Submitted:
30 May 2022
Posted:
31 May 2022
Read the latest preprint version here
Abstract
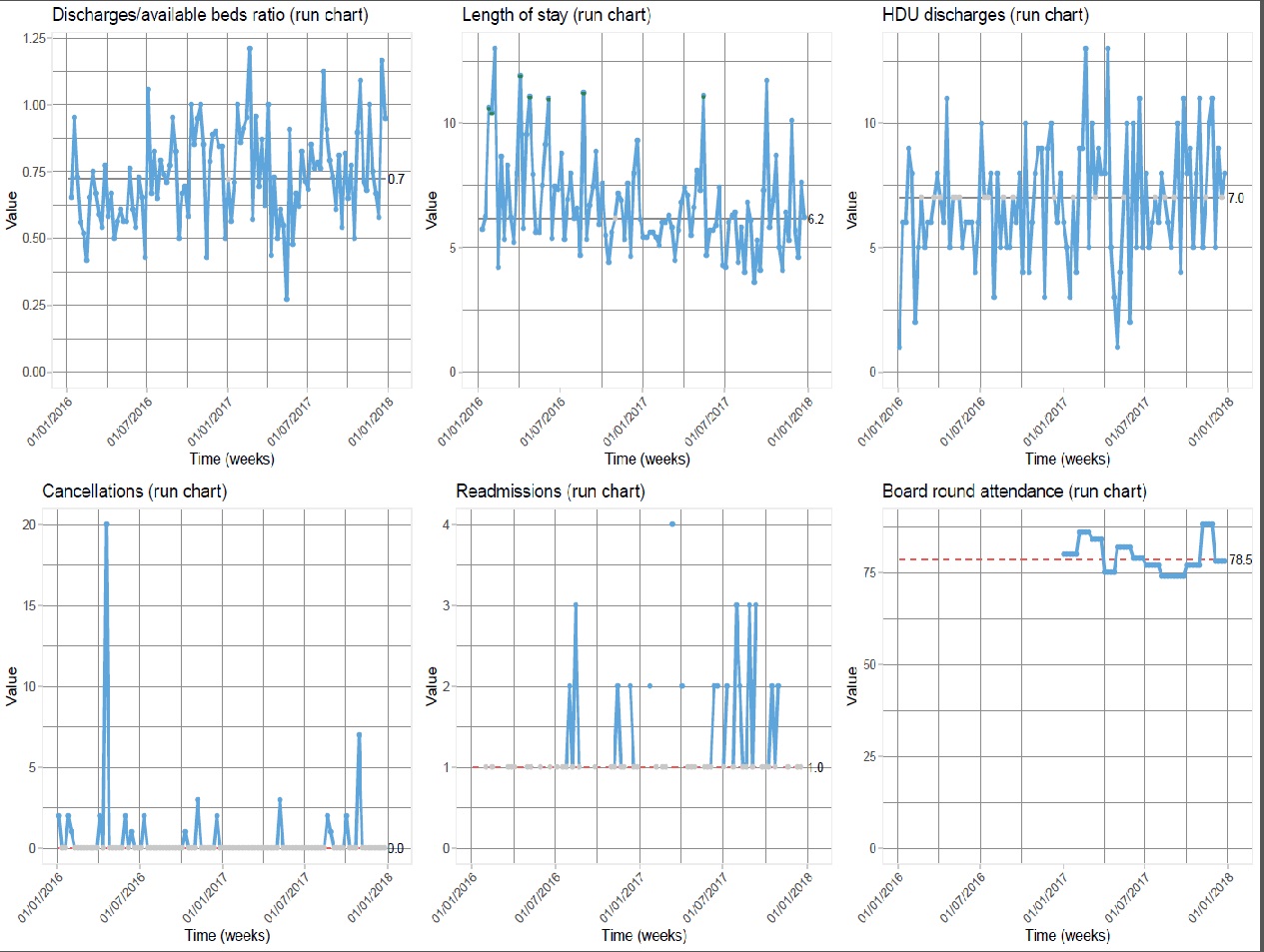
Hospital bed shortage is a worldwide concern on different grounds. Unavailability of postoperative beds occasionally causes hospital-initiated surgery cancellations, at the Royal London Hospital peaking in spring 2016 at over 50% due to saturation of intensive care (ICU) and high-dependency units (HDU), often caused by difficult patient step-down to the ward. In our digestive surgery service, rounds were run on a consultant firm basis on the ward admitting approximately 1000 patients yearly, including surgical cases and “outliers” from different specialties. We report a service improvement study (ISRCTN13976096) introducing a modified “SAFER Red2Green” model to enhance patient flow, comparing the year 2016 to 2017, when the model was applied.We adopted a Plan-Do-Study-Act methodology. Our intervention consisted in 1) systematic communication of the key care plan from the afternoon ward rounds to the nurse in charge; 2) 10AM Monday-to-Friday multidisciplinary (MDT) “board rounds”, attended daily by the senior-team and weekly by hospital and site managers, revising the key care plan aiming at safe, early discharges, assessing appropriateness of each inpatient day and tackling any cause of delay. We measured the improvement by the weekly discharge/available-bed ratio, average length of stay (LOS), HDU step-downs, operation cancellations, monitoring 30-day readmissions, staff satisfaction and senior board round attendance. Assessments were carried out at 3 and 12 months. At three months we recorded a 67% increase in discharges/week (p=0.001) with a 20% LOS reduction from 5 to 4 median days (p=0.023) and -21% HDU step-downs (p=0.205). At 12 months median LOS kept reduced to 4 days (p= 0.003), increased probability of earlier discharge (p=0.023), and 60% cancellations reduction (p=1). Thirty-day readmissions kept at 1.3 % throughout, with board round staff satisfaction and senior attendance over 75%.The model has improved multidisciplinary ward patient care and enhanced patient flow, requiring senior staff commitment to remain sustainable.
Keywords:
Patient flow
; Surgery
; Quality improvement
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



