Submitted:
15 May 2026
Posted:
18 May 2026
You are already at the latest version
Abstract
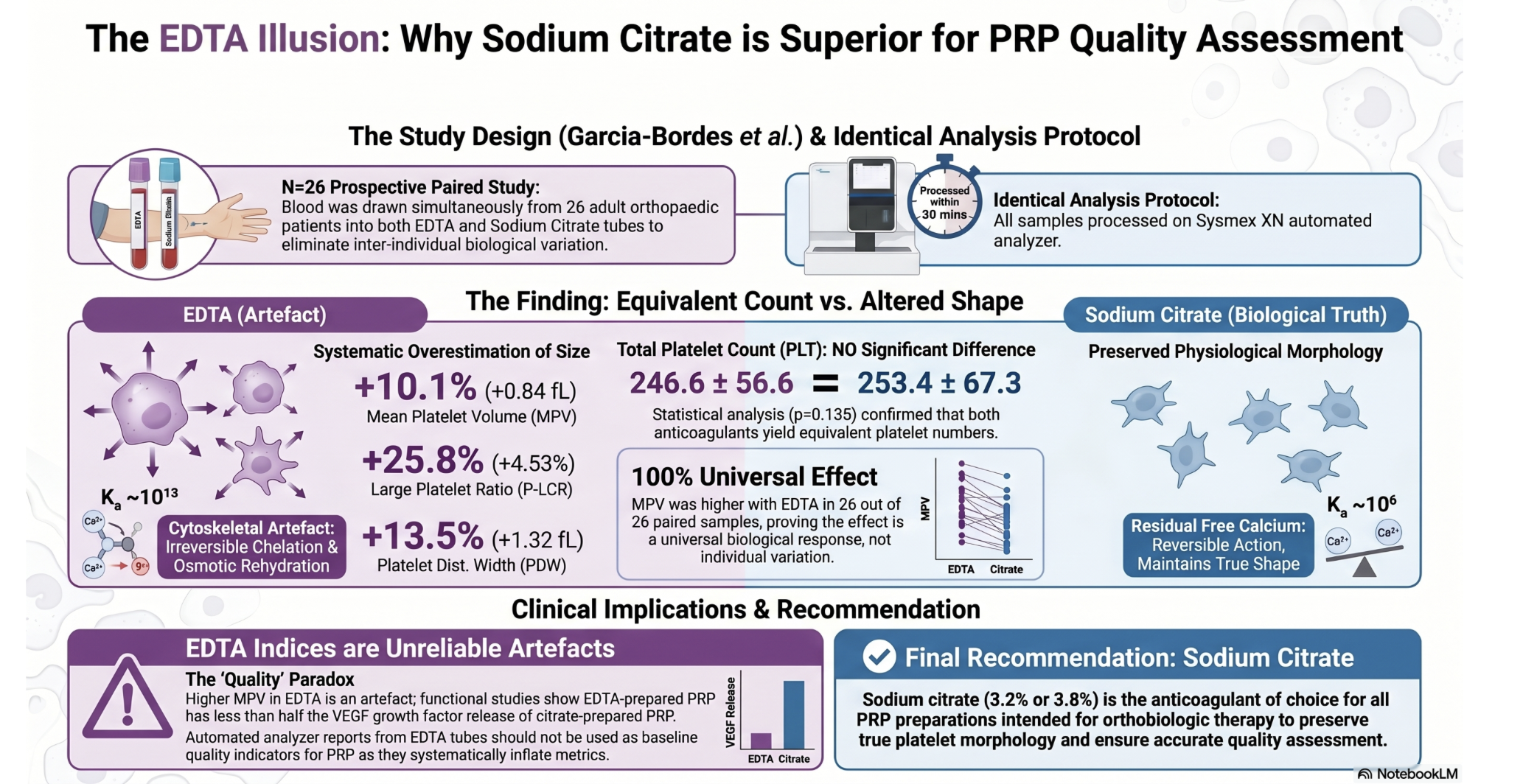
Background/Objectives: The anticoagulant used for blood collection is a fundamental but underexplored variable in platelet-rich plasma (PRP) preparation. Ethylenediaminetetraacetic acid (EDTA) and sodium citrate act on platelets through distinct calcium chelation mechanisms with potentially different consequences for PRP quality. Our group has previously demonstrated that biological and demographic variables independently modulate platelet composition in PRP; the present study extends this analysis to the pre-analytical anticoagulant variable. No prospective paired clinical study has systematically compared the effects of EDTA and sodium citrate on platelet morphological parameters in a real clinical setting. This study aimed to characterise these differences and evaluate their implications for orthobiologic therapy. Methods: A prospective within-subject paired-sample study was conducted at Instituto Cugat – Quirónsalud Barcelona (November 2025–April 2026). Twenty-six consecutive adult patients undergoing routine blood extraction prior to orthopaedic procedures had blood drawn simultaneously into K₂-EDTA and sodium citrate (3.2%) tubes. Full haematological analysis was performed on a Sysmex XN automated analyser within 30 minutes. Primary outcomes were mean platelet volume (MPV), platelet distribution width (PDW), large platelet ratio (P-LCR), large platelet cell count (P-LCC), and plateletcrit (PCT). Statistical comparisons used the paired t-test or Wilcoxon signed-rank test; effect sizes were quantified as Cohen's d. Results: Seven of eight platelet-related parameters differed significantly between anticoagulants (all p<0.001). Compared to sodium citrate, EDTA produced systematically higher MPV (+10.1%, d=2.81), P-LCR (+25.8%, d=2.41), P-LCC (+24.3%, d=1.70), PDW (+13.5%, d=1.33), PCT (+7.3%, d=0.78), RDW-CV (+2.0%, d=0.83), and RDW-SD (+2.6%, d=0.80). MPV was higher with EDTA in all 26/26 paired samples without exception. Total platelet count did not differ significantly (p=0.135). Effect sizes for all morphological parameters were large (d≥0.78). Conclusions: EDTA induces large, reproducible, and universal platelet morphological changes consistent with calcium chelation-induced swelling, not genuine platelet hypertrophy. These artefactual changes systematically overestimate platelet size and large platelet indices by up to 26%, with direct implications for PRP quality assessment in orthobiologic medicine. Sodium citrate should remain the anticoagulant of choice for PRP preparation. Clinicians using EDTA must recognise that morphological parameters do not reflect functional platelet capacity.
Keywords:
platelet-rich plasma
; PRP
; EDTA
; sodium citrate
; anticoagulant
; mean platelet volume
; platelet morphology
; platelet distribution width
; large platelet ratio
; orthobiologics
; regenerative medicine
; orthopedic surgery
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



