finger protein-143, dehydrogenase/reductase-3, and friend-of-GATA2 [92,121]. Overall, hypoxia increases the homing ability of MSCs, ultimately leading to the rapid repair of injured tissue [100]. However, prolonged exposure of MSC to hypoxic microenvironment disrupt their vitality and compromise differentiation potential of MSCs [122]. Thus, an appropriate dose and exposure time for hypoxia is paramount for immune condioning potential of MSCs.
- 3)
- Immune receptor agonist:
Mesenchymal stromal cells express a variety of Toll-like receptors (TLR) which can interact with their specific ligands such as microbiome derived factors , which results in modulation of the immune response [34,123] by activation of phagocytic cells [34,124]. Various preclinical studies employed priming of MSCs with TLR-3 agonists (CpG island) to modulate the immune response which is candidly summarized in Table 3.
- 4)
- 3-dimensional (3D)-culture:
Paracrine signalling is main mechanism of MSC induced immune conditioning which is mediated through various transmembrane adhesion molecules on MSC [94,97,131–134]. This is known to mimics in vivo milieu and exert immunomodulatory effects due to the secretion of MMP-2, VEGF, and TSG-6 [94]. Additionally, 3-dimensional (3D)-spheroid culture enhance the stemness potential and increase the secretion of various immunomodulatory factors such as PGE-2, IDO, TGF-β, and many anti-inflammatory cytokines and soluble factors [106,135]. Therefore preconditioning the MSCs with pro-inflammatory cytokines using 3D-spheroid culture with bioactive materials such as hydrogels, and extracellular matrix increase cell-cell communication, can augment paracrine effect of MSCs [94]. Along with this, a few preclinical studies involve the use of scaffolds and biocompatible nanomaterials (gold nanoparticle, graphene derivatives) that might also enhance the biological properties of MSCs such as differentiation, homing, and migration [136–139]. Overall, the use of bioactive materials warrant their use in promoting the tissue repair and regeneration efficacy of MSCs.
- 5)
- Genetic manipulations:
Several factors such as HIF-1α [132,140], IL-10, IL-4, TGF-β, CXCR4, GATA-4 [132,141], and HGF [142] (Figure 2) can increase the migration, cell survival, proliferation, and immunosuppressive potential of MSCs. Recently, CRISPR Cas-9 technology has been employed to alter the m/miRNA content corresponding to above factors inMSCs or MSCs-derived extracellular vesicles, and transient epigenetic modifications [132,143] to augment their potential in regenerative medicine. However, these are at the early stage of research, so, it is difficult to predict their translational value.
- 6)
- Autophagy alteration:
Several studies have reported that either upregulation or down-regulation of autophagy in MSCs enhances their immunomodulatory effect in inflammatory diseases such as inflammatory bowel disease, colitis, and liver fibrosis. Alteration in autophagy enhances Tregs and decreases Th1 polarization and ultimately decreases the levels of inflammatory cytokines (IL-17A, IFN-γ, IL-2) and mediates immunosuppressive effect through PGE2 secretion [94].
- 7)
- Other agents:
A recent study demonstrates that host derived factors such as serum, plasma or IVIG can potentially influence immunomodulatory potential of MSCs which can be included as component of personalized MSCs therapy. Therefore, MSCs are primed with GVHD patient-derived plasma as GVHD is characterized by cytokine storm and their patient-derived plasma is marked heterogeneous in the proportion of inflammatory cytokines. GVHD plasma enhances the immunomodulatory potency of MSCs by alteration in their morphology, upregulating the expression of cell-adhesion molecule (ICAM-1), and induction of Tregs [144]. Moreover, various bioactive agents and various drugs such as tacrolimus, and rapamycin [132] can be used to enhance homing, survival, and immunoregulatory potential of MSCs so that the efficacy of MSCs augment in clinical trials. In the upcoming section, we are discussing the use of bioactive compounds that can enhance their therapeutic potential as immunoregulatory agents, summarized in Figure 2 and Table 4.
Conclusion of Clinical Perspective
Mesenchymal stromal cells have shown promising results in clinical studies of immune-mediated disorders. However, the response of the recipients towards MSCs-based cellular therapy is quite variable and unpredictable which limits the efficacy of MSCs-based intervention in clinics. It is well demonstrated that MSCs exert their immunoregulatory effect through paracrine secretion of growth factors, cytokine, and other immunoregulatory soluble factors. Owing to this potential, MSCs secretome could be a better therapeutic or prophylactic approach for immune disorders due to the following advantages, 1) it can be manipulated and stored more easily than cells, 2) with fewer costs, it can be a used asready-to-use product suitable for emergency interventions, 3) the possibility of pharmaceuticalizing MSCs-secretome into freeze-dried and stable powder products, could be easily acceptable by the community as a cell-free intervention. Moreover pharmaceuticalization of MSCs derived secretome into a high-quality safe and effective immune pharmaceuticals by exploiting large-scale and GMP procedures. Additionally, there is dire need of developing MSCs secretome, specific for a disease. However, a recent study, paradoxically demonstrates that the secretome of MSCs consists of solely pro-inflammatory cytokines (MCP-1, IL-6, IL-8) while barely consisting of any anti-inflammatory cytokines (IL-10, IL-4) [150] In the clinical scenario, MSCs-derived EVs or whole secretome have not been used for GVHD as a therapeutic or prophylaxis but there are a few preclinical studies that demonstrate that the MSCs-derived EVs have the potential to neutralize GVHD [151] to some extent These studies revealed that MSCs (BM/WJ) derived EVs exert their immunoregulatory effect by decreasing the levels of IL-21, IL-22 [151,152], IFN-γ, TNF-α [151,153], IL-2 [151,154], increasing the levels of IL-10) [151,154], and also modulating the immune cells such as differentiation of CD4+ T cells to a regulatory phenotype (Tregs) [151,155], suppression of CD4+ [151,152] and CD8+ T cells into effector phenotype [151,156] and together improving the survival of GVHD mice model [151,153].A major hurdle in MSCs from the clinical perspective is to identify responders and non-responders of GVHD for MSCs therapy as most of the phase 2/3 clinical trials show the ineffectiveness of MSCs therapy for GVHD. Generally, it is required to develop a biomarker in respect of either cellular or plasma/serum protein that can predict and monitor the clinical response and efficacy of MSCs or their secretome for GVHD patients.
Acknowledgments
The study was supported by Indian Council of Medical Research, New Delhi, India (Grant ID: 2021/14763 and 2021/13853) and Department of Science and Technology-Science and Engineering Board, New Delhi, India (Grant Id: EMR/2016/002633). Figures are created using Biorender.com.
References
- Matheakakis, A.; Batsali, A.; Papadaki, H.A.; Pontikoglou, C.G. Therapeutic Implications of Mesenchymal Stromal Cells and Their Extracellular Vesicles in Autoimmune Diseases: From Biology to Clinical Applications. Int. J. Mol. Sci. 2021, 22, 10132. [Google Scholar] [CrossRef] [PubMed]
- Pontikoglou, C.; Deschaseaux, F.; Sensebé, L.; Papadaki, H.A. Bone Marrow Mesenchymal Stem Cells: Biological Properties and Their Role in Hematopoiesis and Hematopoietic Stem Cell Transplantation. Stem Cell Rev. Rep. 2011, 7, 569–589. [Google Scholar] [CrossRef] [PubMed]
- Friedenstein, A.J.; Petrakova, K.V.; Kurolesova, A.I.; Frolova, G.P. HETEROTOPIC TRANSPLANTS OF BONE MARROW. Transplantation 1968, 6, 230–247. [Google Scholar] [CrossRef] [PubMed]
- Friedenstein, A.J.; Chailakhjan, R.K.; Lalykina, K.S. The Development of Fibroblast Colonies in Monolayer Cultures of Guinea-Pig Bone Marrow and Spleen Cells. Cell Prolif. 1970, 3, 393–403. [Google Scholar] [CrossRef]
- Aj, F. Osteogenic stem cells in bone marrow. Bone Miner Res. 1990;243–72.
- Dominici, M.; Le Blanc, K.; Mueller, I.; Slaper-Cortenbach, I.; Marini, F.C.; Krause, D.S.; Deans, R.J.; Keating, A.; Prockop, D.J.; Horwitz, E.M. Minimal criteria for defining multipotent mesenchymal stromal cells. The International Society for Cellular Therapy position statement. Cytotherapy 2006, 8, 315–317. [Google Scholar] [CrossRef]
- Squillaro, T.; Peluso, G.; Galderisi, U. Clinical Trials with Mesenchymal Stem Cells: An Update. Cell Transplant. 2016, 25, 829–848. [Google Scholar] [CrossRef]
- Viswanathan, S.; Shi, Y.; Galipeau, J.; Krampera, M.; Leblanc, K.; Martin, I.; Nolta, J.; Phinney, D.G.; Sensebe, L. Mesenchymal stem versus stromal cells: International Society for Cell & Gene Therapy (ISCT®) Mesenchymal Stromal Cell committee position statement on nomenclature. Cytotherapy 2019, 21, 1019–1024. [Google Scholar] [CrossRef]
- Stagg, J.; Pommey, S.; Eliopoulos, N.; Galipeau, J. Interferon-γ-stimulated marrow stromal cells: a new type of nonhematopoietic antigen-presenting cell. Blood 2006, 107, 2570–2577. [Google Scholar] [CrossRef]
- Romieu-Mourez R, François M, Boivin MN, Stagg J, Galipeau J. Regulation of MHC Class II Expression and Antigen Processing in Murine and Human Mesenchymal Stromal Cells by IFN-γ, TGF-β, and Cell Density1. J Immunol. 2007 Aug 1;179(3):1549–58.
- Miclau, K.; Hambright, W.S.; Huard, J.; Stoddart, M.J.; Bahney, C.S. Cellular expansion of MSCs: Shifting the regenerative potential. Aging Cell 2022, 22. [Google Scholar] [CrossRef]
- Galipeau, J.; Krampera, M.; Barrett, J.; Dazzi, F.; Deans, R.J.; DeBruijn, J.; Dominici, M.; Fibbe, W.E.; Gee, A.P.; Gimble, J.M.; et al. International Society for Cellular Therapy perspective on immune functional assays for mesenchymal stromal cells as potency release criterion for advanced phase clinical trials. Cytotherapy 2015, 18, 151–159. [Google Scholar] [CrossRef]
- Merimi, M.; El-Majzoub, R.; Lagneaux, L.; Agha, D.M.; Bouhtit, F.; Meuleman, N.; Fahmi, H.; Lewalle, P.; Fayyad-Kazan, M.; Najar, M. The Therapeutic Potential of Mesenchymal Stromal Cells for Regenerative Medicine: Current Knowledge and Future Understandings. [Internet]. 2021 [cited 2023 Jan 11];9. Available from: https://www.frontiersin.org/articles. Front. Cell Dev. Biol. 2021, 9. [Google Scholar] [CrossRef] [PubMed]
- Caplan, AI. Mesenchymal Stem Cells: Time to Change the Name! STEM CELLS Transl Med. 2017;6(6):1445–51.
- Hmadcha, A.; Martin-Montalvo, A.; Gauthier, B.R.; Soria, B.; Capilla-Gonzalez, V. Therapeutic Potential of Mesenchymal Stem Cells for Cancer Therapy. Front. Bioeng. Biotechnol. 2020, 8, 43. [Google Scholar] [CrossRef] [PubMed]
- Salgado AJBOG, Reis RLG, Sousa NJC, Gimble JM, Salgado AJ, Reis RL, et al. Adipose Tissue Derived Stem Cells Secretome: Soluble Factors and Their Roles in Regenerative Medicine. Curr Stem Cell Res Ther. 5(2):103–10.
- Fan, X.-L.; Zhang, Y.; Li, X.; Fu, Q.-L. Mechanisms underlying the protective effects of mesenchymal stem cell-based therapy. Cell. Mol. Life Sci. 2020, 77, 2771–2794. [Google Scholar] [CrossRef] [PubMed]
- Markov A, Thangavelu L, Aravindhan S, Zekiy AO, Jarahian M, Chartrand MS, et al. Mesenchymal stem/stromal cells as a valuable source for the treatment of immune-mediated disorders. Stem Cell Res Ther. 2021 Mar 18;12(1):192.
- Dunavin N, Dias A, Li M, McGuirk J. Mesenchymal Stromal Cells: What Is the Mechanism in Acute Graft-Versus-Host Disease? Biomedicines [Internet]. 2017 Jul 1 [cited 2020 Jul 8];5(3). Available from: https://www.ncbi.nlm.nih. 5618.
- Garcia-Olmo D, Herreros D, Pascual I, Pascual JA, Del-Valle E, Zorrilla J, et al. Expanded Adipose-Derived Stem Cells for the Treatment of Complex Perianal Fistula: a Phase II Clinical Trial. Dis Colon Rectum. 2009 Jan;52(1):79.
- Zhang, Y.; Li, Y.; Zhang, L.; Li, J.; Zhu, C. Mesenchymal stem cells: potential application for the treatment of hepatic cirrhosis. Stem Cell Res. Ther. 2018, 9, 59. [Google Scholar] [CrossRef]
- Wang, Y.-H.; Wu, D.-B.; Chen, B.; Chen, E.-Q.; Tang, H. Progress in mesenchymal stem cell–based therapy for acute liver failure. Stem Cell Res. Ther. 2018, 9, 1–9. [Google Scholar] [CrossRef]
- Fattizzo, B.; Giannotta, J.A.; Barcellini, W. Mesenchymal Stem Cells in Aplastic Anemia and Myelodysplastic Syndromes: The “Seed and Soil” Crosstalk. Int. J. Mol. Sci. 2020, 21, 5438. [Google Scholar] [CrossRef]
- Ansboro, S.; Roelofs, A.J.; De Bari, C. Mesenchymal stem cells for the management of rheumatoid arthritis: immune modulation, repair or both? Curr. Opin. Rheumatol. 2017, 29, 201–207. [Google Scholar] [CrossRef]
- Uccelli, A.; Laroni, A.; Brundin, L.; Clanet, M.; Fernandez, O.; Nabavi, S.M.; Muraro, P.A.; Oliveri, R.S.; Radue, E.W.; Sellner, J.; et al. MEsenchymal StEm cells for Multiple Sclerosis (MESEMS): a randomized, double blind, cross-over phase I/II clinical trial with autologous mesenchymal stem cells for the therapy of multiple sclerosis. Trials 2019, 20, 1–13. [Google Scholar] [CrossRef]
- Volkman, R.; Offen, D. Concise Review: Mesenchymal Stem Cells in Neurodegenerative Diseases. Stem Cells 2017, 35, 1867–1880. [Google Scholar] [CrossRef]
- Lo Furno, D.; Mannino, G.; Giuffrida, R. Functional role of mesenchymal stem cells in the treatment of chronic neurodegenerative diseases. J. Cell. Physiol. 2018, 233, 3982–3999. [Google Scholar] [CrossRef]
- Dasari, V.R.; Veeravalli, K.K.; Dinh, D.H. Mesenchymal stem cells in the treatment of spinal cord injuries: A review. World J. Stem Cells 2014, 6, 120–133. [Google Scholar] [CrossRef]
- Xu R, Feng Z, Wang FS. Mesenchymal stem cell treatment for COVID-19. eBioMedicine [Internet]. 2022 Mar 1 [cited 2023 Jan 22];77. Available from: https://www.thelancet. 2352.
- Kelly, K.; Rasko, J.E.J. Mesenchymal Stromal Cells for the Treatment of Graft Versus Host Disease. Front. Immunol. 2021, 12. [Google Scholar] [CrossRef] [PubMed]
- Liu, S.; Liu, F.; Zhou, Y.; Jin, B.; Sun, Q.; Guo, S. Immunosuppressive Property of MSCs Mediated by Cell Surface Receptors. Front. Immunol. 2020, 11, 1076. [Google Scholar] [CrossRef] [PubMed]
- Matula, Z.; Németh, A.; Lőrincz, P.; Szepesi, A.; Brózik, A.; Buzás, E.I.; Lőw, P.; Német, K.; Uher, F.; Urbán, V.S. The Role of Extracellular Vesicle and Tunneling Nanotube-Mediated Intercellular Cross-Talk Between Mesenchymal Stem Cells and Human Peripheral T Cells. Stem Cells Dev. 2016, 25, 1818–1832. [Google Scholar] [CrossRef] [PubMed]
- Li, H.; Wang, C.; He, T.; Zhao, T.; Chen, Y.-Y.; Shen, Y.-L.; Zhang, X.; Wang, L.-L. Mitochondrial Transfer from Bone Marrow Mesenchymal Stem Cells to Motor Neurons in Spinal Cord Injury Rats via Gap Junction. Theranostics 2018, 9, 2017–2035. [Google Scholar] [CrossRef]
- Bernardo, M.E.; Fibbe, W.E. Mesenchymal Stromal Cells: Sensors and Switchers of Inflammation. Cell Stem Cell 2013, 13, 392–402. [Google Scholar] [CrossRef]
- Eljarrah A, Gergues M, Pobiarzyn PW, Sandiford OA, Rameshwar P. Therapeutic Potential of Mesenchymal Stem Cells in Immune-Mediated Diseases. Adv Exp Med Biol. 2019;1201:93–108.
- Galleu, A.; Riffo-Vasquez, Y.; Trento, C.; Lomas, C.; Dolcetti, L.; Cheung, T.S.; von Bonin, M.; Barbieri, L.; Halai, K.; Ward, S.; et al. Apoptosis in mesenchymal stromal cells induces in vivo recipient-mediated immunomodulation. Sci. Transl. Med. 2017, 9. [Google Scholar] [CrossRef]
- Cheung, T.S.; Bertolino, G.M.; Giacomini, C.; Bornhaeuser, M.; Dazzi, F.; Galleu, A. Mesenchymal Stromal Cells for Graft Versus Host Disease: Mechanism-Based Biomarkers. Front. Immunol. 2020, 11, 1338. [Google Scholar] [CrossRef] [PubMed]
- Cheung, T.S.; Galleu, A.; von Bonin, M.; Bornhäuser, M.; Dazzi, F. Apoptotic mesenchymal stromal cells induce prostaglandin E2 in monocytes: implications for the monitoring of mesenchymal stromal cell activity. Haematologica 2019, 104, e438–e441. [Google Scholar] [CrossRef]
- Huang, Y.; Wu, Q.; Tam, P.K.H. Immunomodulatory Mechanisms of Mesenchymal Stem Cells and Their Potential Clinical Applications. Int. J. Mol. Sci. 2022, 23, 10023. [Google Scholar] [CrossRef]
- Kyurkchiev D, Bochev I, Ivanova-Todorova E, Mourdjeva M, Oreshkova T, Belemezova K, et al. Secretion of immunoregulatory cytokines by mesenchymal stem cells. World J Stem Cells. 2014 Nov 26;6(5):552–70.
- Jiang, W.; Xu, J. Immune modulation by mesenchymal stem cells. Cell Prolif. 2019, 53, e12712. [Google Scholar] [CrossRef]
- Molnar, V.; Pavelić, E.; Vrdoljak, K.; Čemerin, M.; Klarić, E.; Matišić, V.; Bjelica, R.; Brlek, P.; Kovačić, I.; Tremolada, C.; et al. Mesenchymal Stem Cell Mechanisms of Action and Clinical Effects in Osteoarthritis: A Narrative Review. Genes 2022, 13, 949. [Google Scholar] [CrossRef]
- Galipeau, J.; Sensébé, L. Mesenchymal Stromal Cells: Clinical Challenges and Therapeutic Opportunities. Cell Stem Cell 2018, 22, 824–833. [Google Scholar] [CrossRef]
- Fu, X.; Liu, G.; Halim, A.; Ju, Y.; Luo, Q.; Song, G. Mesenchymal Stem Cell Migration and Tissue Repair. Cells 2019, 8, 784. [Google Scholar] [CrossRef]
- Zeisbrich, M.; Becker, N.; Benner, A.; Radujkovic, A.; Schmitt, K.; Beimler, J.; Ho, A.D.; Zeier, M.; Dreger, P.; Luft, T. Transplant-associated thrombotic microangiopathy is an endothelial complication associated with refractoriness of acute GvHD. Bone Marrow Transplant. 2017, 52, 1399–1405. [Google Scholar] [CrossRef]
- Luft, T.; Dietrich, S.; Falk, C.; Conzelmann, M.; Hess, M.; Benner, A.; Neumann, F.; Isermann, B.; Hegenbart, U.; Ho, A.D.; et al. Steroid-refractory GVHD: T-cell attack within a vulnerable endothelial system. Blood 2011, 118, 1685–1692. [Google Scholar] [CrossRef]
- George, J.N.; Li, X.; McMinn, J.R.; Terrell, D.R.; Vesely, S.K.; Selby, G.B. Thrombotic thrombocytopenic purpura-hemolytic uremic syndrome following allogeneic HPC transplantation: a diagnostic dilemma. Transfusion 2004, 44, 294–304. [Google Scholar] [CrossRef]
- Wall, S.A.; Zhao, Q.; Yearsley, M.; Blower, L.; Agyeman, A.; Ranganathan, P.; Yang, S.; Wu, H.; Bostic, M.; Jaglowski, S.; et al. Complement-mediated thrombotic microangiopathy as a link between endothelial damage and steroid-refractory GVHD. Blood Adv. 2018, 2, 2619–2628. [Google Scholar] [CrossRef]
- Young, J.A.; Pallas, C.R.; Knovich, M.A. Transplant-associated thrombotic microangiopathy: theoretical considerations and a practical approach to an unrefined diagnosis. Bone Marrow Transplant. 2021, 56, 1805–1817. [Google Scholar] [CrossRef]
- Li Y, Lin F. Decoy nanoparticles bearing native C5a receptors as a new approach to inhibit complement-mediated neutrophil activation. Acta Biomater. 2019 Nov;99:330–8.
- Moll G, Rasmusson-Duprez I, von Bahr L, Connolly-Andersen AM, Elgue G, Funke L, et al. Are Therapeutic Human Mesenchymal Stromal Cells Compatible with Human Blood? Stem Cells. 2012 Jul 1;30(7):1565–74.
- Moll, G.; Ankrum, J.A.; Kamhieh-Milz, J.; Bieback, K.; Ringdén, O.; Volk, H.-D.; Geissler, S.; Reinke, P. Intravascular Mesenchymal Stromal/Stem Cell Therapy Product Diversification: Time for New Clinical Guidelines. Trends Mol. Med. 2019, 25, 149–163. [Google Scholar] [CrossRef]
- Li, Y.; Lin, F. Mesenchymal stem cells are injured by complement after their contact with serum. Blood 2012, 120, 3436–3443. [Google Scholar] [CrossRef]
- Li, Y.; Qiu, W.; Zhang, L.; Fung, J.; Lin, F. Painting factor H onto mesenchymal stem cells protects the cells from complement- and neutrophil-mediated damage. Biomaterials 2016, 102, 209–219. [Google Scholar] [CrossRef]
- Soland MA, Bego M, Colletti E, Zanjani ED, Jeor SS, Porada CD, et al. Mesenchymal Stem Cells Engineered to Inhibit Complement-Mediated Damage. PLOS ONE. 2013 Mar 26;8(3):e60461.
- Moll, G.; Jitschin, R.; Von Bahr, L.; Rasmusson-Duprez, I.; Sundberg, B.; Lönnies, L.; Elgue, G.; Nilsson-Ekdahl, K.; Mougiakakos, D.; Lambris, J.D.; et al. Mesenchymal Stromal Cells Engage Complement and Complement Receptor Bearing Innate Effector Cells to Modulate Immune Responses. PLOS ONE 2011, 6, e21703. [Google Scholar] [CrossRef]
- Tu, Z.; Li, Q.; Bu, H.; Lin, F. Mesenchymal Stem Cells Inhibit Complement Activation by Secreting Factor H. Stem Cells Dev. 2010, 19, 1803–1809. [Google Scholar] [CrossRef]
- Ignatius, A.; Schoengraf, P.; Kreja, L.; Liedert, A.; Recknagel, S.; Kandert, S.; Brenner, R.E.; Schneider, M.; Lambris, J.D.; Huber-Lang, M. Complement C3a and C5a modulate osteoclast formation and inflammatory response of osteoblasts in synergism with IL-1β. J. Cell. Biochem. 2011, 112, 2594–2605. [Google Scholar] [CrossRef]
- Li, Y.; Fung, J.; Lin, F. Local Inhibition of Complement Improves Mesenchymal Stem Cell Viability and Function After Administration. Mol. Ther. 2016, 24, 1665–1674. [Google Scholar] [CrossRef]
- Zeiser, R.; von Bubnoff, N.; Butler, J.; Mohty, M.; Niederwieser, D.; Or, R.; Szer, J.; Wagner, E.M.; Zuckerman, T.; Mahuzier, B.; et al. Ruxolitinib for Glucocorticoid-Refractory Acute Graft-versus-Host Disease. New Engl. J. Med. 2020, 382, 1800–1810. [Google Scholar] [CrossRef]
- Patriarca, F.; Sperotto, A.; Damiani, D.; Morreale, G.; Bonifazi, F.; Olivieri, A.; Ciceri, F.; Milone, G.; Cesaro, S.; Bandini, G.; et al. Infliximab treatment for steroid-refractory acute graft-versus-host disease. . 2004, 89, 1352–9. [Google Scholar]
- Yalniz, F.F.; Hefazi, M.; McCullough, K.; Litzow, M.R.; Hogan, W.J.; Wolf, R.; Alkhateeb, H.; Kansagra, A.; Damlaj, M.; Patnaik, M.M. Safety and Efficacy of Infliximab Therapy in the Setting of Steroid-Refractory Acute Graft-versus-Host Disease. Biol. Blood Marrow Transplant. 2017, 23, 1478–1484. [Google Scholar] [CrossRef]
- Le Blanc, K.; Rasmusson, I.; Sundberg, B.; Götherström, C.; Hassan, M.; Uzunel, M.; Ringdén, O. Treatment of severe acute graft-versus-host disease with third party haploidentical mesenchymal stem cells. Lancet 2004, 363, 1439–1441. [Google Scholar] [CrossRef]
- Zhao, L.; Chen, S.; Yang, P.; Cao, H.; Li, L. The role of mesenchymal stem cells in hematopoietic stem cell transplantation: prevention and treatment of graft-versus-host disease. Stem Cell Res. Ther. 2019, 10, 1–13. [Google Scholar] [CrossRef]
- Kebriaei, P.; Hayes, J.; Daly, A.; Uberti, J.; Marks, D.I.; Soiffer, R.; Waller, E.K.; Burke, E.; Skerrett, D.; Shpall, E.; et al. A Phase 3 Randomized Study of Remestemcel-L versus Placebo Added to Second-Line Therapy in Patients with Steroid-Refractory Acute Graft-versus-Host Disease. Biol. Blood Marrow Transplant. 2020, 26, 835–844. [Google Scholar] [CrossRef]
- Murata, M.; Terakura, S.; Wake, A.; Miyao, K.; Ikegame, K.; Uchida, N.; Kataoka, K.; Miyamoto, T.; Onizuka, M.; Eto, T.; et al. Off-the-shelf bone marrow-derived mesenchymal stem cell treatment for acute graft-versus-host disease: real-world evidence. Bone Marrow Transplant. 2021, 56, 2355–2366. [Google Scholar] [CrossRef]
- A Fisher, S.; Cutler, A.; Doree, C.; Brunskill, S.J.; Stanworth, S.J.; Navarrete, C.; Girdlestone, J. Mesenchymal stromal cells as treatment or prophylaxis for acute or chronic graft-versus-host disease in haematopoietic stem cell transplant (HSCT) recipients with a haematological condition. Emergencias 2019, 2019, CD009768. [Google Scholar] [CrossRef]
- Murata, M.; Terakura, S.; Wake, A.; Miyao, K.; Ikegame, K.; Uchida, N.; Kataoka, K.; Miyamoto, T.; Onizuka, M.; Eto, T.; et al. Off-the-shelf bone marrow-derived mesenchymal stem cell treatment for acute graft-versus-host disease: real-world evidence. Bone Marrow Transplant. 2021, 56, 2355–2366. [Google Scholar] [CrossRef]
- Nachmias B, Zimran E, Avni B. Mesenchymal stroma/stem cells: Haematologists’ friend or foe? Br J Haematol. 2022;199(2):175–89.
- Zhang, J.; Chen, M.; Liao, J.; Chang, C.; Liu, Y.; Padhiar, A.A.; Zhou, Y.; Zhou, G. Induced Pluripotent Stem Cell-Derived Mesenchymal Stem Cells Hold Lower Heterogeneity and Great Promise in Biological Research and Clinical Applications. Front. Cell Dev. Biol. 2021, 9, 716907. [Google Scholar] [CrossRef]
- Li, Y.; Hao, J.; Hu, Z.; Yang, Y.-G.; Zhou, Q.; Sun, L.; Wu, J. Current status of clinical trials assessing mesenchymal stem cell therapy for graft versus host disease: a systematic review. Stem Cell Res. Ther. 2022, 13, 1–22. [Google Scholar] [CrossRef]
- Kebriaei, P.; Isola, L.; Bahceci, E.; Holland, K.; Rowley, S.; McGuirk, J.; Devetten, M.; Jansen, J.; Herzig, R.; Schuster, M.; et al. Adult Human Mesenchymal Stem Cells Added to Corticosteroid Therapy for the Treatment of Acute Graft-versus-Host Disease. Biol. Blood Marrow Transplant. 2009, 15, 804–811. [Google Scholar] [CrossRef]
- Jurado, M.; De La Mata, C.; Ruiz-García, A.; López-Fernández, E.; Espinosa, O.; Remigia, M.J.; Moratalla, L.; Goterris, R.; García-Martín, P.; Ruiz-Cabello, F.; et al. Adipose tissue-derived mesenchymal stromal cells as part of therapy for chronic graft-versus-host disease: A phase I/II study. Cytotherapy 2017, 19, 927–936. [Google Scholar] [CrossRef]
- Bloor AJC, Patel A, Griffin JE, Gilleece MH, Radia R, Yeung DT, et al. Production, safety and efficacy of iPSC-derived mesenchymal stromal cells in acute steroid-resistant graft versus host disease: a phase I, multicenter, open-label, dose-escalation study. Nat Med. 2020 Nov;26(11):1720–5.
- Galderisi U, Peluso G, Di Bernardo G. Clinical Trials Based on Mesenchymal Stromal Cells are Exponentially Increasing: Where are We in Recent Years? Stem Cell Rev Rep. 2022;18(1):23–36.
- Kurtzberg, J.; Abdel-Azim, H.; Carpenter, P.; Chaudhury, S.; Horn, B.; Mahadeo, K.; Nemecek, E.; Neudorf, S.; Prasad, V.; Prockop, S.; et al. A Phase 3, Single-Arm, Prospective Study of Remestemcel-L, Ex Vivo Culture-Expanded Adult Human Mesenchymal Stromal Cells for the Treatment of Pediatric Patients Who Failed to Respond to Steroid Treatment for Acute Graft-versus-Host Disease. Biol. Blood Marrow Transplant. 2020, 26, 845–854. [Google Scholar] [CrossRef]
- Introna, M.; Lucchini, G.; Dander, E.; Galimberti, S.; Rovelli, A.; Balduzzi, A.; Longoni, D.; Pavan, F.; Masciocchi, F.; Algarotti, A.; et al. Treatment of Graft versus Host Disease with Mesenchymal Stromal Cells: A Phase I Study on 40 Adult and Pediatric Patients. Biol. Blood Marrow Transplant. 2013, 20, 375–381. [Google Scholar] [CrossRef]
- Boome, L.C.J.T.; Mansilla, C.; E Van Der Wagen, L.; A Lindemans, C.; Petersen, E.J.; Spierings, E.; A Thus, K.; Westinga, K.; Plantinga, M.; Bierings, M.; et al. Biomarker profiling of steroid-resistant acute GVHD in patients after infusion of mesenchymal stromal cells. Leukemia 2015, 29, 1839–1846. [Google Scholar] [CrossRef]
- Pérez-Simon, J.A.; López-Villar, O.; Andreu, E.J.; Rifón, J.; Muntion, S.; Campelo, M.D.; Sánchez-Guijo, F.M.; Martinez, C.; Valcarcel, D.; Canizo, C.D. Mesenchymal stem cells expanded in vitro with human serum for the treatment of acute and chronic graft-versus-host disease: results of a phase I/II clinical trial. Haematologica 2011, 96, 1072–1076. [Google Scholar] [CrossRef]
- Servais, S.; Baron, F.; Lechanteur, C.; Seidel, L.; Selleslag, D.; Maertens, J.; Baudoux, E.; Zachee, P.; Van Gelder, M.; Noens, L.; et al. Infusion of bone marrow derived multipotent mesenchymal stromal cells for the treatment of steroid-refractory acute graft-versus-host disease: a multicenter prospective study. Oncotarget 2018, 9, 20590–20604. [Google Scholar] [CrossRef]
- Boberg, E.; Bahr, L.; Afram, G.; Lindström, C.; Ljungman, P.; Heldring, N.; Petzelbauer, P.; Legert, K.G.; Kadri, N.; Le Blanc, K. Treatment of chronic GvHD with mesenchymal stromal cells induces durable responses: A phase II study. STEM CELLS Transl. Med. 2020, 9, 1190–1202. [Google Scholar] [CrossRef]
- Martin, P.; Uberti, J.; Soiffer, R.; Klingemann, H.; Waller, E.; Daly, A.; Herrmann, R.; Kebriaei, P. Prochymal Improves Response Rates In Patients With Steroid-Refractory Acute Graft Versus Host Disease (SR-GVHD) Involving The Liver And Gut: Results Of A Randomized, Placebo-Controlled, Multicenter Phase III Trial In GVHD. Biol. Blood Marrow Transplant. 2010, 16, S169–S170. [Google Scholar] [CrossRef]
- Soder, R.P.; Dawn, B.; Weiss, M.L.; Dunavin, N.; Weir, S.; Mitchell, J.; Li, M.; Shune, L.; Singh, A.K.; Ganguly, S.; et al. A Phase I Study to Evaluate Two Doses of Wharton's Jelly-Derived Mesenchymal Stromal Cells for the Treatment of De Novo High-Risk or Steroid-Refractory Acute Graft Versus Host Disease. Stem Cell Rev. Rep. 2020, 16, 979–991. [Google Scholar] [CrossRef]
- Yi, H.G.; Yahng, S.-A.; Kim, I.; Lee, J.-H.; Min, C.-K.; Kim, J.H.; Kim, C.S.; Song, S.U. Allogeneic clonal mesenchymal stem cell therapy for refractory graft-versus-host disease to standard treatment: a phase I study. Korean J. Physiol. Pharmacol. 2016, 20, 63–67. [Google Scholar] [CrossRef]
- Kurtzberg, J.; Prockop, S.; Teira, P.; Bittencourt, H.; Lewis, V.; Chan, K.W.; Horn, B.; Yu, L.; Talano, J.-A.; Nemecek, E.; et al. Allogeneic Human Mesenchymal Stem Cell Therapy (Remestemcel-L, Prochymal) as a Rescue Agent for Severe Refractory Acute Graft-versus-Host Disease in Pediatric Patients. Biol. Blood Marrow Transplant. 2013, 20, 229–235. [Google Scholar] [CrossRef]
- Ringden, O.; Baygan, A.; Remberger, M.; Gustafsson, B.; Winiarski, J.; Khoein, B.; Moll, G.; Klingspor, L.; Westgren, M.; Sadeghi, B. Placenta-Derived Decidua Stromal Cells for Treatment of Severe Acute Graft-Versus-Host Disease. STEM CELLS Transl. Med. 2018, 7, 325–331. [Google Scholar] [CrossRef]
- Sadeghi B, Remberger M, Gustafsson B, Winiarski J, Moretti G, Khoein B, et al. Long-Term Follow-Up of a Pilot Study Using Placenta-Derived Decidua Stromal Cells for Severe Acute Graft-versus-Host Disease. Biol Blood Marrow Transplant. 2019 Oct 1;25(10):1965–9.
- Muroi, K.; Miyamura, K.; Ohashi, K.; Murata, M.; Eto, T.; Kobayashi, N.; Taniguchi, S.; Imamura, M.; Ando, K.; Kato, S.; et al. Unrelated allogeneic bone marrow-derived mesenchymal stem cells for steroid-refractory acute graft-versus-host disease: a phase I/II study. Int. J. Hematol. 2013, 98, 206–213. [Google Scholar] [CrossRef]
- Muroi, K.; Miyamura, K.; Okada, M.; Yamashita, T.; Murata, M.; Ishikawa, T.; Uike, N.; Hidaka, M.; Kobayashi, R.; Imamura, M.; et al. Bone marrow-derived mesenchymal stem cells (JR-031) for steroid-refractory grade III or IV acute graft-versus-host disease: a phase II/III study. Int. J. Hematol. 2015, 103, 243–250. [Google Scholar] [CrossRef] [PubMed]
- Herrmann, R.; Sturm, M.; Shaw, K.; Purtill, D.; Cooney, J.; Wright, M.; Phillips, M.; Cannell, P. Mesenchymal stromal cell therapy for steroid-refractory acute and chronic graft versus host disease: a phase 1 study. Int. J. Hematol. 2011, 95, 182–188. [Google Scholar] [CrossRef]
- Shen MZ, Liu XX, Qiu ZY, Xu LP, Zhang XH, Wang Y, et al. Efficacy and safety of mesenchymal stem cells treatment for multidrug-resistant graft-versus-host disease after haploidentical allogeneic hematopoietic stem cell transplantation. Ther Adv Hematol. 2022;13:20406207211072840.
- Kale, V.P. Application of “Primed” Mesenchymal Stromal Cells in Hematopoietic Stem Cell Transplantation: Current Status and Future Prospects. Stem Cells Dev. 2019, 28, 1473–1479. [Google Scholar] [CrossRef] [PubMed]
- Kim, D.S.; Jang, I.K.; Lee, M.W.; Ko, Y.J.; Lee, D.-H.; Lee, J.W.; Sung, K.W.; Koo, H.H.; Yoo, K.H. Enhanced Immunosuppressive Properties of Human Mesenchymal Stem Cells Primed by Interferon-γ. EBioMedicine 2018, 28, 261–273. [Google Scholar] [CrossRef]
- Sarsenova, M.; Kim, Y.; Raziyeva, K.; Kazybay, B.; Ogay, V.; Saparov, A. Recent advances to enhance the immunomodulatory potential of mesenchymal stem cells. Front. Immunol. 2022, 13, 1010399. [Google Scholar] [CrossRef]
- Vigo, T.; Procaccini, C.; Ferrara, G.; Baranzini, S.; Oksenberg, J.R.; Matarese, G.; Diaspro, A.; de Rosbo, N.K.; Uccelli, A. IFN-γ orchestrates mesenchymal stem cell plasticity through the signal transducer and activator of transcription 1 and 3 and mammalian target of rapamycin pathways. J. Allergy Clin. Immunol. 2016, 139, 1667–1676. [Google Scholar] [CrossRef] [PubMed]
- De Witte, S.F.H.; Franquesa, M.; Baan, C.C.; Hoogduijn, M.J. Toward Development of iMesenchymal Stem Cells for Immunomodulatory Therapy. Front. Immunol. 2016, 6, 648. [Google Scholar] [CrossRef] [PubMed]
- Noronha, N.D.C., Mizukami, A., Caliári-Oliveira, C., Cominal, J.G., Rocha, J.L.M., Covas, D.T., Swiech, K. and Malmegrim, K.C. Priming approaches to improve the efficacy of mesenchymal stromal cell-based therapies. Stem Cell Res Ther. 2019;10(1):131. [CrossRef]
- Wang, Q.; Yang, Q.; Wang, Z.; Tong, H.; Ma, L.; Zhang, Y.; Shan, F.; Meng, Y.; Yuan, Z. Comparative analysis of human mesenchymal stem cells from fetal-bone marrow, adipose tissue, and Warton's jelly as sources of cell immunomodulatory therapy. Hum. Vaccines Immunother. 2015, 12, 85–96. [Google Scholar] [CrossRef]
- Kanai, R.; Nakashima, A.; Doi, S.; Kimura, T.; Yoshida, K.; Maeda, S.; Ishiuchi, N.; Yamada, Y.; Ike, T.; Doi, T.; et al. Interferon-γ enhances the therapeutic effect of mesenchymal stem cells on experimental renal fibrosis. Sci. Rep. 2021, 11, 1–14. [Google Scholar] [CrossRef]
- Li, M.; Jiang, Y.; Hou, Q.; Zhao, Y.; Zhong, L.; Fu, X. Potential pre-activation strategies for improving therapeutic efficacy of mesenchymal stem cells: current status and future prospects. Stem Cell Res. Ther. 2022, 13, 1–21. [Google Scholar] [CrossRef] [PubMed]
- Croitoru-Lamoury J, Lamoury FMJ, Caristo M, Suzuki K, Walker D, Takikawa O, et al. Interferon-γ Regulates the Proliferation and Differentiation of Mesenchymal Stem Cells via Activation of Indoleamine 2,3 Dioxygenase (IDO). PLOS ONE. 2011 Feb 16;6(2):e14698.
- Noone, C.; Kihm, A.; English, K.; O'Dea, S.; Mahon, B.P. IFN-γ Stimulated Human Umbilical-Tissue-Derived Cells Potently Suppress NK Activation and Resist NK-Mediated Cytotoxicity In Vitro. Stem Cells Dev. 2013, 22, 3003–3014. [Google Scholar] [CrossRef] [PubMed]
- Ryan, J.M.; Barry, F.; Murphy, J.M.; Mahon, B.P. Interferon-γ does not break, but promotes the immunosuppressive capacity of adult human mesenchymal stem cells. Clin. Exp. Immunol. 2007, 149, 353–363. [Google Scholar] [CrossRef] [PubMed]
- Potapova, I.A.; Gaudette, G.R.; Brink, P.R.; Robinson, R.B.; Rosen, M.R.; Cohen, I.S.; Doronin, S.V. Mesenchymal Stem Cells Support Migration, Extracellular Matrix Invasion, Proliferation, and Survival of Endothelial Cells In Vitro. STEM CELLS 2007, 25, 1761–1768. [Google Scholar] [CrossRef] [PubMed]
- Bhang, S.H.; Lee, S.; Shin, J.-Y.; Lee, T.-J.; Kim, B.-S. Transplantation of Cord Blood Mesenchymal Stem Cells as Spheroids Enhances Vascularization. Tissue Eng. Part A 2012, 18, 2138–2147. [Google Scholar] [CrossRef] [PubMed]
- Kouroupis, D.; Correa, D. Increased Mesenchymal Stem Cell Functionalization in Three-Dimensional Manufacturing Settings for Enhanced Therapeutic Applications. Front. Bioeng. Biotechnol. 2021, 9. [Google Scholar] [CrossRef] [PubMed]
- Li, J.; Liu, Y.; Zhang, Y.; Yao, B.; Enhejirigala; Li, Z. ; Song, W.; Wang, Y.; Duan, X.; Yuan, X.; et al. Biophysical and Biochemical Cues of Biomaterials Guide Mesenchymal Stem Cell Behaviors. Front. Cell Dev. Biol. 2021, 9. [Google Scholar] [CrossRef] [PubMed]
- Liu, L.; He, Y.R.; Liu, S.J.; Hu, L.; Liang, L.C.; Liu, D.L.; Liu, L.; Zhu, Z.Q. Enhanced Effect of IL-1β-Activated Adipose-Derived MSCs (ADMSCs) on Repair of Intestinal Ischemia-Reperfusion Injury via COX-2-PGE2 Signaling. Stem Cells Int. 2020, 2020, 1–18. [Google Scholar] [CrossRef]
- Liu, H.; Zhu, X.; Cao, X.; Chi, A.; Dai, J.; Wang, Z.; Deng, C.; Zhang, M. IL-1β-primed mesenchymal stromal cells exert enhanced therapeutic effects to alleviate Chronic Prostatitis/Chronic Pelvic Pain Syndrome through systemic immunity. Stem Cell Res. Ther. 2021, 12, 1–21. [Google Scholar] [CrossRef]
- Yao, M.; Cui, B.; Zhang, W.; Ma, W.; Zhao, G.; Xing, L. Exosomal miR-21 secreted by IL-1β-primed-mesenchymal stem cells induces macrophage M2 polarization and ameliorates sepsis. Life Sci. 2020, 264, 118658. [Google Scholar] [CrossRef]
- McGeachy, M.J.; Cua, D.J.; Gaffen, S.L. The IL-17 Family of Cytokines in Health and Disease. Immunity 2019, 50, 892–906. [Google Scholar] [CrossRef] [PubMed]
- Sivanathan, K.N.; Rojas-Canales, D.; Grey, S.T.; Gronthos, S.; Coates, P.T. Transcriptome Profiling of IL-17A Preactivated Mesenchymal Stem Cells: A Comparative Study to Unmodified and IFN-γModified Mesenchymal Stem Cells. Stem Cells Int. 2017, 2017, 1–16. [Google Scholar] [CrossRef]
- Du-Rocher B, Binato R, de-Freitas-Junior JCM, Corrêa S, Mencalha AL, Morgado-Díaz JA, et al. IL-17 Triggers Invasive and Migratory Properties in Human MSCs, while IFNy Favors their Immunosuppressive Capabilities: Implications for the “Licensing” Process. Stem Cell Rev Rep. 2020 Dec 1;16(6):1266–79.
- Sivanathan, K.N.; Rojas-Canales, D.M.; Hope, C.M.; Krishnan, R.; Carroll, R.P.; Gronthos, S.; Grey, S.T.; Coates, P.T. Interleukin-17A-Induced Human Mesenchymal Stem Cells Are Superior Modulators of Immunological Function. STEM CELLS 2015, 33, 2850–2863. [Google Scholar] [CrossRef]
- Cheng, W.; Su, J.; Hu, Y.; Huang, Q.; Shi, H.; Wang, L.; Ren, J. Interleukin-25 primed mesenchymal stem cells achieve better therapeutic effects on dextran sulfate sodium-induced colitis via inhibiting Th17 immune response and inducing T regulatory cell phenotype. . 2017, 9, 4149–4160. [Google Scholar]
- Kook, Y.J.; Lee, D.H.; Song, J.E.; Tripathy, N.; Jeon, Y.S.; Jeon, H.Y.; Oliveira, J.M.; Reis, R.L.; Khang, G. Osteogenesis evaluation of duck’s feet-derived collagen/hydroxyapatite sponges immersed in dexamethasone. Biomater. Res. 2017, 21, 1–7. [Google Scholar] [CrossRef]
- Linares, G.R.; Chiu, C.-T.; Scheuing, L.; Leng, Y.; Liao, H.-M.; Maric, D.; Chuang, D.-M. Preconditioning mesenchymal stem cells with the mood stabilizers lithium and valproic acid enhances therapeutic efficacy in a mouse model of Huntington's disease. Exp. Neurol. 2016, 281, 81–92. [Google Scholar] [CrossRef]
- Wisel, S.; Khan, M.; Kuppusamy, M.L.; Mohan, I.K.; Chacko, S.M.; Rivera, B.K.; Sun, B.C.; Hideg, K.; Kuppusamy, P. Pharmacological Preconditioning of Mesenchymal Stem Cells with Trimetazidine (1-[2,3,4-Trimethoxybenzyl]piperazine) Protects Hypoxic Cells against Oxidative Stress and Enhances Recovery of Myocardial Function in Infarcted Heart through Bcl-2 Expression. J. Pharmacol. Exp. Ther. 2009, 329, 543–550. [Google Scholar] [CrossRef] [PubMed]
- Hackel A, Aksamit A, Bruderek K, Lang S, Brandau S. TNF-α and IL-1β sensitize human MSC for IFN-γ signaling and enhance neutrophil recruitment. Eur J Immunol. 2021;51(2):319–30.
- Philipp, D.; Suhr, L.; Wahlers, T.; Choi, Y.-H.; Paunel-Görgülü, A. Preconditioning of bone marrow-derived mesenchymal stem cells highly strengthens their potential to promote IL-6-dependent M2b polarization. Stem Cell Res. Ther. 2018, 9, 1–17. [Google Scholar] [CrossRef] [PubMed]
- Kim, Y.; Jin, H.J.; Heo, J.; Ju, H.; Lee, H.-Y.; Kim, S.; Lee, S.; Lim, J.; Jeong, S.Y.; Kwon, J.; et al. Small hypoxia-primed mesenchymal stem cells attenuate graft-versus-host disease. Leukemia 2018, 32, 2672–2684. [Google Scholar] [CrossRef]
- Samal, J.R.K.; Rangasami, V.K.; Samanta, S.; Varghese, O.P.; Oommen, O.P. Discrepancies on the Role of Oxygen Gradient and Culture Condition on Mesenchymal Stem Cell Fate. Adv. Healthc. Mater. 2021, 10, 2002058. [Google Scholar] [CrossRef]
- Waterman, R.S.; Tomchuck, S.L.; Henkle, S.L.; Betancourt, A.M. A New Mesenchymal Stem Cell (MSC) Paradigm: Polarization into a Pro-Inflammatory MSC1 or an Immunosuppressive MSC2 Phenotype. PLOS ONE 2010, 5, e10088. [Google Scholar] [CrossRef]
- Gordon, S.; Mantovani, A. Diversity and plasticity of mononuclear phagocytes. Eur. J. Immunol. 2011, 41, 2470–2472. [Google Scholar] [CrossRef] [PubMed]
- Qiu, Y.; Guo, J.; Mao, R.; Chao, K.; Chen, B.-L.; He, Y.; Zeng, Z.-R.; Zhang, S.-H.; Chen, M.-H. TLR3 preconditioning enhances the therapeutic efficacy of umbilical cord mesenchymal stem cells in TNBS-induced colitis via the TLR3-Jagged-1-Notch-1 pathway. Mucosal Immunol. 2017, 10, 727–742. [Google Scholar] [CrossRef]
- He X, Wang H, Jin T, Xu Y, Mei L, Yang J. TLR4 Activation Promotes Bone Marrow MSC Proliferation and Osteogenic Differentiation via Wnt3a and Wnt5a Signaling. PLOS ONE. 2016 Mar 1;11(3):e0149876.
- Rashedi, I.; Gómez-Aristizábal, A.; Wang, X.-H.; Viswanathan, S.; Keating, A. TLR3 or TLR4 Activation Enhances Mesenchymal Stromal Cell-Mediated Treg Induction via Notch Signaling. STEM CELLS 2016, 35, 265–275. [Google Scholar] [CrossRef] [PubMed]
- Linard, C.; Strup-Perrot, C.; Lacave-Lapalun, J.-V.; Benderitter, M. Flagellin preconditioning enhances the efficacy of mesenchymal stem cells in an irradiation-induced proctitis model. J. Leukoc. Biol. 2016, 100, 569–580. [Google Scholar] [CrossRef]
- Vijayan, A.; Rumbo, M.; Carnoy, C.; Sirard, J.-C. Compartmentalized Antimicrobial Defenses in Response to Flagellin. Trends Microbiol. 2018, 26, 423–435. [Google Scholar] [CrossRef]
- Sangiorgi, B.B.; Leão, V.; Schiavinato, J.L.d.S.; Orellana, M.D.; Zago, M.A.; Covas, D.T.; Panepucci, R.A.; Rego, E.M. TLR9 Priming Promotes Proliferation Of Mesenchymal Stem Cells and Restores The Immunosuppressive Activity Impaired By TLR4 Priming: Potential Involvement Of Non-Canonical NF-Kb Signaling. Blood 2013, 122, 2458–2458. [Google Scholar] [CrossRef]
- Alvites, R.; Branquinho, M.; Sousa, A.C.; Lopes, B.; Sousa, P.; Maurício, A.C. Mesenchymal Stem/Stromal Cells and Their Paracrine Activity—Immunomodulation Mechanisms and How to Influence the Therapeutic Potential. Pharmaceutics 2022, 14, 381. [Google Scholar] [CrossRef]
- Lee, B.-C.; Kang, K.-S. Functional enhancement strategies for immunomodulation of mesenchymal stem cells and their therapeutic application. Stem Cell Res. Ther. 2020, 11, 1–10. [Google Scholar] [CrossRef]
- Kang, H.K.; Sarsenova, M.; Kim, D.-H.; Kim, M.S.; Lee, J.Y.; Sung, E.-A.; Kook, M.G.; Kim, N.G.; Choi, S.W.; Ogay, V.; et al. Establishing a 3D In Vitro Hepatic Model Mimicking Physiologically Relevant to In Vivo State. Cells 2021, 10, 1268. [Google Scholar] [CrossRef]
- Sart, S.; Ma, T.; Li, Y. Preconditioning Stem Cells for In Vivo Delivery. BioResearch Open Access 2014, 3, 137–149. [Google Scholar] [CrossRef] [PubMed]
- Petrenko, Y.; Syková, E.; Kubinová, Š. The therapeutic potential of three-dimensional multipotent mesenchymal stromal cell spheroids. Stem Cell Res. Ther. 2017, 8, 94. [Google Scholar] [CrossRef]
- Vial, S.; Reis, R.L.; Oliveira, J.M. Recent advances using gold nanoparticles as a promising multimodal tool for tissue engineering and regenerative medicine. Curr. Opin. Solid State Mater. Sci. 2016, 21, 92–112. [Google Scholar] [CrossRef]
- Hung, H.-S.; Kung, M.-L.; Chen, F.-C.; Ke, Y.-C.; Shen, C.-C.; Yang, Y.-C.; Tang, C.-M.; Yeh, C.-A.; Hsieh, H.-H.; Hsu, S.-H. Nanogold-Carried Graphene Oxide: Anti-Inflammation and Increased Differentiation Capacity of Mesenchymal Stem Cells. Nanomaterials 2021, 11, 2046. [Google Scholar] [CrossRef] [PubMed]
- Fathi-Achachelouei, M.; Knopf-Marques, H.; da Silva, C.E.R.; Barthes, J.; Bat, E.; Tezcaner, A.; Vrana, N.E. Use of Nanoparticles in Tissue Engineering and Regenerative Medicine. Front. Bioeng. Biotechnol. 2019, 7, 113. [Google Scholar] [CrossRef] [PubMed]
- Bai, R.G.; Muthoosamy, K.; Manickam, S.; Hilal-Alnaqbi, A. Graphene-based 3D scaffolds in tissue engineering: fabrication, applications, and future scope in liver tissue engineering. Int. J. Nanomed. 2019, ume 14, 5753–5783. [Google Scholar] [CrossRef]
- Hnatiuk AP, Ong S, Olea FD, Locatelli P, Riegler J, Lee WH, et al. Allogeneic Mesenchymal Stromal Cells Overexpressing Mutant Human Hypoxia-Inducible Factor 1-α (HIF1-α) in an Ovine Model of Acute Myocardial Infarction. J Am Heart Assoc. 5(7):e003714.
- Yang, J.-X.; Zhang, N.; Wang, H.-W.; Gao, P.; Yang, Q.-P.; Wen, Q.-P. CXCR4 Receptor Overexpression in Mesenchymal Stem Cells Facilitates Treatment of Acute Lung Injury in Rats. J. Biol. Chem. 2015, 290, 1994–2006. [Google Scholar] [CrossRef] [PubMed]
- Nie, W.-B.; Zhang, D.; Wang, L.-S. Growth Factor Gene-Modified Mesenchymal Stem Cells in Tissue Regeneration. Drug Des. Dev. Ther. 2020, 14, 1241–1256. [Google Scholar] [CrossRef]
- Lee, S.; Kim, H.-S.; Roh, K.-H.; Lee, B.-C.; Shin, T.-H.; Yoo, J.-M.; Kim, Y.-L.; Yu, K.-R.; Kang, K.-S.; Seo, K.-W. DNA methyltransferase inhibition accelerates the immunomodulation and migration of human mesenchymal stem cells. Sci. Rep. 2015, 5, srep08020. [Google Scholar] [CrossRef]
- Silva-Carvalho, A.E.; Rodrigues, L.P.; Schiavinato, J.L.; Alborghetti, M.R.; Bettarello, G.; Simoes, B.P.; Neves, F.d.A.R.; Panepucci, R.A.; de Carvalho, J.L.; Saldanha-Araujo, F. GVHD-derived plasma as a priming strategy of mesenchymal stem cells. Stem Cell Res. Ther. 2020, 11, 1–12. [Google Scholar] [CrossRef]
- Oses, C.; Olivares, B.; Ezquer, M.; Acosta, C.; Bosch, P.; Donoso, M.; Léniz, P.; Ezquer, F. Preconditioning of adipose tissue-derived mesenchymal stem cells with deferoxamine increases the production of pro-angiogenic, neuroprotective and anti-inflammatory factors: Potential application in the treatment of diabetic neuropathy. PLOS ONE 2017, 12, e0178011. [Google Scholar] [CrossRef] [PubMed]
- Levy, M.; Huang, L.; Rossi, E.; Blandinières, A.; Israel-Biet, D.; Gaussem, P.; Bischoff, J.; Smadja, D.M. Treprostinil indirectly regulates endothelial colony forming cell angiogenic properties by increasing VEGF-A produced by mesenchymal stem cells. Arthritis Res. Ther. 2015, 114, 735–747. [Google Scholar] [CrossRef] [PubMed]
- Pourjafar M, Saidijam M, Mansouri K, Ghasemibasir H, Karimi dermani F, Najafi R. All-trans retinoic acid preconditioning enhances proliferation, angiogenesis and migration of mesenchymal stem cell in vitro and enhances wound repair in vivo. Cell Prolif. 2017;50(1):e12315.
- Zhang, R.; Yin, L.; Zhang, B.; Shi, H.; Sun, Y.; Ji, C.; Chen, J.; Wu, P.; Zhang, L.; Xu, W.; et al. Resveratrol improves human umbilical cord-derived mesenchymal stem cells repair for cisplatin-induced acute kidney injury. Cell Death Dis. 2018, 9, 965. [Google Scholar] [CrossRef] [PubMed]
- Yang, Z.; Concannon, J.; Ng, K.S.; Seyb, K.; Mortensen, L.J.; Ranganath, S.; Gu, F.; Levy, O.; Tong, Z.; Martyn, K.; et al. Tetrandrine identified in a small molecule screen to activate mesenchymal stem cells for enhanced immunomodulation. Sci. Rep. 2016, 6, 30263. [Google Scholar] [CrossRef]
- Kiselevskii MV, Vlasenko RYa, Stepanyan NG, Shubina IZh, Sitdikova SM, Kirgizov KI, et al. Secretome of Mesenchymal Bone Marrow Stem Cells: Is It Immunosuppressive or Proinflammatory? Bull Exp Biol Med. 2021 Dec 1;172(2):250–3.
- Munoz-Perez, E.; Gonzalez-Pujana, A.; Igartua, M.; Santos-Vizcaino, E.; Hernandez, R.M. Mesenchymal Stromal Cell Secretome for the Treatment of Immune-Mediated Inflammatory Diseases: Latest Trends in Isolation, Content Optimization and Delivery Avenues. Pharmaceutics 2021, 13, 1802. [Google Scholar] [CrossRef] [PubMed]
- Lai, P.; Chen, X.; Guo, L.; Wang, Y.; Liu, X.; Liu, Y.; Zhou, T.; Huang, T.; Geng, S.; Luo, C.; et al. A potent immunomodulatory role of exosomes derived from mesenchymal stromal cells in preventing cGVHD. J. Hematol. Oncol. 2018, 11, 135. [Google Scholar] [CrossRef] [PubMed]
- Collo, G.D.; Adamo, A.; Gatti, A.; Tamellini, E.; Bazzoni, R.; Kamga, P.T.; Tecchio, C.; Quaglia, F.M.; Krampera, M. Functional dosing of mesenchymal stromal cell-derived extracellular vesicles for the prevention of acute graft-versus-host-disease. STEM CELLS 2020, 38, 698–711. [Google Scholar] [CrossRef]
- Wang, L.; Gu, Z.; Zhao, X.; Yang, N.; Wang, F.; Deng, A.; Zhao, S.; Luo, L.; Wei, H.; Guan, L.; et al. Extracellular Vesicles Released from Human Umbilical Cord-Derived Mesenchymal Stromal Cells Prevent Life-Threatening Acute Graft-Versus-Host Disease in a Mouse Model of Allogeneic Hematopoietic Stem Cell Transplantation. Stem Cells Dev. 2016, 25, 1874–1883. [Google Scholar] [CrossRef] [PubMed]
- Zhang, B.; Yeo, R.W.Y.; Lai, R.C.; Sim, E.W.K.; Chin, K.C.; Lim, S.K. Mesenchymal stromal cell exosome–enhanced regulatory T-cell production through an antigen-presenting cell–mediated pathway. Cytotherapy 2018, 20, 687–696. [Google Scholar] [CrossRef]
- Fujii, S.; Miura, Y.; Fujishiro, A.; Shindo, T.; Shimazu, Y.; Hirai, H.; Tahara, H.; Takaori-Kondo, A.; Ichinohe, T.; Maekawa, T. Graft-Versus-Host Disease Amelioration by Human Bone Marrow Mesenchymal Stromal/Stem Cell-Derived Extracellular Vesicles Is Associated with Peripheral Preservation of Naive T Cell Populations. STEM CELLS 2018, 36, 434–445. [Google Scholar] [CrossRef]
Figure 1.
Schematic representation of the mechanism of MSCs in GVHD. Mesenchymal stem cells (MSCs) are believed to alleviate acute GVHD through a number of mechanisms. MSCs release anti-inflammatory cytokines, which can help reduce the inflammatory response associated with GVHD. In addition, MSCs can also modulate the immune system by decreasing T-cell activation and immunological memory, and by inducing T-cell apoptosis. MSCs have also been shown to reduce the production of pro-inflammatory mediators and promote the production of regulatory T-cells, which can suppress the immune system and reduce the severity of GVHD. Finally, MSCs can also promote tissue repair and regeneration, helping to restore damaged tissue that may have been caused by GVHD.
Figure 1.
Schematic representation of the mechanism of MSCs in GVHD. Mesenchymal stem cells (MSCs) are believed to alleviate acute GVHD through a number of mechanisms. MSCs release anti-inflammatory cytokines, which can help reduce the inflammatory response associated with GVHD. In addition, MSCs can also modulate the immune system by decreasing T-cell activation and immunological memory, and by inducing T-cell apoptosis. MSCs have also been shown to reduce the production of pro-inflammatory mediators and promote the production of regulatory T-cells, which can suppress the immune system and reduce the severity of GVHD. Finally, MSCs can also promote tissue repair and regeneration, helping to restore damaged tissue that may have been caused by GVHD.
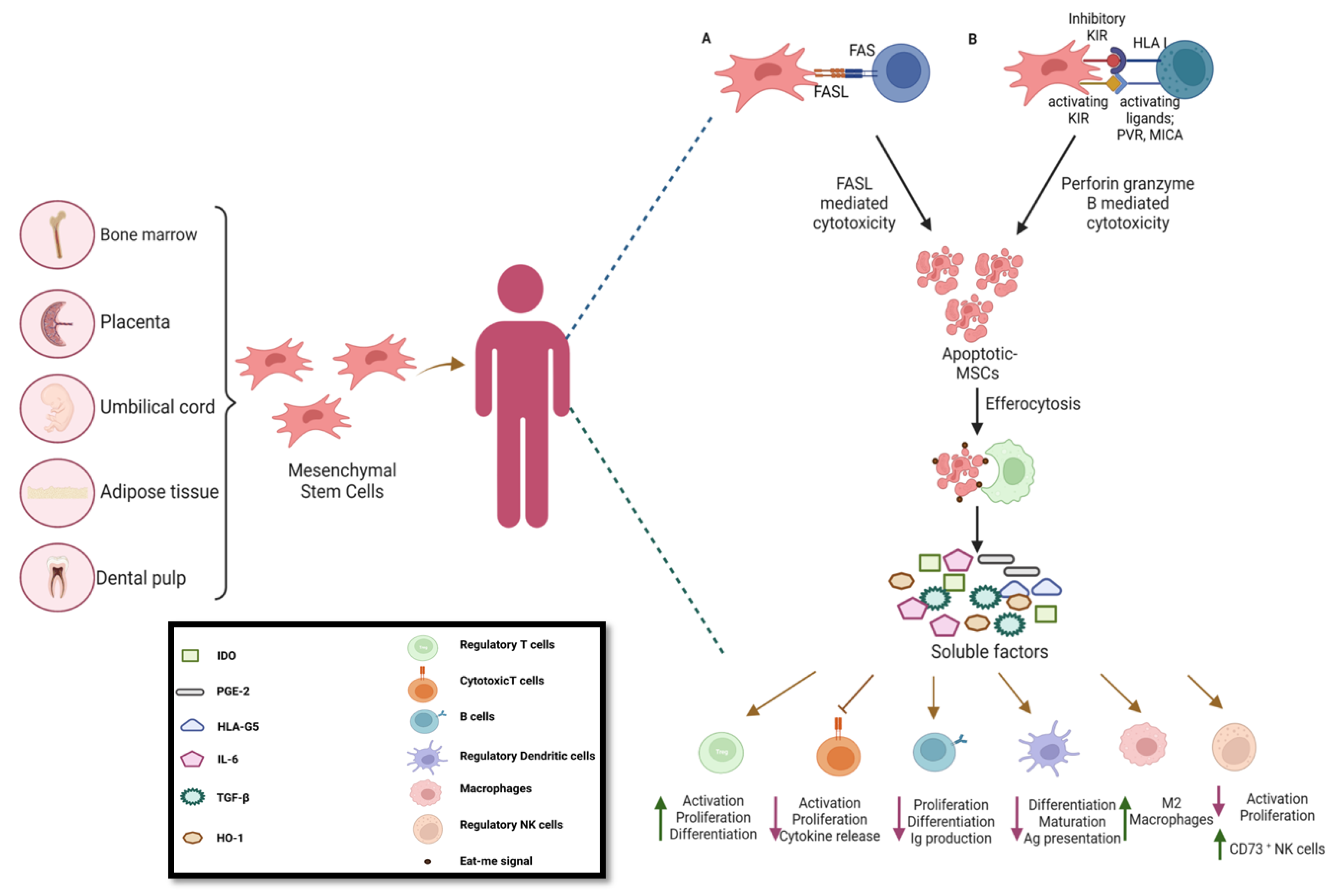
Figure 2.
An overview of available strategies for preconditioning of MSCs to enhance the immunomodulatory potential. Preconditioning of mesenchymal stem cells (MSCs) is the process of exposing them to certain conditions or stimuli that alter their state and behavior. This can be achieved through various methods, including hypoxia, chemical (growth factors, cytokines, and drugs), and genetic stimuli (introduction of genes, small molecules, and microRNAs).
Figure 2.
An overview of available strategies for preconditioning of MSCs to enhance the immunomodulatory potential. Preconditioning of mesenchymal stem cells (MSCs) is the process of exposing them to certain conditions or stimuli that alter their state and behavior. This can be achieved through various methods, including hypoxia, chemical (growth factors, cytokines, and drugs), and genetic stimuli (introduction of genes, small molecules, and microRNAs).

Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



