Submitted:
02 July 2026
Posted:
02 July 2026
You are already at the latest version
Abstract
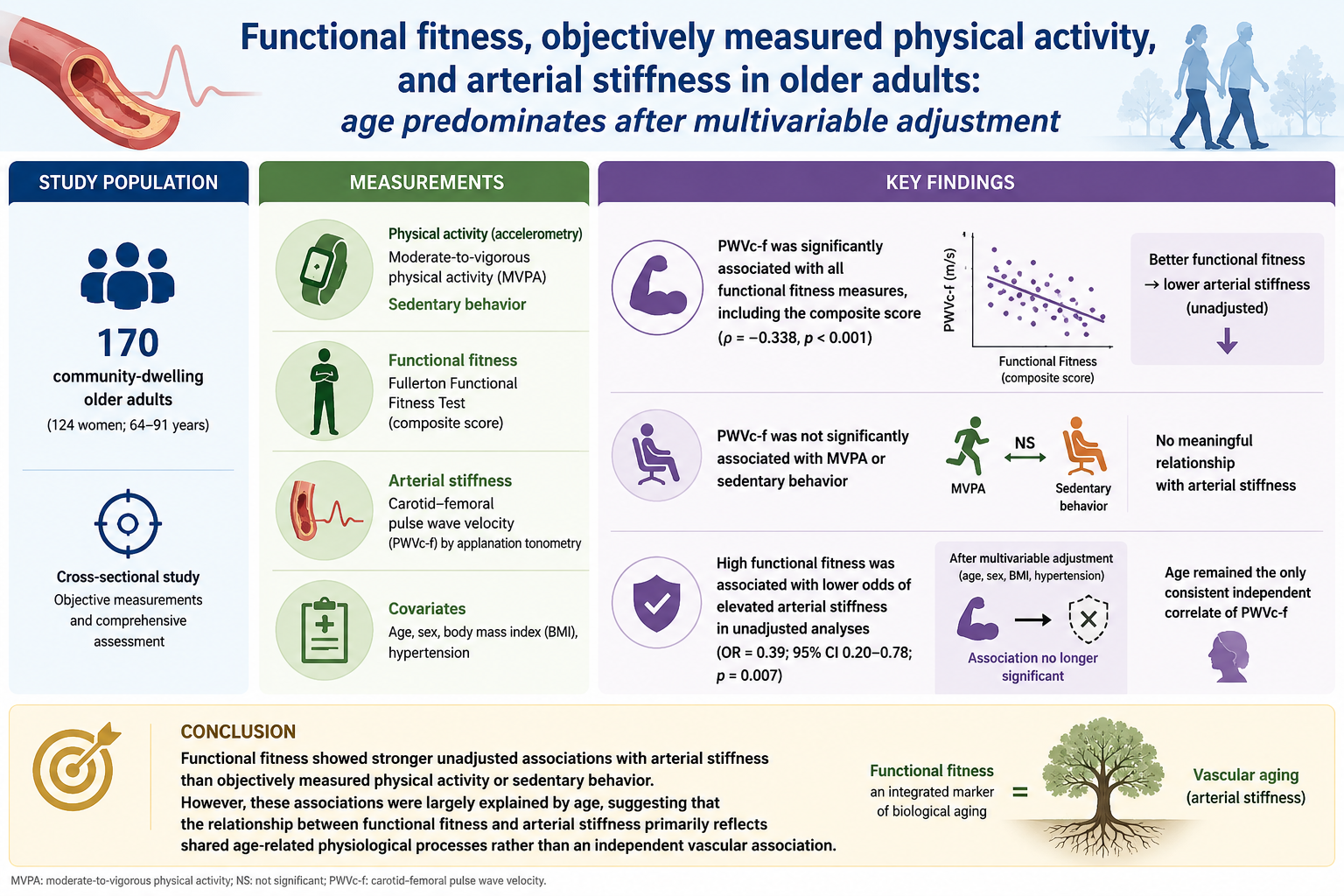
Background: Central arterial stiffness assessed by carotid-femoral pulse wave velocity (PWVc-f) strongly predicts cardiovascular risk. We examined associations of objec-tively measured physical activity, sedentary behavior, and functional fitness with PWVc-f in community-dwelling older adults. Methods: The study included 170 older adults (124 women; 64–91 years). Moderate-to-vigorous physical activity (MVPA) and sedentary behavior were assessed by accelerometry, functional fitness by the Fullerton Functional Fitness Test (composite score), and PWVc-f by applanation tonometry. As-sociations were examined using correlation, hierarchical linear regression, and logistic regression analyses. Results: Elevated arterial stiffness (PWVc-f >10 m/s) was present in 62.3% of participants. PWVc-f associated with all functional fitness measures, in-cluding the composite score (ρ=−0.338, p< 0.001), but not with MVPA or sedentary be-havior. High functional fitness associated with lower odds of elevated PWVc-f in un-adjusted analyses (OR=0.39, 95% CI 0.20–0.78; p=0.007), but this was no longer signifi-cant after adjustment for age, sex, and anthropometric/clinical characteristics. Neither MVPA nor sedentary behavior predicted PWVc-f. Age remained the only independent correlate across all models. Conclusions: Functional fitness showed stronger unad-justed associations with PWVc-f than MVPA or sedentary behavior. However, these associations were largely explained by age, indicating that functional fitness and PWVc-f primarily reflect shared age-related physiological processes.
Keywords:
aging
; arterial stiffness
; carotid-femoral pulse wave velocity
; functional fitness
; physical activity
; sedentary behavior
1. Introduction
Arterial stiffening is among the most important age-related vascular changes and independently predicts cardiovascular morbidity and mortality in older adults [1,2,3,4]. Increased central arterial stiffness contributes to impaired ventricular–vascular coupling, elevated cardiac afterload, reduced coronary perfusion, and progressive loss of cardiovascular reserve, thereby linking vascular aging to declines in physical function and healthy longevity [3,4,5]. These alterations are particularly relevant in older populations, in whom aging-related structural and functional changes of the arterial wall are frequently aggravated by hypertension, obesity, physical inactivity, and metabolic disorders [6,7].
Carotid-femoral pulse wave velocity (PWVc-f) is the gold-standard noninvasive measure of central arterial stiffness and a well-established tool for cardiovascular risk assessment in both clinical and epidemiological settings [8,9]. Given the recognized vascular benefits of exercise, increased physical activity has been proposed as a potentially important determinant of arterial health during aging [10,11]. However, evidence relating physical activity levels to arterial stiffness in older adults remains inconsistent. Although some studies and meta-analyses suggest that physically active individuals exhibit lower PWVc-f values, reported effect sizes are generally modest and highly heterogeneous [12,13,14]. Moreover, associations tend to weaken substantially when physical activity is objectively assessed using accelerometry rather than self-reported questionnaires, suggesting that behavioral measures of physical activity may not fully capture the physiological adaptations relevant to vascular aging [13,14].
One possible explanation for these inconsistencies is that the relationship between movement behavior and vascular health may depend not only on the amount of physical activity performed but also on the individual’s integrated functional capacity. In this context, functional fitness may provide complementary information about biological aging and cardiovascular health because it integrates multiple dimensions of physical function rather than reflecting a single behavioral attribute. Functional fitness reflects the integrated interaction among cardiorespiratory capacity, muscular strength, mobility, balance, flexibility, and neuromuscular coordination required to perform daily tasks safely and independently [15,16]. Declines in these domains are associated with frailty, sarcopenia, reduced exercise tolerance, impaired endothelial function, chronic low-grade inflammation, and autonomic dysfunction, all of which may contribute to arterial stiffening [17,18,19,20].
Previous studies have reported inverse associations between isolated physical fitness components, such as cardiorespiratory fitness, muscular strength, gait performance, and flexibility vs. measures of arterial stiffness [11,17,21,22]. However, most investigations have focused on single fitness domains rather than adopting a multicomponent functional approach reflecting overall physiological reserve. This distinction may be clinically important because functional performance in older adults depends on the interaction of multiple physical capacities rather than isolated physiological traits. Whether functional fitness is more strongly associated with arterial stiffness than objectively measured physical activity and sedentary behavior remains to be determined.
Clarifying these relationships has practical implications for cardiovascular prevention strategies in aging populations. Because arterial stiffness is influenced by multiple demographic, clinical, and behavioral factors, including age, adiposity, hypertension, and movement behaviors, evaluating functional fitness within this broader context may improve our understanding of its relationship with vascular aging. If functional fitness exhibits stronger associations with arterial stiffness than behavioral measures of physical activity, it may provide clinically useful information that complements conventional estimates of weekly activity levels or sedentary time. This perspective may also help explain why older adults with similar physical activity levels often exhibit markedly different vascular and functional profiles.
Therefore, the present study investigated the associations of objectively measured physical activity, sedentary time, and multicomponent functional fitness with carotid-femoral pulse wave velocity in community-dwelling older adults, while accounting for established demographic and clinical correlates of arterial stiffness. We hypothesized that functional fitness would exhibit stronger associations with arterial stiffness than accelerometer-derived measures of physical activity and sedentary behavior, reflecting its multidimensional representation of overall physical function.
2. Materials and Methods
2.1. Participants
This cross-sectional observational study included community-dwelling older adults aged ≥60 years recruited from outpatient clinics and senior community centers in the city of Porto, Portugal. Eligibility criteria included the ability to perform functional assessments independently and the absence of acute or unstable clinical conditions that limit physical testing. Individuals with severe neurological, musculoskeletal, cardiovascular, or cognitive impairments compromising safe participation in the procedures were excluded.
Sample size estimation was performed a priori using G*Power software (version 3.1.3, University of Kiel, Kiel, Germany), assuming α = 0.05, statistical power (1−β) = 0.80, and a moderate effect size (f2=0.15), with a minimum required sample of 84 participants. Approximately 400 community-dwelling older adults were invited to participate through outpatient clinics and senior community centers, of whom 236 agreed to participate in the study procedures. After screening and informed consent, 170 participants completed all study assessments (64–91 years; mean age: 73 ± 7 years).
The study complied with the Declaration of Helsinki and was approved by the Ethics Committee of the Faculty of Sport at the University of Porto (CEFADE 06.2016). All participants provided written informed consent before participation.
2.2. Study Design
The study was reported in accordance with the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) guidelines [23]. Data collection was conducted over 12 months at the research center facilities.
Participants attended two laboratory visits separated by seven days. During the first visit, participants completed medical history, anthropometric, and functional fitness assessments, followed by 7 days of accelerometer monitoring of habitual physical activity. After seven consecutive days of monitoring, participants returned to the laboratory for accelerometer retrieval and cardiovascular assessments, including blood pressure and carotid-femoral pulse wave velocity (PWVc-f) measurements.
2.3. Medical History and Anthropometric Assessments
Clinical and lifestyle information, including medication use, smoking habits, alcohol consumption, hypertension, diabetes mellitus, cardiovascular disease, kidney disease, and endocrine disorders, was obtained through a semi-structured interview.
Body mass and height were measured using a calibrated digital scale and stadiometer (Tanita™ Scan BC532, Tokyo, Japan), and body mass index (BMI) was calculated as body mass divided by height squared (kg/m2). Participants were categorized as normal weight (<25.0 kg/m2), overweight (25.0-29.9 kg/m2), or obesity (≥30.0 kg/m2). For selected analyses, overweight and obesity categories were combined.
Waist circumference was measured at the midpoint between the lower rib margin and the iliac crest, whereas hip circumference was obtained at the largest circumference of the buttocks. Waist-to-hip ratio (WHR) was subsequently calculated. Elevated cardiovascular risk was defined as WHR >1.03 (males) and >0.90 (females) according to ACSM guidelines [21].
2.4. Functional Fitness Assessment
Functional fitness was assessed using the Senior Fitness Test battery (formerly Fullerton Functional Fitness Test), which evaluates multiple physical domains associated with functional independence in older adults [24,25]. The assessment included the 30-s chair stand, arm curl, chair sit-and-reach, back scratch, 8-foot up-and-go, and 6-minute walk tests. All tests were conducted in the morning following a standardized 10-minute warm-up by trained evaluators. Available age- and sex-specific normative values previously were used as reference criteria.
An overall functional fitness score (0–6 points) was calculated by assigning one point for each test in which performance met or exceeded the corresponding normative reference value. This approach was adopted to provide a multidimensional estimate of overall functional capacity across mobility, muscular fitness, flexibility, balance/agility, and aerobic endurance domains.
Because no validated cut-off is available for the composite score, participants were dichotomized according to the distribution of scores in the sample. Individuals meeting normative values in five or six of the six functional tests were classified as having high functional fitness, whereas those meeting normative standards in four or fewer tests were classified as having low functional fitness.
2.5. Physical Activity and Sedentary Time Assessments
Habitual physical activity and sedentary behavior were objectively assessed using uniaxial accelerometers (ActiGraph™ GT1M, Pensacola, FL, USA). Participants were instructed to wear the device on the right hip during waking hours for seven consecutive days, removing it only for bathing, swimming, or water-based activities. Accelerometer data were processed using ActiLife™ software (version 6.11.4). Valid wear time was defined as at least three valid days (2 weekdays and 1 weekend day) with ≥10 h/day of wear time, according to standardized criteria [26]. Data were collected at 30 Hz and analyzed using 60-s epochs.
Physical activity intensity was classified according to established count thresholds [26]: sedentary behavior (0–99 counts/min), light physical activity (100–2019 counts/min), and moderate-to-vigorous physical activity (MVPA; ≥2020 counts/min). Participants were categorized as meeting (≥150 min/week) or not meeting (<150 min/week) current physical activity recommendations for older adults [21]. Sedentary time was additionally categorized according to sample distribution percentiles, with participants in the highest quartile (≥75th percentile) classified as highly sedentary.
2.6. Blood Pressure and Arterial Stiffness Assessments
Participants were instructed to refrain from food intake, caffeine, alcohol consumption, smoking, and vigorous physical activity for at least 60 min before cardiovascular assessments. After 10 min of seated rest in a quiet temperature-controlled room, brachial blood pressure was measured three times at 1-min intervals using a semi-automated oscillometric device (Colin BP-8800, Critikron™, Tampa, FL, USA). The average of the three measurements was used for analysis. Hypertension was defined as systolic blood pressure ≥140 mmHg, diastolic blood pressure ≥90 mmHg, or current use of antihypertensive medication.
Central arterial stiffness was assessed by carotid-femoral pulse wave velocity (PWVc-f) using applanation tonometry (SphygmoCor™ version 8.0, AtCor Medical, Sydney, Australia), according to expert consensus recommendations and established reference values [27,28,29]. Measurements were performed in the supine position following blood pressure assessment. At least two PWVc-f measurements were obtained, and a third measurement was performed when consecutive values differed by >0.5 m/s.
Pulse transit time was determined from simultaneous electrocardiographic gating and carotid/femoral pulse wave recordings, and PWVc-f was calculated as the ratio between pulse transit distance and transit time [30]. Central systolic blood pressure was estimated using a validated generalized transfer function derived from radial artery waveforms [28,29]. Elevated arterial stiffness was defined as PWVc-f >10 m/s [27,30]. All devices were calibrated before testing procedures.
2.7. Statistical Analysis
Data normality was assessed using the Kolmogorov-Smirnov test and visual inspection of distribution plots. Continuous variables are presented as mean ± standard deviation (SD), whereas categorical variables are expressed as absolute and relative frequencies. Sex differences were evaluated using independent-samples Student’s t tests, Mann-Whitney U tests, or chi-square tests, as appropriate. Spearman correlation analyses were performed to examine the associations between PWVc-f and individual functional fitness components, as well as the composite functional fitness score.
Independent correlates of arterial stiffness were investigated using hierarchical multiple linear regression, with PWVc-f entered as the dependent variable. Predictors were entered sequentially according to their established relevance, as determinants of arterial stiffness. Model 1 included age and sex; Model 2 additionally incorporated BMI and hypertension status; Model 3 further included MVPA and sedentary time; and Model 4 added the composite functional fitness score. Changes in explained variance (ΔR2) were calculated at each step to determine the incremental contribution of each block of variables.
Binary logistic regression analyses were subsequently performed to estimate odds ratios (OR) and 95% confidence intervals (95% CI) for elevated arterial stiffness (PWVc-f >10 m/s). Separate crude and adjusted models were constructed for functional fitness classification (high vs. low) and compliance with current MVPA recommendations (≥150 vs. <150 min/week). Adjusted models included age, sex, BMI, and hypertension status as covariates.
To further examine whether the association between age and arterial stiffness differed according to functional fitness, an exploratory two-way analysis of variance (ANOVA) was performed using predefined age strata and functional fitness classification (high vs. low). Main effects for age group and functional fitness, as well as their interaction, were examined.
Model assumptions were evaluated through residual analyses. Multicollinearity in the regression models was assessed using variance inflation factors (VIF) and tolerance statistics, with VIF values <5 and tolerance values >0.20 considered indicative of acceptable collinearity. Missing data were handled using complete-case analyses, as missingness was low (<5% for all variables).
Statistical significance was set at p ≤ 0.05. All statistical analyses were performed using SPSS version 29.0 (IBM Corp., Armonk, NY, USA).
3. Results
3.1. Participant Characteristics
Table 1 summarizes the demographic, anthropometric, clinical, vascular, physical activity, and functional characteristics of the sample. The sample was predominantly composed of women (72.9%) and had a mean age of 72.3 ± 6.7 years. Excess body weight was highly prevalent, with 42.4% and 40.6% classified as overweight and obese, respectively, whereas only 17.1% had normal weight. Mean BMI was 29.4 ± 4.5 kg/m2. Cardiometabolic risk factors were also common. Hypertension, diabetes mellitus, and current smoking were reported by 51.5%, 22.4%, and 14.5% of participants, respectively. In addition, 36.5% were receiving antihypertensive medication and 39.8% were using lipid-lowering drugs. Mean systolic blood pressure was 132.3 ± 17.5 mmHg, and mean PWVc-f was 11.2 ± 2.7 m/s. Overall, 62.3% exceeded the clinical threshold for elevated arterial stiffness (>10 m/s).
Daily MVPA averaged 20.5 ± 19.2 min, whereas sedentary time approached 450 min/day. Functional fitness was generally low according to age-specific normative values, with a mean composite functional fitness score of 4.1 ± 1.4 points and 55.9% of the sample classified as having low functional fitness.
3.2. Sex Differences
Table 2 presents sex-specific comparisons of hemodynamic, vascular, physical activity, and functional fitness variables. Men exhibited lower resting heart rate (p = 0.011) and higher PWVc-f values than women (12.1 ± 2.9 vs. 10.9 ± 2.6 m/s, p = 0.010), whereas peripheral and central blood pressure measures did not differ between sexes. Consistent with these findings, the prevalence of elevated arterial stiffness (PWVc-f >10 m/s) was greater among men than women (76.2% vs. 57.1%, p = 0.030). Sex differences in movement behaviors were modest. Mean MVPA was similar between groups, although women accumulated less sedentary time than men (441 ± 87 vs. 477 ± 69 min/day, p = 0.027). Conversely, the prevalence of insufficient MVPA (<150 min/week) was higher among women (71.0% vs. 51.5%, p = 0.040).
Men performed better in the chair stand and 6-minute walk tests (p < 0.05), whereas no sex differences were observed for upper-body strength, flexibility, or agility. They also achieved higher composite functional fitness scores than women (4.43 ± 1.35 vs. 3.91 ± 1.36 points, p = 0.032). Accordingly, low functional fitness was more prevalent among women than men (61.5% vs. 40.9%, p = 0.019).
3.3. Associations Between Arterial Stiffness and Functional Fitness
Spearman correlation analyses demonstrated significant associations between PWVc-f and all functional fitness measures (Table 3). Higher PWVc-f values were consistently associated with poorer functional performance across all tests, with the strongest association observed for the 8-foot up-and-go test (ρ = 0.479, p < 0.001), followed by the arm curl (ρ = −0.445), 6-minute walk (ρ = −0.428), chair stand (ρ = −0.366), the composite functional fitness score (ρ = −0.338), back scratch (ρ = −0.261), and chair sit-and-reach (ρ = −0.211; all p ≤ 0.010).
3.4. Independent Correlates of Arterial Stiffness
Table 4 presents the hierarchical multiple regression models examining independent correlates of PWVc-f. Age and sex (Model 1) explained 40.4% of the variance in PWVc-f (R2 = 0.404, p < 0.001). The addition of BMI and hypertension status (Model 2) resulted in only a small and non-significant increase in explained variance (ΔR2 = 0.011, p = 0.342). Neither MVPA nor sedentary time (Model 3) improved model fit (ΔR2 < 0.001, p = 0.996). Similarly, adding the composite functional fitness score in Model 4 resulted in only a trivial, non-significant increase in explained variance (ΔR2 = 0.003, p = 0.455). Multicollinearity was low across all models, with VIF values ranging from 1.10 to 1.63 and tolerance values exceeding 0.60 for all predictors.
The final model explained 41.8% of the variance in PWVc-f (R2 = 0.418). Among all predictors, only age remained independently associated with PWVc-f (β = 0.570, p < 0.001), whereas sex showed a borderline association (β = 0.135, p = 0.074). BMI, hypertension status, MVPA, sedentary time, and the composite functional fitness score were not independently associated with arterial stiffness. Given the consistent attenuation of the associations between functional fitness and PWVc-f after multivariable adjustment, an exploratory analysis was subsequently performed to examine whether the relationship between age and arterial stiffness differed according to functional fitness level.
3.5. Functional Fitness, Physical Activity, and Elevated Arterial Stiffness
Logistic regression analyses examining factors associated with elevated arterial stiffness (PWVc-f >10 m/s) are presented in Table 5. In the unadjusted model, participants with high functional fitness exhibited significantly lower odds of elevated arterial stiffness than those with low functional fitness (OR = 0.39, 95% CI = 0.20–0.78, p = 0.007). However, this association was attenuated and no longer statistically significant after adjustment for age, sex, BMI, and hypertension status (OR = 0.56, 95% CI = 0.25–1.29, p = 0.176). Meeting the recommendation of at least 150 min/week of MVPA was not associated with elevated arterial stiffness in either the crude (OR = 0.68, 95% CI = 0.32–1.45, p = 0.319) or adjusted models (OR = 1.21, 95% CI = 0.48–3.06, p = 0.690).
3.6. Exploratory Analysis
Results of the exploratory two-way ANOVA indicated significant differences in PWVc-f across age groups (F = 16.985, p < 0.001, partial η2 = 0.267). In contrast, neither the main effect of functional fitness classification (F = 0.789, p = 0.376, partial η2 = 0.006) nor the interaction between age group and functional fitness (F = 0.358, p = 0.784, partial η2 = 0.008) reached statistical significance. These findings provide no evidence that the age-related pattern of arterial stiffness differs according to functional fitness classification.
4. Discussion
This study examined the associations of objectively measured physical activity, sedentary behavior, and multidimensional functional fitness with PWVc-f in community-dwelling older adults. The main findings were: a) arterial stiffness was inversely associated with all dimensions of functional fitness, whereas no meaningful associations were observed for objectively measured physical activity or sedentary behavior; b) participants with higher functional fitness exhibited substantially lower odds of elevated arterial stiffness in unadjusted analyses; c) however, these associations were markedly attenuated after adjustment for age and other established demographic and clinical correlates, with age emerging as the only consistent independent correlate of PWVc-f across all regression models.
The prominent influence of age presently observed is consistent with current understanding of vascular aging. Central arterial stiffness increases progressively throughout life as a consequence of cumulative structural and functional alterations of the arterial wall, including elastin fragmentation, collagen deposition, medial calcification, endothelial dysfunction, and chronic low-grade inflammation [8,27,29]. Accordingly, age has consistently been identified as the strongest determinant of carotid-femoral PWV across different populations, often outweighing the contribution of modifiable lifestyle factors [1,3,6].
Our findings should therefore be interpreted within this broader context of vascular aging. Although functional fitness demonstrated stronger unadjusted associations with PWVc-f than objectively measured physical activity or sedentary behavior, these relationships were no longer statistically significant after accounting for age and other established correlates. Exploratory analyses likewise provided no evidence that the age-related pattern of arterial stiffness differed according to functional fitness level. Together, these findings indicate that the observed association between functional fitness and arterial stiffness is largely explained by physiological processes accompanying aging rather than by an independent relationship between these variables.
A biological explanation for these findings is that functional fitness integrates the performance of multiple physiological systems that progressively decline with advancing age [21]. These same age-related processes also contribute to arterial stiffening through structural and functional alterations of the arterial wall [8,29], providing a common physiological basis for the observed associations.
Previous studies likewise support this interpretation. Lower carotid-femoral PWV has been associated with greater cardiorespiratory fitness [31], muscular strength [19], gait performance and physical function [32], as well as with composite measures of physical performance [33,34,35,36]. Most previous investigations, however, have evaluated isolated fitness components rather than multidimensional functional capacity, and relatively few have examined these associations after simultaneously accounting for major determinants of vascular aging. Our results therefore extend the existing literature by demonstrating that multidimensional functional fitness exhibits stronger unadjusted associations with central arterial stiffness than objectively measured movement behaviors, while showing that these associations are largely attributable to age.
From a clinical perspective, these findings suggest that functional fitness should be interpreted primarily as an integrated indicator of age-related physiological decline rather than as an independent determinant of arterial stiffness. Functional performance reflects the cumulative effects of aging across multiple physiological systems, many of which are also implicated in vascular aging. Accordingly, its association with PWVc-f is better viewed as an expression of the close interplay between functional and vascular aging than as evidence of a direct vascular effect.
Nevertheless, the cross-sectional nature of the present study does not preclude a beneficial effect of improving functional fitness on vascular health. Exercise interventions capable of enhancing functional fitness have been shown to improve endothelial function, autonomic regulation, blood pressure control, vascular remodeling, and systemic inflammation [10,37]. Accordingly, the absence of an independent association should be interpreted with caution, as observational analyses cannot distinguish shared age-related processes from causal relationships. Whether maintaining or improving functional fitness can attenuate the progression of arterial stiffening remains an important question to be addressed in longitudinal studies and randomized controlled trials.
Contrary to our initial hypothesis, objectively measured physical activity and sedentary behavior were not associated with PWVc-f in the present study. Neither MVPA nor sedentary time correlated significantly with arterial stiffness or independently predicted elevated PWVc-f in the adjusted analyses. Although these results appear to contrast with the well-established cardiovascular benefits of regular physical activity [10,12,13,18,32], they are consistent with systematic reviews indicating that associations between objectively measured habitual physical activity and central arterial stiffness are generally modest [13,14].
One explanation relates to the method used to quantify habitual physical activity. Systematic reviews have consistently shown that studies relying on self-reported questionnaires tend to report stronger associations with arterial stiffness than those using accelerometry [13,14]. Whereas questionnaires are susceptible to recall bias and misclassification of activity intensity and duration, accelerometers provide a more objective estimate of habitual movement behavior. Consequently, objectively measured physical activity may demonstrate weaker associations with PWVc-f despite providing greater measurement validity.
A second explanation is that habitual movement behavior represents only one of several determinants of vascular aging. Arterial stiffness reflects the cumulative influence of aging, blood pressure, adiposity, metabolic health, inflammation, and other long-term physiological processes [8,29]. Within this multifactorial framework, the relatively small contribution of daily movement behavior observed in the present study appears biologically plausible.
Finally, characteristics of the study sample may also have influenced these findings. Participants accumulated relatively little MVPA and spent prolonged periods in sedentary behavior, resulting in a restricted range of movement behaviors. Such limited variability may reduce the ability to detect statistically significant associations, particularly when expected effect sizes are small. Hence, objectively measured movement behaviors alone may not adequately capture the complex physiological processes underlying vascular aging in community-dwelling older adults.
Our findings have practical implications. Although functional fitness was not independently associated with arterial stiffness after adjustment for age and other established correlates, it consistently exhibited stronger unadjusted associations with PWVc-f than objectively measured physical activity or sedentary behavior. These observations reinforce current recommendations advocating the routine assessment of physical function in older adults [21]. Simple performance-based tests may provide clinically useful information about overall physiological status and help identify individuals with less favorable vascular profiles, even if they do not represent independent determinants of arterial stiffness.
The interpretation of these findings is strengthened by several methodological features. Physical activity and sedentary behavior were objectively assessed using accelerometry, minimizing recall bias and improving measurement precision. Arterial stiffness was evaluated by carotid-femoral PWV, the reference standard for assessing central arterial stiffness [8,29]. In addition, functional fitness was assessed using the Fullerton Functional Fitness Test, allowing the construction of a multidimensional composite score that better reflects overall physical function than isolated fitness measures.
Several limitations should also be acknowledged. The cross-sectional design precludes causal inference. Therefore, it cannot be determined whether reduced functional fitness contributes to arterial stiffening, whether vascular aging contributes to functional decline, or whether both processes evolve concurrently with advancing age. Although major confounders, including age, sex, BMI, and hypertension status, were included in the adjusted analyses, residual confounding by unmeasured variables cannot be excluded. The relatively low levels of MVPA and high prevalence of sedentary behavior may also have limited the ability to detect associations between objectively measured movement behaviors and PWVc-f. Finally, because no validated thresholds currently exist for the composite functional fitness score, participants were classified using a sample-derived cut-off, which may limit the external applicability of this classification.
5. Conclusions
Multidimensional functional fitness demonstrated stronger unadjusted associations with central arterial stiffness than objectively measured physical activity or sedentary behavior in community-dwelling older adults. However, these associations were largely explained by age, which emerged as the only consistent independent correlate of PWVc-f. These findings suggest that functional fitness is best interpreted as an integrated expression of age-related physiological decline that parallels vascular aging, rather than as an independent determinant of arterial stiffness. Longitudinal studies and randomized controlled trials are needed to determine whether preserving or improving functional fitness can attenuate the progression of arterial stiffening beyond that expected with chronological aging.
Author Contributions
Conceptualization: Adjane Maria Pontes César and Joana Carvalho; Methodology: Adjane Maria Pontes César, Edmar Lacerda Mendes, Alynne Christian Ribeiro Andaki, André Pereira dos Santos, Jessica Cordeiro, Paulo Farinatti, and Joana Carvalho; Formal analysis and investigation: Adjane Maria Pontes César, Edmar Lacerda Mendes, and Paulo Farinatti; Writing - original draft preparation: Edmar Lacerda Mendes, Alynne Christian Ribeiro Andaki, André Pereira dos Santos, and Paulo Farinatti; Writing - review and editing: Adjane Maria Pontes César, Edmar Lacerda Mendes, Alynne Christian Ribeiro Andaki, André Pereira dos Santos, Jessica Cordeiro, Jorge Mota, Paulo Farinatti, and Joana Carvalho; Resources: Jorge Mota and Joana Carvalho; Supervision: Joana Carvalho. All authors read and approved the final manuscript.
Funding
This research was supported by grants from the ‘Fundação para a Ciência e a Tecnologia’ (FCT, grant UIDB/00617/2020, doi:10.54499/UIDB/00617/2020), ‘Fundação de Amparo à Pesquisa no Estado de Minas Gerais’ (FAPEMIG, grant APQ-05247- 23), ‘Conselho Nacional de Desenvolvimento Científico e Tecnológico’ (CNPq, grant 305262/2023-8), and ‘Fundação Carlos Chagas Filho de Apoio à Pesquisa no Estado do Rio de Janeiro’ (FAPERJ, grant E-26/204.102/2024).
Institutional Review Board Statement
Approval was obtained from the Ethics Committee of the Faculty of Sport at the University of Porto, Portugal (CEFADE 06.2016). The procedures used in this study adhere to the tenets of the Declaration of Helsinki.
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Data Availability Statement
The raw data are available on reasonable request from the corresponding authors to preserve individuals’ privacy under the European General Data Protection Regulation.
Conflicts of Interest
The authors declare no conflicts of interest. The funders had no role in the design of the study; in the collection, analyses, or interpretation of data; in the writing of the manuscript; or in the decision to publish the results.
Abbreviations
The following abbreviations are used in this manuscript:
| BMI | Body Mass Index |
| CI | Confidence Interval |
| DBP | Diastolic Blood Pressure |
| MVPA | Moderate-to-Vigorous Physical Activity |
| OR | Odds Ratio |
| PWVc-f | Carotid-Femoral Pulse Wave Velocity |
| SD | Standard Deviation |
| SBP | Systolic Blood Pressure |
| VIF | Variance Inflation Factor |
| WHR | Waist-to-Hip Ratio |
References
- Vlachopoulos, C.; Aznaouridis, K.; Stefanadis, C. Prediction of cardiovascular events and all-cause mortality with arterial stiffness: a systematic review and meta-analysis. J. Am. Coll. Cardiol. 2010, 55, 1318–27. [Google Scholar]
- Willum-Hansen, T.; Staessen, J. A.; Torp-Pedersen, C.; Rasmussen, S.; Thijs, L.; Ibsen, H.; Jeppesen, J. Prognostic value of aortic pulse wave velocity as index of arterial stiffness in the general population. Circulation 2006, 113, 664–70. [Google Scholar] [CrossRef] [PubMed]
- Mitchell, G. F.; Parise, H.; Benjamin, E. J.; Larson, M. G.; Keyes, M. J.; Vita, J. A.; Vasan, R. S.; Levy, D. Changes in arterial stiffness and wave reflection with advancing age in healthy men and women: the Framingham Heart Study. Hypertension 2004, 43, 1239–45. [Google Scholar] [CrossRef] [PubMed]
- Laurent, S.; Boutouyrie, P.; Asmar, R.; Gautier, I.; Laloux, B.; Guize, L.; Ducimetiere, P.; Benetos, A. Aortic stiffness is an independent predictor of all-cause and cardiovascular mortality in hypertensive patients. Hypertension 2001, 37, 1236–41. [Google Scholar] [CrossRef] [PubMed]
- Meaume, S.; Benetos, A.; Henry, O. F.; Rudnichi, A.; Safar, M. E. Aortic pulse wave velocity predicts cardiovascular mortality in subjects >70 years of age. Arterioscler. Thromb. Vasc. Biol. 2001, 21, 2046–50. [Google Scholar] [CrossRef] [PubMed]
- Eikas, J. G.; Gerdts, E.; Halland, H.; Midtbo, H.; Cramariuc, D.; Kringeland, E. Arterial Stiffness in Overweight and Obesity: Association with Sex, Age, and Blood Pressure. High Blood Press Cardiovasc Prev. 2023, 30, 435–443. [Google Scholar] [CrossRef] [PubMed]
- Kim, H. L. Arterial stiffness and hypertension. Clin. Hypertens. 2023, 29, 31. [Google Scholar] [CrossRef] [PubMed]
- Wilkinson, I. B.; Maki-Petaja, K. M.; Mitchell, G. F. Uses of Arterial Stiffness in Clinical Practice. Arterioscler. Thromb. Vasc. Biol. 2020, 40, 1063–1067. [Google Scholar] [CrossRef] [PubMed]
- Tanaka, H.; Dinenno, F. A.; Monahan, K. D.; Clevenger, C. M.; DeSouza, C. A.; Seals, D. R. Aging, habitual exercise, and dynamic arterial compliance. Circulation 2000, 102, 1270–5. [Google Scholar] [CrossRef] [PubMed]
- Tanaka, H. Antiaging effects of aerobic exercise on systemic arteries. Hypertension 2019, 74, 237–243. [Google Scholar] [CrossRef] [PubMed]
- Brunner, E. J.; Shipley, M. J.; Witte, D. R.; Singh-Manoux, A.; Britton, A. R.; Tabak, A. G.; McEniery, C. M.; Wilkinson, I. B.; Kivimaki, M. Arterial stiffness, physical function, and functional limitation: the Whitehall II Study. Hypertension 2011, 57, 1003–9. [Google Scholar] [CrossRef] [PubMed]
- Park, W.; Park, H. Y.; Lim, K.; Park, J. The role of habitual physical activity on arterial stiffness in elderly Individuals: a systematic review and meta-analysis. J. Exerc Nutr. Biochem 2017, 21, 16–21. [Google Scholar] [CrossRef]
- Germano-Soares, A.; Andrade-Lima, A.; Menêses, A.; Correia, M.; Parmenter, B.; Tassitano, R.; Cucato, G.; Ritti-Dias, R. Association of time spent in physical activities and sedentary behaviors with carotid-femoral pulse wave velocity: A systematic review and meta-analysis. Atherosclerosis 2018, 269, 211–218. [Google Scholar] [CrossRef] [PubMed]
- Lear, R.; Metcalf, B.; Brailey, G.; Nunns, M.; Bond, B.; Hillsdon, M.; Pulsford, R. Associations of habitual physical activity and carotid-femoral pulse wave velocity; a systematic review and meta-analysis of observational studies. PLoS ONE 2023, 18, e0284164. [Google Scholar] [CrossRef] [PubMed]
- Vaitkevicius, P. V.; Fleg, J. L.; Engel, J. H.; O’Connor, F. C.; Wright, J. G.; Lakatta, L. E.; Yin, F. C.; Lakatta, E. G. Effects of age and aerobic capacity on arterial stiffness in healthy adults. Circulation 1993, 88, 1456–62. [Google Scholar] [CrossRef] [PubMed]
- Yamamoto, K.; Kawano, H.; Gando, Y.; Iemitsu, M.; Murakami, H.; Sanada, K.; Tanimoto, M.; Ohmori, Y.; Higuchi, M.; Tabata, I.; Miyachi, M. Poor trunk flexibility is associated with arterial stiffening. Am. J. Physiol. Heart Circ. Physiol. 2009, 297, H1314–8. [Google Scholar] [CrossRef] [PubMed]
- Gando, Y.; Murakami, H.; Kawakami, R.; Yamamoto, K.; Kawano, H.; Tanaka, N.; Sawada, S. S.; Miyatake, N.; Miyachi, M. Cardiorespiratory Fitness Suppresses Age-Related Arterial Stiffening in Healthy Adults: A 2-Year Longitudinal Observational Study. J. Clin. Hypertens. (Greenwich) 2016, 18, 292–8. [Google Scholar] [PubMed]
- Tanaka, H.; DeSouza, C. A.; Seals, D. R. Absence of age-related increase in central arterial stiffness in physically active women. Arterioscler. Thromb. Vasc. Biol. 1998, 18, 127–32. [Google Scholar] [CrossRef] [PubMed]
- Albin, E. E.; Brellenthin, A. G.; Lang, J. A.; Meyer, J. D.; Lee, D.-C. Cardiorespiratory fitness and muscular strength on arterial stiffness in older adults. Med. Sci. Sports Exerc 2020, 52. [Google Scholar] [CrossRef] [PubMed]
- Dvoretskiy, S.; Lieblein-Boff, J. C.; Jonnalagadda, S.; Atherton, P. J.; Phillips, B. E.; Pereira, S. L. Exploring the Association between Vascular Dysfunction and Skeletal Muscle Mass, Strength and Function in Healthy Adults: A Systematic Review. Nutrients 2020, 12. [Google Scholar] [CrossRef] [PubMed]
- American College of Sports Medicine, ACSM’s Guidelines for Exercise Testing and Prescription, 12th ed.; Wolters Kluwer: Philadelphia, 2025; p. 680.
- Migueles, J. H.; Cadenas-Sanchez, C.; Ekelund, U.; Delisle Nystrom, C.; Mora-Gonzalez, J.; Lof, M.; Labayen, I.; Ruiz, J. R.; Ortega, F. B. Accelerometer Data Collection and Processing Criteria to Assess Physical Activity and Other Outcomes: A Systematic Review and Practical Considerations. Sports Med. 2017, 47, 1821–1845. [Google Scholar] [CrossRef] [PubMed]
- von Elm, E.; Altman, D. G.; Egger, M.; Pocock, S. J.; Gotzsche, P. C.; Vandenbroucke, J. P.; Initiative, S. The Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) statement: guidelines for reporting observational studies. Lancet 2007, 370, 1453–7. [Google Scholar] [CrossRef] [PubMed]
- Rikli, R. E.; Jones, C. J. Functional Fitness Normative Scores for Community-Residing Older Adults, Ages 60-94. J. Aging Physl Act. 1999a, 7, 162–181. [Google Scholar] [CrossRef]
- Rikli, R. E.; Jones, C. J. Development and Validation of a Functional Fitness Test for Community-Residing Older Adults. J. Aging Phys. Act. 1999b, 7, 129–161. [Google Scholar] [CrossRef]
- Troiano, R. P.; Berrigan, D.; Dodd, K. W.; Masse, L. C.; Tilert, T.; McDowell, M. Physical activity in the United States measured by accelerometer. Med. Sci. Sports Exerc 2008, 40, 181–8. [Google Scholar] [CrossRef] [PubMed]
- Van Bortel, L. M.; Laurent, S.; Boutouyrie, P.; Chowienczyk, P.; Cruickshank, J. K.; De Backer, T.; Filipovsky, J.; Huybrechts, S.; Mattace-Raso, F. U.; Protogerou, A. D.; Schillaci, G.; Segers, P.; Vermeersch, S.; Weber, T.; Artery, S. European Society of Hypertension Working Group on Vascular, S.; Function; European Network for Noninvasive Investigation of Large, A., Expert consensus document on the measurement of aortic stiffness in daily practice using carotid-femoral pulse wave velocity. J. Hypertens. 2012, 30, 445–8. [Google Scholar] [CrossRef] [PubMed]
- Chen, C. H.; Nevo, E.; Fetics, B.; Pak, P. H.; Yin, F. C.; Maughan, W. L.; Kass, D. A. Estimation of central aortic pressure waveform by mathematical transformation of radial tonometry pressure. Validation of generalized transfer function. Circulation 1997, 95, 1827–36. [Google Scholar] [CrossRef] [PubMed]
- Laurent, S.; Cockcroft, J.; Van Bortel, L.; Boutouyrie, P.; Giannattasio, C.; Hayoz, D.; Pannier, B.; Vlachopoulos, C.; Wilkinson, I.; Struijker-Boudier, H. European Network for Non-invasive Investigation of Large, A., Expert consensus document on arterial stiffness: methodological issues and clinical applications. Eur. Heart J. 2006, 27, 2588–605. [Google Scholar] [CrossRef] [PubMed]
- Reference Values for Arterial Stiffness Collaboration, Determinants of pulse wave velocity in healthy people and in the presence of cardiovascular risk factors: ‘establishing normal and reference values’. Eur. Heart J. 2010, 31, 2338–50. [CrossRef] [PubMed]
- Nayor, M.; Gajjar, P.; Miller, P.; Murthy, V. L.; Shah, R. V.; Houstis, N. E.; Velagaleti, R. S.; Larson, M. G.; Vasan, R. S.; Lewis, G. D.; Mitchell, G. F. Arterial Stiffness and Cardiorespiratory Fitness Impairment in the Community. J. Am. Heart Assoc. 2023, 12, e029619. [Google Scholar] [CrossRef] [PubMed]
- de Sousa, M. K. F.; Silva, R. M.; Freire, Y. A.; Souto, G. C.; Câmara, M.; Cabral, L. L. P.; Macêdo, G. A. D.; Costa, E. C.; Oliveira, R. S. Associations between physical activity and cardiorespiratory fitness with vascular health phenotypes in older adults: a cross-sectional study. Front Physiol. 2023, 14, 1096139. [Google Scholar] [CrossRef] [PubMed]
- Nishiwaki, M.; Kurobe, K.; Kiuchi, A.; Nakamura, T.; Matsumoto, N. Sex differences in flexibility-arterial stiffness relationship and its application for diagnosis of arterial stiffening: a cross-sectional observational study. PLoS ONE 2014, 9, e113646. [Google Scholar] [CrossRef] [PubMed]
- Nihei, S.; Ogawa, M.; Hashimoto, Y.; Kikuchi, N.; Nakazato, K.; Okamoto, T. Arterial stiffness and physical fitness on cognitive function in community-dwelling middle-aged and older adults. Aging Clin. Exp. Res. 2023, 35((9)), 1845–1854. [Google Scholar] [CrossRef] [PubMed]
- Yoo, T. K.; Lee, S.; Park, S. J.; Lee, J. Y. Arterial stiffness expressed as brachial-ankle pulse wave velocity and gait assessment independent of lower extremity strength: a cross-sectional study in the older men population. J. Geriatr. Cardiol. 2023, 20, 91–99. [Google Scholar] [CrossRef] [PubMed]
- Yoo, T. K.; Rhim, H. C.; Park, S. H.; Park, S.; Lee, J. Y. Relationship between physical fitness and arterial stiffness in Korean older adults. Medicine 2022, 101, e30617. [Google Scholar] [CrossRef] [PubMed]
- Farinatti, P.; da Silva Itaborahy, A.; de Paula, T.; Monteiro, W. D.; Neves, M. F. Effects of aerobic, resistance and concurrent exercise on pulse wave reflection and autonomic modulation in men with elevated blood pressure. Sci. Rep. 2021, 11, 760. [Google Scholar] [CrossRef] [PubMed]

Table 1.
Participant characteristics.
 |
Table 2.
Sex differences in hemodynamic, vascular, physical activity, and functional fitness variables.
Table 2.
Sex differences in hemodynamic, vascular, physical activity, and functional fitness variables.
 |
Table 3.
Spearman correlations between PWVc-f and functional fitness variables.
 |
Table 4.
Hierarchical multiple linear regression models examining independent correlates of carotid-femoral pulse wave velocity.
Table 4.
Hierarchical multiple linear regression models examining independent correlates of carotid-femoral pulse wave velocity.
 |
Table 5.
Crude and adjusted logistic regression models for elevated arterial stiffness (PWVc-f > 10 m/s).
Table 5.
Crude and adjusted logistic regression models for elevated arterial stiffness (PWVc-f > 10 m/s).
 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2026 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



