Submitted:
11 July 2026
Posted:
14 July 2026
You are already at the latest version
Abstract
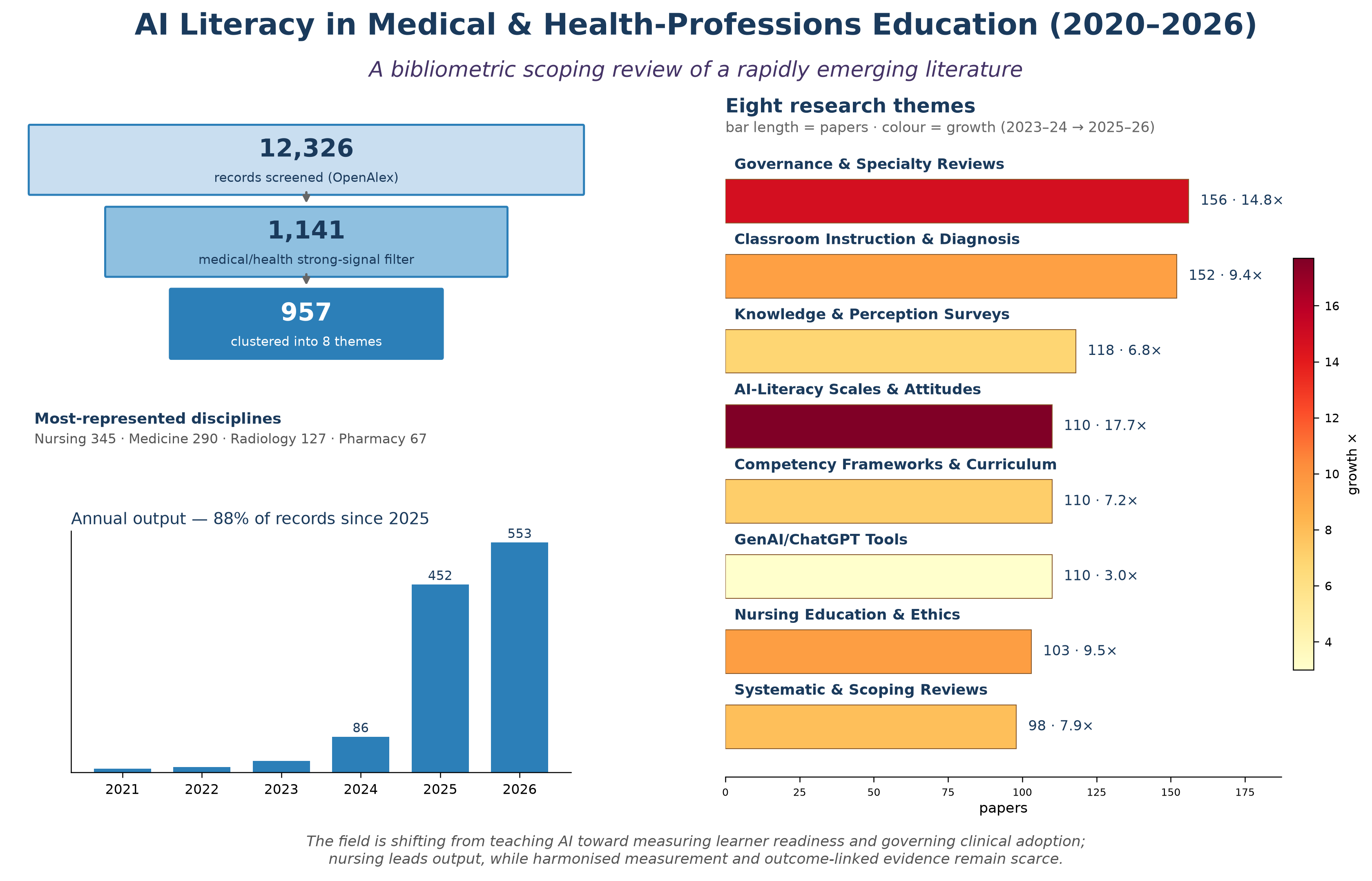
Background: The public release of generative artificial intelligence (AI) tools in late 2022 has spurred rapid interest in preparing health professionals to understand, use, and critically appraise AI. "AI literacy" has emerged as a focal construct, yet the resulting literature has grown so quickly that its structure, thematic composition, and gaps remain poorly characterized. Objective: To map the recent literature on AI literacy in medical and health professions education, identify its principal research themes and their growth trajectories, and highlight gaps to guide future work.Methods: We conducted a bibliometric scoping review. Records indexed in OpenAlex (2020 to mid-2026) matching a family of AI-literacy phrases were retrieved (n = 12,326 screened) and then filtered by an automated rule to retain those with a strong medical/health-professions signal, yielding 1,141 papers. English-language records with a substantive abstract (n = 957) were grouped into candidate themes using unsupervised text clustering (TF-IDF with latent semantic reduction and k-means), and the themes were then interpreted and characterized by two reviewers. Reporting follows the PRISMA extension for Scoping Reviews (PRISMA-ScR). Coverage of the single source was cross-checked against PubMed. Results: The subfield is overwhelmingly recent: fewer than 30 papers appeared in any year before 2023 (single digits in 2021), rising to 28 in 2023, 86 in 2024, and 452 in 2025, with 553 in the first half of 2026 alone. A compound annual growth rate of roughly 302% across the full years 2023–2025. Eight interpretable themes emerged, spanning governance and regulation; classroom instruction and diagnostic reasoning; knowledge and perception surveys; AI-literacy scales and attitudes; competency frameworks; generative AI tools; nursing education and ethics; and evidence syntheses. The fastest-growing themes were AI-literacy scale/attitude studies (17.7×) and governance and regulation (14.8×). Nursing was the most-represented discipline (345 papers), ahead of medicine (290). The most-cited works remained a small set of 2021–2023 curriculum-readiness surveys and evidence syntheses. Conclusions: AI literacy in health professions education has evolved over two years from asking whether to teach AI to measuring learner readiness and governing institutional adoption. Progress is constrained by a proliferation of non-harmonized measurement instruments, a relative scarcity of validated competency standards, and few studies linking AI-literacy interventions to clinical performance or patient outcomes. Harmonized measurement, consensus competency frameworks, and outcome-anchored evaluations are priorities.
Keywords:
artificial intelligence literacy
; medical education
; health-professions education
; nursing education
; generative AI
; competency framework
; bibliometric analysis
; scoping review
1. Introduction
Artificial intelligence (AI) is being incorporated into clinical care at an accelerating pace, from diagnostic imaging and clinical decision support to generative tools that draft documentation and answer clinical questions [2,13]. For health professionals to use these systems safely and effectively, they must develop “AI literacy,” defined as the knowledge, skills, and critical dispositions required to understand what AI can and cannot do, to use AI-enabled tools appropriately, and to appraise their outputs and limitations [3,4]. In medical and health professions education, this has rapidly become a distinct area of scholarship and curriculum development [1,3,4].
Two features make this literature difficult to navigate. First, it is very new: although foundational work on AI curricula for health professionals predates 2022 [3,4,5], the public availability of large language models in late 2022 triggered a step-change in output, and the great majority of the literature has appeared since 2024 [1,9]. Second, it is dispersed across professions (medicine, nursing, dentistry, pharmacy, radiology, and others), study designs (cross-sectional surveys, scale-validation studies, curriculum descriptions, and reviews), and terminologies (“AI literacy,” “AI competency,” “generative AI literacy”), which fragments the evidence base and obscures its overall structure [6,7,8].
Existing reviews have tended to focus on a single profession or a single question. For example, scoping reviews of AI education programs for health professionals [3], evidence syntheses of AI in nursing education [10,11], or narrative overviews of generative AI in medical education [1,9]. What is missing is a map of the entire subfield: its size, its principal research themes, which are growing fastest, and where the gaps lie. Such a map is a prerequisite for coordinated curriculum development, consensus competency standards, and a coherent research agenda.
We therefore conducted a bibliometric scoping review. Consistent with scoping review methodology, our aim was to map the extent, range, and nature of the literature rather than synthesize effect estimates or appraise the quality of individual studies [16]. Our objectives were to (1) delineate the volume and growth of the AI-literacy literature in medical and health professions education; (2) identify its principal research themes and characterize each by size, growth, and exemplar works; (3) describe its disciplinary and geographic distribution; and (4) synthesize gaps and priorities for future research and education.
2. Methods
2.1. Design and Reporting
We conducted a bibliometric scoping review, combining systematic database retrieval with unsupervised text clustering to derive candidate themes, followed by reviewer interpretation. This design maps the extent and structure of a large, fast-moving literature; consistent with the scoping-review framework, formal quality appraisal of individual studies and meta-analysis were outside its scope [16]. Reporting follows the PRISMA extension for Scoping Reviews (PRISMA-ScR); a completed checklist is provided (S2 File). The review protocol was archived retrospectively on the Open Science Framework (OSF; https://doi.org/10.17605/OSF.IO/B9DXC; S3 File) after the analysis was completed [17]; this is an archival, not a prospective, registration, and the protocol records the review as actually conducted, including the iterative refinement of the eligibility rule described in §2.3. No prospective registration was undertaken, and PROSPERO does not accept scoping or bibliometric reviews.
2.2. Data Source and Search
Bibliographic records were retrieved from OpenAlex, an open scholarly database with broad coverage of biomedical, education, and social-science literature, including preprints and repository items. The search was conducted on records published from 1 January 2020 to mid-2026 (last search: mid-2026). We used exact-phrase matching in titles and abstracts for a family of AI-literacy terms: “AI literacy,” “artificial intelligence literacy,” “generative AI literacy,” “GenAI literacy,” “algorithmic literacy,” and “AI competency/competencies.” “Algorithmic literacy” was included because it is used interchangeably with AI literacy in parts of the health professions and digital health literature; a sensitivity analysis excluding it did not materially alter the thematic structure. The exact API query strings and the medical-context filter expressions are provided in the supplementary materials (S1 File) to enable reproduction.
2.3. Eligibility and Selection
Eligible records were published from 2020 to mid-2026, in any publication status (including preprints), and had a medical or health-professions context (defined below). From the parent AI-literacy corpus (n = 12,326 screened), we identified records with a medical or health-professions context using an automated keyword rule. To maximize precision, we required a strong signal: a medical/health professions term in the title, or at least two distinct such terms across the title and abstract. Terms spanned professions and settings (medicine, nursing, dentistry, pharmacy, radiology, surgery, public and veterinary health, and clinical training). An initial, more permissive single-mention rule (n = 1,590) was found on inspection to admit false positives. General-public AI-perception surveys and K-12 studies that mentioned a medical term only incidentally were therefore excluded. The strong-signal rule yielded 1,141 records (excluding 449 weakly matched records). For thematic clustering, we restricted to English-language records with a substantive abstract (n = 957; 184 records without an English abstract were retained for descriptive counts but not clustered). The record flow is shown in Figure 5.
Selection was performed by the automated rule rather than by dual independent human screening; no manual eligibility adjudication or inter-rater agreement statistic was computed at the screening stage. Two reviewers independently inspected the resulting clusters and their representative works and reconciled theme labels by discussion (Section 2.4); reviewer involvement was therefore at the interpretation stage, not the screening stage. This is a deliberate trade-off of a computational approach at this corpus scale and a limitation relative to a conventional dual-screened scoping review.
2.4. Thematic Analysis
Titles (up-weighted) and abstracts were vectorized using sublinear term-frequency–inverse-document-frequency (TF-IDF) representations over unigrams and bigrams, with generic and domain-ubiquitous stop words removed (maximum 8,000 features). Dimensionality was reduced with truncated singular value decomposition (80 components, retaining 0.29 of the variance), and documents were grouped with k-means.
Since AI-literacy abstracts share considerable vocabulary overlap, silhouette scores were consistently low across all candidate cluster numbers and did not reveal a single clear optimal k (silhouette scores by k: 6: 0.048, 7: 0.029, 8: 0.032, 9: 0.047, 10: 0.060, 11: 0.057, 12: 0.043). Therefore, we chose k=8 because it yielded the smallest number of themes that were interpretable, non-redundant, and contained distinct representative works, rather than selecting the one with the highest silhouette score. This choice emphasizes interpretability; the themes serve as an organizational lens rather than a strict taxonomy. To assess stability, we reran k-means with k=8 using 10 random initializations and measured agreement using the adjusted Rand index (ARI) against a reference solution. The agreement was moderate (mean ARI 0.425, range 0.218–0.568), implying the broad thematic structure is reproducible, though borderline assignments vary. An earlier clustering identified a cluster caused by preprint-formatting artifacts, which we removed before re-running the analysis, consistent with the soft boundaries indicated by the ARI.
Two reviewers labeled each cluster based on its highest-weighted terms and its most-cited, representative papers, reconciling disagreements through discussion; every representative work was verified to contain genuine medical/health-professions content. Cluster size, disciplinary composition, and growth were computed. Growth was expressed as the ratio of 2025–2026 to 2023–2024 output; because several themes had near-zero 2023–24 baselines, we report the raw counts alongside each ratio (Table 1) and applied add-one (Laplace) smoothing to the ratio to avoid instability. Disciplinary counts were computed on the full strong-signal set (n = 1,141) using word-boundary keyword matching and are non-exclusive; theme sizes and growth were computed on the clustered set (n = 957). Citation counts are OpenAlex values retrieved at the time of retrieval and are lagging indicators that favor older work.
2.5. Coverage Cross-Check
Because retrieval relied on a single database, we cross-checked coverage against PubMed/MEDLINE. All 15 peer-reviewed works cited in this review with a DOI were also indexed in PubMed (15/15), indicating that OpenAlex captures the core peer-reviewed biomedical literature of this subfield. (A broader spot-check of 24 candidate works, before the reference list was trimmed to those cited, found 23 of 24 indexed.) A PubMed query for AI-literacy terms in an education context over the same window returned 600 records, fewer than in our medical set, consistent with OpenAlex also surfacing preprints and repository items (e.g., Zenodo, Figshare, Research Square) that PubMed does not index. The two sources are therefore complementary, and single-source retrieval is more likely to affect the gray-literature margins than the peer-reviewed core.
2.6. Ethics
This review used only aggregated, published bibliographic metadata and did not involve human participants; therefore, ethical approval was not required.
3. Results
3.1. Volume and Growth
AI literacy in health professions education is a two-year-old subfield at scale, even though isolated papers appeared as early as 2020. Annual output remained in the single- or low-double digits through 2022 (9 papers in 2021, 13 in 2022), then rose sharply: 28 in 2023, 86 in 2024, and 452 in 2025; the first half of 2026 already contains 553 records (Figure 1). This corresponds to a compound annual growth rate of roughly 302% across the years 2023–2025, and more than 85% of the corpus (1,005 of 1,141) was published from 2025 onward. The most-cited works remain a small set of 2021–2023 curriculum-readiness surveys and evidence syntheses [1,3,4,5]; this partly reflects citation lag. Papers from 2025–26 have had little time to accrue citations. Even allowing for that lag, the field’s empirical expansion currently rests on a narrow set of early conceptual anchors.
3.2. Thematic Structure
Unsupervised clustering grouped the 957 abstracted papers into eight interpretable themes (Table 1, Figure 4). The two largest themes were governance, regulation, and clinical specialty reviews, and AI in classroom instruction and diagnostic reasoning (each 16%). The remaining themes comprised student and trainee knowledge and perception surveys; AI literacy scales and attitudes; competency frameworks and curriculum design; generative AI/ChatGPT tools in medical education, nursing education, and ethics; and systematic and scoping reviews (each 10–12%). As noted in Methods, these themes are an interpretive organizing structure with moderate partition stability, not a definitive taxonomy.
3.3. Which Themes are Growing Fastest
All themes grew, but unevenly (Figure 2, Table 1). Growth was steepest for AI-literacy scales and attitudes (5 papers in 2023–24 to 105 in 2025–26; 17.7×) and for governance, regulation, and clinical specialty reviews (9 → 147; 14.8×), followed by nursing education and ethics (9 → 94; 9.5×) and AI in classroom instruction and diagnostic reasoning (13 → 131; 9.4×). The generative AI tools in medical education theme grew the most slowly (27 → 82; 3.0×), suggesting it was already the largest theme early in the 2023 wave of interest rather than a decline in activity. Because 2026 is a half-year and the 2023–24 baselines are small, these ratios should be read alongside the raw counts in Table 1 rather than as precise multipliers.
3.4. Disciplinary and Geographic Distribution
Across the 1,141 papers, nursing was the most-represented discipline (345 papers), ahead of medicine and medical students (290), with radiology the leading clinical specialty (127) (Table 2, Figure 3). Pharmacy, dentistry, public and global health, and surgery each accounted for a smaller share, and veterinary education was minimal. Nursing’s prominence reflects a distinct sub-literature of validated AI literacy and attitude scales, as well as an ethics-focused strand.[10,11,15] Author affiliations were internationally distributed, led by the United States, China, the United Kingdom, Saudi Arabia, and Canada (Table 3). A substantial share of output appeared in preprint and repository venues alongside established journals such as BMC Medical Education, Nurse Education Today, JMIR Medical Education, and BMC Nursing, consistent with a fast-moving field that outpaces conventional publication cycles.
3.5. Foundational Works
The most-cited papers in the subfield were a narrative analysis of ChatGPT and generative AI for medical education [1], a perspective on large-scale AI deployment in healthcare [2], a scoping review of AI education programs for health professionals [3], and early medical-school curriculum-readiness surveys [4,5]. These papers anchor the citation structure and recur as reference points across otherwise disparate empirical studies.
Figure 3.
Disciplinary distribution of the corpus (non-exclusive keyword counts, n = 1,141).

Figure 4.
Relative sizes of the eight themes (n of 957 clustered papers).

Figure 5.
Record identification, screening, and inclusion (PRISMA-ScR flow).

4. Discussion
4.1. Principal Findings
This scoping review maps a subfield that has grown rapidly, become thematically diverse, and spread globally within roughly two years. Three patterns stand out. First, the intellectual center of gravity has shifted from asking whether AI should be taught to measuring learner readiness with attitude and literacy scales and governing adoption at the institutional and specialty levels. The two fastest-growing themes, measurement and governance, together mark this transition. Second, nursing has emerged as a distinct, now leading, disciplinary strand, with its own instruments and an ethics-oriented literature, rather than a peripheral extension of medical student research. Third, the empirical explosion is anchored by a small set of 2021–2023 papers; while citation lag contributes to this pattern (Section 3.1), the conceptual base is narrow relative to the volume of recent empirical work.
4.2. Comparison with Existing Literature
Prior reviews have characterized parts of this landscape. AI education programs for health professionals [3], AI in nursing education [10,11], and generative AI in medical education [1,9] have generally been limited to a single profession or to a single question. Our whole-subfield map contextualizes these: profession-specific syntheses are one of the eight themes (evidence syntheses), and their proliferation (7.9× growth) signals both consolidation and the difficulty of keeping pace with primary studies. The prominence of governance and specialty-specific guidance (for example, radiology society recommendations [13]) suggests the field is beginning to move from individual competence toward institutional and regulatory frameworks.
4.3. Gaps and Implications
Several gaps follow directly from the map.
Measurement is fragmented. Rapid growth in scale development has produced multiple parallel AI-literacy and AI-attitude instruments, validated across diverse national and professional cohorts, with little cross-instrument harmonization [8,12,14]. This impedes comparison and the accumulation of evidence; a harmonization effort or consensus on a core outcome set is warranted.
Competency standards lag demand. Although a competency framework theme exists, it is modest relative to the volume of attitude and perception studies, and few frameworks are validated or accreditation-ready, precisely where curriculum designers and accreditors need support [4].
Outcomes are measured at the learner level. Almost all studies assess knowledge, attitudes, or intentions; studies linking AI-literacy training to downstream clinical performance or patient outcomes are rare, leaving the educational value proposition largely unproven.
Coverage is uneven. Nursing and medicine dominate, whereas pharmacy, dentistry, allied health, public health, and veterinary education remain comparatively underserved.
For educators, the practical implication is to prioritize shared, validated competency frameworks and to design AI-literacy interventions with outcome measures that go beyond self-reported attitudes. For researchers, the priorities are measurement harmonization, outcome-anchored evaluation designs, and expansion into underrepresented professions. For institutions and regulators, the emerging governance literature offers a foundation for coordinated policy but would benefit from alignment with validated individual-level competencies.
4.4. Strengths and Limitations
Strengths include comprehensive, reproducible retrieval from a large open database (with query strings and code deposited), an objective clustering step that reduces reviewer selection bias when deriving candidate themes, verification of representative works, and a quantified cross-check of coverage against PubMed.
Several limitations follow from the method. First, retrieval relied on a single database (OpenAlex). The coverage cross-check indicates that the peer-reviewed core is well captured (all 15 cited peer-reviewed works are also in PubMed), but a single source can still miss records indexed elsewhere (e.g., CINAHL for nursing, Scopus/Web of Science for bibliometrics); counts should be read as a well-covered lower bound rather than an exhaustive census. Second, selection was automated rather than dual-screened by hand, trading some recall and adjudication of borderline records for scalability and consistency; retrieval also depended on explicit AI-literacy terminology, so papers using different vocabulary were missed. Third, the themes are data-driven approximations: silhouette coefficients were low, and seed-to-seed agreement was moderate (ARI 0.425), so the themes are best read as an organizing lens, with borderline assignments uncertain. Fourth, citation counts favor older work, and 2026 counts are partial, so growth ratios (reported with raw counts) are indicative. Finally, as a bibliometric scoping review, this work maps the structure of the literature rather than appraising the methodological quality of individual studies; theme-specific systematic reviews with risk-of-bias assessment remain necessary.
4.5. Conclusions
Over roughly two years, AI literacy in medical and health professions education has evolved from a niche interest into a large, multidisciplinary field organized around measurement, instruction, governance, and profession-specific concerns, with nursing now the leading discipline. The field’s trajectory, from whether to teach AI to measuring readiness and governing adoption, is clear, but its maturation depends on harmonized measurement, validated, consensus-based competency standards, and evaluations that link AI-literacy education to clinical practice and patient outcomes. A coordinated response to these gaps would help convert a rapidly expanding but fragmented literature into a cumulative evidence base.
Supplementary Materials
The following supporting information can be downloaded at the website of this paper posted on Preprints.org.
Author Contributions
N.Z. designed the study, performed the analysis, and drafted the manuscript; L.A. contributed to the manuscript review and editing. Both authors approved the final manuscript.
Funding
None declared.
Ethical approval
Not required.
Data and code availability
All data underlying the findings, the parent AI-literacy corpus (n = 12,326), the strong-signal medical subset (n = 1,141), the clustered set with theme assignments (n = 957; S1 Dataset), and the theme-summary table(S2 Dataset), together with the analysis code (retrieval, filtering, clustering, and figure generation), the verbatim OpenAlex query strings, and full documentation, are openly available in the Zenodo repository: Zary, N. (2026). AI Literacy in Medical and Health-Professions Education (2020–2026): Data and Code [Data set]. Zenodo. https://doi.org/10.5281/zenodo.21141386. Bibliographic metadata are derived from OpenAlex (CC0); the deposited data are released under CC BY 4.0 and the code under the MIT License.
Conflicts of interest
None declared.
References
- Boscardin C, Gin BC, Golde PB, Hauer KE. ChatGPT and Generative Artificial Intelligence for Medical Education: Potential Impact and Opportunity. Acad Med 2024 Jan;99(1):22-27. [CrossRef]
- Esmaeilzadeh P. Challenges and strategies for wide-scale artificial intelligence (AI) deployment in healthcare practices: A perspective for healthcare organizations. Artificial Intelligence in Medicine. 2024. [CrossRef]
- Charow R, Jeyakumar T, Younus S, Dolatabadi E, Salhia M, Al-Mouaswas D, et al. Artificial Intelligence Education Programs for Health Care Professionals: Scoping Review. JMIR Medical Education. 2021. [CrossRef]
- Wood E, Ange BL, Miller DD. Are We Ready to Integrate Artificial Intelligence Literacy into Medical School Curriculum: Students and Faculty Survey. Journal of Medical Education and Curricular Development. 2021. [CrossRef]
- Teng M, Singla R, Yau O, Lamoureux D, Gupta A, Hu Z, et al. Health Care Students’ Perspectives on Artificial Intelligence: Countrywide Survey in Canada. JMIR Medical Education. 2022. [CrossRef]
- Tuygunov N, Samaranayake LP, Khurshid Z, Rewthamrongsris P, Schwendicke F, Osathanon T, et al. The Transformative Role of Artificial Intelligence in Dentistry: A Comprehensive Overview Part 2: The Promise and Perils, and the International Dental Federation Communique. International Dental Journal. 2025. [CrossRef]
- Fahim YA, Hasani IW, Kabba S, Ragab WM. Artificial intelligence in healthcare and medicine: clinical applications, therapeutic advances, and future perspectives. European journal of medical research. 2025. [CrossRef]
- Laupichler MC, Aster A, Meyerheim M, Raupach T, Mergen M. Medical students’ AI literacy and attitudes towards AI: a cross-sectional two-center study using pre-validated assessment instruments. BMC Medical Education. 2024. [CrossRef]
- Preiksaitis C, Ashenburg N, Bunney G, Chu A, Kabeer R, Riley F, et al. The Role of Large Language Models in Transforming Emergency Medicine: Scoping Review. JMIR Medical Informatics. 2024. [CrossRef]
- Arab RAE, Moosa OAA, Abuadas FH, Somerville J. The Role of AI in Nursing Education and Practice: Umbrella Review. Journal of Medical Internet Research. 2025. [CrossRef]
- Hassanein S, Arab RAE, Abdrbo A, Abu-Mahfouz MS, Gaballah MKF, Seweid MM, et al. Artificial intelligence in nursing: an integrative review of clinical and operational impacts. Frontiers in Digital Health. 2025. [CrossRef]
- El-Sayed B, El-Sayed AAI, Alsenany SA, Asal MGR, Asal MGR. The role of artificial intelligence literacy and innovation mindset in shaping nursing students’ career and talent self-efficacy. Nurse Education in Practice. 2024. [CrossRef]
- Kotter E, D’Antonoli TA, Cuocolo R, Hierath M, Huisman M, Klontzas ME, et al. Guiding AI in radiology: ESR’s recommendations for effective implementation of the European AI Act. Insights into Imaging. 2025. [CrossRef]
- Naamati-Schneider L. Enhancing AI competence in health management: students’ experiences with ChatGPT as a learning Tool. BMC Medical Education. 2024. [CrossRef]
- Subaşı DÖ, Sümengen AA, Semerci R, Şimşek E, Çakır GN, Temizsoy E. Paediatric nurses’ perspectives on artificial intelligence applications: A cross-sectional study of concerns, literacy levels and attitudes. Journal of Advanced Nursing. 2024. [CrossRef]
- Tricco AC, Lillie E, Zarin W, O’Brien KK, Colquhoun H, Levac D, et al. PRISMA Extension for Scoping Reviews (PRISMA-ScR): Checklist and Explanation. Annals of Internal Medicine. 2018;169(7):467–473. [CrossRef]
- Zary N, Alkhuja L. Artificial Intelligence Literacy in Medical and Health-Professions Education: A Bibliometric Scoping Review Protocol of a Rapidly Emerging Literature (2020–2026). OSF; 2026 Jul 3. [CrossRef]
Figure 1.
Annual publication counts for AI literacy in medical/health professions education, 2020–2026. The open marker denotes the partial 2026 (January–June) count.
Figure 1.
Annual publication counts for AI literacy in medical/health professions education, 2020–2026. The open marker denotes the partial 2026 (January–June) count.

Figure 2.
Growth ranking of the eight themes (2025–26 vs 2023–24, add-one smoothed); dot size is proportional to theme size (n of 957 clustered papers).
Figure 2.
Growth ranking of the eight themes (2025–26 vs 2023–24, add-one smoothed); dot size is proportional to theme size (n of 957 clustered papers).


Table 1.
Eight themes in AI literacy for medical and health-professions education (2020–mid-2026), by size and growth.
Table 1.
Eight themes in AI literacy for medical and health-professions education (2020–mid-2026), by size and growth.
| Theme | n (%) | 2023–24 → 2025–26 | Growth ratio† | Characteristic terms |
|---|---|---|---|---|
| Governance, Regulation & Clinical-Specialty Reviews | 156 (16%) | 9 → 147 | 14.8× | challenges, human, review, governance, regulatory, future |
| AI in Classroom Instruction & Diagnostic Reasoning | 152 (16%) | 13 → 131 | 9.4× | model, diagnostic, analysis, support, digital, systems |
| Student/Trainee Knowledge & Perception Surveys | 118 (12%) | 14 → 101 | 6.8× | cross sectional, sectional, perceptions, cross, knowledge, attitudes |
| AI Literacy Scales & Attitudes (Nursing/Medical Students) | 110 (11%) | 5 → 105 | 17.7× | nursing, nurses, attitudes, scale, cross sectional, sectional |
| Competency Frameworks & Curriculum Design | 110 (11%) | 12 → 92 | 7.2× | competency, framework, competencies, curriculum, physicians, curricula |
| GenAI/ChatGPT Tools in Medical Education | 110 (11%) | 27 → 82 | 3.0× | systems, technology, human |
| Nursing Education & Ethics (Qualitative) | 103 (11%) | 9 → 94 | 9.5× | nursing, qualitative, undergraduate nursing, perspectives, generative, educators |
| Systematic & Scoping Reviews | 98 (10%) | 10 → 86 | 7.9× | scoping, review, studies, nursing, systematic |
Percentages are based on the 957 clustered papers and sum to 98% due to rounding. †Growth ratio = (2025–2026 count) / (2023–2024 count) with add-one smoothing; raw counts are shown in the adjacent column because several themes have small baselines and 2026 is a half-year.
Table 2.
Disciplinary distribution of the 1,141-paper corpus (non-exclusive, word-boundary keyword counts).
Table 2.
Disciplinary distribution of the 1,141-paper corpus (non-exclusive, word-boundary keyword counts).
| Discipline | Papers (non-exclusive) |
|---|---|
| Nursing | 345 |
| Medicine / medical students | 290 |
| Radiology / imaging | 127 |
| Pharmacy | 67 |
| Dentistry | 61 |
| Public / global health | 48 |
| Surgery | 45 |
| Veterinary | 12 |
Table 3.
Leading countries by author affiliation (n = 1,141; non-exclusive).
| Country | Papers (author affiliation) |
|---|---|
| United States | 258 |
| China | 97 |
| United Kingdom | 70 |
| Saudi Arabia | 60 |
| Canada | 56 |
| India | 55 |
| Türkiye | 50 |
| Pakistan | 46 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2026 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



