
Submitted:
06 November 2018
Posted:
07 November 2018
You are already at the latest version
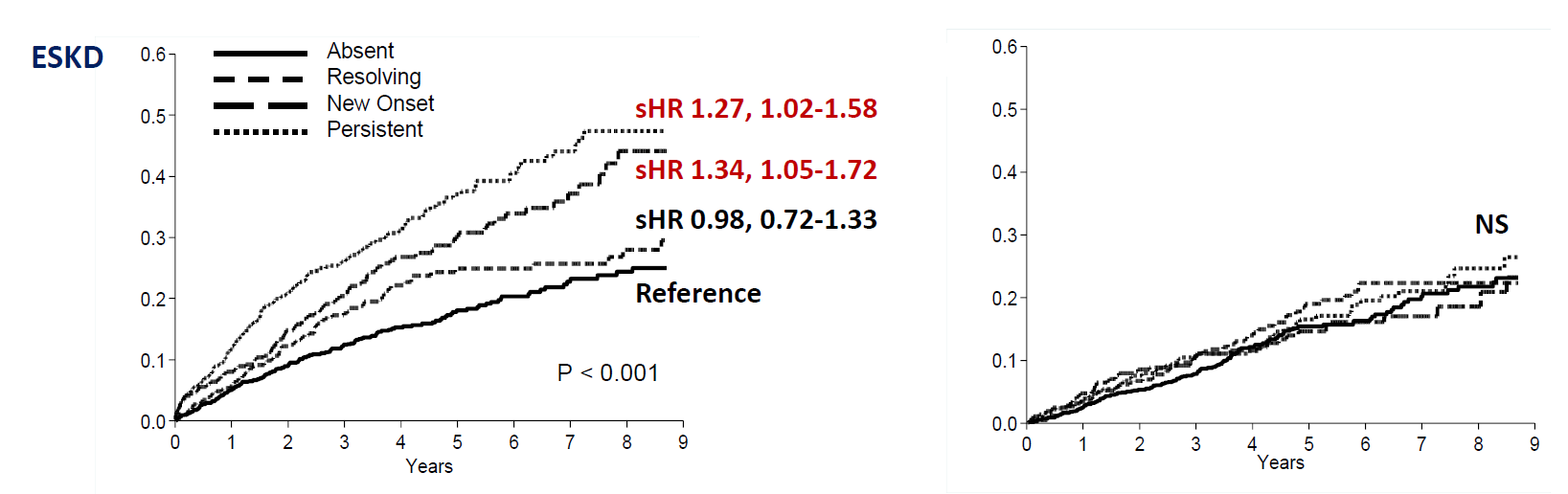
Abstract
Hyperkalemia burden in non-dialysis CKD under nephrology care is undefined. We prospectively followed 2443 patients with two visits (referral and control with 12-month interval) in 46 nephrology clinics. Patients were stratified in four categories of hyperkalemia (sK≥5.0 mEq/L) by sK at visit 1 and 2: Absent (no-no), Resolving (yes-no), New Onset (no-yes), Persistent (yes-yes). We assessed competing risks of ESKD and death after visit 2. Age was 65±15 y, eGFR 35±17 mL/min/1.73 m2, proteinuria 0.40 (0.14-1.21) g/24h. In the two visits sK was 4.8±0.6 and levels ≥6 mEq/L were observed in 4%. Hyperkalemia was absent in 46%, resolving 17%, new onset 15% and persistent 22%. Renin-angiotensin-system inhibitors (RASI) were prescribed in 79% patients. During 3.6-year follow-up, 567 patients reached ESKD and 349 died. Multivariable competing risk analysis [sub-hazard ratio-sHR, 95%Confidence Interval-CI] evidenced that new onset [sHR 1.34, 95%CI 1.05-1.72] and persistent [sHR 1.27, 95%CI 1.02-1.58] hyperkalemia predicted higher ESKD risk versus absent, independently from main determinants of outcome including eGFR change. Conversely, no effect on mortality was observed. Results were confirmed by testing sK as continuous variable. Therefore, in CKD under nephrology care, mild-to-moderate hyperkalemia status is common (37%) and predicts per se higher ESKD risk but not mortality.
Keywords:
CKD
; ESKD
; Death
; anti-RAS
; hyperkalemia
; competing risk
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



