Submitted:
01 June 2026
Posted:
02 June 2026
You are already at the latest version
Abstract
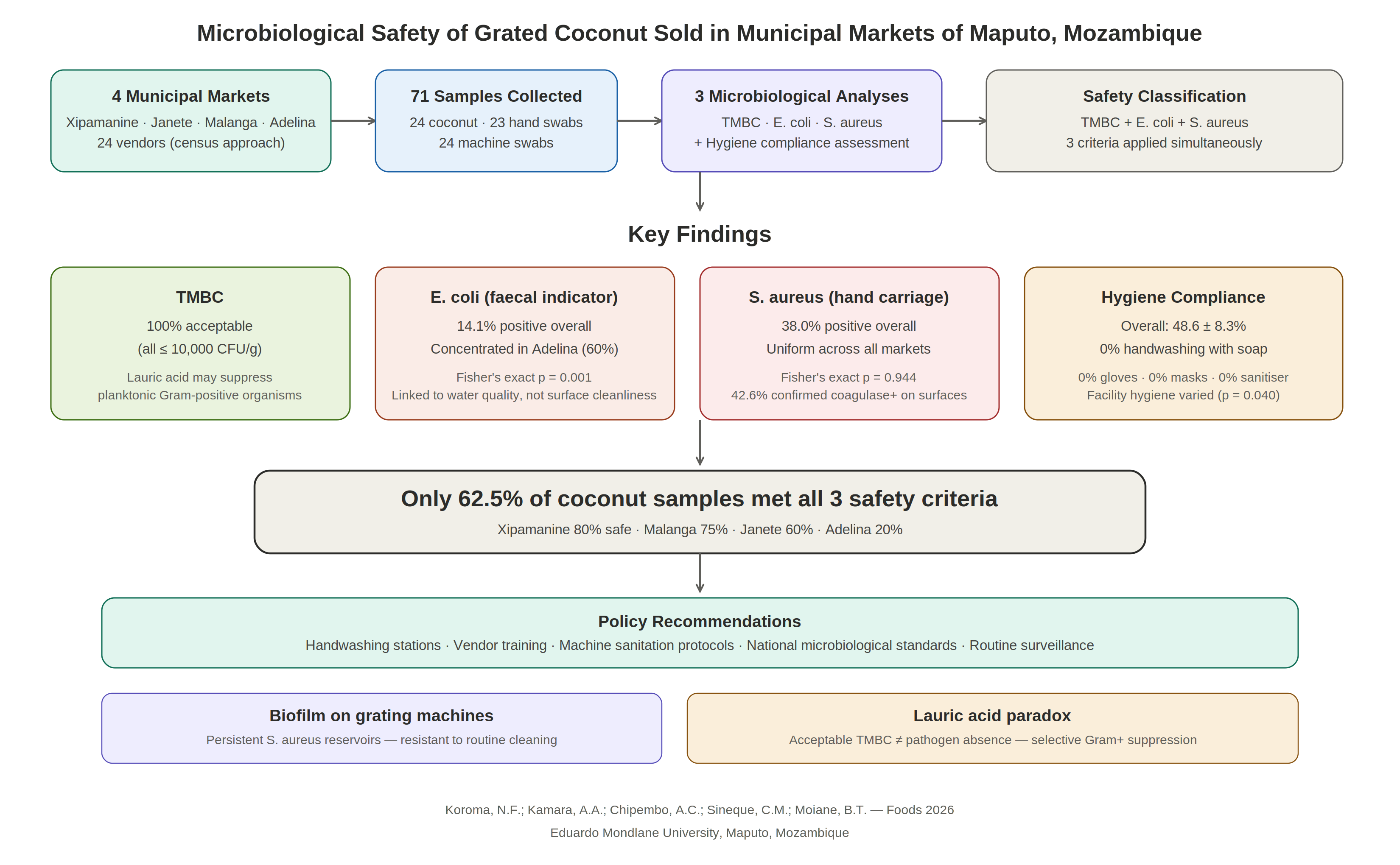
This cross-sectional study assessed the microbiological safety of grated coconut sold in four municipal markets (Xipamanine, Janete, Malanga, and Adelina) in Maputo City. A total of 71 samples, comprising 24 grated coconut samples, 23 vendor hand swabs, and 24 grating machine swabs, were collected from 24 vendors. Hygiene conditions were evalu-ated using structured observational checklists covering 13 personal and 22 facility hygiene items. Laboratory analyses targeted total mesophilic bacteria count (TMBC), Escherichia coli, and Staphylococcus aureus. Statistical comparisons employed Kruskal–Wallis and Fisher’s exact tests. The overall hygiene compliance score was 48.6 ± 8.3%, with facility hygiene scores differing significantly across markets (p = 0.040). All 24 coconut samples exhibited acceptable TMBC (≤ 10,000 CFU/g). Presumptive E. coli was detected in 14.1% of samples, with significant inter-market variation (Fisher’s exact p = 0.001), primarily concentrated in Adelina Market. S. aureus was detected in 38.0% of all samples, with coagulase-positive isolates confirmed on 42.6% of contaminated surfaces. When three safety criteria were ap-plied simultaneously, only 62.5% of coconut samples qualified as “Overall Safe.” These findings indicate that grated coconut sold in Maputo markets carries microbiological safe-ty risks primarily attributable to widespread S. aureus contamination and localized fecal contamination. This underscores the need for improved hygiene infrastructure, vendor training, machine sanitation, and the development of national microbiological standards for minimally processed coconut products.
Keywords:
grated coconut
; microbiological safety
; Staphylococcus aureus
; Escherichia coli
; food hygiene
; informal markets
; Maputo
; Mozambique
1. Introduction
Coconut (Cocos nucifera L.) is a vital perennial tree crop widely cultivated in tropical and subtropical regions, supporting the livelihoods of millions of smallholder farmers in over 90 countries globally [1]. The crop ranks among the most economically important palm species, serving as a source of food, fiber, fuel, and industrial raw materials [2]. Mozambique occupies a prominent position among Africa’s leading coconut producers [3]. Within these communities, coconut plays a dual commercial and subsistence function, underpinning both household food security and small-scale enterprise [4]. In Mozambican cuisine, grated coconut is an indispensable ingredient in traditional preparations such as matapa, caril, and xima-based sauces. It is also routinely purchased as a minimally processed, ready-to-use product from municipal markets.
Grated coconut is produced by mechanically shredding the mature kernel of fresh coconuts at the point of sale, typically using manual or electric graters, and is subsequently packed in plastic bags for household consumption. The product’s intrinsic characteristics, a water activity exceeding 0.9, elevated protein and fat content, and substantially increased surface area following grating, collectively create a moist, nutrient-rich microenvironment that is highly conducive to rapid microbial proliferation, particularly under the ambient tropical temperatures prevalent in Maputo [5], [6], [7], [8]. Among the organisms of greatest concern are mesophilic bacteria, serving as general indicators of hygienic quality, and specific pathogens such as Escherichia coli (indicative of fecal contamination) and Staphylococcus aureus (associated with skin and nasal carriage by food handlers)[9], [10]. These organisms can be introduced through multiple routes, including unsanitary grating equipment, contaminated water used for rinsing, bare-hand contact during packaging, and exposure to airborne particles and insects at open-air vending sites [11], [12], [13], [14], [15].
Food safety constitutes a persistent and escalating public health concern across sub-Saharan Africa, where the World Health Organization (WHO) estimates that foodborne diseases account for approximately 91 million illness episodes and 137,000 deaths annually in Africa, representing the highest regional burden worldwide [16], [17]. On a global scale, contaminated food causes an estimated 600 million cases of illness each year, with children under five years of age bearing a disproportionate share of the morbidity and mortality [18]. In Mozambique, the magnitude of this burden is substantial: over 500,000 episodes of diarrhoeal disease attributable to foodborne pathogens were recorded in Mozambique in 2018 [19]. Previous investigations conducted in Maputo’s informal food sector have documented alarmingly high rates of microbial contamination; one study found that 75% of cold foods sold by street vendors were contaminated above acceptable limits [20]. These studies have consistently attributed contamination to poor vendor hygiene practices and inadequate water quality [21].
Coconut products have been implicated in foodborne disease outbreaks in various international settings. A multistate outbreak of Salmonella Chailey in the United States was traced to pre-cut coconut pieces [22], while S. aureus was recovered from 58% of coconut slice samples examined in an Indian market survey [23]. In Brazil, E. coli was isolated from the majority of shredded coconut samples collected from open-air markets in the municipality of Belém [24]. More recently, a systematic review of street food safety in developing countries noted that street foods are frequently implicated in outbreaks of gastrointestinal diseases [21]. Despite this accumulating international evidence, specific data on the microbiological quality of fresh grated coconut in Maputo remains conspicuously absent from the literature.
This study was therefore undertaken to address this critical knowledge gap. The specific objectives were to: (1) evaluate the hygienic conditions under which grated coconut is handled and sold in municipal markets; (2) detect and quantify total mesophilic bacteria, E. coli, and S. aureus in grated coconut samples and on potential contamination surfaces (vendor hands and grating machines); (3) confirm the identity of S. aureus and E. coli isolates from contamination surfaces through sequential biochemical testing; and (4) classify the microbiological contamination levels of grated coconut against applicable international food safety standards, thereby generating baseline data to inform future regulatory development in Mozambique.
2. Materials and Methods
2.1. Study Design and Setting
A cross-sectional analytical study was conducted between January and March 2025 in four municipal markets situated in Maputo City, Mozambique: Xipamanine, Janete, Malanga, and Adelina. These markets were purposively selected based on their high volume of grated coconut trade and their geographic distribution across distinct districts of the city, thereby ensuring broad spatial representation of the urban market landscape. A total of 24 grated coconut vendors were recruited using a complete census approach, enrolling every eligible vendor operating in the selected markets during the study period. The distribution of participants across sites was as follows: 10 vendors from Xipamanine, 5 from Janete, 4 from Malanga, and 5 from Adelina, respectively. Eligibility criteria required that vendors were actively engaged in coconut grating and sale at the time of recruitment and that they provided written informed consent. Vendors who were absent during data collection visits or who declined participation were excluded from the study.
2.2. Hygiene Assessment
To enhance the methodological rigor and transparency of the reporting, the assessment of hygienic conditions at each vending site was conducted through direct structured observation using standardized checklists, with the reporting framework aligned with the STROBE-nut extension [25], [26]. This alignment ensures that all relevant aspects of the observational component are comprehensively detailed, facilitating a standardized approach to reporting nutritional epidemiology and dietary assessment research. Observations were recorded in real time using the Kobo Collect mobile data collection platform, minimizing recall bias and transcription errors.
The assessment instrument comprised two domains: personal hygiene (13 items) and facility hygiene and sanitation (22 items), yielding a total of 35 binary checklist items. The personal hygiene domain covered handwashing practices, nail cleanliness, use of protective equipment (gloves, masks, hairnets, aprons), absence of smoking, chewing gum, sneezing/coughing behavior, and absence of visible illness or skin disease. The facility hygiene domain covered water availability and quality, equipment condition and maintenance, waste and wastewater management, pest control, food storage practices, machine sanitation, and environmental cleanliness. The full list of individual items and their compliance rates is provided in Supplementary Table S1.
The checklist was adapted from instruments previously validated in Mozambican food safety investigations [17] and was piloted with three vendors prior to deployment to ensure clarity and consistency of scoring. Five of the 13 personal hygiene items were negatively worded — that is, a "Yes" response indicated non-compliance (e.g., "Does the vendor have visible cuts or skin disease?", "Does the vendor smoke while handling coconut?"). Similarly, two of the 22 facility hygiene items were negatively worded (e.g., "Are there visible cracks, rust, or food residues on the machine surfaces?"). For all such items, scores were inverted prior to analysis so that a score of 1 consistently represented compliance across the instrument. Each item was scored as compliant (1) or non-compliant (0), with all items equally weighted within their respective domains.
The percentage compliance score for each domain was calculated as:
- Personal Hygiene (%) = (number of compliant personal hygiene items / 13) × 100
- Facility Hygiene (%) = (number of compliant facility hygiene items / 22) × 100
- Overall Hygiene (%) = (Personal Hygiene % + Facility Hygiene %) / 2
The overall hygiene score was thus computed as the arithmetic mean of the two domain percentages, giving equal weight to personal and facility hygiene regardless of the differing number of items in each domain. This approach was adopted to prevent the facility domain (22 items) from dominating the composite score at the expense of critical personal hygiene practices (13 items). Vendors were subsequently classified into three compliance categories: Poor (<40%), Moderate (40–59%), and Good (≥60%).
2.3. Sample Collection
A total of 71 samples were collected across the four markets, comprising 24 grated coconut samples (one per vendor), 23 vendor hand swabs (one vendor was unavailable for hand swab collection), and 24 grating machine surface swabs. Grating machines were specifically targeted as a sampling site because their surfaces , typically composed of perforated metal sheets with irregular edges and crevices — are susceptible to biofilm formation, particularly under the warm, humid conditions of tropical open-air markets [27], [28], [29]. Bacterial biofilms on food-contact surfaces are recognized as persistent reservoirs of pathogens including S. aureus and Enterobacteriaceae, as sessile communities embedded within an extracellular polymeric matrix exhibit markedly greater resistance to routine cleaning and sanitization than their planktonic counterparts [28], [30]. The inclusion of machine swabs alongside hand swabs was therefore intended to distinguish between transient contamination introduced by human handling and persistent contamination harboured on equipment surfaces.
Grated coconut samples were collected aseptically at the point of sale in pre-labelled sterile containers immediately after the vendor completed the grating process. Surface samples were obtained from vendor hands and grating machine surfaces using sterile premoistened cotton swabs, following standardized swabbing protocols that specified a defined contact area (approximately 25 cm²) to ensure consistency across samples. Each swab was placed into a labeled sterile transport tube containing buffered peptone water. All samples were transported to the Laboratory of Food Safety, Faculty of Veterinary Medicine, Eduardo Mondlane University, in insulated cooler boxes maintained at 4–8 °C, and laboratory processing commenced within 4 hours of collection to preserve sample integrity.
2.4. Microbiological Analysis
Sample preparation followed internationally recognised standard microbiological methods. For grated coconut samples, 10 g of product was weighed aseptically and homogenised in 90 mL of sterile buffered peptone water using a stomacher to obtain a primary 1:10 (10⁻¹) dilution, from which serial decimal dilutions (10⁻² and 10⁻³) were prepared. For surface swab samples, each swab head was vortexed vigorously in 10 mL of buffered peptone water for 60 seconds prior to serial dilution.
Total mesophilic bacteria count (TMBC) was determined using the pour-plate technique on Plate Count Agar (PCA), with plates incubated aerobically at 37 °C for 24–48 hours. Colony enumeration was performed using the summation formula of Roberts and Greenwood [31], whereby counts from duplicate plates at two consecutive countable dilutions were summed and divided by the combined dilution volumes. Results were expressed as colony-forming units per gram (CFU/g) for coconut samples or per millilitre (CFU/mL) for swab suspensions.
Presumptive E. coli was detected by streaking appropriately diluted samples onto Eosin Methylene Blue (EMB) agar plates, which were incubated at 37 °C for 24 hours. Colonies displaying the characteristic metallic green sheen indicative of strong lactose fermentation were recorded as presumptive positives. Confirmatory identification was performed through Gram staining (Gram-negative rods) followed by the Kovacs’ indole reagent test, with indole production confirming E. coli identity.
Presumptive S. aureus was isolated on Mannitol Salt Agar (MSA), a selective medium that exploits the organism’s capacity for mannitol fermentation under high salt concentrations. Colonies exhibiting yellow haloes (mannitol fermentation) were subjected to a sequential three-step confirmatory protocol: (i) Gram staining, with Gram-positive cocci arranged in grape-like clusters recorded as positive; (ii) catalase testing using 3% hydrogen peroxide, with effervescence indicating catalase production; and (iii) tube coagulase testing using rabbit plasma, with clot formation within 4–24 hours confirming coagulase-positive S. aureus [32].
2.5. Classification Against Food Safety Standards
In the absence of Mozambican national standards for minimally processed coconut products, grated coconut samples were classified against three internationally recognised safety criteria applied in parallel: (1) TMBC: Acceptable (≤ 10,000 CFU/g), Marginal (10,001–100,000 CFU/g), or Unsatisfactory (>100,000 CFU/g), following general food safety guidelines; (2) E. coli: Satisfactory (≤ 100 CFU/g) or Unsatisfactory (>100 CFU/g), based on EU Commission Regulation (EC) No. 2073/2005 as amended by Regulation (EC) No. 1441/2007 [33]; and (3) S. aureus: Absent or Present, based on the coagulase test result for coconut samples. A sample was classified as “Overall Safe” only if it simultaneously met all three criteria.
2.6. Statistical Analysis
All statistical analyses were performed using Stata version 17 (StataCorp LLC, College Station, TX, USA). Descriptive statistics included arithmetic means, standard deviations, medians, ranges, and frequency distributions. Given the non-normal distribution of microbiological count data and the small sample sizes per market, the Kruskal–Wallis rank-sum test was employed to compare hygiene compliance scores and microbial counts across the four markets. Fisher’s exact test was used to compare the proportions of positive detections of E. coli and S. aureus across markets and sample types, as cell frequencies were frequently below five, rendering the chi-square approximation unreliable. All tests were two-tailed, and statistical significance was set at α = 0.05. Publication-quality figures were generated using RStudio (version 2024.12.1, Posit PBC, Boston, MA, USA) with the ggplot2 package [34], employing a custom MDPI-compatible theme with 300 dpi resolution for all exported graphics.
3. Results
3.1. Socio-Demographic Profile of Vendors
The socio-demographic characteristics of the 24 participating vendors are summarized in Table 1. The vendor population was predominantly female (n = 14, 58.3%), consistent with the gendered pattern of informal food vending observed across sub-Saharan Africa [21]. The largest age group comprised young adults aged 18–25 years (n = 10, 41.7%), followed by those aged 26–35 years (n = 9, 37.5%) and 36–45 years (n = 5, 20.8%). The majority of vendors reported having completed secondary education (n = 15, 62.5%), while approximately one-third had only primary-level education (n = 8, 33.3%) and one vendor (4.2%) had received no formal education. These findings indicate that the vendor population, while relatively young and predominantly female, possessed a basic educational foundation that could serve as a platform for food safety training interventions.
3.2. Hygienic Conditions
Table 2 presents the hygiene compliance scores disaggregated by market and hygiene dimension. The overall mean hygiene compliance across all 24 vendors was 48.6 ± 8.3%, indicating that vendors met fewer than half of the assessed hygiene criteria on average. Personal hygiene scores (47.8 ± 7.1%) and facility hygiene scores (49.4 ± 14.1%) were broadly comparable in magnitude, though the latter exhibited considerably greater intermarket variability. Several critical personal hygiene practices showed absolute non-compliance (0% across all vendors): handwashing with soap, use of hand sanitizer, use of protective gloves, and wearing face masks. The most commonly observed personal hygiene practice was the wearing of clean clothing or an apron (54%). Among facility-level indicators, all vendors served coconut immediately after grating (100% compliance), but only 4.2% had access to adequate water facilities, and no vendor had toilet access within or near the grating premises.
Facility hygiene scores differed significantly across markets (Kruskal–Wallis H = 8.30, df = 3, p = 0.040), whereas personal hygiene scores did not reach statistical significance (H = 3.81, df = 3, p = 0.282). Overall hygiene compliance also varied significantly by market (H = 9.86, df = 3, p = 0.020). Adelina Market recorded the highest overall compliance (56.4 ± 3.7%), while Malanga recorded the lowest (39.3 ± 2.2%), falling at the boundary of the Poor Compliance category. The majority of vendors (n = 16, 66.7%) were classified within the Moderate Compliance category (40–59%), with equal proportions (n = 4, 16.7% each) classified as Poor (<40%) and Good (≥60%).
At the item level, compliance was highly variable within each domain (Supplementary Table S1). Among the 13 personal hygiene items, four practices exhibited complete non-compliance (0%): handwashing with soap and water, use of hand sanitiser, use of protective gloves, and wearing of face masks. These represent the most critical hand hygiene barriers to pathogen control, as they directly facilitate the transfer of S. aureus and enteric organisms from vendor hands to the product. In contrast, certain behaviours achieved near-universal compliance: absence of smoking (100%), absence of gum chewing (100%), absence of handling while ill (100%), and absence of visible cuts or skin disease (95.8%), though these high scores reflect negatively worded items (i.e., vendors were not engaging in the harmful behaviour) rather than active protective practices. Clean clothing or apron use was the most commonly observed active protective behaviour, at 54.2%. Among the 22 facility hygiene items, complete non-compliance (0%) was observed for toilet access near the grating premises, while only 4.2% of vendors had adequate water facilities and 8.3% stored processed water in clean containers. The highest facility compliance was recorded for immediate serving of coconut after grating (100%), grating from shell (100%), use of clean plastics for packaging (95.8%), and machine drying before storage (91.7%).
Figure 1 provides a visual comparison of these compliance patterns. The grouped bar chart reveals that while personal hygiene scores remain uniformly low across all markets (range: 42.3–50.0%), facility hygiene scores exhibit marked heterogeneity, with Adelina’s facility score (63.6%) exceeding Malanga’s (36.4%) by nearly 27.2 percentage points. This inter-market divergence in infrastructure quality drives the significant overall hygiene differences observed, and suggests that targeted interventions, including both structural upgrades to water and sanitation facilities and machine-specific measures to prevent biofilm formation on damaged grating surfaces [35], are likely to yield greater returns than vendor-level behavior change alone.
3.3. Microbial Contamination
3.3.1. Total Mesophilic Bacteria Count
Table 3 presents the descriptive statistics for TMBC across the three sample types. Mesophilic bacteria were recovered from all 71 samples analyzed (100% detection rate). The overall mean count was 2768 ± 1394 CFU, corresponding to a mean log10 value of 3.37 ± 0.29. Grated coconut samples harbored the highest mean bacterial load (3192 ± 1514 CFU/g; mean log10 = 3.44), followed by machine surface swabs (2830 ± 1216 CFU/mL; mean log10 = 3.41) and vendor hand swabs (2262 ± 1331 CFU/mL; mean log10 = 3.25).
Notably, all 24 grated coconut samples fell within the acceptable category (≤ 10,000 CFU/g); no sample exceeded even the marginal threshold — a finding that may partly reflect the intrinsic antimicrobial activity of lauric acid, the predominant medium-chain fatty acid in coconut flesh, which exerts preferential bactericidal effects against Gram-positive organisms [36]. This selective antimicrobial profile implies that acceptable TMBC should not be interpreted as evidence of pathogen absence, a point examined further in the Discussion.
The distribution of log10-transformed TMBC values is presented in Figure 2, presenting box plots with overlaid individual observations for each sample type across the four markets. The figure demonstrates that all data points cluster well below the 10,000 CFU/g threshold (log10 = 4.0, indicated by the red dashed line), confirming the consistency of this finding across the four markets and sample types. Xipamanine hand swabs exhibited the greatest variability, reflecting the larger sample size (n = 9) and greater diversity of hand hygiene practices at this market.
Machine swabs exhibited the most compact distributions across all markets, suggesting that grating equipment contributes a relatively uniform bacterial load to the product, a pattern consistent with the presence of established biofilms on machine surfaces, which maintain stable microbial populations that are largely independent of day-to-day variation in handling practices [37].
3.3.2. Escherichia coli Detection
Table 4 presents the results of presumptive E. coli detection disaggregated by market and sample type. Presumptive E. coli (identified by the characteristic metallic green colonies on EMB agar) was detected in 10 of 71 samples (14.1%). Detection rates differed significantly across markets (Fisher’s exact p = 0.001). Adelina recorded the highest prevalence, with 60% of its coconut samples and 60% of its machine swabs testing positive. By contrast, no E. coli was detected in any of the 29 samples collected from Xipamanine, suggesting that fecal contamination is localized rather than systemic throughout the market network. Among the three positive coconut samples from Adelina, the mean count was 329 CFU/g, exceeding the EU regulatory threshold of 100 CFU/g for ready-to-eat foods (EC No. 2073/2005)[38] — a benchmark adopted in this study given the absence of Mozambican national standards for fresh coconut products, and consistent with the risk-based approach advocated by the revised Codex Alimentarius General Principles of Food Hygiene (CXC 1-1969, Rev. 2020–2023), which emphasizes preventive food safety culture as a complement to end-product microbiological criteria (FAO/WHO, 2023) [39] — and representing a direct food safety concern.
Confirmed E. coli (Gram-negative rods, Kovacs indole-positive) was present on 14.9% of surface samples, with significant inter-market variation (Fisher's exact p = 0.006). While the present study did not extend to antimicrobial resistance profiling, this represents an important dimension for future investigation, given that recent work in Maputo has documented high rates of multidrug-resistant diarrheagenic E. coli in food and water sources consumed by vulnerable populations [40], raising concerns that faecal contamination of grated coconut may introduce not only pathogenic but also resistant strains into the food chain.
3.3.3. Staphylococcus aureus Detection
S. aureus was the most frequently detected pathogen in this study, recovered from 27 of 71 samples (38.0%). This prevalence is notable given the universally acceptable TMBC reported above, and may reflect the selective antimicrobial profile of coconut's endogenous lauric acid, which exerts preferential bactericidal activity against Gram-positive organisms in their planktonic state but is considerably less effective against surface-associated or biofilm-embedded populations of S. aureus [30], [36]. Detection rates across sample types were 29.2% for grated coconut, 47.8% for hand swabs, and 37.5% for machine swabs — the latter consistent with persistent biofilm-mediated colonization of grating surfaces, where sessile S. aureus communities embedded within an extracellular polymeric matrix can resist cleaning practices [30], [41]. Unlike E. coli, S. aureus prevalence did not differ significantly across markets (Fisher's exact p = 0.944), indicating that staphylococcal contamination is a pervasive, market-independent phenomenon driven by universal human carriage [42] rather than site-specific conditions.
Table 5 presents the results of the sequential confirmatory testing cascade applied to the 47 surface samples (23 hand swabs + 24 machine swabs). Of these, 26 (55.3%) were Gram-positive cocci, 24 (51.1%) were additionally catalase-positive, and 20 (42.6%) produced clot formation in the tube coagulase test, thereby confirming them as coagulase-positive S. aureus. It should be noted that identification relied exclusively on phenotypic biochemical tests; molecular confirmation (e.g., nuc gene PCR) was not performed, and the possibility that a proportion of coagulase-positive isolates may represent other coagulase-producing staphylococcal species cannot be entirely excluded, a methodological limitation addressed further in Section 4. The confirmatory prevalence was 47.8% on vendor hands and 37.5% on machine surfaces, supporting the interpretation that direct hand contact serves as the primary contamination vector [43].
Figure 3 synthesizes the pathogen detection data from Table 4 and Table 5 into a comparative visualization. The figure reveals the contrasting epidemiological profiles of the two pathogens: E. coli contamination is highly localized, absent from Xipamanine and concentrated in Adelina (40%), whereas S. aureus is uniformly distributed across all markets (range: 33.3–41.4%), consistent with its origin in human nasal and dermal carriage rather than environmental or water-borne sources [44], [45]. Notably, the persistence of S. aureus despite coconut's high lauric acid content, which preferentially suppresses planktonic Gram-positive organisms, likely reflects the protective effect of biofilm formation on hands and machine surfaces, where sessile staphylococcal communities exhibit substantially greater tolerance to both endogenous antimicrobials and external cleaning agents than their free-living counterparts[36], [46]. This contrast has direct implications for intervention design: E. coli could be controlled through site-specific water quality improvements, while S. aureus requires universal hand hygiene interventions combined with biofilm-disrupting machine sanitation protocols across all markets.
3.4. Classification Against Food Safety Standards
Table 6 presents the composite safety classification of the 24 grated coconut samples against three concurrent criteria. All 24 samples (100%) met the TMBC acceptability criterion (≤ 10,000 CFU/g). For E. coli, 21 samples (87.5%) were classified as satisfactory (≤ 100 CFU/g), while three samples (12.5%), all from Adelina market, exceeded the EU regulatory threshold of 100 CFU/g [47]. S. aureus was present in 7 coconut samples (29.2%) and absent in 17 (70.8%). When all three criteria were applied simultaneously, only 15 of 24 samples (62.5%) were classified as “Overall Safe,” meaning that more than one-third of the coconut product on sale in these markets failed to meet at least one safety benchmark.
Figure 4 disaggregates the composite classification by market, revealing substantial disparities. Xipamanine achieved the highest proportion of safe samples (80%), followed by Malanga (75%), Janete (60%), and Adelina (20%). The stacked bar chart demonstrates that the primary driver of non-compliance varies by market. In Xipamanine, Janete, and Malanga, the sole failure mode was S. aureus detection, whereas in Adelina, 40% of samples failed due to E. coli levels exceeding limits and a further 20% due to concurrent E. coli and S. aureus contamination. This variation identifies Adelina as the market posing the greatest composite food safety risk, requiring both water quality remediation and enhanced hand hygiene interventions.
Figure 4 provides composite safety classification of grated coconut samples by market (N = 24). Samples were classified based on three criteria applied simultaneously: TMBC, E. coli (EU Regulation EC 2073/2005 [48], and S. aureus (absent by coagulase test [49]). Green indicates samples meeting all criteria; other colours indicate the specific criterion or criteria not met.
4. Discussion
This study contributes to the microbiological safety literature concerning grated coconut sold in the municipal markets of Maputo. Its findings paint a nuanced picture: while general hygiene indicators (TMBC) fall within acceptable limits, the prevalence of specific pathogens, particularly S. aureus, reveal underlying contamination pathways that are masked by aggregate measures of bacterial load.
The overall hygiene compliance score of 48.6% signals that vendors satisfy fewer than half of the assessed hygiene criteria, a finding that is broadly consistent with, though slightly better than, earlier documentation of Maputo’s informal food sector, where 85.76% of food establishments received a “bad” Food Safety Index rating [17]. The complete absence of handwashing with soap across all 24 vendors is a critical deficit, given that contaminated hands are widely recognized as the single most important vehicle for transferring S. aureus from human skin to food products [12]. The organism asymptomatically colonizes the anterior nares and skin of 20–50% of healthy adults [50], and without effective handwashing, the probability of hand-to-food transfer during manual handling operations—such as packing grated coconut into plastic bags, is substantial. Comparable findings have been reported in Tanzania, where poor hand hygiene among market vendors was identified as a primary contributor to E. coli and S. aureus contamination of ready-to-eat foods [51], and in Morocco, where street food vendors with inadequate handwashing facilities exhibited significantly higher coliform counts on both hands and products [52].
The statistically significant inter-market variation in facility hygiene (p = 0.040) but not personal hygiene (p = 0.282) is a finding of considerable practical importance. It indicates that deficits in personal hygiene are systemic, uniformly pervasive across the entire market network, reflecting structural gaps in awareness, training, access to hygiene resources, and cultural norms, whereas facility-level conditions vary substantially depending on the physical infrastructure available at each site. The near-total absence of water facilities (4.2%) and the complete lack of toilet access at vending sites represent binding structural constraints that fundamentally preclude effective hygiene practice, regardless of vendor knowledge or intention. High levels of faecal contamination in water sources used by Maputo food vendors have been previously documented by [40], who demonstrated that 90% of water samples from informal distribution points exceeded WHO guidelines for faecal coliforms. The present findings confirm that these deficiencies persist and extend to the coconut vending subsector.
The universal detection of mesophilic bacteria (100%) at moderate levels (mean 2768 CFU/g) was anticipated, given the ubiquity of these organisms in food processing environments and on human skin. The fact that all coconut samples remained below the 10,000 CFU/g acceptability threshold may partly reflect the inherent antimicrobial properties of coconut flesh, particularly medium-chain fatty acids, notably lauric acid, which constitutes approximately 48% of coconut oil and possesses well-documented bactericidal and bacteriostatic activity against a range of Gram-positive organisms [53], [54]. However, a key lesson from the data is that acceptable TMBC must not be conflated with safety. The TMBC is an indicator of general hygienic quality and processing conditions, not of pathogen presence; a food product may exhibit low TMBC while simultaneously harbouring dangerous concentrations of E. coli or enterotoxigenic S. aureus [17], [20]. The present study substantiates this principle directly: despite universally acceptable TMBC, 37.5% of coconut samples failed at least one pathogen-specific criterion.
The detection of E. coli in 14.1% of all samples, with highly significant inter-market variation (p = 0.001), confirms that faecal contamination is localised rather than systemic. The concentration of positive samples in Adelina, where 60% of coconut and 60% of machine swabs tested positive, with a mean count of 329 CFU/g exceeding the EU regulatory threshold—represents a direct and actionable public health concern. This pattern closely mirrors findings from Brazil, where [24] recovered E. coli from the majority of shredded coconut samples in open-air markets in Belém. An apparent paradox emerges from the data: Adelina simultaneously recorded the highest facility hygiene score (63.6%) and the highest E. coli contamination. This seeming contradiction is resolved by the recognition that faecal contamination is primarily mediated by water quality rather than visible surface cleanliness. A market may appear clean and well-maintained while using water from a contaminated source, a scenario that [40] documented extensively in Maputo’s informal water distribution networks.
S. aureus was detected in 38% of all samples, with remarkably uniform prevalence across markets (p = 0.944), confirming that staphylococcal contamination is a system-wide phenomenon that transcends individual market conditions. This prevalence is lower than the 58% reported for coconut slices in India [23] but exceeds the 19.7% documented for ready-to-eat foods in Morogoro, Tanzania [51]. The observation that detection rates were highest on vendor hands (47.8%), intermediate on machines (37.5%), and lowest in the coconut product itself (29.2%) strongly supports the hand-to-food transfer hypothesis and identifies vendor hands as the primary reservoir. The confirmatory cascade revealed coagulase-positive S. aureus on 42.6% of surfaces, organisms capable of producing heat-stable enterotoxins responsible for staphylococcal food poisoning, one of the most common causes of foodborne illness globally [50].
The observation that 37.5% of machine swabs tested positive for S. aureus, comparable to the 47.8% prevalence on vendor hands, suggests that grating machines are not merely passive intermediaries but function as independent contamination reservoirs. This interpretation is reinforced by the finding that only 12.5% of vendors reported washing their machines regularly, while 33.3% of machines exhibited visible cracks, rust, or food residues. Such surface irregularities create sheltered micro-niches that facilitate bacterial attachment and biofilm formation, a process that is accelerated under the elevated temperatures and humidity characteristic of Maputo's tropical climate [28], [30]. Once established, biofilms on food-contact surfaces are remarkably resistant to removal by simple rinsing or wiping; studies have demonstrated that S. aureus biofilms on stainless steel can withstand conventional cleaning procedures and persist for weeks, serving as a continuous source of product recontamination during successive grating cycles [17]. The practical consequence is that even a vendor who practices adequate hand hygiene may still produce contaminated coconut if the grating machine itself harbours a mature biofilm. This finding underscores the need for intervention strategies that go beyond hand hygiene to include mandatory machine disassembly, scrubbing with detergent, and periodic sanitization with appropriate biocides — measures that are currently absent from the vending practices observed in this study.
The composite safety classification, in which only 62.5% of samples met all three criteria simultaneously, underscores the inadequacy of evaluating food safety through any single indicator in isolation. The pronounced inter-market gradient in composite safety (Xipamanine 80% vs. Adelina 20%) provides a clear evidence base for risk-stratified market surveillance. The absence of national microbiological standards for minimally processed coconut products in Mozambique constitutes a regulatory vacuum that leaves both enforcement agencies and consumers without objective benchmarks. Neither the Codex Alimentarius (which addresses desiccated coconut but not fresh grated coconut [55]) nor existing Mozambican food legislation provides applicable criteria. The development of product-specific national standards, informed by the baseline contamination data generated in this study, represents a necessary step toward formalizing food safety governance in this sector [56].
Several limitations merit acknowledgement. First, the cross-sectional design captured conditions at a single time point during the dry season (January–March), precluding assessment of seasonal variation in contamination patterns that may be expected given Maputo's pronounced wet/dry cycle. Additionally, S. aureus in coconut samples was assessed qualitatively (presence/absence by coagulase test) rather than quantitatively, limiting direct comparison against concentration-based thresholds such as those applied in EU regulations. Similarly, the reliance on phenotypic identification (Gram stain, catalase, tube coagulase) without molecular confirmation such as nuc gene PCR means that the reported S. aureus prevalence may include a small proportion of other coagulase-positive staphylococcal species, though the sequential three-test protocol employed substantially reduces this likelihood. Moreover, antimicrobial susceptibility testing was beyond the scope of this study, representing a significant gap given the documented prevalence of multidrug-resistant Enterobacteriaceae [40] and of S. aureus [57] in Maputo's informal food system. Finally, one hand swab was missing due to vendor unavailability, reducing the total sample count to 71.
Future studies should address these gaps by employing larger sample sizes, longitudinal designs spanning both wet and dry seasons, quantitative S. aureus enumeration using Baird-Parker agar with colony counting, molecular typing (e.g., spa typing or multilocus sequence typing) to characterise the enterotoxigenic potential and clonal relatedness of isolates, and systematic antimicrobial resistance profiling of both E. coli and S. aureus isolates to assess the extent to which contaminated grated coconut may serve as a vehicle for disseminating resistant strains into the community [58].
5. Conclusions
Grated coconut sold in Maputo’s municipal markets, while consistently meeting general mesophilic bacteria acceptability thresholds, carries significant microbiological safety risks attributable to widespread S. aureus contamination (38.0% of all samples) and localized fecal contamination indicated by E. coli (14.1% prevalence, concentrated in Adelina market). Only 62.5% of coconut samples met all three safety criteria simultaneously, and the composite safety rate ranged from 20% (Adelina) to 80% (Xipamanine), demonstrating marked inter-market heterogeneity. These findings are driven by systemic deficiencies in hygiene practices—particularly the universal absence of handwashing with soap—and inadequate market infrastructure, including the near-total lack of water facilities and sanitary installations.
The following five policy actions are recommended to address these gaps: (1) installation of handwashing stations with soap and clean water at all coconut vending sites; (2) implementation of mandatory periodic food safety training programs for vendors, with practical emphasis on hand hygiene and machine sanitation; (3) development and enforcement of national microbiological standards specifically for minimally processed coconut products; (4) establishment of mandatory machine maintenance and sanitation protocols, with particular attention to crack repair and rust prevention; and (5) creation of a routine market-level microbiological surveillance program integrated into the municipal public health system. Addressing these gaps would contribute meaningfully to reducing the foodborne disease burden in Mozambique and to advancing the targets of Sustainable Development Goal 3 (Good Health and Well-Being).
Author Contributions
Conceptualization, N.F.K. and B.T.M.; methodology, N.F.K. and C.M.S.; software, N.F.K.; validation, N.F.K. and C.M.S.; formal analysis, N.F.K.; investigation, N.F.K., A.A.K. and A.C.C.; data curation, N.F.K.; writing—original draft preparation, N.F.K.; writing—review and editing, N.F.K., C.M.S. and B.T.M.; visualization, N.F.K.; resources, B.T.M.; supervision, B.T.M. and C.M.S.; project administration, B.T.M. All authors have read and agreed to the published version of the manuscript.
Funding
Supported by the Center Of Excellence in Agri-Food Systems and Nutrition (CE-AFSN) in Mozambique. IDA grant number EO89-MZ
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki. Authorization for data collection was granted by the Municipality of Maputo, Municipal Council, Administration and Human Resource Management Ward (Ref.: SGM/DSMRH/DPDRH/2025/Class.024.1, dated 21 April 2025), following an Order of 10 April 2025 from the Councillor of the Administration and Human Resource Management Ward. A Presentation Guide (Guia de Apresentação No. 73/DMRH/2025, dated 17 April 2025) was issued to facilitate access to the municipal markets of Malanga, Adelina, Xipamanine, and Janete. Informed consent was obtained from all participating vendors prior to data collection.
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Data Availability Statement
The data presented in this study are openly available in Zenodo at https://doi.org/10.5281/zenodo.20487422.
Acknowledgments
The authors gratefully acknowledge the support of the Laboratory of Food Safety, Faculty of Veterinary Medicine, Eduardo Mondlane University, for providing laboratory facilities. The cooperation of the municipal market authorities and grated coconut vendors in Maputo is also gratefully acknowledged.
Conflicts of Interest
The authors declare no conflicts of interest.
Abbreviations
The following abbreviations apply in this manuscript:
| CAC | Codex Alimentarius Commission |
| CDC | Centers for Disease Control and Prevention |
| CFU | Colony-Forming Units |
| EMB | Eosin Methylene Blue |
| FAO | Food and Agriculture Organization |
| GHP | Good Hygiene Practices |
| INNOQ | National Institute for Standardization and Quality (Mozambique) |
| MISAU | Ministry of Health (Mozambique) |
| MSA | Mannitol Salt Agar |
| PCA | Plate Count Agar |
| SDG | Sustainable Development Goal |
| TMBC | Total Mesophilic Bacteria Count |
| WHO | World Health Organization |
References
- S. W. Adkins, M. A. Foale, and Y. Samosir, “Coconut revival: new possibilities for the ‘tree of life,’” Jan. 2006.
- S. AV and R.Ramki, “Production and Marketing of Coconut Products in Ernakulam District – An Empirical study,” International Journal of Engineering Technology and Management Sciences , vol. 7, no. 1, pp. 204–215, Jan. 2023. [CrossRef]. [CrossRef]
- U. A. Daa-Kpodé, D. Gustave, S. A. Edmond, V. S. Kolawolé, F. Baba-Moussa, and A. Kifouli, “Ethnobotanical study of the coconut palm in the Coastal Zone of Benin,” International Journal of Biodiversity and Conservation , vol. 13, no. 3, pp. 152–164, July 2021. [CrossRef]
- J. F. G. Ramírez, R. C. Muñoz, and J. W. Z. Sossa, “Innovations and trends in the coconut agroindustry supply chain: A technological surveillance and foresight analysis,” Frontiers in Sustainable Food Systems , vol. 7, Apr. 2023. [CrossRef]
- Jiaqi L., Xiaobing H., ShaoDan P., Wei Z., Fuming D., and Jihua L., “Effect of ultrafine grinding treatment on the nutritional and physicochemical properties of coconut pulp,” SHILAP Revista de lepidopterología , Feb. 2025. [CrossRef]
- A. G. Lamdande, M. Prakash, and R. KSMS, “Storage study and quality evaluation of fresh coconut grating,” Journal of Food Processing and Preservation , vol. 42, no. 1, May 2017. [CrossRef]
- A. Lamdande Gopalrao, M. Prakash, and R. S. K. S. M., “Storage study and quality evaluation of fresh coconut grating.,” CFTRI Institutional Repository , Jan. 2018.
- Z. Akbarbaglu, K. Sarabandi, S. H. Peighambardoust, R. Sarabandi, H. S. Kafil, and M. A. Hesarinejad, “Enzymatic modification of cold pressed coconut meal protein: nutritional, functional and biological properties,” Sustainable Food Technology , vol. 2, no. 5, pp. 1545–1557, Jan. 2024. .
- M. Nasrolahei, S. Mirshafiee, S. Kholdi, M. Salehian, and M. Nasrolahei, “Bacterial assessment of food handlers in Sari City, Mazandaran Province, north of Iran,” Journal of Infection and Public Health , vol. 10, no. 2, pp. 171–176, July 2016. [CrossRef]
- D. S. de Oliveira, “Micro-organismos mais prevalentes em mãos de manipuladores de alimentos,” Dec. 2018, Accessed: Nov. 2025. [Online]. Available: https://ri.ucsal.br/handle/prefix/790.
- H. Ebrahim and M. K. Wondimagegn, “Assessment of microbiological quality of some selected street vended foods, vendor’s safety practices, knowledge, and attitudes in Dessie Town, Ethiopia,” Scientific Reports , vol. 15, no. 1, Oct. 2025. [CrossRef]
- A. Amare, T. Worku, B. Ashagirie, M. Adugna, A. Getaneh, and M. Dagnew, “Bacteriological profile, antimicrobial susceptibility patterns of the isolates among street vended foods and hygienic practice of vendors in Gondar town, Northwest Ethiopia: a cross sectional study,” BMC Microbiology , vol. 19, no. 1, June 2019, doi: 10.1186/s12866-019-1509-4. [CrossRef]
- C. for D. C. and P. (CDC) Centers for Disease Control and Prevention (CDC), “Multistate Outbreak of Salmonella Typhimurium Infections Linked to Dried Coconut,” CDC, 2018. Available [online]: https://archive.cdc.gov/www_cdc_gov/salmonella/typhimurium-03-18/index.html.
- M. O. Edema, O. A. Temitope, and D. C. Innocent, “Evaluation of microbial hazards associated with the processing of Suya (a grilled meat product),” Scientific Research and Essays , vol. 3, no. 12, pp. 621–626, Dec. 2008.
- M. R. Adams, M. O. Moss, and P. McClure, Food Microbiology . Royal Society of Chemistry, 2016.
- M. Rhouma, M. Gaucher, B. Souhail, S. Békal, and P. Sandérs, “Food risk assessment in the farm-to-table continuum: report from the conference on good hygiene practices to ensure food safety,” Agriculture & Food Security , vol. 13, no. 1, May 2024. [CrossRef]
- A. M. Glória, de O. E. Susana, T. H. Claudia, M. L. Stefani, and C. Eduardo, “Assessments of good hygienic practice in food markets of Maputo, Mozambique and development of Food Safety Index,” African Journal of Food Science , vol. 13, no. 12, pp. 297–307, Dec. 2019.
- A. H. Havelaar et al. , “World Health Organization Global Estimates and Regional Comparisons of the Burden of Foodborne Disease in 2010,” PLoS Medicine , vol. 12, no. 12, Dec. 2015.
- S. L. Faife, C. Macuamule, J. N. Gichure, T. Hald, and E. M. Buys, “Diarrhoeagenic Escherichia coli and Salmonella spp. Contamination of Food and Water Consumed by Children with Diarrhoea in Maputo, Mozambique,” International Journal of Environmental Research and Public Health , vol. 21, no. 9, pp. 1122–1122, Aug. 2024. [CrossRef]
- A. Salamandane, A. C. Silva, L. Brito, and M. Malfeito-Ferreira, “Microbiological Assessment of Street Foods at the Point of Sale in Maputo (Mozambique),” Food Qual. Saf. , vol. 5, 2021.
- A. Salamandane, M. Malfeito-Ferreira, and L. Brito, “The Socioeconomic Factors of Street Food Vending in Developing Countries and Its Implications for Public Health: A Systematic Review,” Foods , vol. 12, no. 20, pp. 3774–3774, Oct. 2023.
- S. Luna et al. , “Outbreak of Salmonella Chailey Infections Linked To Precut Coconut Pieces — United States and Canada, 2017,” MMWR Morbidity and Mortality Weekly Report , vol. 67, no. 39, pp. 1098–1100, Oct. 2018.
- M. Ghosh, S. Wahi, M. Kumar, and A. Ganguli, “Prevalence of enterotoxigenicStaphylococcus aureusandShigellaspp. in some raw street vended Indian foods,” International Journal of Environmental Health Research , vol. 17, no. 2, pp. 151–156, Apr. 2007. [CrossRef]
- M. G. G. de Abreu, E. da S. Angelim, M. J. do S. F. Mendonça, and S. M. de A. Ribeiro, “Avaliação microbiológica de coco (Cocos nucifera) ralado comercializado em feiras livres do município de Belém, estado do Pará, Brasil,” Revista Pan-Amazônica de Saúde , vol. 9, no. 1, Mar. 2018.
- A. Hörnell et al. , “Perspective: An Extension of the STROBE Statement for Observational Studies in Nutritional Epidemiology (STROBE-nut): Explanation and Elaboration,” Advances in Nutrition , vol. 8, no. 5, pp. 652–678, Sept. 2017. [CrossRef]
- C. Lachat et al. , “Strengthening the Reporting of Observational Studies in Epidemiology – nutritional epidemiology (STROBE-nut): An extension of the STROBE statement,” Nutrition Bulletin , vol. 41, no. 3, pp. 240–251, Aug. 2016. [CrossRef]
- C. Faille, C. Cunault, T. Dubois, and T. Bénézech, “Hygienic design of food processing lines to mitigate the risk of bacterial food contamination with respect to environmental concerns,” Innovative Food Science & Emerging Technologies , vol. 46, pp. 65–73, Oct. 2017.
- C. Carrascosa, D. Raheem, F. Ramos, A. Saraiva, and A. Raposo, “Microbial Biofilms in the Food Industry—A Comprehensive Review,” International Journal of Environmental Research and Public Health , vol. 18, no. 4, pp. 2014–2014.
- L. M. Coughlan, P. D. Cotter, C. Hill, and A. Álvarez-Ordóñez, “New Weapons to Fight Old Enemies: Novel Strategies for the (Bio)control of Bacterial Biofilms in the Food Industry,” Frontiers in Microbiology , vol. 7. Frontiers Media, pp. 1641–1641, Oct. 18, 2016. [CrossRef]
- H. Flemming, J. Wingender, U. Szewzyk, P. D. Steinberg, S. A. Rice, and S. Kjelleberg, “Biofilms: an emergent form of bacterial life,” Nature Reviews Microbiology , vol. 14, no. 9, pp. 563–575, Aug. 2016. [CrossRef]
- R. Diane, “Practical food microbiology,” Jan. 2003, Accessed: Dec. 2025. [Online]. Available: https://www.slideshare.net/slideshow/practical-food-microbiology-3ed-edition-roberts-d/276599549.
- D. S. Katz, “Coagulase Test Protocol,” Am. Soc. Microbiol. , pp. 1–12, 2016.
- European Union, “Commission Regulation (EC) No 1441/2007 of 5 December 2007 Amending Regulation (EC) No 2073/2005 on Microbiological Criteria for Foodstuffs,” Off. J. Eur. Union , pp. 12–29, Dec. 2007, Accessed: Jan.2026. [Online]. Available: https://eur-lex.europa.eu/LexUriServ/LexUriServ.do?uri=OJ:L:2007:322:0012:0029:EN:PDF.
- H. Wickham, ggplot2 . Springer International Publishing, 2016.
- M. Simões, L. C. Simões, and M. J. Vieira, “A review of current and emergent biofilm control strategies,” LWT , vol. 43, no. 4. Elsevier BV, pp. 573–583, Jan. 05, 2010. [CrossRef]
- F. O. Nitbani, P. J. P. Tjitda, F. Nitti, J. Jumina, and A. I. R. Detha, “Antimicrobial Properties of Lauric Acid and Monolaurin in Virgin Coconut Oil: A Review,” ChemBioEng Reviews , vol. 9, no. 5, pp. 442–461, June 2022.
- S. G. Machado et al. , “The Biodiversity of the Microbiota Producing Heat-Resistant Enzymes Responsible for Spoilage in Processed Bovine Milk and Dairy Products,” Frontiers in Microbiology , vol. 8. Frontiers Media, Mar. 01, 2017. [CrossRef]
- A. Pietzka et al. , “Whole Genome Sequencing Based Surveillance of L. monocytogenes for Early Detection and Investigations of Listeriosis Outbreaks,” Frontiers in Public Health , vol. 7. Frontiers Media, June 04, 2019. [CrossRef]
- F. Marconi et al. , “Food safety culture in food companies: evaluation of the perception of food safety culture in three Tuscan food companies,” Italian Journal of Food Safety , vol. 12, no. 1, Mar. 2023.
- A. Salamandane, F. Vila-Boa, M. Malfeito-Ferreira, and L. Brito, “High Fecal Contamination and High Levels of Antibiotic-Resistant Enterobacteriaceae in Water Consumed in the City of Maputo, Mozambique,” Biology , vol. 10, no. 6, pp. 558–558, June 2021. [CrossRef]
- P. M. Schlievert and M. L. Peterson, “Glycerol Monolaurate Antibacterial Activity in Broth and Biofilm Cultures,” PLoS ONE , vol. 7, no. 7, July 2012.
- J. U. E. Sollid, A. Furberg, A.-M. Hanssen, and M. Johannessen, “Staphylococcus aureus: Determinants of human carriage,” Infection Genetics and Evolution , vol. 21, pp. 531–541, Apr. 2013.
- J. Schelin, N. Wallin-Carlquist, M. T. Cohn, R. Lindqvist, and G. C. Barker, “The formation ofStaphylococcus aureusenterotoxin in food environments and advances in risk assessment,” Virulence , vol. 2, no. 6, pp. 580–592, Nov. 2011. [CrossRef]
- A. Sakr, F. Brégeon, J. Mège, J. Rolain, and O. Blin, “Staphylococcus aureus Nasal Colonization: An Update on Mechanisms, Epidemiology, Risk Factors, and Subsequent Infections,” Frontiers in Microbiology , vol. 9. Frontiers Media, Oct. 08, 2018. [CrossRef]
- M. David and R. S. Daum, “Community-Associated Methicillin-ResistantStaphylococcus aureus: Epidemiology and Clinical Consequences of an Emerging Epidemic,” Clinical Microbiology Reviews , vol. 23, no. 3. American Society for Microbiology, pp. 616–687, July 01, 2010.
- D. Chieffi, F. Fanelli, and V. Fusco, “Antimicrobial and biocide resistance in Staphylococcus aureus: genomic features, decontamination strategies, and the role of S. aureus complex-related species, with a focus on ready-to-eat food and food-contact surfaces,” Frontiers in Food Science and Technology , vol. 3, May 2023. [CrossRef]
- “Scientific Opinion on the risk posed by pathogens in food of non-animal origin. Part 2 (Salmonella and Norovirus in leafy greens eaten raw as salads),” EFSA Journal , vol. 12, no. 3, Mar. 2014.
- D. L. Baggesen, A. N. Jensen, J. K. Andersen, J. Boel, A. Wingstrand, and T. Hald, “Vurdering fra DTU Fødevareinstituttet: Mikrobiologiske risici ved frugt og grønt,” Technical University of Denmark, Jan. 2012. Accessed: July 2025. [Online]. Available: https://orbit.dtu.dk/en/publications/vurdering-fra-dtu-f%C3%B8devareinstituttet-mikrobiologiske-risici-ved-/.
- F. Peles et al. , “Characterization of Staphylococcus aureus strains isolated from bovine milk in Hungary,” International Journal of Food Microbiology , vol. 118, no. 2, pp. 186–193, July 2007. [CrossRef]
- H. Wertheim et al. , “The role of nasal carriage in Staphylococcus aureus infections,” The Lancet Infectious Diseases , vol. 5, no. 12, pp. 751–762, Nov. 2005.
- J. N. Ndunguru and D. Ndossi, “Bacteriological Analysis of Ready-to-eat Foods from Morogoro Municipal Market,” Tanzania Veterinary Journal , vol. 37, pp. 17–24, Nov. 2020.
- J. Azanaw, G. T. Engdaw, H. Dejene, S. Bogale, and S. Degu, “Food hygiene knowledge, and practices and their associated factors of street food vendors in Gondar city, Northwest Ethiopia, 2021: A cross-sectional study,” Heliyon , vol. 8, no. 11, Nov. 2022.
- F. M. Dayrit, “The Properties of Lauric Acid and Their Significance in Coconut Oil,” Journal of the American Oil Chemists Society , vol. 92, no. 1, pp. 1–15, Nov. 2014. [CrossRef]
- P. Sandupama, D. Munasinghe, and M. Jayasinghe, “Coconut oil as a therapeutic treatment for alzheimer’s disease: a review,” Journal of Future Foods , vol. 2, no. 1, pp. 41–52, Mar. 2022.
- J. F. Leslie et al. , “A FoodSafeR perspective on emerging food safety hazards and associated risks,” Frontiers in Sustainable Food Systems , vol. 9, Oct. 2025.
- D. Grace, “Food Safety in Low and Middle Income Countries,” International Journal of Environmental Research and Public Health , vol. 12, no. 9, pp. 10490–10507, Aug. 2015. [CrossRef]
- A. Salamandane, A. C. Silva, L. Brito, and M. Malfeito-Ferreira, “Microbiological assessment of street foods at the point of sale in Maputo (Mozambique),” Food Quality and Safety , vol. 5, Nov. 2020.
- D. Aksoy, “Microbiological quality aspects of ready-to-eat foods with focus on antibiotic resistance and biofilm formation abilities of foodborne bacteria,” Acta Alimentaria , vol. 50, no. 3, pp. 433–441, July 2021.
Figure 1.
Hygiene compliance scores (Mean ± SD) across four municipal markets in Maputo.

Figure 2.
Distribution of total mesophilic bacteria count (log10 CFU) by sample type across four municipal markets.
Figure 2.
Distribution of total mesophilic bacteria count (log10 CFU) by sample type across four municipal markets.

Figure 3.
Detection rates (%) of presumptive E. coli (orange) and coagulase-positive S. aureus (purple) across four municipal markets and overall (N = 71).
Figure 3.
Detection rates (%) of presumptive E. coli (orange) and coagulase-positive S. aureus (purple) across four municipal markets and overall (N = 71).


Table 1.
Socio-demographic characteristics of grated coconut vendors (N = 24).
| Variable/Category | Frequency (n) | Percentage (%) |
|---|---|---|
| Sex | ||
| Female | 14 | 58.3 |
| Male | 10 | 41.7 |
| Age Group | ||
| 18-25 | 10 | 41.7 |
| 26-35 | 9 | 37.5 |
| 36-45 | 5 | 20.8 |
| Education Level | ||
| No formal education | 1 | 4.2 |
| Primary | 8 | 33.3 |
| Secondary | 15 | 62.5 |
Table 2.
Hygiene compliance scores by market.
| Market | n | Personal Hygiene (%) | Facility Hygiene (%) | Overall Hygiene (%) |
|---|---|---|---|---|
| Xipamanine | 10 | 50.0 ± 6.5 | 45.0 ± 12.6 | 47.5 ± 6.9 |
| Janete | 5 | 46.2 ± 7.7 | 54.6 ± 15.8 | 50.4 ± 10.3 |
| Malanga | 4 | 42.4 ± 4.4 | 36.4 ± 0.0 | 39.4 ± 2.3 |
| Adelina | 5 | 49.2 ± 8.7 | 63.6 ± 5.6 | 56.4 ± 3.7 |
| Overall | 24 | 47.8 ± 7.1 | 49.4 ± 14.1 | 48.6 ± 8.3 |
Kruskal-Wallis test: Personal p = 0.282; Facility p = 0.040; Overall p = 0.020. Values represent arithmetic mean ± standard deviation (SD). Personal hygiene was assessed across 13 checklist items; facility hygiene across 22 items; overall hygiene was computed as (personal hygiene % + facility hygiene %) / 2. Five personal hygiene items and two facility items were negatively worded (a “Yes” response indicated non-compliance); for these items, scores were inverted prior to computation. All items were equally weighted. Kruskal–Wallis test: personal hygiene H = 3.81, df = 3, p = 0.282; facility hygiene H = 8.30, df = 3, p = 0.040; overall hygiene H = 9.86, df = 3, p = 0.020. Item-level compliance rates are presented in Supplementary Table S1.
Table 3.
Total mesophilic bacteria count by sample type across all markets.
| Sample Type | n | Mean CFU | SD | Median | Min | Max | Mean Log10 | SD Log10 |
|---|---|---|---|---|---|---|---|---|
| Coconut | 24 | 3192 | 1514 | 3250 | 727 | 5455 | 3.44 | 0.26 |
| Hand | 23 | 2262 | 1331 | 2114 | 264 | 4850 | 3.25 | 0.36 |
| Machine | 24 | 2830 | 1216 | 2595 | 1082 | 5455 | 3.41 | 0.20 |
| Overall | 71 | 2768 | 1394 | 2500 | 264 | 5455 | 3.37 | 0.29 |
Table 4.
Presumptive E. coli detection by market and sample type.
| Market | Sample Type | n | Positive n (%) | Negative n (%) | CFU (positive) |
|---|---|---|---|---|---|
| Adelina | Coconut | 5 | 3 (60.0) | 2 (40.0) | 329 (mean) |
| Adelina | Hand | 5 | 0 (0.0) | 5 (100.0) | --- |
| Adelina | Machine | 5 | 3 (60.0) | 2 (40.0) | 298 (mean) |
| Janete | Coconut | 5 | 0 (0.0) | 5 (100.0) | --- |
| Janete | Hand | 5 | 1 (20.0) | 4 (80.0) | 318 (mean) |
| Janete | Machine | 5 | 0 (0.0) | 5 (100.0) | --- |
| Malanga | Coconut | 4 | 0 (0.0) | 4 (100.0) | --- |
| Malanga | Hand | 4 | 1 (25.0) | 3 (75.0) | 482 (mean) |
| Malanga | Machine | 4 | 2 (50.0) | 2 (50.0) | 532 (mean) |
| Xipamanine | Coconut | 10 | 0 (0.0) | 10 (100.0) | --- |
| Xipamanine | Hand | 9 | 0 (0.0) | 9 (100.0) | --- |
| Xipamanine | Machine | 10 | 0 (0.0) | 10 (100.0) | --- |
| Overall | All | 71 | 10 (14.1) | 61 (85.9) | --- |
Fisher’s exact test for E. coli detection by market: p = 0.001.
Table 5.
Confirmed S. aureus on contaminated surfaces by confirmatory test and market.
| Market | Surface | n | Gram+ | Catalase+ | Coagulase+ | Confirmed | Prevalence (%) |
|---|---|---|---|---|---|---|---|
| Adelina | Hand | 5 | 2 (40) | 2 (40) | 2 (40) | 2 | 40.0 |
| Adelina | Machine | 5 | 3 (60) | 2 (40) | 1 (20) | 1 | 20.0 |
| Janete | Hand | 5 | 3 (60) | 3 (60) | 3 (60) | 3 | 60.0 |
| Janete | Machine | 5 | 2 (40) | 2 (40) | 1 (20) | 1 | 20.0 |
| Malanga | Hand | 4 | 2 (50) | 1 (25) | 1 (25) | 1 | 25.0 |
| Malanga | Machine | 4 | 2 (50) | 1 (25) | 2 (50) | 2 | 50.0 |
| Xipamanine | Hand | 9 | 5 (56) | 5 (56) | 5 (56) | 5 | 55.6 |
| Xipamanine | Machine | 10 | 7 (70) | 8 (80) | 5 (50) | 5 | 50.0 |
| Overall | All | 47 | 26 (55) | 24 (51) | 20 (43) | 20 | 42.6 |
Table 6.
Composite safety classification of grated coconut samples.
| Safety Criterion | Classification | n | % |
|---|---|---|---|
| TMBC | Acceptable (≤ 10,000 CFU/g) | 24 | 100.0 |
| Marginal (10,001–100,000) | 0 | 0.0 | |
| Unsatisfactory (>100,000) | 0 | 0.0 | |
| E. coli | Satisfactory (≤ 100 CFU/g) | 21 | 87.5 |
| Unsatisfactory (>100 CFU/g) | 3 | 12.5 | |
| S. aureus | Absent | 17 | 70.8 |
| Present | 7 | 29.2 | |
| Overall Safety | All criteria met | 15 | 62.5 |
TMBC: general criteria. E. coli: EU Regulation EC 2073/2005. S. aureus: coagulase test.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2026 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



