Submitted:
05 May 2026
Posted:
06 May 2026
You are already at the latest version
Abstract
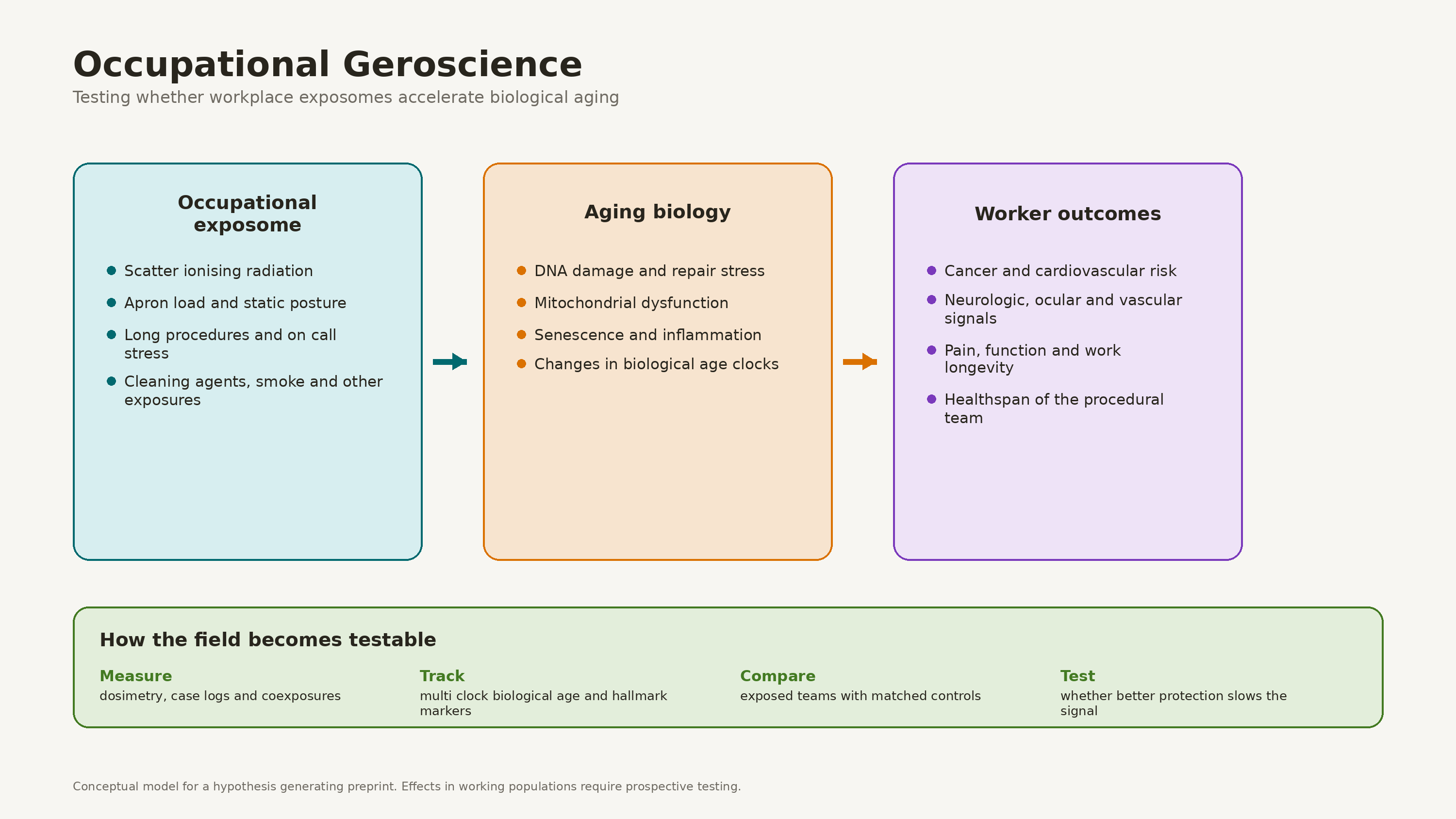
Occupational Geroscience is proposed here as a new scientific discipline at the intersection of geroscience and occupational medicine. It studies how chronic occupational exposomes activate the hallmarks of aging in workforces with defined biological hazards. The primary outcome is the slope of multi-clock estimators of biological age over a career-length follow-up in an exposed cohort versus a matched unexposed comparator. Hallmark-specific markers (γ-H2AX, telomere length, SASP cytokines, cf-mtDNA) are measured alongside, and each worker's lifetime dose record is linked to the biomarker series.Existing exposome aging studies measure population scale environmental drivers without isolating defined occupational cohorts. Existing occupational radiation cohorts measure cancer mortality without measuring biological aging. What is missing is a longitudinal outcome that spans systems, is anchored in the hallmarks of aging, and is tied to a defined occupational exposome with prospective dose data; such an outcome has not yet been established. That gap motivates naming the field.The founding case is fluoroscopy guided interventional medicine. Scatter ionising radiation, biomechanical loads, psychological strain, and material co-exposures plausibly activate several hallmarks of aging across careers that involve thousands of procedures. Cell and animal studies support key elements of the mechanism. Working populations have not yet been studied prospectively, and a cohort study is needed to test the prediction directly.This paper defines Occupational Geroscience by its object, methods, and predictions, and sets inclusion and exclusion criteria. The research agenda begins with a population-level registry and a modular longitudinal biomarker cohort. Shielding analyses can then be nested within the cohort, while tiered radiosensitivity profiling and biological mitigation trials, including the antioxidant pre-exposure trial (Study 5), should follow only after feasibility, safety, and primary cohort signals are established. The interventional studies are hypotheses to be tested, not proven preventive methods.
Keywords:
occupational geroscience
; occupational radiation exposure
; biological aging
; geroscience
; interventional medicine
; radiation protection
; ALARA
; dosimetry
; exposome
; healthspan
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



