Submitted:
12 May 2026
Posted:
13 May 2026
You are already at the latest version
Abstract
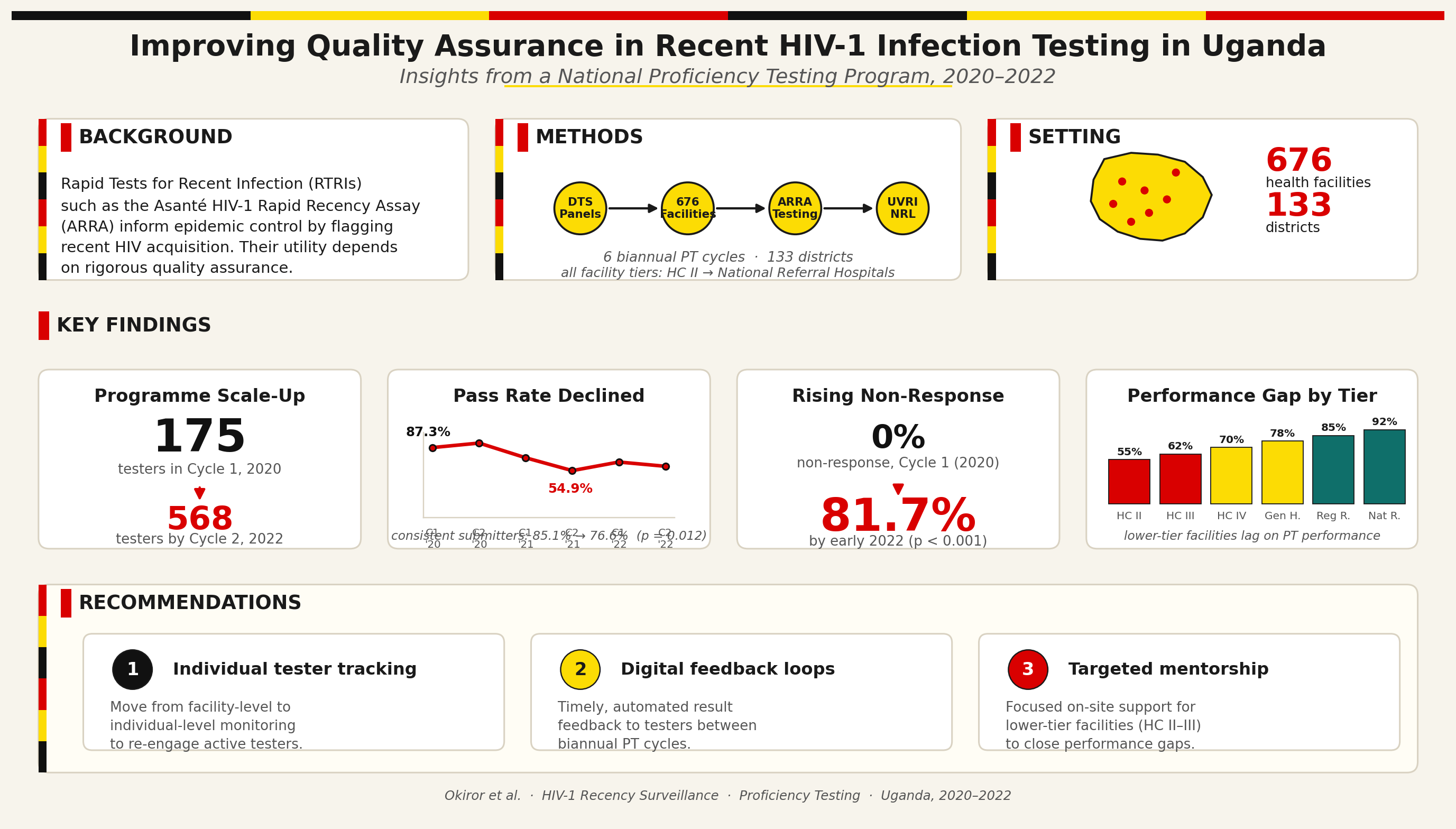
Background: To inform epidemic control, Rapid Test for Recent Infection (RTRI) assays, such as the Asanté HIV-1 Rapid Recency Assay (ARRA), have been developed to detect potential signals of increased HIV acquisition. However, ensuring the accuracy of these tests remains a challenge in resource-limited settings. While ARRA has been implemented for surveillance, there is a lack of documented experiences and lessons learned regarding quality assurance through Proficiency Testing (PT). This study examined Uganda's recent HIV infection PT program from 2020 through 2022 to highlight challenges and successes of implementation in resource-limited settings. Methods: We analyzed proficiency testing (PT) implementation for HIV recency testing in Uganda from 2020–2022. The study included biannual PT cycles (Cycle 1: Jan–Jun, Cycle 2: Jul–Dec) across 676 facilities in 133 districts. We assessed performance using pass rates (percentage of testers correctly identifying all samples in a PT panel) and response rates (proportion of testers submitting results within the stipulated timeframe out of the total number expected to participate). To evaluate sustainability, we longitudinally tracked a fixed cohort of the first 175 testers enrolled at the project's inception, representing diverse facility levels and cadres. Results: Analysis of six proficiency testing cycles from 2020-2022 revealed two key trends: a significant expansion in program participation and a concurrent longitudinal decline in performance among a consistent cohort. Overall, participation grew from 175 testers in Cycle 1, 2020, to 568 testers by Cycle 2, 2022. Among all participating facilities in each cycle, pass rates fluctuated, ranging from a high of 87.3% (Cycle 2, 2020) to a low of 54.9% (Cycle 2, 2021). A longitudinal analysis of the initial 175-testing-site cohort, however, revealed a significant inverse relationship between participation and performance. Non-response within this cohort increased drastically from 0% to 81.7% by early 2022 (p-value for trend <0.001). Among the diminishing subset of sites that continued to submit results, the pass rate showed a statistically significant declining trend, from 85.1% to 76.6% over the study period (p-value for trend = 0.012). Conclusion: This study identified three critical challenges: a steep rise in non-response, declining pass rates, and persistent performance gaps at lower-level health facilities. To address these gaps, we recommend individual tracking with digital feedback and targeted mentorship to re-engage staff and sustain competency at lower-level facilities.
Keywords:
HIV-1 recent infection
; proficiency testing
; quality assurance
; HIV surveillance
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



