Submitted:
21 May 2026
Posted:
22 May 2026
You are already at the latest version
Abstract
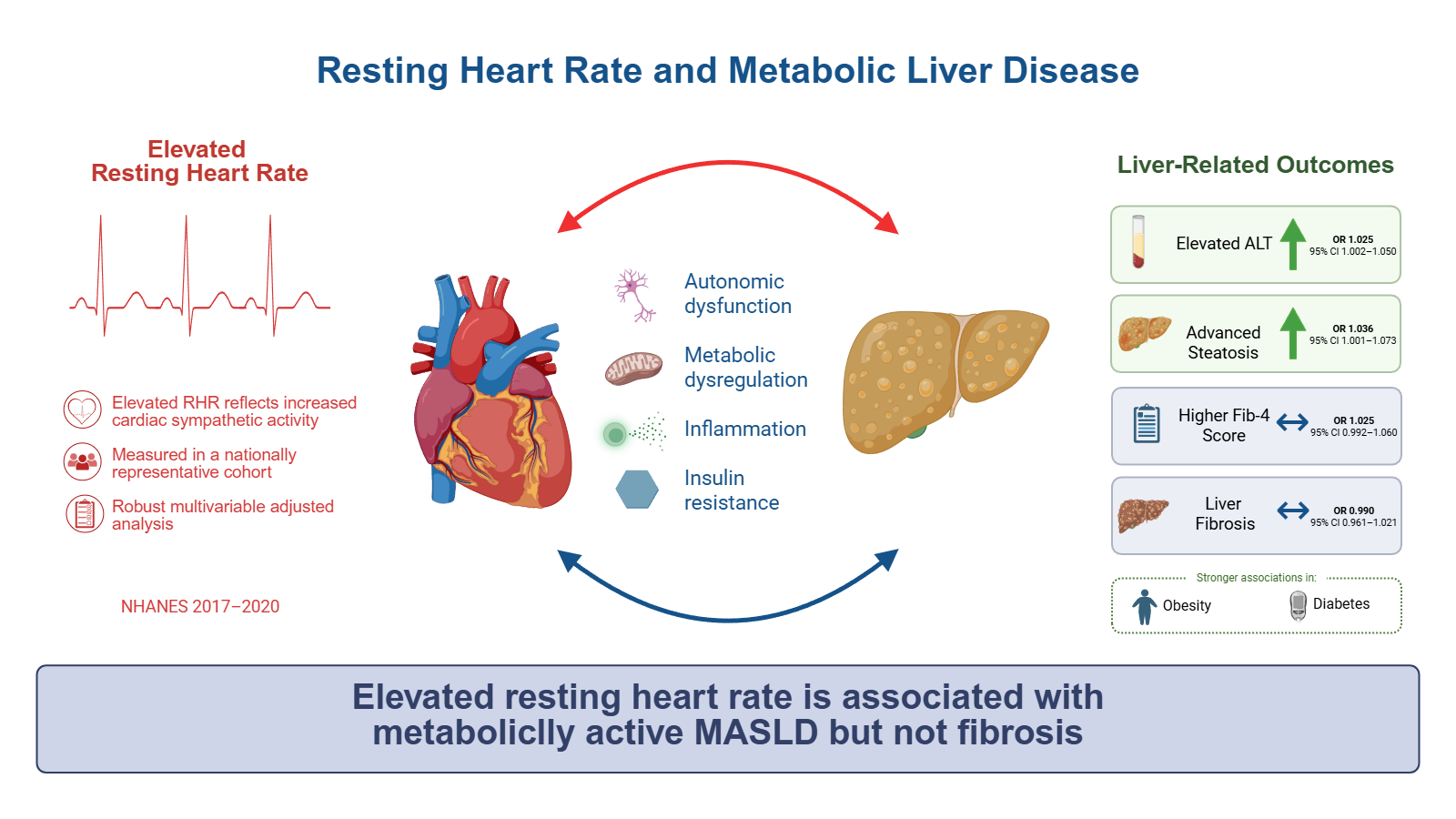
Background and Aims; Metabolic dysfunction–associated steatotic liver disease (MASLD) is closely linked to systemic cardiometabolic dysfunction. Resting heart rate (RHR), a marker of autonomic and metabolic stress, has been associated with metabolic syndrome and cardiovascular disease, though its relationship with MASLD remains incompletely characterized. We evaluated the association between RHR and liver-related outcomes in a nationally representative U.S. cohort. Materials and Methods; We analyzed adults aged 20–79 years from NHANES 2017–2020 with valid vibration-controlled transient elastography (VCTE) measurements. Participants with significant alcohol use, viral hepatitis, pregnancy, beta-blocker use, or missing key data were excluded. Liver outcomes included elevated alanine aminotransferase (ALT), advanced steatosis (CAP ≥290 dB/m), FIB-4 fibrosis category, and VCTE-defined fibrosis. Multivariable regression models adjusted for demographic and metabolic covariates were used to evaluate associations between RHR and liver-related outcomes. Results; A total of 3,567 adults were included. Each 1 beat-per-minute increase in RHR was independently associated with elevated ALT (OR 1.025, 95% CI 1.002–1.050, p=0.026) and advanced steatosis (OR 1.036, 95% CI 1.001–1.073, p=0.033). No significant association was observed between RHR and higher FIB-4 category (OR 1.025, 95% CI 0.992–1.060, p=0.150) or VCTE-defined fibrosis (OR 0.990, 95% CI 0.961–1.021, p=0.511). Associations with ALT and steatosis were attenuated after adjustment for glycemic and lipid parameters. Conclusions; Higher RHR was associated with steatosis-related and metabolic liver outcomes, but not fibrosis, in a nationally representative cohort. These findings suggest that RHR may reflect underlying autonomic and metabolic dysfunction relevant to early MASLD pathogenesis rather than advanced fibrotic disease.
Keywords:
metabolic dysfunction–associated steatotic liver disease (MASLD)
; resting heart rate
; vibration-controlled transient elastography
; hepatic steatosis
; FIB-4
; cardiometabolic dysfunction
; noninvasive liver fibrosis assessment
1. Introduction
Metabolic dysfunction–associated steatotic liver disease (MASLD) is the most common cause of chronic liver disease worldwide, affecting approximately 25% of the global population and closely paralleling the rising prevalence of obesity and type 2 diabetes mellitus [1]. Its pathogenesis is driven by complex interactions between insulin resistance, systemic inflammation, and excess visceral adiposity, placing MASLD within the broader spectrum of cardiometabolic disease [2].
Resting heart rate (RHR) is a readily obtainable physiologic measure that reflects autonomic nervous system activity and overall cardiometabolic stress. Dysregulation of autonomic balance, characterized by increased sympathetic and reduced parasympathetic activity, has been associated with metabolic abnormalities and shown to predict the development of metabolic syndrome [3,4]. Additionally, higher RHR has been linked to impaired glucose regulation, incident metabolic syndrome, and vascular dysfunction, including arterial stiffness [5,6,7,8]. These metabolic disturbances share key pathophysiologic mechanisms with MASLD, including insulin resistance and chronic low-grade inflammation.
A growing body of literature highlights a strong association between MASLD and cardiovascular disease. Observational studies and meta-analyses have demonstrated that MASLD is associated with increased risks of heart failure and major adverse cardiovascular events [9,10,11]. Mechanistic and translational studies further indicate that MASLD may contribute to cardiac remodeling and arrhythmogenesis through pathways involving systemic inflammation, metabolic dysregulation, and autonomic dysfunction [12,13].
Despite these overlapping pathophysiologic pathways, relatively few studies have directly evaluated the relationship between RHR and MASLD. Existing evidence remains limited, with some studies demonstrating an association between elevated RHR and nonalcoholic fatty liver disease (NAFLD) in select populations [14] and incomplete adjustment for key confounders and lacking fibrosis outcomes [15]. We hypothesized that elevated RHR would be associated with MASLD-related liver abnormalities in a heterogeneous population due to the aforementioned shared metabolic pathways.
We analyzed data from the National Health and Nutrition Examination Survey (NHANES) 2017–2020 to evaluate the association RHR and liver-related outcomes, including hepatic steatosis, liver enzyme elevation, and fibrosis. By incorporating vibration-controlled transient elastography (VCTE), FIB-4 scoring, and comprehensive adjustment for cardiometabolic factors, including beta-blocker use, this study aims to determine whether RHR may serve as a simple, low-cost marker for identifying individuals at increased risk for MASLD. To our knowledge, this is the first study to evaluate the association between resting heart rate and MASLD-related liver outcomes in a large and nationally representative U.S. cohort.
2. Materials and Methods
2.1. Study Population and Design
We analyzed data in adults aged 20–79 years using NHANES 2017–2020 cycles that provided valid VCTE measurements. This time frame was specifically selected because it represents the only recent NHANES cycle that simultaneously includes elastography data and detailed medication variables necessary to reliably exclude beta-blocker use. NHANES was utilized as a data source as it employs a complex, multistage probability sampling design to generate nationally representative estimates of the non-institutionalized U.S. population.
Individuals were excluded if they were pregnant, had evidence of chronic viral hepatitis, reported significant alcohol use (>14 drinks/week for men; >7 drinks/week for women), were taking beta-blockers, or had missing laboratory or elastography data required for analysis. The participant inclusion and exclusion process is illustrated in Figure 1.
2.2. Exposure Variable
RHR was calculated as the average of three standardized oscillometric measurements obtained at the time of survey participation in mobile examination centers, in accordance with NHANES protocols. RHR was analyzed as a continuous variable (per 1 beat per minute increment).
2.3. Outcome Definitions
Liver-related outcomes were defined as follows. Elevated alanine aminotransferase (ALT) was defined as >33 IU/L for men and >25 IU/L for women. Fibrosis risk was assessed using the FIB-4 index and categorized as low (<1.3), indeterminate (1.3–2.67), or high risk (>2.67) for study participants under aged 60. For participants 60 years of age and older at time of survey, FIB-4 index was categorized as low (<2.0), indeterminate (2.0-2.67), and high risk (>2.67). Hepatic steatosis was quantified using controlled attenuation parameter (CAP), with advanced steatosis defined as CAP ≥290 dB/m. Liver fibrosis severity was assessed using liver stiffness measurements (LSM) from VCTE and categorized as <8 kPa, 8–12 kPa, and >12 kPa. All liver-related outcome thresholds and fibrosis risk categories were selected based on commonly utilized cutoffs supported by American Association for the Study of Liver Diseases (AASLD) guidance and prior validated MASLD/VCTE literature [16].
2.4. Statistical Analysis
Multivariable logistic regression models were used to assess the association between continuous RHR and each liver-related outcome, adjusting for age, sex, body mass index (BMI), race/ethnicity, diabetes status, smoking status, and alcohol intake. For binary outcomes (elevated ALT and advanced steatosis), standard logistic regression was applied. For ordinal outcomes (FIB-4 category and fibrosis category), proportional odds logistic regression models were used, with the odds ratio interpreted as the odds of being in a higher-risk category per 1 bpm increase in RHR.
Effect modification was evaluated by including interaction terms between RHR and obesity status (BMI ≥30 kg/m²) and diabetes status (HbA1c ≥6.5%) in separate models. Statistically significant interactions were further explored through stratified analyses.
Discriminative performance of RHR alone and in multivariable-adjusted models was assessed using the area under the receiver operating characteristic curve (AUC/C-statistic) for elevated ALT and advanced steatosis.
All analyses incorporated NHANES sample weights, primary sampling units, and strata to account for the complex survey design and to produce nationally representative estimates. Statistical analyses were conducted using SAS 9.4, and statistical significance was defined as a two-tailed p-value <0.05.
3. Results
3.1. Study Population
A total of 3,567 adults aged 20–79 years with valid VCTE were included in the final analysis. The mean age was 47.8 years, 53.8% were male, and the mean RHR was 69.8 beats/min. The cohort had a mean BMI of 29.3 kg/m² and was racially and ethnically diverse. Baseline demographic and clinical characteristics are summarized in Table 1. This nationally representative sample provided a robust cohort to evaluate the association between RHR and liver-related outcomes.
3.2. Association Between Resting Heart Rate and Liver Outcomes
In multivariable logistic regression models adjusted for age, sex, BMI, race/ethnicity, smoking status, alcohol intake, and income-to-poverty ratio, higher RHR was independently associated with multiple liver-related outcomes.
Each 1-beat-per-minute increase in RHR was associated with higher odds of elevated ALT (OR 1.025, 95% CI 1.002–1.050, p=0.026) and advanced hepatic steatosis (OR 1.036, 95% CI 1.001–1.073, p=0.033). No significant association was observed between RHR and liver stiffness–defined fibrosis (OR 0.990, 95% CI 0.961–1.021, p=0.511) or higher FIB-4 category (OR 1.025, 95% CI 0.992-1.060, p=0.1498). Results are portrayed in Figure 1.
3.3. Effect Modification
Effect modification analyses demonstrated significant interactions between RHR and both obesity and diabetes status. Obesity modified the association RHR and elevated ALT, while diabetes modified the association with advanced steatosis. No significant interactions were observed for age, sex, or race/ethnicity.
In stratified analyses, the association between RHR and elevated ALT was more pronounced among individuals with obesity, while the association between RHR and advanced steatosis was stronger among individuals with diabetes (Table A1).
3.4. Sensitivity Analyses and Metabolic Covariate Adjustment
3.4.1. FIB-4 Category
RHR was not associated with liver stiffness–defined fibrosis category in the baseline model, and this null finding persisted across all adjusted models. Effect estimates remained small and non-significant regardless of covariate inclusion (Table A2).
3.4.2. Fibrosis
RHR was not associated with liver stiffness–defined fibrosis in the baseline model, and this null finding persisted across all adjusted models. Effect estimates remained small and non-significant regardless of covariate inclusion (Table A2).
3.4.3. Elevated ALT
The association between RHR and elevated ALT remained significant after adjustment for multiple cardiometabolic and inflammatory covariates, including ferritin, triglycerides, systolic blood pressure, C-reactive protein, HDL cholesterol, and sedentary time (all p<0.05). However, after adjustment for hemoglobin A1C, the association was attenuated and no longer statistically significant, with reversal in the direction of effect (AOR = 0.952, p=0.157), implying that glycemic status may partially explain the observed relationship (Table A2).
3.4.4. Steatosis
Similarly, the association between RHR and hepatic steatosis remained significant after adjustment for several cardiometabolic variables, including ferritin, systolic blood pressure, C-reactive protein, and sedentary time. However, adjustment for hemoglobin A1C attenuated the association and resulted in loss of statistical significance (AOR = 0.963, p=0.2735), with reversal in direction. Adjustment for triglycerides and HDL cholesterol also attenuated the association, though the direction of effect remained positive. These findings suggest that metabolic factors, particularly glycemic and lipid parameters, may partially account for the observed association (Table A2).
3.5. Discriminative Performance
RHR alone demonstrated limited discriminative ability for elevated ALT and advanced steatosis, with area under the receiver operating characteristic curve (AUC) values of 0.56 and 0.57, respectively (Figure 2).
In contrast, multivariable models incorporating RHR alongside established clinical and metabolic covariates demonstrated improved discrimination, with AUC values of 0.65 for elevated ALT and 0.66 for advanced steatosis (Figure 2). These findings indicate that while RHR alone has modest predictive utility, it may provide modest incremental value when incorporated into multivariable risk models.
Figure 3.
Receiver Operating Characteristic (ROC) Curves for Resting Heart Rate and Multivariable Models Predicting Elevated ALT and Advanced Steatosis.
Figure 3.
Receiver Operating Characteristic (ROC) Curves for Resting Heart Rate and Multivariable Models Predicting Elevated ALT and Advanced Steatosis.

4. Discussion
In this nationally representative analysis of U.S. adults, higher RHR was independently associated with elevated ALT and advanced hepatic steatosis, but was not significantly associated with either higher FIB-4 category or liver stiffness–defined fibrosis. These results propose that RHR is more closely linked to metabolically active liver disease, particularly steatosis and biochemical liver injury, rather than fibrosis risk. Associations with ALT and steatosis were attenuated after adjustment for hemoglobin A1C and lipid parameters, suggesting that the observed relationships are partially explained by underlying metabolic dysfunction. The observed effect modification by obesity and diabetes further supports this interpretation.
These results both align with and extend prior literature. Kim and Lee demonstrated an independent association between higher RHR and NAFLD in post-menopausal women, proposing autonomic imbalance, insulin resistance, and inflammation as potential mechanisms [14]. In a UK Biobank study, Jamialahmadi et al. showed that higher RHR was associated not only with fatty liver disease but also with cardiac remodeling phenotypes, supporting the concept that RHR reflects broader cardiometabolic dysfunction rather than isolated hepatic pathology [15]. Unlike these prior studies relying on specific populations, narrow imaging or limited covariate adjustment, our analysis incorporates VCTE and demonstrates that this association is most evident for steatosis-related and metabolic markers, while not extending to fibrosis as assessed by either FIB-4 or VCTE.
A key insight from our results is the agreement between FIB-4 and elastography-based fibrosis outcomes; RHR was not associated with higher FIB-4 category nor liver stiffness–defined fibrosis. This denotes that RHR is more closely tied to earlier and metabolically active stages of MASLD, such as hepatic steatosis and hepatocellular injury, rather than established fibrosis. Elevated RHR reflects increased sympathetic activity and reduced parasympathetic tone, which can contribute to insulin resistance through increased hepatic glucose production, enhanced lipolysis, and increased free fatty acid delivery to the liver [12,14]. These overlapping metabolic pathways may explain the attenuation seen after adjustment for A1C and lipid parameters. In contrast, fibrosis represents a chronic and cumulative process involving stellate cell activation, extracellular matrix deposition, and architectural remodeling that may not be reflected by a single physiologic parameter in a cross-sectional analysis [12].
More broadly, these results reflect the close relationship between MASLD and cardiovascular-metabolic disease. MASLD is increasingly recognized as a multisystem disorder linking hepatic metabolic dysfunction with cardiovascular remodeling. Emerging evidence has also demonstrated a strong association between MASLD and heart failure with preserved ejection fraction (HFpEF), with shared underlying mechanisms including systemic inflammation, insulin resistance, endothelial dysfunction, and myocardial remodeling [17]. Insulin resistance, sympathetic activation, and renin–angiotensin–aldosterone system activity contribute to both hepatic steatosis and cardiac remodeling, while excess fatty acid flux, lipotoxic intermediates, and oxidative stress promote myocardial dysfunction. In parallel, hepatic lipid accumulation drives systemic inflammation and release of cytokines and other mediators that contribute to cardiac remodeling, electrical instability, and autonomic dysfunction [12,13,15]. Together, these pathways help explain why RHR may reflect an integrated state of metabolic stress linking hepatic steatosis with more widespread cardiometabolic disease.
The observed effect modification by obesity and diabetes is consistent with this systemic model. MASLD is highly prevalent in these populations, and prior studies have shown that the cardiovascular consequences of NAFLD/MASLD are more pronounced in individuals with diabetes [15]. In our study, obesity amplified the association between RHR and ALT, while diabetes strengthened the association with steatosis, proposing that RHR is most informative in metabolically high-risk individuals.
From a clinical perspective, these findings align with current MASLD screening strategies, which emphasize identification of at-risk individuals followed by stepwise risk stratification using noninvasive tests such as FIB-4 and elastography [16,18]. RHR is unlikely to serve as a standalone screening tool given its limited discriminative ability; however, its consistent association with metabolic liver disease suggests that it may function as a simple, low-cost adjunctive signal prompting further evaluation, particularly in individuals with obesity or diabetes. Elevated RHR may help identify metabolically high-risk individuals who warrant further evaluation and risk-factor modification.
This study has several strengths, including the use of a large, nationally representative dataset, elastography-based assessment of liver disease, and comprehensive evaluation across multiple liver-related outcomes. The inclusion of detailed metabolic covariates and effect modification analyses allows for more nuanced interpretation of the physiologic relationships underlying these associations. The application of age-adjusted FIB-4 thresholds further strengthens the fibrosis analysis by accounting for the known influence of age on FIB-4 classification.
However, several limitations should be considered. The cross-sectional design limits causal inference, and RHR is influenced by multiple non-hepatic factors, including medications, fitness level, and comorbid conditions. Although key confounders were addressed more expansively than in prior studies, residual confounding remains possible. Additionally, while elastography improves phenotypic accuracy compared with ultrasound, it does not replace histologic assessment. Finally, the null findings for FIB-4 and VCTE-defined fibrosis should be interpreted in the context of a general population cohort, where advanced fibrosis prevalence may be relatively low and longitudinal progression cannot be assessed.
Future studies should evaluate whether elevated RHR identifies patients with MASLD who are more likely to develop worsening metabolic disease, cardiovascular complications, or progression of liver injury over time. This may be particularly important in patients with obesity or diabetes, where the relationship between RHR and liver outcomes appeared strongest in our analysis. Incorporating repeated RHR measurements alongside longitudinal liver assessments may help determine whether RHR is simply a marker of baseline metabolic risk or a useful signal of ongoing cardiometabolic and hepatic disease activity.
5. Conclusions
In conclusion, higher RHR was associated with steatosis-related and metabolic liver outcomes, including elevated ALT and advanced hepatic steatosis, but not with fibrosis as assessed by either FIB-4 or VCTE in a nationally representative cohort. These findings support the concept that RHR reflects underlying autonomic and metabolic dysregulation relevant to early MASLD pathogenesis rather than advanced fibrotic disease. The attenuation of associations after adjustment for glycemic and lipid parameters, along with stronger associations in obesity and diabetes, suggests that RHR functions as an integrative marker of systemic metabolic burden within a broader liver–heart metabolic axis. Although RHR demonstrated limited standalone predictive utility, it may serve as a simple adjunctive physiologic signal prompting further metabolic and liver risk assessment in high-risk populations. Future longitudinal studies may help clarify whether elevated RHR is a marker of early MASLD development or progressive metabolic liver dysfunction.
Author Contributions
Conceptualization, E.S. and P.G.; methodology, E.S. and J.M.; software, E.S. and J.M.; validation, E.S., J.M., and P.G.; formal analysis, E.S.; investigation, E.S., M.M., A.M., and A.A.-K.; resources, E.S.; data curation, E.S.; writing—original draft preparation, E.S., J.M., M.M., A.M., S.R., R.K., M.B., M.H.A.M., F.I.; writing—review and editing, E.S., A.A.-K., and P.G.; visualization, E.S.; supervision, P.G. and A.A.-K.; project administration, E.S.; funding acquisition, none. All authors have read and agreed to the published version of the manuscript.”
Funding
This research received no external funding.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Data Availability Statement
The original data presented in the study are openly available in the National Health and Nutrition Examination Survey (NHANES) 2017–2020 database at https://wwwn.cdc.gov/nchs/nhanes/continuousnhanes/default.aspx?Cycle=2017-2020.
Conflicts of Interest
The authors declare no conflicts of interest.
Abbreviations
| Abbreviation | Definition |
| HbA1c | Hemoglobin A1C |
| AASLD | American Association for the Study of Liver Diseases |
| ALT | Alanine Aminotransferase |
| AUC | Area Under the Curve |
| BMI | Body Mass Index |
| CAP | Controlled Attenuation Parameter |
| CI | Confidence Interval |
| ECG | Electrocardiogram |
| FFA | Free Fatty Acid |
| FIB-4 | Fibrosis-4 Index |
| HDL | High-Density Lipoprotein |
| HFpEF | Heart Failure with Preserved Ejection Fraction |
| IR | Insulin Resistance |
| kPa | Kilopascal |
| LSM | Liver Stiffness Measurement |
| MASLD | Metabolic Dysfunction–Associated Steatotic Liver Disease |
| NAFLD | Nonalcoholic Fatty Liver Disease |
| NHANES | National Health and Nutrition Examination Survey |
| OR | Odds Ratio |
| RAAS | Renin–Angiotensin–Aldosterone System |
| RHR | Resting Heart Rate |
| ROC | Receiver Operating Characteristic |
| SNS | Sympathetic Nervous System |
| VCTE | Vibration-Controlled Transient Elastography |
Appendix A

Table A1.
Stratified Associations Between Resting Heart Rate and MASLD Outcomes by Obesity and Diabetes Status.
Table A1.
Stratified Associations Between Resting Heart Rate and MASLD Outcomes by Obesity and Diabetes Status.
| Participants without Obesity | Participants with Obesity | |||||||
|---|---|---|---|---|---|---|---|---|
| AOR | 95%CI | P-value | AOR | 95%CI | P-Value | |||
| ALT | 1.001 | (0.974,1.029) | 0.9179 | 1.048 | (1.008,1.089) | 0.0194 | ||
| Fib-4 Category | 1.052 | (1.006,1.100) | 0.0291 | 1.007 | (0.957,1.060) | 0.7688 | ||
| Liver Fibrosis | 1.001 | (0.961,1.044) | 0.9511 | 0.990 | (0.955,1.026) | 0.5629 | ||
| Steatosis | 1.035 | (1.003,1.067) | 0.0344 | 1.053 | (1.002,1.107) | 0.0426 | ||
| Participants without Diabetes | Participants with Diabetes | |||||||
| AOR | 95%CI | P-value | AOR | 95%CI | P-value | |||
| ALT | 1.041 | (1.017,1.065) | 0.0014 | 0.982 | (0.935,1.032) | 0.4650 | ||
| Fib-4 Category | 1.034 | (0.995,1.075) | 0.0816 | 1.046 | (0.980,1.116) | 0.1672 | ||
| Liver Fibrosis | 1.008 | (0.962,1.057) | 0.7290 | 0.983 | (0.939,1.030) | 0.4578 | ||
| Steatosis | 1.050 | (1.017,1.085) | 0.0042 | 0.982 | (0.935,1.031) | 0.4528 | ||
Table A2.
Odds ratio results of sensitivity analysis.
| Outcome | Additional Covariate | Odds Ratio | 95% CI | p-value |
|---|---|---|---|---|
| Elevated ALT | ||||
| Baseline | 1.025 | 1.003–1.048 | 0.0357 | |
| Ferritin | 1.024 | 1.000–1.049 | 0.0496 | |
| Triglycerides | 1.023 | 1.001–1.045 | 0.0429 | |
| Systolic Blood Pressure | 1.026 | 1.001–1.052 | 0.0407 | |
| C-Reactive Protein | 1.028 | 1.004–1.052 | 0.0227 | |
| HDL Cholesterol | 1.023 | 1.000–1.047 | 0.0540 | |
| HbA1c (Last A1C) | 0.952 | 0.889–1.021 | 0.1571 | |
| Sedentary Minutes | 1.025 | 1.001–1.050 | 0.0412 | |
| FIB-4 Category | ||||
| Baseline | 1.025 | 0.992–1.062 | 0.1498 | |
| Ferritin | 1.026 | 0.992–1.062 | 0.1308 | |
| Triglycerides | 1.027 | 0.992–1.062 | 0.1240 | |
| Systolic Blood Pressure | 1.025 | 0.990–1.061 | 0.1498 | |
| C-Reactive Protein | 1.025 | 0.989–1.063 | 0.1643 | |
| HDL Cholesterol | 1.025 | 0.989–1.063 | 0.1647 | |
| HbA1c (Last A1C) | 1.054 | 0.990–1.122 | 0.0922 | |
| Sedentary Minutes | 1.026 | 0.991–1.062 | 0.1465 | |
| Liver Fibrosis | ||||
| Baseline | 0.990 | 0.961–1.021 | 0.5179 | |
| Ferritin | 0.991 | 0.962–1.022 | 0.5504 | |
| Triglycerides | 0.991 | 0.961–1.022 | 0.5407 | |
| Systolic Blood Pressure | 0.990 | 0.961–1.020 | 0.4898 | |
| C-Reactive Protein | 0.990 | 0.959–1.021 | 0.4998 | |
| HDL Cholesterol | 0.992 | 0.963–1.022 | 0.5717 | |
| HbA1c (Last A1C) | 0.983 | 0.932– 1.038 | 0.5200 | |
| Sedentary Minutes | 0.991 | 0.961–1.021 | 0.5273 | |
| Hepatic Steatosis | ||||
| Baseline | 1.036 | 1.001–1.073 | 0.0444 | |
| Ferritin | 1.036 | 1.001–1.073 | 0.0458 | |
| Triglycerides | 1.028 | 0.992–1.064 | 0.1197 | |
| Systolic Blood Pressure | 1.038 | 1.004–1.074 | 0.0294 | |
| C-Reactive Protein | 1.035 | 0.999–1.072 | 0.0596 | |
| HDL Cholesterol | 1.032 | 0.993–1.073 | 0.1087 | |
| HbA1c (Last A1C) | 0.963 | 0.897–1.033 | 0.2735 | |
| Sedentary Minutes | 1.033 | 1.001–1.066 | 0.0418 | |
Note: Odds ratios and 95% confidence intervals estimated via logistic regression for average heart rate (per 1 bpm). Bold values indicate statistical significance (p < 0.05). CI = Confidence Interval. Each row represents a model additionally adjusted for the listed covariate beyond the baseline covariates.
References
- Younossi, Z.M. The Global Epidemiology of Nonalcoholic Fatty Liver Disease and Nonalcoholic Steatohepatitis Among Patients With Type 2 Diabetes. Clin. Gastroenterol. Hepatol. 2024, 22(10), 1999–2010 e8. [Google Scholar] [CrossRef] [PubMed]
- Targher, G.; Byrne, C.D.; Tilg, H. MASLD: a systemic metabolic disorder with cardiovascular and malignant complications. Gut 2024, 73(4), 691–702. [Google Scholar] [CrossRef] [PubMed]
- Licht, C.M. Increased sympathetic and decreased parasympathetic activity rather than changes in hypothalamic-pituitary-adrenal axis activity is associated with metabolic abnormalities. J. Clin. Endocrinol. Metab. 2010, 95(5), 2458–66. [Google Scholar] [CrossRef] [PubMed]
- Licht, C.M.; de Geus, E.J.; Penninx, B.W. Dysregulation of the autonomic nervous system predicts the development of the metabolic syndrome. J. Clin. Endocrinol. Metab. 2013, 98(6), 2484–93. [Google Scholar] [CrossRef] [PubMed]
- Yang, Z. Resting heart rate and impaired glucose regulation in middle-aged and elderly Chinese people: a cross-sectional analysis. BMC Cardiovasc Disord. 2017, 17(1), 246. [Google Scholar] [CrossRef] [PubMed]
- Oda, E.; Aizawa, Y. Resting heart rate predicts metabolic syndrome in apparently healthy non-obese Japanese men. Acta Diabetol. 2014, 51(1), 85–90. [Google Scholar] [CrossRef] [PubMed]
- Park, B.J. Association between resting heart rate and arterial stiffness in Korean adults. Arch. Cardiovasc Dis. 2010, 103(4), 246–52. [Google Scholar] [CrossRef] [PubMed]
- Jiang, X. Metabolic syndrome is associated with and predicted by resting heart rate: a cross-sectional and longitudinal study. Heart 2015, 101(1), 44–9. [Google Scholar] [CrossRef] [PubMed]
- Mantovani, A. Risk of Heart Failure in Patients With Nonalcoholic Fatty Liver Disease: JACC Review Topic of the Week. J. Am. Coll. Cardiol. 2022, 79(2), 180–191. [Google Scholar] [CrossRef] [PubMed]
- Mantovani, A. Non-alcoholic fatty liver disease and risk of fatal and non-fatal cardiovascular events: an updated systematic review and meta-analysis. Lancet Gastroenterol. Hepatol. 2021, 6(11), 903–913. [Google Scholar] [CrossRef] [PubMed]
- Simon, T.G. Non-alcoholic fatty liver disease and incident major adverse cardiovascular events: results from a nationwide histology cohort. Gut 2022, 71(9), 1867–1875. [Google Scholar] [CrossRef] [PubMed]
- Zhou, J. Nonalcoholic Fatty Liver Disease and Cardiac Remodeling Risk: Pathophysiological Mechanisms and Clinical Implications. Hepatology 2021, 74(5), 2839–2847. [Google Scholar] [CrossRef] [PubMed]
- Chen, Z. Nonalcoholic Fatty Liver Disease: An Emerging Driver of Cardiac Arrhythmia. Circ. Res. 2021, 128(11), 1747–1765. [Google Scholar] [CrossRef] [PubMed]
- Kim, H.B.; Lee, Y.J. Association of resting heart rate with nonalcoholic fatty liver disease in postmenopausal women. Medicine 2020, 99(14), e19529. [Google Scholar] [CrossRef] [PubMed]
- Jamialahmadi, O. Fatty liver disease, heart rate and cardiac remodelling: Evidence from the UK Biobank. Liver Int. 2023, 43(6), 1247–1255. [Google Scholar] [CrossRef] [PubMed]
- Rinella, M.E. AASLD Practice Guidance on the clinical assessment and management of nonalcoholic fatty liver disease. Hepatology 2023, 77(5), 1797–1835. [Google Scholar] [CrossRef]
- Lian, L.Y. Heart failure with preserved ejection fraction and metabolic dysfunction-associated steatotic liver disease: Twin challenges, one metabolic solution. World J. Cardiol. 2025, 17(2), 103845. [Google Scholar] [CrossRef]
- Kanwal, F. Clinical Care Pathway for the Risk Stratification and Management of Patients With Metabolic Dysfunction-Associated Steatotic Liver Disease. Gastroenterology 2026. [Google Scholar] [CrossRef] [PubMed]
Figure 1.
Participant selection process for inclusion in the study analysis.

Figure 2.
Adjusted odds ratios for the association between resting heart rate and liver outcomes.

Table 1.
Baseline demographic and clinical characteristics of included participants.
 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2026 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



