Submitted:
04 June 2026
Posted:
05 June 2026
You are already at the latest version
Abstract
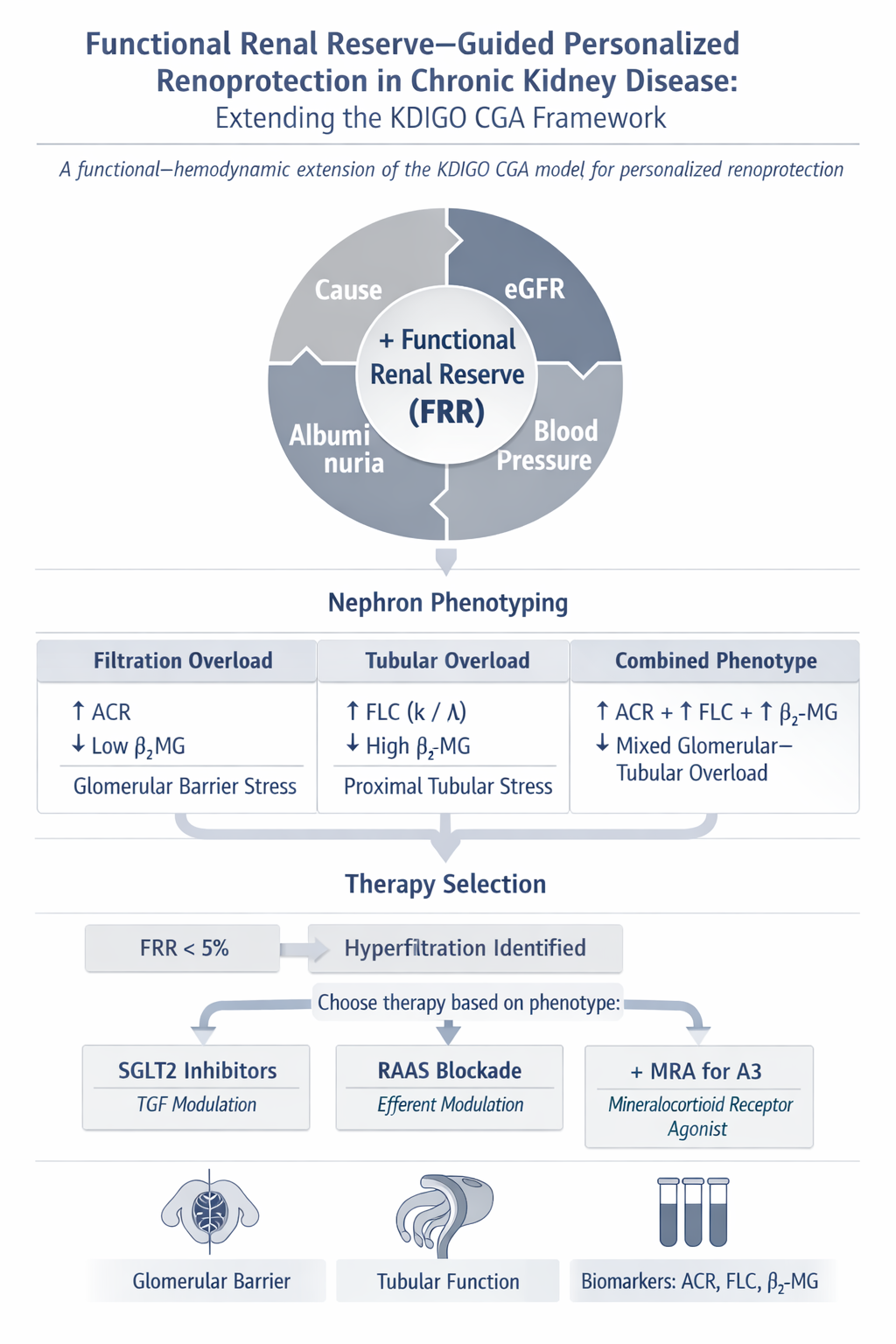
The Kidney Disease: Improving Global Outcomes (KDIGO) classification of chronic kidney disease (CKD) is based on the cause of disease, the category of estimated glomerular filtration rate (eGFR), and the category of albuminuria. This framework is indispensable for risk stratification, yet it does not always identify the functional and hemodynamic mechanism that maintains the current filtration level and drives future progression. In particular, a normal or only moderately reduced eGFR does not exclude relative hyperfiltration of the remaining nephrons, and albuminuria reflects not only glomerular barrier injury but also the limited capacity of the proximal tubule to endocytose and metabolically process filtered proteins. In this conceptual review, we propose a functional-hemodynamic extension of the KDIGO CGA model: Cause + GFR + Albuminuria + Functional Renal Reserve + Blood Pressure. Within this framework, functional renal reserve (FRR) is considered a dynamic stress test of nephron reactivity, whereas blood pressure acts as an essential hemodynamic and therapeutic modifier that influences the safety, sequencing, and intensity of renoprotection. Detailed antihypertensive treatment is beyond the scope of this article; the KDIGO 2021 recommendation of a target systolic blood pressure below 120 mmHg in adults with CKD and elevated blood pressure, when tolerated and measured in a standardized manner, is used as a clinical reference point. A central element of the proposed algorithm is FRR. A zero or negative FRR under standardized testing may indicate an "actionable hyperfiltration phenotype": a clinically meaningful state in which total eGFR does not reflect the true workload imposed on individual nephrons. Depending on the combination of urinary albumin-to-creatinine ratio, eGFR, FRR, blood pressure, metabolic phenotype, and tubular overload markers, the proposed approach may support RAAS-blockade-first, SGLT2-inhibitor-first, early dual therapy, or staged triple renoprotection. A mechanistic distinction is also emphasized. Sodium-glucose cotransporter 2 inhibitors (SGLT2i) directly inhibit proximal tubular sodium and glucose reabsorption, but their key anti-hyperfiltration effect is mediated by increased sodium delivery to the macula densa, restoration of tubuloglomerular feedback, and increased afferent arteriolar tone. By contrast, renin-angiotensin-aldosterone system inhibitors (RAASi) predominantly modulate the efferent/postglomerular compartment and may improve downstream peritubular perfusion, a mechanism potentially relevant to albumin and protein handling by the proximal tubule. The proposed model does not replace KDIGO; rather, it adds physiological phenotyping to the existing risk map. More precise evaluation of proteinuria, including the albumin-to-total-protein ratio, first-morning urine sampling, low-molecular-weight proteins, and tubular markers, may prevent misclassification of physiological, orthostatic, postglomerular, or tubular proteinuria as progressive glomerular CKD. The model requires prospective validation but may help develop practical algorithms for personalized renoprotection, particularly in patients with low or moderate albuminuria, normal or moderately reduced eGFR, diabetes, obesity, hypertension, solitary kidney, reduced nephron mass, or an uncertain progression trajectory.
Keywords:
chronic kidney disease
; functional renal reserve
; hyperfiltration
; albuminuria
; eGFR
; SGLT2 inhibitors
; RAAS blockade
; finerenone
; mineralocorticoid receptor antagonists
; precision nephrology
; tubuloglomerular feedback
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



