Submitted:
26 June 2026
Posted:
30 June 2026
You are already at the latest version
Abstract
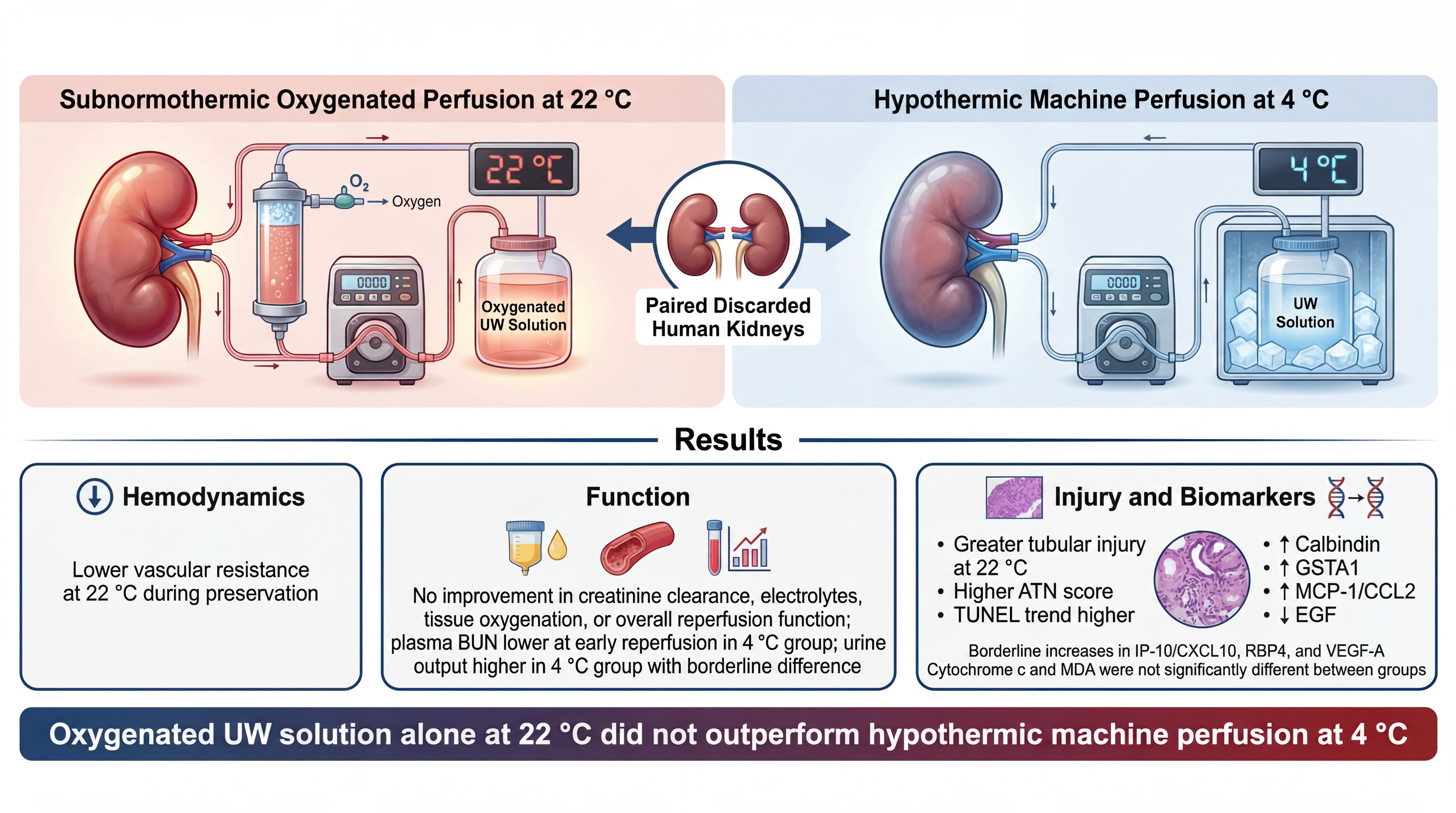
Background: Subnormothermic oxygenated machine perfusion has been shown to improve kidney preservation in the preclinical setting. However, whether oxygenated perfusion without an oxygen carrier provides superior protection over standard hypothermic machine perfusion at 4 °C in human kidneys has not been established.
Methods: In this study, we assessed whether oxygenated University of Wisconsin (UW) solution perfusion at 22 °C provides improved protection compared with conventional hypothermic machine perfusion (HMP) at 4 °C using a paired human kidney model. Five pairs of discarded human kidneys were recruited for the study. For each donor pair, one kidney was randomized to 12 h oxygenated UW perfusion at 22 °C and the contralateral kidney was perfused at 4 °C with a clinically relevant kidney perfusion pump. After preservation, both kidneys were reperfused with whole blood at 37 °C for 4 h. Hemodynamic and functional parameters were assessed during preservation and reperfusion, including vascular resistance, renal blood flow, creatinine clearance, blood urea nitrogen, electrolyte levels, tissue oxygenation, and urine output. Histological injury was evaluated and a panel of kidney injury biomarkers were also measured.
Results: Vascular resistance during the preservation period was significantly lower in the kidneys preserved at 22 °C compared to the HMP group, indicating improved flow dynamics. However, the improved vascular resistance observed during 22 °C preservation did not translate into superior post-reperfusion kidney function or tissue protection compared with 4 °C HMP. Renal blood flow, creatinine clearance, tissue oxygenation, cytochrome c release and malondialdehyde (MDA) levels were comparable between groups, while kidneys preserved at 22 °C had significantly higher acute tubular necrosis scores, higher blood urea nitrogen (BUN) levels, increased calbindin, glutathione S-transferase A1, monocyte chemoattractant protein-1 levels, and lower epidermal growth factor levels.
Conclusion: These data demonstrate that oxygenated UW perfusion at 22 °C fails to provide superior protection to conventional HMP at 4 °C in discarded human kidneys transplantation model.
Keywords:
kidney preservation
; hypothermic machine perfusion
; subnormothermic perfusion
; discarded human kidneys
; Ischemia-reperfusion injury
1. Introduction
Kidney transplantation is the treatment of choice for patients with end-stage renal disease. Compared with dialysis, kidney transplantation provides better long-term survival and quality of life [1,2]. The success of this therapy is dependent on the preservation modality that is applied from organ procurement to transplantation. Ischemia–reperfusion injury (IRI) is one of the most damaging phenomena that occurs during this period. IRI is triggered when an ischemic kidney is suddenly reoxygenated following reperfusion. The process sets off a sequence of metabolic dysregulation, oxidative stress and inflammation that impairs early graft function and contribute to the development of long-term graft dysfunction [3,4]. This is becoming more pressing with increasing transplant demand and greater use of expanded-criteria and donation-after-circulatory-death (DCD) kidneys, which are at higher risk for preservation injury [5]. Therefore, preservation strategies that protect the kidneys during storage are crucial to enlarging the donor pool and promoting successful transplantation.
Traditional kidney preservation has relied on static cold storage or hypothermic machine perfusion (HMP) at 4 °C [6]. Cooling at 4 °C reduces metabolic demand, but prolonged hypothermic storage can cause energy depletion, cellular injury, delayed graft function, and increased immunogenicity [4]. In contrast, normothermic (37 °C) and subnormothermic (20–22 °C) can reduce hypoxic injury, restore bioenergetics, and preserve tissue integrity [7,8,9]. In a previous study, we demonstrated that subnormothermic oxygenated perfusion at 22 °C provided better preservation than cold storage or normothermic perfusion [10]. Despite promising results, the main obstacle to clinical translation of this preservation strategy is the requirement for blood or other oxygen-carrying solutions. However, the need for blood or hemoglobin-based oxygen carriers limits clinical translation because of logistical, biosafety, cost, and availability concerns [11,12,13]. Consequently, a simple and accessible preservation strategy is required to facilitate widespread clinical adoption of subnormothermic perfusion for organ preservation. To this end, in porcine models, previous studies have proposed that subnormothermic oxygenated perfusion without an oxygen carrier can be an effective form of graft preservation. Agius et al. demonstrated that oxygenated University of Wisconsin (UW) solution perfusion at 22 °C improved perfusion, ATP levels and histological results when compared with 4 °C perfusion [14]. Abraham et al. further demonstrated that 22–25 °C acellular perfusion could be maintained for up to 24 hours and improves post-transplant graft function when compared with cold storage [8]. However, none of these studies has systematically evaluated the effectiveness of this strategy in a paired damaged discarded human kidney model in direct comparison with HMP.
In the present study, we hypothesized that oxygenated UW solution at 22 °C would provide superior protection compared with HMP at 4 °C in a simulated paired human discarded kidney transplantation model.
2. Materials and Methods
2.1. Organs’ Handling and Procurement
Five pairs of human kidney grafts were included in this study. This study was approved by Western University Research Ethics Board (106467). All procedures involving human biological materials were conducted in accordance with relevant institutional guidelines, applicable laws and regulations, and the ethical principles outlined in the Declaration of Helsinki. Donor confidentiality and privacy were maintained throughout the study, and no identifiable donor information is reported. All organs were originally retrieved for the purpose of clinical transplantation but were subsequently deemed unsuitable and discarded during post-retrieval evaluation. The discarded grafts were obtained through the International Institute for the Advancement of Medicine (IIAM, USA). All kidneys met our inclusion criteria, which required donor consent for research use, confirmed seronegativity for transmissible infections, and adequate organ integrity upon procurement. Exclusion criteria included evidence of gross anatomical abnormalities, prolonged warm ischemia, cold ischemia time over 48 hours, and positive serology for HIV, HBV, or HCV. Each graft was recovered following standard organ procurement procedures, flushed with cold UW preservation solution and transported on ice to the research facility under monitored cold ischemic conditions. Upon arrival, both kidneys from each donor pair were processed in parallel to minimize inter-donor variability. Warm and cold ischemia times were recorded for each organ pair. Table 1 shows the donors’ demographics.
2.2. Preservation of Grafts
After removal of perinephric adipose tissue, the renal artery and ureter of each kidney graft was cannulated using appropriately sized metal or Teflon cannulas and securely connected to an RM3 perfusion system (Waters Instrument Inc., Rochester, MN, USA). Our perfusion system included a pediatric oxygenator (Medtronic Inc., Minneapolis, MN, USA), PolyScience Circulating Water Bath (PolyScience, Niles, IL, USA), and a clinical preservation cassette (Waters Medical Systems, LLC, Rochester, USA). A detailed description of our perfusion system has been explained previously [15].The kidneys were perfused using UW machine perfusion solution under sterile and temperature-controlled conditions. From each donor pair, one kidney was assigned to subnormothermic oxygenated perfusion at 22 °C, while the contralateral kidney underwent conventional HMP at 4 °C using the same UW solution. The preservation phase was maintained for 12 hours in both groups. Throughout the perfusion, the circuit parameters including perfusion pressure, flow rate, and vascular resistance were continuously monitored and adjusted as needed to maintain stable hemodynamics. The perfusion pressure was kept constant at 50 mmHg during the entire preservation period.
2.3. Simulated Renal Transplantation Model
This study was approved by CBS Research Ethics Program. After the preservation phase, the renal grafts were reperfused with ABO compatible whole blood ( Canadian Blood Services, BC, Canada) diluted with PlasmaLyte solution (Baxter Corporation, Deerfield, IL) at 37 °C for 4 hours. The perfusate was supplemented with 2 mg of Verapamil (Sandoz Canada Inc., Boucherville, QC, Canada), 1 gram Cefazolin (Hikma Canada Limited, Mississauga, ON, Canada), 10,000 units of Heparin (Fresenius Kabi Canada Ltd., Richmond Hill, ON, Canada), and 10 mg/dL of creatinine (Sigma Aldrich, USA). The pH was adjusted to 7.35-7.45 throughout the reperfusion by adding Sodium bicarbonate solution (SteriMax Inc., Oakville, ON, Canada) or adjusting the CO2 levels. Heparin was replenished at a rate of 10,000 units per hour. During the experiment, the circuit pressure was maintained at 85 mmHg.
Urine output, renal blood flow rate, vascular resistance, and tissue oxygenation (monitored using the InSpectra StO₂ Tissue Oxygenation Monitor) were recorded hourly. In addition, urine and blood samples were collected at the same intervals. Blood samples were analyzed with i-STAT Handheld Blood Analyzer (Abbott Laboratories, Chicago, IL, USA). Renal function was assessed by measuring serum creatinine, blood urea nitrogen (BUN), and plasma electrolytes (Na⁺, K⁺) with the same analyzer. Creatinine clearance was measured using a method as described before [15]. After the 4-hour reperfusion period, each kidney was carefully disconnected from the perfusion circuit and bisected sagittally. From one half of each kidney, tissue specimens were excised and immersed in 10% neutral buffered formalin for 48 hours at room temperature. Following fixation, the samples were dehydrated through a graded series of ethanol, cleared in xylene, and subsequently embedded in paraffin wax using a standard histological protocol. Paraffin blocks were then sectioned into 5-µm-thick slices using a rotary microtome, and the sections were mounted onto glass slides. To evaluate tissue morphology and injury, hematoxylin and eosin (H&E) staining was performed. Martius Scarlet Blue (MSB) staining was used to assess hemorrhage. Additionally, TUNEL (Terminal deoxynucleotidyl transferase dUTP nick-end labeling) staining was conducted to detect apoptotic nuclei and quantify cell death within renal tissue. Histopathological images were analyzed by an independent histopathologist who was blinded to the experimental design. From the other half, tissue samples were excised and flash-frozen for biochemical analysis.
2.4. Cytochrome C Measurement
Urine samples collected at Hour 4 of reperfusion were analyzed to quantify cytochrome c as a marker of mitochondrial injury[16] using a Human CYCS / Cytochrome c (Sandwich ELISA Kit, LS-F11267, Vector Laboratories, Inc., CA, United States) according to the manufacturer’s instructions. Final values were normalized to total protein content as determined by a BCA (Thermo Fisher Scientific, Canada) assay.
2.5. Malondialdehyde (MDA) Colorimetric Assay
MDA serves as a key biomarker of oxidative stress and lipid peroxidation. Its detection in biological samples provides an indirect measure of cellular damage caused by reactive oxygen species (ROS) [17]. MDA assay was performed on flash frozen tissues using an MDA assay kit (Thermo Fisher Scientific, Canada, Catalog number EEA015). The results were normalized to the total protein of the tissue lysate measured via BCA assay.
2.6. Injury Markers Analysis
Serum samples collected at Hour 4 of reperfusion were analyzed to quantify a comprehensive panel of kidney injury biomarkers, because this terminal reperfusion time point reflects the cumulative impact of preservation and early reoxygenation injury, allowing detection of established differences in graft injury between groups. The analyzed markers included alpha-1-microglobulin, beta-2-microglobulin, cystatin C, epidermal growth factor (EGF), neutrophil gelatinase-associated lipocalin (NGAL), osteopontin (OPN), trefoil factor 3 (TFF3), tissue inhibitor of metalloproteinases-1 (TIMP-1), uromodulin, calbindin, clusterin (APO-J), glutathione S-transferase A1 (GSTA1), interleukin-18 (IL-18), interferon gamma-induced protein 10 (IP-10/CXCL10), kidney injury molecule-1 (KIM-1/TIM-1/HAVCR1), monocyte chemoattractant protein-1 (MCP-1/CCL2), osteoactivin (GPNMB), retinol-binding protein 4 (RBP4), renin, and vascular endothelial growth factor A (VEGF-A). These biomarkers were quantified using the ProcartaPlex™ Human Kidney Toxicity Panel 1 (11-plex) and Panel 2 (9-plex) assays (Thermo Fisher Scientific, Canada) using Luminex FLEXMAP 3D Instrument System. Data analysis was done by Analytics (software) xPONENT basic plus Thermo fisher connect platform. Final values were normalized to total protein content as determined by a BCA (Thermo Fisher Scientific, Canada) assay. The relative concentrations of these biomarkers were calculated with respect to the 4 °C group and are presented as a heatmap.
2.7. Statistical Analysis
All data were analyzed using GraphPad Prism software (version 11.0, GraphPad Software, San Diego, CA, USA). Results are expressed as mean ± standard deviation (SD). The normality of data distribution was assessed using the Shapiro–Wilk test. Comparisons between 2 groups at a single time point were performed using a paired t-test for normally distributed data and the Wilcoxon matched-pairs signed-rank test when normality assumptions were not met. For comparisons among multiple groups, one-way analysis of variance (ANOVA) followed by Tukey’s multiple comparison post hoc test was performed for normally distributed data. When the data did not meet the assumptions of normality, the Kruskal–Wallis test followed by Dunn’s multiple comparison test was applied. A p-value < 0.05 was considered statistically significant.
3. Results
3.1. Subnormothermic Perfusion at 22 °C Reduced Vascular Resistance During Preservation but Did Not Improve Reperfusion Function Compared with 4 °C
During the preservation and subsequent reperfusion phases, both 4 °C and 22 °C kidneys maintained stable hemodynamic and metabolic performance. However, distinct temperature-dependent trends were observed. During the 12-hour preservation phase, vascular resistance was consistently lower in kidneys preserved at 22 °C (decreasing from 0.32 ± 0.16 mmHg·min/mL at hour 1 to 0.13 ± 0.04 mmHg·min/mL at hour 12) compared with those preserved at 4 °C (declining from 0.436 ± 0.13 mmHg·min/mL at hour 1 to 0.31 ± 0.09 mmHg·min/mL at hour 12), indicating enhanced microvascular relaxation under subnormothermic oxygenated conditions (Figure 1A). Except for the first hour, vascular resistance was significantly lower in the 22 °C group compared with 4 °C group.
Renal blood flow increased steadily during reperfusion, rising from 152 ± 77.91 mL/min at hour 1 to 210 ± 138.20 mL/min at hour 4 in the 4 °C group, and from 137 ± 38.01 mL/min at hour 1 to 238 ± 154.17 mL/min at hour 4 in the 22 °C group (Figure 1B). Differences between groups were not statistically significant in any of the studied time points.
Creatinine clearance increased within the first hour, reaching approximately 3.34 ± 2.04 mL/min in the 4 °C group and 3.39 ± 2.09 mL/min in the 22 °C group, before declining to 1.70 ± 1.90 mL/min in the 4 °C group and 1.17 ± 0.84 mL/min in the 22 °C group at hour 4 (Figure 1C). Differences between groups were not statistically significant in any of the studied time points.
Plasma BUN levels showed a gradual decline throughout reperfusion, decreasing from 9.40 ± 3.28 mg/dL at baseline to 6.20 ± 2.86 mg/dL at hour 4 in the 4 °C group, and from 14.40 ± 6.22 mg/dL at baseline to 10.40 ± 3.43 mg/dL at hour 4 in the 22 °C group (Figure 1D). At hours 1 and 2, BUN levels were significantly lower in the 4 °C group compared with 22 °C group.
Plasma chloride (Cl⁻) and sodium (Na⁺) levels did not significantly differ between the 4 °C and 22 °C groups during the 4-hour reperfusion (Figure 2A and 2B).
Tissue oxygenation values were comparable between groups across the 4-hour reperfusion period (Figure 2C). At baseline (0 h), tissue oxygenation was 70.97 ± 15.54% at 4 °C and 70.41 ± 22.56% at 22 °C. Over time, the 4 °C group showed a modest dip at 2 hour (68.58 ± 16.13%) followed by an increase at 3 and 4 hours (75.10 ± 12.71% and 76.70 ± 15.19%). The 22 °C group showed a gradual rise over time, reaching the highest mean at 4 hour (80.26 ± 26.51%).
Total urine production during reperfusion was higher in the 4 °C group than in the 22 °C group. Mean urine volume was 94.80 ± 86.05 mL in the 4 °C group and 32.20 ± 39.02 mL in the 22 °C group. Differences between groups were not statistically significant (p-value= 0.0506).
3.2. Kidneys Preserved at 22 °C Exhibited Increased Histological Evidence of Tubular Injury Compared with 4 °C
H&E staining (Figure 3) showed early acute tubular necrosis (ATN) in both groups, characterized by tubular dilatation, reactive tubular epithelium, and focal necrotic debris within the tubular lumens. These changes were present in both samples but were more pronounced in the 22 °C sample. ATN scores were significantly higher in 22 °C compared with 4 °C (p-value= 0.0453).
TUNEL immunohistochemical staining was used to identify apoptotic cells within the tubular epithelium as a marker of acute tubular injury. Differences in the quantified TUNEL-positive area did not reach statistical significance between groups (p-value= 0.0702).
MSB staining did not demonstrate any significant thrombus formation within glomerular capillaries or blood vessels in either group.
3.3. Preservation at 22 °C Did Not Significantly Alter Cytochrome C Release or MDA Levels Compared with 4 °C
Urinary concertation of cytochrome c and MDA levels in tissue lysates were not significantly different between the 4 °C and 22 °C groups (Figure 4). The cytochrome c assay revealed a slightly greater normalized cytochrome c release in the 22 °C group in comparison to the 4 °C group, but this was not significant (p = 0.3293). Likewise, the MDA levels were marginally higher in the 22 °C group, but this was also not significant (p = 0.6974).
3.4. Injury Markers Analysis Results
Kidney injury biomarker analysis in plasma samples at hour 4 of reperfusion showed that most measured markers did not differ significantly between kidneys preserved at 4 °C and 22 °C (Figure 5, Figure 6 and Figure 7). Alpha-1-microglobulin (p = 0.2186), beta-2-microglobulin (p = 0.3582), cystatin C (p = 0.9723), osteoactivin (p = 0.2813), NGAL (p = 0.7134), KIM-1 (p = 0.1893), osteopontin (p = 0.3026), renin (p = 0.3209), and TFF3 (p = 0.8129) were comparable between groups. However, several biomarkers were elevated in the 22 °C group. Calbindin was significantly higher after preservation at 22 °C than at 4 °C (p = 0.0173), as were GSTA1 (p = 0.0304) and MCP-1/CCL2 (p = 0.0159). In contrast, EGF was significantly lower in the 22 °C group compared with the 4 °C group (p = 0.0187). IP-10/CXCL10 (p = 0.0508), RBP4 (p = 0.0626), and VEGF-A (p = 0.0637) showed borderline increases in the 22 °C group but did not reach statistical significance. Uromodulin, TIMP-1, clusterin, and IL-18 were excluded from analysis because their concentrations were beyond the detection limit of the assay platform.
The heatmap indicates the relative biomarker profile of kidneys stored at 22 °C when compared with the 4 °C reference group. Overall, the 22 °C group exhibited a mixed injury-marker pattern, with several markers increased and a smaller number decreased, when compared with 4 °C (Figure 8).
4. Discussion
Recent clinical evidence has reinforced the importance of oxygen delivery during kidney machine perfusion. In this context, Jochmans et al. evaluated the potential additive benefit of oxygenated hypothermic machine perfusion (HMPO₂) over standard HMP in a randomized, double-blind, paired phase 3 clinical trial [18]. Oxygenated perfusion did not have a significant effect on the estimated glomerular filtration rate, but there was a trend favoring HMPO₂ group. Oxygenated perfusion, however, was associated with fewer severe postoperative complications, as well as a lower graft failure rate when compared with standard HMP. These results suggest that oxygenation during hypothermic preservation may enhance graft resilience and decrease clinically relevant adverse outcomes. However, one important mechanistic and translational question that this clinical trial raises is if the benefit of oxygenation is only realized under hypothermic conditions, or if this can also be translated to preservation at warmer temperatures where metabolic demand is much higher. At higher temperatures, oxygen delivery is more important, as the kidney is less metabolically suppressed. In these conditions, merely supplementing oxygen to an acellular crystalloid solution may not be sufficient to supply enough oxygen-carrying capacity to meet tissue demands. Recent preclinical data had raised the possibility that subnormothermic oxygenated preservation may not need blood or dedicated oxygen carriers to be successful [8,14]. This formed the rational that a simple, widely available subnormothermic preservation approach might be clinically feasible. However, whether this concept would remain effective in a paired human discarded kidney model had not been examined. We directly tested this question here and found that oxygenated UW solution alone at 22 °C did not compare favorably with HMP at 4 °C.
Our experiments showed that vascular resistance was significantly lower throughout the 12-hour preservation in the 22 °C perfused kidneys when compared with 4 °C perfused kidneys. This is probably due to the ability of subnormothermic conditions to minimize cold-induced vasoconstriction. At hypothermic conditions, the renal vasculature becomes more prone to constriction [19,20], membrane rigidity [21], and impair nitric oxide signaling [22], all of which can increase flow resistance. In contrast, preservation at 22 °C may help maintain a more compliant microvascular bed, allowing easier perfusate passage through the kidney during storage. However, despite this vascular advantage, the improvement in resistance did not translate into superior overall graft protection. Creatinine clearance did not differ between groups at any time point during reperfusion and plasma BUN was significantly lower in 4 °C kidneys at hour 1 and 2. Likewise, plasma sodium, chloride, and tissue oxygenation were comparable between groups. Total urine production was higher in the 4 °C group, with a borderline difference that did not reach statistical significance (p = 0.0506). These results suggest that improved perfusion alone was not sufficient to enhance early graft performance under these conditions.
Histological analysis corroborated this notion, as kidneys preserved at 22 °C had more severe tubular injury on H&E staining and significantly higher ATN scores than kidneys preserved at 4 °C. TUNEL staining revealed a small increase in apoptotic cell death in the 22 °C group, but the difference in TUNEL-positive area was not statistically significant. Likewise, levels of urinary cytochrome c release and tissue MDA did not differ significantly between groups. Therefore, preservation at 22 °C with oxygenated UW solution alone may not have produced a measurable decrease in mitochondrial injury or lipid peroxidation compared with 4 °C. The injury biomarker profile further supports the conclusion that preservation at 22 °C with oxygenated UW solution did not afford superior protection in this model. Although levels of most measured biomarkers were similar between groups, several tubular injury and inflammatory activation biomarkers were increased after preservation at 22 °C. In particular, the injury biomarkers calbindin, GSTA1 and MCP-1/CCL2 were significantly elevated in the 22 °C group. Furthermore, EGF levels were significantly lower in the 22 °C group compared with 4 °C group. Calbindin is a vitamin D–dependent calcium-binding protein and is primarily expressed in the distal tubules and cortical collecting ducts. Urinary calbindin has been shown to be elevated in response to distal tubular injury, such as in patients who have received cisplatin chemotherapy [23]. GSTA1 is a proximal tubular injury biomarker, and its increased excretion has been reported as an indicator of renal tubular damage [24]. MCP-1/CCL2 is a marker of renal inflammatory injury, and higher urinary MCP-1 levels have been linked to greater interstitial fibrosis and tubular atrophy [25]. EGF has been implicated in animal studies as a key factor for the normal function of the glomeruli, and for both the proximal and distal convoluted tubules. It has also been shown as a potentially useful marker of cellular proliferation and tissue repair after ischemic injury. Furthermore, lower levels of EGF have been linked to a greater loss of kidney function [26]. Together, these findings indicate that while oxygenated UW perfusion at 22 °C improved vascular resistance during preservation, this benefit alone was insufficient to improve early reperfusion function or reduce structural, oxidative, mitochondrial, and biomarker evidence of renal injury compared with conventional 4 °C HMP.
This study is associated with several limitations. First, the small number of paired human discarded kidneys was a limiting factor in our ability to detect more subtle differences between groups. Second, we employed an ex vivo reperfusion model as opposed to actual transplantation; therefore, longer-term outcomes like DGF, immunological responses, and post-transplant survival were not addressed. Third, only one subnormothermic temperature was assessed (22 °C), and thus this study cannot inform whether or not a lower intermediate temperature may strike a better balance between metabolic suppression and cellular support by active oxygenation. Finally, while the paired design minimized inter-donor variability, there was substantial variability between donor pairs, including in cold ischemia time, DCD status, donor age, comorbidities, and baseline graft quality. This may have contributed to the relatively large standard deviations in several of the outcome measures.
Based on the findings of the present study, future subnormothermic or near-normothermic perfusion strategies should continue to incorporate an oxygen carrier to ensure adequate oxygen delivery during preservation. In addition, future work should explore lower temperature oxygenated UW perfusion strategies, especially those in the intermediate range between conventional hypothermia and 22 °C (10–15 °C), where metabolic demand may not be as fully suppressed but may still benefit from active oxygenation to some degree. Other treatment modalities, including gradual temperature rewarming [27] , small endogenous molecules supplementation [28,29], mitochondrial protective agents [30], stem cell-based therapies [31], anti-inflammatory additives [32], and targeted therapeutic delivery should also be evaluated [33].
5. Conclusions
In summary, subnormothermic oxygenated UW machine perfusion at 22 °C provided no demonstrable benefit over conventional HMP at 4 °C in this paired, human discarded kidney experimental model. Lower vascular resistance with 22 °C storage did not lead to improved renal function or tissue protection after reperfusion. Kidneys stored at 22 °C exhibited evidence of increased tubular injury on histology, and an adverse biomarker signature with higher calbindin, GSTA1, and MCP-1/CCL2 and lower EGF. Overall, conventional HMP was at least as effective, and with the conditions used in the present study, more protective than subnormothermic oxygenated perfusion at 22 °C.
Acknowledgments
This study was supported by PSI ( Grant #23-25) and AMOSO (AMOSO INN24-015) foundations.
Conflicts of Interest
None.
Disclosure
ChatGPT-5 (OpenAI, San Francisco, CA, USA) was used to improve the English language and readability of the manuscript.
Authors’ contribution
Saeed Farzamfar: conceptualization, methodology, project administration, writing—original draft, writing—review and editing, data analysis, and visualization. Talal Shamma: methodology and data analysis. Tamara S. Ortas: methodology and data analysis. Larry Jiang: methodology. John Mianzhong Wang: methodology. Mahmoud Richard-Mohamed: methodology. Arian Saeidi: methodology. Aaron Haig: data analysis. Aushanth Ruthirakanthan: methodology. Martin Igbokwe: methodology. Ali Bozaci: methodology. Alp Sener: conceptualization, funding acquisition, and supervision. Patrick P. Luke: conceptualization, supervision, funding acquisition, data analysis, and writing—review and editing.
References
- Tonelli, M.; Wiebe, N.; Knoll, G.; et al. Systematic review: kidney transplantation compared with dialysis in clinically relevant outcomes. Am. J. Transplant. 2011, 11(10), 2093–2109. [Google Scholar] [CrossRef] [PubMed]
- Shi, B.; Ying, T.; Chadban, S.J. Survival after kidney transplantation compared with ongoing dialysis for people over 70 years of age: a matched-pair analysis. Am. J. Transplant. 2023, 23(10), 1551–1560. [Google Scholar] [CrossRef] [PubMed]
- Zhao, H.; Alam, A.; Soo, A.P.; et al. Ischemia-reperfusion injury reduces long term renal graft survival: mechanism and beyond. EBioMedicine 2018, 28, 31–42. [Google Scholar] [CrossRef] [PubMed]
- Hosgood, S.A.; Brown, R.J.; Nicholson, M.L. Advances in kidney preservation techniques and their application in clinical practice. Transplantation 2021, 105(11), e202–e214. [Google Scholar] [CrossRef] [PubMed]
- Khan, S.; Zuluaga, D.; Ratner, L.E.; et al. Emerging Therapeutic Strategies for Renal Ischemia-Reperfusion Injury in Kidney Transplantation: Progress and Challenges—A Systematic Review. Clin. Transplant. 2025, 39(8), e70263. [Google Scholar] [PubMed]
- Jing, L.; Yao, L.; Zhao, M.; et al. Organ preservation: from the past to the future. Acta Pharmacol. Sin. 2018, 39(5), 845–857. [Google Scholar] [CrossRef] [PubMed]
- Kawamura, M.; Parmentier, C.; Ray, S.; et al. Normothermic ex vivo kidney perfusion preserves mitochondrial and graft function after warm ischemia and is further enhanced by AP39. Nat. Commun. 2024, 15(1), 8086. [Google Scholar] [CrossRef] [PubMed]
- Abraham, N.; Gao, Q.; Kahan, R.; et al. Subnormothermic oxygenated machine perfusion (24 h) in DCD kidney transplantation. Transplant. Direct 2024, 10(6), e1633. [Google Scholar] [CrossRef] [PubMed]
- Deffrennes, S.; MacMillan, S.; Paterson, A.; et al. Subnormothermic acellular machine perfusion for prolonged preservation of human kidneys. Br. J. Surg. 2025, 112(7), znaf147. [Google Scholar] [CrossRef] [PubMed]
- Bhattacharjee, R.N.; Ruthirakanthan, A.; Sun, Q.; et al. Subnormothermic oxygenated perfusion optimally preserves donor kidneys ex vivo. Kidney Int. Rep. 2019, 4(9), 1323–1333. [Google Scholar] [CrossRef] [PubMed]
- Nouh, T.; Shalhoub, M.; Alburakan, A.; et al. Barriers and challenges to implementing whole blood transfusion protocols in civilian hospitals: A systematic review and meta-analysis. J. Clin. Med. 2024, 13(16), 4726. [Google Scholar] [CrossRef] [PubMed]
- Luke, P.P.; Jiang, L.; Ruthirakanthan, A.; et al. Comparison of centrifugal and pulsatile perfusion to preserve donor kidneys using ex vivo subnormothermic perfusion. J. Investig. Surg. 2022, 35(1), 104–110. [Google Scholar]
- Bhattacharjee, R.N.; Patel, S.V.; Sun, Q.; et al. Renal protection against ischemia reperfusion injury: hemoglobin-based oxygen carrier-201 versus blood as an oxygen carrier in ex vivo subnormothermic machine perfusion. Transplantation 2020, 104(3), 482–489. [Google Scholar] [CrossRef] [PubMed]
- Agius, T.; Songeon, J.; Klauser, A.; et al. Subnormothermic ex vivo porcine kidney perfusion improves energy metabolism: analysis using 31P magnetic resonance spectroscopic imaging. Transplant. Direct 2022, 8(10), e1354. [Google Scholar] [CrossRef] [PubMed]
- Bhattacharjee, R.N.; Richard-Mohamed, M.; Sun, Q.; et al. CORM-401 reduces ischemia reperfusion injury in an ex vivo renal porcine model of the donation after circulatory death. Transplantation 2018, 102(7), 1066–1074. [Google Scholar] [CrossRef] [PubMed]
- Small, D.M.; Gobe, G.C. Cytochrome c: potential as a noninvasive biomarker of drug-induced acute kidney injury. Expert Opin. Drug Metab. Toxicol. 2012, 8(6), 655–664. [Google Scholar] [CrossRef] [PubMed]
- Khoubnasabjafari, M.; Ansarin, K.; Jouyban, A. Reliability of malondialdehyde as a biomarker of oxidative stress in psychological disorders. BioImpacts BI 2015, 5(3), 123. [Google Scholar] [CrossRef] [PubMed]
- Jochmans, I.; Brat, A.; Davies, L.; et al. Oxygenated versus standard cold perfusion preservation in kidney transplantation (COMPARE): a randomised, double-blind, paired, phase 3 trial. The Lancet 2020, 396(10263), 1653–1662. [Google Scholar] [CrossRef]
- De Rosa, S.; Antonelli, M.; Ronco, C. Hypothermia and kidney: a focus on ischaemia–reperfusion injury. Nephrol. Dial. Transplant. 2017, 32(2), 241–247. [Google Scholar] [PubMed]
- Eisenberger, F.; Chaussy, C.; Pfeifer, K.; et al. Changes in blood flow and vasculature of the dog kidney undergoing normothermic and hypothermic ischaemia. Urol. Res. 1977, 5(1), 7–13. [Google Scholar] [CrossRef] [PubMed]
- Reid, T.; Esteban, G.; Clear, M.; et al. Platelet membrane integrity during storage and activation. Transfusion 1999, 39(6), 616–624. [Google Scholar] [CrossRef] [PubMed]
- Kawasaki, N.; Ueyama, K.; Sumii, T.; et al. Effects of cold exposure and shear stress on endothelial nitric oxide synthase activation. Biochem. Biophys. Res. Commun. 2011, 412(2), 318–322. [Google Scholar] [CrossRef]
- Guha, M.; Heier, A.; Price, S.; et al. Assessment of biomarkers of drug-induced kidney injury in cynomolgus monkeys treated with a triple reuptake inhibitor. Toxicol. Sci. 2011, 120(2), 269–283. [Google Scholar] [CrossRef] [PubMed]
- Brüning, T.; Sundberg, A.G.; Birner, G.; et al. Glutathione transferase alpha as a marker for tubular damage after trichloroethylene exposure. Arch. Toxicol. 1999, 73(4), 246–254. [Google Scholar] [CrossRef] [PubMed]
- Menez, S.; Ju, W.; Menon, R.; et al. Urinary EGF and MCP-1 and risk of CKD after cardiac surgery. Jci Insight 2021, 6(11), e147464. [Google Scholar] [CrossRef] [PubMed]
- Postalcioglu, M.; Katz, R.; Ascher, S.B.; et al. Associations of urine epidermal growth factor with kidney and cardiovascular outcomes in individuals with CKD in SPRINT. Kidney Int. Rep. 2024, 9(11), 3167–3176. [Google Scholar] [CrossRef] [PubMed]
- Schopp, I.; Reissberg, E.; Lüer, B.; et al. Controlled rewarming after hypothermia: adding a new principle to renal preservation. Clin. Transl. Sci. 2015, 8(5), 475–478. [Google Scholar] [CrossRef] [PubMed]
- Caumartin, Y.; Stephen, J.; Deng, J.P.; et al. Carbon monoxide-releasing molecules protect against ischemia–reperfusion injury during kidney transplantation. Kidney Int. 2011, 79(10), 1080–1089. [Google Scholar] [CrossRef] [PubMed]
- Dugbartey, G.J.; Juriasingani, S.; Richard-Mohamed, M.; et al. Static cold storage with mitochondria-targeted hydrogen sulfide donor improves renal graft function in an ex vivo porcine model of controlled donation-after-cardiac-death kidney transplantation. Int. J. Mol. Sci. 2023, 24(18), 14017. [Google Scholar] [PubMed]
- Mitchell, T.; Rotaru, D.; Saba, H.; et al. The mitochondria-targeted antioxidant mitoquinone protects against cold storage injury of renal tubular cells and rat kidneys. J. Pharmacol. Exp. Ther. 2011, 336(3), 682–692. [Google Scholar] [CrossRef] [PubMed]
- Hu, H.; Zou, C. Mesenchymal stem cells in renal ischemia-reperfusion injury: biological and therapeutic perspectives. Curr. Stem Cell Res. Ther. 2017, 12(3), 183–187. [Google Scholar] [CrossRef] [PubMed]
- Zhang, J.; Tang, L.; Li, G.S.; et al. The anti-inflammatory effects of curcumin on renal ischemia-reperfusion injury in rats. Ren. Fail. 2018, 40(1), 680–686. [Google Scholar] [PubMed]
- Li, X.; Cantley, L.G.; Xu, L. Engineering polyamidoamine dendrimer nanoparticles for targeted drug delivery to proximal tubular cells after renal ischemia/reperfusion injury. J. Control. Release 2025, 114323. [Google Scholar] [CrossRef] [PubMed]
Figure 1.
Hemodynamic and functional parameters of machine-preserved kidneys at 4 °C and 22 °C during ex vivo perfusion and reperfusion. Panel A: Vascular resistance during the 12-hour preservation period. Panel B: Renal blood flow (ml/min) during 4-hour reperfusion. Panel C: Creatinine clearance at hourly intervals during reperfusion. Panel D: Plasma BUN concentration during the 4-hour reperfusion period. Data are presented as mean ± SD (n = 5 per group). *p < 0.05 and **p < 0.01.
Figure 1.
Hemodynamic and functional parameters of machine-preserved kidneys at 4 °C and 22 °C during ex vivo perfusion and reperfusion. Panel A: Vascular resistance during the 12-hour preservation period. Panel B: Renal blood flow (ml/min) during 4-hour reperfusion. Panel C: Creatinine clearance at hourly intervals during reperfusion. Panel D: Plasma BUN concentration during the 4-hour reperfusion period. Data are presented as mean ± SD (n = 5 per group). *p < 0.05 and **p < 0.01.

Figure 2.
Electrolytes, tissue oxygenation, and urine output during reperfusion following storage at 4 °C and 22 °C. Plasma chloride (Cl⁻, mmol/L) (A), plasma sodium (Na⁺, mmol/L) (B), and tissue oxygenation (%) (C) were monitored over the course of the 4-hour reperfusion period (0–4 h). Total urine output (mL) during the reperfusion period is shown in (D). Data are shown as mean ± SD (n = 5 per group). P-value is shown in panel D on the graph.
Figure 2.
Electrolytes, tissue oxygenation, and urine output during reperfusion following storage at 4 °C and 22 °C. Plasma chloride (Cl⁻, mmol/L) (A), plasma sodium (Na⁺, mmol/L) (B), and tissue oxygenation (%) (C) were monitored over the course of the 4-hour reperfusion period (0–4 h). Total urine output (mL) during the reperfusion period is shown in (D). Data are shown as mean ± SD (n = 5 per group). P-value is shown in panel D on the graph.

Figure 3.
Histological evaluation of kidney tissues preserved at 4 °C and 22 °C. Representative images of H&E, TUNEL, and MSB staining are shown for both groups. Arrows indicate representative areas of tubular injury and luminal necrotic debris. Quantification of ATN score and TUNEL-positive area (%) is presented on the right.
Figure 3.
Histological evaluation of kidney tissues preserved at 4 °C and 22 °C. Representative images of H&E, TUNEL, and MSB staining are shown for both groups. Arrows indicate representative areas of tubular injury and luminal necrotic debris. Quantification of ATN score and TUNEL-positive area (%) is presented on the right.

Figure 4.
Urinary cytochrome c and tissue MDA levels in kidneys preserved at 4 °C and 22 °C. (A) Urinary cytochrome c concentration measured at hour 4 of reperfusion and normalized to total protein content. (B) MDA levels in kidney tissue lysates, measured as an indicator of lipid peroxidation and normalized to total protein content. Data are presented as mean ± SD (n = 5 per group). P-values are shown on the graphs.
Figure 4.
Urinary cytochrome c and tissue MDA levels in kidneys preserved at 4 °C and 22 °C. (A) Urinary cytochrome c concentration measured at hour 4 of reperfusion and normalized to total protein content. (B) MDA levels in kidney tissue lysates, measured as an indicator of lipid peroxidation and normalized to total protein content. Data are presented as mean ± SD (n = 5 per group). P-values are shown on the graphs.

Figure 5.
Plasma kidney injury biomarkers at hour 4 of reperfusion in kidneys preserved at 4 °C and 22 °C. Plasma concentrations of alpha-1-microglobulin, beta-2-microglobulin, cystatin C, calbindin, GSTA1, and EGF were measured at hour 4 of reperfusion and normalized to total protein content. Data are presented as mean ± SD. P-values are shown on the graphs.
Figure 5.
Plasma kidney injury biomarkers at hour 4 of reperfusion in kidneys preserved at 4 °C and 22 °C. Plasma concentrations of alpha-1-microglobulin, beta-2-microglobulin, cystatin C, calbindin, GSTA1, and EGF were measured at hour 4 of reperfusion and normalized to total protein content. Data are presented as mean ± SD. P-values are shown on the graphs.

Figure 6.
Plasma kidney injury biomarkers at hour 4 of reperfusion in kidneys preserved at 4 °C and 22 °C. Plasma concentrations of GSTA1, osteoactivin, NGAL, IP-10/CXCL10, KIM-1, and MCP-1/CCL2 were measured at hour 4 of reperfusion and normalized to total protein content. Data are presented as mean ± SD. P-values are shown on the graphs.
Figure 6.
Plasma kidney injury biomarkers at hour 4 of reperfusion in kidneys preserved at 4 °C and 22 °C. Plasma concentrations of GSTA1, osteoactivin, NGAL, IP-10/CXCL10, KIM-1, and MCP-1/CCL2 were measured at hour 4 of reperfusion and normalized to total protein content. Data are presented as mean ± SD. P-values are shown on the graphs.

Figure 7.
Plasma kidney injury biomarkers at hour 4 of reperfusion in kidneys preserved at 4 °C and 22 °C. Plasma concentrations of osteopontin, RBP4, renin, VEGF-A, and TFF3 were measured at hour 4 of reperfusion and normalized to total protein content. Data are presented as mean ± SD. P-values are shown on the graphs.
Figure 7.
Plasma kidney injury biomarkers at hour 4 of reperfusion in kidneys preserved at 4 °C and 22 °C. Plasma concentrations of osteopontin, RBP4, renin, VEGF-A, and TFF3 were measured at hour 4 of reperfusion and normalized to total protein content. Data are presented as mean ± SD. P-values are shown on the graphs.

Figure 8.
Heatmap of relative kidney injury biomarker levels after reperfusion in human discarded kidneys preserved at 4 °C and 22 °C. Biomarker values were normalized to total protein content and expressed relative to the corresponding values in the 4 °C group.
Figure 8.
Heatmap of relative kidney injury biomarker levels after reperfusion in human discarded kidneys preserved at 4 °C and 22 °C. Biomarker values were normalized to total protein content and expressed relative to the corresponding values in the 4 °C group.


Table 1.
Donor demographics and clinical characteristics.
| Donor pair | Donor profile | Ischemia details | Key clinical background and risk factors |
|---|---|---|---|
| Pair 1 | 68-year-old female; blood type A; BMI 28.1 kg/m²; KDPI 99%; White, not Hispanic/Latino; DCD; anoxia/natural death. | Warm ischemic time: 53 min; cold ischemic time: 28 h | Hypertension (6–10 years; treated/compliant); >20 pack-year smoker. |
| Pair 2 | 74-year-old female; blood type A1; BMI 30.9 kg/m²; KDPI 97%; White, ethnicity not reported; DCD; cerebrovascular/stroke, intracranial hemorrhage/natural death. | Warm ischemic time: 21 min; cold ischemic time: 34 h | Hypertension (0–5 years; treated/compliant); family history of heart disease. |
| Pair 3 | 67-year-old male; blood type A; BMI 32.4 kg/m²; KDPI 85%; White, not Hispanic/Latino; non-DCD; anoxia/cardiovascular mechanism/natural death. | Warm ischemic time: not applicable/reported; cold ischemic time: 37 h | Type 2 diabetes (6–10 years); coronary artery disease. Former smoker (~1 pack/day for 20–25 years). |
| Pair 4 | 73-year-old male; BMI 23.3 kg/m²; KDPI 98%; White, not Hispanic/Latino; non-DCD; anoxia/cardiovascular mechanism/natural death. | Warm ischemic time: not applicable/reported; cold ischemic time: 29 h | Diabetes (6–10 years); hypertension >10 years; former smoker >20 pack-years; heavy alcohol history; daily marijuana use >10 years. |
| Pair 5 | 46-year-old female; BMI 18.0 kg/m²; KDPI 72%; White, not Hispanic/Latino, other origin; non-DCD; cerebrovascular/stroke, intracranial hemorrhage/natural death. | Cold ischemic time: 40 h; warm ischemic time: not applicable/reported; cardiac. | Hypertension of unknown duration. Heavy alcohol use reported. |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2026 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



