Submitted:
02 January 2023
Posted:
26 January 2023
You are already at the latest version
Abstract
There is evidence that behavioral risk factors such as western type diet, and life style can predispose to oxidative stress, deficiency in antioxidant status, hyperglycemia, dyslipidemia and increase in inflammation in tissues of various organs: beta cells of the pancreas, LDL receptors in the hepatocytes, endothelium, neurons, osteocytes and gut. Further studies indicate that diets rich in antioxidant flavonoids, omega-3 fatty acids and fiber in foods were inversely associated whereas western-type foods were positively associated with risk of mortality due to cardiovascular diseases (CVDs). One important cause for beneficial effects of diet may be certain foods and nutrients such as vegetables, fruits and whole grains that are rich in fiber and flavonoids, known to produce liters og molecular hydrogen in the gut. It seems that, high-fiber diets, prebiotic and probiotics can produce greater hydrogen, which acts as an antioxidant and may inhibit free radical generation. Recent studies indicate that molecular hydrogen can inhibit hydroxyl and nitrosyl radicals and can directly act as antioxidant in the cells and tissues, which can cause marked decline in oxidative stress and inflammation leading to significant decline in CVDs and metabolic diseases. Clinical and experimental studies indicate that hydrogen therapy such as hydrogen rich water can provide benefits in the management of CVDs and metabolic diseases. Larger studies are necessary to verify the role of hydrogen administration in CVDs.
Keywords:
Antioxidant
; free radical stress
; endothelial dysfunction
; dyslipidemia
; diet
Introduction
There is evidence that obesity, type 2 diabetes mellitus (T2DM) and cardiovascular diseases (CVDs) have become a major cause of mortality in several countries of the world [1,2,3]. The increase in risk of CVDs and T2DM, may be due to unhealthy diet, tobacco intake and alcoholism and decline in physical activity [1]. Majority of the risk factors, in particular, western diet, are known to predispose oxidative stress, due to decrease in antioxidant state in the body, leading to inflammation [4,5]. Thus, increase in systemic inflammation in the beta cells of the pancreas, LDL receptors in the hepatocytes, endothelium, neurons, osteocytes and gut may predispose CVDs and T2DM leading to increased mortality [6,7]. There are gaps in knowledge how oxidative stress associated with CVDs and metabolic disorders can be alleviated by increasing the intake of antioxidants. The hypothesis is that a healthy dietary pattern may regulate oxidative stress and inflammation and may maintain cell and tissue homeostasis, with decline in inflammation and risk of CVDs as well as metabolic diseases [8,9]. Western type diets, predisposes oxidative stress by elevating the levels of protein carbonylation and lipid peroxidation products [4,5] while reducing the antioxidant defense status, such as decreased production of molecular hydrogen in the gut. It is possible that certain foods and nutrients present in the Mediterranean type of diets, such as dietary fiber, flavonoids and omega-3 fatty acids [10], may generate or may be helpful in producing protective molecules in the gut [11], such as molecular hydrogen, which is known to be a potential antioxidant [12,14]. The exact mechanisms, how molecular hydrogen provide protective effects is still unknown. However, there is evidence that increased supplementation of molecular hydrogen can decrease oxidative stress and inflammation, which may be protective against CVDs as well as metabolic diseases [10,11,12,13,14,15]. This communication aims to highlight the role of molecular hydrogen, in the management of cardio-metabolic diseases (CMDs).
Free Radical Stress and Antioxidants in the Pathogenesis of Chronic Diseases
The substances that generate free radicals can be found in the western foods, pollution and other harmful lifestyle factors. For example, western diet, fried and fast foods, alcoholism, tobacco smoke, pesticides, radiation, and pollutants can all generate free radicals [4,5,12,13,14]. The body tissues are under constant attack from oxidative stress, because inhaled oxygen undergoes single electron reduction to form superoxide radicals (O2-). This radical can initiate radical propagation, and also be converted to hydrogen peroxide (H2O2) and hydroxyl radicals (·OH) [15]. Free oxygen radicals are characterized as having an unpaired electron, which makes them very reactive as they seek another electron to have a stable pair. These free oxygen radicals scavenge the body tissue to seek out other electrons, so they can become a pair, which causes damage to cells, proteins, lipoproteins and DNA resulting in diseases [15].
In the body, numerous free radicals, reactive oxygen species (ROS) and reactive nitrogen species are produced due to endogenous oxidants, exposure to different physiochemical conditions or pathological processes [15]. Balance is needed between free radicals and antioxidant status for proper metabolic function, so that there is no increase in oxidative stress, which is known to damage the tissues resulting in CVDs and T2DM [8,9,12,13,14]. Butylated hydroxytoluene and butylated hydroxyanisole are synthetic antioxidants used as food additives to prevent peroxidation of foods that are known to be hazardous for human health [4,5,15]. Hydroxyl and nitrosyl radicals represent the major cause of the destruction of body tissues, either by a direct reaction, or by triggering a chain reaction of free radicals [4,5,15]. Diets rich in antioxidants can do scavenging of free radicals that may act preventively or therapeutically. A number of antioxidants reacting with free radicals have been found in the Mediterranean type of diets, to serve as scavengers, which increase the internal endogenous potential of antioxidant status to protect tissues against oxidative damage [8,9]. However, western diet is poor in antioxidant nutrients and may produce free radical stress and inflammation leading to CVDs and T2DM [4,5].
There is evidence that physiological levels of free radicals are protective for cells,hence endogenous antioxidants are crucial to prevent free radical-induced damage to tissues [4,5]. Therefore, there is a focused attention toward the role of free radical biochemistry and free radical biology. in the physiology and metabolism as well as in the pathogenesis of chronic diseases [4,5]. It seems that xanthine oxidase, nicotinamide adenine dinucleotide phosphate (NADPH) oxidase, and leakage of electron from the respiratory chain of mitochondria, are crucial in damaging the cells by superoxide radical [16,17]. These free radicals attenuate the biological presence of NO by neutralizing it via conversion to a more detrimental peroxy-nitrite radical. The oxidases that enzymatically generate H2O2 and superoxide, are accumulated in the proteins related to Nox family, the main source of vascular free radicals [16,17,18,19]. The shear stress in the vessels activates the Nox proteins; Nox 1, Nox2 and Nox3 that are considered to have crucial role in vascular function [18,19]. The superoxide radicals are particularly produced via Nox1 and Nox2 via a single transfer of electron to hydrogen molecule. The superoxide radical reacts rapidly in the cells, to inactivate excess of NO, that produces perozxynitrite, known to have adverse effects on the vasodilation induced by nitric oxide[19]. In such situations of oxidative dysfunction in the presence of peroxynitrite, it may inhibit the release of endothelial nitric oxide synthase (eNOS) enzymes causing decline in the production of NO. The cofactor of eNOS, tetrahydrobiopterin (BH4), responsible for oxidation may inactive it to, 7,8-dihydropterin (BH2), causing uncoupling of eNOS. and this mechanism, generates the superoxide. Molecular hydrogen has been found to be useful in protecting against free radical induced damage due to its potential antioxidant effects in various conditions [20,21,22,23,24,25,26,27,28,29].
Diet as Oxidant and Antioxidant Agent
Increased intake of western-type foods in conjunction with low dietary antioxidants results in deficiency of antioxidant nutrients in tissues, along with endogenous antioxidants deficiency, leading to marked increase in free radical stress-induced tissue damage in the body [4,5,12,13,14]. Catalase, superoxide dismutase and ceruloplasmin are important endogenous antioxidants that are protective against damage to cholesterol receptors in the hepatocytes, beta cells of the pancreas, and endothelial damage by inhibiting free radical generation [9]. The variations in blood pressure and blood flow can influence endothelial function, thereby maintaining the appropriate vasomotor tone because the endothelium in the arteries have active function that work to modulate shear stress [13]. Endothelial dysfunction may be associated with accumulation of oxidative stress-induced vascular damage with inflammation, which may predispose to atherosclerosis and CVDs [13]. Endothelium-derived relaxing factors (EDRF), such as nitric oxide (NO), endothelium-derived hyperpolarization factor (EDHF) and prostacyclin are known to play a crucial role in the development of diet induced vascular dysfunction [4,5].
There is evidence that western type diet is deficient in antioxidant nutrients such as favonoida, fiber and omega-3 fatty acids, leading to decreased production of molecular hydrogen in the gut [4,5,14,15]. Previous studies also indicated that western type of diets, poor in dietary fiber, may also cause a decline in gut microbiota known to produce protective molecules: short chain fatty acids, glucagon like peptides and molecular hydrogen (H2), which are potential anti-inflamm- atory agents [13,14,15]. Recent studies have shown that Mediterranean type of diets that are rich in antioxidants such vitamins, minerals, flavonoids, omega-3 fatty acids and fiber can inhibit oxidative stress and inflammation resulting in to decline in CVDs and T2DM [4,5,8,9]. Diets rich in antioxidants, are also known to enhance the production of molecular hydrogen in the gut, which may regulate circadian variations in blood pressure [9,13,14,15]. Molecular hydrogen has been demonstrated to inhibit free radical stress in subjects with endothelial dysfunction as well as other CVDs and diabetes, that occur, due to oxidative stress [14,15]. Figure 1.
Production of Molecular Hydrogen in the Gut
Dietary approaches consisting of Mediterranean-style foods, yoghurt, and butter milk are used to alter the composition and improve function of the communities of the microbes that develop colonies in the gut for improvement of health, and protect against CVDs and T2DM [8,9]. In view of the known beneficial effects of hydrogen therapy [20,21,22,23,24,25,26,27,28,29], there is a need to understand how it is produced in the gut. A pilot study reported increased production of intestinal hydrogen along with recovery in muscle function following intensive exercises [30]. A previous study found that acetate mediates a microbiome–brain–β- cell axis to promote metabolic syndrome [31], whereas increased generation of metabolites such as short chain fatty acids, BDNF and hydrogen from gut microbiota enhance benefits in the metabolism via gut-brain neural circuits [32]. Since all the Mediterranean type of diets rich in fiber promote the growth of gut microbiota, hydrogen is produced in liter quantities by the intestinal bacteria if the individual has a healthy bacterial population and eats a diet of healthy fibers and probiotics [33,34,35]. There is an intensified search for effective, nontoxic natural compounds such as hydrogen, with potential anti-oxidant activity for prevention of CVDs and other chronic diseases [12,13,14,15]. It seems that after the discovery of the biological significance of the molecular hydrogen produced in the intestines, there has been a dramatic shift from the belief that hydrogen has a critical role in global organ function and homeostasis [14,15,16,17].
In the last two decades, it has become increasingly clear that molecular hydrogen, either produced endogenously via consuming healthy foods or via any releasing agents, administered exogenously via inhalation or hydrogen rich water (HRW), acts as potential antioxidant in a wide range of physiological and pathophysiological processes [16,17]. Molecular hydrogen is in itself a potential antioxidant that can also inhibit hydroxyl and nitrosyl radicals in the cells and tissues, causing a marked decline in oxidative stress, leading to a decline in the inflammation that is marker in the pathogenesis of diabetes and CVDs. This potential of molecular hydrogen may be utilized for preventive and therapeutic applications. Slezak et al. and other experts [12,13,14,15] have demonstrated that hydrogen can rapidly diffuse into tissues and cells without affecting metabolic redox reactions and signaling reactive species [12,13,14,15] (Figure 2).
Apart from its direct neutralizing effects on reactive oxidants, hydrogen, directly decreases free radical stress by regulation of expression of genes [16,17]. It seems that molecular hydrogen not only regulate gene expression but also does epigenetic modulation, which could be alternative mechanisms for decline in oxidative stress-induced damage to genes, resulting in to increase in its anti-inflammatory and anti-apoptotic potential [16,17]. Molecular hydrogen appears to be an effective antioxidant for the prevention of CVDs and other chronic diseases in which oxidative stress-related damage is the major problem [16,17]. Hydrogen also alleviates blood-brain barrier impairment and improves cognitive dysfunction [23]. Hydrogen therapy has been found to ameliorate cardiac remodeling [24], dyslipidemia and metabolic syndrome [25] oxygen saturation in chronic lung disease [26] and in NSAID-induced enteropathy [27]. Hydrogen therapy as combine treatment showed beneficial effects in facial paralysis [28], on physical fatigue via prefrontal cortex activation during and after high intensity exercise [29]. microbial conversion of by
Molecular Hydrogen Production by Gastrointestinal Microbiota
The microbiota in the gastrointestinal tract, is crucial in the prevention of diabetes and CVDs. Most of the complex carbohydrates and plant polysaccharides are undigested in the human gut due to the absence of enzymes [32]. There are several biochemical pathways by which microbes convert the complex polysaccharides into monosaccharides, that are mediated by the enzymatic actions. The microbes present in the gut can metabolize several of these polysaccharides into more useful fatty acids. These short-chain fatty acids (SCFAs), have potential anti-inflammatory effects and they are; propionate, butyrate, acetate, and gases; methane and hydrogen. Hydrogen gas in the body is produced through fermentation of carbohydrates – such as lactose, lactulose, and fructose by intestinal bacteria. The bacteria normally present in the large intestine are mainly Bacteroides fragilis group, Clostridium perfringens, Pseudomonas that possess hydrogenases to produce hydrogen. The presence of SCFAs in the gut indicates that fermentation due to microbes, occurs in the colon; with a greater level in the proximal colon but lower in the distal colon. The region of distal colon may have the highest number of microbes and with highest level of gases. The microbiota generates acetate and other metabolites, which can modulate neural function in the brain [31,32] (Figure 3).
The hydrogen production in the gastrointestinal tract in man is primarily dependent upon the delivery of ingested, fermentable fibrous substrates to an abundant intestinal flora [33]. This is normally present mainly in the colon and produce relatively large amounts of H2. The removal of excess hydrogen through methanogenesis from the gut is not the only microbial mechanism to remove excess hydrogen from the gut; this can also be mediated through the reduction of sulphate to sulphide by sulphate-reducing bacteria. The hydrogen produced in this way should significantly outweigh the effect of hydrogen administered in the hydrogen-rich water. At least one explanation is possible applying the “keystone pathogen” hypothesis [34]. Certain low-abundance microbial pathogens may orchestrate inflammatory disease by remodeling a normally benign microbiota into a dysbiotic one [34]. Keystone microorganisms that support and stabilize a microbiota associated with disease states are “keystone pathogens”. And the presence of such microorganisms in the human microbiotas may result in disease. A substantial body of literature now supports a role for “keystone” pathogens that provoke inflammation by remodeling the microbiota [35]. There is evidence that, Citrobacter rodentium causes in mice global changes in microbial community structure, apparently dependent upon the ability of this pathogen to cause inflammation. Chemical induction of gut inflammation by administration of dextran sodium sulfate leads to a dysbiotic microbiota, suggesting an intimate relationship between the inflammatory status of the intestine and gut microbiota. The oxidation of LDL by myeloperoxidase and reactive nitrogen species can cause free radical generation which may be protected by antioxidants produced by the gut microbiota [40].
Molecular Hydrogen Therapy for Cardiovascular Diseases
All the risk factors of CVDs act by damaging the cardiomyocytes, vasculature, including endothelium and smooth muscle cells, resulting in to cardiovascular dysfunction leading to CVDs. It seems that myocardial remodeling and fibrosis, as component of healing are the important function of hydrogen therapy that can influence the outcomes in patients with myocardial infarction [24]. The amount of fibrosis and apoptosis are closely related to the occurrence of heart failure. Therefore, novel therapeutic approaches for the treatment of cardiac remodeling and fibrosis of myocardium are important for increased survival of patients with cardiac ischemia. In an experimental study in rats with myocardial infarction, the rats were administered inhalation of 2 % hydrogen for a duration of 28 days, (daily for 3 hours) [24]. The findings revealed that treatment with hydrogen may cause significant improvement in the function of the heart with decline in the area of fibrosis. The in-vitro experiments also showed that Hydrogen therapy has also been found to decrease the damage due to hypoxia in the cardiac cells and also inhibit migration and activation of cardiac fibroblasts caused by angiotensin II. It is possible that hydrogen exerts special beneficial effect via reducing pyroptosis mediated by NLRP3.
NO is released from the endothelium which may be assessed via examination of the flow-mediated dilation that occur due to hyperemia caused by occlusion of artery. It could be a method of choice for measuring the bioavailability of NO obtained from the endothelium of the brachial artery. This technique can assess the effects of cardiovascular risk factors on endothelial dysfunction, including tobacco, aging, diabetes, and hypertension, as well as hyperglycemia after meals. It seems that the oxidative stress may be increased in presence of all these conditions causing endothelial dysfunction due to redox imbalance. It seems that reactive oxygen species (ROS) have important role in the development of vascular disease, which may also modulate vasomotor function in most of the vessels [13]. Thus the imbalance in the redox state between NO and superoxide radical produced in the endothelial cells may be crucial in causing endothelial dysfunction. Another ROS; H2O2 may cause either detrimental or beneficial influence on vascular function. The role of hydroxyl radical, produced as byproduct of decay of hydrogen peroxide is unclear, although it is known that it causes impairment in the endothelium, which can be neutralized by molecular hydrogen [13]. In a clinical study, treatment with hydrogen therapy was associated with significant rise in flow-mediated dilatation in the group receiving high hydrogen from 6.80%±1.96% to 7.64%±1.68% (mean ± SD) and a decrease from 8.07%±2.41% to 6.87%±2.94% in the placebo group. There was a significant beneficial effect in the ratio of FMD in the high-H2 group than to the control group [13].
It is possible that treatment with hydrogen may protect the vasculature from shear stress-derived detrimental hydroxyl radical by maintaining the nitric oxide-mediated vasomotor response. Since oxidative stress enhances systemic inflammation, it may damage the function of cardiomyocyte and beta cells as well as neurons, apart from endothelium. Figure 4.
Apart from the classical risk factors of coronary artery disease (CAD); hypertension, high lipids, T2DM, or smoking, rheumatoid arthritis, can also predispose to atherosclerosis, which often occurs independently of these factors [36,37]. Reactive oxygen species are generated as an essential co-factors in the oxidative phosphorylation via electron transfer at the time of aerobic metabolism [13,14,15]. CAD and atherosclerosis are important complications of rheumatoid arthritis, that predisposes CVDs with increased deaths in these patients. The cascades of inflammation are common to both rheumatoid arthritis and CAD, free radical stress and pro-inflammatory cytokines appear to be major cause of interrelation with these diseases. It seems that the pro-inflammatory mechanisms may influence the vascular endothelium as well as joint tissues in arthritis. The endothelial cells and smooth muscle cells produce superoxide radical through mechanism of Nox including Nox1, Nox2, Nox4, and Nox5, that are considered crucial in the function of the endothelium and progression of atherosclerosis, concerned with the ROS [36,37,38,39]. The oxidation of low density lipoprotein(LDL) cholesterol, observed at the intersection of the mechanisms, predispose development of plaque in atherosclerosis, leading to high CVD risk [40,41]. The development of CAD or stroke in patients with arthritis may be predisposed by alteration of endothelial phenotypic response to high quantity of harmful stimuli. Oxidative stress initiates greater expression of adhesion molecules; vascular cell adhesion molecule-1 (VCAM-1), intercellular adhesion molecules 1 (ICAM-1), and E-selectin. The pro-inflammatory cytokines (TNF-α, IL-1, interferon-γ, are also activated in the pathogenesis of atherosclerosis [36,37,38,39,40,41]. Interestingly, vascular dysfunction may also occur due to up-regulation of TNFα expression alone, leading to atherosclerosis. There is evidence, that TNFα, administration (80 or 240 ng/min for 30 min), was associated with an acute vascular inflammation, causing impairment in the endothelial structure [42]. In patients with rheumatoid arthritis, anti-TNFα therapies could improve the progression of atherosclerosis, indicating that the pathogenesis of atherosclerosis involves shared TNFα/ROS inflammatory pathways at the crossing between Loop 1 and 2 [43]. Further studies by Slezak and his group [44,45,46,47,48,49] have illustrated the role of molecular hydrogen in hypoxic post-conditioning, radiation-induced heart injury, mediastinal irradiation in rats, acute cardiac injury, radiation-induced heart disease and changes in microRNA-1, -15b and -21 levels in irradiated rat hearts.
It seems that superoxide radical is the primary product among highly active ROS that are released into the extracellular matrix with sequestration within lysosomes. There is spontaneous conversion of superoxide to hydrogen peroxide, that may also be via catalysis under availability of superoxide dismutase (SOD). The beneficial effects of molecular hydrogen for a wide range of disease models and human diseases have been investigated since 2007 [50,51,52,53,54,55,56]. Ichihara et al. [14] reviewed that approximately more than 321 articles have been published from China, Japan and the USA during 2007 to June 2015. Approximately three-quarters of the articles are on experimental studies showing the effects of molecular hydrogen in mice and rats. The studies included on effect of hydrogen water, hydrogen saline, or hydrogen gas via inhalation and during inhalation, hydrogen gas (< 4%) is administered. In many early studies, inhibition of peroxynitrite and hydroxyl radical were reported, but the scavenging of free radicals is not the sole action of hydrogen, because it is not solely accountable for its substantial effects. The effects of molecular hydrogen may be due to modulation of expressions of various molecules, for example; Nox1, NF-κB p65, IκBα, STAT3, NFATc1, c-Fos, Lyn, ERK, p38, JNK, ASK1, Akt, GTP-Rac1, iNOS, , and ghrelin [14,50,51,52,53,54,55,56]. However, the master regulator(s) that drive these modifications remain to be elucidated and are currently being extensively investigated.
Effects of Hydrogen in Stroke
The medicinal value of hydrogen has been shown by inhalation of 2% hydrogen which can significantly decrease the damage of cerebral ischemia/reperfusion caused by oxidative stress via selective elimination of hydroxyl radical (·OH) and peroxynitrite anion (ONOOˉ) [56,57,58,59,60,61,62,63]. Numerous experimental and clinical studies involving the mechanisms underlying hydrogen therapy indicate its anti-oxygenation, anti-inflammation, and anti-apoptosis effects. Since brain tissue is highly susceptible to cell damage, produced by free radicals and other markers, it may be easier to demonstrate the beneficial effects of hydrogen therapy in patients predisposed to stroke [56,57,58,59,60,61,62,63]. A single comprehensive review accounting for the blood-brain barrier, penetrability, possible side effects, and the molecular properties of hydrogen, should contribute to advancing both clinical and experimental research and therapies. In clinical studies, upon ischemic stroke onset, 8.5-30% of patients suffer a hemorrhagic stroke and the others have an ischemic stroke. In animals, small doses of hydrogen can significantly reduce mortality in cases of ischemic strokes that target the entire brain. In both the high-sugar and tMCAO groups, due to its suppressive effects, the risk of brain hemorrhage was reduced upon hydrogen administration. After persistent hydrogen inhalation (2.9%) for 2 hours, oxidation and nitration products and matrix metalloproteinases-9 (MMP-9) showed a significant decline, indicating protection of the blood brain-barrier [56,57,58,59,60,61,62,63]. Chen et al. [59] proposed that this effect contributed to the lower occurrence of hemorrhage accompanying cerebral infarction. In an experimental study, intraperitoneal injection of hydrogen-rich saline during persistent middle cerebral artery occlusion (pMCAO) conformed to continuous ischemia of vessels, showed an elevation in the action of antioxidant enzymes with a decline in infarction areas [57]. Another clinical trial on brain stem infarction showed that treatment with hydrogen and edaravone can cut down recovery time significantly better than using edaravone alone [63].
A hemorrhagic stroke is defined as a cerebral hemorrhage followed by compression and necrosis of brain tissue [60]. Hemorrhagic strokes are typically more dangerous than ischemic strokes because they are characterized by microglia and inflammatory cells, which are activated upon hemorrhage, producing free radicals [61]. In an intracerebral model for mice, inhalation of 2% hydrogen for 1 hour reduced the degree of cerebral edema and improved neural function significantly, though only for 72 hours, suggesting that hydrogen inhalation provides protection only in the acute phase from hemorrhage [62]. This was speculated to be due to neutrophil infiltration and microglial activation, not peaking until after 72 hours, and anti-oxygenation of hydrogen not persistent or sufficient at that time [62]. Lastly, infiltration and activation of mastocytes play an important role in inflammatory responses during the initial stages of stroke, because hydrogen protects the blood-brain barrier and decreases cerebral edema by amelioration of mastocytes activity [62,63]. In an experiment of acute hyperglycemia in rat, treatment with hydrogen-rich saline was associated with increased hemorrhagic transformation in a focal ischemia [59].
Effects of Molecular Hydrogen on Blood Lipoproteins
Increased concentrations of blood lipids and pro-inflammatory cytokines are risk factors of CVDs. Clinical and experimental studies indicate that hydrogen administration has beneficial lipid-lowering effects. In a case study of 20 patients of metabolic syndrome, HRW (0.9-1.0 l/day) was administered to determine its effects on biological activities of serum lipoproteins [34,54]. The intake of HRW for 10 weeks showed a decline in total-cholesterol (TC) and LDL-cholesterol (LDL-C) concentrations. There was also a significant decline in apoE, and apolipoprotein (apo)B100 and improvement in function of HDL. The intake of HRW was associated with rise in superoxide dismutase enzyme and a reduction in thiobarbituric acid-reactive substances(TBARS) in the LDL and serum. These markers are important indicators of metabolic syndrome. In a clinical trial, 68 patients with high cholesterol randomized to either HRW(0.9L/day) (n = 34) or placebo (n = 34) for a total period of 10 weeks [35,55]. The HDL cholesterol isolated from the HRW group revealed an improved capability in the promotion of binding of ATP cholesterol efflux ex- vivo, concerned to cassette transporter A. There was an upregulation of plasma pre-β-HDL concentrations, without any alteration in HDL-cholesterol concentrations. Moreover, treatment with HRW was associated with improvement in other HDL functions, related to LDL oxidation, inhibition of pro-inflammatory oxidized-LDL, with protection of endothelial cells apoptosis. In addition, therapy with HRW was associated with the improved down-regulation of total cholesterol (47.06% vs. 17.65%) and LDL cholesterol (47.06% vs. 23.53%). There was a significant decline in apolipoprotein B100 with rise in apolipoprotein M in in the H2 group. Treatment with, H2 was associated with a marked decline in the concentrations of multiple pro- inflammatory markers and indicators of oxidative stress in the plasma and in the particle of HDL. The present results emphasize the potential efficacy of hydrogen therapy in the reduction of cholesterol as well as atherosclerosis.
Effects of Molecular Hydrogen in Diabetes Mellitus and Metabolic Syndrome.Metabolic syndrome is characterized by cardiometabolic risk factors that include obesity, insulin resistance, hypertension and dyslipidemia. Oxidative stress is known to play a major role in the pathogenesis of metabolic syndrome. The objective of this study was to examine the effectiveness of hydrogen rich water (1.5–2 L/day) in an open label, 8-week study on 20 subjects with potential metabolic syndrome. Hydrogen rich water was produced, by placing a metallic magnesium stick into drinking water (hydrogen concentration; 0.55–0.65 mM), by the following chemical reaction; Mg + 2H2O → Mg (OH)2 + H2. The consumption of hydrogen rich water for 8 weeks resulted in a 39% increase (p<0.05) in antioxidant enzyme superoxide dismutase (SOD) and a 43% decrease (p<0.05) in thiobarbituric acid reactive substances (TBARS) in urine. Further, subjects demonstrated an 8% increase in high density lipoprotein (HDL)-cholesterol and a 13% decrease in total cholesterol/HDL-cholesterol from baseline to week 4. There was no change in fasting glucose levels during the 8 week study. In conclusion, drinking hydrogen rich water represents a potentially novel therapeutic and preventive strategy for metabolic syndrome. The portable magnesium stick was a safe, easy and effective method of delivering hydrogen rich water for daily consumption by participants in the study.
Keywords: hydrogen, drinking water, magnesium, oxidative stress, metabolic syndrome
Metabolic syndrome may be defined as an accumulation of at least three risk factors out of obesity, diabetes, hypertension, hyperlipidemia and low HDL etc. It is possible that free radical stress with or without inflammation are crucial in the development of metabolic syndrome and T2DM [54,55,64]. Therapy with HRW can improve metabolism of glucose and lipids in T2DM patients or those with glucose intolerance because both conditions are associated with oxidative stress [64,65]. The effectiveness of hydrogen-rich water (1.5–2 L/day) was examined in an open label, 8-week study in 20 subjects with potential metabolic syndrome [64]. Hydrogen- rich water was produced by placing a metallic magnesium stick into drinking water (hydrogen concentration; 0.55–0.65 mM) by the following chemical reaction: Mg + 2H2O → Mg (OH)2 + H2. The consumption of hydrogen-rich water for 8 weeks resulted in a 39% increase (p<0.05) in antioxidant enzyme superoxide dismutase (SOD) and a 43% decrease (p<0.05) in thiobarbituric acid reactive substances (TBARS) in urine [64]. Further, subjects showed an 8% increase in high-density lipoprotein (HDL)-cholesterol and a 13% decrease in total cholesterol/HDL-cholesterol from reference to week 4. There was no change in fasting glucose concentrations during the 8-week study. Drinking hydrogen-rich water may represent a potentially novel therapeutic and preventive strategy for metabolic syndrome.
Singh's group did a randomized, controlled trial in which treatment with HRW showed favorable effects on multiple parameters after treatment for 24-week, as compared to control group (P < 0.05), (P = 0.309), with accompanied significant decline in the parameters of central obesity BMI and WHR after treatment with HRW (P < 0.05) [25]. In addition, treatment with HRW caused a significant decline in blood lipids as given in the Table 1.
Treatment with HRW also showed decline in fasting blood glucose after 24-week, in the active treatment group, along with a significant decline in HbA1C (12%, P < 0.05) compared to baseline levels and placebo group. Treatment with HRW also reduced the markers of inflammation; TNF-α, and IL-6 (P<0.05). Interestingly, markers of oxidation showed significant decline, while vitamins C and E showed rise in the hydrogen group. Serum levels of angiotensin converting enzyme showed significant decline whereas serum nitrite level showed significant increase, which may cause decline in blood pressures Table 2.
In a cross-over, randomized, controlled, trial in 30 patients with T2DM and 6 patients with impaired glucose tolerance, patients took either 900 mL/d of HRW or 900 mL of placebo water for 8 weeks, with a 12-week period of washout [65]. Intake of hydrogen-rich water was associated with a significant decline in the concentrations of modified LDL cholesterol (i.e., modifications that increase the net negative charge of LDL), small dense LDL, and urinary 8-isoprostanes by 15.5% (P < 0.01), 5.7% (P < 0.05), and 6.6% (P < 0.05), respectively. Hydrogen-rich water intake was also associated with a trend of decreased serum concentrations of oxidized LDL and free fatty acids, and increased plasma concentrations of adiponectin and extracellular-superoxide dismutase. These results suggest that supplementation with hydrogen-rich water may have a beneficial role in the prevention of T2DM and insulin resistance. Hydrogen may activate ATP-binding cassette transporter A1-dependent efflux, enhance HDL anti-atherosclerotic functions, and have beneficial lipid-lowering effects. Since metabolic syndrome has become a worldwide problem, hydrogen therapy may be a new approach for the prevention of CMDs [64,65,66,67,68]. A recent review has also reemphasized, that Indo-Mediterranean type of foods that can produce greater hydrogen may be a better option for prevention of hypertension [69].
Hydrogen therapy may positively affect mitochondrial bioenergetics. In a experimental study in rats, Gvozdjakova et al. reported, increased state 3 respiration with both CI and CII-linked substrates in cardiac mitochondria after H2 administration [70]. It is proposed that H2 may convert the quinone intermediates in the Q-cycle to the fully reduced ubiquinol, increasing this way antioxidant capacity of the quinone pool and preventing mitochondrial ROS generation [71].
The increase in the rate of ATP production was accompanied with increased concentration of CoQ9 in heart tissue and mitochondria and decreased plasma levels of malondialdehyde [71]. Beneficial effects of molecular hydrogen in various experimental models of human diseases and in many clinical studies was documented. H2 can be administered by various ways, as a gas inhalation, drinking of hydrogen-enriched water, or taking a hydrogen-dissolved bath as well as in saline infusions [70,71,72]. As antioxidant, hydrogen selectively scavenges hydroxyl and peroxynitrite radicals, and decreases oxidative stress, however, the hydrogen effect on antioxidant–coenzyme Q information is lacking. The results from recent studies, can contribute to the explanation of a new beneficial mechanism of hydrogen on a part of antioxidant protection in organism [71,72,73,74]. The hydrogen produced in the large intestine is metabolized, and excreted in the large intestine [72], by the microbes. [73]. The largest amount of hydrogen is produced by Blautia coccoides and Clostridium leptum. [73]. However, depending on microbiota composition, substantial amounts of hydrogen molecules are consumed by methanogenic and sulfate-reducing bacteria [73].
Conclusions
In brief, there is considerable evidence that hydrogen reacts with highly reactive oxidants, such as hydroxyl radical (•OH) and peroxynitrite (ONOO-) inside cells; but it has also its own antioxidant and anti-inflammatory effects. Hydrogen administration has been found beneficial in CVDs; atherosclerosis, stroke, hyperlipidemia and possibly in coronary artery disease and diabetes. Hydrogen concentrations can be monitored by gas chromatography. Since hydrogen rapidly diffuses into tissues and cells, its results show efficient effects, hence it has been proposed to have potential for preventive and therapeutic applications. There are several methods to ingest or consume hydrogen: inhaling H2 gas, drinking hydrogen-dissolved water (H2-water), injecting hydrogen-dissolved saline (H2-saline), taking an hydrogen bath, or dropping H2-saline onto the eyes. Hydrogen functions as an anti-inflammatory, anti-allergic, and anti-apoptotic molecule, and stimulates energy metabolism. Hydrogen therapy may differ from conventional pharmaceutical drugs because of its great efficacy. Hydrogen is mild enough neither disturbs metabolic redox reactions nor to affect signaling by reactive oxygen species. Hydrogen therapy, therefore, should have no or little adverse effects.
Authors Contributions
The first draft of the manuscript was made by RBS and VM which was read by SZ, JF, GF, VM, AT, OP, AG, KJL, KF, JV, BK, BK, JS and CSK. All coauthors made critical comments which were incorporated in the article.
Funding
This research received no external funding.
Institutional Review Board Statement
Ethical approval and permission not required as it is a review article.
Informed Consent Statement
Consent not required as it is a review article.
Data Availability Statement
Data support statement not required as it is a review article.
Acknowledgments
Are given to the Department of Gerontology and Geriatric, PJ Safarik University and MEDIPARK—University Research Park, from grant number: ITMS2014+: 313011AUB13001 by Slovak Research Agency, PJ Safarik University, Kosice, Slovakia, and to the International College of Nutrition and International College of Cardiology and the Tsimtsoum Institute, Krakow, Poland and Biovid: ITMS2014+: 313011AVG3“, for logistic support.
Conflict of interest
All the authors have declared that there is no conflict of interest. However, AT has conflict of interest that he is commercially involved with trading of HRW.
References
- Roth GA, Mensah GA, Johnson CO, Addolorato G, Ammirati E, Baddour LM, et al. Global burden of cardiovascular diseases and risk factors, 1990–2019: update from the GBD 2019 study. J Am Coll Cardiol. (2020) 76:2982–3021. [CrossRef]
- Roth GA, Abate D, Abate KH, Abay SM, Abbafati C, Abbasi N, et al. Global, regional, and national age-sex-specific mortality for 282 causes of death in 195 countries and territories, 1980–2017: a systematic analysis for the Global Burden of Disease Study 2017. Lancet. (2018) 392:1736–88. [CrossRef]
- Vaduganathan M, Mensah GA, Varieur Turco J, et al. The Global Burden of Cardiovascular Diseases and Risk: A Compass for Future Health. Journal of the American College of Cardiology. 12 December 2022. [CrossRef]
- Jiang S, Liu H, Li C. Dietary regulation of oxidative stress in chronic metabolic diseases. Foods. 2021 Aug 11;10(8):1854. [CrossRef]
- Aleksandrova K, Koelman L, Rodrigues CE. Dietary patterns and biomarkers of oxidative stress and inflammation: A systematic review of observational and intervention studies. Redox Biology, 2021; 42:101869.
- Micha R, Penalyo JL, Cidhea F, Imamura F, Rehm CD, Mozaffarian D. Association between dietary factors and mortality from heart disease, stroke, and type 2 diabetes in the United States. JAMA 2017; 317 (9): 912-924. [CrossRef]
- Sacco RL, Roth GA, Reddy KS, Arnett DK, Bonita R, Gaziano TA, Heidenreich PA, Huffman MD, Mayosi BM, Mendis S, Murray CJL, Perel P, Piñeiro DJ, Smith SC Jr, Taubert KA, Wood DA, Zhao D, Zoghbi WA. The heart of 25 by 25: achieving the goal of reducing global and regional premature deaths from cardiovascular diseases and stroke: a modeling study from the American Heart Association and World Heart Federation. Circulation 2016; 133: e674-e690. [CrossRef]
- Singh, R.B.; Fedacko, J.; Fatima, G.; Magomedova, A.; Watanabe, S.; Elkilany, G. Why and How the Indo-Mediterranean Diet May Be Superior to Other Diets: The Role of Antioxidants in the Diet. Nutrients 2022; 14, 898. [CrossRef]
- Singh, R.B.; Fedacko, J.; Pella, D.; Fatima, G.; Elkilany, G.; Moshiri, M.; Hristova, K.; Jakabcin, P.; Vanova, N. High Exogenous Antioxidant, Restorative Treatment (Heart) for Prevention of the Six Stages of Heart Failure: The Heart Diet. Antioxidants 2022, 11, 1464. [CrossRef]
- Mojto V, Singh RB, Gvozdjakova A, Pella D, Fedacko J, Pella D. Molecular hydrogen: a new approach for the management of cardiovascular diseases. World Heart J 2018;10: 83-93.
- Ichikawa Y, Yamamoto H, Hirano Si, Sato B, Takefuji Y, Satoh F. The overlooked benefits of hydrogen-producing bacteria. Med Gas Res 2022;12. [cited 2022 Dec 20]. Available from: https://www.medgasres.com/preprintarticle.asp?id=344977.
- Slezák, J.; Kura, B.; Frimmel, K.; Zálešák, M.; Ravingerová, T.; Viczenczová, C.; Okruhlicová, Ľ.; Tribulová, N. Preventive and therapeutic application of molecular hydrogen in situations with excessive production of free radicals. Physiol. Res. 2016; 65 (Suppl. 1): S11–S28.
- Sakai T, Sato B, Hara K, Hara Y, Naritomi Y, Koyanagi S, Hara H, Nagao T, Ishibashi T. Consumption of water containing over 3.5 mg of dissolved hydrogen could improve vascular endothelial function. Vascular Health and Risk Management 2014; 10: 591–597.
- Ichihara, M.; Sobue, S.; Ito, M.; Ito, M.; Hirayama, M.; Ohno, K. Beneficial biological effects and the underlying mechanisms of molecular hydrogen- Comprehensive review of 321 original articles. Med. Gas Res. 2015; 5: 1–21.
- Lobo V, Patil A, Phatak A, Chandra N. Free radicals, antioxidants and functional foods: Impact on human health. Pharmacognosy Reviews 2010; 4 (8): 118-126. [CrossRef]
- Takac I, Schroder K, Brandes RP. The Nox family of NADPH oxidases: friend or foe of the vascular system. Curr Hypertens Rep 2012; 14: 70–78.
- Montezano AC, Touyz RM. Reactive oxygen species and endothelial function role of nitric oxide synthase uncoupling and Nox family nicotinamide adenine dinucleotide phosphate oxidases. Basic Clin Pharmacol Toxicol 2012; 110: 87–94.
- Al Ghouleh I, Khoo NK, Knaus UG. Oxidases and peroxidases in cardiovascular and lung disease: new concepts in reactive oxygen species signaling. Free Radic Biol Med 2011; 51: 1271–1288.
- Bedard K, Krause KH. The NOX family of ROS-generating NADPH oxidases: physiology and pathophysiology. Physiol Rev 2007; 87: 245–313.
- Deryugina AV, Danilova DA, Brichkin YD, Taranov EV, Nazarov EI, Pichugin VV, Medvedev AP, Riazanov MV, Fedorov SA, Andrej YS, Makarov EV. Molecular hydrogen exposure improves functional state of red blood cells in the early postoperative period: a randomized clinical study.Med Gas Res. 2023 Apr-Jun;13(2):59-66. [CrossRef]
- Yang M, Dong Y, He Q, et al. Hydrogen: a novel option in human disease treatment. Oxid Med Cell Longev. 2020;2020:8384742. [CrossRef]
- Ohsawa I, Ishikawa M, Takahashi K, et al. Hydrogen acts as a therapeutic antioxidant by selectively reducing cytotoxic oxygen radicals. Nat Med. 2007;13(6):688-694. [CrossRef]
- Yu Y, Feng J, Lian N, et al. Hydrogen gas alleviates blood-brain barrier impairment and cognitive dysfunction of septic mice in an Nrf2-dependent pathway. Int Immunopharmacol. 2020;85:106585.
- Nie C, Zou R, Pan S, A R, Gao Y, Yang H, Bai J, Xi S, Wang X, Hong X, Yang W. Hydrogen gas inhalation ameliorates cardiac remodelling and fibrosis by regulating NLRP3 inflammasome in myocardial infarction rats. J Cell Mol Med. 2021 Sep;25(18):8997-9010. [CrossRef]
- LeBaron T, Singh RB, Fatima G, Kartikey K, Sharma JP, Ostojic SM, Gvozdjakova A, Kura B, Noda M, Mojto V, Niaz MA, Slezak J.The Effects of 24-Week, High-ConcentrationHydrogen-Rich Water on Body Composition, Blood Lipid Profiles and Inflammation Biomarkers in Men and Women with Metabolic Syndrome: A Randomized Controlled Trial. Diabetes, Metabolic Syndrome and Obesity: Targets and Therapy.2020;13:889-896.
- Singh RB, Halabi G, Fatima G, Rai RH, Tarnava AT, LeBaron TW. Molecular hydrogen as an adjuvant therapy may be associated with increased oxygen saturation and improved exercise tolerance in a COVID-19 patient. Clin Case Reports 9: e05039. 1 of 6. [CrossRef]
- Akita Y, Higashiyama M, Kurihara C, Ito S, Nishii S, Mizoguchi A, Inaba K, Tanemoto R, Sugihara N, Hanawa Y, Wada A, Horiuchi K, Okada Y, Narimatsu K, Komoto S, Tomita K, Takei F, Satoh Y, Saruta M, Hokari R. Ameliorating Role of Hydrogen-Rich Water Against NSAID-Induced Enteropathy via Reduction of ROS and Production of Short-Chain Fatty Acids.
- Dig Dis Sci. 2022 Dec 7:1-11. [CrossRef]
- Koyama Y, Harada S, Sato T, Kobayashi Y, Yanagawa H, Iwahashi T, Tanaka H, Ohata K, Imai T, Ohta Y, Kamakura T, Kobayashi H, Inohara H, Shimada S. Therapeutic strategy for facial paralysis based on the combined application of Si-based agent and methylcobalamin.
- Biochem Biophys Rep. 2022 Nov 21;32:101388. [CrossRef]
- Hong Y, Dong G, Li Q, Wang V, Liu M, Jiang G, Bao D, Zhou J. Effects of pre-exercise H2 inhalation on physical fatigue and related prefrontal cortex activation during and after high-intensity exercise. Front Physiol. 2022 Sep 2;13:988028. eCollection 2022. [CrossRef]
- Eda, N.; Tsuno, S.;Nakamura, N.; Sone, R.; Akama, T.;Matsumoto, M. Effects of Intestinal Bacterial Hydrogen Gas Production on Muscle Recovery following Intense Exercise in Adult Men: A Pilot Study. Nutrients 2022, 14, 4875. [CrossRef]
- Perry RJ, Peng L, Barry NA, Cline GW, Zhang D, Cardone RL, Petersen KF, Kibbey RG, Goodman AL, Shulman GI. Acetate mediates a microbiome–brain–β- cell axis to promote metabolic syndrome. Nature 2016; 534: 213-217. [CrossRef]
- De Vadder F, Kovatcheva-Datchary P, Goncalves D, Vinera J, Zitoun C, Duchampt A, Bäckhed F, Mithieux G. Microbiota-generated metabolites promote metabolic benefits via gut-brain neural circuits. Cell 2014; 156: 84-96. [CrossRef]
- Levitt MD. Excretion of hydrogen gas in man. N Engl J Med 1969; 281: 122-127. https://doi.org/10.1056/NEJM196907172810303.
- Hajishengallis G, Darveau RP, Curtis MA. The keystone-pathogen hypothesis. Nat Rev Microbiol 2012; 10 (10): 717–725. [CrossRef]
- Lupp C, Robertson ML, Wickham ME, Sekirov I, Champion OL, Gaynor EC, Finlay BB. Host-mediated inflammation disrupts the intestinal microbiota and promotes the overgrowth of Enterobacteriaceae. Cell Host Microbe 2007; 2: 119–129.
- Donovan SM. Introduction to the special focus issue on the impact of diet on gut microbiota composition and function and future opportunities for nutritional modulation of the gut microbiome to improve human health. Gut Microbes 2017; 8 (2): 75-81.
- LeBaron TW, Kura B, Kalocayova B, Tribulova N, Slezak J. A New Approach for the Prevention and Treatment of Cardiovascular Disorders. Molecular Hydrogen Significantly Reduces the Effects of Oxidative Stress. Molecules 2019; 24(11): 276. [CrossRef]
- LeBaron TW, Sharpe R, Ohno K. Electrolyzed-Reduced Water: Review I. Molecular Hydrogen Is the Exclusive Agent Responsible for the Therapeutic Effects. Int J Mol Sci. 2022 Nov 25;23 (23):14750. [CrossRef]
- Ohta, S. Recent Progress Toward Hydrogen Medicine: Potential of Molecular Hydrogen for Preventive and Therapeutic Applications. Curr. Pharm. Des. 2011; 17:2241-52.
- Carr AC, McCall MR, Frei B. Oxidation of LDL by myeloperoxidase and reactive nitrogen species: reaction pathways and antioxidant protection. Arterioscler Thromb Vasc Biol 2000;20: 1716–1723.
- Yoshida H, Kisugi R. Mechanisms of LDL oxidation. Clin Chim Acta 2010; 411: 1875–1882.
- Chia S, Qadan M, Newton R, Ludlam CA, Fox KA, Newby DE. Intra-arterial tumor necrosis factor-alpha impairs endothelium-dependent vasodilatation and stimulates local tissue plasminogen activator release in humans. Arterioscler Thromb Vasc Biol 2003; 23: 695–701.
- Szekanecz Z, Kerekes G, Soltesz P. Vascular effects of biologic agents in RA and spondyloarthropathies. Nat Rev Rheumatol 2009; 5: 677–684.
- Zálešák M, Kura B, Graban J, Farkašová V, Slezák J, Ravingerová T. Molecular hydrogen potentiates beneficial anti-infarct effect of hypoxic postconditioning in isolated rat hearts: Novel cardioprotective intervention. Can J Physiol Pharmacol 2017; 95 (8): 888-893. [CrossRef]
- Slezak J, Kura B, Babal P, Barancik M, Ferko M, Frimmel K, Kalocayova B, Kukreja RC, Lazou A, Mezesova L, Okruhlicova L, Ravingerova T, Singal PK, Szeiffova Bacova B, Viczenczova C, Vrbjar N, Tribulova N. Potential markers and metabolic processes involved in mechanism of radiation-induced heart injury. Can J Physiol Pharmacol 2017; 95 (10): 1190-1203. [CrossRef]
- Kura B, Bagchi AK, Akolkar G, Singal P, Slezák J. Myocardial changes after mediastinal irradiation in rats: molecular mechanisms and potential targets to minimize the adverse effects. In: Adaptation Biology and Medicine, Volume 8: Current Trends. New Delhi: Narosa Publishing House; 2017. pp. 93-122. ISBN 978-81-8487-567-6.
- Viczenczova C, Kura B, Chaudagar KK, Szeiffova Bacova B, Egan Benova T, Barancik M, Knezl V, Ravingerova T, Tribulova N, Slezak J. Myocardial connexin-43 is up-regulated in response to acute cardiac injury in rats. Can J Physiol Pharmacol 2017; 95 (10): 1190-1203. [CrossRef]
- Kura B, Babal P, Slezak J. Implication of microRNAs in the development and potential treatment of radiation-induced heart disease. Can J Physiol Pharmacol 2017; 95 (10): 1236-1244. [CrossRef]
- Kura B, Yin C, Frimmel K, Krizak J, Okruhlicova L, Kukreja RC, Slezak J. Changes of microRNA-1, -15b and -21 levels in irradiated rat hearts after treatment with potentially radioprotective drugs. Physiological Research 2016; 65 (Suppl. 1): S129-S137.
- Ohsawa I, Ishikawa M, Takahashi K, Watanabe M, Nishimaki K, Yamagata K, Katsura K, Katayama Y, Asoh S, Ohta S. Hydrogen acts as a therapeutic antioxidant by selectively reducing cytotoxic oxygen radicals. Nat Med 2007; 13 (6): 688-694.
- Ishibashi T. Molecular hydrogen: New antioxidant and anti-inflammatory therapy for rheumatoid arthritis and related diseases. Current Pharmaceutical Design 2013; 19: 6375-6381. [CrossRef]
- Ishibashi T, Sato B, Shibata S, Sakata T, Hara Y, Naritomi Y, Koyanagi S, Hara H, Nagao T. Therapeutic efficacy of infused molecular hydrogen in saline on rheumatoid arthritis: A randomized, double-blind placebo-controlled pilot study. Int Immunopharmacol 2014; 21: 468-473.
- Korovljev D, Trivic T, Drid P, Ostojic SM. Molecular hydrogen affects body composition, metabolic profiles, and mitochondrial function in middle-aged overweight women. Ir J Med Sci 2018; 187 (1): 85-89. [CrossRef]
- Song G, Li M, Sang H, Zhang L, Li X, Yao S, Yu Y, Zong C, Xue Y, Qin S. Hydrogen-rich water decrease serum low-density lipoprotein cholesterol levels and improves high density lipoprotein function in patients with potential metabolic syndrome. J Lipid Res 2013; 54: 1884-1893.
- Song G, Lin Q, Zhao H, Liu M, Ye F, Sun Y, Yu Y, Guo S, Jiao P, Wu Y, Ding G, Xiao Q, Qin S. Hydrogen activates ATP-binding cassette transporter A1-dependent efflux ex vivo and improves high-density lipoprotein function in patients with hypercholesterolemia: A double-blinded, randomized, and placebo-controlled trial. J Clin Endocrinol Metab 2015; 100 (7): 2724-2733. Epub 2015 May 15. [CrossRef]
- Liu CL, Zhang K, Chen G. Hydrogen therapy: from mechanism to cerebral diseases. Med Gas Res 2016; 6 (1): 48-54.
- Nagatani K, Wada K, Takeuchi S, Kobayashi H, Uozumi Y, Otani N, Fujita M, Tachibana S, Nawashiro H. Effect of hydrogen gas on the survival rate of mice following global cerebral ischemia. Shock (Augusta, Ga) 2012; 37: 645–652.
- Zhang Y, Sun Q, He B, Xiao J, Wang Z, Sun X. Anti-inflammatory effect of hydrogen-rich saline in a rat model of regional myocardial ischemia and reperfusion. Int J Cardiol 2011; 148: 91–95.
- Chen CH, Manaenko A, Zhan Y, Liu WW, Ostrowki RP, Tang J, Zhang JH. Hydrogen gas reduced acute hyperglycemia-enhanced hemorrhagic transformation in a focal ischemia rat model. Neuroscience 2010; 169: 402–414.
- Chen S, Yang Q, Chen G, Zhang JH. An update on inflammation in the acute phase of intracerebral hemorrhage. Transl Stroke Res 2015; 6: 4–8.
- Engelhardt B, Sorokin L. The blood-brain and the blood-cerebrospinal fluid barriers: function and dysfunction. Semin Immunopathol 2009; 31: 497–511.
- Manaenko A, Lekic T, Ma Q, Ostrowski RP, Zhang JH, Tang J. Hydrogen inhalation is neuroprotective and improves functional outcomes in mice after intracerebral hemorrhage. Acta Neurochir Suppl. 2011; 111: 179–183.
- Munakata A, Ohkuma H, Shimamura N. Effect of a free radical scavenger, edaravone, on free radical reactions: related signal transduction and cerebral vasospasm in the rabbit subarachnoid hemorrhage model. Acta Neurochir Suppl. 2011; 110: 17–22.
- Nakao A, Toyoda Y, Sharma P, Evans M, Guthrie N. Effectiveness of hydrogen rich water on antioxidant status of subjects with potential metabolic syndrome—an open label pilot study. Journal of Clinical Biochemistry and Nutrition 2010; 46 (2): 140-149. [CrossRef]
- Kajiyama S, Hasegawa G, Asano M, Hosoda H, Fukui M, Nakamura N, Kitawaki J, Imai S, Nakano K, Ohta M, Adachi T, Obayashi H, Yoshikawa T. Supplementation of hydrogen-rich water improves lipid and glucose metabolism in patients with type 2 diabetes or impaired glucose tolerance. Nutr Res 2008; 28 (3): 137-143. [CrossRef]
- Kamimura N, Ichimiya H, Iuchi K, Ohta S. Molecular hydrogen stimulates the gene expression of transcriptional coactivator PGC-1α to enhance fatty acid metabolism. NPJ Aging Mech Dis. 2016 Apr 28;2:16008. eCollection 2016. [CrossRef]
- Sobue S, Inoue C, Hori F, Qiao S, Murate T, Ichihara M. Molecular hydrogen modulates gene expression via histone modification and induces the mitochondrial unfolded protein response. Biochem Biophys Res Commun. 2017 Nov 4;493(1):318-324. Epub 2017 Sep 7. [CrossRef]
- Singh RB, Fedacko J, Saboo B, Niaz MA, Maheshwari A, Verma N, Bharadwaj K. Association of higher omega-6/omega-3 fatty acids in the diet with higher prevalence of metabolic syndrome in North India. MOJ Public Health. 2017; 6 (6): 00193. [CrossRef]
- Singh, R.B.; Nabavizadeh, F.; Fedacko, J.; Pella, D.; Vanova, N.; Jakabcin, P.; Fatima, G.; Horuichi, R.;Takahashi, T.; Mojto, V.; et al. Dietary Approaches to Stop Hypertension viaIndo-Mediterranean Foods, May Be Superior to DASH Diet Intervention.Nutrients 2023, 15, 46. [CrossRef]
- Gvozdjáková A, Kucharská J, Kura B, Vančová O, Rausová Z, Sumbalová Z, Uličná O, Slezák J. A new insight into the molecular hydrogen effect on coenzyme Q and mitochondrial function of rats. Can J Physiol Pharmacol. 2020 Jan;98(1):29-34. [CrossRef]
- Kucharská J, Gvozdjáková A, Kura B, et al. Effect of molecular hydrogen on coenzyme Q in plasma, myocardial tissue and mitochondria of rats. J Nutr Health Food Eng. 2018;8(5): 362‒364. [CrossRef]
- Christl SU, Murgatroyd PR, Gibson GR, Cummings JH. Production, metabolism, and excretion of hydrogen in the large intestine. Gastroenterology. 1992,102(4 Pt 1):1269-77.
- Suzuki A, Ito M, Hamaguchi T, Mori H, Takeda Y, Baba R, Watanabe T, Kurokawa K, Asakawa S, Hirayama M, Ohno K. Quantification of hydrogen production by intestinal bacteria that are specifically dysregulated in Parkinson's disease. PLoS One. 2018, 13(12):e0208313. [CrossRef]
- Ishibashi T. Therapeutic Efficacy of Molecular Hydrogen: A New Mechanistic Insight. Curr Pharm Des. 2019;25(9):946-955. [CrossRef]
Figure 1.
Mechanisms of diet on oxidative stress and inflammation with reference to molecular hydrogen, on development of cardiovascular and metabolic diseases.
Figure 1.
Mechanisms of diet on oxidative stress and inflammation with reference to molecular hydrogen, on development of cardiovascular and metabolic diseases.
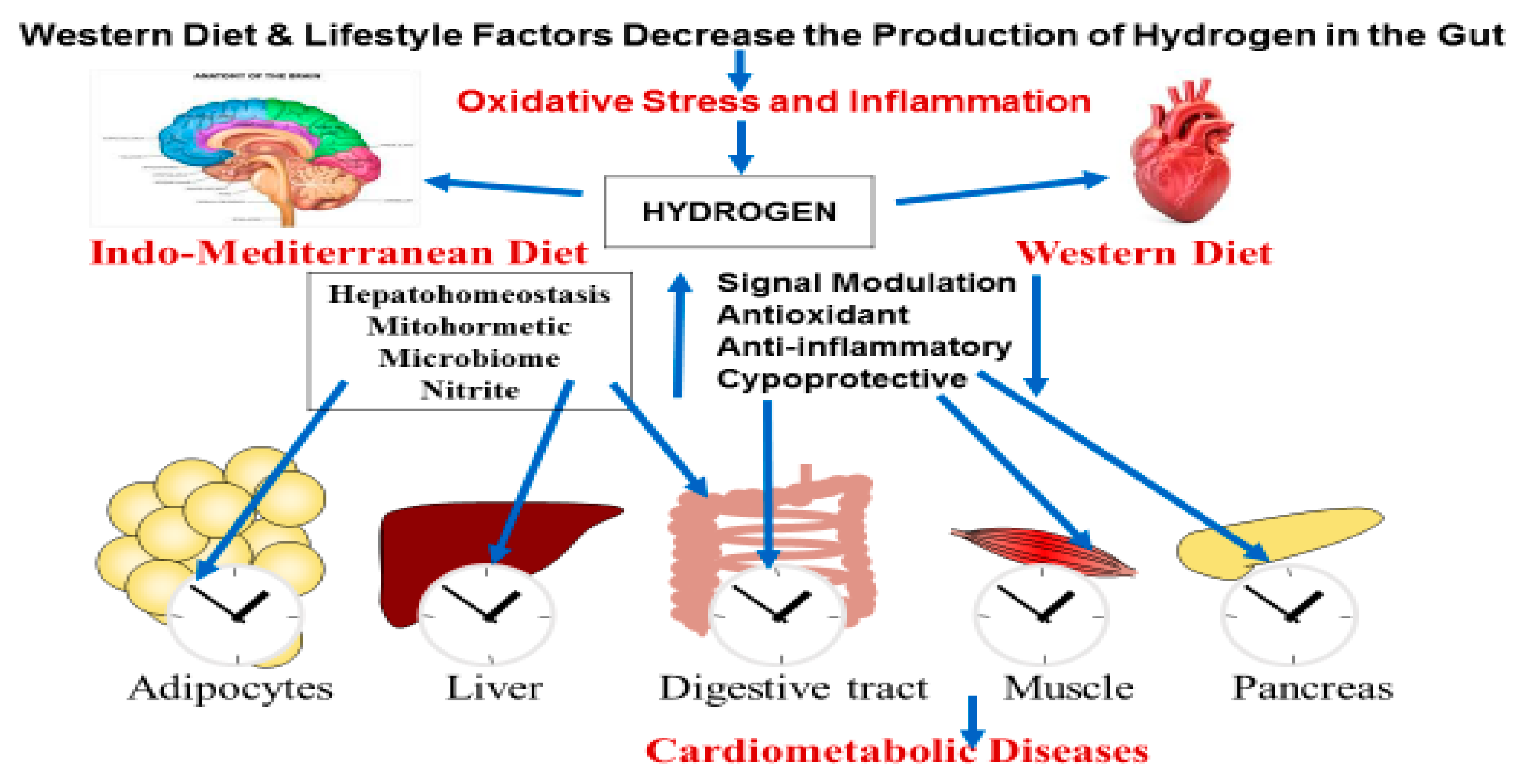
Figure 2.
Mechanism of action of molecular hydrogen in the pathogenesis and control of cardiovascular and metabolic diseases (Modified from reference [14]).
Figure 2.
Mechanism of action of molecular hydrogen in the pathogenesis and control of cardiovascular and metabolic diseases (Modified from reference [14]).
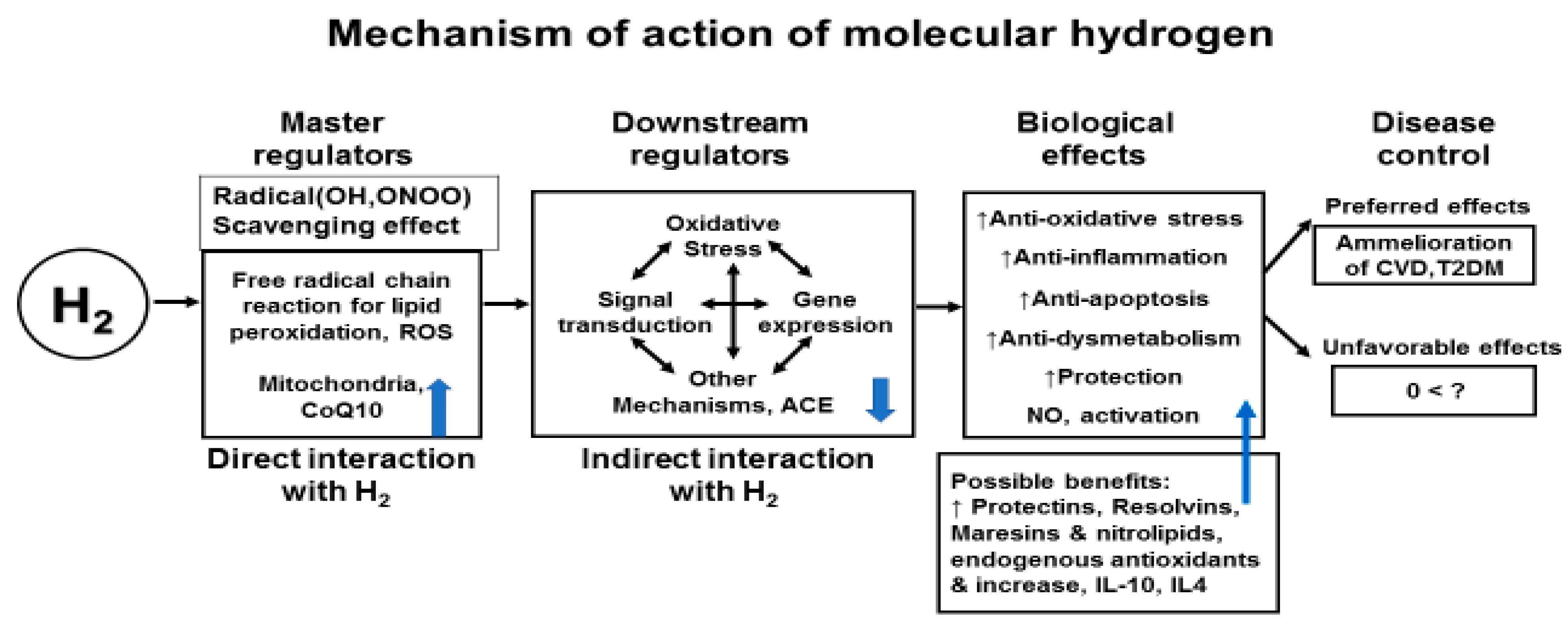
Figure 3.
Mechanism of production and inhibition of molecular hydrogen due to diets via microbiota in the gut, and its effects on anti-inflammatory molecules and cardio-metabolic diseases.
Figure 3.
Mechanism of production and inhibition of molecular hydrogen due to diets via microbiota in the gut, and its effects on anti-inflammatory molecules and cardio-metabolic diseases.

Figure 4.
Mechanisms of the effects of hydrogen therapy on pro-inflammatory biomarkers and cardio-metabolic diseases. (Modified from LeBaron et al, 2019, reference 17).
Figure 4.
Mechanisms of the effects of hydrogen therapy on pro-inflammatory biomarkers and cardio-metabolic diseases. (Modified from LeBaron et al, 2019, reference 17).
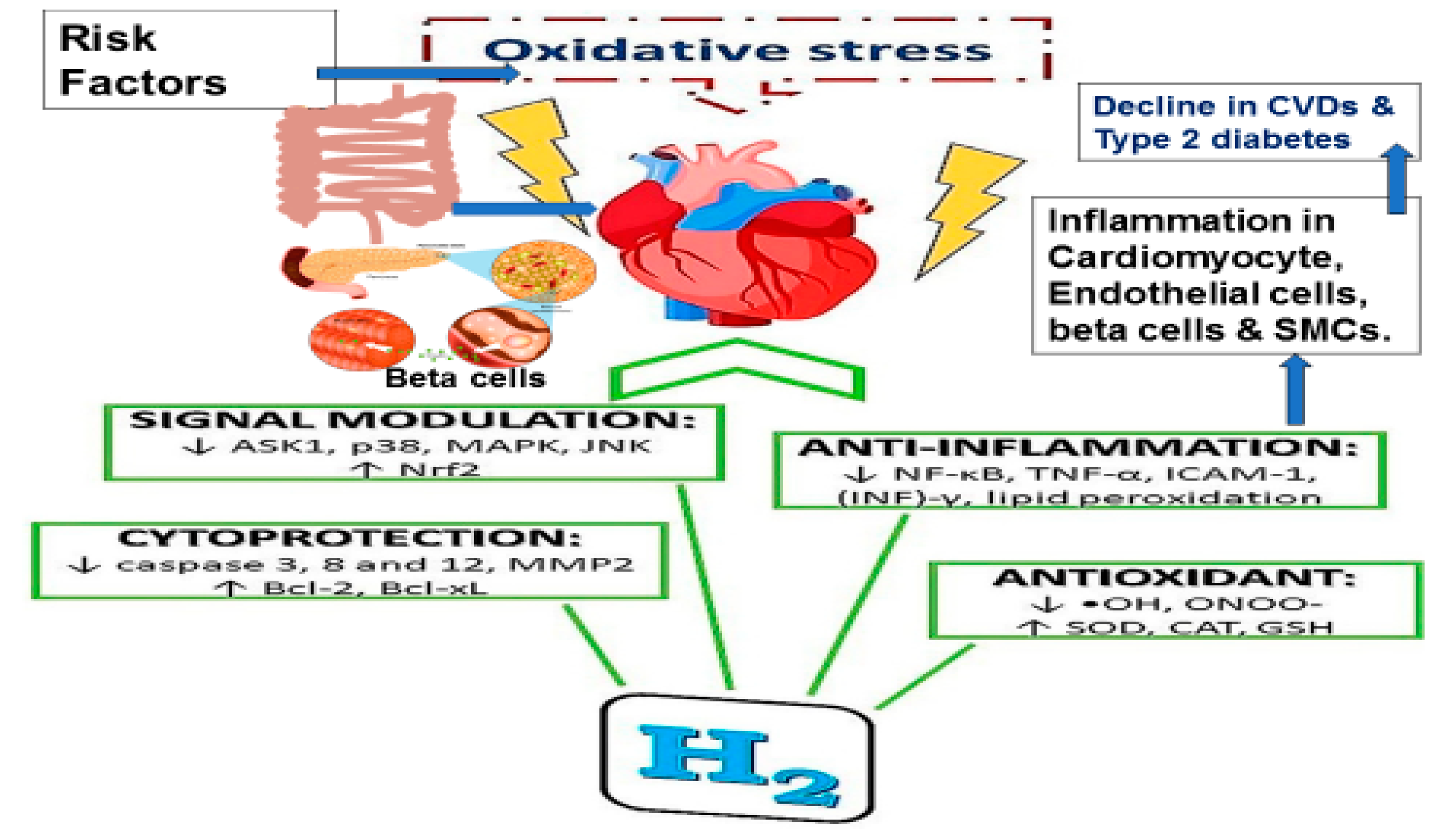

Table 1.
Effects of hydrogen rich water on blood lipoproteins in patients with metabolic syndrome [25].
Table 1.
Effects of hydrogen rich water on blood lipoproteins in patients with metabolic syndrome [25].
| Data | Hydrogen rich water (n-30) | Placebo (n=30) | ||
|---|---|---|---|---|
| Data, mg/dl | Baseline | After 24 weeks | Baseline | After 24 weeks |
| Cholesterol | 187.7 ± 32.4 | 169.2 ± 26.1*** | 184.3 ± 37.4 | 184.4 ± 38.6 |
| LDL-Cholesterol | 109.0 ± 34.4 | 102.5 ± 28.0 | 105.5 ± 42.0 | 106.0 ± 43.3 |
| HDL cholesterol | 41.7 ± 4.2 | 40.4 ± 1.8 | 41.8 ± 2.3 | 42.3 ± 2.4 |
| VLDL cholesterol | 37.3 ± 17.9 | 28.0 ± 11.3** | 36.8 ± 20.6 | 37.3 ± 20.5 |
| Triglycerides | 189.8 ± 93.3 | 142.4 ± 65.0** | 184.4 ± 102.8 | 185.6 ± 101.3 |
| C-reactive proteins | 0.5 ± 0.2 | 0.5 ± 0.1* | 0.6 ± 0.5 | 0.6 ± 0.5 |
*** = p value <0.0001, **= p value <0.01, *= p value <0.05, by comparison of baseline and after follow up using analysis of variance. (Modified from reference 25}.
Table 2.
Effect of hydrogen rich water on glycaemia, oxidative stress and cytokines in patients with metabolic syndrome [25].
Table 2.
Effect of hydrogen rich water on glycaemia, oxidative stress and cytokines in patients with metabolic syndrome [25].
| Hydrogen rich water(n=30) | Placebo (n=30) | |||
|---|---|---|---|---|
| Data, mg/dl | Baseline | After 24 weeks | Baseline | After 24 weeks |
| Fasting blood glucose | 121.5 ± 61.0 | 103.1 ± 33.0* | 123.9 ± 43.4 | 126.4 ± 42.3 |
| HbA1c, % | 5.8 ± 0.9 | 5.1 ± 0.2*** | 6.2 ± 1.2 | 6.1 ± 1.2 |
| TNF-α | 4.8 ± 1.2 | 3.9 ± 0.6*** | 4.8 ± 1.3 | 4.8 ± 1.3 |
| IL-6 | 1.9 ± 0.7 | 1.6 ± 0.2** | 1.6 ± 0.6 | 1.7±0.6 |
| TBARS | 2.5 ± 0.3 | 1.6 ± 0.3* | 2.5 ± 0.3 | 2.5 ± 0.3 |
| Melondialdehyde | 3.4 ± 0.2 | 2.7 ± 0.2*** | 3.4 ± 0.2 | 3.5 ± 0.2 |
| Diene conjugates | 27.8 ± 1.0 | 26.7 ± 0.5*** | 28.3 ± 0.8 | 28.3 ± 0.8 |
| Vitamin E | 23.0 ± 2.3 | 26.8 ± 1.9*** | 23.0 ± 1.5 | 23.1 ± 1.1 |
| Vitamin C | 20.7 ± 2.5 | 24.2 ± 1.8*** | 20.7 ± 2.5 | 20.8 ± 2.4 |
| Nitrite | 0.63 ± 0.06 | 0.68 ± 0.06*** | 0.66 ± 0.04 | 0.65 ± 0.03 |
| Angiotensin converting enzyme | 85.2 ± 7.8 | 80.7 ± 5.8*** | 84.5 ± 8.8 | 83.8 ± 8.7 |
*** = p value <0.0001, **= p value <0.01, *= p value <0.05, by comparison of baseline and after follow up using analysis of variance. (Modified from reference 25}.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



